Embed Size (px)
Citation preview
11/30/2016
1
December 1, 2016
Steve Reinhart, MBA
Director, Clinical Quality | HRET
THE POWER OF HIINOVATION
PROJECT BACKGROUND, SCOPE, & GOALS
1
This activity is jointly-provided by SynAptiv and the Colorado Hospital Association
11/30/2016
2
CONFLICT OF INTEREST DISCLOSURE STATEMENT
I have no financial interest or other relationships with the industry relative to the topics being discussed.
• Overview of HIIN
–HEN 1.0 and HEN 2.0
–HIIN: where we are going & why it is different
• Assistance you get as a HIIN hospital
–Education
– Site visits and technical assistance
– Fellowship
–CDS reports
AGENDA

11/30/2016
3
Hospital type:
• General medical/surgical?
• Teaching?
• Rural/CAH?
HOW MANY OF YOU ARE JOINING US FROM…
Hospital size:
• CAH?
• Not CAH, <100 beds?
• Not CAH, 100-299 beds?
• Not CAH, 300+ beds?
HOW MANY OF YOU ARE JOINING US FROM…

11/30/2016
4
WHAT BEST DESCRIBES YOUR EXPOSURE TO HIIN/QI WORK?
A. We are familiar with HEN/HEN 2.0 and are a high reliability organization.
B. We are familiar with HEN/HEN 2.0 and are looking to take our hospital to the next level and free education, free resources and free assistance sounded like a good idea.
C. We are not familiar with HEN/HEN 2.0 and would like to learn more.
D. We are here because someone told us we needed to attend.
PARTNERSHIP FOR PATIENTS
The 40/20 goal set December 2011:
Keep patients from getting injured or sicker.• Reduce preventable hospital-acquired conditions by 40 percent.
–1.8 million fewer injuries to patients, with more than 60,000 lives saved over the next three years.
Help patients heal without complication.• Reduce all hospital readmissions by 20 percent.
–1.6 million patients will recover from illness without suffering a preventable complication requiring re-hospitalization within 30 days of discharge.

11/30/2016
5
Substantial progress thru 2014, compared to 2010 Baseline:
• 17 percent reduction in overall harm; 39 percent reduction in preventable harm.
• 87,000 lives saved.
• $19.8B in cost savings from harm avoided.
• 2.1M fewer harms over four years.
NATIONAL RESULTS ON PATIENT SAFETY
Source: Agency for Healthcare Research & Quality. “Saving Lives and Saving Money: Hospital-Acquired Conditions Update. Interim Data From National Efforts To Make Care Safer, 2010-2014.” December 1, 2015.
AHA/HRET ORIGINAL HEN RESULTS
11/30/2016
6
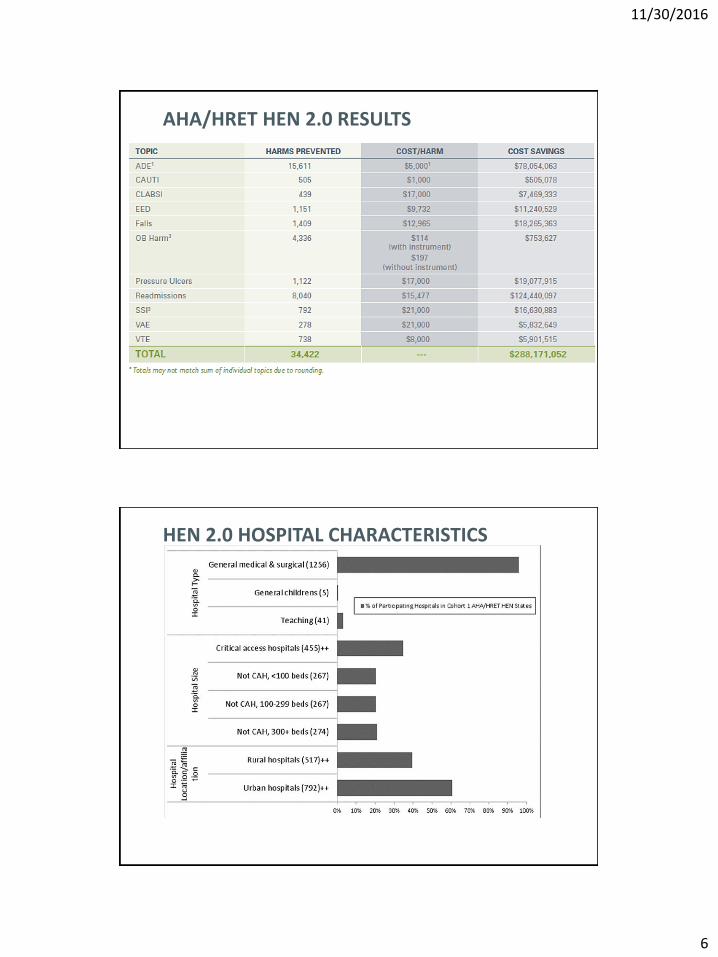
AHA/HRET HEN 2.0 RESULTS
HEN 2.0 HOSPITAL CHARACTERISTICS

