Embed Size (px)
Citation preview

lable at ScienceDirect
The Breast 18 (2009) 351–355
Contents lists avai
The Breast
journal homepage: www.elsevier .com/brst
Original article
The prognostic significance of single hormone receptor positive metastatic breastcancer: An analysis of three randomised phase III trials of aromatase inhibitors
R. Stuart-Harris a,*, B. Shadbolt b, C. Palmqvist a, H.A. Chaudri Ross c
a Medical Oncology Unit, The Canberra Hospital, Woden ACT 2606, Australiab The Centre for Advances in Epidemiology & Information Technology, The Canberra Hospital, Woden ACT 2606, Australiac Novartis Pharma AG, Basel, Switzerland
a r t i c l e i n f o
Article history:Received 26 July 2009Received in revised form7 September 2009Accepted 7 September 2009
Keywords:Estrogen receptorERProgesterone receptorPgRMetastatic breast cancerSurvival
* Corresponding author. Tel.: þ61 2 6244 2738; faxE-mail addresses: [email protected]
[email protected] (B. Shadbolt), [email protected]@novartis.com (H.A. Chaudri Ross).
0960-9776/$ – see front matter � 2009 Elsevier Ltd.doi:10.1016/j.breast.2009.09.002
a b s t r a c t
We analysed the outcomes of women with metastatic breast cancer (MBC) from three randomised phaseIII trials of aromatase inhibitors according to oestrogen receptor (ER) and progesterone receptor (PgR)status. Both receptors were analysed in 1010 of the 1870 women (54%), including 31 that were ER-/PgR-,which were excluded. Of the remaining 979, 726 (74%) were ERþ/PgRþ but 253 were single hormonereceptor positive (213 ERþ/PgR-, 40 ER-/PgRþ). Although there were no differences in clinical benefit ortime to progression, the median overall survival of women with ERþ/PgRþ tumours was significantlylonger than those with single HR positive tumours (800 versus 600 days, p¼ 0$01). In women with ERþtumours, the median overall survival of those with tumours that were also PgRþwas significantly longerthan those that were PgR- (800 versus 625 days, p¼ 0$02). The PgR status is an important prognosticfactor for survival in MBC.
� 2009 Elsevier Ltd. All rights reserved.
Introduction
About three quarters of breast cancers are oestrogen receptor(ER) positive (þ) and an ERþ tumour is usually also progesteronereceptor positive (PgRþ) whereas an ER negative (ER-) tumour isalso usually PgR-. In a minority of breast cancers only one hormonereceptor (HR) is positive (i.e. ERþ/PgR- or ER-/PgRþ). ERþ/PgR-tumours account for the majority of single HRþ tumours and ER-/PgRþ tumours are rare, possibly because a functioning ER isbelieved to be necessary for the expression of the PgR.
Predominantly, the HR status of a breast cancer is important asa predictive factor for response to endocrine therapy but the HRstatus may also be prognostic for survival.1,2 Most centres assessboth the ER and PgR status of a breast cancer routinely and, if eitheris positive, the tumour is classified as HR positive, although theutility of assessing both receptors routinely has been questioned.3
In metastatic breast cancer (MBC), very few studies have repor-ted response to endocrine therapy according to single or double HRstatus. The results of four small studies involving a total of 337 MBC
: þ61 2 6244 2887.(R. Stuart-Harris), bruce.
(C. Palmqvist), hilary_anne.
All rights reserved.
