Embed Size (px)
Citation preview

ORIGINAL RELEASE: April 1, 2017
COPE COURSE ID:53202-GL
LAST REVIEW: March 17, 2017
COPE COURSE CATEGORY: GLAUCOMA
EXPIRATION: March 16, 2020
in GlaucomaChallenging CasesManaging
THE PRESSURE’S ON!
CE MONOGRAPH
Sponsored by
This continuing medical education activity is supported through
an unrestricted educational grant from Bausch & Lomb Incorporated.
Visit http://tinyurl.com/ThePressuresOnCOPE for online testing and instant CE certificate.
FACULTY
MURRAY FINGERET, OD
BEN GADDIE, OD
Administrator
Distributed with

2
LEARNING METHOD AND MEDIUMThis educational activity consists of a supplement and ten (10) study questions. The participant should, in order, read the learning objectives contained at the beginning of this supplement, read the supplement, answer all questions in the post test, and complete the Activity Evaluation/Credit Request form. To receive credit for this activity, please follow the instructions below in the section titled To Obtain CE Credit. This educational activity should take a maximum of 1 hour to complete.
CONTENT SOURCEThis continuing education (CE) activity captures content from a regional dinner meeting series.
ACTIVITY DESCRIPTIONDespite the variety of treatments available for glaucoma, some patients continue to have vision-threatening intraocular QSFTTVSF�*01�MFWFMT��/FX�ESVHT �OFX�mYFE�DPNCJOBUJPOT�of existing drugs, and new procedures constantly challenge the traditional treatment paradigm and are showing promise in lowering IOP and slowing disease progression by multiple mechanisms of action. The purpose of this activity is to update optometrists on the current state of the art and science for treating patients with glaucoma.
TARGET AUDIENCEThis educational activity is intended for optometrists.
LEARNING OBJECTIVESUpon completion of this activity, participants will be better able to:t�"TTFTT�USBEJUJPOBM�BOE�FNFSHJOH�SJTL�GBDUPST �TVDI�BT�PDVMBS��� QFSGVTJPO�QSFTTVSF�BOE�DFSFCSPTQJOBM�nVJE�QSFTTVSF �JO�UIF�� global risk assessment of glaucomat�%FTDSJCF�UIF�NFDIBOJTN�PG�BDUJPO�PG�DVSSFOU�BOE�FNFSHJOH�� topical glaucoma therapiest�&WBMVBUF�UIF�DMJOJDBM�SFMFWBODF�PG�TBGFUZ�BOE�FGmDBDZ�EBUB�GPS� emerging topical therapies for the treatment of glaucomat�%FWFMPQ�USFBUNFOU�QMBOT�UP�BDIJFWF�FWJEFODF�CBTFE�UBSHFU�� IOP in patients with glaucoma
ACCREDITATION STATEMENTThis course is COPE approved for 1 hour of CE credit for optometrists.
COPE Course ID 53202-GLCOPE Course Category: GlaucomaAdministrator:
DISCLOSURESMurray Fingeret, OD, IBE�B�mOBODJBM�BHSFFNFOU�PS�BGmMJBUJPO�during the past year with the following commercial interests in the form of Consultant/Advisory Board: Allergan; and Bausch & Lomb Incorporated.
Ben Gaddie, OD, IBE�B�mOBODJBM�BHSFFNFOU�PS�BGmMJBUJPO�EVSJOH�the past year with the following commercial interests in the form of Consultant/Advisory Board: Aerie Pharmaceuticals, Inc;
p
Alcon; Allergan; Bausch & Lomb Incorporated; Diopsys, Inc; Marco; Reichert, Inc; TearLab Corporation; TearScience; and Zeiss.
'DYLG�6��*UHHQÀHOG��0'��IBE�B�mOBODJBM�BHSFFNFOU�PS�BGmMJBUJPO�EVSJOH�UIF�QBTU�ZFBS�XJUI�UIF�GPMMPXJOH�DPNNFSDJBM�interests in the form of Consultant/Advisory Board: Aerie Pharmaceuticals, Inc; Alcon; Allergan; Bausch & Lomb Incorporated; and Quark.
EDITORIAL SUPPORT DISCLOSURES7RQ\�5HDOLQL��0'��03+��IBE�B�mOBODJBM�BHSFFNFOU�PS�BGmMJBUJPO�EVSJOH�UIF�QBTU�ZFBS�XJUI�UIF�GPMMPXJOH�DPNNFSDJBM�interests in the form of Consultant/Advisory Board: Alcon; Bausch & Lomb Incorporated; Inotek Pharmaceuticals Corporation; and Smith & Nephew; Contracted Research: Alcon; and F. Hoffmann-La Roche Ltd.
'LDQH�0F$UGOH��3K'��&\QWKLD�7RUQDOO\D\��5'��0%$��&+&3��.LPEHUO\�&RUELQ��&+&3��%DUEDUD�$XEHO��and 0LFKHOOH�2QJ�have no relevant commercial relationships to disclose.
DISCLOSURE ATTESTATIONThe contributing physicians listed above have attested to the following:�� UIBU�UIF�SFMBUJPOTIJQT�BGmMJBUJPOT�OPUFE�XJMM�OPU�CJBT�PS��� � PUIFSXJTF�JOnVFODF�UIFJS�JOWPMWFNFOU�JO�UIJT�BDUJWJUZ�2) that practice recommendations given relevant to the � � DPNQBOJFT�XJUI�XIPN�UIFZ�IBWF�SFMBUJPOTIJQT�BGmMJBUJPOT�� will be supported by the best available evidence or, absent evidence, will be consistent with generally accepted medical practice; and3) that all reasonable clinical alternatives will be discussed when making practice recommendations.
PRODUCT USAGE IN ACCORDANCE WITH LABELING1MFBTF�SFGFS�UP�UIF�PGmDJBM�QSFTDSJCJOH�JOGPSNBUJPO�GPS�FBDI�drug discussed in this activity for approved indications, contraindications, and warnings.
GRANTOR STATEMENTThis continuing education activity is supported through an unrestricted educational grant from Bausch & Lomb Incorporated.
TO OBTAIN CE CREDIT8F�PGGFS�JOTUBOU�DFSUJmDBUF�QSPDFTTJOH�BOE�TVQQPSU�(SFFO�$&��Please take this post test and evaluation online by going to http://tinyurl.com/ThePressuresOnCOPE. Upon passing, you XJMM�SFDFJWF�ZPVS�DFSUJmDBUF�JNNFEJBUFMZ��:PV�NVTU�BOTXFS���out of 10 questions correctly in order to pass, and may take the test up to 2 times. Upon registering and successfully DPNQMFUJOH�UIF�QPTU�UFTU �ZPVS�DFSUJmDBUF�XJMM�CF�NBEF�BWBJMBCMF�POMJOF�BOE�ZPV�DBO�QSJOU�JU�PS�mMF�JU��1MFBTF�NBLF�TVSF�you take the online post test and evaluation on a device that has printing capabilities. There are no fees for participating in and receiving CE credit for this activity. DISCLAIMERThe views and opinions expressed in this educational activity are those of the faculty and do not necessarily represent UIF�WJFXT�PG�5IF�4UBUF�6OJWFSTJUZ�PG�/FX�:PSL�$PMMFHF�PG�Optometry, MedEdicus LLC, Bausch & Lomb Incorporated, or Optometry Times.
5IJT�$&�BDUJWJUZ�JT�DPQZSJHIUFE�UP�.FE&EJDVT�--$�ª������All rights reserved.

3
in GlaucomaChallenging CasesManaging
THE PRESSURE’S ON! FACULTY
MURRAY FINGERET, ODClinical ProfessorState University of New York College of OptometryNew York, New York
BEN GADDIE, ODOwner and DirectorGaddie Eye CentersLouisville, Kentucky
IntroductionThe science of glaucoma evaluation and management is progressing. New drugs with novel mechanisms of action and promising phase 3 clinical data are poised for US Food and Drug Administration review in the near future. New risk factors to guide clinical decision-making are emerging. In this series of clinical cases, key decisions faced daily in the evaluation and management of patients with suspected or established HMBVDPNB�XJMM�CF�JEFOUJmFE�BOE�EJTDVTTFE�
&DVH����$VVHVVLQJ�WKH�1HHG�IRU�7UHDWPHQW�LQ�2FXODU�+\SHUWHQVLRQFrom the Files of Murray Fingeret, OD
A 36-year-old African American male presents for a comprehensive eye examination complaining of blurred vision. His last eye examination was 2 years ago. His medical and family histories are unremarkable.
On examination, his visual acuity is 20/20 OU, with a -1.00 D spherical correction in each eye. Anterior segment examination is unremarkable. Goldmann tonometry at 9 AM
is 28 mm Hg in the right eye and 29 mm Hg in the left eye. 1BDIZNFUSZ�SFWFBMT�DPSOFBM�UIJDLOFTT�PG�����BOE�����çN�in the right and left eye, respectively. The angles are open on gonioscopy. Figure 1 shows his optic nerves, optical DPIFSFODF�UPNPHSBQIZ�0$5�JNBHJOH �BOE�WJTVBM�mFMET�
4��:KDW�LV�JODXFRPD"(MBVDPNB�JT�B�EJGmDVMU�EJTFBTF�UP�EJBHOPTF �JO�QBSU�CFDBVTF�JU�JT�EJGmDVMU�UP�EFmOF��5IF������FEJUJPO�PG�UIF�"NFSJDBO�Academy of Ophthalmology’s (AAO’s) Preferred Practice 1BUUFSO�GPS�1SJNBSZ�0QFO�"OHMF�(MBVDPNB�10"(�EFmOFT�POAG as “a chronic, progressive optic neuropathy in adults in which there is a characteristic acquired atrophy of the optic nerve and loss of retinal ganglion cells and their axons. This condition is associated with an open anterior chamber angle by gonioscopy.”1
5IJT�EFmOJUJPO�JT�OPUFXPSUIZ�JO�TFWFSBM�XBZT��'JSTU �UIF�EJBHOPTJT�PG�HMBVDPNB�JT�CBTFE�TPMFMZ�PO�DMJOJDBM�mOEJOHT��UIFSF�JT�OP�MBCPSBUPSZ�UFTU�UP�HJWF�B�QPTJUJWF�PS�OFHBUJWF�DPOmSNBUJPO��This means that clinicians must have excellent clinical skills to detect glaucoma, and because it is typically asymptomatic until later stages, it must be looked for in every patient.
4��+RZ�GR�ZH�LGHQWLI\�JODXFRPD�LQ�FOLQLFDO�SUDFWLFH"What should be looked for? What clinical skill is the most important to detect glaucoma? The optic nerve head (ONH) FYBNJOBUJPO��5IF�QBUIPHOPNPOJD�DMJOJDBM�mOEJOH�JO�BMM�GPSNT�of glaucoma is glaucomatous optic neuropathy, a nebulous UFSN�UIBU�JT�QPPSMZ�EFmOFE�BOE�FBTJMZ�DPOGVTFE�XJUI�OPSNBM�anatomic variants of optic nerve appearance. The preceding EFmOJUJPO�JT�PG�MJUUMF�IFMQ�UP�DMJOJDJBOT �IFEging on precisely
Figure 1. Clinical data from the patient presented in Case 1. (A) Color optic nerve QIPUPHSBQIT��#�0QUJDBM�DPIFSFODF�UPNPHSBQIZ�SFTVMUT��$�7JTVBM�mFME�SFTVMUT�
Images courtesy of Murray Fingeret, OD
C
A
B

4
what they should be looking for. Describing glaucoma nerve damage as “characteristic acquired atrophy of the optic nerve”1 is only helpful if clinicians already know what they are looking for and assumes that they will know it when they see it.
4��:KDW�GRHV�D�JODXFRPDWRXV�RSWLF�QHUYH�KHDG�ORRN�OLNH"5IF�DMBTTJD�mOEJOH�JO�HMBVDPNBUPVT�PQUJD�OFVSPQBUIZ�JT�cupping of the ONH. Every ONH has 2 main components: the neuroretinal rim, which is made up of axons from retinal ganglion cells coursing through the scleral canal to form the optic nerve, and the physiologic cup, the leftover space not occupied by the neuroretinal rim. In glaucoma, the axons are lost, the rim becomes thinner, and the cup becomes enlarged over time.
On initial examination, however, whether a given cup is healthy and stable or has enlarged over time because of progressive rim loss cannot be known. Larger cups—above 0.5 or so—are more suggestive of glaucoma damage, but healthy eyes can have normal physiologic cups as large as 0.9. So how can a large cup be determined as glaucomatous or healthy?
One clue is disc size. The size of the ONH is determined by the size of the scleral canal (which is quite variable among eyes), whereas the amount of neuroretinal rim is determined by the number of retinal ganglion cells in the eye (which is fairly consistent among eyes). If the same number of axons pass through a large hole and a small hole, there will be more leftover space in the former and less in the latter. Therefore, larger-diameter ONHs tend to have larger physiologic cups, and smaller-diameter ONHs tend to have smaller physiologic cups. A moderate or large cup in a small ONH is potentially worrisome when evaluating for glaucoma. Physiologic cups tend to be round in shape, with an intact neuroretinal rim 360° around the cup. Also, in a healthy physiologic ONH, the ISNT rule often applies: the neuroretinal rim is thickest Inferiorly, UIFO�4VQFSJPSMZ �UIFO�/BTBMMZ �BOE�mOBMMZ�5FNQPSBMMZ��*G�UIJT�ISNT the case, then the ONH likely ISNT healthy.2
*O�BEEJUJPO�UP�DVQQJOH �UIFSF�BSF�PUIFS�0/)�mOEJOHT�UIBU�suggest the diagnosis of glaucoma. One is focal rim notching. Often, in glaucoma, cupping is not concentric. The superior and inferior poles of the ONH have more axons bunched up than the nasal and temporal sectors of the ONH. These crowded regions tend to get preferentially damaged by glaucoma. As a result, the optic cup appears focally thinned in these regions. Damage to the superior or inferior neuroretinal rim typically appears as a focal notch in the rim. If both the superior and inferior rims are thinned, the cup appears vertically elongated.
Focal notching of the neuroretinal rim frequently produces BOPUIFS�DMBTTJD�HMBVDPNB�TJHO��UIF�OFSWF�mCFS�MBZFS�CVOEMF�defect. These wedge-shaped defects can often be seen radiating from the ONH’s notched sector(s). Clinically, they are best observed under red-free illumination. Other ONH mOEJOHT�TVHHFTUJWF�PG�HMBVDPNB�JODMVEF�EJTD�IFNPSSIBHFT�BOE�peripapillary atrophy of the retinal pigment epithelium (Figure 2).
4��:KDW�UROH�GRHV�RSWLF�QHUYH�KHDG�LPDJLQJ�SOD\�LQ�WKH�GLDJQRVLV�RI�JODXFRPD"Two forms of ONH imaging are of value in glaucoma: stereo disc photography and OCT imaging. Disc photographs capture the clinical appearance of the ONH at a moment in time—usually the baseline assessment at the time of diagnosis—to provide a basis for detecting change over time. Photographs may also provide better detection of
disc hemorrhages compared with the clinical examination.3 OCT imaging is best used to assess the status of the retinal OFSWF�mCFS�MBZFS�3/'-��#PUI�EJGGVTF�BOE�GPDBM�3/'-�MPTT�can be detected by OCT. Further, OCT can be helpful in distinguishing between physiologic and glaucomatous ONH cupping; a fully intact RNFL in an eye with a large round cup is suggestive of physiologic cupping. Both photography and OCT can assist in detecting progression over time. Serial ONH photographs must be manually compared, whereas serial OCT images can be automatically compared to detect changes over time.
Neither form of ONH imaging can or should replace a thorough clinical examination of the optic nerve. Universal OCT screening for glaucoma is inappropriate and will result in high rates of false-positive tests (so-called “red disease”), which generate unnecessary anxiety for patients BOE�TJHOJmDBOU�DPTUT�UP�UIF�IFBMUI�DBSF�TZTUFN�GPS�GPMMPX�VQ�DPOmSNBUPSZ�UFTUT�UIBU�XJMM�VMUJNBUFMZ�SVMF�PVU�HMBVDPNB��0$5�imaging should be obtained only if the clinical examination suggests glaucoma.
4��:KDW�UROH�GRHV�SHULPHWU\�SOD\�LQ�WKH�GLDJQRVLV�RI�JODXFRPD"Glaucoma occurs in a continuum that begins with early axon loss that cannot be detected using current examination or testing techniques (Figure 3).4 Early glaucomatous ONH EBNBHF�JT�UZQJDBMMZ�JOTVGmDJFOU�UP�DBVTF�B�NFBTVSBCMF�WJTVBM�mFME�EFGFDU�VTJOH�TUBOEBSE�BDISPNBUJD�BVUPNBUFE�QFSJNFUSZ��"DDPSEJOHMZ �WJTVBM�mFME�MPTT�JT�OPU�OFDFTTBSZ�UP�NBLF�UIF�EJBHOPTJT�PG�HMBVDPNB��5IJT�JT�SFnFDUFE�JO�UIF�QSFDFEJOH�""0�EFmOJUJPO�PG�HMBVDPNB �XIJDI�NBLFT�OP�NFOUJPO�PG�WJTVBM�mFME�MPTT�BT�B�GFBUVSF�PG�UIF�EJTFBTF��1FSJNFUSZ�JT�VTFGVM�JO�EJBHOPTJOH�BOE�TUBHJOH�HMBVDPNB��&BSMZ�WJTVBM�mFME�EFGFDUT�generally appear with moderate ONH damage. The greater
Figure 2. Typical features of glaucomatous optic neuropathy. (A) Concentric enlargement of the cup resulting from diffuse axon loss. Note that this is easily confused with normal physiologic cupping. (B) Focal neuroretinal rim notching. (C) A nerve mCFS�MBZFS�CVOEMF�EFGFDU�BTTPDJBUFE�XJUI�a focal neuroretinal rim notch. (D) A disc hemorrhage. (E) Peripapillary atrophy of the retinal pigment epithelium.
Images courtesy of Murray Fingeret, OD
A B
C D
E

5
4��6KRXOG�WKLV�SDWLHQW�EH�WUHDWHG�RU�QRW"5IFSF�BSF�CFOFmUT�UP�USFBUJOH�UIJT�QBUJFOU��*G�UIF�QBUJFOU�IBT�early POAG, treatment will reduce the risk of progression.� If the patient has ocular hypertension, treatment will reduce the risk of developing POAG.8 There are also detriments to treating this patient. This patient may not have, and may never develop, POAG; thus, treatment may be unnecessary. All interventions to lower IOP, such as medications or laser or incisional surgery, have potential side effects, costs, and a negative effect on quality of life. Subjecting patients to risks XJUIPVU�CFOFmUT�TIPVME�CF�BWPJEFE�XIFOFWFS�QPTTJCMF�
With these considerations in mind, how can patients most MJLFMZ�UP�CFOFmU�GSPN�*01�MPXFSJOH�UIFSBQZ�CF�JEFOUJmFE �#Z�identifying those at highest risk of developing visual disability from glaucoma and treating those patients preferentially. Global risk assessment in glaucoma can help identify high-risk patients. This process involves comprehensive assessment of all known and suspected risk factors for glaucoma, then synthesizing the results into an overall risk impression. Some risk factors are well established, including age, IOP, central corneal thickness, and a family history of glaucoma.1,9,10 Others are less clear, such as myopia,11 diabetes,12 and abnormalities on specialty perimeters like frequency-doubling technology13 or short-wavelength automated perimetry.14 4UJMM�PUIFST�BSF�POMZ�OPX�FNFSHJOH �BOE�UIFSF�BSF�JOTVGmDJFOU�data to fully understand their effect on glaucoma risk. These include corneal hysteresis,15 ocular perfusion pressure (OPP),16 DFSFCSPTQJOBM�nVJE�QSFTTVSF �� and obstructive sleep apnea.18
Several of these risk factors have been incorporated into a validated risk calculator developed from data collected in a pair of major clinical trials: the Ocular Hypertension Treatment Study9 and the European Glaucoma Prevention Study.19 The calculator considers the most well-established risk factors, weighs them accordingly, and generates the probability of QSPHSFTTJOH�UP�10"(�XJUI�SFQSPEVDJCMF�WJTVBM�mFME�MPTT�XJUIJO�5 years.20 This tool is available without charge online at http://ohts.wustl.edu/risk/calculator.html. Expert consensus supports the following treatment guidelines based on risk level: if the risk is below 5%, observation is prudent; for a risk between 5% and 15%, the decision to treat or observe should follow an informed discussion with the patient; and for a risk in excess of 15%, treatment should be encouraged.4
Applying the risk calculator to the patient in Case 1 reveals an 18.5% probability that the patient will develop POAG within the next 5 years �7DEOH���� On this basis, treatment was recommended and the patient agreed.
UIF�mFME�MPTT �UIF�NPSF�BEWBODFE�UIF�HMBVDPNB��1FSJNFUSZ�is also useful in detecting progression of glaucoma over UJNF��4JNQMF�NBOVBM�SFWJFX�PG�TFSJBM�mFMET�PWFS�UJNF�XJMM�PGUFO�demonstrate progression. Modern perimeters also feature advanced progression analysis software that can identify subtle changes over time and assist in differentiating between HMBVDPNBUPVT�QSPHSFTTJPO�BOE�mFME�MPTT�BUUSJCVUBCMF�UP�PUIFS�causes, such as cataract progression.
As with ONH imaging, using perimetry to screen for glaucoma is inappropriate and ineffective. Perimetry is a subjective test and prone to false-positive results based on patient performance FSSPST �FTQFDJBMMZ�PO�mSTU�BUUFNQUT��1FSJNFUSZ�TIPVME�CF�PCUBJOFE�only if the clinical evaluation suggests its value.
4��:KDW�UROH�GRHV�LQWUDRFXODU�SUHVVXUH�SOD\�LQ�WKH�GLDJQRVLV�RI�JODXFRPD"5IF�""0�EFmOJUJPO�PG�HMBVDPNB�OPUFE�QSFWJPVTMZ�NBLFT�no mention of intraocular pressure (IOP) as a feature of the disease. Many patients with POAG do not have elevated IOP,5 and others may have elevated IOP only part of the time. Therefore, a normal IOP in no way rules out the presence of glaucoma. Conversely, the presence of elevated IOP does OPU�NFBO�UIBU�UIF�QBUJFOU�IBT�HMBVDPNB��6Q�UP����PG�IFBMUIZ�adults have IOP greater than 21 mm Hg and no glaucoma.5 However, population studies have demonstrated that the likelihood of glaucoma does increase with increasing IOP.5,6
The relevance of IOP to glaucoma is that IOP reduction is the only established method of reducing the risk of glaucoma progression over time. Regardless of the absolute level of IOP at the time of diagnosis, therapy should be instituted to achieve adequate IOP reduction to slow or halt the rate of progression over time.
4��'RHV�WKLV�SDWLHQW�KDYH�JODXFRPD"The patient described in Case 1 has elevated IOP, healthy-appearing optic nerves, normal OCT imaging of the RNFL, BOE�BO�BCOPSNBM�WJTVBM�mFME�JO�UIF�SJHIU�FZF��)PXFWFS �UIJT�XBT�UIF�QBUJFOU�T�mSTU�WJTVBM�mFME �BOE�UIFSF�JT�B�MFBSOJOH�DVSWF�GPS�DPSSFDUMZ�QFSGPSNJOH�QFSJNFUSZ��8IFO�UIF�WJTVBM�mFME�XBT�repeated, the results were normal in both eyes.
In this case, the differential diagnosis includes both ocular IZQFSUFOTJPO�BOE�FBSMZ�10"( �XJUI�JOTVGmDJFOU�EBNBHF�GPS�detection using standard methods (examination, perimetry, and OCT). At present, there is no easy way to differentiate between these 2 entities other than longitudinal follow-up; POAG will progress over time,� whereas ocular hypertension will not.8
Figure 3. Glaucoma continuum covering the spectrum from early, undetectable disease to advanced disease with visual dysfunction4
"CCSFWJBUJPO��7' �WJTVBM�mFME��
Reprinted from American Journal of Ophthalmology, 138, Weinreb RN, Friedman DS, Fechtner RD, et al, Risk assessment in the management of patients with PDVMBS�IZQFSUFOTJPO �������� �$PQZSJHIU����� �XJUI�QFSNJTTJPO�GSPN�&MTFWJFS�
UN
DET
ECTA
BLE
DISE
ASE
ASYMPTOMATIC DISEASE
FUNCTIONAL IMPA
IRM
EN
T
FACTORS
Age 36RIGHT EYE
MEASUREMENTSLEFT EYE
MEASUREMENTS
1st 2nd 3rd 1st 2nd 3rd
Untreated Intraocular Pressure(mm Hg)
28 27 28 29 30 28
Central Corneal Thickness�ѥP�
520 522 516 510 505 505
Vertical Cup to Disc Ratio by Contour 0.45 0.45
Pattern Standard DeviationHumphrey Octopus loss variance
(dB) (dB)
1.7 1.6 1.4 1.4
This risk assessment tool is available for use free of charge at http://ohts.wustl.edu/risk/calculator.html.
Reprinted with permission.
7KH�SDWLHQW·V�HVWLPDWHG���\HDU�ULVN�����of developing glaucoma in at least 1 eye
�����
7DEOH����Global Risk Assessment of the Patient Presented in Case 1

6
&DVH����,QLWLDO�7KHUDS\�IRU�1HZO\�'LDJQRVHG�3ULPDU\�2SHQ�$QJOH�*ODXFRPDFrom the Files of Murray Fingeret, OD
A 68-year-old Hispanic male with diabetes mellitus presents for an eye examination to screen for diabetic eye disease. He has no personal history of any eye problems. His family history includes a brother with open-angle glaucoma. His medical history is TJHOJmDBOU�GPS�UZQF���EJBCFUFT�NFMMJUVT�EJBHOPTFE����ZFBST�BHP �which is well controlled with oral metformin; his recent HbA1c was 5.8%. He also has hyperlipidemia, which is controlled with simvastatin, and systemic hypertension, which is controlled with atenolol and hydrochlorothiazide.
On examination, his visual acuity is 20/20 in each eye, with a small IZQFSPQJD�DPSSFDUJPO��*OUSBPDVMBS�QSFTTVSF�JT����BOE����NN�)H in the right and left eye, respectively, measured at 9 AM with (PMENBOO�UPOPNFUSZ��$FOUSBM�DPSOFBM�UIJDLOFTT�JT�����BOE�����çN in the right and left eye, respectively. Gonioscopy revealed angles open to the ciliary body band in both eyes. Figure 4 TIPXT�IJT�PQUJD�OFSWFT �3/'- �0$5 �BOE�WJTVBM�mFMET�
4��:KDW�LV�WKH�GLDJQRVLV"Careful inspection of the optic nerve photographs (Figure 4A) reveals thinning of the inferior neuroretinal rim in the right eye, with an associated RNFL bundle defect. A similar inferior RNFL bundle defect can be seen in the left eye. OCT imaging of the 3/'-�DPOmSNT�UIJOOJOH�JOGFSPUFNQPSBMMZ�JO�CPUI�FZFT (Figure 4B). 5IF�WJTVBM�mFME�JO�UIF�SJHIU�FZF�IBT�B�DPSSFTQPOEJOH�TVQFSJPS�BSDVBUF�EFGFDU �XIFSFBT�UIF�MFGU�WJTVBM�mFME�SFNBJOT�FTTFOUJBMMZ�full. Thus, this patient has functional loss in the right eye that correlates with the structural damage evident both clinically and on OCT imaging. In the left eye, however, there is no FWJEFOU�WJTVBM�mFME�MPTT�PO�TUBOEBSE�BVUPNBUFE�QFSJNFUSZ��0O�the basis of these observations, the patient has POAG.
Intraocular pressure values for this patient are within the normal SBOHF��)JTUPSJDBMMZ �UIF�DMBTTJD�mOEJOHT�PG�*01�JO�BO�FZF�XJUI�normal IOP would be considered normal-tension glaucoma (NTG). It is unclear, however, whether NTG is a distinct entity from POAG or simply a subset of POAG. Given that there is no QBUIPHOPNPOJD�mOEJOH�PUIFS�UIBO�*01�UIBU�EJTUJOHVJTIFT�/5(�from POAG, it is likely that they are the same disease and that POAG exists across the full spectrum of IOP.
This patient has been examined only once. Intraocular pressure is a dynamic biologic parameter and exhibits TJHOJmDBOU�WBSJBUJPO�UISPVHIPVU�UIF�EBZ�BOE�GSPN�EBZ�UP�EBZ�JO�both healthy and glaucomatous eyes.21,22 Unless the clinical setting necessitates urgent IOP reduction, there is value in delaying the initiation of therapy to more fully characterize IOP through multiple assessments. After initiating therapy, multiple on-therapy measurements may be necessary to fully characterize the therapeutic response to treatment.23
The patient was asked to return in 2 weeks for a repeat IOP assessment before starting therapy. At that visit, IOP was ���NN�)H�06�BU���PM. The diagnosis of POAG with normal IOP was made. A target IOP of 13 mm Hg (25% reduction) was established.
4��:KDW�LV�WKH�EHVW�ÀUVW�OLQH�WKHUDS\�IRU�WKLV�SDWLHQW"The choice of therapy should consider treatment goals. The AAO Preferred Practice Pattern for POAG recommends an initial 25% IOP reduction for patients with early-to-moderate POAG, citing numerous lines of evidence that this degree of IOP lowering can slow the progression of disease.1 Other considerations when selecting therapy include safety, tolerability, convenience of dosing, and cost.
Prostaglandin analogues optimally provide the desired GFBUVSFT�PG�B�mSTU�MJOF�JOUFSWFOUJPO��5PQJDBM�CFUB�CMPDLFST�represent an alternative medical option. Of note, topical CFUB�CMPDLFST�IBWF�SFEVDFE�FGmDBDZ�JO�TVCKFDUT�PO�TZTUFNJD�beta-blockers (such as this patient), presumably because of a partial therapeutic effect from systemic administration.24 Selective laser trabeculoplasty (SLT) is an effective and safe alternative to daily medical therapy25 that minimizes issues related to side effects, daily dosing, and cost. In a retrospective analysis, SLT was shown to effectively reduce IOP and eliminate medication use in patients with ocular hypertension.26 Surgical interventions are very effective for
Figure 4. Clinical data from the patient presented in Case 2. (A) Right and left PQUJD�OFSWF�QIPUPHSBQIT��HSFFO�BSSPXT�JOEJDBUF�SFUJOBM�OFSWF�mCFS�MBZFS�CVOEMF�EFGFDUT��#�0QUJDBM�DPIFSFODF�UPNPHSBQIZ�JNBHFT�PG�UIF�SFUJOBM�OFSWF�mCFS�MBZFS��$�7JTVBM�mFMET�
Images courtesy of Murray Fingeret, OD
A
B
C
SS 24-2 SS 24-2

