Embed Size (px)
Citation preview

The presence of amyloid in abdominal and oral mucosal tissuesin patients initially diagnosed with multiple myeloma:a pilot studyEric T. Stoopler, DMD,a Dan T. Vogl, MD,b Faizan Alawi, DDS,c Martin S. Greenberg, DDS,d
Thomas P. Sollecito, DMD,d German Salazar, DMD,e and Edward A. Stadtmauer, MD,f
Philadelphia, PAUNIVERSITY OF PENNSYLVANIA SCHOOL OF DENTAL MEDICINE AND UNIVERSITY OFPENNSYLVANIA SCHOOL OF MEDICINE
Objectives. The aims of this study were to (1) determine the feasibility of tandem assessment of the presence ofamyloid in subcutaneous abdominal fat by fine-needle aspiration and oral mucosal tissue biopsy in patients initiallydiagnosed with multiple myeloma (MM) and (2) determine the optimal site for detection of amyloid in the oral cavity(tongue compared with labial minor salivary glands) in the same cohort of patients.Study design. A prospective, cross-sectional study was performed on patients with newly diagnosed MM. Subjectscompleted an abdominal fat pad aspirate and biopsies of both the tongue and labial minor salivary glands (LMSGs).All specimens were analyzed for presence of amyloid via standard techniques.Results. Eleven subjects completed the protocol. Amyloid was not detected in any abdominal fat pad specimens.Amyloid was not detected in any tongue specimens; however, 2 subjects demonstrated amyloid deposition in LMSGs.Neither of these subjects demonstrated evidence of systemic amyloidosis or recurrence of MM at least 3 years aftercompleting the study protocol.Conclusions. The results of this study suggest that the labial minor salivary glands may be the optimal site to detectamyloid in patients with newly diagnosed MM. Additional studies are warranted to determine if amyloid in the LMSGs
represents a high-risk prognostic factor for MM. (Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2011;111:326-332)Multiple myeloma (MM) is characterized by the pro-liferation of malignant plasma cells derived from asingle clone in the bone marrow and accounts for 13%of all hematologic cancers.1,2 The frequency of MM in theUS population is twice as high among African Americans
Portions of this research were presented at the 62nd Annual Meeting,American Academy of Oral Medicine, Scottsdale, AZ, 2008, andpublished as an abstract in Oral Surg Oral Med Oral Pathol OralRadiol Endod 2008;106:e7-8.Supported by a Senior Research Grant from the Multiple MyelomaResearch Foundation (MMRF).aAssistant Professor, Department of Oral Medicine, University ofPennsylvania School of Dental Medicine.bAssistant Professor, Department of Medicine, University of Penn-sylvania School of Medicine.cAssistant Professor, Department of Pathology, University of Penn-sylvania School of Dental Medicine.dProfessor, Department of Oral Medicine, University of PennsylvaniaSchool of Dental Medicine.eAssistant Professor, Department of Graduate Education, School ofDental Medicine, University of Puerto Rico, San Juan, PR.fProfessor, Department of Medicine, University of PennsylvaniaSchool of Medicine.Received for publication Sep 27, 2010; returned for revision Oct 19,2010; accepted for publication Oct 27, 2010.1079-2104/$ - see front matter© 2011 Mosby, Inc. All rights reserved.
doi:10.1016/j.tripleo.2010.10.028326
compared with whites with the median age of diagnosis inthe early sixth decade.1-4 Common presenting clinicalfeatures of MM are bone pain and pathologic fracturesecondary to lytic lesions, renal failure, fatigue second-ary to anemia, and recurrent infections.5 Treatment ofMM primarily consists of corticosteroid administration,high-dose chemotherapy, and autologous stem celltransplantation (ASCT).6 Newer immunomodulatorydrugs, such as thalidomide, lenalidomide, and bort-ezomib, have played a critical role in successfully treat-ing both newly diagnosed and relapsed MM.7 The useof high-potency intravenous bisphosphonates, such aspamidronate and zolendronate, has provided consider-able symptomatic relief of bone pain to patients withMM; however, many reports have implicated thesemedications in causing osteonecrosis of the jaw.8-15
Many factors are considered when determining appropri-ate therapy for MM, including patient age, presence ofcomorbidities, presence of disease-related complications, el-igibility for ASCT, patient choice, and disease-related fac-tors, such as presence of cytogenetic abnormalities.16-18
The median survival of patients with MM averages 3 to 5years dependent on type of clinical treatment and responseto therapy; however, overall survival duration ranges fromless than 1 year to more than 10 years owing to disease
heterogeneity.5 One potential source of variability in out-
OOOOEVolume 111, Number 3 Stoopler et al. 327
comes is comorbidity owing to the presence of occultamyloid deposition.
