Embed Size (px)
DESCRIPTION
THE PROFILE OF THE HEART FAILURE PATIENT WHO DOESN’T BENEFIT FROM AN ICD. Giosuè Mascioli, MD, FESC Humanitas Gavazzeni - Bergamo. Death in Heart Failure. Possible role of ICD. ICD. ICD ?. Modified from: Henkel DM, Circ Heart Fail, Jul 2008. ICD benefit is not homogeneous. - PowerPoint PPT Presentation
Citation preview

THE PROFILE OF THE HEART FAILURE PATIENT WHO DOESN’T BENEFIT
FROM AN ICD
Giosuè Mascioli, MD, FESCHumanitas Gavazzeni - Bergamo

Death in Heart Failure
ICDPossible role
of ICD
ICD ?
Modified from: Henkel DM, Circ Heart Fail, Jul 2008

ICD benefit is not homogeneous
Risk FactorRisk Factor HRHR 95% CI95% CI p valuep value
NYHA > 2 1.87 1.23 - 2.86 0.004
AF 1.87 1.05 - 3.22 0.034
QRS > 120 msec 1.65 1.08 - 2.51 0.020
Age > 70 yrs 1.57 1.02 - 2.41 0.042
BUN>26 mg/dl (and < 50)
1.56 1.00 - 2.42 0.048
VHR: BUN ≥ 50 mg/dl and serum creatinine ≥ 2.5 mg/dl
Goldenberg I, JACC Jan 2008

Greater or lesser benefit
Burden of cardiovascular illness
Mag
nit
ud
e o
f b
en
efi
t (l
ow
er
nu
mb
er
need
ed
to t
reat)
Cost-efficacythreshold
Low risk of SDLow overall risk of death
High risk of SDIntermediate overall
risk of death
Intermediate risk of SDHigh overall risk of death

The deadly duo
Goldenberg I, Circulation Jun 2006

ICD therapy and Competing Death
First appropriate ICD therapyDeath before first appropriate ICD therapy
Koller MT, Circulation Apr 2008

ICD and Comorbidities
Bruch C, Europace Sep. 2007

THE SICKEST THE WORST ? - 1
Analysis of MADIT 2 patients:
Mutivariate analysis of predictor of mortality:
Age > 65 yrs
NYHA class III - IV
AF
Increased level of BUNCygankiewicz I, Heart Rhythm Apr 2009

THE SICKEST THE WORST ? - 2
BMI < 26
Schernthaner C, Croat Med Journ 2007

Reverse epidemiology and acute HF
Burger AJ, Int J Cardiol Mar 2008

BMI and unadjusted all-cause mortality
Curtis JP, Arch Intern Med 2005

Importance of number of HF episodes
Setoguchi S, CMAJ Mar 2009

Badly treated,worst prognosis- 1
In MADIT 2, use of ICD was associated with a significant 39% increase in risk of HF
Risk can be reduced used the corrected therapy:
With B-blockers + ACE-inhibitors HR 0.36
With B-blockers only HR 0.51 (metoprolol 0.49, carvedilol 0.48)
With ACE-inhibitors only HR 0.64 (p NS)
Pietrasik G, JCE Apr. 2009

Badly treated,worst prognosis- 2
Gardiwal A, Europace Oct 2008

Predictors of early mortality in ICD patients
ParameterParameter p value in univ. anal.p value in univ. anal. p value in multiv. anal.p value in multiv. anal.
History of AFHistory of AF < 0.0001 p < 0.001
DiabetesDiabetes = 0.0001 = 0.004
Failure to use statinsFailure to use statins < 0.001 NS
Use of digitalisUse of digitalis < 0.0001 NS
Use of diureticsUse of diuretics < 0.0001 NS
Low BMILow BMI < 0.0001 = 0.001
Increasing AGEIncreasing AGE < 0.0001 NS
Low EFLow EF < 0.0001 NS
Low activity hoursLow activity hours < 0.0001 NS
Elevated resting HRElevated resting HR = 0.014 NS
Low MAPLow MAP = 0.007 = 0.04
Poor NYHA classPoor NYHA class < 0.0001 = 0.006
Stein KM, Europace Mar 2009

Predictors of late mortality in ICD patients
FactorFactor Hazard RatioHazard Ratio(95% CI)(95% CI) p valuep value
DigoxinDigoxin1.86
(1.12 - 2.86)= 0.0046
Loops diureticsLoops diuretics1.59
(1.06 - 2.38)= 0.024
ACE-inhibitors or ACE-inhibitors or Aldosterone Aldosterone
receptor blockersreceptor blockers
0.50(0.31 - 0.80)
= 0.0038
Thibodeau JB, Am J Cardiol Mar 2008

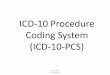
ICD and kidney disease
Stage/
Age
Stage 1
Stage 2
Stage 3
Stage 4
Stage 5
< 65 yrs
< 75 yrs
< 80 yrs
Favo
red
Unf
avor
ed
* At standard procedural mortality. At procedural mortality rates increased,age thresholds for ICD implant decrease.
Amin MS, JCE Dec. 2008

ICD and eGRF
Goldenberg I, Am J Cardiol Aug 2006

Cause-specific mortality in ICD patients: evadef study - 1
Marijon E, Am Heart J Feb 2009

Cause-specific mortality in ICD patients: evadef study - 2
Among characteristics at implantation:
EF < 30% and history of AF related to SCD
Age, NYHA class, systemic HT, QRS duration, EF < 30% and lack of B-blockers related to HF death
An EF < 30% at implant appears to be the most important predictor of ICD-unresponsive SCD
Marijon E, Am Heart J Feb 2009

Age and ICDs- 1
Healey JS, Eur Heart J Feb 2007

Age and ICDs- 2
Cause - specific mortality ratesAge < 75 yrsAge < 75 yrs
(1614 pts)(1614 pts)Age ≥ 75 yrsAge ≥ 75 yrs
(252 pts)(252 pts) p valuep value
Arrhythmic deathArrhythmic death 3,84 6,73 0,03
Heart Failure DeathHeart Failure Death 3,96 8,74 0,001
Non-cardiac deathNon-cardiac death 1,51 4,72 0,001
Non-arrhythmic deathNon-arrhythmic death 5,47 13,46 0,001
All-cause deathAll-cause death 9,31 20,19 0,001
Arrhythmic/All-cause Arrhythmic/All-cause death ratiodeath ratio
0,41 0,33
Healey JS, Eur Heart J Feb 2007

Conclusions - 1
We MUST keep in mind that we do not use ICD to reduce sudden death, but to reduce TOTAL mortality
If we cannot reach this goal, to implant an ICD is absolutely USELESS (if not negative for the patient)
The problem is: how I identify patients whose greater risk is to die of non cardiac cause of of HF ?

Conclusions - 2
Predictors od adverse prognosis in HF can be used to identify patients whose prognosis do not deserve an ICD
Among this factor we can recognize: non optimal drug therapy, too low EF, comorbidities, AF, low BMI and - particularly - kidney function
Score tables can be of some help in taking the right decision, together with good clinical sense

Extending Life, Defibrillators Can Prolong Misery
By Gina KolataMarch 25, 2002
Out of the Blue, a Lightning Bolt to the Heart
By Sandeep Jahuar Febrary 10, 2004

The final answer ...

... and the final comment
I’ve stopped smoking. My life will be one week longer.And that week will rain all the time!
Woody Allen