7
instillation. Conjunctival or ocular hyperemia rates were similar CFUXFFO�-#/����BOE�MBUBOPQSPTU�������"�QBJS�PG�QIBTF���trials—APOLLO and LUNAR—compared the IOP reduction of LBN, 0.024%, with that of timolol, 0.5%, twice daily. In the APOLLO trial, LBN was superior to timolol, providing a TJHOJmDBOUMZ�MPXFS�*01�BU�BMM���UJNF�QPJOUT���AM, 12 PM, and 4 PM at weeks 2, 6, and 12).33 In the LUNAR trial, LBN was found to CF�OPOJOGFSJPS�UP�UJNPMPM �MPXFSJOH�*01�TJHOJmDBOUMZ�NPSF�UIBO�did timolol at 8 of the 9 time points.34 Across the 2 studies, NFBO�*01�SFEVDUJPO�SBOHFE�GSPN�����UP�����NN�)H with LBN and from 6.6 to 8.0 mm Hg with timolol. In a more recent study in Japanese subjects, LBN was shown to lower IOP by an average of 22% in eyes with low baseline IOP (mean, 19.6 ± 2.9 mm Hg before treatment).35 In an open-label extension study, LBN lowered IOP by 32% to 34%, and the mean diurnal decrease in IOP was 6.3% to 8.3% (Figure 5).36 LBN has also been shown to effectively lower IOP throughout the full 24-hour period, including at night.�� Other NO-donating molecules are in earlier stages of development, including formulations of bimatoprost38 as well as dorzolamide and brinzolamide.39
Another product in late-stage development is netarsudil mesylate, a drug that inhibits both rho-kinase and norepinephrine transporter. Inhibition of the enzyme SIP�LJOBTF�SFTVMUT�JO�CPUI�JODSFBTFE�USBCFDVMBS�PVUnPX�and reduced episcleral venous pressure.40 Inhibition of norepinephrine transporter increases adrenergic activity, which in turn reduces the rate of aqueous production. All 3 of these actions contribute to IOP reduction. Phase 3 studies of netarsudil mesylate have produced mixed results and remain unpublished to date.41 Netarsudil is currently undergoing FWBMVBUJPO�BT�B�mYFE�DPNCJOBUJPO�XJUI�MBUBOPQSPTU�42 In a QIBTF��C�TUVEZ �UIF�DPNCJOBUJPO�TJHOJmDBOUMZ�MPXFSFE�*01�compared with latanoprost or netarsudil alone (P < .0001). Hyperemia, reported as mild in severity, occurred in 40% of patients treated with netarsudil alone or in combination with latanoprost �7DEOH�����
Also in phase 3 evaluation is trabodenoson, an adenosine SFDFQUPS�BHPOJTU�XJUI�IJHI�BGmOJUZ�BOE�TQFDJmDJUZ�GPS�UIF�adenosine A1 receptor. When activated, the A1 receptor lowers IOP in nonhuman primates, in part by regulating the composition of the extracellular matrix of the trabecular meshwork, resulting in increasFE�BRVFPVT�PVUnPX�43,44
achieving low IO1 �CVU�IBWF�B�MFTT�GBWPSBCMF�TBGFUZ�QSPmMF�BOE�BSF�OPU�UZQJDBMMZ�DPOTJEFSFE�GPS�mSTU�MJOF�UIFSBQZ�JO�FBSMZ�PS�moderate glaucoma.
In the current case, generic latanoprost was prescribed for dosing at bedtime OU. One month later, the patient returned with an IOP of 15 mm Hg OU. Intraocular pressure was rechecked 2 weeks later and was 16 mm Hg OU. The patient has suboptimally responded to prostaglandin analogue therapy.
4��:KDW�LV�WKH�QH[W�EHVW�WKHUDSHXWLF�VWHS"Should an additional medication be added to achieve a target IOP of 13 mm Hg? The decision to switch or add should be NBEF�PO�UIF�CBTJT�PG�FGmDBDZ�BOE�TBGFUZ��*G�UIF�UIFSBQZ�XBT�ineffective or poorly tolerated, it should be discontinued and alternative therapy should be implemented. If therapy was well tolerated and provided IOP reduction consistent with its known FGmDBDZ�QSPmMF �JU�TIPVME�CF�DPOUJOVFE�BOE�BEKVODUJWF�UIFSBQZ�should be added.
For patients who cannot tolerate or do not respond to a prostaglandin analogue, alternative therapies must be considered. Prostaglandin analogues have set the bar high BT�UIF�HPME�TUBOEBSE�mSTU�MJOF�UIFSBQZ�GPS�HMBVDPNB �PGGFSJOH�VOSJWBMFE�FGmDBDZ�BOE�TBGFUZ�XJUI�DPOWFOJFOU�PODF�EBJMZ�dosing. Topical beta-blockers can also be dosed once daily and can produce IOP reductions comparable to those of prostaglandin analogues,�� but with more contraindications, including bradycardia, heart block, and pulmonary disease.28
Also, as discussed previously, beta-blockers provide reduced FGmDBDZ�JO�QBUJFOUT�VTJOH�TZTUFNJD�CFUB�CMPDLFST 24 such as this patient. SLT is also a reasonable option. Numerous studies have demonstrated that SLT provides IOP reduction comparable to that seen with prostaglandin analogue therapy.25,29 SLT has the added advantage of eliminating the need for daily adherence with medical therapy and has been shown to be more cost-effective than medications in a model of glaucoma.30
4��:KDW�QRYHO�GUXJV�DUH�LQ�WKH�GHYHORSPHQW�SLSHOLQH"5IJT�DBTF�EFNPOTUSBUFT�B�TJHOJmDBOU�VONFU�OFFE�GPS�NFEJDBM�UIFSBQJFT�UIBU�QSPWJEF�FRVJWBMFOU�PS�TVQFSJPS�FGmDBDZ �TBGFUZ �and dosing convenience compared with prostaglandin analogues for patients who have contraindications to, cannot UPMFSBUF �PS�FYIJCJU�TVCPQUJNBM�FGmDBDZ�XJUI�QSPTUBHMBOEJO�analogues. Several promising drugs are in late-stage development and are expected to garner approval for use in the United States in the near future.
Among these is latanoprostene bunod (LBN), a nitric oxide (NO)-donating form of the latanoprost molecule. Nitric oxide plays key roles in both health and disease throughout the body, including the eye. The molecule relaxes smooth muscle, thus promoting vasodilation. Disease states in which NO is a therapeutic target include angina pectoris, pulmonary hypertension, erectile dysfunction, and, more recently, glaucoma. In the trabecular meshwork, NO activates the cyclic guanosine monophosphate signaling pathway, resulting JO�USBCFDVMBS�SFMBYBUJPO�BOE�JODSFBTFE�USBCFDVMBS�PVUnPX�31 Coupled with latanoprost’s effect on increasing uveoscleral PVUnPX �-#/�XPVME�CF�FYQFDUFE�UP�QSPWJEF�HSFBUFS�*01�SFEVDUJPO�UIBO�MBUBOPQSPTU�BMPOF��*O�UIF�QIBTF���70:"(&3�trial comparing LBN in various doses with latanoprost in 413 subjects, LBN, 0.024%, once daily lowered IOP 1 to 1.5 mm Hg more than did latanoprost, 0.005%, once daily.32 The most common adverse event associated with LBN was pain upon
Figure 5. APOLLO/LUNAR open-label extension study.36 Follow-up times for APOLLO and LUNAR were 9 and 3 months, respectively.
$32//2�/81$5��/RQJ�WHUP�(IÀFDF\�DQG�6DIHW\�2SHQ�ODEHO�([WHQVLRQ�6WXG\
&RPELQHG�QXPEHU�RI�VXEMHFWV�����
&URVVRYHU�IURP�WLPRORO�WR�/%1�DOORZHG
���$GGLWLRQDO�decrease in mean diurnal IOP: 6.3%-8.3%
0HDQ�UHGXFWLRQ�LQ�,23�IRU�DOO�VXEMHFWV����������(P��������IURP�EDVHOLQH�
$GYHUVH�HYHQWV�ZHUH�SULPDULO\�PLOG�WR�PRGHUDWH��!�������
���&RQMXFWLYDO�K\SHUHPLD��������(\H�LUULWDWLRQ���������(\H�SDLQ������
,QWUDRFXODU�3UHVVXUH/DWDQRSURVW 1HWDUVXGLO������� )L[HG�&RPELQDWLRQ
1� �����WRWDO
Baseline, mm Hg 26.0 25.4 25.1
Final, mm Hg 18.4 19.1 16.5
Reduction, mm Hg 7.6 6.3 8.6
* P < .0001 compared with both latanoprost alone or netarsudil alone
7DEOH����1IBTF��C�4UVEZ�PG�'JYFE�$PNCJOBUJPO�/FUBSTVEJM�-BUBOPQSPTU��&GmDBDZ42

8
A topical ophthalmic formulation of trabodenoson is in clinical development for the reduction of elevated IOP in patients with ocular hypertension or POAG. In a dose-ranging phase 1/2 study, IOP reductions with the highest tested dose ranged from -4 to -7 mm Hg.45 In this study, the prevalence of conjunctival hyperemia did not increase from pretreatment baseline in any dose group. Phase 3 clinical development is under way.
Several novel delivery systems for existing glaucoma drugs are also in development. Among these are a punctal plug46 and an intraocular implant47 delivering travoprost, as well as an intraocular implant48 and a conjunctival ring49 delivering bimatoprost. Several of these products are in late-stage development, and the role of these products in current management practice patterns has yet to be established.
Case 3. Glaucoma Progression Despite Low Intraocular Pressure)URP�WKH�)LOHV�RI�'DYLG�6��*UHHQÀHOG��0'
A 70-year-old white female with a 20-year history of POAG presents for a scheduled follow-up visit. She has advanced 10"(�BOE�MPTU�mYBUJPO�JO�IFS�SJHIU�FZF����ZFBST�BHP��)FS�current treatment regimen includes latanoprost OU at bedtime and dorzolamide OU twice daily. She reports excellent adherence to therapy. Her medical history is remarkable for migraine headache, hyperlipidemia controlled with simvastatin, and hypertension controlled with atenolol.
0O�FYBNJOBUJPO �IFS�WJTVBM�BDVJUZ�JT�DPVOUJOH�mOHFST�JO�UIF�right eye and 20/40 in the left eye (due to moderate cataract). Her IOP is 13 mm Hg in the right eye and 14 mm Hg in the left eye. Of note, her pretreatment IOP level was 24 mm Hg in the right eye and 32 mm Hg in the left eye, and her IOP on therapy has never been above 15 mm Hg in the past 10 years. Her central corneal thickness in the right and left FZF�JT�����BOE�����çN �SFTQFDUJWFMZ��)FS�BOHMFT�BSF�PQFO�PO�gonioscopy. Figure 6 shows the left optic nerve photograph, 0$5 �BOE�WJTVBM�mFME�SFTVMUT�UIBU�EFNPOTUSBUF�QSPHSFTTJPO�
Q: Why is this patient progressing with intraocular pressure in the low teens?When confronted with any patient with glaucoma whose EJTFBTF�JT�QSPHSFTTJOH �UIF�mSTU�RVFTUJPO�JT�XIFUIFS�*01�IBT�CFFO�BEFRVBUFMZ�MPXFSFE�GSPN�VOUSFBUFE�CBTFMJOF��*O�UIJT�case, the patient’s left eye IOP has been consistently reduced from 32 to 14 mm Hg, a 56% reduction. This magnitude of IOP reduction would be expected to halt, or at least dramatically slow, glaucoma progression. This is not the case, so alternative explanations must be considered.
An important consideration is whether the patient is adherent to therapy. Some patients use their medications only in the EBZT�QSFDFEJOH�PGmDF�WJTJUT �XIJDI�QSFTFOUT�B�NJTMFBEJOH�BQQFBSBODF�PG�BEFRVBUF�*01�DPOUSPM�UP�UIF�QIZTJDJBO��5IF�reasons for this behavior are poorly understood and likely complex. Such patients are probably unlikely to admit to such behavior, and physicians are generally unable to identify the patients who are most likely to be nonadherent.50 This patient consistently reports excellent adherence to therapy, but such CFIBWJPS�JT�EJGmDVMU�UP�WFSJGZ�PCKFDUJWFMZ�
Central corneal thickness can contribute to artifact in the NFBTVSFNFOU�PG�*01�CZ�BQQMBOBUJPO�UPOPNFUSZ��4QFDJmDBMMZ �UIJO�DPSOFBT�XIJDI�UFOE�UP�CF�nBUUFS�BOE�MFTT�SJHJE�applanate with less force than thicker corneas and can lead to VOEFSFTUJNBUJPO�PG�USVF�*01��5IJT�QBUJFOU�T�DPSOFBT�BSF�RVJUF�
UIJO�MFTT�UIBO�����çN�XIJDI�JT�MJLFMZ�BTTPDJBUFE�XJUI�B�DMJOJDBMMZ�relevant underestimation of IOP. Although the ocular hypotensive SFTQPOTF�UP�UIFSBQZ�BQQFBST�UP�CF�BEFRVBUF �IFS�USVF�BCTPMVUF�
Figure 6. Clinical data from the patient presented in Case 3. (A) Color optic nerve photograph. (B) Optical coherence tomography data showing a decline JO�SFUJOBM�OFSWF�mCFS�MBZFS�UIJDLOFTT�PWFS�UJNF��$�7JTVBM�mFME�EBUB�TIPXJOH�QSPHSFTTJPO�PG�WJTVBM�mFME�MPTT�PWFS�UJNF�
*NBHFT�DPVSUFTZ�PG�%BWJE�4��(SFFOmFME �.%
C
A
B

9
IOP level may be considerably higher than the 14 mm Hg value measured with Goldmann tonometry, and a lower target IOP may be appropriate in light of her recent progression.
This patient’s IOP has consistently been 15 mm Hg or lower XIFO�NFBTVSFE�EVSJOH�SPVUJOF�PGmDF�IPVST �ZFU�*01�UFOET�UP�peak at night when lying down asleep. This is because IOP is higher in the supine position than in the sitting position and also because IOP tends to rise at night as part of its own circadian rhythm.51
4��+RZ�FDQ�LQWUDRFXODU�SUHVVXUH�EH�DVVHVVHG�RXWVLGH�RIÀFH�KRXUV"Routine clinical assessment of 24-hour IOP is impractical because of a lack of safe, affordable, and user-friendly home tonometry devices. Recently, the US Food and Drug "ENJOJTUSBUJPO�BQQSPWFE�UIF�5SJHHFSmTI�DPOUBDU�MFOToCBTFE�24-hour IOP monitor. This device is worn like a regular contact lens and contains a strain gauge that detects changes in corneal curvature that are attributable to changes in IOP. This information is transmitted wirelessly to a receiver worn around the periocular region and is stored on a small data drive connected to the receiver by a wire. The device can record and store up to 24 hours of continuous IOP data. The contact lens has been shown to be well tolerated through 24 hours,52 but data—reported in mV and not mm Hg—are limited to relative changes in IOP curve shape and not to absolute IOP values over time. Optimal use of this device, including both patient selection and data interpretation, has not been described to date.
4��&RXOG�WKH�SDWLHQW·V�V\VWHPLF�K\SHUWHQVLRQ�EH�UHODWHG�WR�KHU�JODXFRPD�SURJUHVVLRQ"Systemic blood pressure tends to dip at night.53 This can be QBSUJDVMBSMZ�TJHOJmDBOU�JO�QBUJFOUT�XIP�UBLF�CMPPE�QSFTTVSF�medications, especially those who dose their antihypertensive therapy in the evening before bed. The nocturnal concurrence of high IOP and low systemic blood pressure may result in a TJHOJmDBOU�SFEVDUJPO�JO�011��011�JT�UIF�EJGGFSFODF�CFUXFFO�systemic blood pressure and IOP and represents the relative pressure of blood perfusing the eye. Numerous epidemiologic studies have demonstrated a higher prevalence of POAG in subjects with low OPP vs normal or high OPP.54-58 A role for OPP in the development of POAG is biologically plausible because low OPP indicates reduced perfusion of ocular tissues, which may contribute to hypoxia/ischemia of optic nerve tissue. Importantly, IOP is typically highest at night when systemic blood pressure is typically lowest, resulting in low OPP.53
4��,V�DQ\�DGGLWLRQDO�ZRUN�XS�DSSURSULDWH�IRU�WKLV�SDWLHQW"This patient is progressing despite a 50% reduction in baseline IOP to the low teens. An additional diagnostic evaluation might be warranted. Ambulatory 24-hour blood pressure monitoring may reveal nocturnal dips. Nocturnal blood pressure dips might be mitigated by reducing the dose of systemic antihypertensive medication, using morning dosing rather than evening dosing, or having the patient ingest salty snacks (such as tomato juice or potato chips) before bed to raise blood pressure. There are no data from epidemiologic studies or trials to support salt loading in this TFUUJOH��-JLFXJTF ����IPVS�*01�NPOJUPSJOH�VTJOH�UIF�5SJHHFSmTI�TZTUFN�NBZ�SFWFBM�TJHOJmDBOU�*01�FMFWBUJPOT�JO�UIF�OJHIUUJNF�hours. Nocturnal IOP peaks may be reduced by sleeping with an extra pillow or 2 to elevate the head.59,60 Coupling 24-hour IOP and blood pressure monitoring can provide insight into circadian OPP and might reveal nocturnal dips in
OP1��011�JT�QPUFOUJBMMZ�NPEJmBCMF �NPTU�FBTJMZ�CZ�BEKVTUJOH�antihypertensive medications to avoid periods of hypotension.
A simpler approach to 24-hour blood pressure assessment JT�UP�PCUBJO�CMPPE�QSFTTVSF�NFBTVSFNFOUT�EVSJOH�PGmDF�based glaucoma visits. Routine daytime blood pressure measurements in all patients is expensive, cumbersome, and may be of limited value. Selecting patients at high risk for progression (eg, patients who report a history of low blood pressure or eyes with optic disc hemorrhage) may provide a snapshot and reveal systemic hypotension, which may CF�NPSF�QSPOPVODFE�BU�OJHIU��5IFTF�QBUJFOUT�NBZ�CFOFmU�most from adjustment of the dose or time of administration of antihypertensive therapy by the primary care physician.
An additional consideration is the possibility that her optic nerve damage is unrelated to her glaucoma. Central nervous system lesions can mimic glaucoma and should be considered when the clinical scenario is atypical for glaucoma progression, such as this case of progression at low IOP. Neuroimaging can help identify potential lesions and should be considered in patients with other signs suggestive of central nervous system involvement, including optic EJTD�QBMMPS�HSFBUFS�UIBO�DVQQJOH��WJTVBM�mFME�EFGFDUT�PVU�PG�proportion to cupping; bitemporal, homonymous, or vertically BMJHOFE�WJTVBM�mFME�EFGFDUT��FBSMZ�MPTT�PG�DFOUSBM�WJTVBM�BDVJUZ �early dyschromatopsia; or an afferent pupillary defect without asymmetric cupping.61
4��:KDW�LV�WKH�QH[W�WKHUDSHXWLF�VWHS�IRU�WKLV�SDWLHQW"This patient is progressing by both structural and functional criteria, despite having an IOP in the low teens on 2 glaucoma medications (prostaglandin analogue and carbonic anhydrase inhibitor). Alternative likely explanations for her progression have been ruled out, and inadequately controlled glaucoma is the likely explanation. Additional IOP lowering is necessary to halt disease progression. A reasonable goal would be an additional 15% to 20% reduction in IOP (approximately 10-11 mm Hg). One therapeutic approach is to add a third topical medication, such as a beta-blocker or adrenergic agonist, to achieve the target IOP and continue close surveillance.
Other options include proceeding directly with laser trabeculoplasty or incisional surgery. Selective laser trabeculoplasty can lower IOP in patients on multidrug regimens.62�)PXFWFS �JO�QBUJFOUT�XJUI�DPOmSNFE�QSPHSFTTJPO�who require a very low target IOP, traditional glaucoma surgery, such as trabeculectomy or tube-shunt implantation, may be the preferred approach.63 Because this patient BMTP�IBT�B�WJTVBMMZ�TJHOJmDBOU�DBUBSBDU�BOE�JT�GVODUJPOBMMZ�monocular, she may be a candidate for a combined cataract and glaucoma procedure. Lastly, a new generation of minimally invasive glaucoma surgery has emerged in recent years, and these procedures may be acceptable in eyes with coexisting cataract and mild-to-moderate open-angle glaucoma. It should be noted that cataract surgery alone often lowers IOP by several points in eyes with elevated IOP.64-66
SummaryGlaucoma evaluation and management are evolving. New risk factors enable better evaluation of the value of treatment in glaucoma suspects and better understanding of the complex pathophysiology of glaucoma. New treatments will soon come to market, offering novel ways to lower IOP. Each of these advances improves clinicians’ ability to ensure that their patients with glaucoma maintain their sight and preserve their quality of life.