Amyloid is an otherwise normal protein that formsinsoluble fibrils in certain disease states.19 It consists ofrigid, nonbranching fibrils that range in width from 7.0to 12.0 nm, with each fibril composed of �-pleatedsheets that twist, giving amyloid its characteristiccross-� spine evident on x-ray diffraction.19 Amyloidprecursor proteins vary, but the most common is themonoclonal immunoglobulin light chain that causesamyloid light chain (AL) amyloidosis; this is related toan underlying monoclonal plasma cell proliferation,similar to that seen in MM.
AL amyloidosis is a well-recognized complication ofMM.20 Clinically, occult AL amyloid occurs in up to38% of patients with MM,21 whereas 3% to 7% ofpatients with MM have overt organ dysfunction owingto deposition of AL amyloid.22 AL amyloidosis canresult in damage to the kidneys, heart, gastrointestinaltract, liver, spleen, and peripheral and autonomic ner-vous system.23 Life-threatening illnesses caused by am-yloid deposition include nephrotic syndrome, renal fail-ure, cardiac failure, arrhythmias, hepatosplenomegaly,malabsorption, hemorrhage, and infarction.24
Search for amyloidosis is initiated on the basis of clin-ical suspicion; a tissue biopsy is used to establish a defin-itive diagnosis.25 The sampling of subcutaneous abdomi-nal fat has been advocated for diagnosis of amyloid,26,27
with 85% of patients demonstrating amyloid depositionwith this technique.28 Historically, other biopsy sites thathave been reported to have a high predictive value fordetection of amyloid include the kidney and the rec-tum.20,29-34 In the absence of clinical symptoms, oraltissues have been advocated for use in biopsy to detectamyloid deposition; however, the site of biopsy has beencontroversial. Oral biopsy sites that have demonstratedpresence of amyloid are numerous, including the gingiva,palate, parotid gland, and buccal mucosa25,35-45; however,the tongue and labial minor salivary glands (LMSGs)have been consistently reported as the most commonintraoral sites of amyloid deposition.46-52
The aims of this pilot study were to (1) determine thefeasibility of tandem assessment of the presence of amy-loid in subcutaneous abdominal fat by fine-needle aspira-tion and oral mucosal tissue biopsy in patients with newlydiagnosed MM and (2) determine the optimal site fordetection of amyloid in the oral cavity (tongue comparedwith LMSGs) in the same cohort of patients.
MATERIALS AND METHODSStudy population
Patients with newly diagnosed MM (defined as �6months from the start of myeloma therapy and not yet
received a peripheral stem cell transplant) who were notpreviously diagnosed with amyloidosis were eligible toparticipate in this study. Subjects with a previous diag-nosis of amyloidosis before diagnosis of MM were ex-cluded from the study. There were no inclusion/exclusioncriteria based on age, gender, race, or ethnicity.
Study designThis was a prospective, cross-sectional study ap-
proved by the institutional review board (IRB) of theUniversity of Pennsylvania and the Clinical Trials Sci-entific Review Monitoring Committee of the AbramsonCancer Center (ACC) of the University of PennsylvaniaHealth System. Subjects were identified and recruited,in accordance with the inclusion/exclusion criteria,from the ACC by several coinvestigators (E.A.S.,D.T.V., G.S.). The protocol was described and if will-ing to participate, the subject was presented with anIRB approved Informed Consent Document andHIPAA Document, which were reviewed in detail andsigned by the subject and investigator(s). The subjectwas referred to the Division of Oral Medicine forconduct of the protocol by a board certified specialist inoral medicine (E.T.S., M.S.G., T.P.S.). After reviewingthe subject’s medical history and laboratory values, aclinical examination was completed and the subjectunderwent 2 biopsies of clinically normal-appearingtissue in the oral cavity under local anesthesia (2%lidocaine with 1:100,000 epinephrine). Specimen 1 wastaken from the left lateral surface of the tongue, con-taining mucosal and muscle tissue. Specimen 2 wastaken from the labial mucosa on the left side of thelower lip, containing at least 2 to 3 minor salivaryglands. Both specimens were formalin fixed and sent toa board-certified oral and maxillofacial pathologist(F.A.) at the Hospital of the University of Pennsylvania(HUP), for histopathologic evaluation for amyloid.Analysis consisted of reviewing each specimen withboth hematoxylin and eosin and Congo red stains. Thespecimens demonstrating amyloid displayed character-istic apple-green birefringence when viewed under po-larized light.
After the oral tissue biopsies were completed, thesubject underwent a subcutaneous abdominal fat biopsyvia fine-needle aspiration (FNA) in the dental operatoryby the cytopathology service at HUP. This aspirate wasanalyzed for presence of amyloid via Congo red stain-ing performed with proper controls.
