Embed Size (px)
Citation preview
2007; 29: e269–e275
WEB PAPER
The profession of medicine: a joint US–Germancollaborative project in medical education
REGINE WOOD TILLMANNS1,2,4, ANNA RINGWELSKI1, JOHANNA KRETSCHMANN2,LUITA D. SPANGLER3 & RAYMOND H. CURRY1
1Northwestern University Feinberg School of Medicine, USA, 2Charite – Universitatsmedizin Berlin, Germany, 3FreieUniversitat Berlin, Germany, 4Texas Tech University Health Sciences Center School of Medicine at El Paso, USA
Abstract
Background: International collaborations between medical institutions occur frequently in research and clinical training, but less
often in undergraduate medical education. Collaborative programs in psychosocial, ethical and cultural topics are rare. ‘‘The
Profession of Medicine’’, an elective undergraduate course based on the ‘‘Patient, Physician and Society’’ curriculum at
Northwestern University’s Feinberg School of Medicine in Chicago, USA, was introduced in 2005 at the Charite–
Universitatsmedizin Berlin, Germany, in order to provide students with a learning opportunity in this field and to introduce an
international context to student education.
Methods: The five-day course is offered to preclinical medical students twice a year and includes topics such as cultural diversity,
end of life issues, mistakes in medicine, vulnerable populations, and interactions with the pharmaceutical industry. The course
language is English, in a format consisting of both plenary and small group sessions. To date, one-fifth of the instructors have been
from the U.S. institution. Educational methods include small group discussions, presentations by guest speakers, movie and video
clips, role plays, and reading and writing assignments.
Results: The participants have evaluated the course very favourably, with average scores ranging from 1.2 to 1.5 (1¼ best/agree
the most and 5¼worst/agree the least). Pre- and post-course self-assessment with regard to knowledge, interest and professional
attitude revealed a statistically significant increase for all course topics.
Conclusions: In sum, the integration of Northwestern University’s Feinberg School of Medicine’s ‘‘Patient, Physician and Society’’
course concept into the Charite - Universitatsmedizin Berlin has been an effective method to develop students’ professional skills
and to stimulate international educational collaboration.
Background
Owing to groundbreaking reforms in medical education in
the U.S. in the eighties (Association of American Medical
Colleges 1984), by the mid-nineties courses devoted to
communication skills, personal and professional ethics,
medical humanities and behavioural sciences had become
incorporated into educational programs as integrated,
comprehensive curricula at many U.S. medical schools
(Makoul & Curry 1998b). The ‘‘Patient, Physician and
Society’’ course is one such curriculum, introduced at
Northwestern University’s Feinberg School of Medicine in
1993. Initially encompassing about 30% of the first and
second year curriculum at Northwestern, and now extend-
ing into the third and fourth years as well, the course is
designed to provide a comprehensive, integrated introduc-
tion to professional skills and perspectives, and to
familiarize students with the concept of patient-centred
medicine. Curricular units address such topics as personal
and professional ethics, medical humanities, behavioural
sciences, physician-patient communication, health services
organization and financing, the health of vulnerable groups,
and cultural dynamics in medicine. Course sessions focus
on active and interactive learning formats, with an
educational philosophy of encouraging students to find
answers on their own (Makoul & Curry 1998b;
Montgomery et al. 2003).
In Germany, reform efforts in medical education have
also been under way (Murrhardter Kreis 1989, 1995;
Wissenschaftsrat 1992), but have not to date resulted in
comprehensive curricula such as those described by Makoul &
Curry (1998a, b) in the United States. Nevertheless, innovative
Practice points
. Comprehensive courses in professional skills and
perspectives have become a common curricular
component in U.S. medical schools.
. The ‘‘translation’’ of one of these courses to a medical
school in Germany was well received by students
electing the course.
. Among the many benefits of this collaboration, a
meaningful inter-institutional relationship has developed
between the two schools.
Correspondence: Regine Wood Tillmanns, MD, FACP, Texas Tech Health Sciences Center, Department of Internal Medicine, School of Medicine at
El Paso, 4800 Alberta Avenue, El Paso, Texas 79905, USA. Email: [email protected]
ISSN 0142–159X print/ISSN 1466–187X online/07/09-100269–7 � 2007 Informa UK Ltd. e269DOI: 10.1080/01421590701551706
Med
Tea
ch D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y Su
ny G
enes
eo o
n 10
/27/
14Fo
r pe
rson
al u
se o
nly.

courses, projects, and reformed curricula emphasising the
psychosocial, ethical and cultural dimensions of medicine
have been developed and offered sporadically through
individual efforts, through both faculty and student
initiatives (Schuppel et al. 1998; Kiessling et al. 2003;
Schildmann et al. 2004; Burger 2006).
The Charite – Universitatsmedizin Berlin is Germany’s
largest medical school, formed in 2003 by the fusion of the
medical faculties of Humboldt University (in the former
East Berlin) and Free University (West Berlin). In Germany,
medical education is based on a six-year medical curriculum,
divided into a preclinical part (first and second year), a clinical
part (third to fifth year), and a final practical year. All courses
are typically in German, are required, and are taught in lecture-
style formats, seminars, bedside teaching and practical training
(Pabst 1995). In 2003, licensing regulation reforms went into
effect, mandating one elective course in each of the
preclinical and clinical stages of the curriculum (Von Jagow
& Loholter 2006).