10
1. American Academy of Ophthalmology. Preferred Practice Pattern®. Primary Open-Angle Glaucoma. San Francisco, CA: American Academy of Ophthalmology; 2015.2. Harizman N, Oliveira C, Chiang A, et al. The ISNT rule and differentiation of normal from glaucomatous eyes. Arch Ophthalmol.����������������������3. Budenz DL, Anderson DR, Feuer WJ, et al; Ocular Hypertension Treatment Study � (SPVQ��%FUFDUJPO�BOE�QSPHOPTUJD�TJHOJmDBODF�PG�PQUJD�EJTD�IFNPSSIBHFT�EVSJOH�UIF�� Ocular Hypertension Treatment Study. Ophthalmology.����������������������4. Weinreb RN, Friedman DS, Fechtner RD, et al. Risk assessment in the management of patients with ocular hypertension. Am J Ophthalmol.�������������������5. Sommer A, Tielsch JM, Katz J, et al. Relationship between intraocular pressure and primary open angle glaucoma among white and black Americans. The Baltimore Eye Survey. Arch Ophthalmol. 1991;109(8):1090-1095.��� -FTLF�.$ �8V�4: �)FOOJT�" �)POLBOFO�3 �/FNFTVSF�#��#&4T�4UVEZ�(SPVQ��3JTL�� factors for incident open-angle glaucoma: the Barbados Eye Studies. Ophthalmology. 2008;115(1):85-93.��� Heijl A, Leske MC, Bengtsson B, Hyman L, Bengtsson B, Hussein M; Early Manifest Glaucoma Trial Group. Reduction of intraocular pressure and glaucoma progression: results from the Early Manifest Glaucoma Trial. Arch Ophthalmol. ���������������������8. Kass MA, Heuer DK, Higginbotham EJ, et al. The Ocular Hypertension Treatment Study: a randomized trial determines that topical ocular hypotensive medication delays or prevents the onset of primary open-angle glaucoma. Arch Ophthalmol.�������������������9. Gordon MO, Beiser JA, Brandt JD, et al. The Ocular Hypertension Treatment Study: baseline factors that predict the onset of primary open-angle glaucoma. Arch Ophthalmol. ������������������10. Tielsch JM, Katz J, Sommer A, Quigley HA, Javitt JC. Family history and risk of primary open angle glaucoma. The Baltimore Eye Survey. Arch Ophthalmol.�����������������11. Loyo-Berrios NI, Blustein JN. Primary-open glaucoma and myopia: a narrative review. WMJ.���������������� ����12. Costa L, Cunha JP, Amado D, Pinto LA, Ferreira J. Diabetes mellitus as a risk factor in glaucoma’s physiopathology and surgical survival time: a literature review. J Curr Glaucoma Pract. 2015;9(3):81-85.13. Medeiros FA, Sample PA, Weinreb RN. Frequency doubling technology perimetry � BCOPSNBMJUJFT�BT�QSFEJDUPST�PG�HMBVDPNBUPVT�WJTVBM�mFME�MPTT��Am J Ophthalmol. ����������������������4QSZ�1( �+PIOTPO�$" �.BOTCFSHFS�4- �$JPGm�("��1TZDIPQIZTJDBM�JOWFTUJHBUJPO�PG�� ganglion cell loss in early glaucoma. J Glaucoma. 2005;14(1):11-19.15. Mansouri K, Leite MT, Weinreb RN, Tafreshi A, Zangwill LM, Medeiros FA. Association between corneal biomechanical properties and glaucoma severity. Am J Ophthalmol. ������������������F��16. Costa VP, Harris A, Anderson D, et al. Ocular perfusion pressure in glaucoma. Acta Ophthalmol. 2014;92(4):e252-e266.����#FSEBIM�+1 �"MMJOHIBN�33 �+PIOTPO�%)��$FSFCSPTQJOBM�nVJE�QSFTTVSF�JT�EFDSFBTFE�JO�� primary open-angle glaucoma. Ophthalmology.�������������������18. Coleman AL, Kodjebacheva G. Risk factors for glaucoma needing more attention. Open Ophthalmol J. 2009;3:38-42.19. Miglior S, Pfeiffer N, Torri V, Zeyen T, Cunha-Vaz J, Adamsons I; European Glaucoma Prevention Study (EGPS) Group. Predictive factors for open-angle glaucoma among patients with ocular hypertension in the European Glaucoma Prevention Study. Ophthalmology.���������������20. Gordon MO, Torri V, Miglior S, et al; Ocular Hypertension Treatment Study Group; European Glaucoma Prevention Study Group. Validated prediction model for the development of primary open-angle glaucoma in individuals with ocular hypertension. Ophthalmology.�����������������21. Realini T, Weinreb RN, Wisniewski S. Short-term repeatability of diurnal intraocular pressure patterns in glaucomatous individuals. Ophthalmology.�����������������22. Realini T, Weinreb RN, Wisniewski SR. Diurnal intraocular pressure patterns are not repeatable in the short term in healthy individuals. Ophthalmology. ��������������������23. Realini T. Assessing the effectiveness of intraocular pressure-lowering therapy. Ophthalmology.��������������������������4DIVNBO�+4��&GGFDUT�PG�TZTUFNJD�CFUB�CMPDLFS�UIFSBQZ�PO�UIF�FGmDBDZ�BOE�TBGFUZ�� of topical brimonidine and timolol. Brimonidine Study Groups 1 and 2. Ophthalmology. ��������������������25. Katz LJ, Steinmann WC, Kabir A, Molineaux J, Wizov SS, Marcellino G; SLT/Med Study Group. Selective laser trabeculoplasty versus medical therapy as initial treatment of glaucoma: a prospective, randomized trial. J Glaucoma.����������������������(BOEPMm�4" �6OHBSP�/��-PX�QPXFS�TFMFDUJWF�MBTFS�USBCFDVMPQMBTUZ�4-5�SFQFBUFE�ZFBSMZ�� as primary treatment in ocular hypertension: long term comparison with conventional SLT and ALT. Invest Ophthalmol Vis Sci. 2014;55(13):818.����8BUTPO�1 �4UKFSOTDIBOU[�+��"�TJY�NPOUI �SBOEPNJ[FE �EPVCMF�NBTLFE�TUVEZ�DPNQBSJOH�� latanoprost with timolol in open-angle glaucoma and ocular hypertension. The Latanoprost Study Group. Ophthalmology.�������������������28. Lama PJ. Systemic adverse effects of beta-adrenergic blockers: an evidence-based assessment. Am J Ophthalmol. ������������������29. McIlraith I, Strasfeld M, Colev G, Hutnik CM. Selective laser trabeculoplasty as initial and adjunctive treatment for open-angle glaucoma. J Glaucoma. 2006;15(2):124-130.30. Stein JD, Kim DD, Peck WW, Giannetti SM, Hutton DW. Cost-effectiveness of medications compared with laser trabeculoplasty in patients with newly diagnosed open-angle glaucoma. Arch Ophthalmol.�������������������31. Cavet ME, Vollmer TR, Harrington KL, VanDerMeid K, Richardson ME. Regulation of endothelin-1-induced trabecular meshwork cell contractility by latanoprostene bunod. Invest Ophthalmol Vis Sci. 2015;56(6):4108-4116.����8FJOSFC�3/ �0OH�5 �4DBTTFMMBUJ�4GPS[PMJOJ�# �7JUUJUPX�+- �4JOHI�, �,BVGNBO�1-��70:"(&3�� Study Group. A randomised, controlled comparison of latanoprostene bunod and latanoprost 0.005% in the treatment of ocular hypertension and open angle glaucoma: � UIF�70:"(&3�TUVEZ��Br J Ophthalmol.������������������33. Weinreb RN, Scassellati Sforzolini B, Vittitow J, Liebmann J. Latanoprostene bunod 0.024% versus timolol maleate 0.5% in subjects with open-angle glaucoma or ocular hypertension: the APOLLO Study. Ophthalmology. ������������������34. Medeiros FA, Martin KR, Peace J, Scassellati Sforzolini B, Vittitow JL, Weinreb RN. Comparison of latanoprostene bunod 0.024% and timolol maleate 0.5% in open-angle glaucoma or ocular hypertension: the LUNAR Study. Am J Ophthalmol. 2016;168:250-259.35. Kawase K, Vittitow JL, Weinreb RN, Araie M; JUPITER Study Group. Long-term safety � BOE�FGmDBDZ�PG�MBUBOPQSPTUFOF�CVOPE��������JO�+BQBOFTF�TVCKFDUT�XJUI�PQFO�BOHMF�� glaucoma or ocular hypertension: the JUPITER Study. Adv Ther.��������������������
36. Vittitow JL, Liebmann JM, Kaufman PL, Medeiros FA, Martin KR, Weinreb RN. Long-term � FGmDBDZ�BOE�TBGFUZ�PG�MBUBOPQSPTUFOF�CVOPE��������GPS�JOUSBPDVMBS�QSFTTVSF�MPXFSJOH�JO�� patients with open-angle glaucoma or ocular hypertension: APOLLO and LUNAR studies. Invest Ophthalmol Vis Sci.��������������������-JV�+) �4MJHIU�+3 �7JUUJUPX�+- �4DBTTFMMBUJ�4GPS[PMJOJ�# �8FJOSFC�3/��&GmDBDZ�PG�� latanoprostene bunod 0.024% compared with timolol 0.5% in lowering intraocular pressure over 24 hours. Am J Ophthalmol.������������������38. Impagnatiello F, Toris CB, Batugo M, et al. Intraocular pressure-lowering activity of NCX � ��� �B�OPWFM�OJUSJD�PYJEF�EPOBUJOH�CJNBUPQSPTU�JO�QSFDMJOJDBM�NPEFMT��Invest Ophthalmol Vis Sci. 2015;56(11):6558-6564.����)VBOH�2 �3VJ�&: �$PCCT�. �FU�BM��%FTJHO �TZOUIFTJT �BOE�FWBMVBUJPO�PG�/0�EPOPS�� containing carbonic anhydrase inhibitors to lower intraocular pressure. J Med Chem. 2015;58(6):2821-2833.40. Bacharach J, Dubiner HB, Levy B, Kopczynski CC, Novack GD; AR-13324-CS202 Study Group. Double-masked, randomized, dose-response study of AR-13324 versus latanoprost in patients with elevated intraocular pressure. Ophthalmology. 2015;122(2):� ��������41. Katz LJ, Weiss MJ, Heah T, Kopczynski C, Novack GD. Two phase 3 studies of the � FGmDBDZ�BOE�TBGFUZ�PG�"3�������PQIUIBMNJD�TPMVUJPO��������JO�QBUJFOUT�XJUI�PQFO�BOHMF�� glaucoma and ocular hypertension. Invest Ophthalmol Vis Sci.�����������42. Lewis RA, Levy B, Ramirez N, Kopczynski CC, Usner DW, Novack GD; PG324-CS201 Study Group. Fixed-dose combination of AR-13324 and latanoprost: a double-masked, 28-day, randomised, controlled study in patients with open-angle glaucoma or ocular hypertension. Br J Ophthalmol. 2016;100(3):339-344. 43. Shearer TW, Crosson CE. Adenosine A1 receptor modulation of MMP-2 secretion by trabecular meshwork cells. Invest Ophthalmol Vis Sci. 2002;43(9):3016-3020.����;IPOH�: �:BOH�; �)VBOH�8$ �-VP�9��"EFOPTJOF �BEFOPTJOF�SFDFQUPST�BOE�HMBVDPNB�� an updated overview. Biochim Biophys Acta. 2013;1830(4):2882-2890.45. Myers JS, Sall KN, DuBiner H, et al. A dose-escalation study to evaluate the safety, � UPMFSBCJMJUZ �QIBSNBDPLJOFUJDT �BOE�FGmDBDZ�PG���BOE���XFFLT�PG�UXJDF�EBJMZ�PDVMBS�� trabodenoson in adults with ocular hypertension or primary open-angle glaucoma. J Ocul Pharmacol Ther. 2016;32(8):555-562.����0DVMBS�5IFSBQFVUJY �*OD��1IBTF��C�TUVEZ�FWBMVBUJOH�TBGFUZ�BOE�FGmDBDZ�PG�059�51�� compared to timolol drops in the treatment of subjects with open angle glaucoma or ocular hypertension. ClinicalTrials.gov Web site. https://clinicaltrials.gov/ct2/show/ � /$5����������6QEBUFE�%FDFNCFS��� �������"DDFTTFE�.BSDI�� ����������(MBVLPT�$PSQPSBUJPO��4UVEZ�DPNQBSJOH�USBWPQSPTU�JOUSBPDVMBS�JNQMBOUT�UP�UJNPMPM�� ophthalmic solution. ClinicalTrials.gov Web site. https://clinicaltrials.gov/ct2/show/ � /$5����������6QEBUFE�"QSJM��� �������"DDFTTFE�%FDFNCFS�� ����������"MMFSHBO��&GmDBDZ�BOE�TBGFUZ�PG�CJNBUPQSPTU�TVTUBJOFE�SFMFBTF�43�JO�QBUJFOUT�XJUI�PQFO�� angle glaucoma or ocular hypertension. ClinicalTrials.gov Web site. https://clinicaltrials. � HPW�DU��TIPX�/$5����������6QEBUFE�+BOVBSZ��� �������"DDFTTFE�.BSDI�� ������49. Brandt JD, Sall K, DuBiner H, et al. Six-month intraocular pressure reduction with a topical bimatoprost ocular insert: results of a phase II randomized controlled study. Ophthalmology. 2016;123(8):1685-1694.50. Okeke CO, Quigley HA, Jampel HD, et al. Adherence with topical glaucoma medication monitored electronically the Travatan Dosing Aid Study. Ophthalmology. 2009;116(2): 191-199.51. Liu JH, Zhang X, Kripke DF, Weinreb RN. Twenty-four-hour intraocular pressure pattern associated with early glaucomatous changes. Invest Ophthalmol Vis Sci. 2003;44(4): 1586-1590.52. Mansouri K, Medeiros FA, Tafreshi A, Weinreb RN. Continuous 24-hour monitoring of intraocular pressure patterns with a contact lens sensor: safety, tolerability, and reproducibility in patients with glaucoma. Arch Ophthalmol. 2012;130(12):1534-1539.53. Costa VP, Jimenez-Roman J, Carrasco FG, Lupinacci A, Harris A. Twenty-four-hour ocular perfusion pressure in primary open-angle glaucoma. Br J Ophthalmol. 2010;94(10):1291-1294.����.FNBS[BEFI�' �:JOH�-BJ�. �$IVOH�+ �"[FO�41 �7BSNB�3��-PT�"OHFMFT�-BUJOP�&ZF�4UVEZ�� Group. Blood pressure, perfusion pressure, and open-angle glaucoma: the Los Angeles Latino Eye Study. Invest Ophthalmol Vis Sci.������������������������-FTLF�.$ �8V�4: �/FNFTVSF�# �)FOOJT�"��*ODJEFOU�PQFO�BOHMF�HMBVDPNB�BOE�CMPPE�� pressure. Arch Ophthalmol. ������������������56. Bonomi L, Marchini G, Marraffa M, Bernardi P, Morbio R, Varotto A. Vascular risk factors for primary open angle glaucoma: the Egna-Neumarkt Study. Ophthalmology. � ������������������������5JFMTDI�+. �,BU[�+ �4PNNFS�" �2VJHMFZ�)" �+BWJUU�+$��)ZQFSUFOTJPO �QFSGVTJPO�QSFTTVSF �� and primary open-angle glaucoma. A population-based assessment. Arch Ophthalmol. 1995;113(2):216-221.58. Quigley HA, West SK, Rodriguez J, Munoz B, Klein R, Snyder R. The prevalence of glaucoma in a population-based study of Hispanic subjects: Proyecto VER. Arch Ophthalmol. 2001;119(12):1819-1826.����#VZT�:. �"MBTCBMJ�5 �+JO�:1 �FU�BM��&GGFDU�PG�TMFFQJOH�JO�B�IFBE�VQ�QPTJUJPO�PO�JOUSBPDVMBS�� pressure in patients with glaucoma. Ophthalmology.���������������������60. Malihi M, Sit AJ. Effect of head and body position on intraocular pressure. Ophthalmology. ����������������������(SFFOmFME�%4 �4JBULPXTLJ�3. �(MBTFS�+4 �4DIBU[�/+ �1BSSJTI�3,��OE��5IF�DVQQFE�EJTD��� Who needs neuroimaging? Ophthalmology.��������������������������'SBODJT�#" �*BODIVMFW�5 �4DIPmFME�+, �.JODLMFS�%4��4FMFDUJWF�MBTFS�USBCFDVMPQMBTUZ�� as a replacement for medical therapy in open-angle glaucoma. Am J Ophthalmol. 2005;140(3):524-525.63. Gedde SJ, Schiffman JC, Feuer WJ, Herndon LW, Brandt JD, Budenz DL; Tube Versus Trabeculectomy Study Group. Treatment outcomes in the Tube Versus Trabeculectomy � 575�TUVEZ�BGUFS�mWF�ZFBST�PG�GPMMPX�VQ��Am J Ophthalmol.�������������������F��64. Mansberger SL, Gordon MO, Jampel H, et al; Ocular Hypertension Treatment Study Group. Reduction in intraocular pressure after cataract extraction: the Ocular Hypertension Treatment Study. Ophthalmology. 2012;119(9):1826-1831.65. Poley BJ, Lindstrom RL, Samuelson TW, Schulze R Jr. Intraocular pressure reduction� BGUFS�QIBDPFNVMTJmDBUJPO�XJUI�JOUSBPDVMBS�MFOT�JNQMBOUBUJPO�JO�HMBVDPNBUPVT�BOE�� nonglaucomatous eyes: evaluation of a causal relationship between the natural lens and open-angle glaucoma. J Cataract Refract Surg. 2009;35(11):1946-1955.����4IJOHMFUPO�#+ �-BVM�" �/BHBP�, �FU�BM��&GGFDU�PG�QIBDPFNVMTJmDBUJPO�PO�JOUSBPDVMBS�� pressure in eyes with pseudoexfoliation: single-surgeon series. J Cataract Refract Surg. 2008;34(11):1834-1841.
5HIHUHQFHV

11
To obtain COPE CE Credit for this activity, read the material in its entirety and consult referenced sources as necessary. 8F�PGGFS�JOTUBOU�DFSUJmDBUF�QSPDFTTJOH�BOE�TVQQPSU�(SFFO�$&��1MFBTF�UBLF�UIJT�QPTU�UFTU�BOE�FWBMVBUJPO�POMJOF�CZ�HPJOH�UP KWWSV���WLQ\XUO�FRP�7KH3UHVVXUHV2Q&23(��6QPO�QBTTJOH �ZPV�XJMM�SFDFJWF�ZPVS�DFSUJmDBUF�JNNFEJBUFMZ��:PV�NVTU�TDPSF�����PS�IJHIFS�UP�SFDFJWF�DSFEJU�GPS�UIJT�BDUJWJUZ �BOE�NBZ�UBLF�UIF�UFTU�VQ�UP���UJNFT��
CE Post Test Questions
)RU�LQVWDQW�SURFHVVLQJ��FRPSOHWH�WKH�&(�3RVW�7HVW�RQOLQHKWWS���WLQ\XUO�FRP�7KH3UHVVXUHV2Q&23(�
1. Which of the following is necessary to make a diagnosis of POAG? a. Elevated IOP b. Optic nerve damage� D�� 7JTVBM�mFME�MPTT d. All the above
2. When examining a patient’s ONH, which of the following � mOEJOHT�JT�/05�TVHHFTUJWF�PG�HMBVDPNB a. Disc hemorrhage b. Small optic nerve and cup c. Focal notching of the neuroretinal rim d. Vertical elongation of the optic cup
3. With which stage of glaucoma are early visual defects associated? a. Early b. Moderate c. Advanced d. End-stage
4. When evaluating a patient with suspected glaucoma, which component is the least valuable for assessing risk of � GVUVSF�WJTVBM�mFME�MPTT a. IOP b. Central corneal thickness c. Presence of diabetes d. Refractive error
��� :PV�BSF�DPOTJEFSJOH�UIF�VTF�PG�UPQJDBM�UJNPMPM�UP�NBOBHF�B�� patient’s glaucoma. When taking the patient’s medical history, use of which systemic hypertension medication might prompt you to select a different IOP-lowering agent? a. Angiotensin-converting enzyme inhibitor b. Beta-blocker c. Thiazide diuretic d. Angiotensin receptor blocker
6. In glaucoma, NO can lower IOP by:� B�� *ODSFBTJOH�USBCFDVMBS�PVUnPX b. Reducing aqueous production� D�� *ODSFBTJOH�VWFPTDMFSBM�PVUnPX d. Increasing episcleral venous pressure
��� 8IJDI�PG�UIF�GPMMPXJOH�CFTU�EFTDSJCFT�MBUBOPQSPTUFOF�� bunod? a. Latanoprostene bunod lowers IOP better than timolol, but not as well as latanoprost b. Latanoprostene bunod only has a single mechanism of action c. The most common side effect of LBN is conjunctival hyperemia d. Latanoprostene bunod lowers IOP by 32% to 34%
8. When initiating IOP-lowering therapy in a newly diagnosed patient with early POAG and baseline IOP of 20 mm Hg, what is a reasonable target IOP? a. 15% reduction b. < 21 mm Hg c. 25% reduction d. < 18 mm Hg
9. Which is NOT generally an important consideration when selecting initial therapy for early-stage POAG? a. Dosing frequency� C�� *01�MPXFSJOH�FGmDBDZ c. Mechanism of action d. Safety
�����*O�UIF�QIBTF��C�TUVEZ�PG�mYFE�DPNCJOBUJPO�OFUBSTVEJM �� 0.02%, plus latanoprost, the IOP reduction over baseline was: a. 6.0 mm Hg b. 8.6 mm Hg c. 5.8 mm Hg d. 9.1 mm Hg

in GlaucomaChallenging CasesManaging
THE PRESSURE’S ON!
101D

By Carl H. Spear, OD, MBA, FAAO
For optometrists, many of their daily frustra-
tions revolve around vision care plans (VCP).
To name a few gripes, each provider has
its own set of rules, patients don’t know what
plans or benefits they have, staffers spend a lot
of time verifying benefits or explaining ben-
efits to patients, and reimbursements are low.
To gain more insight in preparation for a
lecture on the topic, I crowdsourced on so-
cial media.
I posted on two optometry Facebook groups,
ODs on Facebook and ODs on Practice Man-
agement and Insurance, asking for complaints
about VCPs in preparation for a SECO lecture.
After reviewing the comments, I divided
them into four topic buckets.
Here are the top four complaints ODs have
with VCPs.
By Justin Bazan, OD
With much of the digital revolution occur-
ring after 2008 and most contact lens tech-
nology developing well before it, there is
an inherent design feature mismatch. The
majority of the available contact lenses are
not designed for how patients are using their
eyes. Specifically, older-generation materials
and designs feature technology that isn’t op-
timized for how we stare at multiple digital
devices for nearly all of our waking hours.
Technology revolutionIt wasn’t until just a few short years ago that
we became a digital-device–obsessed nation.
ODs’ top 4 gripes about vision care plans
Upgrade your patients to new technology
See Contact lens technology on page 16
See VCP gripes on page 6
As primary-care optometrists, we are
the gatekeepers for baby boomers in-
quiring about cataract surgery. To-
day’s patients have treatment options
available not only to address their lifestyle
complaints but to provide them with better
vision and possibly reduced dependence on
glasses or contact lenses.
This generation of active seniors are eager
to embrace their intraocular lens (IOL) op-
tions. They include both traditional cata-
ract surgery and femtosecond laser surgery.
Many optometrists assume that
patients already know what cat-
aracts are. I find most patients think cata-
racts are a “film over the eye.” It is impor-
tant for patients to understand cataracts so
they can better realize why their vision is
changing, and the cause of the glare at night
when they drive, read, or watch television.
Together, we pinpoint their lifestyle com-
plaints—once the cataract is removed, we
see if the complaints have been resolved.
The analogy of a camera works very well
to explain to patients the basic optics of
light entering a normal eye as well as dif-
fraction when light passes through a cata-
ract. I explain that the natural lens in our
eye focuses light onto the retina, and over
See Cataract options on page 18
By Barbara J. Fluder, OD
Offer options to your cataract patientsWhat you need to know about standard
vs. femtosecond laser surgery
&Q A | DR. KATHERINE SCHUETZ PEDIATRIC OPTOMETRY, DAILY DISPOSABLES, AND NAPPING SEE PAGE 38
OptometryTimes.com
APRIL 2017VOL . 9 , NO. 04
PRACTICAL CHAIRSIDE ADVICE
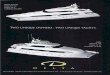
FIGURE 1 LenSx imaging. Image courtesy of Alcon
THE FALSE SECURITY OF A FULL SCHEDULE page 12 N E W S E R I E S O N P O C T E S T I N G page 32
1
DAILIESCHOICE.com*Via mail-in or online rebate on an annual supply of DAILIES TOTAL1® or
DAILIES® AquaComfort Plus® contact lenses. Rebate is in the form of an Alcon Visa Prepaid Card. Must be a new patient to DAILIES TOTAL1® or DAILIES® AquaComfort Plus® contact lenses and must purchase an annual supply of the lenses within 90 days of eye exam and/or contact lens fitting. Applies to purchases from participating retailers only. Visit DAILIESCHOICE.COM for full terms and conditions. Offer ends 12-31-17.
See product instructions for complete wear, care and safety information.
© 2016 Novartis 12/16 US-DAL-16-E-4914
ALCON DAILIES®
CH ICEPROGRAM
S T A R T Y O U R P A T I E N T S O N A
HEALTHY ROUTINE TODAY
Now, you can upgrade your weekly and monthly replacement lens wearers with the ALCON DAILIES® CHOICE PROGRAM
Recommend a healthy choice for your patients and practice
Reduce the price barrier with $200 savings* on a year’s supply
A convenient alternative to weekly and monthly replacement lenses

By Carl H. Spear, OD, MBA, FAAO
For optometrists, many of their daily frustra-
tions revolve around vision care plans (VCP).
To name a few gripes, each provider has
its own set of rules, patients don’t know what
plans or benefits they have, staffers spend a lot
of time verifying benefits or explaining ben-
efits to patients, and reimbursements are low.
To gain more insight in preparation for a
lecture on the topic, I crowdsourced on so-
cial media.
I posted on two optometry Facebook groups,
ODs on Facebook and ODs on Practice Man-
agement and Insurance, asking for complaints
about VCPs in preparation for a SECO lecture.
After reviewing the comments, I divided
them into four topic buckets.
Here are the top four complaints ODs have
with VCPs.
By Justin Bazan, OD
With much of the digital revolution occur-
ring after 2008 and most contact lens tech-
nology developing well before it, there is
an inherent design feature mismatch. The
majority of the available contact lenses are
not designed for how patients are using their
eyes. Specifically, older-generation materials
and designs feature technology that isn’t op-
timized for how we stare at multiple digital
devices for nearly all of our waking hours.
Technology revolutionIt wasn’t until just a few short years ago that
we became a digital-device–obsessed nation.
ODs’ top 4 gripes about vision care plans
Upgrade your patients to new technology
See Contact lens technology on page 16
See VCP gripes on page 6
As primary-care optometrists, we are
the gatekeepers for baby boomers in-
quiring about cataract surgery. To-
day’s patients have treatment options
available not only to address their lifestyle
complaints but to provide them with better
vision and possibly reduced dependence on
glasses or contact lenses.
This generation of active seniors are eager
to embrace their intraocular lens (IOL) op-
tions. They include both traditional cata-
ract surgery and femtosecond laser surgery.
Many optometrists assume that
patients already know what cat-
aracts are. I find most patients think cata-
racts are a “film over the eye.” It is impor-
tant for patients to understand cataracts so
they can better realize why their vision is
changing, and the cause of the glare at night
when they drive, read, or watch television.
Together, we pinpoint their lifestyle com-
plaints—once the cataract is removed, we
see if the complaints have been resolved.
The analogy of a camera works very well
to explain to patients the basic optics of
light entering a normal eye as well as dif-
fraction when light passes through a cata-
ract. I explain that the natural lens in our
eye focuses light onto the retina, and over
See Cataract options on page 18
By Barbara J. Fluder, OD
Offer options to your cataract patientsWhat you need to know about standard
vs. femtosecond laser surgery
&Q A | DR. KATHERINE SCHUETZ PEDIATRIC OPTOMETRY, DAILY DISPOSABLES, AND NAPPING SEE PAGE 38
OptometryTimes.com
APRIL 2017VOL . 9 , NO. 04
PRACTICAL CHAIRSIDE ADVICE
FIGURE 1 LenSx imaging. Image courtesy of Alcon
THE FALSE SECURITY OF A FULL SCHEDULE page 12 N E W S E R I E S O N P O C T E S T I N G page 32
1

Prescribe up to the oxygen1
at the price of conventional hydrogel lenses.
clariti®
1 dayAvailable in sphere, toric and multifocal
100% corneal oxygen consumption2

3Chief Optometric EditorFROM THE
| PRACTICAL CHAIRSIDE ADVICE
It’s the time of year when state legisla-
tures convene to do the people’s business.
Which means it is also the time optometry
undertakes legislation to expand scope of
practice to better care for our patients. For
better or worse, we are a legislated profes-
sion. News abounds of the various states
attempting to add this or that to their op-
tometric scope of practice acts.
If you’ve never been involved in this pro-
cess, I highly recommend you participate
in your state’s efforts. It is an eye-opening
experience. An old saying goes that there
are two things you never want to see: sau-
sage being made and laws being passed.
That figurative pungent aroma emanating
from your state capital is legislation being
crafted. It is not an easy nor gentle process.
I can recall years ago my blood boiling dur-
ing an open floor hearing when the oppo-
sition stated how Georgia residents would
die in the streets if optometrists were given
the right to prescribe topical beta-blockers.
When optometrists go before their state
governing body attempting to enact a piece of
legislation to enhance patient care, it seems
that every special interest group comes out
of the woodwork against us. Ophthalmol-
ogy, the general medical lobby, you name
‘em, they come out to lobby against us.
Meanwhile, on the other side of the aisle,
who aligns with optometry? While we may
garner occasional outside support, often it’s
just us. We’re the ones advocating for our
profession and for our patients’ care. As Dr.
Ben Casella, president of the Georgia Opto-
metric Association, said to me, “If you have
never felt lonely in a crowd, then go to the
Capitol as an optometrist!”
The next time you write a pa-
tient a medical prescription,
take just a moment to think
about that privilege. These
days, we take it for granted.
Yet, that privilege didn’t always
exist and didn’t just magically
happen. It took a lot of our prede-
cessors with the foresight and the willing-
ness to spend their time and their treasure
to win that privilege for our profession so
you can better care for your patients. Those
of us in practice today are standing on the
shoulders of giants past and reaping the
benefits of their efforts.
The process for optometry continues every
year. We need more young giants in our
profession like Dr. Casella and Dr. Johndra
McNeely, South Carolina Optometric Physi-
cian’s Association president-elect, to take
up the mantle.
So, join or become active in your state
association. Associations are our advocates
in the political arena and always work for
our best interests and the interests of the
patients we serve. New and enthusiastic
members are always welcome. Even if you’re
not politically inclined, contribute to
your state association’s political ac-
tion committee (PAC).
It is entirely up to us. The only
people who are going to ensure our
ability to provide absolute state-of-
the-art, cutting-edge patient care
are optometrists. It’s just us.
Optometry stands alone
Our point-of-
care series starts on page
32. Check it out.
Editorial Advisory BoardErnie Bowling, OD, FAAO Chief Optometric Editor
Editorial Advisory Board members are optometric thought leaders. They contribute ideas, offer suggestions, advise the editorial staff, and act as industry ambassadors for the journal.
By Ernie Bowling, OD, FAAOChief Optometric EditorHe is in private practice in Gadsden, AL and is the chair of the Comprehensive Eye Care Section of the American Academy of Optometry.
[email protected] 256-295-2632
Jeffrey Anshel, OD, FAAOOcular Nutrition SocietyENCINITAS, CA
Sherry J. Bass, OD, FAAOSUNY College of OptometryNEW YORK, NY
Justin Bazan, ODPark Slope Eye,BROOKLYN, NY
Marc R. Bloomenstein, OD, FAAOSchwartz Laser Eye CenterSCOTTSDALE, AZ
Crystal Brimer, OD, FAAOCrystal Vision Services,WILMINGTON, NC
Michael Brown, OD, FAAO U.S. Department of Veterans Affairs HUNTSVILLE, AL
Mile Brujic, OD, FAAOPremier Vision GroupBOWLING GREEN, OH
Dori Carlson, OD, FAAOHeartland Eye CarePARK RIVER, ND
Benjamin P. Casella, OD, FAAOCasella Eye CenterAUGUSTA, GA
Michael A. Chaglasian, OD, FAAOIllinois Eye InstituteCHICAGO, IL
A. Paul Chous, OD, MA, FAAOChous Eye Care AssociatesTACOMA, WA
Clark Y. Chang, OD, MSA, MSc, FAAOWills Eye HospitalPHILADELPHIA, PA
Michael S. Cooper, ODWindham Eye GroupWILLIMANTIC, CT
Melanie Denton, OD, MBA, FAAOSalisbury Eyecare and EyewearSALISBURY, NC
Douglas K. Devries, ODEye Care Associates of NevadaSPARKS, NV
Steven Ferucci, OD, FAAOSepulveda VA Ambulatory Care Center & Nursing HomeSEPULVEDA, CA
Barbara Fluder, ODWilliams Eye Institute, MERRILLVILLE, IN
Lisa Frye, ABOC, FNAOEye Care Associates,BIRMINGHAM, AL
Ben Gaddie, OD, FAAOGaddie Eye CentersLOUISVILLE, KY
David I. Geffen, OD, FAAOGordon Weiss Schanzlin Vision InstituteSAN DIEGO, CA
Jeffry D. Gerson, OD, FAAOWestGlen EyecareSHAWNEE, KS
Alan Glazier, OD, FAAO Shady Grove Eye and Vision Care ROCKVILLE, MD
Scott G. Hauswirth, OD, FAAO Minnesota Eye Consultants MINNEAPOLIS, MN
Milton M. Hom, OD, FAAOAZUSA, CA
David L. Kading, OD, FAAOSpecialty Eyecare Group, KIRKLAND, WA
Danica J. Marrelli, OD, FAAOUniversity of Houston College of OptometryHOUSTON, TX
Katherine M. Mastrota, MS, OD, FAAOOmni Eye SurgeryNEW YORK, NY
Ron Melton, OD, FAAOEducators in Primary Eye Care LLCCHARLOTTE, NC
Pamela J. Miller, OD, FAAO, JDHIGHLAND, CA
Brittany Mitchell, ODAlabama Vision Center, BIRMINGHAM, AL
Patricia A. Modica, OD, FAAOSUNY College of OptometryNEW YORK, NY
Leslie O’Dell, OD, FAAODry Eye Treatment Center, HANOVER, PA
Laurie L. Pierce, LDO, ABOMHillsborough Community CollegeTAMPA, FL
Mohammad Rafi eetary, OD, FAAOCharles Retina InstituteMEMPHIS, TN
Stuart Richer, OD, PhD, FAAOJames Lovell Federal Health Care FacilityNORTH CHICAGO, IL
Michael Rothschild, ODWest Georgia Eye CareCARROLLTON, GA
John Rumpakis, OD, MBA, FAAOPractice Resource ManagementLAKE OSWEGO, OR
John L. Schachet, ODEyecare Consultants Vision SourceENGLEWOOD, CO
Scott E. Schachter, ODAdvanced EyecarePISMO BEACH, CA
Leo P. Semes, OD, FAAOUniversity of Alabama at BirminghamSchool of OptometryBIRMINGHAM, AL
Diana L. Shechtman, OD, FAAONova Southeastern UniversityFORT LAUDERDALE, FL
Joseph P. Shovlin, OD, FAAO, DPNAPNortheastern Eye InstituteSCRANTON, PA
Kirk Smick, OD, FAAOClayton Eye CentersMORROW, GA
Joseph Sowka, OD, FAAONova Southeastern University College of OptometryFORT LAUDERDALE, FL
Carl H. Spear, OD, MBA, FAAOPanhandle Vision InstituteNAVARRE, FL
Tracy L. Schroeder Swartz, OD, FAAOMadison Eye CareMADISON, AL
Loretta B. Szczotka-Flynn, OD, MS, FAAOUniversity Hospitals Case Medical CenterCLEVELAND, OH
Marc B. Taub, OD, MS, FAAO, FCOVDSouthern College of OptometryMEMPHIS, TN
William D. Townsend, OD, FAAOAdvanced Eye CareCANYON, TX
William J. Tullo, OD, FAAOTLC Laser Eye Centers/Princeton Optometric PhysiciansPRINCETON, NJ
Walter O. Whitley, OD, MBA, FAAOVirginia Eye ConsultantsNORFOLK, VA
Thomas A. Wong, ODState University of New York College of OptometryNEW YORK, NY