patients with MBC and at least one positive HR, suggest that patientswith single HRþ tumours may have a lower response rate toendocrine therapy than those with double HRþ tumours.4–7 A morerecent series of 342 women with ERþMBC noted that women withtumours that were also PgRþ were significantly more likely torespond to tamoxifen, had a significantly longer time to treatmentfailure (TTF) and significantly longer overall survival (OS) than thosewith PgR- tumours.8 In another series of 346 patients with MBC,those with ER- or PgR- tumours had a significantly shorter survivalin univariate analysis, although only PgR negativity remaineda significant predictor of worse survival in multivariate analysis.9
In early breast cancer (EBC), the results of the ATAC trial sug-gested that patients with ERþ/PgR- tumours who received anas-trozole had a significantly longer time to recurrence than thosewho received tamoxifen.10 However, when the HR results of 34% ofthe patients entered onto the monotherapy arms were reviewedcentrally, the PgR status did not appear to influence time torecurrence.11 A recent update of the MA17 trial found that thedisease free survival (DFS) and OS of patients who received fiveyears of letrozole as extended adjuvant therapy was significantlybetter in those with ERþ/PgRþ tumours than in those with ERþ/PgR- tumours,12 whereas the results of the BIG 1-98 trial indicatedthat the PgR status did not influence the benefit of adjuvantletrozole.13 The latest overview by the Early Breast Cancer Trialists’Collaborative Group found that the PgR status added little

R. Stuart-Harris et al. / The Breast 18 (2009) 351–355352
prognostic information, over and above the ER status, with respectto recurrence and mortality.14
A recent analysis of 1944 primary breast cancers showed that963 (55$3%) were ERþ/PgRþ, 272 (15$6%) were ERþ/PgR-, 60(3$4%) were ER-/PgRþ and 448 (25$7%) were ER-/PgR-.15 Thisanalysis revealed that the two groups of single HRþ tumoursappeared biologically and clinically distinct. The median age ofpatients with ERþ/PgR- tumours was significantly older thanpatients with ER-/PgRþ tumours. Grade 3 tumours were signifi-cantly more common in the ER-/PgRþ group, whereas grade 2tumours were more common in the ERþ/PgR- group. There were nosignificant differences in outcomes between the ERþ/PgR- and ER-/PgRþ groups, whose outcomes were midway between the doubleHRþ group (best outcomes) and the double HR- group (worstoutcomes). This study also found that in ERþ patients, those thatwere also PgRþ had a lower recurrence rate and better OS afteradjuvant endocrine therapy than those that were ERþ/PgR-.Another retrospective study of 1228 patients also observed that theDFS of patients with single HRþ tumours lay between those ofpatients with double HRþ and double HR- tumours.16
Laboratory assessment of ER and PgR
Initially, ER and PgR were assessed using biochemical ligandbinding assays (LBA), giving a quantitative result. These assays weretechnically difficult and required fresh tissue, frozen on collection.In recent years these LBAs have been replaced with immunohis-tochemical (IHC) assays which can be performed on archivaltumour material. There is good correlation of ER results by IHC andLBAs,17 but IHC is preferred because it is easier, safer, less expensiveand has equivalent or better ability to predict response to adjuvantendocrine therapy.18
The aims of the current study were to investigate whethertreatment outcomes (clinical benefit [CB], time to progression [TTP]and OS) differed between patients with single HRþ and doubleHRþ tumours entered onto three international, randomised, phaseIII controlled trials of aromatase inhibitors as second line therapyfor MBC. In addition, we analysed the outcomes of those patientswith ERþ tumours that were also PgRþ and compared them withpatients whose tumours were PgR- to assess whether the PgRstatus added additional prognostic information in ERþ patients.
Materials and methods
The data from three international, randomised, controlled,phase III trials of aromatase inhibitors in postmenopausal womenwith MBC, as second line therapy after antioestrogen therapy werecollected and pooled. The results of these studies have been pub-lished previously.19–21 The ANA trial19 compared anastrozole (1 mgor 10 mg daily) with megestrol acetate (160 mg daily). The AR/BC220 trial compared letrozole (0$5 mg or 2$5 mg daily) withmegestrol acetate (160 mg daily). The AR/BC321 trial comparedletrozole (0$5 mg or 2$5 mg daily) with aminoglutethimide(250 mg twice daily plus glucocorticoid supplementation). The datawere obtained from AstraZeneca for the ANA trial and fromNovartis for the AR/BC2 and AR/BC3 trials. The data obtainedincluded patient demographics, tumour HR status (by LBA or IHC)and patient outcomes, including objective response, TTP and OS.The study was approved by the local ethical boards of participatinginstitutions.
Design of the studies
Women entered into the trials were required to be post-menopausal, have a WHO performance status of 2 or less, have
a tumour that was ERþ or PgRþ or HR unknown, have an estab-lished diagnosis of MBC, have received prior first line antioestrogentherapy for metastatic disease, or have relapsed during or within 12months of adjuvant antioestrogen therapy. The ANA trial19 alsoallowed entry of patients known to have a tumour that was ER-/PgR-, if they had responded to endocrine therapy previously. Allthree trials allowed entry of patients who had received not morethan one line of chemotherapy for advanced disease. The AR/BC220
trial also allowed entry of patients with locally advanced orlocoregionally recurrent disease in addition to those with MBC. Allthree trials excluded patients with potentially rapidly progressivedisease or a history of prior malignancy.
