Embed Size (px)
Citation preview

Available online at www.annclinlabsci.org
The Promotion of Neural Regeneration in A Rat Facial Nerve Crush Injury Model Using Collagen-Binding NT-3Handong Wang1,*, Hongbin Ni1,*, Sufang Han2,*, Wu Xu1, Jing Wang1, Baoyu Yuan1, Tiansheng Zhu1, Wei Jin1, Weibang Liang1, and Jianwu Dai2
1Department of Neurosurgery, Nanjing Drum Tower Hospital, Medical School of Nanjing University, Nanjing, Jiangsu and 2State Key Laboratory of Molecular Developmental Biology, Institute of Genetics and Developmental Biology, Chinese Academy of Sciences, Beijing, China
Abstract. Traumatic facial nerve injury, an important cause of facial paralysis, has a number of adverse ef-fects, including facial muscle dysfunction and facial asymmetry. It has been demonstrated in our previous work that native human NT-3 fused with a collagen-binding domain (CBD-NT-3) could bind to collagen, specifically to exert neurotrophic effects, promoting axonal regeneration. To evaluate the effect of CBD-NT-3 in inducing facial nerve regeneration and functional recovery, the differing effects of CBD-NT-3 and native neurotrophin-3 (NAT-NT-3) were observed using the results of facial nerve functional recovery, electrophysiological testing, and axonal and myelin changes in a rat model of facial nerve crush injury. The rats were injected in the epineurium in crushed fibers of the facial nerve with CBD-NT-3, NAT-NT-3, and PBS respectively. After 4 weeks, the CBD-NT-3 group demonstrated significantly more ordered growth of axons and nerve functional recovery than the NAT-NT-3 group. The results suggest that CBD-NT-3 con-siderably enhances facial nerve regeneration and functional recovery.
Key words: Facial nerve injury, collagen-binding domain, neurotrophin-3, nerve regeneration.
Introduction
Traumatic facial nerve injury is an important cause of facial paralysis; it can occur from external causes or iatrogenic injury and results in a number of ad-verse effects, including facial muscle dysfunction and facial asymmetry [1]. For surgical repair of large lesions, the gold standard is the insertion of an autologous graft between the two nerve stumps; however the functional outcome of autograft-based repair remains unsatisfactory [2-4], as this tradi-tional treatment can also produce synkinesis, hemi-facial spasm or other sequelae. The mechanism for protection of the structure of facial nerves and res-toration motor function after traumatic facial nerve injury has become a hot topic in medical research.
In recent years, the novel class of compounds known as growth factors has been found in periph-eral nerves, and these neurotrophins have been shown to influence nerve regeneration in the pe-ripheral nervous system [5], the most studied of which is neurotrophin-3 (NT-3). Since the purifi-cation of NT-3 in 1990 [6-8], research has focused on its central role in brain development, physiolo-gy, and pathology [9]. In the central nervous sys-tem, NT-3 plays a key role in the survival of neu-rons during development, differentiation, growth, and the maintenance of normal physiological func-tion. Aside from its important role in neural devel-opment, NT-3 appears essential to the molecular mechanisms of synaptic plasticity and nerve sur-vival. The NT-3 molecule interacts with neurons that express the appropriate tropomyosin-related kinase receptor, trkC, and the p75 receptor [10,11]. NT-3 has unprecedented stimulatory effects on outgrowth of specific neuronal populations [12,13]. Neurotrophic factors have been delivered to injured nerves systemically [14], or locally using osmotic minipumps [15,16], injection into a graft, [17] or a slow-release device [18-20]. Most studies have
0091-7370/16/0600-578. © 2016 by the Association of Clinical Scientists, Inc.
Annals of Clinical & Laboratory Science, vol. 46, no. 6, 2016
*These authors contributed equally to this work. Address correspondence to Weibang Liang, Department of Neurosurgery, Drum Tower Hospital, 321 Zhongshan Road, Nanjing 210008, Jiangsu Province, P. R. China; phone: 86 25 83106666; e mail: [email protected]; or Wei Jin, Department of Neurosurgery, Drum Tower Hospital, 321 Zhongshan Road, Nanjing 210008, Jiangsu Province, P. R. China; phone: 86 25 83106666; e mail: [email protected]; or Jianwu Dai,State Key Laboratory of Molecular Developmental Biology, Institute of Genetics and Developmental Biology, Chinese Academy of Sciences, 3 Nanyitiao, Zhongguancun, Beijing 100190, China; phone: 86 10 82614426; e mail: [email protected]
578

shown that important aspects of regeneration, in-cluding axon growth, Schwann cell function, and myelination, are affected positively [21].