11/30/2016
7
13
HEN 2.0 RESOURCES
HEN 2.0 RESULTS – COLORADO
14
Topic
CO Hospital Results(Data submitted as of 9/1/2016) AHA/HRET
Baselinesubmission
Baseline rate
Mar – May rate
Relative reduction
Relative reduction
Catheter-Associated Urinary Tract Infection (CAUTI) 26 (100%) 0.87 0.75 -14.3% -4.1%
Central Line-Associated Blood Stream Infection (CLABSI) 26 (100%) 0.30 0.42 39.4% -11.2%
Early Elective Deliveries (EED) 17 (100%) 2.08 0.68 -67.5% -44.2%
Obstetrical Harm (OB Harm) 16 (94%) 19.54 10.08 -48.4% -49.2%
Falls 25 (96%) 0.51 0.58 14.0% -5.2%
Pressure Ulcers (PrU) 26 (100%) 0.80 1.22 52.9% -43.0%
Surgical Site Infections (SSI) 19 (100%) 1.48 1.54 3.8% -21.2%
Ventilator-Associated Events (VAE) 12 (100%) 0.41 0.24 -42.0% 13.8%
Venous Thromboembolism (VTE) 19 (100%) 5.93 8.29 39.7% -34.0%
Adverse Drug Events (ADE) 26 (100%) 1.44 1.26 -12.4% -11.7%
Readmissions 26 (100%) 5.33 5.21 -2.3% -4.0%
1 Relative reduction calculated by comparing baseline to quarterly rate Mar– May 2016
11/30/2016
8
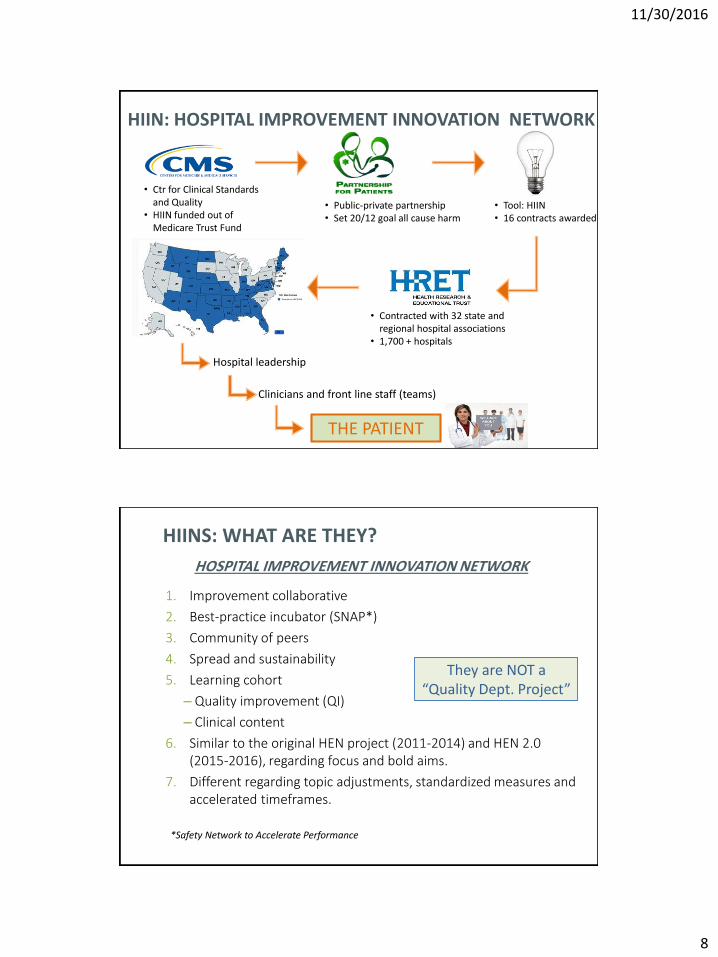
Hospital leadership
Clinicians and front line staff (teams)
THE PATIENT
• Public-private partnership• Set 20/12 goal all cause harm
• Tool: HIIN• 16 contracts awarded
• Contracted with 32 state and regional hospital associations
• 1,700 + hospitals
• Ctr for Clinical Standards and Quality
• HIIN funded out of Medicare Trust Fund
HIIN: HOSPITAL IMPROVEMENT INNOVATION NETWORK
1. Improvement collaborative
2. Best-practice incubator (SNAP*)
3. Community of peers
4. Spread and sustainability
5. Learning cohort
– Quality improvement (QI)
– Clinical content
6. Similar to the original HEN project (2011-2014) and HEN 2.0 (2015-2016), regarding focus and bold aims.