OPTOMETRY TIMES (Print ISSN: 0890-7080, Digital ISSN: 2328-3904) is published monthly (12 issues) by UBM Medica 131 W. First Street, Duluth, MN 55802-2065. Subscription rates: $49 for one year in the United States & Possessions; $59 for one year in Canada and Mexico, and $89 for one year for all other countries. Periodicals Postage paid at Duluth MN 55806 and additional mailing offi ces. POSTMASTER: Please send address changes to OPTOMETRY TIMES, P.O. Box 6089, Duluth, MN 55806-6089. Canadian G.S.T. number: R-124213133RT001, PUBLICATIONS MAIL AGREEMENT NO. 40612608, Return Undeliverable Canadian Addresses to: IMEX Global Solutions, P. O. Box 25542, London, ON N6C 6B2, CANADA. Printed in the U.S.A.©2017 UBM. All rights reserved. No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical including by photocopy, recording, or information storage and retrieval without permission in writing from the publisher. Authorization to photocopy items for internal/educational or personal use, or the internal/educational or personal use of specifi c clients is granted by UBM for libraries and other users registered with the Copyright Clearance Center, 222 Rosewood Dr. Danvers, MA 01923, 978-750-8400 fax 978-646-8700 or visit http://www.copyright.com online. For uses beyond those listed above, please direct your written request to Permission Dept. fax 440-756-5255 or email: [email protected].
ContentCONTENT CHANNEL DIRECTOR Gretchyn M. Bailey, NCLC, [email protected] 215/412-0214
ASSOCIATE EDITOR Giovanni [email protected] 440/891-2602
VP, CONTENT & STRATEGY Sara [email protected] 203/523-7107
GROUP CONTENT DIRECTOR Mark L. [email protected] 440/891-2633
DIRECTOR, DESIGN AND DIGITAL PRODUCTION Nancy [email protected] 203/523-7074
ART DIRECTOR Lecia A. Landis
Publishing/AdvertisingEXECUTIVE VICE PRESIDENT, MANAGING DIRECTOR Georgiann [email protected] 440/891-2778
GROUP PUBLISHER Leonardo [email protected] 302/239-5665
PUBLISHER Erin [email protected] 215/886-3804
NATIONAL ACCOUNT MANAGER Cherie [email protected] 609/636-0172
SALES MANAGER CLASSIFIED/DISPLAY ADVERTISING Tod [email protected] 440/891-2739
ACCOUNT MANAGER, RECRUITMENT ADVERTISING Joanna [email protected] 440/891-2615
VICE PRESIDENT, DIGITAL SOLUTIONS Sarah Cameron Mifsud [email protected] 203/523-7055
SALES DIRECTOR, DIGITAL MEDIA Don [email protected] 203/523-7013
DIGITAL TRAFFIC COORDINATOR Terry [email protected] 218/740-6585
SPECIAL PROJECTS DIRECTOR Meg [email protected] 732/346-3039
VICE PRESIDENT, MARKETING Amy [email protected] 201/523-7041
DIRECTOR OF MARKETING & RESEARCH SERVICES Gail [email protected] 732/346-3042
SALES SUPPORT Kathy [email protected] 732/346-3055
REPRINTS 877/652-5295 ext. 124, [email protected] US, UK, direct dial: 281/419-5725. Ext. 124
LIST ACCOUNT EXECUTIVE Renée [email protected] 440/891-2613
PERMISSIONS/INTERNATIONAL LICENSING Maureen [email protected] 440/891-2742
ProductionSENIOR PRODUCTION DIRECTOR Karen Lenzen
CirculationVICE PRESIDENT, MARKETING & AUDIENCE DEVELOPMENT Joy PuzzoDIRECTOR, AUDIENCE DEVELOPMENT Kristina BildeauxAUDIENCE DEVELOPMENT MANAGER Molly TomfohrdeUBM Medica provides certain customer contact data (such as customers’ names, addresses, phone numbers, and e-mail addresses) to third parties who wish to promote relevant products, services, and other opportunities that may be of interest to you. If you do not want UBM Medica to make your contact information available to third parties for marketing purposes, simply call toll-free 866/529-2922 between the hours of 7:30 a.m. and 5 p.m. CST and a customer service representative will assist you in removing your name from UBM Medica’s lists. Outside the U.S., please phone 218/740-6477.
OPTOMETRY TIMES does not verify any claims or other information appearing in any of the advertisements contained in the publication, and cannot take responsibility for any losses or other damages incurred by readers in reliance of such content.
OPTOMETRY TIMES cannot be held responsible for the safekeeping or return of unsolicited articles, manuscripts, photographs, illustrations or other materials.
Library Access Libraries offer online access to current and back issues of Optometry Times through the EBSCO host databases.To subscribe, call toll-free 888-527-7008. Outside the U.S. call 218/740-6477. UBM Medica provides certain customer contact data (such as customers’ names, addresses, phone numbers, and e-mail addresses) to third parties who wish to promote relevant products, services, and other opportunities that may be of interest to you. If you do not want UBM Medica to make your contact information available to third parties for marketing purposes, simply call toll-free 866/529-2922 between the hours of 7:30 a.m. and 5 p.m. CST and a customer service representative will assist you in removing your name from UBM Medica’s lists. Outside the U.S., please phone 218/740-6477.
OPTOMETRY TIMES does not verify any claims or other information appearing in any of the advertisements contained in the publication, and cannot take responsibility for any losses or other damages incurred by readers in reliance of such content.
OPTOMETRY TIMES cannot be held responsible for the safekeeping or return of unsolicited articles, manuscripts, photographs, illustrations or other materials.
Library Access Libraries offer online access to current and back issues of Optometry Times through the EBSCO host databases.
To subscribe, call toll-free 888-527-7008. Outside the U.S. call 218/740-6477.
APRIL 2017 • VOL. 9, NO. 04@Digit l4
Optometry Times is part of the ModernMedicine Network, a Web-based portal for health professionals offering best-in-class content and tools in a rewarding and easy-to-use environment for knowledge-sharing among members of our community.
OptometryTimes.com
By Gretchyn M. Bailey, NCLC, FAAO
Editor in Chief, Content Channel Director
Optometrists in North Carolina hope to ex-
pand patient access to care by adding laser
procedures to their scope of practice, con-
tinuing optometry’s ongoing goal of best pa-
tient care possible.
HB 36, also known as the Enhanced Ac-
cess to Eye Care Act, would allow ODs in
North Carolina to perform:
– YAG capsulotomy (YAG)
– Laser peripheral iridotomy (PI)
– Selective laser trabeculoplasty (SLT)
– Removal and identification of skin le-
sions around the eye
HB 36 passed its first reading and awaits
a hearing in the House Health Committee.
North Carolina Optometric Society (NCOS)
leadership hopes this hearing takes place by
mid-March, although the hearing has not yet
been scheduled.
By A. Paul Chous, MA, OD, FAAO
Patients with diabetes may present a variety of find-
ings best unveiled by use of spectral domain opti-
cal coherence tomography (SD-OCT). OCT is one
of the best way to assess patients for the presence
of diabetic macular edema (DME). It is extremely
useful for monitoring responses to treatments such
as anti-VEGF injections, grid or focal laser, intra-
vitreal steroids, or any combination thereof in pa-
tients with DME.
Let’s consider a few cases showing multiple OCT
presentations that might be encountered in patients
NC ODs say laser
privileges will expand
access to care
USING OCT WITH YOUR
DIABETES PATIENTS
See OCT and diabetes on page 14
See NC lasers on page 6
The time we are spending on digital de-
vices is on the rise, and it’s unlikely to
slow down any time soon. With more
and more apps, games, and social media
options, we have all become more depen-
dent on smartphones, tablets, and other elec-
tronic devices.
This increased time is trickling down to
kids and teens as well. American teens use
nine hours of media per day, in addition to
time spent on homework and schoolwork.2
A 2014 study (n=288) showed that increased
time on smartphones was significant for
dry eye disease; however, interestingly, time
spent watching television and using com-
puters were not factors.1
Meibomian gland dysfunc-
tion (MGD) and dry eye disease (DED) are
thought to primarily affect the older pop-
ulation. However, data shows that digital
device use is an important dry eye disease
risk factor in children.1
Devices and blink rate
Blink quality and quantity suffer when fo-
cused on near tasks. When blink rates de-
cline, problems ensue.
The tear film will likely begin to break
up prior to the blink response. This lack
of protection from the tear film leaves the
surface of the eye vulnerable, resulting in
damage to cells of the cornea and conjunc-
tiva and impaired functional visual acuity
See Digital devices on page 24
By Scott Schachter, OD
MARCH 2017VOL . 9 , NO. 03
How digital device usage
is affecting youthIf you aren’t screening your younger patients,
you should
FIGURE 1a AND b.
These images with different lighting show the same lid in the same patient. A 16-year-old female has
worn soft contact lenses for two years. She regularly wears mascara and uses digital devices. Note
she exhibits almost 40 percent gland loss.
&Q A | DR. SHAUNA THORNHILL Toys for free eye exams, community service, and $2,000 Manolos SEE PAGE 38
PRACTICAL CHAIRSIDE ADVICE
1a
1b
How to survive allergy season as a contact lens wearer page 16 3 STEPS TO SCRIPT FOR SECOND-PAIR SALES page 22
&
Optometry Times offers weekly blogs from some of the leaders in the optometric profession. Haven’t read them yet? Here’s what you’re missing.
MISSION STATEMENT Optometry Times delivers easily digested, practical information by ODs for ODs. This information can be immediately applied to improve the clinical experience of the next patient in your chair as well as your practice performance. In partnering with our readers, Optometry Times provides data, analysis, tools, and resources which are available whenever and wherever our readers want them.Optometry Times blogs
6 steps to survive a ransomware attack Cyberattacks are on the rise as ODs move more daily tasks to a digital platform. Dr. Melanie Denton explains the steps she followed when her practice suffered a ran-somware attack on its files.OptometryTimes.com/Ransomware
6 challenges when changing from a group to private practiceMaking the switch from a group to private practice can be daunting. Dr. Leslie O’Dell ex-plains the difficulties she faced when changing the direction of her practice. OptometryTimes.com/ChangingPractice
12
TOP HEADLINES Check out what your colleagues are reading.
What patients are tweeting about their ODsOptometryTimes.com/ODTweets
5 things you don’t know about punctal plugsOptometryTimes.com/PunctalPlugs
A different approach to treating demodex blepharitisOptometryTimes.com/BlepharitisTreatment3
APP Get access to all the benefits Optometry
Times offers at your finger-tips. The Optometry Times
app for iPad and iPhone is now free in the iTunes store.
© R
awpix
el.co
m/Sh
utter
stock
.com
TOP SOCIAL See what others arereading on Facebook, Twitter, and Instagram.
12
Roth spots show as initial presentation in multiple myelomaOptometryTimes.com/RothSpots
Retinal prosthesis offers hope to blind patientsOptometryTimes.com/RetinalProsthesis
Handling patients who want you to adjust glasses purchased onlineOptometryTimes.com/AdjustOnline3
©Hal Bohlman, OD, FAAO LIKE USfacebook.com/OptometryTimes
TWEET UStwitter.com/OptometryTimes
FOLLOW USinstagram.com/optometrytimes
STAY IN TOUCH

Designed and Manufactured by NIDEK - Represented by Marco800-874-5274 • marco.com
Refractive
TRS Total Refraction Automation
OPD-Scan III Wavefront
ARK Autorefraction Systems
EPIC Refraction Workstation
ion Anterior Segment Imaging
SOLUTIONS Marco Refraction Systems — Advanced automated instrumentation includes the OPD-Scan III Integrated Wavefront Aberrometer, the TRS-3100/TRS-5100 and EPIC Digital Refraction Workstation, Autorefractors/Keratometers (with VA measurement, 6XEMHFWLYH�6SKHUH�5HÀ�QHPHQW��7RQRPHWU\��*ODUH�WHVWLQJ�RQ�FHUWDLQ�PRGHOV��DQG�Lensmeters–all with EMR integration. And introducing ion IMAGINGSM System– D�KLJKO\�VRSKLVWLFDWHG�VOLW�ODPS�LQWHJUDWHG�DQWHULRU�VHJPHQW�LPDJLQJ�V\VWHP�WKDW�HPSKDVL]HV�LPDJH�TXDOLW\��VLPSOLFLW\�DQG�HIÀ�FLHQF\��The Difference is Marco.TRS-5100
Product/Model name:
REFRACTOR RT-5100

In Focus6 APRIL 2017 |
Here are some comments:
– “The fact that you need a PhD
in ‘EOB [explanation of benefits]
Understanding’ to know what you
get paid.”
– “Too time consuming for op-
tical staff to explain to patients.”
– “[VCPs] never mail ID cards,
so patients don’t know what they
have.”
– “Lack of universal reimburse-
ment across all plans within a VCP.”
– “600-page VCP manual.”
2 REIMBURSEMENTSIt’s not surprising that a
major gripe is reimbursements.
What surprised me was that
reimbursements was not the
top complaint.
Comments include:
– “Low exam fees, terrible pay
for frames and lenses.”
– “In many years no increase in
reimbursement (in fact a decrease)
despite the cost of business going
up—making profitability increas-
ingly difficult.”
– “Getting paid less for an exam
than I did in 1984 when I started
practice.”
– “More and more documenta-
tion, less reimbursement.”
– “ H o r r i b l e e x a m
reimbursement.”
3 COMPETING WITH ODS FOR RETAIL
SALES, PATIENTSODs are feeling the pressure as
VCPs move toward a model that
not only cuts reimbursement but
competes with ODs for patients,
goods, and services.
ODs say:
– “Their newest ploy to drive
patients to purchase their glasses
or contact lenses online and use
their benefits from the website
the insurance company owns.”
– “Two [VCPs] that I know of are
actively emailing patients about
using their benefits online as soon
as the exam authorization is pulled.
We’ve resorted to waiting to pull
those until patients are in office.”
– “Promoting their own online
contact lens sales when they are
already giving me extremely low
reimbursements.”
– “Vertical integration means
they push patients to their physical
entities vs. private practice ODs.”
4 MISLEADING AND INCORRECT
INFORMATIONOf all the categories, this one has
the most responses and raw emo-
tion. The general tone of the re-
sponses and conversations with
my colleagues is that VCPs mis-
lead patients about what is covered
and what is not covered.
Most of this discontent centers
around patients with a known med-
ical diagnosis who expect medi-
cal care from the VCP.
Optometrists say:
– “Too many patients come in
with medical complaints and think
they are covered. Many times the
caring doc feels compelled to take
care of people so he takes care of
the patient. Thus, insurance com-
panies get away with not paying
for medical care.”
– “Patients with medical com-
plaints think these plans should
cover the visit. When the patients
1 DOES IT HAVE TO BE THIS DIFFICULT?
Many people commented on how
difficult VCPs have made the vision
coverage process. ODs say their
staff members invest too much
time with VCP coverage before,
during, and after the exam.
I love my bulb projector!
- Said no one ever
Never changing a projector bulb again is just one of the benefits of upgrading to Acuity Pro digital acuity systems! Plus, faster and more accurate refractions. #notabulber
Don’tbe a bulber...
switch to Acuity Pro
Go from this
to THIS!
Call: 580.243.1301
Toll-Free: 1.877.228.4890 AcuityPro.com
and think outside the bulb!
038520 pgs 03 11 2017 03:10 ADVANSTAR PDF/X-1ablackyellowmagentacyan
ODs’ top 4 gripes about vision care plansContinued from page 1
Within the comments and complaints are very real misunderstandings and opportunities for practices to minimalize these challenges

| PRACTICAL CHAIRSIDE ADVICE In Focus 7
S15294 09/16©2016 Shire All Rights Reserved
A Closer Look At Innovation in Eye Care
Interest in wearables is growing, in fact it's estimated that more than 12 million smartglasses will be ordered by 2020.
Source: "The Future of mHealth Wearables May Focus on Smartglasses," mHealth Intelligence. February 2016
12M
SEE MORE ON MANAGED VISION CARE PLANS
10 tips for reducing staff time on managed vision care plansOptometryTimes.com/10tipsMVCP
The shifting sands of vision care plansOptometryTimes.com/shiftingsandsVCP
Vision care plan industry’s vertical monopolyOptometryTimes.com/verticalmonopoly
4 ways to change your thinking—and your reimbursementOptometryTimes.com/4waystochange
call the VCP, customer service always re-
spond that the plan will cover the exam.
These plans have created a huge issue when
we try to explain this. Also, these plans are
simply discount plans!”
– “One of the plans says it covers diabetic
exams and to pay an extra $5 or $10 for the
diabetic exam.”
Moving forwardMany ODs recognize that VCPs bring pa-
tients into the office and help provide ac-
cess to patients.
ODs might accept reduced payments if the
other problems were mitigated:
– Patients knowing their plans
– VCP reimbursement process streamlined
– Representatives available with consis-
tent, accurate information
– Clear distinction made between medical
coverage and VCPs
– Payment systems that are easy to
understand
If these other problems were addressed,
then the trade-off in reimbursement might
be easier to accept.
I know the list is not inclusive, and I expect
a lot of feedback. Within the comments and
complaints are very real misunderstandings
and opportunities for practices to minimize
these challenges.
Our offices accepted every VCP and were
able to build a successful and thriving busi-
ness by understanding the insurances, devel-
oping processes, and providing high-quality
customer service.
Stay tuned for more. I will share ideas on
how ODs can view these problems as oppor-
tunities to grow their practices.
Dr. Carl Spear’s lecture, “What’s My Beef
with Vision Plans?” was heard at SECO 2017
in Atlanta and was a part of SECO’s “What’s
My Beef” series of lectures.
BASEL, SWITZERLAND—Alcon has received ap-
proval from the U.S. Food and Drug Admin-
istration (FDA) for its AcrySof IQ ReStor+2.5
Multifocal Toric intraocular lens (IOL) with
ActiveFocus optical design for patients un-
dergoing cataract surgery who choose to ad-
dress their astigmatism and presbyopia at
the same time.
The optical design of the ActiveFocus toric
lens delivers both crisp, clear distance vi-
sion and a range of vision for patients who
desire less dependence on glasses, accord-
ing to the company.
Previous presbyopia-correcting IOL designs
tend to compromise on distance vision in
order to provide patients with a range of vi-
sion, according to the company—ActiveFo-
cus toric IOL’s central portion is 100 percent
dedicated to distance vision.
“Presbyopic cataract patients with astig-
matism have had limited options in the past,”
says Sergio Duplan, region president, North
America for Alcon.
“Alcon’s ActiveFocus toric IOL is a break-
through for these patients, correcting astig-
matism and allowing them to achieve uncom-
promised distance vision with an increased
range of vision at the same time,” he says.
The ActiveFocus toric IOL is also engi-
neered for stability, according to the com-
pany. Toric IOLs perform optimally if they
stay on axis to correct the astigmatism. In
a retrospective study of IOL orientation data
by Potvin et al in the September 2016 issue
of Clinical Ophthalmology, the AcrySof IQ
toric IOL platform was two and a half times
less likely to rotate than the leading com-
petitor lens.
“The ActiveFocus toric IOL is the mar-
riage of the design features of my two go-to
IOLs for patients wanting outstanding dis-
tance vision and less dependence on glasses
after cataract surgery,” says Bret L. Fisher,
MD, medical director at Eye Center of North
Florida.
“By combining the unique optical proper-
ties of the ActiveFocus design with the un-
paralleled rotational stability of the AcrySof
IQ toric platform, I can now offer a range of
vision to more patients,” he says.
Nearly four million cataract surgeries are
performed each year in the United States, and
more than 50 percent of those patients have
treatable levels of astigmatism that could
be addressed with AcrySof IQ toric IOLs,
including the new ActiveFocus toric IOL,
according to the company.
Alcon plans to commercialize the Active-
Focus toric IOL in the United States begin-
ning in mid-2017.
Alcon gets FDA nod for ActiveFocus Toric IOLIN BRIEF

APRIL 2017 | 8 Focus On DRY EYE
She also is very smart, and sassy,
having earned a PhD in organic
chemistry decades ago. Mom is
a tough old bird whose career
included teaching grade school
science to performing histocom-
patability research at Memorial
Sloan Kettering Cancer Center
in New York. She has a unique
perspectives and interests in top-
ics from community gardening
to urban planning.
Mom has pseudoexfoliation
syndrome (PXF) clinically vis-
ible in both eyes. She experiences pops
of elevated intraocular pressure (IOP) in
one eye and uses glaucoma medications.
We decided that it was in her best in-
terest to proceed with cataract surgery
because she was experiencing difficulty
traveling home at night from local com-
munity board meetings.
Pre-surgery preparations Pre-surgery presented a question-and-an-
swer period that included lecture-qual-
ity review of the ocular manifestations
and potential surgical complications of
cataract surgery—especially in patients
with PXF.
After the pre-surgery preparations,
Mom hesitantly agreed to proceed with
cataract surgery.
Although PXF is considered a systemic
condition,1 its clinical signs are mostly
identified in the eye. Most practitioners
are familiar with the grey-white material
that is deposited on the anterior struc-
tures, notably the anterior lens capsule.
This material, consisting of
nanometer-sized fibrils within a
loose matrix, is generated mul-
tifocally within the eye. The fi-
brils in PXF are thought to be
generated by polymorphisms in
a gene named LOXL-1(lysyl oxi-
dase like 1) that is responsible
for the biogenesis of connec-
tive tissue.2
One must recognize that the
aberrant material deposited in
PXF impacts many structures
of the eye and may compromise
its proper function.
Disorders associated with PXFWith respect to dry eye and the ocu-
lar surface, patients with PXF appear
to have a higher predisposition of tear
function disorders.
One study, using the Schirmer II test
and assessment of lid parallel conjunc-
tival folds in PXF patients, demonstrated
that there was a statistically significant
difference in tear film break-up time com-
pared to controlled patients.3
There is also an up-regulation of the
non-specific inflammatory marker MMP-9
(matrix metalloproteinase-9) in tear film
in PXF-syndrome.4
Studies show tear osmolarity is higher
in both eyes of patients when compared
with normal subjects, and pseudoexfo-
liation is suggested to alter basic features
of goblet cell morphology—thus affect-
ing tear film stability.5,6
PXF can cause zonular weakness that
can allow for excessive lens movement,
or dislocation, at the time of cataract
surgery. Postoperative inflammation and
corneal edema associated with cataract
surgery may also be increased in eye
with PXF.7
Naturally, I discussed all these things
with my mother prior to her surgery.
Post-surgery outlookFast forward to Mom’s post-operative
statement, “I have no pain.”
My mother had no comment about
her vision, or her lack of possible PXF-
related complications. The comfort of
her eye was the key indicator of success
in her surgery.
It surprised me that in light of my
concerns, it was only lack of discom-
fort that my mother discussed. This ex-
ercise made me re-evaluate my cataract
surgery procedures and how I discuss
surgery with patients.
Would it be better to start by saying,
“We expect minimal postoperative dis-
comfort?”
REFERENCES1. Miglior S, Bertuzzi F. Exfoliative glaucoma: new evidence in the pathogenesis and treatment. Prog
Brain Res. 2015;221:233-41
2. Wiggs JL, Pasquale LR. Expression and regulation of LOXL1 and elastin-related genes in eyes with exfoliation syndrome. J Glaucoma. 2014 Oct-Nov;23(8 Suppl 1):S62-63
3. Škegro I, Suic SP, Kordic R, Jandrokovic S, Petricek I, Kuzman M, Peric S, Masnec S. Ocular surface disease in pseudoexfoliation syndrome. Coll Antropol. 2015 Mar;39(1):43-5.
4. Zimmermann N, Erb C. [Immunoassay for matrix metalloproteinase-9 in the tear film of patients with pseudoexfoliation syndrome - a pilot study]. Klin
Monbl Augenheilkd. 2013 Aug;230(8):804-7.
5. Öncel BA, Pinarci E, Akova YA. Tear osmolarity in unilateral pseudoexfoliation syndrome. Clin Exp
Optom. 2012 Sep;95(5):506-9.
6. Kozobolis VP, Christodoulakis EV, Naoumidi II, Siganos CS, Detorakis ET, Pallikaris LG. Study of conjunctival goblet cell morphology and tear film stability in pseudoexfoliation syndrome. Graefes
Arch Clin Exp Ophthalmol. 2004 Jun;242(6):478-83.
7. Shingleton BJ, Crandall AS, Ahmed II. Pseudoexfoliation and the cataract surgeon: preoperative, intraoperative, and postoperative issues related to intraocular pressure, cataract, and intraocular lenses. J Cataract Refract Surg. 2009 Jun;35(6):1101-20.
Cataract surgery for patients with PXFThese patients are more likely to experience tear function disordersI am fortunate to be able to share stories about my mother.
Many of my article topics have been inspired by experi-
ences and thoughts shared with my mom. For background,
my mother is 79 years old and, except for a bum knee, is
in excellent health.
Patients with PXF appear to have a higher predisposition of tear function disorders
BY KATHERINE M. MASTROTA, MS, OD, FAAO is clinical director of Omni Center for Dry Eye Specialty Care in New York City