Upon the completion of the abdominal fat biopsy, thesubject was dismissed and given an appointment toreturn to the Division of Oral Medicine in 1 week forfollow-up evaluation. Subjects undergoing active treat-ment for MM were scheduled for follow-up with thetreating oncologist (E.A.S., D.T.V.) as per their recom-
mendations.
OOOOE328 Stoopler et al. March 2011
Statistical methodsA 95% exact Clopper-Pearson confidence interval
was computed for the prevalence of amyloid deposition inthe abdominal fat, tongue, and LMSGs. To test equality ofprevalences of amyloid deposition in oral tissue and ab-dominal fat, an exact McNemar test was used.
RESULTSThis pilot study enrolled 13 subjects during a 3-year
period (2006 to 2008). Two subjects withdrew beforeinitiating the protocol; therefore, analysis of biopsyspecimens was completed on 11 patients (Table I).Subject demographics (of those who completed theprotocol) are as follows: 8 males and 3 females, 8whites and 3 African Americans, mean age 61.5 years(range of 44 to 71 years). All subjects who participatedin the study were classified as Stage 1 MM according tothe International Staging System. Fluorescence in situhybridization and cytogenetic testing were not standardpractice at our institution at the time of this study andwere therefore not done. Systemic therapy for myelomaat the time of study biopsies was thalidomide/dexa-methasone in 5 patients, lenalidomide/dexamethasonein 2 patients, bortezomib/dexamethasone in 1 patient,dexamethasone alone in 1 patient, and no prior sys-temic therapy in 2 patients; 3 patients had receivedlocal radiation. Amyloid was not detected in any ab-dominal fat specimens. In addition, amyloid was notobserved in any tongue specimens from the cohort;however, 2 subjects (05 and 08) demonstrated amyloiddeposition in the LMSGs only (Fig. 1, A-D).
A further objective was to calculate a McNemar’stest of the null hypothesis that the prevalence of depo-sition was the same in both oral and abdominal tissues.Because all tests for amyloid deposition in the tongueand abdominal fat were negative, the McNemar statistic for
Table I. Demographic and histologic characteristics o
Subject Sex Race Age, y
01 Male African American 6402 Male African American 4403 Male White 6904 Male White 6605 Female White 6406 Male White 5607 Male White 6108 Male White 4409 Male African American 6910 Male White 7111 Female White 6512 Female White 6913 Female White 60
this comparison was undefined. For the comparison of prev-
alences in LMSGs and abdominal fat, the McNemar test wasnot significant (P � .5).
The 2 subjects positive for LMSG amyloid deposi-tion had both received thalidomide and dexamethasonetherapy before their oral biopsies. Both went on toreceive further therapy with high-dose cyclophosph-amide, peripheral blood hematopoietic stem cell collec-tion, and then high-dose melphalan with ASCT. One ofthe 2 patients had evidence of myeloma progressionapproximately 1 year after ASCT and has requiredongoing further therapy; the other patient has no evi-dence of disease recurrence. With more than 3 years offollow-up, neither has demonstrated any signs or symp-toms of systemic amyloidosis.
DISCUSSIONDiagnosis, staging, and risk stratification for patients
with newly diagnosed MM is continuously evolving.Currently, MM is diagnosed in accordance with theInternational Myeloma Working Group Criteria, with 3major categories based on specific clinical, laboratory,and histopathologic findings: monoclonal gammopathyof unknown significance (MGUS), smoldering MM(SMM), and MM (active or symptomatic) (TableII).1,53,54 It is recommended that therapy should beinitiated only for symptomatic disease.7,53,54 The Du-rie-Salmon staging system uses calcium and hemoglo-bin levels, presence of lytic bone lesions, and amountsof monoclonal protein to stage MM55 and was usedprimarily until 2005, when the International StagingSystem (ISS) was widely adapted (Table III).18,56 TheISS uses 2 markers, albumin and �2 microglobulin, tostage MM and provides useful information regardingbiological characteristics of the disease and progno-sis.18 The updated Mayo Stratification of Myeloma andRisk-Adapted Therapy (mSMART) Consensus Guide-
tudy populationAmyloid in
abdominal fatAmyloid in
tongueAmyloid in labial
minor salivary glands
Not present Not present Not presentNot present Not present Not presentNot present Not present Not presentNot present Not present Not presentNot present Not present PresentNot present Not present Not presentWithdrawn Withdrawn WithdrawnNot present Not present PresentNot present Not present Not presentNot present Not present Not presentWithdrawn Withdrawn WithdrawnNot present Not present Not presentNot present Not present Not present
f the s
lines recommends that all MM patients undergo fluo-

the sa
OOOOEVolume 111, Number 3 Stoopler et al. 329
rescent in situ hybridization (FISH), metaphase cyto-genetics, and when feasible, plasma cell labeling index(PCLI) for risk stratification as standard risk (75% ofcases) versus high risk (25% of cases).7 FISH andcytogenetic abnormalities are generally associated witha more proliferative myeloma and increase likelihoodof a poor treatment outcome.18 Presence of deletion 13(del 13), t(4:14), t(14:16), del 17p, and hypodiploidyare associated with significantly shorter overall survivaland duration of response.7,18,57 PCLI measures plasmacell proliferative rate; typically plasma cells have a lowrate of proliferation with a PCLI index of less than 1%.7
