Embed Size (px)
Citation preview

antinuclear antibodies, rheumatoid factor, and C-reactiveprotein.
As it was thought that our patient had experienceda pathergy reaction, additional pathergy testing was per-formed so that a biopsy could be obtained after 24 hoursrather than 5 days. We performed a histamine trap test byintradermally injecting 0.05 mL of 1-mg/mL histaminesolution into the volar surface of the right forearm, per theprotocol outlined by Jorizzo et al4 in their study of histo-logic changes in pathergy reactions. After 24 hours, anerythematous macule was present at the site of injectionand a punch biopsy was obtained after infiltration of 1%lidocaine without epinephrine. Histopathologic examina-tion revealed superficial and deep perivascular mixed der-mal infiltrate of neutrophils and lymphocytes, endothelialswelling of blood vessel walls, perivascular accumulationof neutrophils, and minor focal leukocytoclasis andhyaline deposition (Fig 2, D). Immunostaining for lym-phocyte markers was again performed, and the lympho-cytes present were almost all T cells, but no appreciabledifference was found in the weak staining for CD4 andCD8. These clinical and histologic findings are consistentwith the pathergy response observed in patients withBehcxet’s disease, the prototypical disease that exhibitspathergy.4
Although previous skin test results were available,records of the patient’s past immunotherapy prescriptioncould not be obtained. No correlation was found betweenprevious skin prick test results and allergen sites thatsubsequently developed a pathergy response; pathergyreactions sites were evenly split between 18 allergens thathad been previously positive on skin prick testing and20 allergens that had been previously negative on skinprick testing. Presumably only allergens that gave positiveresponses on previous skin prick testing would havebeen used for immunotherapy. Thus, we do not believethe pathergy reaction of this patient was a response toprevious immunotherapy.
Pathergy has been associated with several diseaseentities, including Behcxet’s disease, pyoderma gangreno-sum, eosinophilic pustular folliculitis, cutaneous ulcerativelichen planus, bowel-associated dermatosis-arthritis syn-drome, rheumatoid arthritis, leukocytoclastic vasculitis,non-hodgkin lymphoma, and chronic myeloid leukemiatreated with interferon-a.4-9 Jorizzo et al4 proposed that thepathergy response in Behcxet’s disease may be explained bya combination of circulating immune complexes, perhapsfrom associated diseases, and an unknown factor in the se-rum that enhances neutrophil migration. A previous reportshowed no pathergy response after skin prick testing tocommon aeroallergens in a collection of 30 patients withBehcxet’s disease, despite many of them having a positivepathergy test.5 Physicians conducting skin prick testingshould be aware of pathergy as a rare adverse event and con-sider associated diseases in patients in whom this reactionoccurs. Given the uncertain etiology of the developmentof a pathergy response in this patient, immunotherapy wasnot offered as a treatment option. Our patient may overtime develop symptoms consistent with a known pathergy-
associated illnesses, which may explain why she devel-oped this response after skin prick testing.
We thank our dermatopathologists, Lt Col (Dr) Michael R.
Murchland and Lt Col (Dr) Marcus S. Fisher, for their assistance.
Thomas L. Johnson, Maj, USAF, MC, MDa
Patrick E. McCleskey, Capt, USAF, MC, MDb
Melinda Rathkopf, Maj, USAF, MC, MDa
Jeffrey J. Meffert, MDc
Larry L. Hagan, Col, USAF, MC, MDa
From the Departments of aAllergy and Immunology and bDermatology,
Wilford Hall Medical Center, Lackland Air Force Base, San Antonio,
Tex; and cthe Division of Dermatology, University of Texas Health Science
Center, San Antonio, Tex. E-mail: [email protected].
Disclosure of potential conflict of interest: M. Rathkopf has received grant
support from Novartis and ZLB Behring; is employed by Allergy, Asthma,
and Immunology Center of Alaska, LLC; and is on the speakers’ bureau for
Genentech. The rest of the authors have declared that they have no conflict
of interest.
REFERENCES
1. Lin RY. Delayed hypersensitivity to pollen skin prick tests and seasonal
rhinitis. J Allergy Clin Immunol 1995;95:911-2.
