The Problem The Goal The Intervention Progress to Date Next
Steps A hospital-wide, comprehensive approach to recognizing and
responding to delirium is needed to minimize the consequences of
hospital-acquired delirium, and contribute meaningfully to our goal
of eliminating preventable harm. This project aimed to minimize
adverse consequences of hospital-acquired delirium through a
multi-pronged approach that a) identified patients at risk for
delirium; b) prevented delirium in at-risk patients; c) monitored
at-risk patients for development of delirium; and d) provided early
and effective intervention for patients at-risk or who developed
delirium. The GRACE Delirium Precautions pilot: Took an innovative
approach to providing early and effective prevention and
intervention for patients who developed delirium; Utilized the
institutions Precautions culture and associated care plans;
Targeted a multi-disciplinary care bundle over an 8-week period
(March April 2014) on one medical floor in the hospital (CC7). Our
Team Deb Adduci, PT: Manager Inpatient OT/PT May Adra, BS, Pharm D:
Clinical Pharmacy Coordinator Andrea J. Branchaud, MPH: Healthcare
Quality Suzanne Burger, MSN, RN: Unit-Based Educator Katelyn
Campbell, OTR/L: Occupational Therapist Anthony Ishak, PharmD:
Clinical Pharmacist Chris Kristeller, RN: Clinical Nurse Specialist
Tracy Lee, MSN, RN: Nurse Manager Melissa Mattison, MD: Associate
Chief, Hospital Medicine Robin McLaughlin, RN, RRT: Unit-Based
Educator Jaclyn Miller, RN: Resource RN Crystal Sannella, OTR/L:
Occupational Therapist Kim Sulmonte, RN, MHA, CSHA: Associate Chief
Nurse, Quality & Safety Julius Yang, MD, PhD: Director,
Inpatient Quality GRACE Delirium Precautions OTs and RNs using
common language/tools for clinical discussion for patients (How was
pts test of attention?) RNs reporting satisfaction with having
Cognition/Toolkit resources (real-time availability of materials)
MD satisfaction with consultant responses pharmacy especially
Culture built around delirium Team approach to patient care
Non-pilot floor delirium precautions orders being entered: 47 other
hospital-wide orders 27% had ICU stay 41% admitted from Home 76%
discharged to Extended Care Facility 60% aged 81 and older Average
rate for previous 5 years Average rate for previous 5 months
Average rate during pilot 3.735.22 1.97 Targeted Outcomes Establish
reliable prevalence of delirium Decrease falls w/injury Increase
discharge to home Decrease length of stay 59 patients over 8
weeks:Correlational effect on falls: General satisfaction with
pilot: CC7: RN & MD components re-launching February 2015
Hospital-wide: RN & MD components as part of Roadshow
Brainstorming around pharmacy components Brainstorming about
transfer of information to post- discharge facilities/home care:
discharge summary, plan Click on an image below to explore the
components of our intervention!
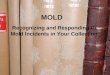
Bin for used items Clean bins to place new items & bring to
pt rooms Suggested Items to use & Comments list Program
Overview & Delirium 1-Point lessons Drawers sorted &
Labeled by: Cognition Sensory Impairments Sleep/Wake, Other Labeled
as: Reusable 1-TIME Use RN Packet: Drawer 3 DP Sign, Fall Sign,
Education Fact Sheet, About Me poster, Markers Light for evening
shift (requested) Cognition Toolcart/Closet