International collaborations and interactions between
medical institutions occur frequently in the fields of research
and clinical training, while less frequently in undergraduate
medical education (Armstrong & Fischer 2001; De Vries et al.
2002; Imperato 2004; Margolis et al. 2004; Finkel & Fein 2006).
To our knowledge, no international partnerships between
medical schools have been described in the field of
psychosocial education and professional skills. In this report,
we present the course ‘‘The Profession of Medicine’’, the
implementation of a joint international project in this area of
undergraduate medical education between Charite –
Universitatsmedizin Berlin, Germany, and Northwestern
University Feinberg School of Medicine Chicago, U.S.A. The
course is founded on the concepts and borrows from the
content of Northwestern’s ‘‘Patient, Physician and Society’’
curriculum, and was introduced at Charite –
Universitatsmedizin Berlin in 2005 as an elective during the
preclinical stage of medical school.
Course description
Course topics are guided by the content and philosophy of the
‘‘Patient, Physician and Society’’ curriculum at Northwestern
University’s Feinberg School of Medicine (Makoul & Curry
1998a, b) and are currently devoted to the following subjects:
Cultural Diversity in Medicine, Making Mistakes, End-of-Life
Issues, Vulnerable Groups, and Interactions with the
Pharmaceutical Industry. The course has the following four
educational objectives: (1) to cultivate interest in and respect
for the values that characterise medical practice, (2) to
encourage attention to the social, cultural, and ethical aspects
of medicine, (3) to consider the experiences of the patient,
family and physician, and (4) to introduce students to
situations and problems that they will likely deal with as
physicians. The course director is typically assisted by four
student teaching assistants or co-instructors who have
participated in the course in a previous session. They are
oriented to small group teaching in a pre-course meeting with
the course director, and receive a small stipend.
The course is a week\long seminar, offered as an elective
during the final weeks of spring and autumn break. The daily
course sessions are each three hours long, and divided into
three parts. During the first hour, the topic is introduced,
typically with a ‘‘trigger tape’’ followed by a short discussion
with the whole group. In the second hour, the class divides
up into small groups of 6–8 students, each led by the course
director or a teaching assistant. In the third hour, the entire
class meets again in order to present the small groups’
discussion results as a role play or in a debate, or to listen to
a guest speaker’s presentation on the topic.
Registration is open to all students enrolled in the
preclinical years at Charite – Universitatsmedizin Berlin.
The course is announced via a medical student internet
forum and student mailing lists. Acceptance in the course
follows a first come, first serve basis, up to a maximum of
40 students. The course syllabus is sent to the students
via electronic mail approximately 6–8 weeks prior to the
beginning of the course.
Medical school policy requires that the course be graded,
and stratified into ‘‘sehr gut’’ (very good ), ‘‘gut’’ ( good),
‘‘befriedigend’’ (satisfactory), and ‘‘ausreichend’’ (sufficient)
categories. This is accomplished through a point system based
on attendance, participation, knowledge, and quality of the
writing assignments.
Course evaluation as ofAugust 2006
By August 2006, a total of 142 students had participated in the
course during four different sessions. Almost 75% of partici-
pants to date have been female, compared to a female
student body of approximately 64% at the Charite –
Universitatsmedizin Berlin (Humboldt – Universitat 2005).
Questionnaires. Upon the conclusion of the course, students
completed a questionnaire addressing course content, effi-
ciency, and the quality of instruction. They rated the course
very favourably, with average scores between 1.2 and 1.5,
with 1 being the best, 5 being the worst value (Table 1).
Students indicated a high propensity to recommend the course
to others, and in fact more than 50% were taking the
course based on recommendations by previous course
participants.
Students were also asked to rank their motivations
to participate in the course. The most important of these was
the choice of course topics, followed by the fact that the course
was given in English (Table 2). Timing was an intermediate
factor, and place and ease of getting a certificate were rated
as of lesser importance.
Pre- and post - course surveys. In order to obtain information
about educational outcomes, students were asked to estimate
their knowledge, interest and professional attitude pertaining
to the course topics by completing surveys before and after the
course. Pre- and post course self-assessment scores were
compared via a t-test applied to all three variables of
knowledge, interest and professional attitude. Pre-course
knowledge was low, with a statistically significant increase in
all five course topics after completion of the course.
R. W. Tillmanns et al.
e270
Med
Tea
ch D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y Su
ny G
enes
eo o
n 10
/27/
14Fo
r pe
rson
al u
se o
nly.