Studies have shown the prognostic value of an elevatedPCLI in MM58,59 and the mSMART Consensus Guide-lines have established a PCLI of 3% or more to cate-gorize high-risk MM patients.7 The use of these tech-niques has greatly affected clinical treatment algorithmsfor patients with MM based on their risk, specifically as itrelates to selection and implementation of therapeuticagents as well as timing and number of ASCT proce-
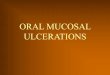
Fig. 1. A, Abdominal fat pad aspirate negative for amyloiddemonstrating amorphous and relatively acellular material a�100 magnification). C, Congo red stain viewed under whitefocally within the salivary gland lobule (�100 magnificatiopresence of diffuse amyloid deposits (green material) within
dures.7
A recent study has suggested AL amyloidosis asso-ciated with MM as an independent high-risk prognosticfactor and presence of amyloid may confer a poordisease prognosis.60 This study evaluated 201 patientswith MM for presence of AL amyloid via FNA sam-pling of periumbilical abdominal fat analyzed viaCongo red stain. Sixty-eight patients (34%) demon-strated presence of AL amyloid and during long-termfollow-up; 69% of these patients ultimately developedsymptoms of systemic amyloidosis. The patients withMM associated AL amyloidosis in this study demon-strated higher frequency of positive disease markers(Bence Jones proteinuria, anemia, hypercalcemia, in-creased serum alkaline phosphatase, decreased serumalbumin, increased serum lactate dehydrogenase [LDH]levels) and demonstrated a poorer response to chemo-therapy compared with the group without AL amyloid-osis. A previous study also supported the theory thatMM patients with coexisting AL amyloid may have apoorer prognosis as compared with patients without AL
o red stain, �63 magnification). B, LMSG biopsy speciment to the salivary gland lobule (Hematoxylin and eosin stain,emonstrates amyloid (orange color) primarily adjacent to andCongo red stain viewed under polarized light confirms thelivary gland tissue (�100 magnification).
(Congdjacenlight dn). D,
amyloid present.61 Some authors have advocated man-

OOOOE330 Stoopler et al. March 2011
datory fat pad analysis for amyloid in patients withMM,60 whereas others suggest that the clinical andtherapeutic value of a positive result appears to beinconsequential.21 The results of our pilot study dem-onstrate that the prevalence of occult amyloid deposi-tion in patients with myeloma may be even higher. Inour limited size sample, none of the patients had de-tectable amyloid deposition on FNA of the abdominal fatpad. However, we were able to detect amyloid depositionin labial minor salivary glands in 2 (18%) of 11 patients.This suggests that subclinical amyloid deposition may bemore easily detected on oral biopsy, and the oral cavitymay be the preferred biopsy site for detecting amyloiddeposition in myeloma patients with no symptoms ofsystemic amyloidosis.
As stated previously, various locations within theoral cavity have been advocated for biopsy to detectamyloid. Historically, the tongue is the most frequentlyreported intraoral location for amyloid deposition andhas been advocated as the optimal site for biopsy withinthe oral cavity for detection of amyloid.39,47,50-52,62
More recently, various studies have demonstrated theutility of LMSG biopsy for the detection of amyloidwith correlation to primary and secondary systemicamyloidosis.46,48,49,63-65 In our study, amyloid was de-tected only in the LMSGs; these results further supportthe concept that the LMSGs may be the optimal site for
Table II. Criteria for the diagnosis of multiple my-eloma and related disordersSymptomatic multiple myeloma (all are required):
1. Clonal plasma cells present on biopsy of bone marrow orplasmacytoma
2. M-protein present in serum or urine (either intactimmunoglobulin or free light chains)
3. Evidence of related organ or tissue impairment (lytic bonelesions, renal insufficiency, anemia, hypercalcemia,hyperviscosity, amyloidosis, or recurrent infections)
Asymptomatic (smoldering) myeloma:1. Serum M-protein �3 g/dL and/or clonal plasma cells � 10%
of bone marrow2. No symptoms or evidence of related organ or tissue
impairmentMonoclonal gammopathy of unknown significance (MGUS)
1. Serum M-protein present but �3 g/dL2. Bone marrow plasma cells � 10% of aspirate and low level
of infiltration on biopsy3. No symptoms or evidence of related organ or tissue impairment
Adapted from The International Myeloma Working Group. Criteriafor the classification of monoclonal gammopathies, multiple my-eloma and related disorders: a report of the International MyelomaWorking Group. Br J Haematol 2003;121:749-57.Reprinted from Stoopler ET, Vogl DT, Stadtmauer EA. Medical man-agement update: multiple myeloma. Oral Surg Oral Med Oral PatholOral Radiol Endod 2007;103:599-609; with permission from Elsevier.
intraoral biopsy for early detection of amyloid.