Based on the previous research, it appears that NT-3 has the potential to enhance peripheral nerve regeneration. However, due to its rapid diffusion in extracellular fluids, NT-3 simply delivered in solu-tion is difficult to retain at the injured area. In order to maintain a high concentration of NT-3, multi-ple injections are needed; however, these would in-crease the surgical risk and the cost of treatment. Thus, a delicate control of NT-3 in localization is critical to apply NT-3 safely and efficiently. In our previous study, we demonstrated that native hu-man BDNF fused with a collagen-binding domain can bind to collagen specifically to exert a neuro-trophic effect, promoting axonal regeneration. Now we use the same method to prepare CBD-NT-3. Collagen, as a natural scaffold, is the main component of extracellular matrix; it accumulates after nerve crush injury [22,23] and could provide a therapeutic target for treatment. Extracellular matrix collagen could also be a potential binding target for CBD-NT-3, which would retain and
enrich NT-3 at the injury site. We tested this new therapeutic strategy in a rat facial nerve crush injury model.
Materials and Methods
Preparation of CBD-NT-3 and NAT-NT-3. CBD-NT-3 and NT-3 without collagen-binding domain (NAT-NT-3) were prepared. pET-NAT-NT-3 and pET-CBD-NT-3 carried by Escherichia coli BL21 (DE3) strain were used to express NAT-NT-3 and CBD-NT-3, which contained a 6×His purification tag for purifica-tion and detection. The purification of the solubilized NAT-NT-3 and CBD-NT-3 was performed under dena-turing conditions by nickel chelate chromatography (Amersham Bioscience, Uppsala, Sweden). The purified NAT-NT-3 and CBD-NT-3 were dialyzed in the gluta-thione redox-refolding system for renaturing.
Surgical procedures of facial nerve crush injury and application of NT-3. Experiments were performed in accordance with the Guide for the Care and Use of Laboratory Animals from the National Institute of Health and approved by the Animal Care and Use Committee of Nanjing University. Sprague Dawley rats (250±10 g) were anesthetized by an intraperitoneal in-jection of sodium pentobarbital (50mg/kg body weight).
Figure 1. Surgical procedures of facial nerve crush injury and application of NT-3. A segment of 4 mm nerve was exposed. Thirty seconds compression with a vascular clip was performed around the exposed facial nerve to induce crush injury (A). After drug injection, a mark was made at the distal site of the crushed area using 10/0 monofilament nylon (B). The epi-neurium injection at the facial nerve injury area (C).
Collagen-binding NT-3 promotes neural regeneration in a rat facial nerve crush injury model 579
After sterilization, an incision was made subcutaneously to expose the trunk of the left extracranial facial nerve, as shown in Figure 1, and a 4mm segment of nerve was exposed. Thirty seconds compression with a vascular clip (10g force, Kent Scientific Corporation, INS 650911, USA) was performed around the exposed facial nerve to induce crush injury. After the drug injection, a mark was made at the distal site of the crushed area using 10/0 monofilament nylon. The muscle layers and the skin were then sutured separately.
Following the induced injury, the animals were divided into three groups according to treatment. The NAT-NT-3 group (n=40), had NAT-NT-3 (0.25nmol, 5μL) intrathecally injected into the crush site of the crush-in-jured facial nerve; the CBD-NT-3 group (n=40) had CBD-NT-3 (0.25nmol, 5μL) intrathecally injected into
the crush site of the crush-injured facial nerve; and a sham group (n=40) had the same volume of PBS inject-ed to the site. The animals were kept under standardized laboratory conditions in an air-conditioned room with unrestricted access to food and water. The rats were sac-rificed by cervical dislocation at different time points.
Collagen content evaluation. The sham group rats were sacrificed for sample collection at time points 24 h, 48 h, 72 h after injury (n=5). Crushed facial nerve measuring approximately 0.4 cm in length was rapidly excised and fixed in 4% (vol/vol) formaldehyde for 48 h. The seg-ments were then embedded in paraffin and 5μm sections were cut from each segment and examined by immuno-histochemistry using an antibody to collagen (anti-colla-gen, 1:200 dilution; Santa Cruz, Texas, USA) to identify the collagen content.
NT-3 retaining assay. At 24 h, 48 h, and 72 h following injury, the NAT-NT-3 and CBD-NT-3 group rats were killed by cervical dislocation (n=5). Crushed facial nerves measuring approximately 0.4cm were excised and frozen immediately in liquid nitrogen. Then proteins were ex-tracted for western blot analysis, and retained NT-3 was indentified using an antibody to NT-3. (anti-collagen, 1:1000 dilution; Abcam). Western blotting was per-formed as follows: A facial nerve protein sample (40μg) was subjected to electrophoresis on a 15% sodium do-decylsulfate-polyacrylamide gel for 45 minutes at 80 V, followed by 100 minutes at 100 V, and was then trans-ferred onto nitrocellulose for 1 hour at 100 V. The mem-brane was blocked with 5% skim at 4°C overnight and was then incubated for 1 hour in the presence of primary antibodies directed against NT-3 (anti-collagen, 1:1000 dilution; Abcam), and GAPDH (Santa Cruz Biotechnology) diluted 1:10000 in PBST (Sigma-Aldrich) was used as a loading control. It was then se-quentially incubated with a horseradish peroxidase-con-jugated secondary antibody (diluted 1:400 in phosphate-buffered saline Tween-20) for 2 hours.