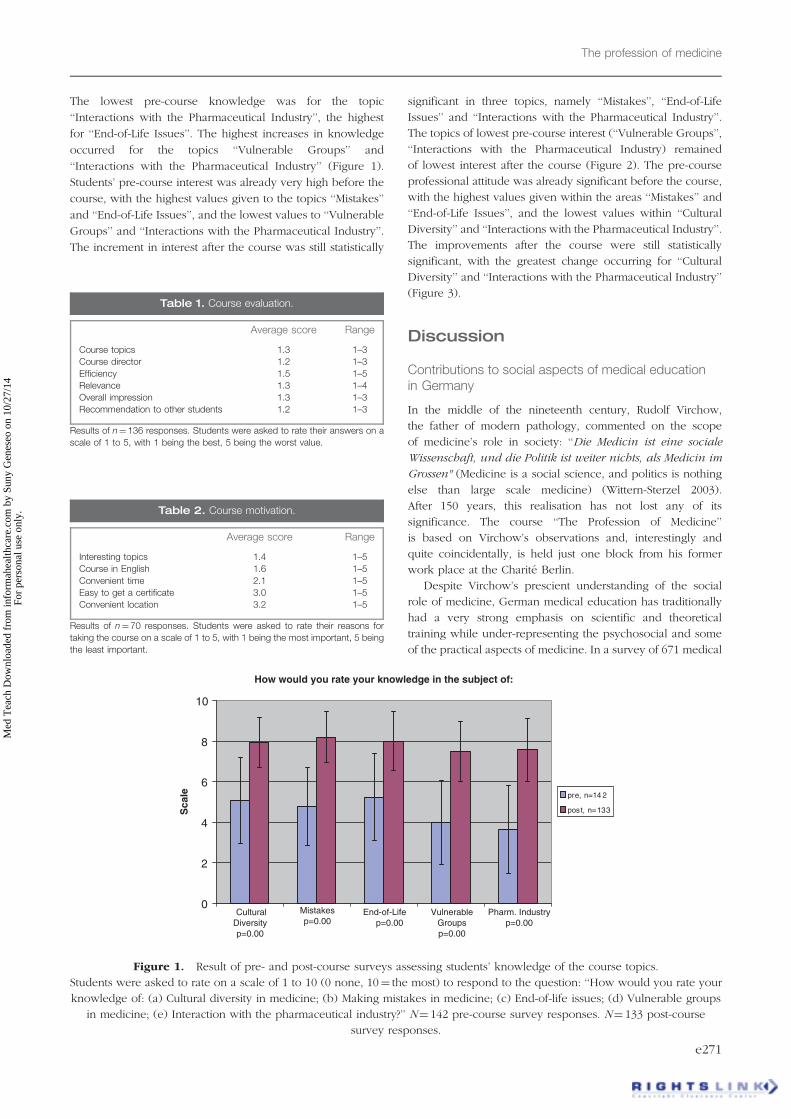
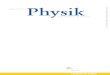
The lowest pre-course knowledge was for the topic
‘‘Interactions with the Pharmaceutical Industry’’, the highest
for ‘‘End-of-Life Issues’’. The highest increases in knowledge
occurred for the topics ‘‘Vulnerable Groups’’ and
‘‘Interactions with the Pharmaceutical Industry’’ (Figure 1).
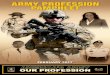
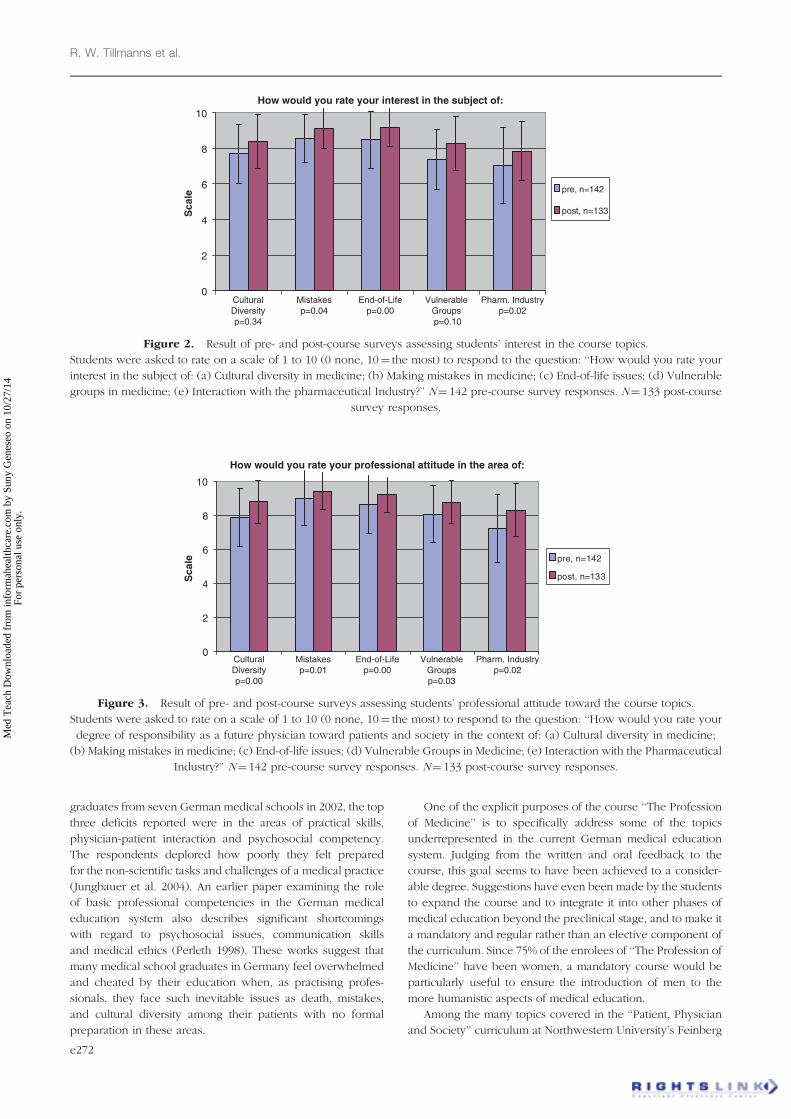
Students’ pre-course interest was already very high before the
course, with the highest values given to the topics ‘‘Mistakes’’
and ‘‘End-of-Life Issues’’, and the lowest values to ‘‘Vulnerable
Groups’’ and ‘‘Interactions with the Pharmaceutical Industry’’.