7. Different regarding topic adjustments, standardized measures and accelerated timeframes.
HIINS: WHAT ARE THEY?
HOSPITAL IMPROVEMENT INNOVATION NETWORK
They are NOT a “Quality Dept. Project”
*Safety Network to Accelerate Performance
11/30/2016
9
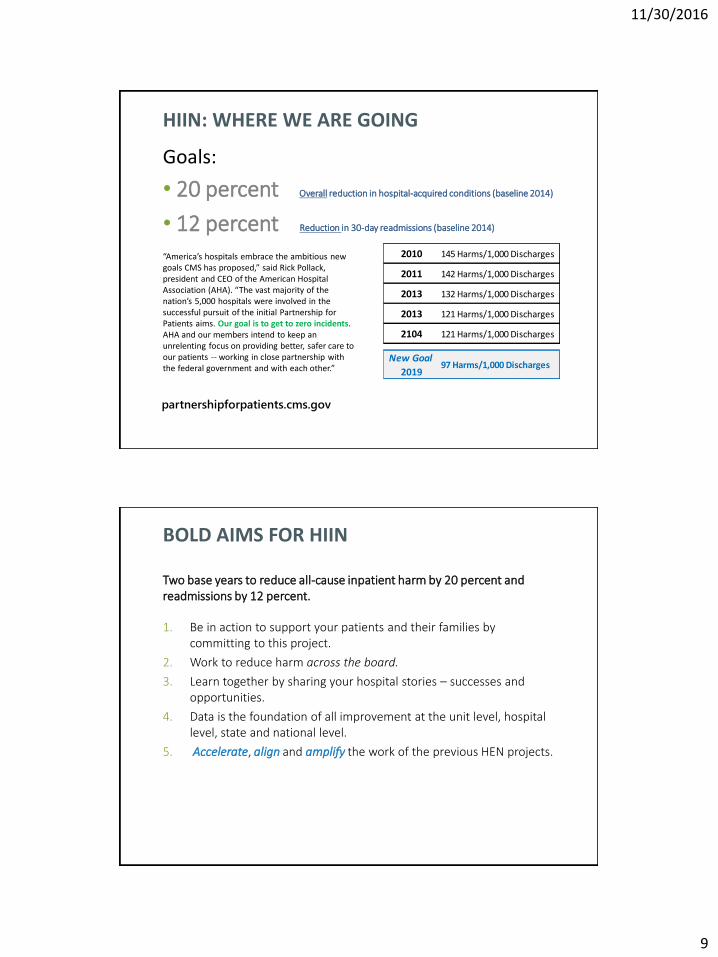
HIIN: WHERE WE ARE GOING
• 20 percent Overall reduction in hospital-acquired conditions (baseline 2014)
• 12 percent Reduction in 30-day readmissions (baseline 2014)
“America’s hospitals embrace the ambitious new goals CMS has proposed,” said Rick Pollack, president and CEO of the American Hospital Association (AHA). “The vast majority of the nation’s 5,000 hospitals were involved in the successful pursuit of the initial Partnership for Patients aims. Our goal is to get to zero incidents. AHA and our members intend to keep an unrelenting focus on providing better, safer care to our patients -- working in close partnership with the federal government and with each other.”
Goals:
partnershipforpatients.cms.gov
2010 145 Harms/1,000 Discharges
2011 142 Harms/1,000 Discharges
2013 132 Harms/1,000 Discharges
2013 121 Harms/1,000 Discharges
2104 121 Harms/1,000 Discharges
New Goal
201997 Harms/1,000 Discharges
Two base years to reduce all-cause inpatient harm by 20 percent and readmissions by 12 percent.
1. Be in action to support your patients and their families by committing to this project.
2. Work to reduce harm across the board.
3. Learn together by sharing your hospital stories – successes and opportunities.
4. Data is the foundation of all improvement at the unit level, hospital level, state and national level.
5. Accelerate, align and amplify the work of the previous HEN projects.
BOLD AIMS FOR HIIN