There were limitations of this study that may haveaffected research outcomes. The sample size of thestudy was small and may not accurately represent thetrue prevalence of amyloid deposition in this patientpopulation. Although each operator performing the pro-cedures was standardized, biopsy techniques are oper-ator and patient sensitive and may not have been con-sistent. Most patients enrolled had already receivedsome form of treatment for MM—this could have po-tentially affected the overall course of disease as well asamyloid burden. Subjects did not complete FISH andcytogenetic testing and, therefore, it was not knownwhether these subjects were considered standard- ver-sus high risk-patients. Although 2 of 11 subjects dem-onstrated amyloid in the oral cavity without evidence ofdeposition in the abdominal fat, the clinical significance
Table III. Staging system for multiple myelomaDurie-Salmon Stage I (associated with a low cell mass of
�0.6 � 1012 cells/m2):All of the following are required:● Hemoglobin �10 g/dL● Low serum monoclonal protein (IgG �5 g/dL
or IgA �3 g/dL)● Normal serum calcium level● Low urinary monoclonal protein excretion
(�4 g/24 hours)● Absence of lytic bone lesionsStage II Any patient not meeting criteria for
Stages I or IIIStage III (associated with a high cell mass of
�1.2 � 1012 cells/m2):At least one of the following is required:● Hemoglobin �8.5 g/dL● High serum monoclonal protein (IgG �7 or
IgA �5)● Serum calcium � 12 mg/dL● High urinary monoclonal protein excretion
(�12 g/24 hours)● Advanced lytic bone lesions (usually �3
lesions)International
stagingsystem
Stage I: serum albumin � 3.5 g/dL and serum�2-microglobulin � 3.5 mg/L
Stage II: serum albumin � 3.5 g/dL or�2-microglobulin 3.5 to 5.5 mg/L
Stage III: �2-microglobulin � 5.5 mg/L
IG, immunoglobulin.Adapted from Durie BG, Salmon SE. A clinical staging system formultiple myeloma: correlation of measured myeloma cell mass withpresenting features, response to treatment and survival. Cancer 1975;36:842-54.Adapted from Greipp PR, Miguel JS, Durie BG, Crowley JJ, BarlogieB, Blade J, et al. International staging system for multiple myeloma.J Clin Oncol 2005;23:3412-20.Reprinted from Stoopler ET, Vogl DT, Stadtmauer EA. Medical man-agement update: multiple myeloma. Oral Surg Oral Med Oral PatholOral Radiol Endod 2007;103:599-609; with permission from Elsevier.
of these findings remains unclear, as neither has devel-

OOOOEVolume 111, Number 3 Stoopler et al. 331
oped signs or symptoms of systemic amyloidosis. Am-yloidosis has been generally recognized as a long-termcomplication of MM.45 The 2 subjects reported herewith occult amyloidosis received active treatment,which caused disease remission and this may decreasethe risk of late development of amyloid-related organdysfunction. The amyloid detected in the LMSG biop-sies was not analyzed for type; however, there is a highprobability that it was of AL type because of (1) theconcurrent myeloma disease process and (2) neither ofthese subjects had a history of chronic infectious, in-flammatory, or neoplastic diseases responsible for pro-duction of other types of amyloid.
CONCLUSIONSThe results of this study support the oral cavity as an
important location for diagnostic testing for presence ofamyloid in patients with MM. Specifically, this pilotstudy demonstrates the value of LMSG biopsy as amore reliable intraoral location for detection of amyloidas compared with other anatomical locations in the oralcavity. Additional studies are warranted to further supportLMSG biopsy as a potential site for establishing presenceof amyloid early in the MM disease process and to vali-date previous studies that the presence of amyloid may bean independent high-risk factor for MM.
The authors thank and acknowledge Dr Prabodh Guptaand the cytopathology team at the University of PennsylvaniaMedical Center for services provided. The authors also thankand acknowledge Dr Daniel Heitjan in the Department ofBiostatistics and Epidemiology at the University of Penn-sylvania School of Medicine for statistical design and analysiscompleted for this study.