Nerve functional assessment. Vibrissal whisking and nictating reflex evaluations were performed to evaluate
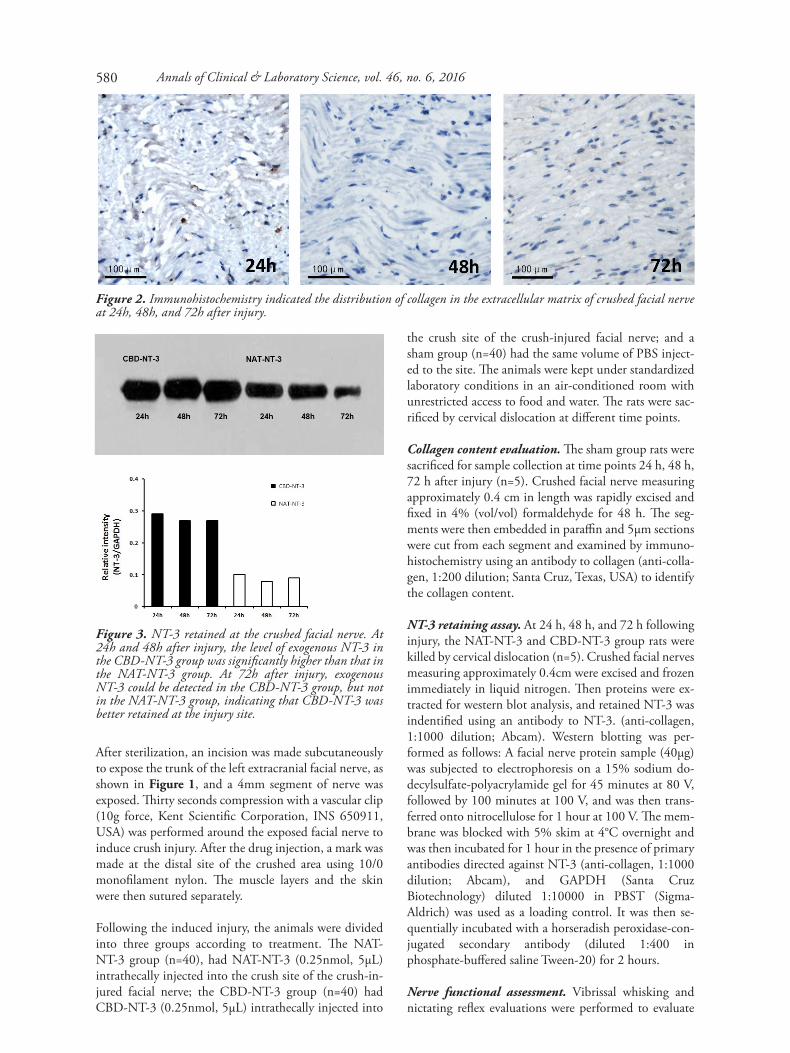
Figure 2. Immunohistochemistry indicated the distribution of collagen in the extracellular matrix of crushed facial nerve at 24h, 48h, and 72h after injury.
Figure 3. NT-3 retained at the crushed facial nerve. At 24h and 48h after injury, the level of exogenous NT-3 in the CBD-NT-3 group was significantly higher than that in the NAT-NT-3 group. At 72h after injury, exogenous NT-3 could be detected in the CBD-NT-3 group, but not in the NAT-NT-3 group, indicating that CBD-NT-3 was better retained at the injury site.
Annals of Clinical & Laboratory Science, vol. 46, no. 6, 2016580

Collagen-binding NT-3 promotes neural regeneration in a rat facial nerve crush injury model
facial nerve function. As previously described by Kobayashi et al., whisker movements were divided into four different categories with scores ranging from 0 to 3 (0, no whisker movement; 1, slight whisker movement; 2, slow whisker movement; 3, rapid whisker movement undistinguishable from the contralateral uninjured side). The nictating reflex was scored using the following clas-sification: 0, no eye movement; 1, slight eye movement; 2, slow and incomplete eye closure; 3, rapid and com-plete eye closure undistinguishable from the contralat-eral non-lesioned side [24]. The whisker movement and nictating reflex evaluations were conducted by two inde-pendent observers at 1 day, 3 days, 1 week, 2 weeks, 3 weeks, and 4 weeks after injury.
Electrophysiological examination. Electrophysiological examination was carried out using an electromyography system (RM6240, Chengdu, China) at the time points of immediately after injury and 4 weeks after injury (n=5). The stimulating electrode was placed in the proxi-mal end of the crushed area of the facial nerve,
the recording electrode was inserted into the ipsilateral orbicularis oris muscle, and the reference electrode was inserted into the ipsilateral fore limb, subcutaneously. The compound muscle action potentials (CMAPs) in both sides were measured. The CMAP ratio of the in-jured side to the normal side was used to evaluate facial nerve functional recovery.