Provide a wider range of patients with all-day
comfort and consistently clear vision1
THE BAUSCH + LOMB ULTRA® CONTACT LENS FAMILY IS NOW COMPLETE
FOR MORE INFORMATION, CONTACT YOUR
REPRESENTATIVE OR CALL 1-800-828-9030.
Now for Astigmatism
Helps lenses maintain
95% of their moisture
for a full 16 hours2
Featuring
REFERENCES: 1. Results from a 7-investigator, multi-site 2-week study of Bausch + Lomb ULTRA® for Astigmatism contact lenses on 157 current soft contact lens wearer. 2. Data on file. Bausch & Lomb Incorporated. Rochester, NY; 2013.
®/™ are trademarks of Bausch & Lomb Incorporated or its affiliates. ©2017 Bausch & Lomb Incorporated. UFA.0092.USA.17

APRIL 2017 | 10 Focus On LENS CARE
Many contact lens-wearing patients ask their eyecare pro-
fessional (ECP) about makeup brands, applying makeup,
and how this affects their contact lens wear. What we use
on our faces likely ends up either on the contact lenses
before insertion or in our eyes on the lenses.This includes facial moisturizers,
eye makeup remover, makeup
primers, and most importantly
mascara. A few tips regarding
wearing cosmetics and contact
lens wear can help our patients
wear their lenses with more
comfort.
1Wash hands before applying contact lenses
Always instruct all patients to
wash their hands prior to applying con-
tact lenses. This prevents any type of
contamination or possible infections dur-
ing application.
2Apply contact lenses prior to any facial productSuggest to your patients that they apply
any type of face moisturizers or products
after they handle their contact lenses.
Just like discussing washing hands prior
to applying contact lenses, it is also im-
portant that their hands be free of any
products. Our patients likely assume that
washing hands, then applying facial prod-
ucts means that their hands are clean.
Their hands might not necessarily be
dirty, but that product is now on the con-
tact lenses. Oils and other chemicals pres-
ent in facial cosmetics can affect contact
lens comfort and vision.
3Eye makeup should be hypoallergenic or ECP approved
Most products from major cosmetic compa-
nies have been tested with contact lenses
and are deemed safe. However, many
patients will ask if a brand is safe, es-
pecially if they have had an adverse re-
action in the past.
Always make sure the products they
use are safe to use with contact lenses
and the patient understands the impor-
tance of cleanliness and safety
when using cosmetics around
the eye or when touching the
lids or lashes.
4Makeup removersAll makeup removers are not
made the same and can come
in many forms such as liquids,
foams, oils, pads, cloths, and
creams. Recommend that patients
remove their contact lenses prior
to using an eye makeup remover.
With most of those products, there is a
good deal of scrubbing involved that may
cause some concerns with the contact
lenses. Some brands that work best with
contact lenses are Neutrogena (Johnson
& Johnson) and Clinique (Estée Lauder
Companies), while typical lid scrubs like
OcuSoft (OcuSoft) and Blephadex (Lu-
novus) work well to remove cosmetics
as well. Typically, I recommend the lat-
ter two for your blepharitis patients, but
they also work well for makeup removal
in general.
5Mascara replacementMascara is applied directly to the top
and lower lashes with the same brush
used daily from the same tube. It is rec-
ommended that a single tube of mascara
be replaced every three months. Patients
should replace their mascara immediately
if they contract any type of conjunctivitis.
This three-month rule should also apply
to any cosmetic applicators such as eye
shadow as well. In addition, brushes used
on lids or brows can be cleaned with mild
soap and water.
6Daily replacement contact lenses vs. two-week/monthly
While I think that daily disposable con-
tact lenses are the healthiest choice for
patients, not all patients will be open to
this option. Because of this we must be
prepared to assist even our two-week/
monthly wearers.
For your two-week and monthly re-
placement makeup-wearing contact lens
patients, instruct them to put their con-
tact lenses in their hands and rub for at
least 20 seconds. This will remove any
makeup or debris that has built up. This
even applies to solutions that are “no rub”
because this step may ensure a cleaner
lens, which leads to more comfortable
contact lens wear.
7Case replacementMany makeup-wearing patients store
their contact lens cases in their cos-
metic bags. This causes the cases to be
covered in makeup both on the inside
and the outside of the case.
The cosmetic bag is usually covered in
bacteria from the makeup brushes, con-
tainers, and bottles. Recommend your
patients have a separate bag for their
contact lens products. In general, con-
tact lens cases should be replaced every
three months.
I receive questions almost daily from
patients about cosmetics, face products,
and makeup remover in regard to their
eyes and contact lenses. Making a list of
cosmetic dos and don’ts and printing it
out for your contact lenses patients can
help them better remember and follow
your recommendations and understand
why these steps are important to healthy
lens wear.
Properly discussing these tips can help
our patients wear their contact lenses
safely and avoid any complications.
7 tips for safer lens wear with cosmeticsClean, safe habits when applying makeup can help avoid lens wear complications
Dr. Brittany Mitchell practices in Birmingham, AL, in an OD/MD setting. She is a graduate of the University of Alabama at Birmingham School of Optometry. She is a consultant for Bausch + Lomb and member of B+L’s speaker’s bureau. She also consults for Shire.
Recommend your patients have a separate bag for their contact lens products
BY DR. BRITTANY MITCHELL, ODpractices at Alabama Vision Center

APRIL 2017 | 12 Focus On PRACTICE MANAGEMENT
A filled appointment book is com-
forting; it gives assurances that
the practice will have similar
success in the future as it has
enjoyed in the past. We have
become convinced that filling
our appointment books should
be our primary goal, and ev-
erything else will take care of
itself—and it has worked.
Because filling the appoint-
ment book has been so effec-
tive, we put intense energy into
filling appointment slots. We partnered
with vision insurance companies. We even
took the lead from our dentist mentors
by stressing “recall” and “pre-appoint-
ing”—which also worked.
Many practices that have been estab-
lished and haven’t shown significant
growth find themselves “booked out”—
and that’s a problem.
Full appointment book offers false securityA filled appointment book requires that
your patients are willing to wait until
you are available to see them. This re-
quires your patients to be both patient
and loyal—or they have no other reason-
able choice. If you are in a community
where options are limited, either by lo-
cation or insurance participation, a full
book may serve you well.
Today’s consumers are less willing
to wait for what they want and are less
loyal to your practice than ever before. A
2014 Consumer Health Study found that
61 percent of all American consumers
would change their healthcare
provider for a more convenient
appointment, compared to 47
percent who would change for
a better price.1
These are existing patients
willing to switch providers.
New patients don’t have that
much loyalty and may sched-
ule an appointment with you
but then have an exam at a
competitor later that afternoon.
The cost of no-showsA recent study from the National Insti-
tute of Health estimates that no-shows
cost an average healthcare practice over
$1,000 each and every day.2 And logic
dictates that the further into the future
an appointment is made, the more likely
it is to not be kept.
While simply not showing up for an
appointment is rude, changing the ap-
pointment also costs our practices money.
Staff time taken to communicate with pa-
tients about needs to change an appoint-
ment can add up to significant expenses.
People tend to cancel appointments with
little notice. The longer patients have to
wait to re-schedule, the more likely they
are to cancel.
Pre-appointing vs. recallAlmost everyone in eye care agrees
that annual comprehensive eye exams
are the standard of care maintain visual
wellness. We have implemented a recall
or pre-appointing strategy to help our pa-
tients adhere to this annual exam stan-
dard. These systems have many names
and employ a variety of techniques. For
the sake of this discussion, we will break
the systems into two well-accepted cat-
egories: recall and pre-appointing.
Recall is any action to remind patients
that it is time for them to take action to
schedule their yearly exams. Postcards,
phone calls, email, and text messages are
some examples of tactics used to make
contact. Sometimes the messages con-
veyed are automated to maximize effi-
ciency; others use real people to add the
personal touch. Recalled patients do not
have an existing appointment scheduled
when being “recalled.”
Pre-appointing is the close cousin of re-
call with one difference: Patients already
have an appointment scheduled. A pre-
appointment is different from a standard
appointment because it is scheduled in
the future—typically a year in advance.
As time for the appointment approaches,
many techniques are used to remind the
patient of their appointments, and in-
structions are given to confirm or ad-
just the appointment time. If confirmed,
the pre-appointment is converted to an
appointment.
I have found in my practice that pre-ap-
pointed patients are more likely to sched-
ule their next annual exams, and some
ODs believe they are more likely to come
to that exam. I have also found that pre-
appointed patients are also more likely
to cancel or no-show for their appoint-
ments than recalled patients.
The answer is the systemProper scheduling techniques depend
heavily on the practice’s situation. The
most important factor is that having an
established system in place and adjusting
it frequently based on your ever-chang-
ing circumstances. New practices with
plenty of openings may be a perfect place
for pre-appointments, but a “booked-out”
The false security of a full scheduleBooking strategies important to keep patients happy, ODs stress levels downIt is not uncommon to hear people talk about the health
of their practices by confidently stating how far they are
“booked out.” How long it takes for a patient to get an ap-
pointment is often a statement of practice wellness.
Many practices that have been established and haven’t shown significant growth find themselves “booked out”—and that’s a problem
BY MICHAEL ROTHSCHILD, OD is the CEO of Leadership OD
what no-shows cost an average healthcare practice per day ac-cording to the National Institute of Health estimates
$1K

| PRACTICAL CHAIRSIDE ADVICE 13PRACTICE MANAGEMENT Focus On
practice trying to attract new patients should consider discontinuing
their pre-appointments practice.
Define the primary scheduling objective of your practice by decid-
ing which is more important:
– Availability for new patients within the next few days
– Comfort of a full appointment book for the next few weeks
Consider this strategyCommit to keeping your schedule 80 percent, instead of 100 percent,
full. Full capacity is measured at 100 percent and anything over that
causes stress and strain. Think about what happens to a balloon when
it exceeds capacity. If you are booked at 100 percent and add an emer-
gency appointment, it is difficult to perform at your best.
Reserve the final 20 percent of your appointments for emergen-
cies, urgencies, and new patients. This allows you to add patients
who call and want to
come in today or to-
morrow without over-
stressing the practice.
The challenge comes
when a loyal, long-time
patient wants one of
those final spots. The team needs to be reminded of the practice’s
policy because loyal patients are more willing to wait.
The strategy listed is not perfect for every practice, but it is a strat-
egy with clear definitions, goals, targets, and room for flexibility.
Every scheduling plan needs clear direction.
REFERENCES1. Collier M, Bashman LM. Patient loyalty: It’s up for grabs. Accenture 2014
Consumer Health Study. 2016. Available at: https://www.accenture.com/t20160322T034105__w__/us-en/_acnmedia/Accenture/Conversion-Assets/DotCom/Documents/Global/PDF/Strategy_7/Accenture-Strategy-Patient-
Dr. Rothschild is also a consultant for Alcon, Optos, and Vision Source; a member of the speakers’ bureau for VSP; and a clinical researcher for CIBA Vision.
Recall is any action to remind patients that it is time for them to take action to schedule their yearly exams
of American consumers would change their healthcare provider for a more convenient appointment61%
Engagement-Consumer-Loyalty.pdf. Accessed 3/15/17.
2. Berg B, Murr M, Chermak D, Woodall J, Pignone M, Sandler RS, Denton B. Estimating the cost of no-shows and evaluating the effects of mitigation strategies. Med Decis Making. 2013 Nov;33(8):976-985.
RALEIGH, NC—The Food and Drug Administration (FDA) has approved Icare
USA’s Icare Home tonometer for patient use at home.
According to the company, the unit’s built-in Icare EyeSmart tech-
nology performs automatic OD/OS recognition. Icare EasyPos uses red
and green light signals to help patients correctly position the tonom-
eter. Icare Home also features Icare AMS, an automated measuring
sequence that can take a single measurement or a series of six mea-
surements with one touch of a button.
Icare Home involves no puff of air and requires no drops. In the
hands of patients, it is quick, effortless and effective, according the
company.
For eyecare professionals, Icare Home may help manage patients
who could benefit from additional intraocular pressure monitoring.
FDA approves Icare HomeIN BRIEF
UniversalSmart PhoneAdaptor forSlit LampImaging
Digital Photography
Solutionsfor Slit Lamp
Imaging
Toll free: 800-322-7373
email: [email protected]
www.ttimedical.com
TTI MedicalTransamerican Technologies International
Made in USA
e
Sample Images
All-in-One Digital SLR Camera Adaptor

APRIL 2017 | 14 Focus On RETINA
Exam findingsOn examination, her visual acu-
ity was corrected to 20/20 and
20/25 in the right and left eyes.
The anterior segments of each
eye were unremarkable with ap-
planation tonometry pressures
measured at 16 mm Hg.
Dilated fundus evaluation re-
vealed the picture depicted in
Figure 1. The presence of blurred
disc margins was prominent.
With access to B-scan ultraso-
nography, we performed a scan
of each eye at standard as well
as reduced gain. See Figure 2.
Optical coherence tomography (OCT)
was also performed. Figure 3 shows OD
results. The upper left shows a
reflectance image of the optic
nerve head. The lower left is
a representative cross-section
through the disc. Note that the
elevation is confined within the
scleral ring, consistent with optic
nerve head drusen (ONHD).
Topographic representation of
the disc, color image on Figure
3, reflects the elevation seen in
the cross-sectional presentation.
The scale bar indicates that hot-
ter colors are consistent with
greater elevation.
Figure 4 is a composite representing the
fundus photo and OCT data OD. Clockwise
from the center left are the fundus photo,
OCT cross-section, and topographic data;
the lower right image is a presentation of
the data cube emphasizing not only the
elevation, but confirming the elevation
being confined within the scleral ring.
Any encounter of an elevated optic disc
raises the question of whether the pa-
tient is presenting with true or pseudo-
papilledema. The data in this case are
consistent with a diagnosis of optic disc
drusen. These findings spare the patient
a neuro-ophthalmic workup.
Further analysis included a visual field
evaluation. See Figure 5. Both eyes had
good reliability with only a few sporadic
depressions OD but a pattern consistent
with retinal nerve fiber damage second-
ary to the ONHD.
The patient has been asked to return
annually to monitor visul field changes.
Recent discussionsA recent study examined the use of spectral
domain OCT (SD-OCT) as the gold stan-
dard in distinguishing optic disc drusen
(ODD), ONHD, or optic disc edema (ODE).1
The authors also identified the halo sign
for making the distinction using fundus
photography. In all cases of ODD, the halo
sign was present, indicating the confine-
ment of the elevation within the scleral
The case of blurred disc marginsManaging blurred disc margins can present a challenge for ODsA 16-year-old female was scheduled for her periodic oph-
thalmic evaluation to update her spectacle lens prescrip-
tion. At the visit, she reported a history of migraines, but
the remainder of her personal and family medical history
was non-contributory. She took no medications and had
a history of low hyperopic refractive correction.
Figure 1. Fundus photos of the OD and OS. Note the normal appearance of the maculae but apparent elevation of each optic nerve head.
Figure 3. OD results.
Figure 4. Composite of fundus and OCT.
Figure 2. Ultrasound scans of the OD and OS. Left, OD and OS at standard gain. Right, OD and OS at reduced gain. Note that there is hyperereflectivity localized at the position of the ONH. In addition, the A-scan reflects the same.
BY LEO SEMES, OD, FAAO Professor of optometry at the University of Alabama-Birmingham
1
2
3
4

| PRACTICAL CHAIRSIDE ADVICE 15RETINA Focus On
ring/disc margin. For those without ac-
cess to SD-OCT, identifying the halo sign
at fundus examination and on photogra-
phy may serve as a valuable diagnostic
tool to prevent unnecessary work-ups.2
In cases of mild/early papilledema, oth-
ers have reported that OCT perhaps does
not offer a final adjudication.3 With ad-
vances in OCT technology, the utility as
a differentiator may become more wide-
spread. Alternative imaging may prove
valuable, but not widely available.4 The
utility of OCT for establishing a diagnosis
of optic disc drusen had been suggested
several years ago as a benchmark.5
REFERENCES 1. Lee KM, Woo SJ, Hwang JM. Differentiation between optic disc drusen and optic disc oedema using fundus photography. Acta Ophthalmol. 2017 Jan 13. doi: 10.1111/aos.13338.
2. Costello F. Optical Coherence Tomography in Neuro-ophthalmology. Neurol Clin. 2017 Feb;35(1):153-163.
3. Kulkarni KM, Pasol J, Rosa PR, Lam BL. Differentiating mild papilledema and buried optic nerve head drusen using spectral domain optical coherence tomography. Ophthalmology. 2014 Apr;121(4):959-63.
4. Shah A, et al. Optic disc drusen in a child: diagnosis using noninvasive imaging tools. Optom
Vis Sci. 2013 Oct;90(10):e269-73.
5. Katz BJ, et al. Optic disc edema and optic nerve head drusen. J Neuroophthalmol. 2013 Jun;33(2):204-5.
Figure 5. Visual fields show a pattern consistent with retinal nerve fiber damage secondary to the ONHD.
Dr. Semes is a founding member of the Optometric Glaucoma Society and a founding fellow of the Optometric Retina Society.
5

APRIL 2017 | Contact lenses16
For example, it seems like smartphones have
been part of our lives forever, but the reality
is that the first iPhone debuted in mid-2007.
The iPad was released in 2010. Factor in so-
cial media not really taking off until 2008,
and you begin to see a picture that
helps explain why so many of our
patients are struggling with contact
lens technology that predates their
mobile technology.
Many of my patients are also on
laptops, desktops, tablets, and TVs—
many of them using multiple devices
at the same time. That is a great deal
of screen time, and it only seems to
be increasing. The jury is still out
on how much these digital devices
are harming our ocular health, but one
thing is for certain: While using these devices,
our blink rates drop dramatically.
This reduction in blinking has led to con-
tact lens-related dryness for patients who have
likely upgraded their smartphones but not
their contact lenses. Optometrists should be
proactive in offering their patients solutions
to digital device-induced dryness.
Missing the opportunityHowever, ODs may be missing the opportunity
to offer their patients the solutions they need.
For example, it’s become a habit for ODs
to simply ask their patients how they are
doing with their contact lenses. If we hear,
“Fine,” we move on. This saves us time, but
is it really in the best interest of the patient?
Our patients are accepting end-of-day dis-
comfort as the norm because they don’t real-
ize there are better options. It’s also important
to point out that in the past, we often didn’t
have a better option to offer. All we could
often hope to hear was, “Fine,” because we
didn’t have the upgrade available.
Now, however, I encourage all optometrists
to ask questions to find out how their patients
are really doing with their contacts lenses.
Uncover concerns that patients may perceive
as just a normal part of wearing lenses, such
as dryness.
What works well for me is to assume that
those long hours in front of a laptop or device
are leading to comfort problems. A question
that works well for me is, “How dry are your
lenses feeling around 8 o’clock or 9 o’clock
at night?”
That question accomplishes a few
goals. It alerts patients that dryness
is expected and something I want to
hear more about. It also lets them
know that even if they thought their
contact lenses were fine, there is
something that may be better. Once
a challenge is uncovered, it is easy
to get a trial of the upgraded con-
tact lens on patients’ eyes and out
for a test drive.
Upgrade mindsetPatients know that the next generation of
smartphone will be “better”—that is, faster,
more powerful, more storage, better camera,
and so on. They know this because smart-
phone manufacturers market to them in very
effective ways.
Unfortunately, contact lens companies don’t
have the means necessary to replicate that
type of marketing. So, ODs need to step up to
the plate to inform patients about the benefits
of upgraded contact lens technology.
Contact lens manufacturers are bringing
new technology to your practice. Consider
upgrading your patients to some of these new
technology lenses:
– Acuvue Vita (Johnson & Johnson Vision
Care) monthly lenses feature the company’s
HydraMax Technology for a non-coated sili-
cone hydrogel material to maintain lens hy-
dration throughout the day.
– Biofinity Energys (CooperVision) monthly
lenses address device usage with the com-
pany’s aspheric Digital Zone Optics to re-
duce fatigue and Aquaform Technology to
reduce dryness.
– Biotrue ONEday (Bausch + Lomb) daily
disposables incorporate the company’s Surface
Active Technology—hydrophilic polyvinylpyr-
rilidone (PVP), a water loving molecule, and
Poloxamer 407, a surface active macromer—
to form a dehydration barrier that helps the
lens maintain moisture for most of the day.
This lens is available in toric and presbyopic
designs as well.
– Dailies Total 1 (Alcon) daily disposable
water-gradient lenses combine high oxygen
permeability with high water content for a
soft hydrophilic surface gel for improved com-
fort. These lenses are available in a multifo-
cal design as well.
– MyDay (CooperVision) daily disposable
incorporates Smart Silicone, the company’s
material that uses only 4.4 percent silicon,
allowing for the soft feel of a hydrogel lens
with the oxygen transmission of silicone hy-
drogel material.
– Ultra (Bausch + Lomb) monthly lenses
feature the company’s MoistureSeal Technol-
ogy to help maintain 95 percent of the lens
moisture for most of the day plus aspheric op-
tics, high-water content, and low modulus for
better comfort and vision with device usage.
Offer a trialInnovations have united comfort, health, and
vision in ways that will far surpass previous
technology—much like smartphones have vir-
tually eliminated flip phones. That trinity is
the goal for our contact lens wearers.
Once achieved, we find patients loving their
contact lens experiences. They have:
– Lenses that don’t require attention through-
out the day because they are drying out
– Lenses that don’t interrupt their daily flow
– Lenses that don’t disrupt their lives
So many patients who were doing “fine”
are now doing great.
Often optometrists do patients a huge dis-
service by not at least offering a trial of in-
novative technology. Allowing a patient
to experience how much better these new
lenses can be may make a huge difference.
Upgrade patients to new contact lens technologyContinued from page 1
BY JUSTIN BAZAN, OD is owner of Park Slope Eye in Brooklyn, NY
TAKE-HOME MESSAGE More patients are using digital devices for longer periods. This can adversely affect contact lens discomfort. Much like your patients know to upgrade their device technology, offer them upgrades in their contact lens technology. Patients will better value your services when you offer them more value with education and solutions to contact lens discomfort.
ODs need to step up to the plate to inform patients about the benefits of upgraded contact lens technology

| PRACTICAL CHAIRSIDE ADVICE
be may make a huge difference. It certainly pays
off for the patient. How does it pay off for you?
Finally, consider this common story. A patient
contacts the office to say, “I know my prescrip-
tion is expired, but I also know my prescription
hasn’t changed. Can you just send me a new
copy of it, please?”
Let me translate that into what the patient
is really saying.
“I know that when I come in, you are going to
ask me how my contact lenses are. When I say,
‘Fine,’ you are just going to give me the same
brand you have given me for the last 10 years.
I resent having to pay you for that!”
Have you become a burden to your patients?
Are you an unnecessary step standing in the
way of them ordering their cheap contact lenses
online? Yes! Make sure your patients value your
services by providing them with value in turn.
Beyond the education you should be provid-
ing, there is a psychological aspect to our contact
lens exam. If you present innovative technol-
ogy to your patients the same way technology
companies present new features, expect to see
your patients look forward to upgrading their
contact lenses much in the same way they do
their smartphones.
Six Full Months of
Effective Dry Eye Relief
The doctor gave me
six months…
OMG!
…to my next visit!
Beaver-Visitec International, Inc., 411 Waverley Oaks Road, Waltham, MA 02452
BVI, BVI Logo and all other trademarks (unless noted otherwise) are property of
Beaver-Visitec International (“BVI”) © 2017 BVI
The Extend 180® Long-Term Dissolvable Implant
Featuring
*� Simple insertion technique
*� No foreign body sensation
*� Exceptionally reliable retention
Indications
*� Post-ocular surgery or seasonal dry eye
*� Contact lens intolerance
*� Dry eye associated with digital eye strain
For pre-order introductory pricing
*� 866-906-8080
Coming Soon!
Extend 180
4 sizes!
Dr. Bazan is a 2004 SUNY grad. Reach him on his Facebook page.
So many patients who were doing “fine” are now doing great
WANT MORE CONTACT LENS CONTENT? WE HAVE IT!
Surviving allergy season as a contact lens wearerOptometryTimes.com/allergyCLwear
7 strategies for fitting keratoconus patientsOptometryTimes.com/7KCstrategies
6 contact lens wear and care habits for patients and ODsOptometryTimes.com/6CLhabits
Why accountable contact lens fitting mattersOptometryTimes.com/accountableCLfitting
Fitting ortho-k contact lensesOptometryTimes.com/fittingorthoklenses

18S P E C I A L S E C T I O N
APRIL 2017 |
Comanagement
time this lens gets cloudy and loses
its ability to change focus. This leads
to presbyopia and eventually cata-
racts. Online resources can demon-
strate this very well.
Explaining proceduresYour patients will have a flood of
questions about cataract surgery. They
will ask if it will be performed at a
hospital or an outpatient facility, how
long the procedure takes, and which
surgeon will perform the procedure.
I recommend contacting your co-
managing surgeons to obtain their
protocols so you can better prepare your pa-
tients’ expectations. Patients will feel much
more comfortable and have a sense of con-
tinuity of care if what you say is reiterated
at the surgeon’s office.
I explain that we operate on only one eye
at a time. If patients require IOLs in both
eyes, the surgeries are scheduled one to two
weeks apart. Cataract surgery is an outpatient
procedure, and the patient will be in the sur-
gery center for approximately two hours, with
the procedure taking only 15 to 20 minutes.
In general, patients experience no
pain, no patching, and no sutures. We
numb the eye with a local anesthetic,
dilate the pupil, and give patients
medication, usually Versed (mid-
azolam, Roche), under the tongue
to relax them.
I use an eye model while explain-
ing the procedure and point out the
structures as I talk. Patients will
typically better understand the pro-
cedure if they see the structures of
the eye. I have found that the big-
gest misconception of cataract sur-
gery is that patients believe they
no longer have to wear eyeglasses or contact
lenses. This is very important to clarify with
your patients.
Patients having cataract surgery need to be
informed that they will be seeing you again
during the postoperative period if you coman-
age cataract surgery or they will be seeing
you after their postoperative care for a new
eyeglass prescription.
Preop clinical concernsDuring your preoperative exam, be sure to
examine the lids and tear film. Starting pa-
tients on warm compresses and lid scrubs
twice a day and artificial tears four times a
day before the surgical consult helps to en-
sure accurate measurements. This is very im-
portant for patients interested in advanced
technology lenses along with femtosecond
laser surgery.
Patients with significant map-dot-finger-
print corneal dystrophy may not be ideal can-
didates for laser surgery. Patients with cor-
neal dystrophy, age-related macular degen-
eration, previous refractive surgery, or other
ocular conditions (such as keratoconus or a
history of retinal detachments) may not be
candidates for multifocal IOLs.
Watch for large or small pupils and iris
atrophy. Patients with large pupils are at a
greater risk for experiencing glare postoper-
atively. Small pupils can cause concerns re-
garding a centered capsulorrhexis. Patients
with iris atrophy are at risk for glare, light
sensitivity, and weak zonules.
After your exam and patient discussion, it
is up to you to offer the cataract surgery op-
tions that best fit your patient and his lifestyle.
Regardless of which surgery the patient
receives, both options begin with IOLMaster
(Zeiss) data. It is the gold standard in opti-
cal biometry. It will show IOL power selec-
Offer options to your cataract patientsContinued from page 1
See Cataract options on page 21
BARBARA J. FLUDER, ODhas been in practice for 22 years and currently practice at Williams Eye Institute in Merrillville, IN
TAKE-HOME MESSAGE Patients requiring cataract surgery usually see ODs first. ODs undertake the bulk of patient education about cataracts, the surgical process, and procedure and IOL options. Coordinate with comanaging or referring surgeons for optimal continuity of care. Understand that femtosecond laser surgery addresses astigmatism while phaco procedures do not. Allow clinical data to help determine if patients are good candidates for premium IOLs.
Figure 2. Verion image showing ocular landscape. Image courtesy of Alcon
Figure 3. Marco OPD Calculations Scan
2
3
I use an eye model while explaining the procedure and point out the structures as I talk