2. Lierl MB. Isolated late cutaneous reactions to allergen skin testing in chil-
dren. Ann Allergy Asthma Immunol 2000;84:294-8.
3. Green GR, Zweiman B, Beerman H, Hildreth EA. Delayed skin reactions
to inhalant antigens. J Allergy 1967;40:224-36.
4. Jorizzo JL, Hudson RD, Schmalstieg FC, Daniels JC, Apisarnthanarax P,
Henry JC, et al. Behcet’s syndrome: immune regulation, circulating
immune complexes, neutrophil migration, and colchicine therapy. J Am
Acad Dermatol 1984;10:205-14.
5. Dinc A, Karaayvaz M, Caliskaner AZ, Pay S, Erdem H, Turan M. Der-
mographism and atopy in patients with Behcet’s disease. Invest Allergol
Clin Immunol 2000;10:368-71.
6. Henderson RL, Williford PM, Molnar JA. Cutaneous ulcerative lichen
planus exhibiting pathergy, response to acitretin. J Drugs Dermatol 2004;3:
191-2.
7. Burney IA, Moatter T, Siddiqui T, Yaqoob N. Pathergy in non-Hodgkin
lymphoma. J R Soc Med 2003;96:127-9.
8. Hsu PJ, Huang CJ, Wu MT. Pathergy in atypical eosinophilic pustular
folliculitis. Int J Dermatol 2005;44:203-5.
9. Budak-Alpdogan T, Demircay Z, Alpdogan O, Direskeneli H, Ergun T,
Ozturk A, et al. Skin hyperreactivity of Behcet’s patients is also positive
in interferon alpha-treated chronic myeloid leukaemia patients, indecation
similarly altered neutrophil functions in both disorders. Brit J Rheum
1998;37:1148-51.
Available online March 15, 2007.doi:10.1016/j.jaci.2007.01.033
J ALLERGY CLIN IMMUNOL
MAY 2007
1272 Letters to the Editor
Lette
rsto
the
Edito
r
The predictive relationship of food-specificserum IgE concentrations to challengeoutcomes for egg and milk varies bypatient ageTo the Editor:It is complicated to interpret food-allergy symptoms in
children because of the dynamic nature of the allergicresponse that changes with time: the acquisition of foodtolerance and amelioration of symptoms is reported inchildren with all types of food allergy.1 The various diag-nostic errors and pitfalls in the management of foodallergy suggest that we should utilize all available testsmore fully in the best interests of the patient. Sampson
J ALLERGY CLIN IMMUNOL
VOLUME 119, NUMBER 5
Letters to the Editor 1273
ett
ers
toth
eEd
itor
and Ho2 and Sampson3 were first to publish studies on uti-lization of serum specific IgE in order to predict whichfood-allergic patients were likely to fail in oral food chal-lenge. They suggested threshold values for egg 7 kilounitsof specific IgE antibodies per liter ( kUA/L) and for milk 15kUA/L, respectively, ie, food-specific serum IgE concen-trations in which approximately 95% of the patients arepredicted to have clinical reaction.3 These diagnosticvalues were helpful to the physician in deciding if foodchallenge was necessary or potentially harmful to the pa-tients and also led to an interest among other researchers toinvestigate these relationships. Boyano-Martinez et al4
and Garcia-Ara et al5 found that the 90% diagnostic valuefor egg was >0.35 kUA/L and for milk 1.5, 6, and 14 kUA/L in the age range 13-18 months, 19-24 months, and in thethird year, respectively. Osterballe and Bindslev-Jensen6
showed the 95% diagnostic value was 1.5 kUA/L foregg. Celik-Bilgili et al7 found diagnostic values for 95%probability of allergy to hen’s egg was 10 kUA/L and tocow’s milk 46 kUA/L, values showing substantial differ-ence from those published previously.
These differences in diagnostic values may be explainedby the fact that their study populations differed. Wehypothesized that the age of the child additionally influ-ences the specific IgE diagnostic values when predictingthe outcome of food challenge for egg and milk.