Histological and ultrastructural analysis. Histological assessments were performed 4 weeks after facial nerve injury (n=5). The crushed nerves were isolated and fixed in 4% (vol/vol) formaldehyde for 48 h and the segments were then embedded in paraffin. Sections measuring 5 μm were cut from each segment and examined by Chromotrope 2R-Brilliant green staining and immuno-histochemistry using antibodies to neurofilament (anti-NF, 1:1000 dilution; Abcam).
For electron microscopy analysis, 4 weeks after injury samples (n=5) were fixed in phosphate-buffered glutara-dehyde (2.5%) and osmium tetroxide (1%). Dehydration of the crushed nerve was carried out in acetone solutions at increasing concentrations. The tissue was embedded in an epoxy resin and semi-thin (1 μm) sections through the nerve were made and stained with toluidine blue. Then, 600 A-thin sections were made from a selected area of tissue defined by the semi-thin section, and stained with lead citrate and uranyl acetate. The ultra-structure of the facial nerve was observed under a trans-mission electron microscope (JEM-1200X).
Statistical analysis. SPSS 19.0 was used for all statistical analysis. Statistically significant differences in parameters were determined as *P<0.05 and **P<0.01 by a Student’s two-tailed t-test.
Results
Collagen-binding assay. It has been reported that after nerve injury, collagen is expressed and accu-mulated at the injury site [25]. As shown in Figure 2, immunohistochemistry indicated the distribu-tion of collagen in the extracellular matrix of crushed facial nerve at 24h, 48h, and 72h after in-jury. Therefore, native collagen at the injury site could be the binding target for CBD-NT-3 to exert its neurotrophic effects.
After intrathecal injection of NAT-NT-3 or CBD-NT-3, NT-3 retained at the crushed facial nerve was evaluated by western blot at the time points of 24h, 48h, and 72h after injury (Figure 3). At 24h and 48h after injury, the level of exogenous NT-3 in the CBD-NT-3 group was significantly higher than
Figure 4. Functional recovery of the facial nerve. The re-covery of the whisker movements and nictating reflex were evaluated at different time points after injury.
Figure 5. Electrophysiological recovery assessment. Immediately after injury, CMAPs in the injured sides were almost shut down. Compared with the sham group, CMAP was significantly restored at week 4 after injury in the CBD-NT-3 and NAT-NT-3 groups (n=5, p<0.01). CMAP restoration of the CBD-NT-3 group was signifi-cantly higher than that of the NAT-NT-3 group (n=5, p<0.01).
581
that in the NAT-NT-3 group. At 72h after injury, exogenous NT-3 could be detected in the CBD-NT-3 group, but not in the NAT-NT-3 group, in-dicating that CBD-NT-3 was better retained.
Functional recovery of the crushed facial nerve. As facial nerve controls the movements of the facial muscles, facial paralysis happens after facial nerve injury. In rats, the most obvious phenotype after facial nerve crush injury is the paralysis of whisker movements and nictating reflex obstruction. The recovery of whisker movements and the nictating reflex were measured to reflect the reconstruction of the nerve conduction function. We added the scores of whisker movements and nictating reflex together for each rat at different time points in order to ob-tain an average score for each group. As shown in Figure 4, all the animals showed complete facial paralysis on the injured side immediately after the surgery. One week after injury, some rats began to have a functional recovery. As recovery time ex-tended, nerve function improved in each group. Finally, all groups reached a high level of function at week 4, not distinguishable from the facial move-ment of normal rats. The animals in groups CBD-BDNF and NAT-BDNF recovered faster than
those in the sham group throughout the experi-ment, especially at day 7, day 14, day 21 and day 28 (P<0.01). Compared with the NAT-BDNF group, the rats in the CBD-BDNF group recov-ered faster, especially at day 14 and day 18 (P<0.01). At day 28, the rats in the CBD- NT-3 and NAT- NT-3 groups had almost recovered their function and exhibited no difference from normal rats.
Electrophysiological recovery assessment. The electrophysiological index CMAPs at the injured and uninjured sides were measured immediately, and 4 weeks after surgery. The CMAPs ratio of the injured side to the uninjured side was used to eval-uate facial nerve functional recovery, as shown in Figure 5. Immediately after injury, CMAPs in the injured sides were almost shut down, meaning the crushed facial nerve injury model was successful. Compared with the sham group, CMAP was sig-nificantly restored at week 4 after injury in the CBD-NT-3 and NAT-NT-3 groups (n=5, p<0.01). CMAP restoration of the CBD-NT-3 group was significantly higher than that of the NAT-NT-3 group (n=5, p<0.01), indicating that CBD-NT-3 provided greater neuroprotective effect.