The increment in interest after the course was still statistically
significant in three topics, namely ‘‘Mistakes’’, ‘‘End-of-Life
Issues’’ and ‘‘Interactions with the Pharmaceutical Industry’’.
The topics of lowest pre-course interest (‘‘Vulnerable Groups’’,
‘‘Interactions with the Pharmaceutical Industry) remained
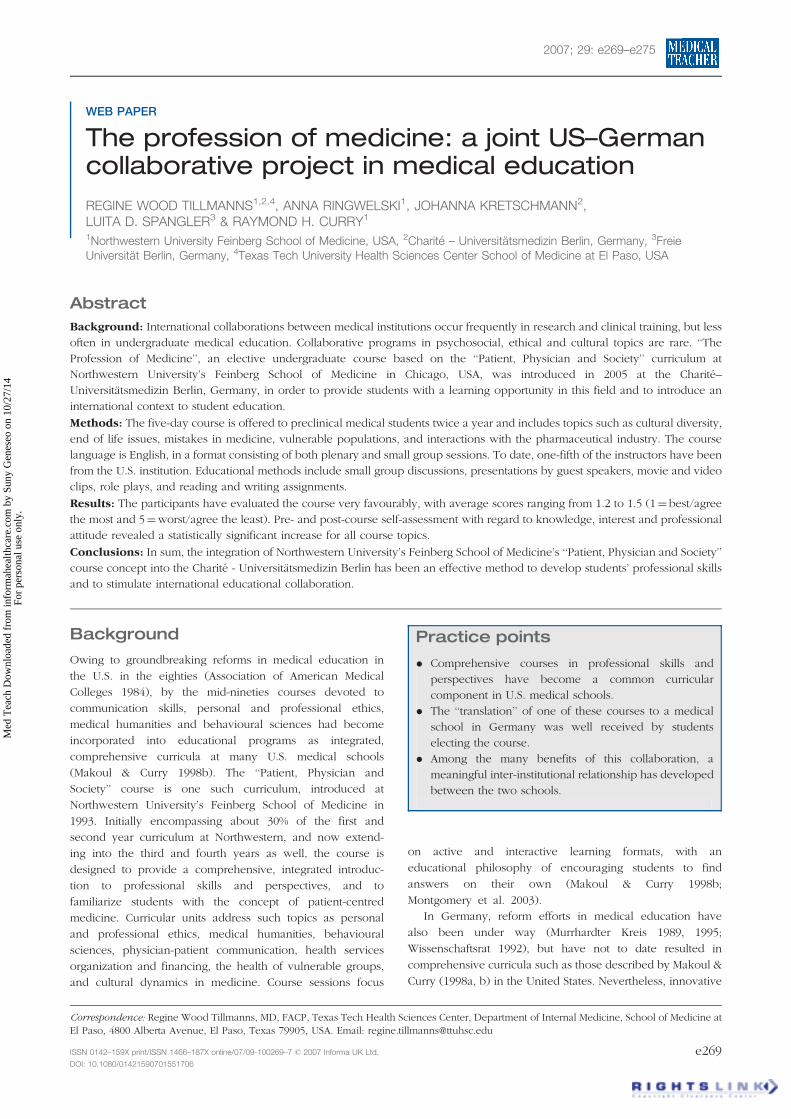
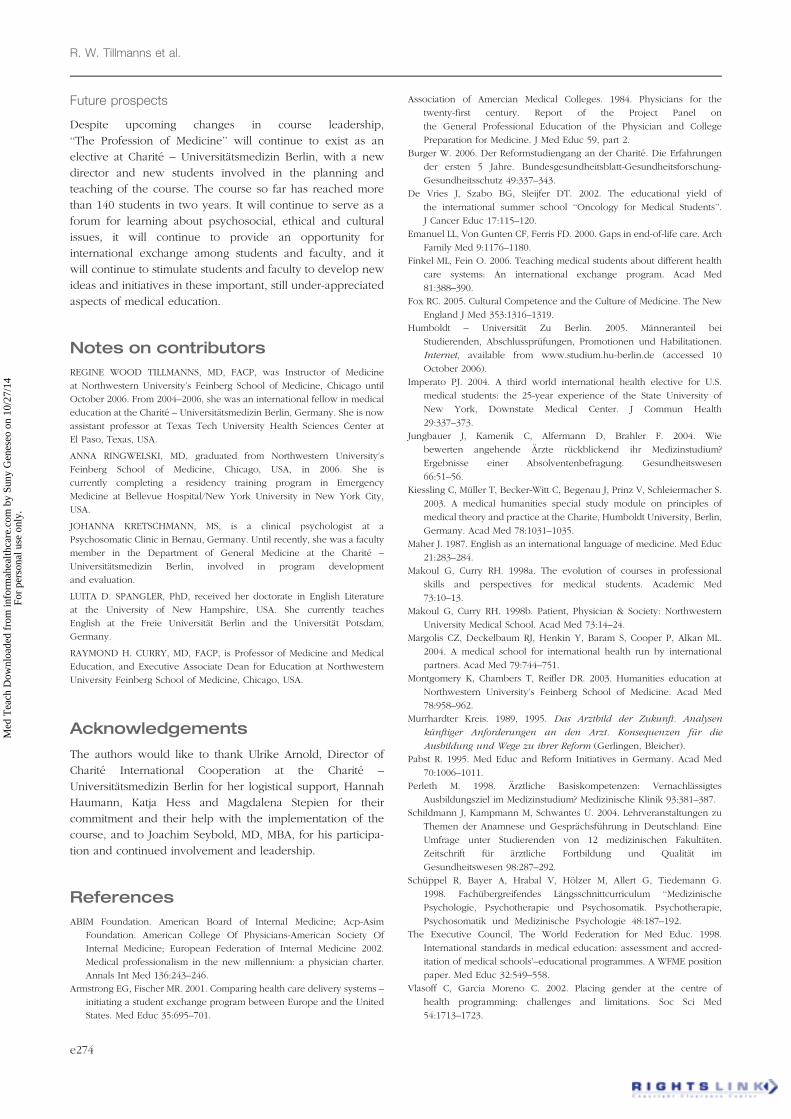
of lowest interest after the course (Figure 2). The pre-course
professional attitude was already significant before the course,
with the highest values given within the areas ‘‘Mistakes’’ and
‘‘End-of-Life Issues’’, and the lowest values within ‘‘Cultural
Diversity’’ and ‘‘Interactions with the Pharmaceutical Industry’’.
The improvements after the course were still statistically
significant, with the greatest change occurring for ‘‘Cultural
Diversity’’ and ‘‘Interactions with the Pharmaceutical Industry’’
(Figure 3).
Discussion
Contributions to social aspects of medical educationin Germany
In the middle of the nineteenth century, Rudolf Virchow,
the father of modern pathology, commented on the scope
of medicine’s role in society: ‘‘Die Medicin ist eine sociale
Wissenschaft, und die Politik ist weiter nichts, als Medicin im
Grossen" (Medicine is a social science, and politics is nothing
else than large scale medicine) (Wittern-Sterzel 2003).
After 150 years, this realisation has not lost any of its
significance. The course ‘‘The Profession of Medicine’’
is based on Virchow’s observations and, interestingly and
quite coincidentally, is held just one block from his former
work place at the Charite Berlin.
Despite Virchow’s prescient understanding of the social
role of medicine, German medical education has traditionally
had a very strong emphasis on scientific and theoretical
training while under-representing the psychosocial and some
of the practical aspects of medicine. In a survey of 671 medical
Table 2. Course motivation.
Average score Range
Interesting topics 1.4 1–5
Course in English 1.6 1–5
Convenient time 2.1 1–5
Easy to get a certificate 3.0 1–5
Convenient location 3.2 1–5
Results of n¼70 responses. Students were asked to rate their reasons for