The objective of this study was to relate the specific IgEantibody concentration to egg and milk to the outcome offood challenge for children of various ages suspected ofsuffering from egg and milk allergy.
Eight hundred sixty-one oral challenges were per-formed for cow’s milk and 764 oral challenges for hen’segg among 969 children (median age 1.3 years, range:0.2-14.6). Of a total 1625 oral food challenges, 1606 wereopen challenges according to recommendations of Euro-pean Academy of Asthma and Clinical Immunology andthe American Academy of Asthma, Allergy & Immunol-ogy. Seventy-four percent of patients had atopic dermatitisand 18% had asthma; allergic rhinitis and allergic con-junctivitis were present in 8% and 5% of the patients,respectively. Allergen-specific IgE antibody levels weremeasured using the Pharmacia CAP System (Phadia AB,Uppsala, Sweden) towards hen’s egg and cow’s milk. Thedetection limit of the assay was 0.35 kUA/L.
Oral food challenge was used as the gold standard bywhich the sensitivity, specificity, and receiver operator
TABLE I. Symptoms provoked by oral food challenge
Total
(n 5 589)
No. (%)
Egg white
(n 5 374)
No. (%)
Cow’s milk
(n 5 215)
No. (%)
Cutaneous 581 (99) 368 (98) 213 (99)
Mucous membrane 16 (3) 7 (2) 9 (4)
Lower respiratory 36 (6) 21 (6) 15 (7)
Gastrointestinal 48 (8) 34 (9) 14 (7)
Anaphylaxis 16 (3) 8 (2) 8 (4)
Other 3 (1) 1 (0) 2 (1)
L
characteristic curve analysis were calculated. The rela-tionship between sensitization status and outcome measurewas analyzed using logistic regression. Fitted predictedprobability curves were plotted using the results from thelogistic regression.
Forty-nine percent of the performed egg challengesand 25% of the performed cow’s milk challenges wereassessed as positive. Symptoms provoked by the oral foodchallenge are listed in Table I.
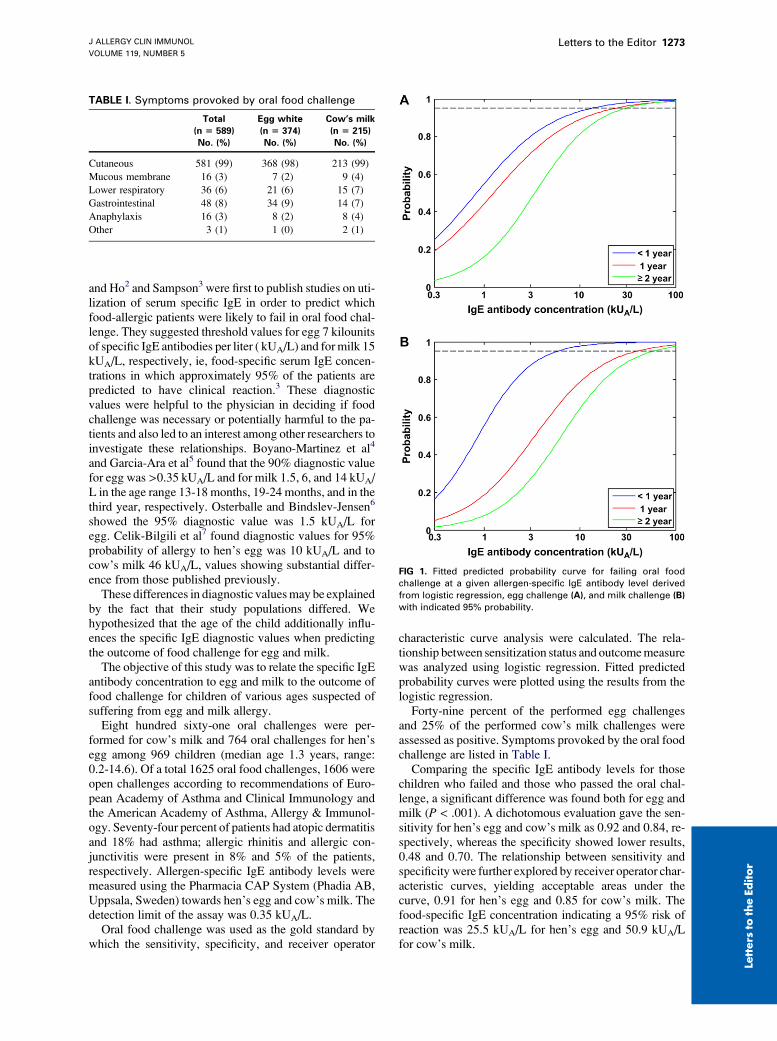
Comparing the specific IgE antibody levels for thosechildren who failed and those who passed the oral chal-lenge, a significant difference was found both for egg andmilk (P < .001). A dichotomous evaluation gave the sen-sitivity for hen’s egg and cow’s milk as 0.92 and 0.84, re-spectively, whereas the specificity showed lower results,0.48 and 0.70. The relationship between sensitivity andspecificity were further explored by receiver operator char-acteristic curves, yielding acceptable areas under thecurve, 0.91 for hen’s egg and 0.85 for cow’s milk. Thefood-specific IgE concentration indicating a 95% risk ofreaction was 25.5 kUA/L for hen’s egg and 50.9 kUA/Lfor cow’s milk.