11/30/2016
10
1. Alabama
2. Arizona
3. Arkansas
4. Colorado
5. Connecticut
6. Dallas Fort-Worth
7. Delaware
8. Florida
9. Georgia
10.Idaho
11.Indiana
12.Kansas
13.Kentucky
14.Louisiana
15.Maine
16.Maryland
17.Massachusetts
18.Mississippi
19.Missouri
20.Montana
21.Nebraska
22.New Hampshire
23.New Mexico
24.North Dakota
25.Oklahoma
26.Rhode Island
27.Tennessee
28.Texas
29.Virginia
30.West Virginia
31.Wyoming
HRET HIIN STATE PARTNERS
• Framing all HIIN work as a single, cross-cutting improvement initiative rather than series of discrete efforts
–Group a few interventions together (leadership, current/accurate data, physician engagement, culture of safety, PFE)
• Emphasize “doing” within the hospital rather than “attending” as the route to substantive progress
– Look at the improvement occurring within the organization
• Stressing rapid progress vs chance
– Focus on rapid change linked to process improvement
HRET’S APPROACH
11/30/2016
11
Organizational Engagement
– Leadership engagement
• Leverage HIT resources to promote improvement
• Making the financial case
• Monitoring and promoting improvement
– Physician Engagement
• Training and coaching to project leaders regarding how to effectively engage physicians
• Training and coaching for physicians on how they can champion improvement efforts
– Patient / Family Insights
• Provide guidance and coaching on how to leverage PFE insights to reduce harm
• Focused guidance on how PFE can directly contribute to avoid infections, prevent falls
HRET’S EMPHASES
Hands on Improvement Support
– Site Visits
• Well-planned and executed site visits
• Foster leadership support
• Facilitate physician engagement
• Provide a forum to receive practical advice on topics
– Coaching calls
• Focus on implementation challenges
• Allow hospitals to ask questions, get advice and encouragement
• Obtain improvement insights
– Panels
• Clinical and implementation experts
• Hospital staff
• Peer level sharing
HRET’S EMPHASES

