Embed Size (px)
Citation preview

THE PROSTHETIC PROBLEMS OF BELOW KNEE AMPUTEES
THE PROSTHETIC PROBLEMS OF BELOW KNEE AMPUTEESWITH FLEXION CONTRACTURES1
P. J. BANNISTER, DIP.PHTY.
Repatriation Artificial Limb and Appliance Centre, New South Wales
21
It has always been difficult to pravide thepatient who has had a below knee amputationand has a fixed flexion contracture, with asuitable artificial limb. The adaptation of thePatellar Tendon Bearing (PTB) below kneeprosthesis and the subsequent SupracondylarVariation ePTS) of this type of prosthesishas been applied to this problem.
The aim of the surgeon when doing anamputation is to preserve the knee jointwherever possible, and the last fifteen yearshave seen a considerable increase in the per..centage of below knee amputees. As this trendhas continued, the number of patients withknee flexion contractures has grown. In thepast the patients with severe knee flexioncontractures could not he fitted with a con..ventional below knee leg but were fitted withan appliance called a kneeling knee hearer.This was made with the patient's knee fixedin 90° flexion and had a shank which couldswing freely from a hinge located at kneelevel. It served the patient moderately well asan aid to mobility although the patient's kneewas not used and he was walking with all thebiomechanical disadvantages of an above kneeamputee.
At N.S.W. R.A"L.A.C. an alternative suspension to the conventional thigh lacing sus..pension for a kneeling knee bearing prosthesishas heen tried, with marked success on twopatients who had flexion contractures greaterthan 40°. This has involved the use of thePTB principle, the value of which is thatwhatever remaining function is left in theknee is used so that the patient is effectivelywalking with the loss of only the ankle joint.
The contractnres may develop before orafter surgery. In some patients their flexioncontracture is already present, before ampu-
lReceived March, 1977.
tation, because of j oint disease or prolongedinactivity resulting from peripheral ischaemiaand associated surgery. These patients areusually old and if vascular disease has affectedtheir peripheral vessels, then the coronaryand cerebral vessels may also be affected.Those who have suffered a cerebrovascularaccident either before or after amputationare particularly prone to flexion contracturesbecause of varying degrees of paresis andmuscular imbalance. It is clearly very dif..ficult to prevent flexion contractures insome geriatric patients, particularly thosewho have had a long debilitating illness priorto surgery and it is unwise to wait in thehope that prolonged intensive physiotherapywill increase the range of knee movementdramatically. The patient's most urgentpsychological need is to look normal; whetherin a wheelchair or using crutches a patientfeels and is less conspicuous with two legs.This is evidenced by the number of womenwho continue to wear long skirts until theyare fitted with a prosthesis. Up until now thethigh lacing kneeling knee hearer has beenthe only answer for these people who havesevere flexion contracture.
A thigh lacing kneeling knee hearer closelyresembles a conventional thigh lacing pros..thesis, the design of which has changed littlein the last 150 years. In the early nineteenthcentury with advent of anaesthetics and improved surgical procedures, more patientssurvived surgery and this, coupled with thewars in the first half of the century, causedan increase in the amputee population whichresulted in a greater emphasis on giving theamputees a useful replacement of their limb.With the accent slowly shifting from surgeryto save life, to consideration of the qualityof the life that was saved, the nineteenth century pr-oduced many varieties of below kneelegs but the basic principles of such early
Aust.!.Physiother., XXIV, 1, March, 1978
22 THE AUSTRALIAN JOURNAL OF PHYSIOTHERAPY
designs as the Verduin Leg (1696) and theAnglesea Leg (1800) remained until the1950's.
The Anglesea Leg, so named for the Marquis of Anglesea for whom it was made, hadan articulated foot, a hollow wooden shankand a leather thigh corset attached to theshank with metal side-bars and hinges. A fairpercentage of the patient's weight was trans...mitted directly through the thigh corset andsuspension was maintained by it during theswing phase of walking. The modern thighlacing leg is virtually the same as the legdescribed above, the leg is still made of wood,leather, metal and rubber, the only additionalmaterial used is plastic to reinforce thewooden shank, and the articulated foot hasbeen replaced with a rubber SACH (solidankle cushion heel) foot.
The kneeling knee bearer itself has beenknown in various forms for hundreds ofyears, serving as a useful support and aidto mobility.