FIG 1. Fitted predicted probability curve for failing oral food
challenge at a given allergen-specific IgE antibody level derived
from logistic regression, egg challenge (A), and milk challenge (B)
with indicated 95% probability.

Bronchoalveolar lavage invariant natural killerT cells are not increased in asthma
To the Editor:Asthma is characterized by variable airflow obstruction
and airway hyperresponsiveness (AHR) in associationwith chronic inflammation. The airway inflammation inasthma is typically eosinophilic with increased expressionof TH2 cytokines1 and mast cell infiltration of the airwaysmooth muscle bundle.2 Emerging evidence also supportsa possible role in the pathophysiology of asthma for natu-ral killer (NK) T cells and, in particular, CDd1 restrictedor invariant NKT (iNKT) cells. NKT cells are a recen-tly identified distinct subset of T cells that express markersof both NK cells and T cells and seem to be potent immu-noregulatory cells because of their ability to secrete largequantities of both TH1 and TH2 cytokines.3 In an animalmodel of asthma, NKT cell–deficient mice were shownto be unable to develop AHR after allergen sensitizationand challenge although these animals did show TH2 re-sponses after the allergen challenge.4 Subsequent adoptivetransfer of NKT cells into these mice restored AHR, andthis was shown to occur via an IL-4–dependent and anIL-13–dependent pathway. Furthermore, this transferseemingly occurs independent of eosinophils, B cells,and CD41 T cells, which indicates an additional effectorrole for these cells in this model of asthma.5 In a humanstudy of moderate-to-severe patients with asthma, up to60% of the CD4 T cells in bronchoalveolar lavage(BAL) were identified as iNKT cells. In addition, thesepulmonary iNKT cells were shown to produce exclusivelyTH2 cytokines.6 The scale of this finding is surprising, andgiven the differing properties of these cells from the con-ventional CD4 T cells, this does have important implica-tions in understanding the pathophysiology of asthma,especially steroid-resistant asthma, and the developmentof future treatment strategies. We have therefore
J ALLERGY CLIN IMMUNOL
MAY 2007
1274 Letters to the Editor
Lette
rsto
the
Edito
r
Poststratification into age groups showed diagnosticvalues for 95% probabilities for failing oral challenge, forchildren less than 1 year old (13.0 kUA/L), 1 year old (23.0kUA/L) and 2 years or older (30.0 kUA/L) for egg (Fig 1,A). Corresponding numbers for cow’s milk were for chil-dren less than 1 year old (5.8 kUA/L), 1 year old (38.6kUA/L), and 2 years or older (57.3 kUA/L) (Fig 1, B).
