Embed Size (px)
Citation preview

The pros and cons of the early identification of language
difficulties:-
Where have we got to and where are we going?James Law
Professor of Language and Communication Science
and Director
Centre for Integrated Healthcare Research, Edinburgh
Hoe vroeger, hoe beter?! Katholieke Universitert, Leuven 11th October 2008

Identification, intervention and natural history – an epidemiological
approach to language disorders
Identification

Identification, intervention and natural history – an epidemiological
approach to language disorders
Natural historyIdentification

Identification, intervention and natural history – an epidemiological
approach to language disorders
Prevalence
Natural historyIdentification

Identification, intervention and natural history – an epidemiological
approach to language disorders
Prevalence Intervention
Natural historyIdentification

What we will be covering today
• The literature on early identification and screening – the tests and review conclusions in 1997 and ten years on;
• Intervention: The Cochrane Review;• Natural history: What we can learn from prognostic
studies?• Implications for policy and practice.

What we will be covering today
• The literature on early identification and screening – the tests and review conclusions in 1997 and ten years on;
• Intervention: The Cochrane Review• Natural history: What we can learn from prognostic
studies?• Implications for policy and practice

What did we conclude in 1998?
• Looked at prevalence, natural history, efficacy and screening;• Many screens available but gold standards and criteria vary;• No screening tests have been used to predict across time;• Few comparisons across tests;• Specificity consistently higher than sensitivity – easier to say
who is not a case than who is a case;• Not possible to recommend population screening
Law, Boyle, Harris, Harkness and Nye 1998

And in 2006?Key questions:-• Does screening for speech and language delay result in improved
speech and language as well as improved other non-speech and language outcomes
• Do screening evaluations in the primary care setting accurately identify children for diagnostic evaluation and interventions?
• Does identification of risk factors improve screening?• What are screening techniques? What is the accuracy of
screening techniques and how does it vary by age?• What are the optimal ages and frequency for screening• What are the adverse effects of screening?• Plus a series of questions about intervention.Nelson, Nygren, Walker and Panoscha 2006 for the US Preventive
Services Task Force

And concluded..
• There was no literature to help answer many of the questions that they were interesting in addressing;
• Much more is needed about understanding “risk” factors;
• The optimal approach to screening had yet to be identified;
• No “gold standard”;• Few comparisons of the performance of different
measures;• Studies may not translate (from UK to USA);• Need long term outcomes and economic evaluation.

What we will be covering today
• The literature on early identification and screening – the tests and review conclusions in 1997 and ten years on;
• Intervention: The Cochrane Review• Natural history: What we can learn from population
studies – the example of the British Cohort Study of 18,000 children born in 1970;
• Implications for policy and practice.

Intervention
Law,Garrett and Nye 2003 and update in preparation

Expressive vocabulary: subgroup analysis - expressive difficulties
only (Law, Garrett and Nye 2003)

The role of intervention – what can/should be treated?
• It makes sense to identify children when we know that we can do something about it;
• Although many believe that the earlier we intervene the better, speech and language therapists are probably most confident treating children with speech and language difficulties between three and four years and that this is reflected in the intervention literature;
• So far we have reasonably good intervention data on expressive language and speech/phonological disorders;
• The pattern is much less clear for receptive language disorders.

What we will be covering today
• The literature on early identification and screening – the tests and review conclusions in 1997 and ten years on;
• Intervention: The Cochrane Review• Natural history: What we can learn from prognostic
studies?• Implications for policy and practice

Natural history
Study 1: Law, Tomblin and Zhang 2008
Study 2: Law, Rush, Parsons and Schoon (submitted)

Study 1 - The classification of language disorders and their trajectories across
time• Many classification systems have evolved;• The only published replication is the Conti-Ramsden
replication of the Rapin and Allen Nosological System (even R and A could not replicate their own system);
• We took this model and plotted their trajectories between 6 and 11 years;
• We used the Test of Reception of Grammar (TROG) as the measure because receptive language is one of the key determinants of poor outcomes and because we had values at each time point.