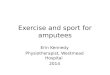
FIGURE 1
Chelsea. Peg c. early Eighteenth Century.
Aust.l.Phrsiother., XXIV, 1, March, 1978
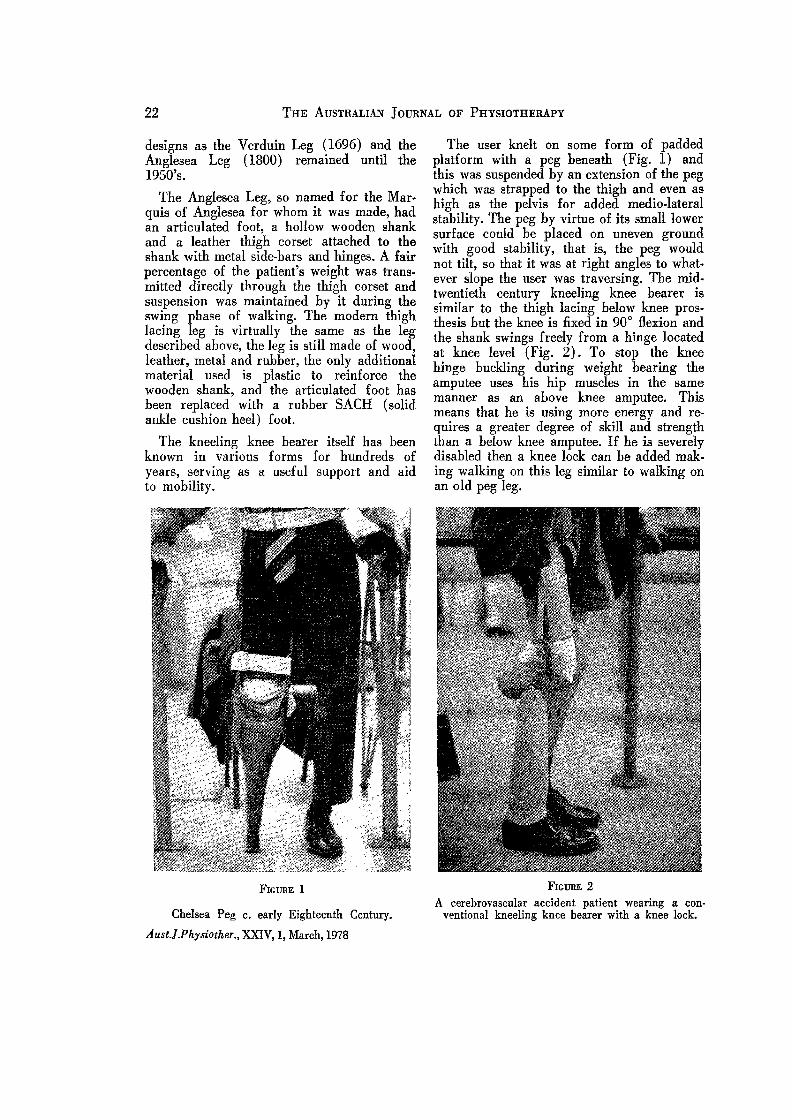
The user knelt on some form of paddedplatform with a peg beneath (Fig. 1) andthis was suspended by an extension of the pegwhich was strapped to the thigh and even ashigh as the pelvis for added medio-lateralstability. The peg by virtue of its small lowersurface could be placed on uneven groundwith good stability, that is, the peg wouldnot tilt, so that it was at right angles to what..ever slope the user was traversing. The mid..twentieth century kneeling knee hearer issimilar to the thigh lacing below knee prosthesis but the knee is fixed in 900 flexion andthe shank swings freely from a hinge locatedat knee level (Fig. 2). To stop the kneehinge buckling during weight hearing theamputee uses his hip muscles in the samemanner as an above knee amputee. Thismeans that he is using more energy and requires a greater degree of skill and strengththan a below knee amputee. If he is severelydisabled then a knee lock can he added mak..ing walking on this leg similar to walking onan old peg leg.
FIGURE 2A cerebrovascular accident patient wearing a con
ventional kneeling knee bearer with a knee lock.