The treatment protocols
The protocols for the AR/BC2 and the AR/BC3 trials were similar,apart from the comparator agent and the fact that the AR/BC2 trialwas double-blind whereas the AR/BC3 trial was open-label.Patients were seen for tumour evaluation before randomisationand then at three month intervals. Radiological investigations wereperformed at entry and again at six months if negative initially, or atthree month intervals, if positive initially.
In the ANA trial, patients were assessed four weeks prior toentry and then every four weeks for the first 24 weeks, and then atthree month intervals. Bone scans were ordered at 24 week inter-vals until there was evidence of disease progression or withdrawalfrom the trial. Other radiological investigations were performed at12 week intervals if positive initially, or as clinically indicated.
Outcomes
Clinical benefitAll three trials used UICC criteria for assessment of response,
which assigned patients to the categories of: complete response(CR), partial response (PR), stable disease (SD) or no change (NC), orprogressive disease (PD). In the ANA trial, an algorithm was used toassess response for those with measurable disease, but for thosewith non measurable disease, PR was not permitted and patientscould only be categorised as achieving CR, SD or PD. In all of thetrials, assignment of CR or PR required verification on two separateoccasions, at least four weeks apart. The two letrozole trials usedthe category of NC, whereas the ANA trial used SD. The ANA trialcategorised SD into <24 or >24 week’s duration, whereas in theletrozole trials, NC had to last at least 24 weeks, otherwise patientswere classed as inevaluable.
Time to progression and survivalThe three trials recorded TTF, TTP and OS. For our analysis we
used TTP (the interval between commencement of therapy and thetime of first assignment of PD) and OS, which were available in allthree trials.
Data modificationsThe classifications of CR, PR and SD from the three trials were
combined into a single category of CB and the ANA trial subclassi-fication of SD into <24 weeks or >24 weeks was ignored. The AR/BC2 and AR/BC3 databases had a combined TTF/TTP field (witha censor for each variable). TTP from the ANA trial and the AR/BC2and AR/BC3 trials were integrated. No attempt was made to contactthe authors of the trials to update the data and no comparisonswere made between the three trials.
Statistical methodsData were analysed using SPSS V16$0. The results were sum-
marised using univariate statistics including the means, standard
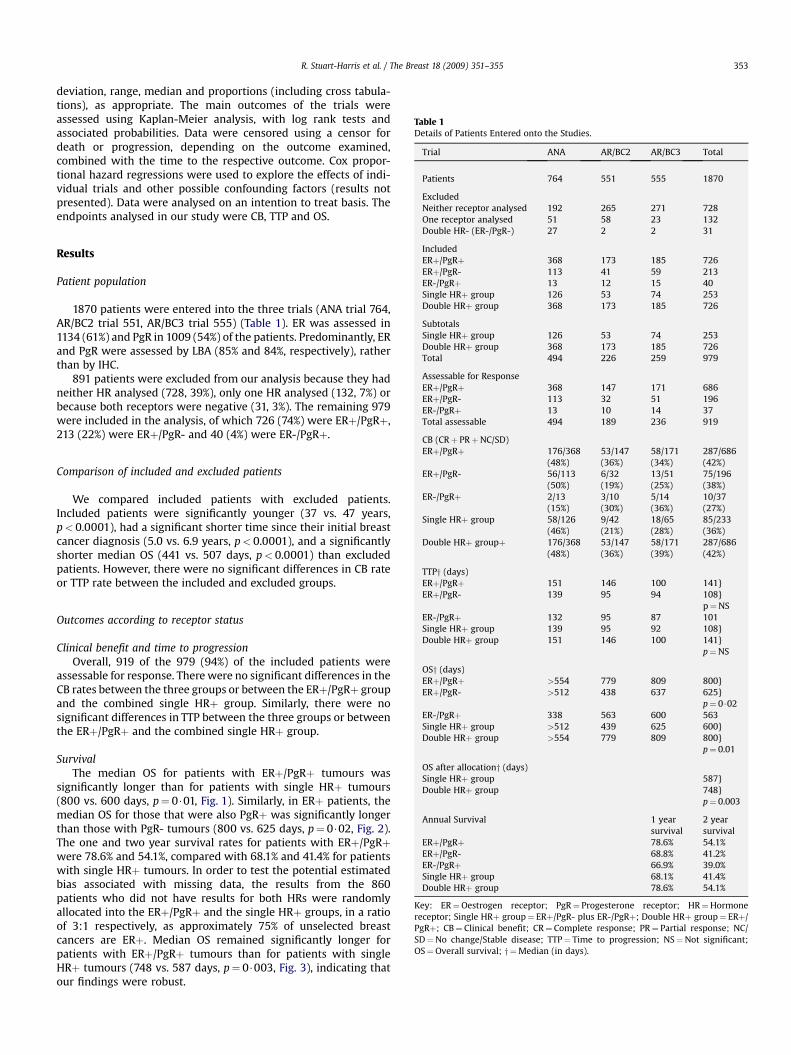
Table 1Details of Patients Entered onto the Studies.