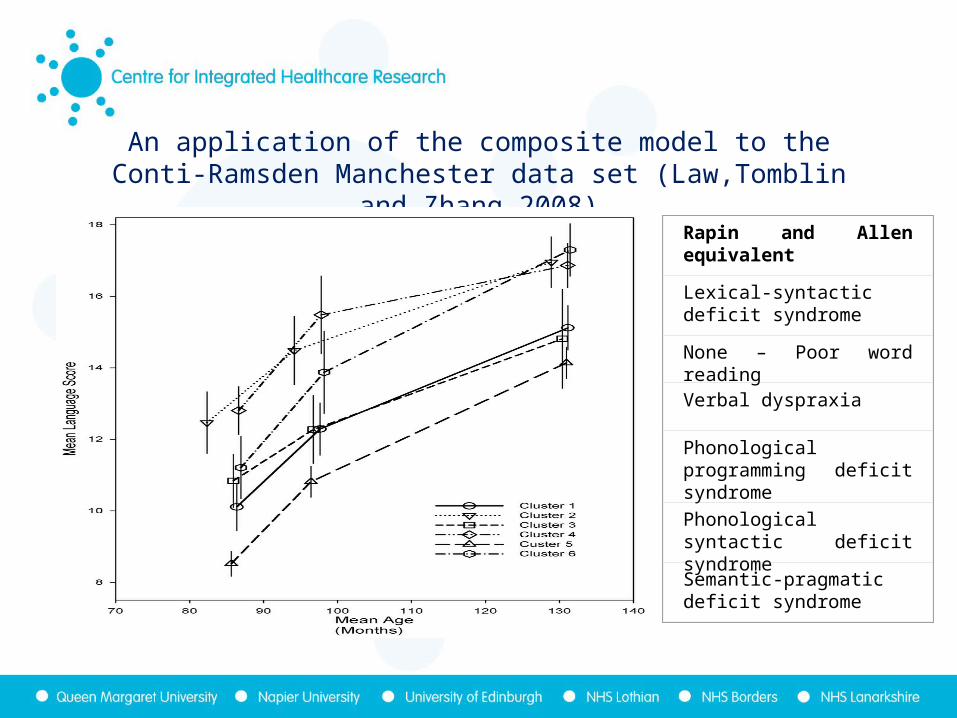
An application of the composite model to the Conti-Ramsden Manchester data set (Law,Tomblin and Zhang 2008)
Conti-Ramsden Cluster
Rapin and Allen equivalent
Description
1 Lexical-syntactic deficit syndrome
Good articulation but other language skills poor
2 None Poor word reading
3 Verbal dyspraxia General poor language but with good naming vocabulary
4 Phonological Programming deficit syndrome
Poor articulation and phonology. Normal language
5 Phonological syntactic deficit syndrome
Articulation is fair but all other tests are poor
6 Semantic-pragmatic deficit syndrome
Good articulation and reasonable expressive language but poor receptive language
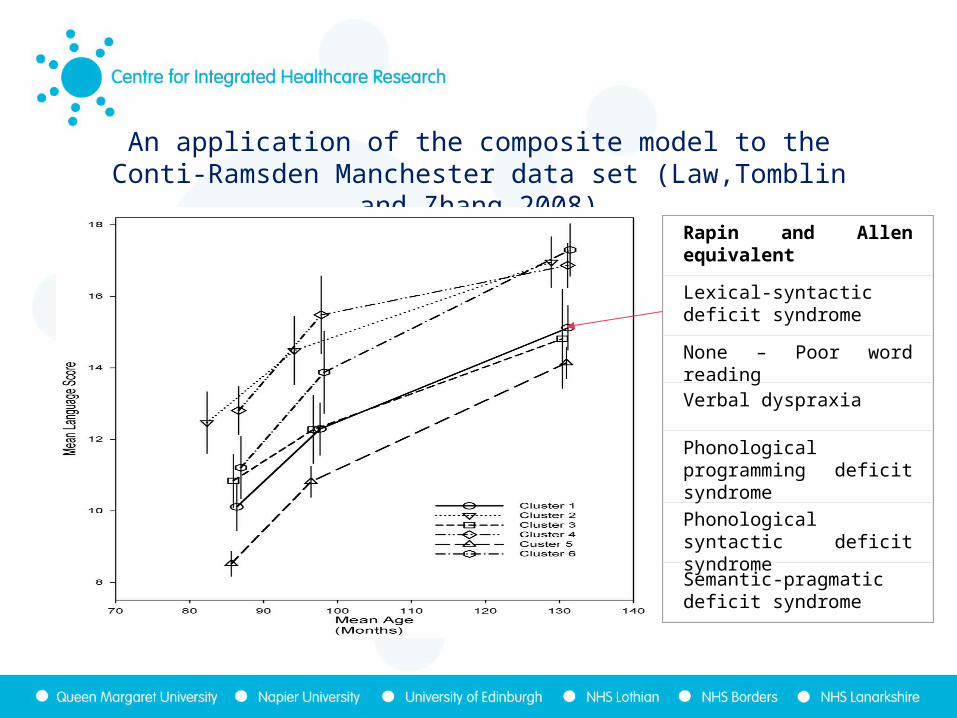
An application of the composite model to the Conti-Ramsden Manchester data set (Law,Tomblin and Zhang 2008)
Rapin and Allen equivalent
Lexical-syntactic deficit syndrome
None – Poor word readingVerbal dyspraxia
Phonological programming deficit syndrome
Phonological syntactic deficit syndrome
Semantic-pragmatic deficit syndrome
An application of the composite model to the Conti-Ramsden Manchester data set (Law,Tomblin and Zhang 2008)
Rapin and Allen equivalent
Lexical-syntactic deficit syndrome
None – Poor word readingVerbal dyspraxia
Phonological programming deficit syndrome
Phonological syntactic deficit syndrome
Semantic-pragmatic deficit syndrome