Our results confirm that increasing IgE levels to milkand egg correlate with increasing risks for reactions uponfood challenge are useful to predict outcomes and areinfluenced by age. Of note, the specific IgE levels indi-cating a 95% risk of reaction were much higher in ourpatient population compared to those observed in previ-ous studies.2-7 There are several possible explanationsfor these differences, including different selection crite-ria, the influence of age, and different criteria for deter-mining a failed or passed food challenge. If very mildand transient symptoms are counted as positive, thishas a definite influence on the diagnostic values. IgElevels have been regarded as a useful predictor of chal-lenge outcome but as a less useful predictor for the de-gree of reaction severity during failed food challenge.Hourihane et al8 have also recently shown that peanut-specific IgE concentration can predict severity of reac-tion in double-blind, placebo-controlled food challengeif the dose of allergen is considered. Our data add toprevious studies from other investigators showing thatthe specific predictive values may vary among studies.This variation should be explored in further studiesand currently requires caution in applying results to dis-tinct patient populations.
We conclude that there is a relationship betweenallergen-specific IgE levels to egg and milk and oral foodchallenge outcome and that this relationship is influencedby age. Younger children react on low levels of specificIgE antibody concentration to egg and milk comparedto older children.
We thank Professor Youshikatsu Eto for comments and critical
review.
Takatsugu Komata, MDa,b
Lars Soderstrom, MScc
Magnus P. Borres, MD, PhDc,d
Hiroshi Tachimoto, MD, PhDa
Motohiro Ebisawa, MD, PhDe
From athe Department of Pediatrics, Sagamihara National Hospital, Kana-
gawa, Japan; bthe Department of Pediatrics, Jikei University School of
Medicine, Tokyo, Japan; cPhadia AB, Uppsala, Sweden; dthe Department
of Pediatrics, Sahlgrenska Academy of Goteborg University, Goteborg,
Sweden; and ethe Clinical Research Center for Allergy and Rheumatology,
Sagamihara National Hospital, Sagamihara-City, Japan. E-mail: m-ebisawa@
sagamihara-hosp.gr.jp.
Supported by the Ministry of Health, Labour and Welfare, Japan.
Disclosure of potential conflict of interest: The authors have declared that they
have no conflict of interest.
REFERENCES
1. Ikematsu K, Tachimoto H, Sugisaki C, Syukuya A, Ebisawa M. [Feature
of food allergy developed during infancy—acquisition of tolerance against
hen’s egg, cow’s milk, wheat, and soybean up to 3 years old]. Arerugi
2006;55:533-41.
2. Sampson HA, Ho DG. Relationship between food-specific IgE concentra-
tions and the risk of positive food challenges in children and adolescents.
J Allergy Clin Immunol 1997;100:444-51.
3. Sampson HA. Utility of food-specific IgE concentrations in predicting
symptomatic food allergy. J Allergy Clin Immunol 2001;107:891-6.
4. Boyano-Martinez T, Garcia-Ara C, Diaz-Pena JM, Munoz FM, Garcia-
Sanchez G, Esteban MM. Validity of specific IgE antibodies in children
with egg allergy. Clin Exp Allergy 2001;31:1464-9.
5. Garcia-Ara MC, Boyano-Martinez MT, Diaz-Pena JM, Martin-Munoz
MF, Martin-Estaban M. Cow’s milk-specific immunoglobulin E levels
as predictors of clinical reactivity in the follow-up of the cow’s milk
allergy infants. Clin Exp Allergy 2004;34:866-7.
6. Osterballe M, Binslev-Jensen C. Treshold levels in food challenge and
specific IgE in patients with egg allergy: is there a relationship? J Allergy
Clin Immunol 2003;112:196-201.
7. Celik-Bilgili S, Mehl A, Verstege A, Staden U, Nocon M, Beyer K, et al.
The predictive value of specific immunoglobulin E levels in serum for the
outcome of oral food challenges. Clin Exp Allergy 2005;35:268-73.
8. Hourihane JO, Grimshaw KEC, Lewis SA, Briggs RA, Trewin JB, King
RM, et al. Does severity of low-dose, double-blind, placebo-controlled
food challenges reflect severity of allergic reactions to peanut in the
community? Clin Exp Allergy 2005;35:1227-33.
Available online March 10, 2007.doi:10.1016/j.jaci.2007.01.038





