REFERENCES1. Raab MS, Podar K, Breitkreutz I, Richardson PG, Anderson KC.
Multiple myeloma. Lancet 2009;374:324-39.2. Rajkumar SV. Multiple myeloma. Curr Probl Cancer 2009;
33:7-64.3. Landgren O, Gridley G, Turesson I, Caporaso NE, Goldin LR,
Baris D, et al. Risk of monoclonal gammopathy of undeterminedsignificance (MG, US) and subsequent multiple myeloma amongAfrican American and white veterans in the United States. Blood2006;107:904-6.
4. Landgren O, Weiss BM. Patterns of monoclonal gammopathy ofundetermined significance and multiple myeloma in various eth-nic/racial groups: support for genetic factors in pathogenesis.Leukemia 2009;23:1691-7.
5. Lin P. Plasma cell myeloma. Hematol Oncol Clin North Am2009;23:709-27.
6. Stoopler ET, Vogl DT, Stadtmauer EA. Medical managementupdate: multiple myeloma. Oral Surg Oral Med Oral Pathol OralRadiol Endod 2007;103:599-609.
7. Kumar SK, Mikhael JR, Buadi FK, Dingli D, Dispenzieri A,Fonseca R, et al. Management of newly diagnosed symptomaticmultiple myeloma: updated Mayo stratification of myeloma andrisk-adapted therapy (mSMART) consensus guidelines. Mayo
Clin Proc 2009;84:1095-110.8. Migliorati CA, Schubert MM, Peterson DE, Seneda LM. Bis-phosphonate-associated osteonecrosis of mandibular and maxil-lary bone: an emerging oral complication of supportive cancertherapy. Cancer 2005;104:83-93.
9. Migliorati CA, Siegel MA, Elting LS. Bisphosphonate-associ-ated osteonecrosis: a long-term complication of bisphosphonatetreatment. Lancet Oncol 2006;7:508-14.
10. Sawatari Y, Marx RE. Bisphosphonates and bisphosphonate in-duced osteonecrosis. Oral Maxillofac Surg Clin North Am 2007;19:487-98, v-vi.
11. Grewal VS, Fayans EP. Bisphosphonate-associated osteonecro-sis: a clinician’s reference to patient management. Todays FDA2008;20:38-41, 43-6.
12. Migliorati CA. Intravenous bisphosphonate therapy may lead toosteonecrosis of the jaw in multiple myeloma, breast, and pros-tate cancer patients. J Evid Based Dent Pract 2008;8:93-4.
13. Almazrooa SA, Woo SB. Bisphosphonate and nonbisphospho-nate-associated osteonecrosis of the jaw: a review. J Am DentAssoc 2009;140:864-75.
14. Ruggiero SL, Dodson TB, Assael LA, Landesberg R, Marx RE, Meh-rotra B, et al. Position paper on bisphosphonate-related osteonecrosis ofthe jaws—2009 update. J Oral Maxillofac Surg 2009;67:2-12.
15. Migliorati CA, Woo SB, Hewson I, Barasch A, Elting LS,Spijkervet FK, et al. Bisphosphonate Osteonecrosis Section, OralCare Study Group, multinational association of supportive carein cancer (MASCC)/International Society of Oral Oncology(ISOO). A systematic review of bisphosphonate osteonecrosis(BON) in cancer. Support Care Cancer 2010;18:1099-106.
16. Harousseau JL, Dreyling M, ESMO Guidelines Working Group.Multiple myeloma: ESMO clinical recommendations for diagno-sis, treatment and follow-up. Ann Oncol 2009;20(Suppl 4):97-9.
17. Kumar S. Multiple myeloma—current issues and controversies.Cancer Treat Rev 2010;36(Suppl 2):S3-11.
18. Lonial S. Presentation and risk stratification—improving prog-nosis for patients with multiple myeloma. Cancer Treat Rev2010;36(Suppl 2):S12-7.
19. Sideras K, Gertz MA. Amyloidosis. Adv Clin Chem 2009;47:1-44.
20. Bayer-Garner IB, Smoller BR. AL amyloidosis is not present asan incidental finding in cutaneous biopsies of patients withmultiple myeloma. Clin Exp Dermatol 2002;27:240-2.
21. Desikan KR, Dhodapkar MV, Hough A, Waldron T, JagannathS, Siegel D, et al. Incidence and impact of light chain associated(AL) amyloidosis on the prognosis of patients with multiplemyeloma treated with autologous transplantation. Leuk Lym-phoma 1997;27:315-9.
22. Kyle RA. Multiple myeloma: review of 869 cases. Mayo ClinProc 1975;50:29-40.
23. Barlogie B, Shaughnessy J, Tricot G, Jacobson J, Zangari M, AnaissieE, et al. Treatment of multiple myeloma. Blood 2004;103:20-32.