Trial ANA AR/BC2 AR/BC3 Total
Patients 764 551 555 1870
ExcludedNeither receptor analysed 192 265 271 728One receptor analysed 51 58 23 132
R. Stuart-Harris et al. / The Breast 18 (2009) 351–355 353
deviation, range, median and proportions (including cross tabula-tions), as appropriate. The main outcomes of the trials wereassessed using Kaplan-Meier analysis, with log rank tests andassociated probabilities. Data were censored using a censor fordeath or progression, depending on the outcome examined,combined with the time to the respective outcome. Cox propor-tional hazard regressions were used to explore the effects of indi-vidual trials and other possible confounding factors (results notpresented). Data were analysed on an intention to treat basis. Theendpoints analysed in our study were CB, TTP and OS.
Double HR- (ER-/PgR-) 27 2 2 31
IncludedERþ/PgRþ 368 173 185 726ERþ/PgR- 113 41 59 213ER-/PgRþ 13 12 15 40Single HRþ group 126 53 74 253Double HRþ group 368 173 185 726
SubtotalsSingle HRþ group 126 53 74 253Double HRþ group 368 173 185 726Total 494 226 259 979
Assessable for ResponseERþ/PgRþ 368 147 171 686ERþ/PgR- 113 32 51 196ER-/PgRþ 13 10 14 37Total assessable 494 189 236 919
CB (CRþ PRþNC/SD)
Results
Patient population
1870 patients were entered into the three trials (ANA trial 764,AR/BC2 trial 551, AR/BC3 trial 555) (Table 1). ER was assessed in1134 (61%) and PgR in 1009 (54%) of the patients. Predominantly, ERand PgR were assessed by LBA (85% and 84%, respectively), ratherthan by IHC.
891 patients were excluded from our analysis because they hadneither HR analysed (728, 39%), only one HR analysed (132, 7%) orbecause both receptors were negative (31, 3%). The remaining 979were included in the analysis, of which 726 (74%) were ERþ/PgRþ,213 (22%) were ERþ/PgR- and 40 (4%) were ER-/PgRþ.
ERþ/PgRþ 176/368(48%)
53/147(36%)
58/171(34%)
287/686(42%)
ERþ/PgR- 56/113(50%)
6/32(19%)
13/51(25%)
75/196(38%)
ER-/PgRþ 2/13(15%)
3/10(30%)
5/14(36%)
10/37(27%)
Single HRþ group 58/126(46%)
9/42(21%)
18/65(28%)
85/233(36%)
Double HRþ groupþ 176/368(48%)
53/147(36%)
58/171(39%)
287/686(42%)
TTPy (days)ERþ/PgRþ 151 146 100 141}
Comparison of included and excluded patients
We compared included patients with excluded patients.Included patients were significantly younger (37 vs. 47 years,p< 0.0001), had a significant shorter time since their initial breastcancer diagnosis (5.0 vs. 6.9 years, p< 0.0001), and a significantlyshorter median OS (441 vs. 507 days, p< 0.0001) than excludedpatients. However, there were no significant differences in CB rateor TTP rate between the included and excluded groups.
ERþ/PgR- 139 95 94 108}p¼NS
ER-/PgRþ 132 95 87 101Single HRþ group 139 95 92 108}Double HRþ group 151 146 100 141}
p¼NS
OSy (days)ERþ/PgRþ >554 779 809 800}ERþ/PgR- >512 438 637 625}
p¼ 0$02ER-/PgRþ 338 563 600 563Single HRþ group >512 439 625 600}Double HRþ group >554 779 809 800}
p¼ 0.01
OS after allocationy (days)Single HRþ group 587}Double HRþ group 748}
p¼ 0.003
Annual Survival 1 yearsurvival
2 yearsurvival
ERþ/PgRþ 78.6% 54.1%ERþ/PgR- 68.8% 41.2%ER-/PgRþ 66.9% 39.0%Single HRþ group 68.1% 41.4%Double HRþ group 78.6% 54.1%
Key: ER¼Oestrogen receptor; PgR¼ Progesterone receptor; HR¼Hormonereceptor; Single HRþ group¼ ERþ/PgR- plus ER-/PgRþ; Double HRþ group¼ ERþ/PgRþ; CB¼ Clinical benefit; CR¼ Complete response; PR¼ Partial response; NC/SD¼No change/Stable disease; TTP¼ Time to progression; NS¼Not significant;OS¼Overall survival; y ¼Median (in days).