An application of the composite model to the Conti-Ramsden Manchester data set (Law,Tomblin and Zhang 2008)
Rapin and Allen equivalent
Lexical-syntactic deficit syndrome
None – Poor word readingVerbal dyspraxia
Phonological programming deficit syndrome
Phonological syntactic deficit syndrome
Semantic-pragmatic deficit syndrome

An application of the composite model to the Conti-Ramsden Manchester data set (Law,Tomblin and Zhang 2008)
Rapin and Allen equivalent
Lexical-syntactic deficit syndrome
None – Poor word readingVerbal dyspraxia
Phonological programming deficit syndrome
Phonological syntactic deficit syndrome
Semantic-pragmatic deficit syndrome

An application of the composite model to the Conti-Ramsden Manchester data set (Law,Tomblin and Zhang 2008)
Rapin and Allen equivalent
Lexical-syntactic deficit syndrome
None – Poor word readingVerbal dyspraxia
Phonological programming deficit syndrome
Phonological syntactic deficit syndrome
Semantic-pragmatic deficit syndrome

An application of the composite model to the Conti-Ramsden Manchester data set (Law,Tomblin and Zhang 2008
Rapin and Allen equivalent
Lexical-syntactic deficit syndrome
None – Poor word readingVerbal dyspraxia
Phonological programming deficit syndrome
Phonological syntactic deficit syndrome
Semantic-pragmatic deficit syndrome

An application of the composite model to the Conti-Ramsden Manchester data set (Law,Tomblin and Zhang 2008)
Rapin and Allen equivalent
Lexical-syntactic deficit syndrome
None – Poor word readingVerbal dyspraxia
Phonological programming deficit syndrome
Phonological syntactic deficit syndrome
Semantic-pragmatic deficit syndrome

Conclusions
The groupings hold across time and the trajectories are similar;The most important determinant is the starting point or “intercept”. If you start low, you end up low.Suggests that, by five/six years, the pattern is set – at least across the primary school age range;But remember these are clinical cases – what about in the population as a whole?And what about any support (special education/speech and language therapy) that they may have received?

Study 2 - Our research questions
• If you have poor language skills at five years, how much does this affect your adult performance?
• What is the extent of the relationship between proximal, distal and biological “risk” factors and both specific (SLI) and non-specific (N-SLI) language impairment at school entry?
• To what extent does the pattern of association differ for non-specific language impairment (N-SLI)?
• What is the risk associated with early SLI and N-SLI in terms of literacy, mental health and unemployment at 34
years?

The data source?
• British Cohort Study (BCS70), one of Britain's richest research resources for the study of human development;
• Over 18,000 persons living in Great Britain who were born in one week in April 1970;
• Data available about the cohort members at birth, 5, 10, 16, 26, 30 and most recently in 2004 when aged 34 years;
• Wide range of information collected from parent’s report, school report, tests and medical examinations;
• Excluded children whose first language was not English and whose ethnicity was not white European.

The measures at 5 years
– The English Picture Vocabulary Test (EPVT)
– The Copying Designs Test
The participants?3 discrete groups. “Typical Language Group” (TL) had EPVT and Copying
scores falling above one standard deviation below the mean for each assessment.
“Non-Specific Language Impairment Group” (N-SLI) had EPVT scores two or more standard deviations below the mean and scores of at least one standard deviation below the mean on the Test of Copying Skills.
“Specific Language Impairment Group” (SLI) also had scores of two or more standard deviations below the mean on the EPVT and scores of more than one standard deviation above the mean (ie. within the normal range) on the Test of Copying Skills.

Flow diagram indicating derivation of the sample
Completed EPVT & Copying designsn = 11330
Number of cohort members in database BCS70 at birth
n = 17196
English spoken at home & White Europeann = 12099
Not completedEPVT n = 750Copying Designs n = 19
English language not used at homen = 439Not white European n = 562Not stated n = 33Not known n = 2
TLn=9613
N-SLIn=195
SLIn=211
Good EPVT/ Poor copyingn=1311

The “exposures” of interest• Distal factors
– Child gender– Age mother left school before 16 years– Mother single parent
• Proximal factors– Persons per room ratio (more than 1 per room)– Child had some kind of pre-school– Parent read to child in past week– Parent a poor reader
• Biological and developmental risk– Mother smoked during pregnancy– Child small for dates– Child behavioural difficulties– Child seen a speech and language therapist