taking the course on a scale of 1 to 5, with 1 being the most important, 5 being
the least important.
How would you rate your knowledge in the subject of:
0
2
4
6
8
10
Cultural Diversity p=0.00
Mistakes p=0.00
End-of-Life p=0.00
Vulnerable Groups p=0.00
Pharm. Industry p=0.00
Sca
le pre, n=14 2
post, n=133
Figure 1. Result of pre- and post-course surveys assessing students’ knowledge of the course topics.
Students were asked to rate on a scale of 1 to 10 (0 none, 10¼ the most) to respond to the question: ‘‘How would you rate your
knowledge of: (a) Cultural diversity in medicine; (b) Making mistakes in medicine; (c) End-of-life issues; (d) Vulnerable groups
in medicine; (e) Interaction with the pharmaceutical industry?’’ N¼ 142 pre-course survey responses. N¼ 133 post-course
survey responses.
Table 1. Course evaluation.
Average score Range
Course topics 1.3 1–3
Course director 1.2 1–3
Efficiency 1.5 1–5
Relevance 1.3 1–4
Overall impression 1.3 1–3
Recommendation to other students 1.2 1–3
Results of n¼136 responses. Students were asked to rate their answers on a
scale of 1 to 5, with 1 being the best, 5 being the worst value.
The profession of medicine
e271
Med
Tea
ch D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y Su
ny G
enes
eo o
n 10
/27/
14Fo
r pe
rson
al u
se o
nly.
graduates from seven German medical schools in 2002, the top
three deficits reported were in the areas of practical skills,
physician-patient interaction and psychosocial competency.
The respondents deplored how poorly they felt prepared
for the non-scientific tasks and challenges of a medical practice
(Jungbauer et al. 2004). An earlier paper examining the role
of basic professional competencies in the German medical
education system also describes significant shortcomings
with regard to psychosocial issues, communication skills
and medical ethics (Perleth 1998). These works suggest that
many medical school graduates in Germany feel overwhelmed
and cheated by their education when, as practising profes-
sionals, they face such inevitable issues as death, mistakes,
and cultural diversity among their patients with no formal
preparation in these areas.