Outcomes according to receptor status
Clinical benefit and time to progressionOverall, 919 of the 979 (94%) of the included patients were
assessable for response. There were no significant differences in theCB rates between the three groups or between the ERþ/PgRþ groupand the combined single HRþ group. Similarly, there were nosignificant differences in TTP between the three groups or betweenthe ERþ/PgRþ and the combined single HRþ group.
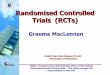
SurvivalThe median OS for patients with ERþ/PgRþ tumours was
significantly longer than for patients with single HRþ tumours(800 vs. 600 days, p¼ 0$01, Fig. 1). Similarly, in ERþ patients, themedian OS for those that were also PgRþ was significantly longerthan those with PgR- tumours (800 vs. 625 days, p¼ 0$02, Fig. 2).The one and two year survival rates for patients with ERþ/PgRþwere 78.6% and 54.1%, compared with 68.1% and 41.4% for patientswith single HRþ tumours. In order to test the potential estimatedbias associated with missing data, the results from the 860patients who did not have results for both HRs were randomlyallocated into the ERþ/PgRþ and the single HRþ groups, in a ratioof 3:1 respectively, as approximately 75% of unselected breastcancers are ERþ. Median OS remained significantly longer forpatients with ERþ/PgRþ tumours than for patients with singleHRþ tumours (748 vs. 587 days, p¼ 0$003, Fig. 3), indicating thatour findings were robust.
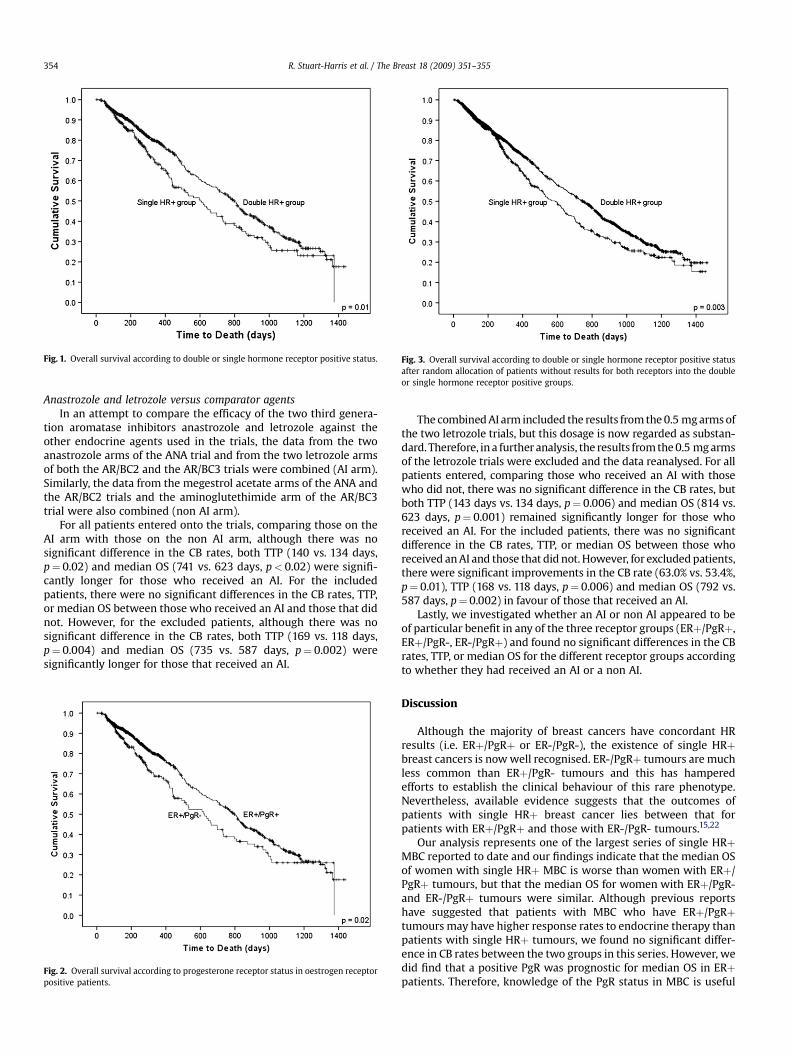
Fig. 1. Overall survival according to double or single hormone receptor positive status. Fig. 3. Overall survival according to double or single hormone receptor positive statusafter random allocation of patients without results for both receptors into the doubleor single hormone receptor positive groups.