11/30/2016
12
• Data System
– Simple, straight forward, user-friendly, non-duplicative
• Education and resources development
–Best practice dissemination
–Active engagement by participants
– Implementation challenges addressed
• Virtual support, tools and resources
–Easily accessible, relevant
–Website and LISTSERV®
• SMEs, IAs, Physician Advisors
• Site visits
HRET’S TACTICS
THE HRET HIIN STRUCTURE
Patients
and families
Hospital teams (YOU!)
SHA (Colorado Hospital Association) and QIN-QIO (Telligen) teams
HRET HIIN team

11/30/2016
13
CORE TOPICS – AIM IS 20 PERCENT REDUCTION
1. Adverse drug events (ADE)
2. Catheter-associated urinary tract infections (CAUTI)
3. C. difficile infections (C. diff)
4. Central line-associated blood stream infections (CLABSI)
5. Injuries from falls and immobility
6. Pressure ulcers (PrU)
7. Sepsis
8. Surgical site infections (SSI)
9. Venous thromboembolisms (VTE)
10. Ventilator-associated events (VAE)
11. Readmissions (12 percent reduction)
Note: patient and family engagement (PFE) and health care disparities (HCD) woven throughout all topics.
ALL OTHER FORMS OF HARM
1. Multi-drug resistant organisms (e.g. MRSA)*
2. Hospital patient safety culture*
3. Diagnostic error**
4. Airway safety**
5. Iatrogenic delirium**
6. Undue exposure to radiation**
7. Malnutrition in the inpatient setting**
*HRET will have a strong focus on MRSA and hospital patient safety culture throughout the project.
**HRET HIIN will provide support on the topics and encourages you to work on them, but Colorado is not requiring these.

11/30/2016
14
• Customized by hospitals’ needs:
– High-level and targeted.
– Didactic and interactive.
– Full-hour and condensed virtual events.
– Highly technical and practical implementation vs theory.
• Cross-cutting:
– UP
– PFE
– Disparities
• Topics will be prioritized based on our direction from CMS, you and your
project data (including a needs assessment).
• Data webinars
– Will cover how you can use project data and analytics to inform quality
improvement.
EDUCATIONAL OPPORTUNITIES
Creating Systems to Prevent Falls: Coming Together to Get Up!December 1 |11:00–11:50am MT
It is time to start teaming if we want to move the needle on falls. Nurses can’t do this alone. Hospitals have seen an unintentional shift towards restricting independent mobility to prevent falls when there is not a structured mobility program, resources and teamwork to mobilize patients safely and regularly. In this kick off Falls Learning Event for HIIN, we will look at safe mobility from the nurses’ perspective and build a case for increasing the influence of Physical Therapists on interdisciplinary teams to make it a reality. Please come prepared to react to the different perspectives being shared and bring your organization or unit’s needs, experiences, solutions and aspirations to share.
Audience: Executive Leadership, Interdisciplinary Falls Teams, Front Line Nurses, Front Line Physical Therapists, Nursing Leaders, Physical Therapy Leaders, Physicians, Physician Leadership, Patient Family Advisors.
Download the agenda and register today.
JOIN OUR UPCOMING VIRTUAL EVENTS!
http://www.hret-hiin.org/events/index.shtml