For additional safety information, see accompanying Brief Summaryof Safety Information and Full Prescribing Information on Xiidra-ECP.com.
Marks designated ® and ™�>Ài��Ü�i`�LÞ�-��Ài��À�>��>vw���>Ìi`�V��«>�Þ°�^Óä£Ç�-��Ài�1-���V°��iÝ��}Ì��]��Ƃ�äÓ{Ó£�������-ÓnÇn{ 01/17
Indication Xiidra®�NKƂ�VGITCUV�QRJVJCNOKE�UQNWVKQP�����KU�KPFKECVGF�HQT�VJG�VTGCVOGPV�QH�UKIPU�CPF�U[ORVQOU�QH�FT[�G[G�FKUGCU�G�&'&��
Important Safety Information+P�ENKPKECN�VTKCNU��VJG�OQUV�EQOOQP�CFXGTUG�TGCEVKQPU�TGRQTVGF�KP�������QH�RCVKGPVU�YGTG�KPUVKNNCVKQP�UKVG�KTTKVCVKQP��F[UIGWUKC�CPF�TGFWEGF�XKUWCN�CEWKV[��1VJGT�CFXGTUG�TGCEVKQPU�TGRQTVGF�KP����VQ����QH�VJG�RCVKGPVU�YGTG�DNWTTGF�XKUKQP��EQPLWPEVKXCN�J[RGTGOKC��G[G�KTTKVCVKQP��JGCFCEJG��KPETGCUGF�NCETKOCVKQP��G[G�FKUEJCTIG��G[G�FKUEQOHQTV��G[G�RTWTKVWU�CPF�UKPWUKVKU�
6Q�CXQKF�VJG�RQVGPVKCN�HQT�G[G�KPLWT[�QT�EQPVCOKPCVKQP�QH�VJG�UQNWVKQP��RCVKGPVU�UJQWNF�PQV�VQWEJ�VJG�VKR�QH�VJG�UKPING�WUG�EQPVCKPGT�VQ�VJGKT�G[G�QT�VQ�CP[�UWTHCEG�
%QPVCEV�NGPUGU�UJQWNF�DG�TGOQXGF�RTKQT�VQ�VJG�CFOKPKUVTCVKQP�QH�:KKFTC�CPF�OC[�DG�TGKPUGTVGF����OKPWVGU�HQNNQYKPI�CFOKPKUVTCVKQP�
5CHGV[�CPF�GHƂ�ECE[�KP�RGFKCVTKE�RCVKGPVU�DGNQY�VJG�CIG�QH����[GCTU�JCXG�PQV�DGGP�GUVCDNKUJGF�
Proven to treat the signs of inferior corneal staining in 12 weeks and symptoms of eye dryness in 12, 6, and as little as 2.
:KKFTC�JGNRGF�RTQXKFG�U[ORVQO�TGNKGH�HTQO�G[G�FT[PGUU�KP�UQOG�RCVKGPVU�CV�YGGM��tCPF�C�OGCUWTCDNG�TGFWEVKQP�KP�UKIPU�QH�KPHGTKQT�EQTPGCN�UVCKPKPI�KP�LWUV����YGGMU��%QPUKFGT�:KKFTC�VQ�JGNR�[QWT�&T[�'[G�RCVKGPVU�Ƃ�PF�VJG�TGNKGH�VJG[oXG�DGGP�YCKVKPI�HQT�
Check it out at Xiidra-ECP.com
(QWT�TCPFQOK\GF��FQWDNG�OCUMGF�����YGGM�VTKCNU�GXCNWCVGF�VJG�GHƂ�ECE[�CPF�UCHGV[�QH�:KKFTC�XGTUWU�XGJKENG�CU�CUUGUUGF�D[�KORTQXGOGPV�KP�VJG�UKIPU�OGCUWTGF�D[�+PHGTKQT�%QTPGCN�5VCKPKPI�5EQTG��CPF�U[ORVQOU�OGCUWTGF�D[�'[G�&T[PGUU�5EQTG��QH�&T[�'[G�&KUGCUG�0��������
MAKE XIIDRA YOUR FIIRST CHOICE
7�i��>ÀÌ�w�V�>��Ìi>ÀÃ�>Ài�½Ì�i��Õ}�]�V��Ã�`iÀ�«ÀiÃVÀ�L��}�8��`À>�v�À�ÃÞ�«Ì��>Ì�V��ÀÞ� Þi�«>Ì�i�Ìð�

BRIEF SUMMARY:Consult the Full Prescribing Information for complete product information.
INDICATIONS AND USAGEXiidra®�NKƂVGITCUV�QRJVJCNOKE�UQNWVKQP�����KU�KPFKECVGF�for the treatment of the signs and symptoms of dry eye FKUGCUG�&'&��
DOSAGE AND ADMINISTRATIONInstill one drop of Xiidra twice daily (approximately 12 JQWTU�CRCTV��KPVQ�GCEJ�G[G�WUKPI�C�UKPING�WUG�EQPVCKPGT��Discard the single use container immediately after using in each eye. Contact lenses should be removed prior to VJG�CFOKPKUVTCVKQP�QH�:KKFTC�CPF�OC[�DG�TGKPUGTVGF����minutes following administration.
ADVERSE REACTIONSClinical Trials ExperienceBecause clinical studies are conducted under widely varying conditions, adverse reaction rates observed in clinical studies of a drug cannot be directly compared to rates in the clinical trials of another drug and may PQV�TGƃGEV�VJG�TCVGU�QDUGTXGF�KP�RTCEVKEG��+P�ƂXG�ENKPKECN�UVWFKGU�QH�FT[�G[G�FKUGCUG�EQPFWEVGF�YKVJ�NKƂVGITCUV�ophthalmic solution, 1401 patients received at least ��FQUG�QH�NKƂVGITCUV������QH�YJKEJ�TGEGKXGF�NKƂVGITCUV������6JG�OCLQTKV[�QH�RCVKGPVU������JCF�Ű��OQPVJU�QH�VTGCVOGPV�GZRQUWTG������RCVKGPVU�YGTG�GZRQUGF�VQ�NKƂVGITCUV�HQT�CRRTQZKOCVGN[����OQPVJU��6JG�OCLQTKV[�QH�VJG�VTGCVGF�RCVKGPVU�YGTG�HGOCNG�������6JG�OQUV�EQOOQP�CFXGTUG�TGCEVKQPU�TGRQTVGF�KP��������QH�RCVKGPVU�were instillation site irritation, dysgeusia and reduced XKUWCN�CEWKV[��1VJGT�CFXGTUG�TGCEVKQPU�TGRQTVGF�KP����VQ����QH�VJG�RCVKGPVU�YGTG�DNWTTGF�XKUKQP��EQPLWPEVKXCN�hyperemia, eye irritation, headache, increased lacrimation, eye discharge, eye discomfort, eye pruritus and sinusitis.
USE IN SPECIFIC POPULATIONSPregnancy6JGTG�CTG�PQ�CXCKNCDNG�FCVC�QP�:KKFTC�WUG�KP�RTGIPCPV�women to inform any drug associated risks. Intravenous +8��CFOKPKUVTCVKQP�QH�NKƂVGITCUV�VQ�RTGIPCPV�TCVU��HTQO�RTG�OCVKPI�VJTQWIJ�IGUVCVKQP�FC[�����FKF�PQV�RTQFWEG�teratogenicity at clinically relevant systemic exposures. +PVTCXGPQWU�CFOKPKUVTCVKQP�QH�NKƂVGITCUV�VQ�RTGIPCPV�rabbits during organogenesis produced an increased incidence of omphalocele at the lowest dose tested, ��OI�MI�FC[�����HQNF�VJG�JWOCP�RNCUOC�GZRQUWTG�CV�the recommended human ophthalmic dose [RHOD], DCUGF�QP�VJG�CTGC�WPFGT�VJG�EWTXG�=#7%?�NGXGN���5KPEG�JWOCP�U[UVGOKE�GZRQUWTG�VQ�NKƂVGITCUV�HQNNQYKPI�ocular administration of Xiidra at the RHOD is low, the CRRNKECDKNKV[�QH�CPKOCN�ƂPFKPIU�VQ�VJG�TKUM�QH�:KKFTC�WUG�KP�humans during pregnancy is unclear.
Animal Data .KƂVGITCUV�CFOKPKUVGTGF�FCKN[�D[�KPVTCXGPQWU�+8�� KPLGEVKQP�VQ�TCVU��HTQO�RTG�OCVKPI�VJTQWIJ�IGUVCVKQP�FC[�����ECWUGF�CP�KPETGCUG�KP�OGCP�RTGKORNCPVCVKQP�NQUU�and an increased incidence of several minor skeletal CPQOCNKGU�CV����OI��MI��FC[��TGRTGUGPVKPI�������HQNF the human plasma exposure at the RHOD of Xiidra, based on AUC. No teratogenicity was observed in the rat at ���OI��MI��FC[�����HQNF�VJG�JWOCP�RNCUOC�GZRQUWTG�CV�VJG�4*1&��DCUGF�QP�#7%����+P�VJG�TCDDKV��CP�KPETGCUGF�incidence of omphalocele was observed at the lowest FQUG�VGUVGF����OI��MI��FC[�����HQNF�VJG�JWOCP�RNCUOC�GZRQUWTG�CV�VJG�4*1&��DCUGF�QP�#7%���YJGP�CFOKPKUVGTGF�D[�+8�KPLGEVKQP�FCKN[�HTQO�IGUVCVKQP�FC[U���through 19. A fetal No Observed Adverse Effect Level 01#'.��YCU�PQV�KFGPVKƂGF�KP�VJG�TCDDKV�
Lactation 6JGTG�CTG�PQ�FCVC�QP�VJG�RTGUGPEG�QH�NKƂVGITCUV�KP�JWOCP�milk, the effects on the breastfed infant, or the effects on OKNM�RTQFWEVKQP��*QYGXGT��U[UVGOKE�GZRQUWTG�VQ�NKƂVGITCUV�HTQO�QEWNCT�CFOKPKUVTCVKQP�KU�NQY��6JG�FGXGNQROGPVCN�CPF�JGCNVJ�DGPGƂVU�QH�DTGCUVHGGFKPI�UJQWNF�DG�EQPUKFGTGF��along with the mother’s clinical need for Xiidra and any potential adverse effects on the breastfed child from Xiidra.
Pediatric Use 5CHGV[�CPF�GHƂECE[�KP�RGFKCVTKE�RCVKGPVU�DGNQY�VJG�CIG�QH����[GCTU�JCXG�PQV�DGGP�GUVCDNKUJGF��
Geriatric Use No overall differences in safety or effectiveness have been observed between elderly and younger adult patients.
NONCLINICAL TOXICOLOGYCarcinogenesis, Mutagenesis, Impairment of Fertility Carcinogenesis: Animal studies have not been conducted VQ�FGVGTOKPG�VJG�ECTEKPQIGPKE�RQVGPVKCN�QH�NKƂVGITCUV� Mutagenesis: .KƂVGITCUV�YCU�PQV�OWVCIGPKE�KP�VJG�in vitro #OGU�CUUC[��.KƂVGITCUV�YCU�PQV�ENCUVQIGPKE�KP�VJG�in vivo mouse micronucleus assay. In an in vitro chromosomal aberration assay using mammalian cells (Chinese JCOUVGT�QXCT[�EGNNU���NKƂVGITCUV�YCU�RQUKVKXG�CV�VJG�JKIJGUV�concentration tested, without metabolic activation. Impairment of fertility: .KƂVGITCUV�CFOKPKUVGTGF�CV�KPVTCXGPQWU�+8��FQUGU�QH�WR�VQ����OI�MI�FC[� �����HQNF�VJG�JWOCP�RNCUOC�GZRQUWTG�CV�VJG�TGEQOOGPFGF�JWOCP�QRJVJCNOKE�FQUG�4*1&��QH�NKƂVGITCUV�QRJVJCNOKE�UQNWVKQP������JCF�PQ�GHHGEV�QP�fertility and reproductive performance in male and female treated rats.
/CPWHCEVWTGF�HQT��5JKTG�75�+PE�������5JKTG�9C[��.GZKPIVQP��/#��������
(QT�OQTG�KPHQTOCVKQP��IQ�VQ�YYY�:KKFTC�EQO�QT�ECNN����������������
Marks designated ®�CPF�v�CTG�QYPGF�D[�5JKTG� QT�CP�CHƂNKCVGF�EQORCP[�
������5JKTG�75�+PE� 75�2CVGPVU���������������������������������������������������������������������������������������������������������������������������������CPF�RGPFKPI�RCVGPV�CRRNKECVKQPU�� .CUV�/QFKƂGF�������������5�����
Rx Only

21S P E C I A L S E C T I O N
| PRACTICAL CHAIRSIDE ADVICE
Comanagement
tions, keratometry, anterior chamber depth,
and axial length. Its Haigis-L formula helps
determine surgical parameters for patients
with a history of myopic/hyperopic LASIK. The
newer 700 model incorporates swept-source
OCT technology into biometry, allowing it to
detect tilt or decentration of the crystalline
lens.1 It eliminates the need for A-scans be-
cause it is able to scan through dense cata-
racts. It also performs toric IOL calculations.
Standard phaco surgeryUnless otherwise specified, our goal is to re-
duce the patient’s dependence on her glasses.
We will decrease myopia or hyperopia as much
as we can with standard phaco cataract sur-
gery. Remember, however, that astigmatism
is not being addressed, and residual myopia
or hyperopia may persist. It is important to
explain astigmatism and review the amount
of astigmatism the patient has.
I next explain how femto cataract surgery
addresses astigmatism. The laser will make
incisions in the cornea to relax small amounts
of astigmatism. The laser can usually relax
up to 0.75 D corneal cylinder.
I make sure patients understand that stan-
dard phaco cataract surgery begins with a
small incision in the cornea. With the pupil
dilated, the surgeon will make a capsule open-
ing on the lens and break up the lens with
ultrasound. Next, the surgeon will vacuum
the lens through the corneal incision and in-
sert a lens implant in its place.
I have a sample implant lens so patients
can see for themselves what is being placed
in the eye. Be prepared to answer concerns
regarding implant rejection or “going bad,”
IOL replacement, or dislodged or loosening
IOLs. These may seem like silly questions
to us, but to the patient these are very real
concerns.
Femto laser surgeryIf the patient is interested in femtosecond
laser refractive cataract surgery, we obtain
biometric scans with an IOL Master, Verion
Image Guided System (Alcon), and OPD-Scan
(Marco). We compare the astigmatism data
from all three scans to ensure consistency.
For contact lens-wearing patients, we recom-
mend repeat measurements after discontinu-
ing lens wear for several days.
Verion (Figure 1) offers precision and con-
sistency for refractive cataract surgery when
fitting multifocal and toric IOLs. It captures
the landscape of the patient’s eye by taking
a high-resolution digital image useful for ref-
erencing in the operating room.
This “fingerprint” of the eye allows for
Cataract optionsContinued from page 18
SAN DIEGO—Imprimis Pharmaceuticals, Inc. shares
positive findings from a study published in
2017’s volume four of Current Pharmaceuti-
cal Design.
Dropless Cataract Surgery is a single-use,
injectable combination of antibiotic and ste-
roid formulation administered at the end of
cataract surgery to almost eliminate the need
for post-surgery eye drops.
Findings of the study included:
– Compliance concerns are diminished with
Dropless Therapy compared to standard post-
surgery topical drop regimens.
Lack of patient adherence to topical regi-
mens are due to “drop phobia” and improper
instillation of the drops especially in elderly
patients with tremors, poor near vision and
lack of dexterity. The article refers to a recent
study showing more than 90 percent of pa-
tients incorrectly administered eye drops fol-
lowing cataract surgery. High costs may also
deter some patients from filling all of their
prescribed medications.
– Cost savings to patients can range from
$200 to $600 per cataract procedure.
As health care shifts toward capitated care,
the authors believe it is essential to use safe,
efficacious and cost-effective therapy, such
as Dropless.
– Staff time is significantly reduced without
patient, insurance and pharmacy callbacks
about eye drop substitutions and confusion
over topical regimens.
Jeffrey T. Liegner, MD, one of the authors
of the paper, calculates that callbacks require
an estimated 3,000 staff hours annually, or 1.5
full-time equivalents. Although staff time is
significantly reduced, Dropless requires edu-
cating patients about the procedure, why drops
are not being prescribed, and explaining the
perception of floaters following surgery until
excellent vision is experienced.
– A retrospective review of Dropless Therapy
cases found no postoperative endophthalmitis.
Post- surgery infection and inflammation
rates were similar to reported rates with other
alternative prophylactic therapies, such as top-
ical drops.
– There have been no reported major intra-
operative complications associated with the
transzonular injection technique.
The authors concluded, “We believe that
injection of needed medications at the time of
surgery is an important change in the doctor-
patient relationship. Rather than depending
on the patient to take the necessary steps to
obtain a good result, the surgeon can admin-
ister the drugs directly, gaining greater cer-
tainty that the proper dose will be achieved
and gaining greater confidence in the outcome.
It has been our experience that patients very
much appreciate the opportunity to reduce or
eliminate eye drops after surgery.”
“We continue to capture market share as
more and more physicians understand the ben-
efits of Dropless as a prophylactic alternative
to improve the patient experience, eliminate
their own concerns about compliance and help
lower costs for patients,” says John Saharek,
chief commercial officer at Imprimis.
The paper “Dropless Cataract Surgery: An
Overview” was authored by Richard L. Lind-
strom, MD; M. Stewart Galloway, MD; Andrzej
Grzybowski, MD, PhD, MBA; and Jeffrey T.
Liegner, MD.
The paper is available online at http://www.
eurekaselect.com/147752/article?trendmd-
shared=3#.
Imprimis shares positive Dropless therapy resultsIN BRIEF
After your exam and patient discussion, it is up to you to offer the cataract surgery options that best fit your patient and his lifestyle
See Cataract options on page 22

22S P E C I A L S E C T I O N
APRIL 2017 |
Comanagement
precise positioning of incisions and real-time
accurate alignment. Verion will provide IOL
selection, primary and secondary incision
locations, capsulorhexis location, surgically-
induced astigmatism (SIA), and lens position-
ing. Because Verion knows the exact land-
scape of the patient’s eye, it will automati-
cally track in real time and adjust for any eye
movements, including cyclorotation.2
Marco OPD-Scan III (Figure 2) is a corneal
analyzer that uses wavefront data to perform
autorefraction, keratometer, Placido disc to-
pography, wavefront aberrometry, lenticular
residual astigmatism, angle kappa, pre and
post toric IOL measurements, mesopic and
photopic pupil sizes, Zernike graphs, corneal
refractive power map, and IOL tilt/decentra-
tion.3 I rely on the corneal coma, angle kappa,
and mesopic and photopic measurements for
patients interested in a multifocal IOL.
The femtosecond laser procedure begins
by first making the capsulorhexis (Figure 3).
A femtosecond laser capsulorrhexsis is more
regularly shaped, has better centration, and
shows better intraocular lens/capsule over-
lap than a manual one.4
Next, the laser performs nuclear division.
I inform my patients that there is more pre-
cision and less stress on the eye with the
laser because less ultrasound is being used.
Then stair-step primary and secondary inci-
sions are made.
The patient is then transferred from the
laser room to the operating room where the
rest of the procedure is performed. Patients
with small fissures, deep-set eyes, prominent
brows, or significant blepharospasm may not
be candidates for femtosecond laser if the
surgeon does not feel confident docking on
the globe (Figure 4) Aligning the laser to the
patient takes about five minutes. Local anes-
thesia is used, and the laser procedure itself
takes only 30 seconds.
Premium IOLsAll IOL manufacturers offer plenty of printed
material as well as animated video to show
your patients their options. These resources
can help patients better understand the ben-
efits of premium IOLs.
If a patient is interested in a multifocal IOL,
I adhere to the recommended guidelines for
patient candidacy. Our office works mainly
with Alcon IOLs, so I have more experience
with them. We like the patient to be hyper-
opic; however, these patients tend to have a
larger angle kappa.
Angle kappa is the difference between the
pupillary axis and the visual axis (Figure
5).5 It is defined as the angle between the vi-
sual axis (line connecting the fixation point
with the fovea) and the pupillary axis (line
that perpendicularly passes through the en-
trance pupil and the center of curvature of
the cornea).
It can be identified clinically by the nasal
displacement of the corneal light reflex from
the pupil center, and it represents a misalign-
ment of light passing through the refractive
surface of the cornea and the bundle of light
formed by the pupil.5 Angle kappa is not af-
fected by gender, and it tends to decrease
with age.
A large angle kappa is important clinically
because it may lead to alignment errors and
decentration during laser refractive cataract
surgery. Decentration of the IOL can lead to
photopic phenomena (glare and halos) as well
as decrease in lens effectiveness. An option
to compensate for a large angle kappa is to
Cataract optionsContinued from page 21
Figure 4. LenSx docking device. Image courtesy of Alcon
4
U.S. surgeon adoption of femtosecond laser surgery
Source: Market Scope Cataract & Refractive Surgeon Reports Q1 2015–Q4 2016
50
45
40
35
30
25
20
15
10
5
0
10
9
8
7
6
5
4
3
2
1
0Q1 ‘15
% offer today % femto procedure share
Q2 ‘15 Q3 ‘15 Q4 ‘15 Q1 ‘16 Q2 ‘16 Q3 ‘16 Q4 ‘16
Ado
ptio
n ra
te
Fem
to p
roce
dure
sha
re
IOL manufacturers offer printed material and animated video to explain options

23S P E C I A L S E C T I O N
| PRACTICAL CHAIRSIDE ADVICE
Comanagement
purposely decenter the IOL toward the visual
axis. Centering the IOL on the corneal reflex
will greatly reduce the incidence of photopic
phenomena. A decentered IOL can decrease
multifocal function.
Let the patient know multifocal IOLs are not
for everyone, and clinical measurements will
determine if the patient is a good candidate.
Higher order aberrations consist of spher-
ical aberration, coma, and trefoil. Corneal
coma is an imperfection that results in off-
axis point sources such as stars appearing
to have a tail—or coma. Vertical coma is the
most common higher order aberration in pa-
tients with keratoconus, corneal injuries, or
abrasions.6
One study involving 119 eyes undergoing
uncomplicated cataract surgery with a 2.2-
mm incision showed those patients who re-
ceived a superior incision showed significant
negative changes in vertical coma. Patients
who had a nasal incision showed significant
changes in oblique trefoil, and those that had
a temporal incision had insignificant changes
in higher order aberrations.7
We make sure the corneal coma is less than
0.32 μm for each eye. The angle kappa should
be less than 0.43 mm for ReStor (Alcon) and
0.50 mm for Tecnis (Johnson & Johnson Vi-
sion Care) IOL. Also, the photopic pupil size
should be no smaller than 2.0 mm and the
mesopic pupil size no larger than 6.00 mm.
I find this data on Marco OPD.
Patients who currently wear multifocal con-
tact lenses may also be good candidates. They
tend to have more realistic expectations as
well as those with an easy-going personality.
Tell patients the brain will learn to adapt to
the new vision with an IOL. This is called neu-
roadaptation, and it can take several months
to adapt. Look at the patient as a whole. For
example, a patient who is a +6.00 D hyperope
with a mature cataract will be thrilled with
her new vision. However, a -3.00 D myope
with mild to moderate cataracts may be a bit
more critical of the results.
AcrySof IQ ReStor +2.50 D (Alcon) features
the company’s ActiveFocus optical design with
seven diffractive steps. It has a distance cen-
ter with a large peripheral zone that allows
more light to the distance focal point as the
pupil diameter increases and an apodized
diffractive multifocal zone. This IOL is de-
signed for individuals with an active lifestyle
wanting distance and intermediate vision.2
If the patient has 1.00 D or more of cor-
neal cylinder, we opt for toric IOL instead of
a standard implant.
AcrySof IQ Toric (Alcon) IOL is a biconvex
toric with aspheric design and ranges from
+6.0 to +34.0 with seven cylinder powers.
I use the company’s online calculator (ac-
rysoftoriccalculator.com) to calculate the toric
power and axis placement.
ITCH RELIEF24 HOURS OF OCULAR ALLERGY
IN ONE DROP1
Help your patients SAVE on their co-pay for PAZEO® Solution
Your eligible commercially insured patients may pay as little as $10
with the Co-Pay Savings Card!
Limitations apply.*
Olopatadine is licensed from Kyowa Hakko Kirin Co., Ltd. Japan
Novartis Pharmaceuticals CorporationEast Hanover, New Jersey 07936-1080 ©2017 Novartis 3/17 PAL-1342348
Visit www.pazeohcp.com to learn more about PAZEO® Solution and patient savings.
Alcon Pharmaceuticals
$10*
ELIGIBLE COMMERCIALLY
INSURED PATIENTS MAY PAY AS LITTLE AS
CO-PAY OFFER
PAZEO® Solution: The ONLY FDA-approved therapy with
demonstrated 24-hour ocular allergy itch relief in ONE DROP1
PAZEO® Solution has the highest concentration of
olopatadine available on the market1,2
No generic therapeutic equivalent is available2
PAZEO® (olopatadine hydrochloride
ophthalmic solution) 0.7%:
INDICATION AND DOSING
PAZEO® Solution is indicated for the treatment of ocular itching associated with allergic conjunctivitis. The recommended dosage is to instill one drop in each aff ected eye once a day.
IMPORTANT SAFETY INFORMATION
As with any eye drop, care should be taken not to touch the eyelids or surrounding areas with the dropper tip of the bottle to prevent contaminating the tip and solution. Keep bottle tightly closed when not in use.
Patients should not wear a contact lens if their eye is red. PAZEO® Solution should not be used to treat contact lens-related irritation. The preservative in PAZEO® Solution, benzalkonium chloride, may be absorbed by soft contact lenses. Patients who wear soft contact lenses and whose eyes are not red should be instructed to wait at least fi ve minutes after instilling PAZEO® Solution before they insert their contact lenses.
The most commonly reported adverse reactions in a clinical study occurred in 2%-5% of patients treated with either PAZEO® Solution or vehicle. These events were blurred vision, dry eye, superfi cial punctate keratitis, dysgeusia, and abnormal sensation in eye.
For additional information on PAZEO® Solution, please refer to the brief summary of the full Prescribing Information on the following page.
References: 1. PAZEO® Solution Package Insert. 2. US Department of Health and Human Services. Food and Drug Administration. Approved drug products with therapeutic equivalence evaluations. In: The Orange Book. 36th ed. Rockville, MD: US Department of Health and Human Services; 2016.
* Terms and Conditions: Limitations apply. For commercially insured patients. Up to a $125 cap per bottle. Patient will be responsible for any co-pay once limit per bottle is reached. This off er is not valid under Medicare, Medicaid, or any other federal or state program. Not valid for cash-paying patients. Novartis reserves the right to rescind, revoke, or amend this program without notice. Off er expires 12/31/2017.
Patients with large pupils are at a greater risk for experiencing glare postoperatively
See Cataract options on page 24