R. Stuart-Harris et al. / The Breast 18 (2009) 351–355354
Anastrozole and letrozole versus comparator agentsIn an attempt to compare the efficacy of the two third genera-
tion aromatase inhibitors anastrozole and letrozole against theother endocrine agents used in the trials, the data from the twoanastrozole arms of the ANA trial and from the two letrozole armsof both the AR/BC2 and the AR/BC3 trials were combined (AI arm).Similarly, the data from the megestrol acetate arms of the ANA andthe AR/BC2 trials and the aminoglutethimide arm of the AR/BC3trial were also combined (non AI arm).
For all patients entered onto the trials, comparing those on theAI arm with those on the non AI arm, although there was nosignificant difference in the CB rates, both TTP (140 vs. 134 days,p¼ 0.02) and median OS (741 vs. 623 days, p< 0.02) were signifi-cantly longer for those who received an AI. For the includedpatients, there were no significant differences in the CB rates, TTP,or median OS between those who received an AI and those that didnot. However, for the excluded patients, although there was nosignificant difference in the CB rates, both TTP (169 vs. 118 days,p¼ 0.004) and median OS (735 vs. 587 days, p¼ 0.002) weresignificantly longer for those that received an AI.
Fig. 2. Overall survival according to progesterone receptor status in oestrogen receptorpositive patients.
The combined AI arm included the results from the 0.5 mg arms ofthe two letrozole trials, but this dosage is now regarded as substan-dard. Therefore, in a further analysis, the results from the 0.5 mg armsof the letrozole trials were excluded and the data reanalysed. For allpatients entered, comparing those who received an AI with thosewho did not, there was no significant difference in the CB rates, butboth TTP (143 days vs. 134 days, p¼ 0.006) and median OS (814 vs.623 days, p¼ 0.001) remained significantly longer for those whoreceived an AI. For the included patients, there was no significantdifference in the CB rates, TTP, or median OS between those whoreceived an AI and those that did not. However, for excluded patients,there were significant improvements in the CB rate (63.0% vs. 53.4%,p¼ 0.01), TTP (168 vs. 118 days, p¼ 0.006) and median OS (792 vs.587 days, p¼ 0.002) in favour of those that received an AI.
Lastly, we investigated whether an AI or non AI appeared to beof particular benefit in any of the three receptor groups (ERþ/PgRþ,ERþ/PgR-, ER-/PgRþ) and found no significant differences in the CBrates, TTP, or median OS for the different receptor groups accordingto whether they had received an AI or a non AI.
Discussion
Although the majority of breast cancers have concordant HRresults (i.e. ERþ/PgRþ or ER-/PgR-), the existence of single HRþbreast cancers is now well recognised. ER-/PgRþ tumours are muchless common than ERþ/PgR- tumours and this has hamperedefforts to establish the clinical behaviour of this rare phenotype.Nevertheless, available evidence suggests that the outcomes ofpatients with single HRþ breast cancer lies between that forpatients with ERþ/PgRþ and those with ER-/PgR- tumours.15,22
Our analysis represents one of the largest series of single HRþMBC reported to date and our findings indicate that the median OSof women with single HRþ MBC is worse than women with ERþ/PgRþ tumours, but that the median OS for women with ERþ/PgR-and ER-/PgRþ tumours were similar. Although previous reportshave suggested that patients with MBC who have ERþ/PgRþtumours may have higher response rates to endocrine therapy thanpatients with single HRþ tumours, we found no significant differ-ence in CB rates between the two groups in this series. However, wedid find that a positive PgR was prognostic for median OS in ERþpatients. Therefore, knowledge of the PgR status in MBC is useful

R. Stuart-Harris et al. / The Breast 18 (2009) 351–355 355
and we recommend that the PgR status of a breast cancer continueto be made available, routinely. We also analysed whether any ofthe different receptor groups gained particular benefit from an AI ora non AI, but found no significant differences in outcomes. There-fore, we were unable to confirm the previous suggestion that thirdgeneration aromatase inhibitors (anastrozole and letrozole) aremore effective than other agents with respect to survival.23 Inaddition, we found no evidence to support the suggestion from theATAC trial that anastrozole is more effective than a non AI inpatients with ERþ/PgR- tumours.10
We acknowledge a number of limitations in our study. Firstly,we had to rely on the original data from the three trials as we wereunable to update or validate the data. Secondly, the majority of theHR analyses were performed by LBA rather than IHC, which is nowthe preferred technique. We also acknowledge that the HR resultswere obtained from multiple different laboratories and thata central review of the HR results would have been preferable andthat this might have altered some of the HR results.13 Moreover, it isconceivable that the HR of the metastatic disease may have differedfrom the HR of the primary tumour.24 Nevertheless, we believe thatour findings are robust, despite these limitations.