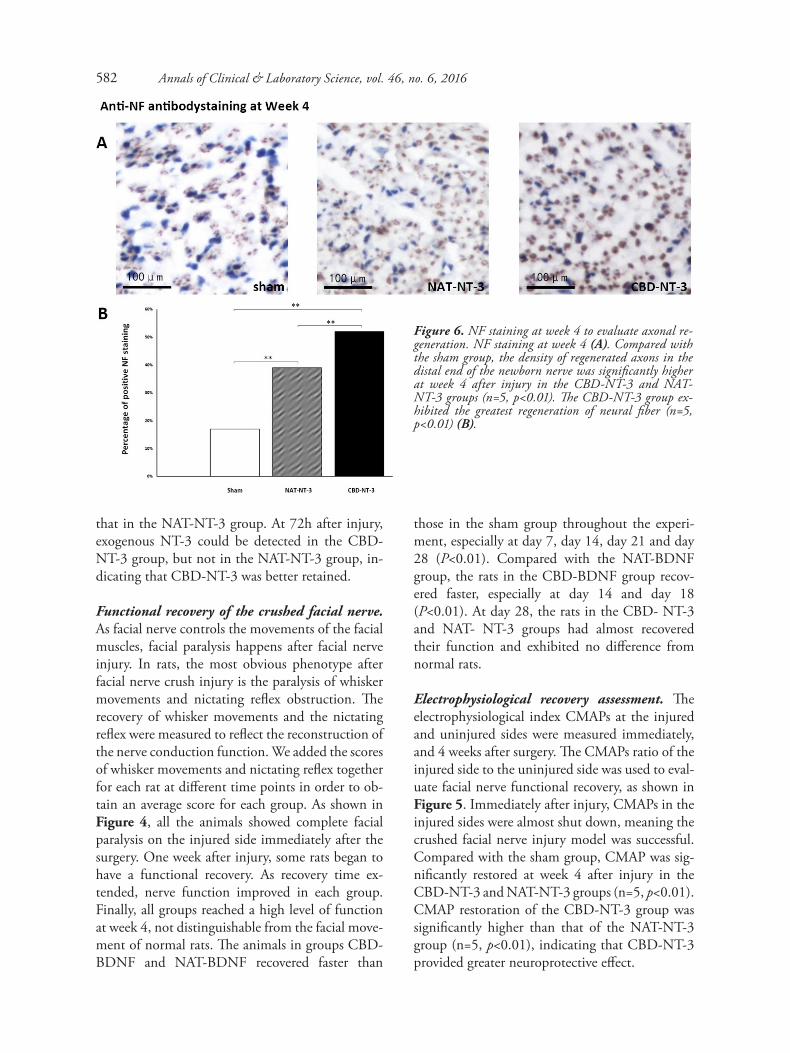
Figure 6. NF staining at week 4 to evaluate axonal re-generation. NF staining at week 4 (A). Compared with the sham group, the density of regenerated axons in the distal end of the newborn nerve was significantly higher at week 4 after injury in the CBD-NT-3 and NAT-NT-3 groups (n=5, p<0.01). The CBD-NT-3 group ex-hibited the greatest regeneration of neural fiber (n=5, p<0.01) (B).
Annals of Clinical & Laboratory Science, vol. 46, no. 6, 2016582
Collagen-binding NT-3 promotes neural regeneration in a rat facial nerve crush injury model
Histological and ultrastructural analysis. Axonal regeneration was evaluated by staining NF-positive axons in sections at the crush injury site of the facial nerve injury. Neural fiber density at the injury site of each group was quantified by analyzing the den-sity of NF-positive area (Figure 6). Compared with the sham group, the density of regenerated axons in the distal end of the newly generated nerve was sig-nificantly higher 4 weeks after injury in the CBD-NT-3 and NAT-NT-3 groups (n=5, p<0.01). The CBD-NT-3 group exhibited the greatest regenera-tion of neural fiber (n=5, p<0.01), demonstrating that CBD-NT-3 promoted more axonal regenera-tion at the crush injury site.