One of the explicit purposes of the course ‘‘The Profession
of Medicine’’ is to specifically address some of the topics
underrepresented in the current German medical education
system. Judging from the written and oral feedback to the
course, this goal seems to have been achieved to a consider-
able degree. Suggestions have even been made by the students
to expand the course and to integrate it into other phases of
medical education beyond the preclinical stage, and to make it
a mandatory and regular rather than an elective component of
the curriculum. Since 75% of the enrolees of ‘‘The Profession of
Medicine’’ have been women, a mandatory course would be
particularly useful to ensure the introduction of men to the
more humanistic aspects of medical education.
Among the many topics covered in the ‘‘Patient, Physician
and Society’’ curriculum at Northwestern University’s Feinberg
How would you rate your interest in the subject of:
0
2
4
6
8
10
Cultural Diversity p=0.34
Mistakes p=0.04
End-of-Life p=0.00
Vulnerable Groups p=0.10
Pharm. Industry p=0.02
Sca
lepre, n=142
post, n=133
Figure 2. Result of pre- and post-course surveys assessing students’ interest in the course topics.
Students were asked to rate on a scale of 1 to 10 (0 none, 10¼ the most) to respond to the question: ‘‘How would you rate your
interest in the subject of: (a) Cultural diversity in medicine; (b) Making mistakes in medicine; (c) End-of-life issues; (d) Vulnerable
groups in medicine; (e) Interaction with the pharmaceutical Industry?’’ N¼ 142 pre-course survey responses. N¼ 133 post-course
survey responses.
How would you rate your professional attitude in the area of:
0
2
4
6
8
10
Cultural Diversity p=0.00
Mistakes p=0.01
End-of-Life p=0.00
Vulnerable Groups p=0.03
Pharm. Industry p=0.02
Sca
le pre, n=142
post, n=133
Figure 3. Result of pre- and post-course surveys assessing students’ professional attitude toward the course topics.
Students were asked to rate on a scale of 1 to 10 (0 none, 10¼ the most) to respond to the question: ‘‘How would you rate your
degree of responsibility as a future physician toward patients and society in the context of: (a) Cultural diversity in medicine;
(b) Making mistakes in medicine; (c) End-of-life issues; (d) Vulnerable Groups in Medicine; (e) Interaction with the Pharmaceutical
Industry?’’ N¼ 142 pre-course survey responses. N¼ 133 post-course survey responses.
R. W. Tillmanns et al.
e272
Med
Tea
ch D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y Su
ny G
enes
eo o
n 10
/27/
14Fo
r pe
rson
al u
se o
nly.

School of Medicine, only five could be integrated into this
one-week version at Charite – Universitatsmedizin Berlin.
The five topics were carefully chosen, each encompassing
a certain degree of social and professional taboo. It is
important to lift the silence surrounding these issues.
This is particularly important in face of the fact that today’s
graduating physician faces a very different patient population
than in the past, a more proactive population armed
with internet education, expectations of cultural sensitivity,
and demands for honesty, information, and choices from
their medical practitioners.
Multiple movements from within society have encour-
aged changes within medical education – immigrant
initiatives (Fox 2005), gender equality (Vlasoff & Garcia
Moreno 2002), the hospice and palliative medicine move-
ment (Emanuel et al. 2000), patient safety initiatives
(Wachter et al. 2002), and the evolving standards of medical
ethics (ABIM Foundation et al. 2002), to name a few. The
vitality of these movements is made apparent to our
students by the willingness of guest speakers to offer
presentations during ‘‘The Profession of Medicine’’ about
their various projects, including medical assistance for
undocumented immigrants, women and disability, assistance
for victims of domestic violence, and mental health issues of
immigrants. The topics have also encouraged the students to
question the traditional paternalistic model of patient care in
light of a more patient-centred, egalitarian patient-physician
relationship.
Student surveys both before and after the course generally
rated the ‘‘Mistakes’’ and ‘‘End-of-Life Issues’’ topics as more
interesting and important than ‘‘Cultural Diversity in
Medicine’’, ‘‘Vulnerable Groups’’, and ‘‘Interactions with the
Pharmaceutical Industry’’. Perhaps the former topics,
which deal more directly with personal aspects of the
patient-physician relationship, were more effectively
addressed in these brief sessions than were larger, more
complex social issues. Traditional notions of the physician’s
greater responsibility toward the individual patient than
toward society as a whole may also be at work here.
Contribution to international medical education
Significant developments in medicine have come from
international communication among scientists and clinicians
around the world (The Executive Council, The World
Federation for Medical Education 1998). The accelerating
globalisation of medicine was specifically kept in mind when
the course ‘‘The Profession of Medicine’’ was established,
with the intention of exposing students to transnational
similarities as well as cultural differences in the psychosocial,
cultural and ethical aspects of patient care. The course is
taught in English in order to give students the opportunity to
apply the international language of medicine in speaking and
writing (Maher 1987).
This course project has facilitated the development of an
institutional alliance between Charite – Universitatsmedizin
Berlin and Northwestern University Feinberg School
of Medicine Chicago, with an ongoing student exchange in
clinical medicine and prospects for additional levels of
institutional collaboration. One Northwestern medical student
has also already served as a teaching assistant and small group
preceptor in the course at Charite – Universitatsmedizin Berlin,
in fulfilment of the fourth year curricular requirement
at Northwestern for a supervised experience in teaching.