The PgR is believed to be induced by the binding of oestrogen tothe ER, thereby producing various oestrogen responsive elements,including the PgR. As a result, the presence of the PgR has becomeaccepted as an indicator of a functioning ER. There are many potentialcauses for a breast cancer to have only one positive HR. The aetiologyof ER-/PgRþ- tumours is particularly interesting because, if a func-tioning ER is necessary for the production of the PgR, then ER-/PgRþtumours should not exist. Further investigation into this interestingphenotype should yield a better understanding of the molecularmechanisms behind the endocrine sensitivity of breast cancer.
Conclusions
By analysing the data from these three randomised phase III trialsof aromatase inhibitors as second line therapy in MBC, we haveestablished that those patients with tumours that are double HRþhave a longer median OS than those with tumours that are only singleHRþ. In addition, we have established that, in patients with ERþpositive tumours, those whose tumours are also PgRþ have a longermedian survival than those whose tumours are PgR-. Thus, a positivePgR is a prognostic factor for OS in MBC and we recommend that thePgR status of a tumour continue to be assessed routinely.
Conflicts of interest
R Stuart-Harris, B Shadbolt and C Palmqvist have no conflicts ofinterest to declare. HA Chaudri Ross is an employee of Novartis andowns stock in Novartis.
Acknowledgements
We are grateful to both AstraZeneca and Novartis for providingthe data from their trials.
References
1. Collett K, Hartveit F, Skjaerven R, Maehle BO. Prognostic role of oestrogen andprogesterone receptors in patients with breast cancer: relation to age andlymph node status. J Clin Pathol 1996;49:920–5.
2. Elledge RM, Green S, Pugh R, Allred DC, Clark GM, Hill J, et al. Estrogen receptor(ER) and progesterone receptor (PgR), by ligand-binding assay compared withER, PgR and pS2, by immuno-histochemistry in predicting response totamoxifen in metastatic breast cancer: a southwest oncology group study. Int JCancer 2000;89:111–7.
3. Olivotto IA, Truong PT, Speers CH, Bernstein V, Allan SJ, Kelly SJ, et al. Time tostop progesterone receptor testing in breast cancer management. J Clin Oncol2004;22:1769–70.
4. Osborne CK, Yochmowitz MG, Knight 3rd WA, McGuire WL. The value ofestrogen and progesterone receptors in the treatment of breast cancer. Cancer1980;46(12 Suppl.):2884–8.
5. Bloom ND, Tobin EH, Schreibman B, Degenshein GA. The role of progesteronereceptors in the management of advanced breast cancer. Cancer 1980;45:2992–7.
6. Young PC, Ehrlich CE, Einhorn LH. Relationship between steroid receptors andresponse to endocrine therapy and cytotoxic chemotherapy in metastaticbreast cancer. Cancer 1980;46(12 Suppl.):2961–3.
7. Barnes DM, Harris WH, Smith P, Millis RR, Rubens RD. Immunohistochemicaldetermination of oestrogen receptor: comparison of different methods ofassessment of staining and correlation with clinical outcome of breast cancerpatients. Br J Cancer 1996;74:1445–51.
8. Ravdin PM, Green S, Dorr TM, McGuire WL, Fabian C, Pugh RP, et al. Prognosticsignificance of progesterone receptor levels in estrogen receptor-positivepatients with metastatic breast cancer treated with tamoxifen: results ofa prospective southwest oncology group study. J Clin Oncol 1992;10:1284–91.
9. Chang J, Clark GM, Allred DC, Mohsin S, Chamness G, Elledge RM. Survival ofpatients with metastatic breast carcinoma: importance of prognostic markersof the primary tumour. Cancer 2003;97:545–53.