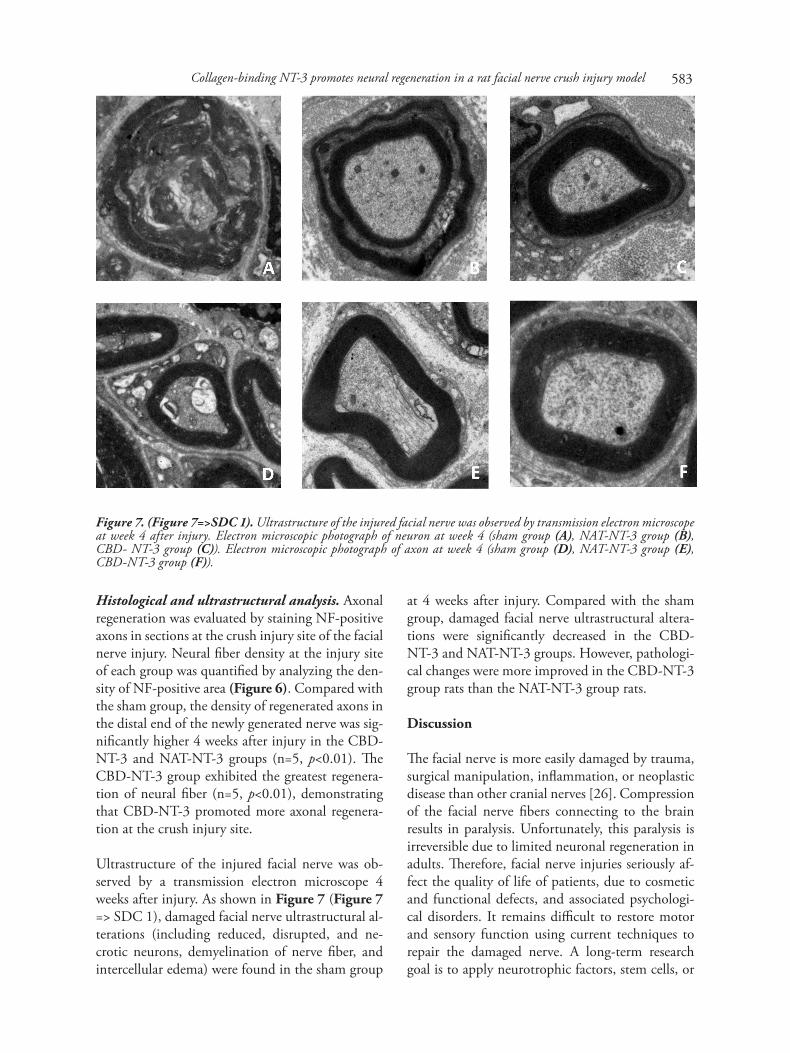
Ultrastructure of the injured facial nerve was ob-served by a transmission electron microscope 4 weeks after injury. As shown in Figure 7 (Figure 7 => SDC 1), damaged facial nerve ultrastructural al-terations (including reduced, disrupted, and ne-crotic neurons, demyelination of nerve fiber, and intercellular edema) were found in the sham group
at 4 weeks after injury. Compared with the sham group, damaged facial nerve ultrastructural altera-tions were significantly decreased in the CBD-NT-3 and NAT-NT-3 groups. However, pathologi-cal changes were more improved in the CBD-NT-3 group rats than the NAT-NT-3 group rats.
Discussion
The facial nerve is more easily damaged by trauma, surgical manipulation, inflammation, or neoplastic disease than other cranial nerves [26]. Compression of the facial nerve fibers connecting to the brain results in paralysis. Unfortunately, this paralysis is irreversible due to limited neuronal regeneration in adults. Therefore, facial nerve injuries seriously af-fect the quality of life of patients, due to cosmetic and functional defects, and associated psychologi-cal disorders. It remains difficult to restore motor and sensory function using current techniques to repair the damaged nerve. A long-term research goal is to apply neurotrophic factors, stem cells, or
Figure 7. (Figure 7=>SDC 1). Ultrastructure of the injured facial nerve was observed by transmission electron microscope at week 4 after injury. Electron microscopic photograph of neuron at week 4 (sham group (A), NAT-NT-3 group (B), CBD- NT-3 group (C)). Electron microscopic photograph of axon at week 4 (sham group (D), NAT-NT-3 group (E), CBD-NT-3 group (F)).
583

other treatments for the regeneration of axons [27]. The development of effective treatment to promote axonal regeneration and functional recovery in fa-cial nerve injury is slow and still a major clinical challenge. Our study reports that after facial nerve crush injury, rats treated with CBD-NT-3 regained function and recovered structural nerve.
As an important part of extracellular matrix, colla-gen exists in almost every organ of the human body, maintaining the structure of tissue [28]. Collagen plays a key role in the development of the human nervous system, such as in the differentiation of neural cells and the generation of the cerebral cor-tex [29-31]. It could be used as a carrier for neuro-trophic factors to maintain the growth of neuro-cytes and promote nerve regeneration in rat nerve injury [32,33]. After nerve crush injury, collagen is overexpressed and accumulates at the injury site [34]. Fibroblasts, astrocytes, and endothelial cells may produce collagen post-injury in adult rats. It has been suggested that collagen influences axonal outgrowth through its associated molecules [35,36]. Collagen ECM matrix also serves as a scaffold for fibroblasts, blood vessels, and macrophages move-ment at the injury site. Therefore, the native colla-gen at the injury site could be a binding target for CBD-NT-3 to exert its neurotrophic effects.
The process of nerve regeneration is complex, with many co-ordinating factors involved. As a member of the NTs, NT-3 has been proven to prevent the process of neuron death, adapting the injured neu-ron and protecting its structure and function. However, in practice, it is difficult to retain NT-3 simply delivered in solution at the injury site due to its rapid diffusion in the extracellular fluid. Because of its collagen-binding domain, CBD- NT-3 could be retained at the injury site by binding to collagen, which would increase the benefit/risk ratio. In this work, in vivo releasing results demonstrated that a one-time intrathecally injected CBD- NT-3 bound specifically to endogenous collagen and maintained a higher concentration at the facial nerve crush site. Nerve functional assessment, electrophysiological evaluation (SSERs), and histological analysis were carried out to assess neural regeneration after crush injury. The CBD-NT-3 group demonstrated the
most favorable locomotion recovery as measured by functional recovery scores. An electrophysiological evaluation also showed significantly better restora-tion of SSERs in the CBD-NT-3 group. Histological analysis also indicated that the CBD-NT-3 group showed better axonal regeneration.