THE PROSTHETIC PROBLEMS OF BELOW KNEE AMPUTEES 23
After WarId War II, because of the in·crease in the amputee population, there wasa great deal of research by the American"Artificial Limb Programme" aimed at improving the design of prostheses. The basicproblem of below knee legs resulted from theconflict between the single axis of the prosthetic j oint and the changing axes of thepolycentric anatomical knee joint. In con..sequence where the corset is firmly attachedto the thigh the stump moves in and {Jut ofthe socket as the knee flexes and extends andthis causes damage to the skin.
In 1958 the Biomechanics Laboratory ofthe University of California published itswork on the PTB (Patellar Tendon Bearing)prosthesis. It consists of a SACH foot, ashank of hollow wood reinforced by a plasticlaminate and a total contact (supporting alltissues of the stump) plastic socket lined withsoft leather and Kemblo rubber. The frontand sides of the socket are higher than thesocket of a thigh lacing leg (level with themid..patella) to give greater medio..lateralstability in place of the side..bars and corset.Suspension is attained by means of a leatherstrap above the patella.
The advantages of this leg are that it islighter and less cumbersome, the intimate fitof the socket allows minimal movement hetween the socket and stump and the patientcan walk with a near normal gait, that is, hisknee remains in a few degrees of flexionthroughout stance. Total contact providesbetter proprioception and the support fordistal tissues prevents the development ofoedema and cyanosis often leading to Verrucous Hyperplasia sometimes seen on stumpsfitted with open ended sockets.
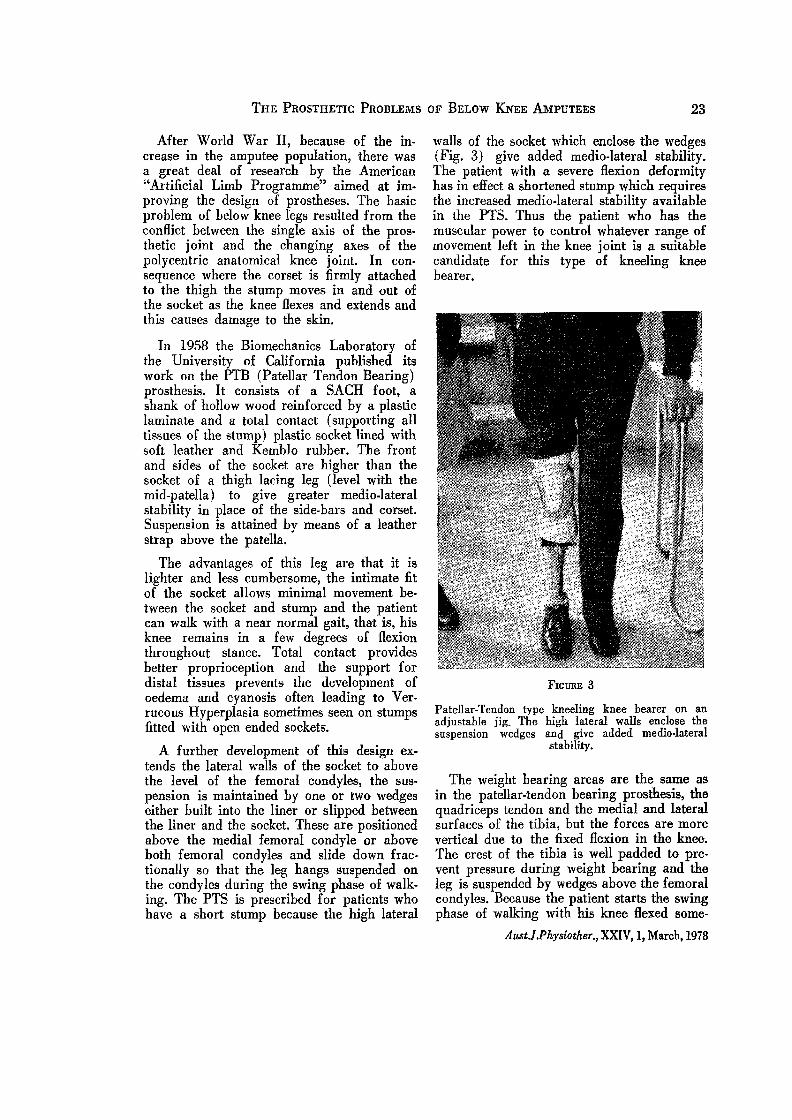
A further development of this design extends the lateral walls of the socket to abovethe level of the femoral condyles, the sus·pension is maintained by one or two wedgeseither built into the liner or slipped betweenthe liner and the socket. These are positionedabove the medial femoral condyle or aboveboth femoral condyles and slide down fractionally so that the leg hangs suspended onthe condyles during the swing phase of walk.ing. The PTS is prescribed for patients whohave a short stump because the high lateral
walls of the socket which enclose the wedges(Fig. 3) give added medio..lateral stability.The patient with a severe flexion deformityhas in effect a shortened stump which requiresthe increased medio-Iateral stability availablein the PTS. Thus the patient who has themuscular power to control whatever range ofmovement left in the knee joint is a suitablecandidate for this type of kneeling kneebearer.