The outcomes at 34 years
• Literacy– above level 2 in the national curriculum (measured at 34).
Level 2 = equivalent to GCSE A-C.
• Mental health– 3 or more signs of having had a mental health problem (four
scales)• Rutter Malaise Inventory
• Satisfaction with life scale
• Measure of perception of control over life
• Measure of self efficacy
• Employment– More than twelve months unemployment before 34 years

Measuring associationsThe analyses measure associations NOT causes using odd
ratiosThe odds ratio is a way of calculating the probability of
someone achieving something, winning, having a disease etc.relative to the probability that they will not do so;
So if a horse has a 60% probability of winning (and therefore a 40% chance of losing) the odds of it winning is 60/40 or 1.5;
An odds ratio of 0.5 means that the outcome is half as likely to occur in the target group. An odds ratio of 2.0 means that it is twice as likely to occur.

The association between language and both demographic and within child factors
at school entry(odds)Multivariate analysis indicates statistically significant associations :-• SLI is associated with gender (0.64), going to pre-school (1.71)
parent being a poor reader (2.71), and the child having seen a speech and language therapist (2.40);
• N-SLI is associated with all variables [mother’s schooling, mother a single parent, overcrowding, preschool experience, parent reads to child, parental reading ability (4.91), smoking during pregnancy, small for dates (4.08) , behaviour problems, seen a speech and language therapist (6.26)], except gender and mother smoking in pregnancy.

The association between five year performance and demographic factors for 34 year outcomes
- literacy-• Although SLI is predictive of 34 year performance on its
own and with aspects of the model, once all factors are added in SLI drops out as a predictor;
• By contrast, N-SLI remains in the model as the highest predictor of adult literacy even after taking demographic factors into consideration.

The association between five year performance and demographic factors for 34 year outcomes
- mental health-
• SLI does not predict mental health difficulties at 34 years either on its own or in combination with other variables;
• By contrast, N-SLI continues to act as a predictor once all the other variables are includes. Indeed, it remains the strongest single predictor most closely followed by
behaviour difficulties.

The association between five year performance and demographic factors for 34 year outcomes
- employment-
• SLI at five years is not associated with poor employment outcomes except on its own (ie. without the other demographic factors) (2.15);
• N-SLI remains associated with poor employment (1.99). Indeed it remains the highest predictor apart from gender (being a boy) (2.04).

What we will be covering today
• The literature on early identification and screening – the tests and review conclusions in 1997 and ten years on;
• Intervention: The Cochrane Review• Natural history: What we can learn from prognostic
studies?• Implications for policy and practice

Summary of key points• Screening is a complex process drawing on all our knowledge about
speech and language difficulties• An epidemiological approach to early identification is essential• Intervention can be effective for speech and expressive language;• BUT receptive language remains a problem and we know less about
long term outcomes of intervention;• In a longitudinal study of a clinical population the intercept is critical
at school entry, the trajectories remain similar;• BUT in a population sample risk is very different for N-SLI and SLI
groups.• There is clear evidence of strong effects of demographic risk at five
years for both groups but SLI status alone does not predict adult outcomes (whereas N-SLI status does).

Potential implications“Screening” of all children remains problematic for those
who are likely to have problems (better for those who don’t);
Clear evidence of adult risk status by 5 years. SLI may be a protective factor-SLI;
Environmental factors are key to understanding potential outcomes;
We need to develop an understanding of what can be done in terms of environmental modification to mitigate the effects of these poor early profiles – Special needs or public health?
There is more that can be done to link adult outcomes with changes across childhood (eg school transitions) and across the life course.

Conclusions 1
• Where have we got to..

In terms of early identification – the “when” question…
• A good public health case for drawing language development to parent’s attention;
• Very early identification requires a better understanding of risk. Delays in expressive language development can be determined very early but this is not enough for screening;
• The nature of intervention probably becomes more targeted [and thus more likely to be effective] across time;
• Receptive language at school entry would be a good target for screening but we need to know more about intervention for these children;

Conclusions 2
• Where are we going..

• Need a better understanding of outcomes – what are we trying to change? Is it language, mental health, social inclusion etc.?
• Need a better understanding of the role of demographic risk and of co-morbidities;
• This needs to be integrated into the relevant university curricula;
• More work needed on trajectories;• More work needed on resilience – who starts off with
difficulties but manages well?

With thanks to:Cochrane Review
Zoe Garrett, Chad Nye and the Cochrane Collaboration
The support of the Nuffield Foundation
Manchester Child Language StudyBruce Tomblin, Xuyang Zhang and Gina Conti-Ramsden
BCS70 studyRobert Rush, Ingrid Schoon and Sam Parsons
The support of the Economic and Social Science Research Council (RES-000-22-1748).





