Contributions to methods in medical education
Teaching methods drawn from experiential education
methods – role play, discussion-based seminar formats, and
reflective writing techniques, for example–have gained wide
acceptance in U.S medical curricula over the last two decades.
In the course ‘‘The Profession of Medicine’’, learning was
primarily achieved by these more active and interactive means,
and our students found them effective. Despite the introduc-
tion of these learning methods in several curriculum reform
projects (Kiessling et al. 2003; Schildmann et al. 2004;
Burger 2006), much of German medical education remains
rooted in more traditional methods. We hope to have
contributed to the acceptance of newer educational principles
and methods through the introduction of this course.
Unresolved issues
For practical reasons, only a very small portion of the ‘‘mother’’
curriculum ‘‘Patient, Physician and Society’’ could be
introduced at Charite – Universitatsmedizin Berlin. Due to
the ironies of course scheduling, it has not yet been possible
to involve students from the Reformstudiengang, or
‘‘Reform Curriculum,’’ a vibrant and progressive component
of the Charite – Universitatsmedizin Berlin educational
programs (Burger 2006). Resolution of these logistical issues
would create new opportunities for further curriculum
development and intra- as well as inter-institutional collabora-
tion. Other logistical barriers will remain, however, not the
least of which is difficulty in providing small group settings
to the large Charite – Universitatsmedizin student body,
which is nearly eight times the size of the student body
at Northwestern.
Some students thought the predominance of reading
materials from English-language medical journals created an
over-emphasis on U.S. perspectives. On the other hand,
with only the occasional American faculty member or student
in attendance, the literature provided some assurance of an
international component to class discussions.
The Charite’s Office of Medical Education requires a scaled
grading system with five grades, the worst grade being
equivalent to failing the course. The authors were not in
favour of this grading method; they would have preferred a
pass-fail grading system, as is the case for the course
at Northwestern, to help keep a population of highly
competitive students focused on the course topics rather
than on concerns and ambitions surrounding their
grades. The students in ‘‘The Profession of Medicine’’ were
consequently graded rather leniently. Although student
evaluations revealed that ‘‘ease of getting a certificate’’ was
rated as of lesser importance (Table 2), the possibility of the
course developing a reputation as an ‘‘easy pass’’ remains
unresolved.
The profession of medicine
e273
Med
Tea
ch D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y Su
ny G
enes
eo o
n 10
/27/
14Fo
r pe
rson
al u
se o
nly.
Future prospects
Despite upcoming changes in course leadership,
‘‘The Profession of Medicine’’ will continue to exist as an
elective at Charite – Universitatsmedizin Berlin, with a new
director and new students involved in the planning and
teaching of the course. The course so far has reached more
than 140 students in two years. It will continue to serve as a
forum for learning about psychosocial, ethical and cultural
issues, it will continue to provide an opportunity for
international exchange among students and faculty, and it
will continue to stimulate students and faculty to develop new
ideas and initiatives in these important, still under-appreciated
aspects of medical education.
Notes on contributors
REGINE WOOD TILLMANNS, MD, FACP, was Instructor of Medicine
at Northwestern University’s Feinberg School of Medicine, Chicago until
October 2006. From 2004–2006, she was an international fellow in medical
education at the Charite – Universitatsmedizin Berlin, Germany. She is now
assistant professor at Texas Tech University Health Sciences Center at
El Paso, Texas, USA.
ANNA RINGWELSKI, MD, graduated from Northwestern University’s
Feinberg School of Medicine, Chicago, USA, in 2006. She is
currently completing a residency training program in Emergency
Medicine at Bellevue Hospital/New York University in New York City,
USA.
JOHANNA KRETSCHMANN, MS, is a clinical psychologist at a
Psychosomatic Clinic in Bernau, Germany. Until recently, she was a faculty
member in the Department of General Medicine at the Charite –
Universitatsmedizin Berlin, involved in program development
and evaluation.
LUITA D. SPANGLER, PhD, received her doctorate in English Literature
at the University of New Hampshire, USA. She currently teaches
English at the Freie Universitat Berlin and the Universitat Potsdam,
Germany.
RAYMOND H. CURRY, MD, FACP, is Professor of Medicine and Medical
Education, and Executive Associate Dean for Education at Northwestern
University Feinberg School of Medicine, Chicago, USA.
Acknowledgements
The authors would like to thank Ulrike Arnold, Director of
Charite International Cooperation at the Charite –
Universitatsmedizin Berlin for her logistical support, Hannah
Haumann, Katja Hess and Magdalena Stepien for their
commitment and their help with the implementation of the
course, and to Joachim Seybold, MD, MBA, for his participa-
tion and continued involvement and leadership.
References
ABIM Foundation. American Board of Internal Medicine; Acp-Asim
Foundation. American College Of Physicians-American Society Of
Internal Medicine; European Federation of Internal Medicine 2002.
Medical professionalism in the new millennium: a physician charter.
Annals Int Med 136:243–246.
Armstrong EG, Fischer MR. 2001. Comparing health care delivery systems –
initiating a student exchange program between Europe and the United
States. Med Educ 35:695–701.
Association of Amercian Medical Colleges. 1984. Physicians for the
twenty-first century. Report of the Project Panel on
the General Professional Education of the Physician and College
Preparation for Medicine. J Med Educ 59, part 2.