24S P E C I A L S E C T I O N
APRIL 2017 |
Comanagement
I also use an online visual simulator which
shows patients simulated visual results with
an IOL for activities including golfing, gar-
dening, shopping, and night driving. Enter
the patient’s astigmatism, level of cataract
development, and IOL option to demonstrate
the visual outcome. Obviously, results may
vary, but it is a great way to demonstrate a
patient’s expected visual results with vari-
ous IOL options.
We also implement the ORA System with
VerifEye+ technology. It offers real-time intra-
operative IOL sphere, cylinder, and alignment
suggestions. This is especially useful in the
operating room for patients with a history of
refractive surgery, including LASIK, PRK, and
RK procedures. It helps to account for both
anterior and posterior corneal astigmatism.
The goal is to reduce the incidence of unin-
tended residual postoperative astigmatism.2
After the surgeryComplications associated with cataract sur-
gery are rare. Cataract surgery is one of the
most successful procedures performed in the
United States.8 However, it can include bleed-
ing, retinal detachment, and infection. I as-
sure patients that they will be using antibi-
otics to prevent infection. Bleeding is usually
limited to the conjunctiva and will resolve in
one to two weeks.
We let our patients know there are no restric-
tions. I tell them they can bend, lift, shower,
BRIEF SUMMARY
PAZEO (olopatadine hydrochloride ophthalmic solution) 0.7%. For topical ophthalmic administration. The following is a brief summary only; see full prescribing information for complete product information.
CONTRAINDICATIONS
None.
WARNINGS AND PRECAUTIONS
Contamination of Tip and Solution
As with any eye drop, care should be taken not to touch the eyelids or surrounding areas with the dropper tip of the bottle to prevent contaminating the tip and solution. Keep bottle tightly closed when not in use.
Contact Lens Use
Patients should not wear a contact lens if their eye is red.
The preservative in PAZEO solution, benzalkonium chloride, may be absorbed by soft contact lenses. Patients who wear soft contact lenses and whose eyes are not red, should be instructed to wait at least five minutes after instilling PAZEO before they insert their contact lenses.
ADVERSE REACTIONS
Clinical Trials Experience Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in the practice.
In a randomized, double-masked, vehicle-controlled trial, patients at risk for developing allergic conjunctivitis received one drop of either PAZEO (N=330) or vehicle (N=169) in both eyes for 6 weeks. The mean age of the population was 32 years (range 2 to 74 years). Thirty-five percent were male. Fifty-three percent had brown iris color and 23% had blue iris color. The most commonly reported adverse reactions occurred in 2-5% of patients treated with either PAZEO or vehicle. These events were blurred vision, dry eye, superficial punctate keratitis, dysgeusia and abnormal sensation in eye.
USE IN SPECIFIC POPULATIONS
Pregnancy Risk Summary There are no adequate or well-controlled studies with PAZEO in pregnant women. Olopatadine caused maternal toxicity and embryofetal toxicity in rats at levels 1,080 to 14,400 times the maximum recommended human ophthalmic dose (MRHOD). There was no toxicity in rat offspring at exposures estimated to be 45 to 150 times that at MRHOD. Olopatadine should be used during pregnancy only if the potential benefit justifies the potential risk to the fetus.
Animal Data In a rabbit embryofetal study, rabbits treated orally at 400 mg/kg/day during organogenesis showed a decrease in live fetuses. This dose is 14,400 times the MRHOD, on a mg/m2 basis.
An oral dose of 600 mg/kg/day olopatadine (10,800 times the MRHOD) was shown to be maternally toxic in rats, producing death and reduced maternal body weight gain. When administered to rats throughout organogenesis, olopatadine produced cleft palate at 60 mg/kg/day (1080 times the MRHOD) and decreased embryofetal viability and reduced fetal weight in rats at 600 mg/kg/day. When administered to rats during late gestation and throughout the lactation period, olopatadine produced decreased neonatal survival at 60 mg/kg/day and reduced body weight gain in offspring at 4 mg/kg/day. A dose of 2 mg/kg/day olopatadine produced no toxicity in rat offspring. An oral dose of 1 mg/kg olopatadine in rats resulted in a range of systemic plasma area under the curve (AUC) levels that were
45 to 150 times higher than the observed human exposure [9.7 ng∙hr/mL] following administration of the recommended human ophthalmic dose.
Nursing Mothers
Olopatadine has been identified in the milk of nursing rats following oral administration. Oral administration of olopatadine doses at or above 4 mg/kg/day throughout the lactation period produced decreased body weight gain in rat offspring; a dose of 2 mg/kg/day olopatadine produced no toxicity. An oral dose of 1 mg/kg olopatadine in rats resulted in a range of systemic plasma area under the curve (AUC) levels that were 45 to 150 times higher than the observed human exposure [9.7 ng∙hr/mL] following administration of the recommended human ophthalmic dose. It is not known whether topical ocular administration could result in sufficient systemic absorption to produce detectable quantities in the human breast milk. Nevertheless, caution should be exercised when PAZEO is administered to a nursing mother.
Pediatric Use
The safety and effectiveness of PAZEO have been established in pediatric patients two years of age and older. Use of PAZEO in these pediatric patients is supported by evidence from adequate and well-controlled studies of PAZEO in adults and an adequate and well controlled study evaluating the safety of PAZEO in pediatric and adult patients.
Geriatric Use No overall differences in safety and effectiveness have been observed between elderly and younger patients.
NONCLINICAL TOXICOLOGY
Carcinogenesis, Mutagenesis, Impairment of Fertility Carcinogenicity Olopatadine administered orally was not carcinogenic in mice and rats in doses up to 500 mg/kg/day and 200 mg/kg/day, respectively. Based on a 35 μL drop size and a 60 kg person, these doses are approximately 4,500 and 3,600 times the MRHOD, on a mg/m2 basis.
Mutagenesis No mutagenic potential was observed when olopatadine was tested in an in vitro bacterial reverse mutation (Ames) test, an in vitro mammalian chromosome aberration assay or an in vivo mouse micronucleus test.
Impairment of fertility Olopatadine administered at an oral dose of 400 mg/kg/day (approximately 7,200 times the MRHOD) produced toxicity in male and female rats, and resulted in a decrease in the fertility index and reduced implantation rate. No effects on reproductive function were observed at 50 mg/kg/day (approximately 900 times the MRHOD).
PATIENT COUNSELING INFORMATIONG�!.80�4+��439&2.3&9.43B��);.8*�5&9.*398�94�349�94:(-�)7455*7 tip to eyelids or surrounding areas, as this may contaminate the dropper tip and ophthalmic solution.
G��43(42.9&39�#8*�4+��439&(9�D*38*8B��);.8*�5&9.*398�349�94 wear contact lenses if their eyes are red. Advise patients that PAZEO should not be used to treat contact lens-related irritation. Advise patients to remove contact lenses prior to instillation of PAZEO.
The preservative in PAZEO solution, benzalkonium chloride, may be absorbed by soft contact lenses. Lenses may be reinserted 5 minutes following administration of PAZEO.
Patents: 8,791,154
ALCON LABORATORIES, INC.
Fort Worth, Texas 76134 USA
© 2015 Novartis.
PAL-1342347
Cataract optionsContinued from page 23
See Cataract options on page 26
Figure 5. Diagram of angle kappa. Image courtesy of Wolters Kluwer5
5
I recommend contacting coman-aging surgeons to obtain their protocols so you can better prepare your patients

© 2016 OCuSOFT, Inc., Rosenberg, TX 77471
Kills Bacteria on Contact -“0” Eye Irritationy
Stable 18 Months Opened or Unopened
Ask Yourself This Question...
“Why Prescribe?”
For more information and to order,
call (800) 233-5469 or visit www.ocusoft.com
www.whyprescribe.com

26S P E C I A L S E C T I O N
APRIL 2017 |
Comanagement
shampoo, and do all their usual activities. We
ask them to avoid swimming or hot tubs for
a week. Patients can usually drive after the
one-day postoperative appointment as long
as pupil dilation is resolving and they feel
comfortable driving. Always check the vi-
sual acuity of both eyes. It is common cour-
tesy to send a short postoperative report to
the surgeon.
REFERENCES1. Carl Zeiss. Zeiss presents the new IOLMaster 700 for better predictability and optimized workflows in cataract surgery. Available at: https://www.zeiss.com/meditec/int/media-news/press-releases/iolmaster-700-with-
sweptsource-biometry.html. Accessed 3/15/17.
2. Alcon. The AcrySof Advantage. Available at: https://www.myalcon.com/products/surgical/acrysof-iq-cataract-iols/index.shtml. Accessed 3/15/17.
3. Marco. OPD-SCAN III Wavefront Aberrometer. Available at: https://marco.com/products/wavefront-aberrometry/opd-scan-iii-wavefront-aberrometer/. Accessed 3/15/17.
4. Nagy ZZ, Kránitz K, Takacs AI, Miháltz K, Kovács I, Knorz MC. Comparison of intraocular lens decentration
parameters after femtosecond and manual capsulotomies J Refract Surg. 2011 Aug;27(8):564-9.
5. Moshirfar M, Hoggan RN, Muthappan V. Angle Kappa and its importance in refractive surgery. Oman J
Ophthalmol. 2013 Sep;6(3):151-8.
6. Gordon-Shaag A, Millodot M, Ifrah R, Shneor E. Aberrations and topography in normal, keratoconus-suspect, and keratoconic eyes. Optom Vis Sci. 2012 Apr;89(4):411-8.
7. Seok Song I, Hoon Park J, Hyoung Park H, Young Moon
S, Yong Kim J, Joon Kim M, Tchah H. Corneal coma and trefoil changes associated with incision location in cataract surgery. J Cataract Refract Surg. 2015 Oct;41(10):2145-2151.
8. Torpy JM, Lynm C, Glass RM. Cataracts. JAMA. 2003; 290(2):286.
Cataract optionsContinued from page 24
6 Figure 6. ORA showing positioning of limbal relaxing incisions. Image courtesy of Alcon
Dr. Fluder is a member of the American Optometric Association and the Indiana Optometric Association. She has no financial interest in any of the devices discussed. [email protected]
BEDFORD, MA—Ocular Therapeutix, Inc. announced
positive results of a patient experience study
of Dextenza (dexamethasone insert) 0.4 mg
for intracanalicular use.
The study, published in Patient Preference
and Adherence, evaluated the overall patient
experience and perceived value of Dextenza
following cataract surgery.
Dextenza is a hydrogel-based drug-eluting
intracanalicular insert that incorporates the
U.S. Food and Drug Administration (FDA)-
approved corticosteroid, dexamethasone, as
the active ingredient.
Inserted non-invasively through the punc-
tum, Dextenza resides within the canalicu-
lus and delivers dexamethasone to the ocular
surface for approximately 30 days. Follow-
ing the completion of treatment, Dextenza
resorbs and exits the nasolacrimal system
without need for removal.
The goal associated with Dextenza is to
reduce noncompliance of patient adminis-
tration of topical eye drops following oph-
thalmic surgery by enabling the physician to
control the entire course of steroid therapy
with a single administration.
In parallel, Dextenza aims to remove the
issues commonly associated with non-com-
pliance of post-operative medications follow-
ing ophthalmic surgery.
A New Drug Application (NDA) for Dex-
tenza is currently under review by the FDA
for the treatment of ocular pain occurring
after ophthalmic surgery. The FDA has set
a PDUFA target action date for July 19, 2017.
According to the company, the patient ex-
perience retrospective study was conducted
with 25 patients who had received active treat-
ment in the company’s Phase 3 clinical trials
of Dextenza for the treatment of post-surgical
ocular pain and inflammation.
– All patients reported that the intracana-
licular insert was comfortable.
– Ninety-six percent felt the insert was ex-
tremely or very convenient compared to topi-
cal eye drops on a tapered schedule.
– Ninety-two percent reported the highest
level of overall product satisfaction, with 88
percent saying they would request the insert if
they were to undergo cataract surgery again.
– Ninety-two percent of patients surveyed
said they would recommend Dextenza to
friends or family members.
“We are encouraged by the experiences
these patients shared, which add another di-
mension to the clinical results achieved in
the Phase 3 clinical trials,” says Jonathan H.
Talamo, MD, chief medical officer of Ocular
Therapeutix.
“If approved, we believe that Dextenza,
which incorporates the Company’s proprietary
hydrogel platform technology, will offer an
attractive alternative to the current post-op-
erative standard of care of steroid eye drops
for those recovering from ophthalmic sur-
gery,” he says.
In the company’s third and most recent
Phase 3 clinical trial, Dextenza successfully
met the two primary efficacy endpoints, ab-
sence of ocular pain on Day Eight and ab-
sence of ocular inflammation on Day 14, when
compared to placebo.
According to the company, Dextenza has
exhibited a favorable safety profile and has
been well tolerated in all clinical trials, re-
gardless of indication.
Subject to the approval of the NDA for post-
surgical ocular pain by the FDA, Ocular Thera-
peutix intends to submit an NDA supplement
for Dextenza to broaden its label to include
a post-surgical inflammation indication.
Study positive Dextenza results prior to FDA review date
IN BRIEF

Biotrue® solution helps their lenses keep up
Lenses alone may not always be able to meet the demands of the digital age.
Biotrue® keeps lenses comfortable all day long, with a unique bio-inspired
formulation that works like your patients’ eyes. No wonder it’s the
multi-purpose solution used by more patients.*
Let patients know their solution matters.
Recommend Biotrue® multi-purpose solution.
For more information, call 1-800-828-9030 or visit Bausch.com/ecp
Patients check their devices
110 times a dayBiotruth #32
#
3 BIO-INSPIRED INNOVATIONS
Matches the pH of healthy tears(7.5)1
Keeps key benefi cial tear proteins such as lysozyme active1
Has hyaluronan (HA), a lubricant found naturally in the eyes, helping to provide up to 20 hours of moisture 2
REFERENCES: 1. Data on fi le. Bausch & Lomb Incorporated. Rochester, NY. 2. In vitro studies evaluated the rate of release of sodium hyaluronate (HA), a conditioning agent in the BPZ02 multi-purpose solution, from both conventional and silicone hydrogel contact lenses over a twenty-hour time period. HA was adsorbed on all traditional and silicone hydrogel contact lenses tested upon soaking in the solution overnight. HA is then released from the lenses throughout at least a twenty hour time period when rinsed with Hank’s balanced salt solution at a rate mimicking tear secretions. The in-vitro performance of BPZ02 multi-purpose solution suggests that it will provide lens conditioning throughout a twenty hour time period.
*Highest household penetration among multi-purpose solutions; IRI Panel 52 weeks ending 12/25/16.
® / ™ are trademarks of Bausch & Lomb Incorporated or its affi liates.© 2017 Bausch & Lomb Incorporated. BIO.0050.USA.17

SPECIAL SECTION28 APRIL 2017 |
When it comes to optometric
care, stroke survivors are
often an under-served pop-
ulation—especially when
most of them have visual or ocular
deficits. Stroke survivors with visual
problems are often dead-ended in
neuro-ophthalmology offices because
the internists and cardiologists who
refer them to neuro-ophthalmology
don’t know that ODs can treat stroke-
related visual/ocular challenges. Plus,
many optometrists are unfamiliar
with how they can help stroke survivors.
Although a background in behavioral op-
tometry, vision therapy, and/or neuro-opto-
metric rehabilitation is helpful, primary-care
ODs can easily learn the basics necessary
to treat the most common visual problems
of those who have had a stroke.
Stroke basicsAlmost 800,000 people suffer a stroke every
year, and it is the most common disability
among American adults.1 A stroke occurs
when there is an interruption of the blood
flow to an area of the brain.
There are two types of strokes: an isch-
emic stroke, occurring when a blood clot
blocks a blood vessel, and a hemorrhagic
stroke, occurring when a blood vessel in the
brain ruptures and causes damage. Some
strokes are preceded by brief episodes of
stroke symptoms known as transient isch-
emic attacks (TIA), which are temporary
interruptions of blood supply to the brain.
Because a TIA can occur hours, days, or
weeks before a full stroke, it behooves us to
be aware of the symptoms and signs—tem-
porary episodes of weakness, numbness, pa-
ralysis of the face, arm or leg (especially on
one side of the body), difficulty speaking or
understanding simple statements, and loss
of balance or coordination.2 These symp-
toms can occur on only one side of the body.
To that list should be added any report of
momentary diplopia, transient loss of visual
field, or a passing episode of blurry vision.
Every primary-care optometrist
can—and should—as a minimum
perform the following work-up on a
patient presenting with any signs:
– History of stroke-related signs
and symptoms
– Best-corrected visual acuity
– Pupil reflexes
– Cover test, phorias, ocular
range of motion
– Threshold visual field testing
– Dilated fundus examination
– Stethoscope auscultation of the
carotid arteries for bruits
Whether a clinical ocular deficit is dis-
covered, any transient visual episode should
trigger a call to the patient’s internist or
cardiologist to urge the physician to sched-
ule the patient for a physical. In addition, I
proactively write the patient an Rx for ca-
rotid Doppler testing and/or a CT scan—
this starts the ball rolling.
When a patient presents with a known,
previously documented stroke, pay attention
to current complaints of persisting hemi-
anopsia, diplopia, or eyelid dysfunction.
These conditions can often be treated by
the primary-care optometrist.
DiplopiaDiplopia from a recent stroke is confusing
to the patient because adaptation by a head
turn or suppression has not yet occurred.
Diplopia also causes symptoms of dizzi-
ness, poor balance, trouble reading, psycho-
logical stress, asthenopia, and headaches.
Patients with double vision may mention
those complaints but not say “double vi-
sion” unless asked.
Most stroke survivors with a known cere-
brovascular accident (CVA)-related diplopia
have been instructed to patch the deviating
eye. This makes the patient happy because
the patch resolves the diplopia. Unfortu-
nately, patching the deviating eye for too
many weeks can embed the binocular dys-
function, reducing the possibility of gain-
ing binocular vision.
Therefore, as a minimum, ensure that the
eye patch is alternated daily from the right
eye to left eye. To keep the schedule simple,
I tell patients to patch the right eye on even-
numbered calendar days and to patch the
left eye on odd-numbered calendar days.
Keep in mind that when patching to com-
pensate for diplopia, the patient may be an-
noyed or uncomfortable because of the re-
duced peripheral vision caused by the patch.
In those cases, selective occlusion can be
used by cutting a piece of Transpore surgical
tape into a small rectangle to block central
vision in front of the pupil of the deviating
eye. The tape blocks double vision and al-
lows the patient to retain an awareness of
periphery in the occluded eye, which feels
more comfortable and is safer than a tra-
ditional eye patch.
Some patients with obvious large angles
of paretic strabismus do not complain of
diplopia. That is because the angle of stra-
bismus is so large that the patient can con-
centrate on the image straight ahead of the
non-strabismic eye while ignoring (but not
necessarily suppressing) the diplopic image
located way off center. Although patients
may not complain of diplopia, they may
still have behavioral symptoms of confu-
sion, poor balance, or poor ambulation due
to visual confusion induced by the ambi-
ent diplopic image. This problem requires
consultation with an OD skilled in treating
binocular vision dysfunction.
Stroke-related binocular dysfunctions with
How to care for stroke patientsODs can help these overlooked patients with visual needs
ERROL RUMMEL, OD, FAAO, FCOVD, FNORA, FIALVSis in private practice in Jackson, NJ
TAKE-HOME MESSAGE Optometrists are able to address the visual needs of stroke survivors, an underserved population. Consider using alternate patching or prism for diplopia. For hemianopsia, prescribe separate pairs of glasses for both distance and near for or consider Side Vision Awareness Glasses designed by the author. Lid massage may help lid paresis.
Comanagement
By Errol Rummel, OD, FAAO, FCOVD, FNORA, FIALVS

29S P E C I A L S E C T I O N
| PRACTICAL CHAIRSIDE ADVICE
mild-to-moderate paretic angles of strabis-
mus often are capable of gaining a wider
range of motion of the effected eye. This can
be achieved by having the patient monocu-
larly track a moving target (pursuits) in the
direction of the restrictions several times
per day for a few weeks.
Using prismMany patients are told by non-optometric
doctors that double vision may resolve on
its own within a vague timeline of months
without mentioning vision therapy or prism.
It is dismaying that people with stroke-re-
lated hemiplegia are recommended to have
physical and occupational therapy, but pa-
tients with diplopia are given only an eye
patch and not afforded a chance for bin-
ocular rehabilitation. I suggest prescribing
prism glasses as a stopgap measure to help
the patient feel more comfortable.
Simple vision therapy procedures using a
Brock string or red-green tranaglyphs may
help until vision therapy is initiated. Never
prescribe a ground prism into glasses until
a two- to three-month trial with a Fresnel
prism has shown the angle of deviation to
be steady and that the double vision has
been resolved.
It is important to prescribe the total amount
of Fresnel prism with the prismatic com-
pensation broken up between the two eyes
to allow the Fresnel-induced reduction in
contrast to be distributed evenly between
both eyes.
For example, if an esotropia-related dip-
lopia is resolved with 20 D base-out prism,
it may seem simple to prescribe a single 20
D base-out Fresnel prism before the deviat-
ing eye. However, the patient will usually
complain of blur in the eye with the Fres-
nel prism. Two 10 D base-out prisms are a
better choice because they equalize the 20
D Fresnel-induced poor contrast, which re-
duces patient complaints.
Furthermore, splitting the prism power
between two eyes allows the freedom to
fine tune the prism power when, or if, the
patient’s angle of deviation changes. Peel
off one of the Fresnel prisms and replace
it with another power as is clinically indi-
cated. Keep in mind that the angle of the
paresis measured when viewing at distance
may be very different than at near, so sepa-
rate prismatic distance glasses and reading
glasses are often required.
When prescribing compensating prism
for vertical diplopias, remember that the
angle of deviation usually varies depend-
ing on head position. Be sure to prescribe
the vertical prism with the patient’s head
in a straight-ahead position and warn the
patient that a chin-up or chin-down head
position will likely cause him to see double
in spite of the prism.
A patient whose diplopia is resolved with
prism may begin to complain again of dip-
lopia in a few months. Never assume that
a renewed complaint of diplopia implies a
worsening of the condition. It may mean
that the strabismic angle is decreasing.
Do not be disheartened if a rare patient
can’t fuse binocularly with any amount of
prism. A prism bar may seem to neutral-
ize the diplopia while the patient is in the
chair, but you may find that when you pre-
scribe Fresnel prisms, the patient still com-
Comanagement
See Stroke patients on page 30
Figures 1 and 2.SVAG (Side Vision Awareness Glasses) clear side vision with a wide viewing area when looking through the prism lens.
1
2

30S P E C I A L S E C T I O N
APRIL 2017 |
plains of double vision. At times despite
re-measuring, fine tuning, and changing
prism power, the patient continues to not
fuse the diplopic images.
Some neuro-related diplopias are difficult
to resolve because of damage in the brain
pathways responsible for the binocular vi-
sion reflex, and horror fusionalis, when it
occurs, is difficult or impossible to resolve—
an alternating eye patch may be the only
treatment available.
HemianopsiaStroke-related hemianopsia is reasonably
common. The field defect is obvious on a
24-2 threshold visual field test.
However, some stroke survivors have
hemi-spatial inattention (also known as
“neglect”), which is an inattention to or
lack of sensory awareness of visual space
to one side. It may or may not be associated
with a hemianopsia.
Patients with hemi-spatial inattention
will usually be unaware of their inability
to perceive space on the affected side, may
not be able to follow a moving target in the
direction of the neglect, and may say that
their physician or occupational therapist
“said” that they have visual concerns to the
side (although the patient is not cognitively
aware of the hemianopic like loss of visual
field). That is a difficult concern to address
and should be referred to an optometrist
skilled in neuro-optometric rehabilitation.
Hemianopsia usually leaves a person dis-
oriented and struggling to make it through
daily living. People with hemianopsia are
often afraid to leave their homes and are
concerned about their safety. They are con-
fused in a busy visual environment—such
as the mall where they may bump into peo-
ple—or have the fear of falling off a curb.
Hemianopsia can cause a sense of loss
of independence due to discontinuing driv-
ing. Others find that ambulatory activities
are more difficult. People with hemianopsia
(but without hemi-spatial inattention) can
often be helped by an optometrist.
As a minimum, recommend two sepa-
rate pairs of glasses: one for distance and
one for near. Separate pairs are needed be-
cause with hemianopsia, bifocals or pro-
gressive lenses limit the width of the see-
ing area through the glasses. In my expe-
rience, hemianopsia patients usually have
fewer field-related complaints with full-field
single-vision glasses.
I have prescribed specially-designed eye-
glasses over the past 20 years to help those
with hemianopsia. The optical care of hemi-
anopsia is based on using prism to expand
side vision awareness. Available hemianop-
sia-related glasses I worked with were dif-
ficult to prescribe, difficult for the patient
to use, or had optical design flaws.
I learned what worked and what didn’t
work. I designed a prism technology called
SVAG (Side Vision Awareness Glasses) that
can be prescribed by any trained optome-
trist (See Figures 1 and 2).
Prior to developing SVAG, hemianopsia-
related eyeglasses afforded only a limited
circular viewing area. This limited the pa-
tients’ appreciation of the expanded field
awareness or required a highly-cognitive
patient who could adjust to simultaneously
viewing straight ahead while noticing out-
of-focus peripheral images caused by Fres-
nel prism.
I developed SVAG with a high Abbe value
because patients with older hemianopsia
glasses complained of distracting color ab-
errations. SVAG also have a higher index of
refraction, making them thinner and more
cosmetically acceptable. There is also no
prism button or Fresnel lens strip on the
front of the lens. SVAG provides clear side
vision with a wide viewing area when look-
ing through the prism lens.
Eyelid paresisSome stroke patients develop blepharopa-
resis, while others develop ptosis.
If there is ptosis, avoid disuse of the ptotic
eye by taping it open about a centimeter
for five minutes a few times per day using
Transpore surgical tape. Be sure to allow
enough slack in the tape for blinking. Pa-
tients should instill an artificial tear every
minute to prevent discomfort and drying
during the interval the eye is taped open.
If there is a blepharoparesis and the eye
won’t close, be sure to use Transpore sur-
gical tape to keep the eye closed to prevent
corneal staining and discomfort.
After years of watching physical therapists
work use massage with stroke patients, I
decided to try a similar massage technique
on the eyelids. I found that some patients
with stroke-related ptosis or blepharopare-
sis responded to an eyelid massage.
The massage is conducted with your fin-
ger, using a brisk moderate stroking of the
affected lid in a lateral and radial fan shape.
An alternating warm or cool pack applied
before lid massages may increase sensory
stimulation to the lids, enhancing the ef-
fect. Massage for a few minutes four times
per day for three weeks. Discontinue if no
change in ptosis or belpharoparesis.
Some ptosis patients have what I call dip-
lopic pseudo-ptosis or DPP. Stroke survivors
with a stroke-related esotropia or exotropia
subconsciously learn to close the offending
eye to avoid diplopia. Although they will
appear to have ptosis, it is not ptosis. Cover
the non-ptotic eye; if the patient is capable
of opening the apparently ptotic eye, you
have discovered a DPP.
For blepharoparesis, I sometimes use
commercially available eyelid weights to
pull the lid down. The lid weights come
in a fitting set of graded weights with an
adhesive backing. These test weights are
used to determine the weight of a gold lid
implant used by oculoplastic surgeons. Op-
tometrists can use the test set weights to
treat blepharoparesis noninvasively until
surgery is indicated.
Specialty optometric consultation is avail-
able through colleagues associated with
Neuro-Optometric Rehabilitation Associa-
tion (NORA) and the College of Optometrists
in Vision Development (COVD).
REFERENCES1. National Stroke Association. What is stroke? Available at http://www.stroke.org/understand-stroke/what-stroke. Accessed 3/22/16.
2. National Stroke Association. Transient Ischemic
Attack. 1999. Print.
Comanagement
Stroke patientContinued from page 29
Dr. Rummel is director of the Neuro-Optometric Rehabilitation and Visual Perception Clinic at the Bacharach Institute for Rehabilitation. He has developed protocols for prescribing reverse telescope glasses and Rummel Reading Guides are used by occupational therapists and neuro-rehab optometrists to help patients with hemianopsia. He has served in the United States Army as a Captain in the Optometry Section of the Medical Service Corps.
– History of stroke-related signs and symptoms– Best-corrected visual acuity– Pupil reflexes– Cover test, phorias, ocular range of motion– Threshold visual field testing– Dilated fundus examination– Stethoscope auscultation of the carotid
arteries for bruits
What to include in a possible stroke workup

Toll free 888 - 519 - [email protected] www.oculususa.com
Follow us!
OCULUS Keratograph® 5M
Comprehensive Analysis of the Meibomian Glands
• NEW: The JENVIS Grading Scales for the meibomian glands
• Meibo-Scan: Analysis of the meibomian glands of the upper and lower eyelids
• Comparative display of meibomian glands from up to four examinations
Toll free [email protected] www.oculususa.com
Fol
Please note: The availability of the products and features may differ in your country.
Specifications and design are subject to change. Please contact your local distributor for details.