24. Rocken C, Sletten K. Amyloid in surgical pathology. VirchowsArch 2003;443:3-16.
25. Stoopler ET, Sollecito TP, Chen SY. Amyloid deposition in the oralcavity: a retrospective study and review of the literature. Oral SurgOral Med Oral Pathol Oral Radiol Endod 2003;95:674-80.
26. Libbey CA, Skinner M, Cohen AS. Use of abdominal fat tissueaspirate in the diagnosis of systemic amyloidosis. Arch InternMed 1983;143:1549-52.
27. Duston MA, Skinner M, Shirahama T, Cohen AS. Diagnosis ofamyloidosis by abdominal fat aspiration. Analysis of four years’experience. Am J Med 1987;82:412-4.
28. Falk RH, Comenzo RL, Skinner M. The systemic amyloidoses.N Engl J Med 1997;337:898-909.
29. Bergesio F, Ciciani AM, Santostefano M, Brugnano R, Manganaro
M, Palladini G, et al., Immunopathology Group, Italian Society of
OOOOE332 Stoopler et al. March 2011
Nephrology. Renal involvement in systemic amyloidosis—anItalian retrospective study on epidemiological and clinical data atdiagnosis. Nephrol Dial Transplant 2007;22:1608-18.
30. von Hutten H, Mihatsch M, Lobeck H, Rudolph B, Eriksson M,Rocken C. Prevalence and origin of amyloid in kidney biopsies.Am J Surg Pathol 2009;33:1198-205.
31. Osawa Y, Kawamura K, Kondo D, Imai N, Ueno M, Nishi S, etal. Renal function at the time of renal biopsy as a predictor ofprognosis in patients with primary AL-type amyloidosis. ClinExp Nephrol 2004;8:127-33.
32. Kyle RA, Spencer RJ, Dahlin DC. Value of rectal biopsy in thediagnosis of primary systemic amyloidosis. Am J Med Sci1966;251:501-6.
33. Kuroda T, Tanabe N, Sakatsume M, Nozawa S, Mitsuka T,Ishikawa H, et al. Comparison of gastroduodenal, renal andabdominal fat biopsies for diagnosing amyloidosis in rheumatoidarthritis. Clin Rheumatol 2002;21:123-8.
34. Hachulla E, Grateau G. Diagnostic tools for amyloidosis. JointBone Spine 2002;69:538-45.
35. Balatsouras DG, Eliopoulos P, Assimakopoulos D, Korres S.Primary local amyloidosis of the palate. Otolaryngol Head NeckSurg 2007;137:348-9.
36. Selikoff IJ, Robitzek EH. Gingival biopsy for the diagnosis ofgeneralized amyloidosis. Am J Pathol 1947;23:1099-111.
37. Gorlin R, Gottsegen R. The role of the gingival biopsy insecondary amyloid disease. Oral Surg Oral Med Oral Pathol1949;2:864-6.
38. Nandapalan V, Jones TM, Morar P, Clark AH, Jones AS. Localizedamyloidosis of the parotid gland: a case report and review of thelocalized amyloidosis of the head and neck. Head Neck 1998;20:73-8.
39. Fahrner KS, Black CC, Gosselin BJ. Localized amyloidosis ofthe tongue: a review. Am J Otolaryngol 2004;25:186-9.
40. Stoopler ET, Alawi F, Laudenbach JM, Sollecito TP. Bullousamyloidosis of the oral cavity: a rare clinical presentation andreview. Oral Surg Oral Med Oral Pathol Oral Radiol Endod2006;101:734-40.
41. Kokong DD, Ibekwe TS, Okolo CA, Kodiya AM, Fasunla JA,Nwaorgu OG, et al. Amyloid angiopathy of the floor of themouth: a case report and review of the literature. J Med CaseReports 2007;1:117.
42. Lee SY, Chang H, Chen TC, Hsu HH, Fang JT, Yang CW.Lingual amyloidosis—a rare complication of long-term haemo-dialysis. Nephrol Dial Transplant 2007;22:1471-2.
43. Shah SS, Freedman PD. Amyloidomas of the jawbones withunderlying occult plasma cell dyscrasias: a report of 2 cases withreview of the literature. J Oral Maxillofac Surg 2007;65:1655-60.
44. Henley E, Houghton N, Bucknall R, Triantafyllou A, Field EA. Local-ized amyloidosis of the palate. Clin Exp Dermatol 2008;33:100-1.
45. Elad S, Czerninski R, Fischman S, Keshet N, Drucker S, Davidovich T,et al. Exceptional oral manifestations of amyloid light chain protein(AL) systemic amyloidosis. Amyloid 2010;17:27-31.