After injury, the NAT-NT-3 and CBD-NT-3 groups exhibited an earlier locomotion recovery, and most of the CBD-NT-3 group rats had com-plete recovery at week 4. The electrophysiology ex-amination also showed that nerve conduct restora-tion was significantly higher in the CBD-NT-3 group than those in the other two groups. Consistent with the functional recovery results, CBD-NT-3 treatment ameliorated the pathological process and promoted axon regeneration. It also re-duced neuron necrosis and intercellular edema, providing a permissive regeneration microenviron-ment at the injured area. Our results show that CBD-NT-3 obviously increased the amount of my-elinated axons, accompanied by striking electro-physiological activity recovery in the rat facial nerve injury model. These data indicate that the use of CBD-NT-3 leads to functional recovery in facial nerve injury, at least partially based on the regen-eration of the myelin sheath structure.
CBD-NT-3 could be useful in promoting neural regeneration after facial nerve injury. In crush inju-ries of the facial nerve, we could directly utilize CBD-NT-3 by using the native extracellular matrix component collagen as the target for therapy.
Conclusion. We have combined a collagen-binding domain to NT-3 and applied it in a facial nerve injury model. Both CBD-NT-3 and NAT-NT-3, particularly the former, could promote the growth of axons, and effectively improve nerve functional recovery.
Acknowledgment
We thank LetPub (www.letpub.com) for its linguistic assis-tance during the preparation of this manuscript. This work was supported by grants from the National Natural Science Foundation of China (81171153 and 81200938), the Natural Science Foundation of Jiangsu Province (BK20151083), and the Medical Science and technology development Foundation of Nanjing Department of Health (JQX13007).
Annals of Clinical & Laboratory Science, vol. 46, no. 6, 2016584

Collagen-binding NT-3 promotes neural regeneration in a rat facial nerve crush injury model
References
1. Sardesai MG, Moe K. Recent progress in facial paralysis: ad-vances and obstacles. Curr Opin Otolaryngol Head Neck Surg 2010; 18:266-71.
2. Höke A. Mechanisms of disease: what factors limit the success of peripheral nerve regeneration in humans? Nat Clin Pract Neurol 2006. 2, 448–454.
3. Ray WZ, Mackinnon SE. Management of nerve gaps: auto-grafts, allografts, nerve transfers, and end-to-side neurorrha-phy. Exp Neurol 2010. 223, 77–85.
4. Pondaag W, Malessy MJA. Intercostal and pectoral nerve transfers to re-innervate the biceps muscle in obstetric brachial plexus lesions. J Hand Surg Eur Vol 2013. 39,647–652.
5. Boyce VS, Mendell LM. Neurotrophins and spinal circuit function. Front Neural Circuits 2014 Jun 5;8:59.
6. Hohn A, Leibrock J, Bailey K & Barde YA. Identification and characterization of a novel member of the nerve growth factor/brainderived neurotrophic factor family. Nature 1990.344 339–341.
7. Maisonpierre PC, Belluscio L, Squinto S, Ip NY, Furth ME, Lindsay RM &Yancopoulos GD. Neurotrophin-3: a neuro-trophic factor related to NGF and BDNF. Science 1990. 247 1446–1451.
8. Rosenthal A, Goeddel DV, Nguyen T, Lewis M, Shih A, Laramee GR, Nikolics K & Winslow JW. Primary structure and biological activity of a novel human neurotrophic factor. Neuron 1990. 4 767–773.
9. Jones KR, Reichardt LF. Molecular cloning of a human gene that is a member of the nerve growth factor family. Proc Natl Acad Sci USA 1990. 87:8060–8064.
10. Chao MV, Hempstead BL. p75 and Trk: a two-receptor sys-tem. Trends Neurosci 1995. 18, 321–326.
11. Huang EJ, Reichardt LF. Neurotrophins: roles in neuronal de-velopment and function. Ann Rev Neurosci 2001. 24, 677–736.
12. Aloe L, Rocco ML, Bianchi P, Manni L. Nerve growth factor: from the early discoveries to the potential clinical use. J Transl Med 2012. 10, 239.
13. Bothwell M. NGF, BDNF, NT3, and NT4. Handb Exp Pharmacol 2014. 220, 3–15.
14. Sahenk Z, Seharaseyon J, Mendell JR. CNTF potentiates pe-ripheral nerve regeneration. Brain Res 1994. 655, 246–250.
15. Newman JP, Verity AN, Hawatmeh S, Fee WE, Terris DJ. Ciliary neurotrophic factors enhances peripheral nerve regen-eration. Arch Otolaryngol Head Neck Surg 1996. 122, 399–403.