FIGURE 3
Patellar..Tendon type kneeling knee bearer on anadjustable jig. The high lateral walls enclose thesuspension wedges and give added medio·lateral
stability.
The weight hearing areas are the same asin the patellar-tendon hearing prosthesis, thequadriceps tendon and the medial and lateralsurfaces of the tibia, hut the forces are morevertical due to the fixed flexion in the knee.The crest of the tibia is well padded to prevent pressure during weight hearing and theleg is suspended by wedges above the femoralcondyles. Because the patient starts the swingphase of walking with his knee Hexed some..
Aust.!.Physiother., XXIV, 1, March, 1978
24 THE AUSTRALIAN JOURNAL OF PHYSIOTHERAPY
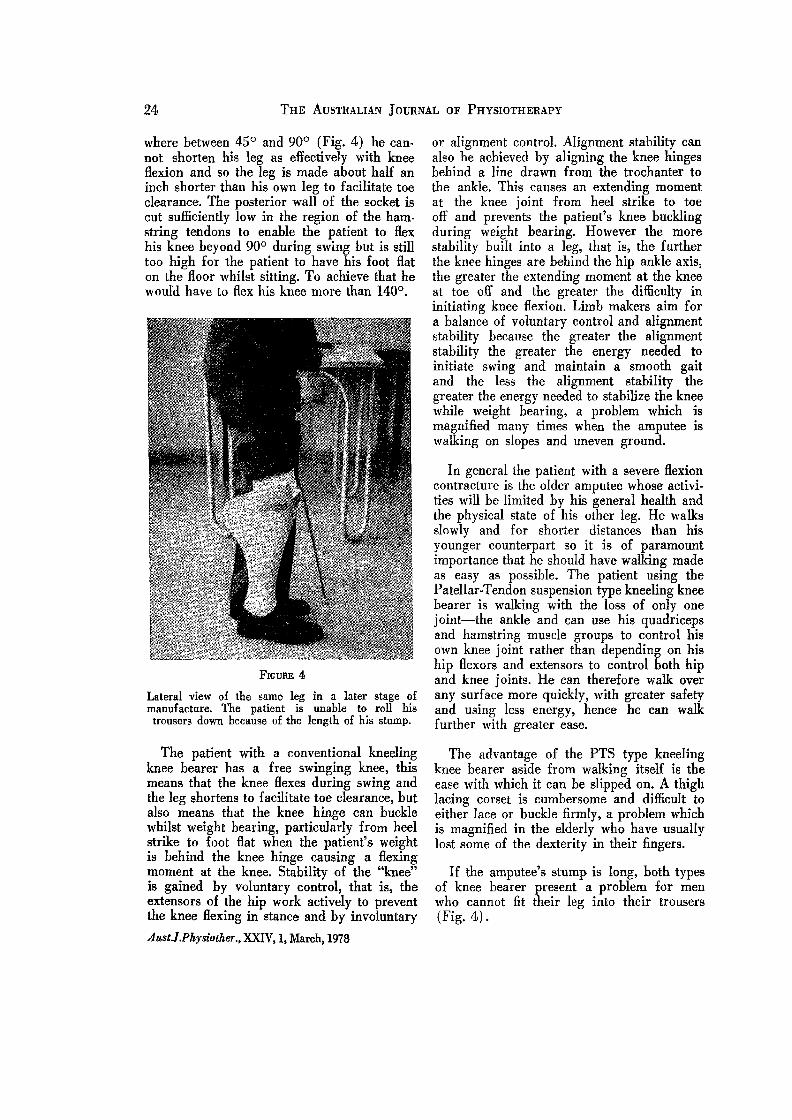
where between 45° and 90° (Fig. 4) he cannot shorten his leg as effectively with kneeflexion and so the leg is made about half aninch shorter than his own leg to facilitate toeclearance. The posterior wall of the socket iscut sufficiently low in the region of the ham~
string tendons to enable the patient to flexhis knee beyond 900 during swing hut is stilltoo high for the patient to have his foot flaton the floor whilst sitting. To achieve that hewould have to flex his knee more than 1400 •
FIGURE 4
Lateral view of the same leg in a later stage ofmanufacture. The patient is unable to roll histrousers down because of the length of his stump.