46. Delgado WA, Mosqueda A. A highly sensitive method for diag-nosis of secondary amyloidosis by labial salivary gland biopsy.J Oral Pathol Med 1989;18:310-4.
47. Madani M, Harwick RD, Chen SY, Miller AS. Amyloidosis of theoral cavity: report of five cases. Compendium 1991;12:338-42.
48. Hachulla E, Janin A, Flipo RM, Saile R, Facon T, Bataille D, et al.Labial salivary gland biopsy is a reliable test for the diagnosis ofprimary and secondary amyloidosis. A prospective clinical and immu-nohistologic study in 59 patients. Arthritis Rheum 1993;36:691-7.
49. Delgado WA, Arana-Chavez VE. Amyloid deposits in labialsalivary glands identified by electron microscopy. J Oral Pathol
Med 1997;26:51-2.50. van der Waal RI, van de Scheur MR, Huijgens PC, Starink TM,van der Waal I. Amyloidosis of the tongue as a paraneoplasticmarker of plasma cell dyscrasia. Oral Surg Oral Med Oral PatholOral Radiol Endod 2002;94:444-7.
51. Went R, Chan-Lam D, Thornhill M. Isolated tongue amyloid ina patient with multiple myeloma. Br J Haematol 2008;143:606.
52. Angiero F, Seramondi R, Magistro S, Crippa R, Benedicenti S,Rizzardi C, et al. Amyloid deposition in the tongue: clinical andhistopathological profile. Anticancer Res 2010;30:3009-14.
53. International Myeloma Working Group. Criteria for the classifi-cation of monoclonal gammopathies, multiple myeloma and re-lated disorders: a report of the International Myeloma WorkingGroup. Br J Haematol 2003;121:749-57.
54. Rajkumar SV, Buadi F. Multiple myeloma: new staging systemsfor diagnosis, prognosis and response evaluation. Best Pract ResClin Haematol 2007;20:665-80.
55. Durie BG, Salmon SE. A clinical staging system for multiplemyeloma. Correlation of measured myeloma cell mass withpresenting clinical features, response to treatment, and survival.Cancer 1975;36:842-54.
56. Greipp PR, San MJ, Durie BG, Crowley JJ, Barlogie B, Blade J,et al. International staging system for multiple myeloma. J ClinOncol 2005;23:3412-20.
57. Avet-Loiseau H, Attal M, Moreau P, Charbonnel C, Garban F,Hulin C, et al. Genetic abnormalities and survival in multiplemyeloma: the experience of the Intergroupe francophone duMyelome. Blood 2007;109:3489-95.
58. Greipp PR, Lust JA, O’Fallon WM, Katzmann JA, Witzig TE,Kyle RA. Plasma cell labeling index and beta 2-microglobulinpredict survival independent of thymidine kinase and C-reactiveprotein in multiple myeloma. Blood 1993;81:3382-7.
59. Witzig TE, Timm M, Larson D, Therneau T, Greipp PR. Mea-surement of apoptosis and proliferation of bone marrow plasmacells in patients with plasma cell proliferative disorders. Br JHaematol 1999;104:131-7.
60. Vela-Ojeda J, Garcia-Ruiz Esparza MA, Padilla-Gonzalez Y,Sanchez-Cortes E, Garcia-Chavez J, Montiel-Cervantes L, et al.Multiple myeloma-associated amyloidosis is an independenthigh-risk prognostic factor. Ann Hematol 2009;88:59-66.
61. Abraham RS, Geyer SM, Price-Troska TL, Allmer C, Kyle RA,Gertz MA, et al. Immunoglobulin light chain variable (V) regiongenes influence clinical presentation and outcome in light chain-associated amyloidosis (AL). Blood 2003;101:3801-8.
62. Pan WH, Li NP. Clinical pathological feature of early tongueamyloidosis. Chin Med Sci J 2006;21:104-6.
63. Finkel KJ, Kolansky DM, Giorgadze T, Thaler E. Amyloidinfiltration of the salivary glands in the setting of primary sys-temic amyloidosis without multiple myeloma. Otolaryngol HeadNeck Surg 2006;135:471-2.
64. Caporali R, Bonacci E, Epis O, Bobbio-Pallavicini F, Morbini P,Montecucco C. Safety and usefulness of minor salivary glandbiopsy: retrospective analysis of 502 procedures performed at asingle center. Arthritis Rheum 2008;59:714-20.
65. do Amaral B, Coelho T, Sousa A, Guimaraes A. Usefulness oflabial salivary gland biopsy in familial amyloid polyneuropathyPortuguese type. Amyloid 2009;16:232-8.
Reprint requests:
Eric T. Stoopler, DMDUniversity of Pennsylvania School of Dental Medicine240 South 40th StreetPhiladelphia, PA 19104
[email protected]