Burger W. 2006. Der Reformstudiengang an der Charite. Die Erfahrungen
der ersten 5 Jahre. Bundesgesundheitsblatt-Gesundheitsforschung-
Gesundheitsschutz 49:337–343.
De Vries J, Szabo BG, Sleijfer DT. 2002. The educational yield of
the international summer school ‘‘Oncology for Medical Students’’.
J Cancer Educ 17:115–120.
Emanuel LL, Von Gunten CF, Ferris FD. 2000. Gaps in end-of-life care. Arch
Family Med 9:1176–1180.
Finkel ML, Fein O. 2006. Teaching medical students about different health
care systems: An international exchange program. Acad Med
81:388–390.
Fox RC. 2005. Cultural Competence and the Culture of Medicine. The New
England J Med 353:1316–1319.
Humboldt – Universitat Zu Berlin. 2005. Manneranteil bei
Studierenden, Abschlussprufungen, Promotionen und Habilitationen.
Internet, available from www.studium.hu-berlin.de (accessed 10
October 2006).
Imperato PJ. 2004. A third world international health elective for U.S.
medical students: the 25-year experience of the State University of
New York, Downstate Medical Center. J Commun Health
29:337–373.
Jungbauer J, Kamenik C, Alfermann D, Brahler F. 2004. Wie
bewerten angehende Arzte ruckblickend ihr Medizinstudium?
Ergebnisse einer Absolventenbefragung. Gesundheitswesen
66:51–56.
Kiessling C, Muller T, Becker-Witt C, Begenau J, Prinz V, Schleiermacher S.
2003. A medical humanities special study module on principles of
medical theory and practice at the Charite, Humboldt University, Berlin,
Germany. Acad Med 78:1031–1035.
Maher J. 1987. English as an international language of medicine. Med Educ
21:283–284.
Makoul G, Curry RH. 1998a. The evolution of courses in professional
skills and perspectives for medical students. Academic Med
73:10–13.
Makoul G, Curry RH. 1998b. Patient, Physician & Society: Northwestern
University Medical School. Acad Med 73:14–24.
Margolis CZ, Deckelbaum RJ, Henkin Y, Baram S, Cooper P, Alkan ML.
2004. A medical school for international health run by international
partners. Acad Med 79:744–751.
Montgomery K, Chambers T, Reifler DR. 2003. Humanities education at
Northwestern University’s Feinberg School of Medicine. Acad Med
78:958–962.
Murrhardter Kreis. 1989, 1995. Das Arztbild der Zukunft. Analysen
kunftiger Anforderungen an den Arzt. Konsequenzen fur die
Ausbildung und Wege zu ihrer Reform (Gerlingen, Bleicher).
Pabst R. 1995. Med Educ and Reform Initiatives in Germany. Acad Med
70:1006–1011.
Perleth M. 1998. Arztliche Basiskompetenzen: Vernachlassigtes
Ausbildungsziel im Medizinstudium? Medizinische Klinik 93:381–387.
Schildmann J, Kampmann M, Schwantes U. 2004. Lehrveranstaltungen zu
Themen der Anamnese und Gesprachsfuhrung in Deutschland: Eine
Umfrage unter Studierenden von 12 medizinischen Fakultaten.
Zeitschrift fur arztliche Fortbildung und Qualitat im
Gesundheitswesen 98:287–292.
Schuppel R, Bayer A, Hrabal V, Holzer M, Allert G, Tiedemann G.
1998. Fachubergreifendes Langsschnittcurriculum ‘‘Medizinische
Psychologie, Psychotherapie und Psychosomatik. Psychotherapie,
Psychosomatik und Medizinische Psychologie 48:187–192.
The Executive Council, The World Federation for Med Educ. 1998.
International standards in medical education: assessment and accred-
itation of medical schools’–educational programmes. A WFME position
paper. Med Educ 32:549–558.
Vlasoff C, Garcia Moreno C. 2002. Placing gender at the centre of
health programming: challenges and limitations. Soc Sci Med
54:1713–1723.
R. W. Tillmanns et al.
e274
Med
Tea
ch D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y Su
ny G
enes
eo o
n 10
/27/
14Fo
r pe
rson
al u
se o
nly.

Von Jagow G, Loholter R. 2006. Die neue Arztliche Approbationsordnung.
Bundesgesundheitsblatt-Gesundheitsforschung-Gesundheitsschutz 49:
330–336.
Wachter RM, Shojania KG, Saint S, Markowitz AJ, Smith M. 2002. Learning
from Our Mistakes: Quality Grand Rounds, a New Case-Based Series on
Medical Errors and Patient Safety. Annals Int Med 136:850–852.
Wissenschaftsrat. 1992. Leitlinien zur Reform des Medizinstudiums (Koln,
Wissenschaftsrat).
Wittern-Sterzel R. 2003. ‘‘Die Politik ist weiter nichts, als Medicin im
Grossen’’ – Rudolf Virchow und seine Bedeutung fur die Entwicklung
der Sozialmedizin. Verhandlungen der Deutschen Gesellschaft fur
Pathologie 87:150–157.
The profession of medicine
e275
Med
Tea
ch D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y Su
ny G
enes
eo o
n 10
/27/
14Fo
r pe
rson
al u
se o
nly.