The patient with a conventional kneelingknee hearer has a free swinging knee, thismeans that the knee Hexes during swing andthe leg shortens to facilitate toe clearance, hutalso means that the knee hinge can bucklewhilst weight bearing, particularly from heelstrike to foot flat when the patient's weightis hehind the knee hinge causing a flexingmoment at the knee. Stability of the "knee"is gained by voluntary control, that is, theextensors of the hip work actively to preventthe knee flexing in stance and by involuntary
Aust.l.Physiother., XXIV, 1, Marcht 1978
or alignment control. Alignment stability canalso be achieved by aligning the knee hingesbehind a line drawn from the trochanter tothe ankle. This causes an extending momentat the knee joint from heel strike to toeoff and prevents the patient's knee bucklingduring weight bearing. However the morestability built into a leg, that is, the furtherthe knee hinges are behind the hip ankle axis,the greater the extending moment at the kneeat toe off and the greater the difficulty ininitiating knee flexion. Limb makers aim fora balance of voluntary control and alignmentstability because the greater the alignmentstability the greater the energy needed toinitiate swing and maintain a smooth gaitand the less the alignment stability thegreater the energy needed to stabilize the kneewhile weight bearing, a problem which ismagnified many times when the amputee iswalking on slopes and uneven ground.
In general the patient with a severe flexioncontracture is the older amputee whose activi..ties will be limited by his general health andthe physical state of his other leg. He walksslowly and for shorter distances than hisyounger counterpart so it is of paramountimportance that he should have walking madeas easy as possible. The patient using thePatellar..Tendon suspension type kneeling kneebearer is walking with the loss of only onejoint-the ankle and can use his quadricepsand hamstring muscle groups to control hisown knee joint rather than depending on hiship flexors and extensors to control both hipand knee joints. He can therefore walk overany surface more quickly, with greater safetyand using less energy, hence he can walkfurther with greater ease.
The advantage of the PTS type kneelingknee bearer aside from walking itself is theease with which it can be slipped on. A thighlacing corset is cumbersome and difficult toeither lace or buckle firmly, a problem whichis magnified in the elderly who have usuallylost some of the dexterity in their fingers.
If the amputee's stump is long, both typesof knee hearer present a problem for menwho cannot fit their leg into their trousers(Fig. 4).

THE PROSTHETIC PROBLEMS OF BELOW KNEE AMPUTEES 25
The only disadvantage of the PTS suspension is that the patient cannot sit with his footflat on the floor, it sticks out in front of himand so there is a danger other people may tripover it. It is a particular disadvantage if theamputee is still spry enough to travel onpublic transport where there is little leg roomhut in a private car he can sit comfortably inthe front seat.
In conclusion if the amputee has the musclestrength to control the remaining range of
knee movement the patellar-tendon suspensionis easier and quicker to don, it is lighter andless cumbersome and is far superior to theconventional knee bearer because the amputeewalks with the biomechanical advantages ofa below knee amputee rather than with thedisadvantages of an above knee amputee. Hehas a lower energy consumption and can traverse steps, slopes and uneven ground withgreater facility.
Aust.J.Physiother., XXIV, 1, March, 1978











![PolyProPylene PolyProPylene Technology Technology · 2 “The [polypropylene] prosthetic technology [...] is an attractive and durable solution for trans-tibial amputees, which can](https://img.pdfslide.us/doc/110x75/5f0fa1467e708231d4451d6a/polypropylene-polypropylene-technology-technology-2-aoethe-polypropylene-prosthetic.jpg)