APRIL 2017 | 32 Point-of-care testing
By William Townsend, OD, FAAO
Even in our era of modern health
care, it is often challenging to
identify and manage dry eye
disease (DED)—at least in part be-
cause it is often difficult to diag-
nose.1 This disparity may be due
to the fact that in many instances,
the signs, symptoms, and severity
of the condition correlate poorly or
not at all.2 For the patient, perhaps
the most significant symptom of DED is fluc-
tuating or reduced vision.
Dry eye and osmolarityAccording to the Dry Eye WorkShop (DEWS)
definition, dry eye is “a multifactorial disease
of the tears and ocular surface that results in
symptoms of discomfort, visual disturbance,
and tear film instability with potential dam-
age to the ocular surface. It is accompanied
by increased osmolarity of the tear film and
inflammation of the ocular surface.”3
Stern et al identified the disparate compo-
nents that function together to protect and
nourish the ocular surface:4
– Cornea
– Conjunctiva
– Accessory lacrimal glands
– Meibomian glands
– Main lacrimal gland
– Interconnecting innervation
system
This cumulative system eventu-
ally came to be known as the lac-
rimal functional unit (LFU).4 The
concept of a multi-component unit
that protects the ocular surface is
vital; it reinforces the theory that
failure of one or more segments of the unit
can lead to DED. We must consider dry eye
as a chronic, bilateral, asymmetric, progres-
sive disease.
In 2014, Bron and colleagues sought to
dispel several misconceptions that hamper
clinical diagnosis and management of DED.
They concluded that “osmolarity appears to
be the best marker across all levels of dis-
ease severity as well as in different subtypes
of DED.”5
Tear osmolarityThe concept of an association between in-
creased tear osmolarity (TO) and DED is not
new. In 1981, Farris published the first re-
port showing a positive correlation among
female gender, increasing age, contact lens
wear, and elevated TO. Large-scale studies
have reinforced the value of TO as a consis-
tent marker in DED.6
In 2006, Tomlinson’s meta-analysis of TO
in normal eyes and diverse subtypes of dry
eye showed a predictive accuracy of 89 per-
cent for the diagnosis of DED.7
Early research directed at the relation-
ship between elevated TO and DED used
the freezing point method of osmometry.8
This method has largely been confined to
research facilities because it requires signifi-
TAKE-HOME MESSAGE Tear osmolarity testing in OD offices can help ODs better diag-nose and manage dry eye patients. In-office testing allows ODs to access more information in a timely fashion, retest as needed for better management, better educate patients, and better recognize the severity of a patient’s condition.
How to use tear osmolarity to help treat dry eye diseaseIn-office testing provides more information for better patient management
WILLIAM TOWNSEND, OD, FAAO, practices in Canyon, TX
Figure 1.The device has a small footprint, making it easy to add tear osmolarity testing to your examination flow. Images courtesy William Townsend, OD, FAAO.
1
See Tear osmolarity on page 34
FIRST OF A FOUR-PART SERIES

References 1. Guthrie S, Dumbleton K. Jones L. Financial implications of patient compliance. Contact Lens Spectrum. 2014;29:42-45. 2. Dumbleton K, Richter D, Bergenske P, Jones LW. Compliance with lens replacement and the interval between eye examinations. Optom Vis Sci. 2013;90(4):351-358. 3. Muya L, Lemp J, Kern J, Sentell K, Lane J, Perry S. Impact of packaging saline wetting agents on wetting substantivity and lubricity. Invest Ophthalmol Vis Sci. 2016; 57(12):ARVO E-abstract 1463. 4. Alcon data on file, 2016. 5. Dewetting analysis; Alcon data on file, 2016. 6. Marx S, Sickenberger W. Wettability of different silicone hydrogel lens materials and blister solutions measured using non-invasive keratographic drying up time (NIK-DUT). Optom Vis Sci. 2016;93:E-abstract 165113. 7. Eiden SB, Davis R, Bergenske P. Prospective study of lotrafilcon B lenses comparing 2 versus 4 weeks of wear for objective and subjective measures of health, comfort, and vision. Eye Contact Lens. 2013;39(4):290-294. 8. Lemp J, Kern J. A comparison of real time and recall comfort assessments. Poster presented at: American Academy of Optometry 2016 Annual Meeting; November 9-12, 2016; Anaheim, CA. 9. In a survey of 310 optometrists in the US; Alcon data on file, 2014.
See product instructions for complete wear, care and safety information. © 2017 Novartis 02/17 US-AOH-17-E-0184 Sponsored by
Our passion is to help your patients see, look
and feel their best.
Important information for AIR OPTIX® plus HydraGlyde (lotrafilcon B), AIR OPTIX® AQUA Multifocal (lotrafilcon B) and AIR OPTIX® for Astigmatism (lotrafilcon B) contact lenses: For daily wear or extended wear up to 6 nights for near/far-sightedness, presbyopia and/or astigmatism. Risk of serious eye problems (i.e., corneal ulcer) is greater for extended wear. In rare cases, loss of vision may result. Side effects like discomfort, mild burning or stinging may occur.
Important information for AIR OPTIX® COLORS (lotrafilcon B) contact lenses: For daily wear only for near/far-sightedness. Contact lenses, even if worn for cosmetic reasons, are prescription medical devices that must only be worn under the prescription, direction and supervision of an eye care professional. Serious eye health problems may occur as a result of sharing contact lenses. Although rare, serious eye problems can develop while wearing contact lenses. Side effects like discomfort, mild burning or stinging may occur. To help avoid these problems, patients must follow the wear and replacement schedule and the lens care instructions provided by their eye doctor.
Important information for AIR OPTIX® NIGHT & DAY® AQUA (lotrafilcon A) contact lenses: Indicated for vision correction for daily wear (worn only while awake) or extended wear (worn while awake and asleep) for up to 30 nights. Relevant Warnings: A corneal ulcer may develop rapidly and cause eye pain, redness or blurry vision as it progresses. If left untreated, a scar, and in rare cases loss of vision, may result. The risk of serious problems is greater for extended wear vs. daily wear and smoking increases this risk. A one-year post-market study found 0.18% (18 out of 10,000) of wearers developed a severe corneal infection, with 0.04% (4 out of 10,000) of wearers experiencing a permanent reduction in vision by two or more rows of letters on an eye chart. Relevant Precautions: Not everyone can wear for 30 nights. Approximately 80% of wearers can wear the lenses for extended wear. About two-thirds of wearers achieve the full 30 nights continuous wear. Side Effects: In clinical trials, approximately 3-5% of wearers experience at least one episode of infiltrative keratitis, a localized inflammation of the cornea which may be accompanied by mild to severe pain and may require the use of antibiotic eye drops for up to one week. Other less serious side effects were conjunctivitis, lid irritation or lens discomfort including dryness, mild burning or stinging. Contraindications: Contact lenses should not be worn if you have: eye infection or inflammation (redness and/or swelling); eye disease, injury or dryness that interferes with contact lens wear; systemic disease that may be affected by or impact lens wear; certain allergic conditions or using certain medications (ex. some eye medications). Additional Information: Lenses should be replaced every month. If removed before then, lenses should be cleaned and disinfected before wearing again. Always follow the eye care professional’s recommended lens wear, care and replacement schedule. Consult package insert for complete information, available without charge by calling (800) 241-5999 or go to myalcon.com.
*Savings via mail-in (or online) rebate. Rebate is in the form of an Alcon VISA® pre-paid card. Certain criteria must be met to be eligible for the full rebate. Must be a new patient to the AIR OPTIX® Family of contact lenses or an existing patient that is switching lenses within the AIR OPTIX® Family. Must purchase an annual supply (four 6-ct boxes) of AIR OPTIX® brand contact lenses (excluding AIR OPTIX® AQUA lenses) within 90 days of eye exam or contact lens fitting. Partial rebate available for purchasing a 6-month supply (two 6-ct boxes) of AIR OPTIX® brand contact lenses (excluding AIR OPTIX® AQUA lenses) within 90 days of eye exam or contact lens fitting. Rebate submission must be postmarked (or submitted electronically) within 60 days of lens purchase date. Valid on purchases made at participating retailers through 6/30/17. Visit AIROPTIXCHOICE.com for complete terms and conditions.
†Based on a clinical study with AIR OPTIX® AQUA, AIR OPTIX® for Astigmatism, and AIR OPTIX® AQUA Multifocal contact lenses.
At Alcon, we are committed to helping you move ALL of your contact lens patients to a more compliant replacement schedule. Recent studies show that a monthly replacement frequency can have several benefits: 65% of monthly
replacement wearers replaced their lenses on time vs. 30% of 2-week replacement wearers1; and the interval between annual
office visits was shorter with monthly replacement vs. 2-week replacement.2 Because we believe that all patients should have access to contact lenses with a healthy replacement schedule, we are proud to introduce the Alcon AIR OPTIX® Choice Program. Now, patients will benefit when upgrading to many of the products in the AIR OPTIX® contact lens family,* including AIR OPTIX® plus HydraGlyde®, our latest monthly lens innovation combining our 2 breakthrough technologies—SmartShield® surface technology and HydraGlyde® Moisture Matrix—for long-lasting lens surface wettability.3-6
As a practitioner, you expertly consider several factors when choosing which lens brands to recommend to a patient, including lens materials, ocular technologies, and replacement frequencies. The goal of your recommendation is to best meet the needs of your patient as well as the needs of your practice; but, another factor sometimes gets in the way of your top choice: cost. That’s why Alcon continues to
pioneer support programs like the Alcon AIR OPTIX® Choice Program—to allow your patients to save on Alcon’s monthly replacement contact lenses.
The Alcon AIR OPTIX® Choice Program is intended to help your 2-week replacement lens wearers upgrade to a monthly replacement contact lens option within the AIR OPTIX® family of contact lenses—so you can continue to help your patients see, look and feel their best with up to $100 savings on their first annual supply.* Patients can sign up for the Alcon AIR OPTIX® Choice Program and access program benefits at AIROPTIXCHOICE.com. Your Alcon sales representative can also provide you with Point-of-Purchase (POP) materials to help promote the AIR OPTIX® Choice Program to your patients.
The Alcon AIR OPTIX® Choice Program offers savings that significantly reduce the retail price of a 6-month or 1-year supply of AIR OPTIX® contact lenses. Patients new to the AIR OPTIX® family of contact lenses or patients switching within the AIR OPTIX® family (excluding AIR OPTIX® AQUA lenses) can save $100 on an annual purchase or $40 on a semi-annual purchase of eligible AIR OPTIX® contact lenses, via mail-in or online rebate. Current AIR OPTIX® wearers who re-purchase a supply of the same lens may qualify for a $60 savings on an annual supply via mail-in (or online) rebate and a $25 savings on a semi-annual supply purchase via mail-in (or online) rebate through Alcon’s Family Rebate offer. Purchases of AIR OPTIX® AQUA contact lenses do not qualify for the Alcon AIR OPTIX® Choice Program or the Alcon Family Rebate; consider upgrading your AIR OPTIX® AQUA patients to AIR OPTIX® plus HydraGlyde contact lenses where they can save up to $100* and benefit from long-lasting lens surface moisture.3-6
ADVERTORIAL
THE IMPORTANCE OF
SmartShield® Technology delivers consistent comfort from Day 1 to Day 303,4
A consistently comfortable lens with lasting lens surface moisture5-8
The #1 eye doctor recommended contact lens for patients who sleep in their contact lenses9
PRECISION BALANCE 8/4™ lens design that provides outstanding stability for astigmatic patients
A multifocal lens with Precision Profile™ Design that provides seamless vision, near through far
A naturally beautiful lens that enhances eye color with 3-in-1 color technology
ent vs 2-week The Alcon
astigmatic patients
thl l
their contact lenses
t AIR OPTIX®XX Choice Prog
on, near through far
AIR
visio
gram offers savings thatoffice visits was shorter withith

APRIL 2017 | 34 Point-of-care testing
cant expertise, takes considerable time, and
necessitates large volume samples of tears.7
In 2009, OcuSense, Inc. received FDA clear-
ance for the TearLab Osmolarity System, a
tear osmometer that determines osmolarity
values via electrical impedance of tears.9 This
‘‘lab-on-a-chip’’ technology requires a tear
sample of approximately 50 nanoliters (nL)
to measure osmolarity, and I have found the
instrument to be effective and easy use.
To put the required sample size into per-
spective, a nanoliter is one billionth of a liter.
The older freezing point technique required
nearly 500 to 1,000 times the volume used
by the TearLab system.10
Homeostasis and dry eyeHomeostasis is the process by which biologi-
cal systems maintain stability in order to
survive. Diabetes is good systemic example
of failure to maintain homeostasis. When
the endocrine system fails to maintain blood
glucose levels with a normal range of values,
disease and damage result.11
DED can be thought of as a failure of the
LFU to maintain homeostasis.5
Failure to maintain normal TO is a com-
mon and diagnostic feature of evaporative
dry eye disease (EDED), aqueous deficiency
dry eye (ADDE), or most commonly a combi-
nation of the two.3 In dry eye states, regard-
less of the type, TO is frequently elevated or
asymmetric between the eyes, and the dis-
parity increases with severity of the DED.5,12
Incorporating osmolarityBefore I used TearLab in my practice, I was
confident in my ability to diagnose DED. As
I gained experience in DED management, I
realized that in relying on biomicroscopic
evaluation, Schirmer strips (now over 100
years old), vital dye staining, and other tests,
I missed many patients who had DED. Tear-
Lab provided a true biomarker utilizing a lab
test in my own office. It changed the way I
diagnose and manage DED.
Older techniques still have value, but they
are much less consistent and accurate than
obtaining osmolarity values.13 We now real-
ize that corneal and conjunctival staining,
which are often used as markers to initiate
treatment, occur late in the DED process.12
Using staining alone as an indication for ini-
tiating dry eye therapy may result in delayed
treatment for the majority of dry eye patients.
Because TearLab is a lab test, your office
will be considered as such and a Clinical
Laboratory Improvement Act (CLIA)-waived
category license is required. The process is
straightforward. Plus, once you obtain a li-
cense, it is typically good for two years and
allows other CLIA-waived tests to be per-
formed at your point-of-care clinic.
You will be required to perform several
steps to ensure quality control. They are able
to be conducted by office staff, and they are
essential to ensure your that patients are get-
ting precise readings. This is a small price
to pay for having the access to lab tests per-
formed and read in our clinics with quick re-
sults in less than eight seconds per eye and
available while the patient is in the office.
I recommended implementing two steps in
your patient flow protocols to be efficient and
effective in determining which patients re-
ceive the test and how it will be administered.
First, ask your patients to complete a dry
eye-specific questionnaire prior to their exam.
Second, empower technicians to review the
questionnaire based on a protocol that you
establish, then advise patients who fail the
questionnaire that the doctor will want os-
molarity test results available for the exam.
This process allows me to review patients’
TO values and discuss results with them
during my exam. It also promotes office ef-
ficiency and better patient care.
Patients should refrain from using any eye-
drops, including over-the-counter and pre-
scription drops for at least two hours prior
to osmolarity testing. If not, we may obtain
false low readings. The only two exceptions
Tear osmolarityContinued from page 32
If I have a high suspicion of DED, especially with significant intereye difference, retesting TO on subsequent visits may reveal higher values
Figure 2.Using the device is simple to learn and delegate. My techs conduct the test so I have results available to review with the patient during the exam.
2
– Variations in tear stability and osmolarity are at the core of the complex etiologic mechanism of dry eye pathology.
– In non-dry eye individuals, TO ranges 280 to 295 Osml/L (equivalent to normal blood serum osmolarity) and is maintained within a tight range of values in both eyes.
– Intereye difference is a hallmark in DED and is correlated to disease severity.
FDA labeling requires both eyes to be tested; the severity level is based on the higher of the two eyes’ TO value.
Osmolarity testing pearls
See Tear osmolarity on page 36

Find your inspiration
for excellence.
Registration opens April 24, 2017. For more information visit www.aaopt.org
�&72%(5©��g��`©���!© È© �&�250,&.©�/$&(
Find your inspiration for excellence at Academy 2017 Chicago. Join us in Chicago for four days of brilliant speakers, clinically-relevant CE sessions, the latest products and technology in the exhibit hall, captivating papers and posters and cherished social events.

APRIL 2017 | 36 Point-of-care testing
are topical anesthetic drops and/or dilating
drops, which may be used less than two
hours prior to osmolarity testing. Ideally, TO
is the first test administered, even prior to
tonometry or any bright lights, that could
cause significant reflex tearing.
Retest and followPatient education is the foundation of good
care. You may describe dry eye to your pa-
tients as simply having too much salt (sol-
utes) in the tear layer and explain that it
causes some patients to have any number
of symptoms. I explain that our goal is to
reduce that level of abnormal osmolarity.
Remember we are evaluating patients’
risk in the management process. There is
no “magic” number. Patients like to know
their findings and understand their signifi-
cance. A good example is our colleagues in
internal medicine and their long-term model
for cholesterol management. They educate
patients about the risks of hypercholesterol-
emia and benefits of preventive care.
Using the higher of a patient’s two eyes’
values as a starting point allows me to as-
sign a severity range. Typically, mild patients
range 300 to 320; moderate 320 to 340; and
the severe category (only about eight percent
of all dry eye) fall above 340.14
Because the TearLab device ranges from
275 to 400 mOsml/L, I can show each pa-
tient where he falls along a severity scale
and avoid obsessing on an absolute number.
Keep in mind the CV with TearLab is <1.5
percent, which is the equivalent to about
± 4 mOsm/L.
Going back to our cholesterol example, in-
ternists are not concerned about whether a
patient’s total cholesterol is 201 or 198 mg/
dL—rather, they want to know if the patient
is in a mild, moderate, or high risk category
for cardiovascular disease. Once they review
the lab results, they establish a specific goal
of therapy for each patient.
The same holds true for our management
of patients with dry eye disease.
In some cases, patients may present very
early in the process with intereye differences
>8 mOsm/L but still have bilateral TO read-
ings less than 300 mOsml/L; this is the clas-
sic sign of an unstable tear film.
If I have a high suspicion of DED, espe-
cially with significant intereye difference,
retesting TO on subsequent visits may reveal
higher values. Knowing that lab tests are not
about an exact number but rather a range
of values, I do not hesitate to repeat tests.
The caveat is that an intereye difference
>8 mOsm/L is considered to be abnormal.
If patients show normal values on a subse-
quent visit, I follow them over time to ensure
they do not convert to elevated levels of hy-
perosmolarity that are potentially harmful.
Monitoring treatmentOnce you have determined the underlying
etiology of the DED, explained the results to
the patient, and developed a treatment plan,
the next step is monitoring the process. One
additional benefit to tear testing is improved
compliance because patients understand that
you will be repeating this test when they
return. Remind the patient not to use any
drops on the day of the next visit to prevent
unreliable test results.
Avoid the error of bringing the patient
back too soon. A 10 mOsml/L decrease is
considered clinically significant, but some
therapies require at least four to six weeks
before this goal is reached.
In some cases, a patient may return and
despite good compliance have TO values
higher than those obtained on the initial
evaluation. The patient should be advised
this is valuable information because it tells
you her DED is more severe than initially
thought and you will prescribe more aggres-
sive therapy.
In my experience, the patient-doctor edu-
cation made possible by lab tests facilitates
a very high level of patient management.
Dry eye care is one of the most reward-
ing but challenging facets of my practice.
Osmolarity testing has changed my treat-
ment philosophy by providing additional in-
formation to help me diagnose and manage
DED more effectively. In my opinion, many
unsuccessful dry eye treatment plans result
from failing to recognize the true severity of
a patient’s condition and prescribe appropri-
ate therapeutic measures.
REFERENCES1. Bartlett JD, Keith MS, Sudharshan L, Snedecor SJ. Associations between signs and symptoms of dry eye disease: a systematic review. Clin Ophthalmol. 2015 Sep 16;9:1719-1730.
2. Barabino S, et al. Understanding symptoms and quality of life in patients with dry eye syndrome. Ocul
Surf. 2016 Jul;14(3):365-376.
3. The Definition and Classification of Dry Eye Disease: Report of the Definition and Classification Subcommittee of the International Dry Eye WorkShop (2007). Ocul Surf. 2007 Apr;5(2):75-92.
4. Stern ME, et al. The role of the lacrimal functional unit in the pathophysiology of dry eye. Exp Eye Res. 2004 Mar;78(3):409-416.
5. Bron AJ, Tomlinson A, Foulks GN, Pepose JS, Baudouin C, Geerling G, Nichols KK, Lemp MA. Rethinking dry eye disease: a perspective on clinical implications. Ocul Surf. 2014 Apr;12(2 Suppl):S1-31.
6. Farris RL, Stuchell RN, Mandel ID. Basal and reflex human tear analysis. I. Physical measurements: osmolarity, basal volumes, and reflex flow rate. Ophthalmology. 1981 Aug;88(8):852-857.
7. Tomlinson A, McCann LC, Pearce EI. Comparison of human tear film osmolarity measured by electrical impedance and freezing point depression techniques. Cornea. 2010 Sep;29(9):1036-1041.
8. Gilbard JP, Farris RL. Ocular surface drying and tear film osmolarity in thyroid eye disease. Acta
Ophthalmol (Copenh). 1983 Feb;61(1):108-116.
9. Jacobi C, Jacobi A, Kruse FE, Cursiefen C. Tear film osmolarity measurements in dry eye disease using electrical impedance technology. Cornea. 2011 Dec;30(12):1289-1292.
10. Zarbin MA, Montemagno C, Leary JF, Ritch R. Nanotechnology in ophthalmology. Can J Ophthalmol. 2010 Oct;45(5):457-476.
11. Holst JJ, Gribble F, Horowitz M, Rayner CK. Roles of the Gut in Glucose Homeostasis. Diabetes Care. 2016 Jun;39(6):884-892.
12. Lemp MA, Bron AJ, Baudouin C, Benítez Del Castillo JM, Geffen D, Tauber J, Foulks GN, Pepose JS, Sullivan BD. Tear osmolarity in the diagnosis and management of dry eye disease. Am J Ophthalmol. 2011 May;151(5):792-798.e1.
13. Versura P, Profazio V, Campos EC. Performance of tear osmolarity compared to previous diagnostic tests for dry eye diseases. Curr Eye Res. 2010 Jul;35(7):553-564.
14. Potvin R, Makari S, Rapuano CJ. Tear film osmolarity and dry eye disease: a review of the literature. Clin Ophthalmol. 2015 Nov 2;9:2039-3047.
Dr. Townsend is an adjunct professor at the University of Houston College of Optometry and preceptor for senior externs who rotate through his practice. He conducts research in pharmaceutical agents, contact lens materials and solutions, and ocular surface disease and serves on the advisory board and conducts research for TearLab. When not seeing patients, Dr. Townsend enjoys splitting wood at his cabin in New Mexico.
Tear osmolarityContinued from page 34
Osmolarity testing has changed my treatment philosophy by providing additional information to help me diagnose and manage DED more effectively

APRIL 2017 / OptometryTimes.com MarketplaceMarketplace 37
CAREERS
CONNECTICUTNATIONAL
ALLDocs (The Association of
LensCrafters Leaseholding Doctors)
has dozens of OD job opportunities.
One of the nation’s leading
optometry organizations, ALLDocs
members hire only the finest ODs,
and provide cutting-edge
technology with tremendous
growth opportunities.
Optometry Jobs Nationwide
Visit
https://www.alldocsod.com/jobs/
for the job listings.
Email [email protected] | Call 860-442-1466 | Visit www.ronaldmedwickod.com
Optometric Associates, P.C. is looking to hire an Optometrist. We are a well-established practice in Waterford, Connecticut. Waterford is a beautiful coastal community, that is located between Boston and New York!
We are very excited to be adding an OD to our team! If you are ready for a change of pace and want to live at the beach, then apply today!
Benefits include
Competitive Salary Health Insurance No Weekends Paid Vacations
We have been providing eye care to the community for over 40 years. The practice has maintained a high level of care by utilizing cutting edge technology, both clinically and in practice management.
This position is open to a well-qualified doctor who is looking for a full time position, with the possibility of practice purchase in the near future!
Acuity Pro Vision Science Software 6
Aerie Pharmaceuticals, Inc. 11
Alcon Laboratories Inc CVTIP, CV4 Tel: 800-862-5266Web: www.alcon.com
American Academy Of Optometry 35
Bausch And Lomb 9, 27
Beaver Visitec International 17
Cooper Vision CV2 Web: www.coopervision.com
Marco Ophthalmic Inc 5
Mibo Medical Group 15Tel: 214-507-8091
Novabay Pharmaceuticals CV3
Novartis Ophthalmics 23, 24
Oculus Inc 31
Ocusoft 25
Shire Ophthalmic 7, 19-20Tel: 415-971-4650
TTI Medical 13Tel: 4800-322-7373Web: www.ttimedical.com
This index is provided as an additional service. The publisher does not assume any liability for errors or omissions.
Advertisers IndexAdvertiser Page
Optometrists and allied
eye care professionals.
Contact me today to
place your ad.
Reach your target audience.
Our
audience.
Tamara PhillipsAccount Manager
440-891-2773
Place a recruitment ad in
Optometry Times—
in print or online.
Joanna ShippoliAccount Manager
440-891-2615
Narrow your candidate
search to the best.

APRIL 2017 | 38 A&Q
boards of kids’ frames—we’ve
got five times that. We have
such a great selection that we
can fit most kids. Our techs
are really good. They’re fast
and efficient, and they do a
wonderful job at making the
kids comfortable. In terms
of clinical stuff, one of the
things that makes us stand
out is our passion for myopia
prevention. All these kids are
coming in, and they’re getting
worse every year. If we can
talk to them about strategies
to slow that down, that’s defi-
nitely something that makes
us unique and is lots of fun.
With both monthly and biweekly contact lenses
available, why a daily dispos-ables-only practice? The ben-
efits with daily disposables
are huge, especially with my
pediatric population. Let’s be
honest, kids are dirtier than
we are. There are a multitude
of valid reasons why these
kids should not be reusing
their contact lenses, even
with the best hygiene. It just
makes a lot of sense for them
to be in daily disposables;
they reduce the risks
so, so much. The pa-
tients enjoy the con-
venience. But the
main purpose is
to reduce the
risk of contact
lens-related
complications.
There’s a huge, huge amount of folks in the Asian population who are myopic. Because we see such a large portion of the myopes in central Indiana who are pediatric, you start looking into ways that you can help people. For my whole career, it’s been glasses and contact lenses, which it still is for the most part, but I can look at world-wide trends and ask how I can help my little piece of the world not become so myopic and learn more and do bet-ter for them. We do our part in myopia preven-tion from Indianapolis.
QQHow did you get involved in the global myopia
problem?
What three things would you advise new ODs who
want to go into pediatric op-tometry? Have the right mo-
tivation. [Laughs] It’s not an
easy task. And know your
own personality, make sure
you can make that work
with kids. I know clinically
I can make kids feel at ease
and do my job quickly and
professionally so that I can
be a good doctor for chil-
dren and make it fun. Num-
ber two: Surround yourself
with staff who can do it. We
went through staff at the be-
ginning who are great tech-
nicians and opticians, but
they’re not meant to work
with kids. The third thing
would be to be brave and
just go for it because it’s not
an easy niche of optometry.
People are looking for it, but
it’s not selling $700 frames.
It’s completely different from
a vision therapy practice or a
primary-care practice.
What do you do for downtime? I really
enjoy my family, of course.
I have two kids, so we enjoy
lots of things with their
sports and activities. I like
to work out, read, and have
a good nap. If I can get those
three things on a regular
basis, I am a happy camper.
What was the biggest challenge starting up
Little Eyes, and how did you meet it? Awareness. People
don’t think about preventa-
tive care for their kids. They
think about, “Oh, my kid
complained that the board is
blurry, so I’m going to bring
him in to the eye doctor.”
Our marketing campaign fo-
cuses on letting people know
that preventative eye care
is just as important as your
yearly checkup at the pedia-
trician or your twice a year
visit to the dentist. The pub-
lic awareness has been huge.
The real boost in awareness
has been schools, pediatri-
cians, and day cares.
What do you consider Lit-tle Eye’s best practices?
An incredible dispensary;
our optician is wonderful.
We have a lot of outside Rxs
come to us because we have
a huge selection of frames.
Most offices have one or two
Pediatric optometry, daily disposables, and nappingKatherine Schuetz, OD Optometrist at Little Eyes, Carmel, IN
Phot
o co
urte
sy K
athe
rine
Schu
etz,
OD
Why did you add ortho-keratology, and how has
it changed your practice? We
added it because we knew
the need was there in terms
of myopia prevention. We
also have a ripe practice pop-
ulation for ortho-k. It’s kids
who are getting worse, we’re
trying to slow that down,
and they’re motivated to try
other things. I had referred a
few patients out over the first
couple of years to a colleague
locally, and I thought, “This
is crazy, I need to learn or-
tho-k, I need to become an
expert and offer it to my pa-
tients.” And that’s what we
did.
—Vernon Trollinger
To hear the full interview with
Katherine Schuetz, listen online:
optometrytimes.com/KatherineSchuetz

AV E N O VA . C O M | � � � � � � � � � � � � | R X O N LY
Daily lid and lash hygiene.
Avenova.The essential part of
any lid hygiene regimen.
Antibiotic and resistance free Avenova
with Neutrox®. The one no-sting solution
that helps manage the itchy, burning,
irritated eyelids often caused by blepharitis,
MGD and dry eye. Used alone or
concomitantly, Avenova is the essential
part of any lid and lash hygiene regimen.
Avenova. Every day.
Avenova contains Neutrox, a proprietary pure hypochlorous acid that mimics the body’s immune response. It works without creating mammalian cell toxicity
or bacterial resistance. It’s well tolerated for daily use.
BRUSH. FLOSS. AVENOVA®.
Visit NovaBay at Vision Source Exchange – Booth #235

-10.00D+6.00DWATER CONTENT (%)
PERFORMANCE DRIVEN BY SCIENCE®
See product instructions for complete wear, care and safety information.
© 2016 Novartis 9/16 US-DTM-16-E-3722
Ask your Alcon representative for details
how these revolutionary lenses may be able
to help your presbyopic patients see clearly.
WATER GRADIENT TECHNOLOGY MEETS
PRECISION PROFILETM DESIGN
DAILIES TOTAL1® Multifocal contact lenses
UNIQUE WATER
GRADIENT
TECHNOLOGY
0.25 steps
LO MED HI
ADDs