10. Dowsett M, Cuzick J, Wale C, Howell T, Houghton J, Baum M. Retrospectiveanalysis of time to recurrence in the ATAC trial according to hormone receptorstatus: an hypothesis-generating study. J Clin Oncol 2005;23:7512–7.
11. Dowsett M, Allred DC, Knox J, Quinn E, Salter J, Wale C, et al. Relationshipbetween quantitative estrogen and progesterone receptor expression andhuman epidermal growth factor receptor 2 (HER-2) status with recurrence inthe arimidex, tamoxifen, alone or in combination trial. J Clin Oncol2008;26:1059–65.
12. Goss PE, Ingle JN, Martino S, Robert NJ, Muss HB, Piccart MJ, et al. Efficacy ofletrozole extended adjuvant therapy according to estrogen receptor andprogesterone receptor status of the primary tumor: national cancer institute ofCanada clinical trials group MA 17. J Clin Oncol 2007;25:2006–11.
13. Viale G, Regan MM, Maiorano E, Mastropasqua MG, Dell’Orto P,Rasmussen BB, et al. Prognostic and predictive value of centrally reviewedexpression of estrogen and progesterone receptors in a randomized trialcomparing letrozole and tamoxifen adjuvant therapy for postmenopausalearly breast cancer: BIG 1-98. J Clin Oncol 2007;25:3846–52.
14. Early breast cancer trialist’s collaborative group (EBCTCG). Effects of chemo-therapy and hormonal therapy for early breast cancer on recurrence and15-year survival: an overview of the randomised trials. Lancet 2005;365:1687–717.
15. Rakha EA, El-Sayed ME, Green AR, Paish EC, Powe DG, Gee J, et al. Biologic andclinical characteristics of breast cancer with single hormone receptor-positivephenotype. J Clin Oncol 2007;25:4772–8.
16. Colomer R, Beltran M, Dorcas J, Cortes-Funes H, Hornedo J, Valentin V, et al. It isnot time to stop progesterone receptor testing in breast cancer. J Clin Oncol2005;23:3868–70.
17. Saccani Jotti G, Johnston SR, Salter J, Detre S, Dowsett M. Comparison of newimmunohistochemical assay for oestrogen receptor in paraffin wax embeddedbreast carcinoma tissue with quantitative enzyme immunoassay. J Clin Pathol1994;47:900–5.
18. Harvey JM, Clark GM, Osborne CK, Allred DC. Estrogen receptor status byimmunohistochemistry is superior to the ligand-binding assay for predictingresponse to adjuvant endocrine therapy in breast cancer. J Clin Oncol1999;17:1474–81.
19. Buzdar A, Jonat W, Howell A, Jones SE, Blomqvist C, Vogel CL, et al, for theArimidex study group. Anastrozole, a potent and selective aromatase inhibitor,versus megestrol acetate in postmenopausal women with advanced breastcancer: results of overview analysis of two phase III trials. J Clin Oncol1996;14:2000–11.
20. Dombernowsky P, Smith I, Falkson G, Leonard R, Panasci L, Bellmunt J, et al.Letrozole, a new oral aromatase inhibitor for advanced breast cancer: double-blind randomized trial showing a dose effect and improved efficacy andtolerability compared with megestrol acetate. J Clin Oncol 1998;16:453–61.
21. Gershanovich M, Chaudri HA, Campos D, Lurie H, Bonaventura A, Jeffrey M,et al. Letrozole, a new oral aromatase inhibitor: randomized trial comparing2.5 mg daily. 5 mg daily and aminoglutethimide in postmenopausal womenwith advanced breast cancer. Letrozole International Trial Group (AR/BC3). AnnOncol 1998;6:639–45.
22. Fisher ER, Sass R, Fisher B. Pathologic findings from the national surgicaladjuvant breast project. Correlations with concordant and discordant estrogenand progesterone receptors. Cancer 1987;59:1554–9.
23. Mauri D, Pavlidis N, Polyzos NP, Ioannidis JPA. Survival with aromatase inhib-itors and inactivators versus standard hormonal therapy in advanced breastcancer: meta-analysis. J Natl Cancer Inst 2006;98:1285–91.
24. MacFarlane R, Speers C, Masoudi H, Chia S. Molecular changes in the primarybreast cancer versus relapsed/metastatic lesion from a large population-baseddatabase and tissue microarray series. J Clin Oncol 2008;26(May 20 suppl).Abstract 1000.