16. Utley DS, Lewin SL, Cheng ET, Verity AN, Sierra D, Terris DJ. Brain-derived neurotrophic factor and collagen tubuliza-tion enhance functional recovery after peripheral nerve tran-section and repair. Arch Otolaryngol Head Neck Surg 1996. 122,407–413.
17. Chu TH, Li SY, Guo A, Wong WM, Yuan Q, Wu W. Implantation of neurotrophic factor-treated sensory nerve graft enhances survival and axonal regeneration of motoneurons af-ter spinal root avulsion. J Neuropathol Exp Neurol 2009. 68, 94–101.
18. Sterne GD, Coulton GR, Brown RA, Green CJ, Terenghi G. Neurotrophin-3-enhanced nerve regeneration selectively im-proves recovery of muscle fibers expressing myosin heavy chains 2b. J Cell Biol 1997. 139, 709–715.
19. Fine EG, Decosterd I, Papaloïzos M, Zurn AD, Aebischer P. GDNF and NGF released by synthetic guidance channels sup-port sciatic nerve regeneration across a long gap. Eur J Neurosci 2002. 15, 589–601.
20. Wood MD, Moore AM, Hunter DA, Tuffaha S, Borschel GH, Mackinnon SE, Sakiyama Elbert SE. Affinity-based release of glial-derived neurotrophic factor from fibrin matrices enhances sciatic nerve regeneration. Acta Biomater 2009. 5, 959– 968.
21. Klimaschewski L, Hausott B, Angelov DN. The pros and cons of growth factors and cytokines in peripheral axon regenera-tion. Int Rev Neurobiol 2013. 108, 137–171.
22. Stichel CC, Niermann H, D'Urso D, Lausberg F, Hermanns S, Müller HW. Basal membrane-depleted scar in lesioned CNS: characteristics and relationships with regenerating axons. Neuroscience 1999; 93:321-33.
23. Klapka N, Muller HW. Collagen matrix in spinal cord injury. J Neurotrauma 2006; 23:422-35.
24. Kobayashi S, Koyama J, Yokouchi K, Fukushima N, Oikawa S, Moriizumi T. Functionally essential neuronal population of the facial motor nucleus. Neurosci Res 2003; 45:357-61.
25. Liang W, Han Q, Jin W, Xiao Z, Huang J, Ni H, Chen B, Kong J, Wu J, Dai J. The promotion of neurological recovery in the rat spinal cord crushed injury model by collagen-binding BDNF. Biomaterials 2010; 31:8634-41.
26. Choi D, Dunn LT. Facial nerve repair and regeneration: an overview of basic principles for neurosurgeons. Acta Neurochir (Wien) 2001; 143:107-14.
27. Bradbury EJ, McMahon SB. Spinal cord repair strategies: why do they work? Nat Rev Neurosci 2006; 7:644-53.
28. Myllyharju J, Kivirikko KI. Collagens, modifying enzymes and their mutations in humans, flies and worms. Trends Genet 2004; 20:33-43.
29. Ali SA, Pappas IS, Parnavelas JG. Collagen type IV promotes the differentiation of neuronal progenitors and inhibits astro-glial differentiation in cortical cell cultures. Brain Res Dev Brain Res 1998; 110:31-8.
30. Levitt P, Eagleson KL, Chan AV, Ferri RT, Lillien L. Signaling pathways that regulate specification of neurons in developing cerebral cortex. Dev Neurosci 1997; 19:6-8.
31. Tonge DA, Golding JP, Edbladh M, Kroon M, Ekström PE, Edström A. Effects of extracellular matrix components on axo-nal outgrowth from peripheral nerves of adult animals in vitro. Exp Neurol 1997; 146:81-90.
32. Houweling DA, Lankhorst AJ, Gispen WH, Bär PR, Joosten EA. Collagen containing neurotrophin-3 (NT-3) attracts re-growing injured corticospinal axons in the adult rat spinal cord and promotes partial functional recovery. Exp Neurol 1998; 153:49-59.
33. Cao J, Xiao Z, Jin W, Chen B, Meng D, Ding W, Han S, Hou X, Zhu T, Yuan B, Wang J, Liang W, Dai J. Induction of rat facial nerve regeneration by functional collagen scaffolds. Biomaterials 2013; 34:1302-10.
34. Klapka N, Muller HW. Collagen matrix in spinal cord injury. J Neurotrauma 2006; 23:422-35.
35. Tillet E, Ruggiero F, Nishiyama A, Stallcup WB. The mem-brane-spanning proteoglycan NG2 binds to collagens V and VI through the central nonglobular domain of its core protein. J Biol Chem 1997;272:10769-76.
36. Bachmann M, Conscience JF, Probstmeier R, Carbonetto S, Schachner M. Recognition molecules myelin-associated glyco-protein and tenascin-C inhibit integrinmediated adhesion of neural cells to collagen. J Neurosci Res 1995;40:458-70.
585





