11/30/2016
15
JOIN OUR UPCOMING VIRTUAL EVENTS!
http://www.hret-hiin.org/events/index.shtml
HRET HIIN CAUTI Virtual EventDecember 6 | 10:00–10:50am MT
The technical changes needed to reduce catheter-associated urinary tract infections (CAUTI) are well documented. Over the past five years, evidence has mounted to support reducing the number of indwelling catheters placed, ensuring reliable aseptic placement, conducting daily review of catheter necessity according to indications, and removing catheters in a timely manner. Why then, are hospitals still struggling to reduce hospital-acquired CAUTI? In this initial HIIN CAUTI event, we will pose and discuss the “wicked questions” that address the complex adaptive issues that contribute to the current state, as well as hear strategies to address barriers to cultural and behavioral changes. Please come prepared for a lively discussion and to ask some “wicked questions” of your own!
Audience: Executive Leaders, Nursing Leaders, Front Line Nurses, Physicians, Infection Preventionists, Infectious Disease Physicians, Hospital Epidemiologists, Quality Directors, Patient Family Advisors, Nursing Assistive Personnel
Register today!
JOIN OUR UPCOMING VIRTUAL EVENTS!
http://www.hret-hiin.org/events/index.shtml
HRET HIIN Quality Improvement & Patient Family Engagement Fellowships Informational SessionDecember 8 |10:00 – 11:00 pm MT
Are you passionate about improving patient care but not sure how to go about it? Do you have a desire to increase patients’ autonomy and involvement in their own care? Please join HRET, Tanya Lord and IHI to learn more about the amazing opportunities to be a fellow with a quality improvement (QI) or patient and family engagement (PFE) focus! This event is held specially for HRET HIIN hospital staff members and quality workers who are interested in learning more and participating in the HIIN QI and/or PFE fellowships.
Download the agenda and register today.

11/30/2016
16
LISTSERV® COLLABORATION
• Subscriber-based email group.
• Each email group covers a different topic or group of topics.
• Ideal for:
• Peer-shared learning.
• Asking questions about barriers.
• Sharing data collection opportunities.
• Clarifications about measures or inclusion/exclusion criteria.
HIIN WEBSITE…IN DEVELOPMENT
www.hret-hiin.org
11/30/2016
17
FOR NOW, HEN 2.0 SITE IS A GREAT REFERENCE
Resources:• Click on
resources• Sort by topic
www.hret-hen.org
• QI: Foundations for Change Fellowship
– For new HIIN participants or those new to quality improvement.
• QI: Accelerating Improvement Fellowship
– For QI-trained HIIN participants or those who have been focused on quality improvement and patient safety for more than five years.
• PFE Fellowship
– For hospital staff and patient/family advisors seeking to support PFE at their institution and guide patient and family advisors on how to support QI and patient safety efforts.
Details for each include:
• Integrated learning across topics, QI and PFE fellowships.
• Deliverables throughout the fellowship to drive pace.
• Focus on peer-to-peer learning.
• Projects will highlight individual hospital progress toward HIIN project goals.
• Supported by virtual and on-site collaboration.
FELLOWSHIPS: QI AND PATIENT & FAMILY ENGAGEMENT (PFE)

11/30/2016
18
• Alarm fatigue
• Patient satisfaction
• Closing the referral loop
• Catheter reduction
• Rounding
• Adverse drug events
• Falls
EXAMPLES OF QI FELLOWSHIP PROJECTS FROM HEN 2.0
• Colorado Hospital Association will contact you to set up a mutually agreeable date and time for them to visit and review the project, data and your organization’s goals.
• During site visits:
–You will complete an action plan with your state partner.
• What to expect:
–Focused attention, support and guidance.
–Site visits are meant to set you up for success in HIIN.
SITE VISITS

11/30/2016
19
3 CO hospitals have taken the #123forEquity pledge
HEALTH CARE DISPARITIES
http://www.equityofcare.org/pledge/index.shtml
• Simple, straightforward and explainable!
• Capitalize on existing data where possible.
• Use standardized measures.
• Be responsive to unique needs.
• We have done this for 4+ years – the team has the experience and understanding to help support your hospital in gathering data.
MEASUREMENT PHILOSOPHY

11/30/2016
20
Reports available in the Comprehensive Data System (CDS)
CDS
Additional reports in CDS:
• All measures
• Custom data
• Current improvement
• Relative improvement
• Ad-hoc reports
CDS interpretation guide is available here.
CDS
11/30/2016
21
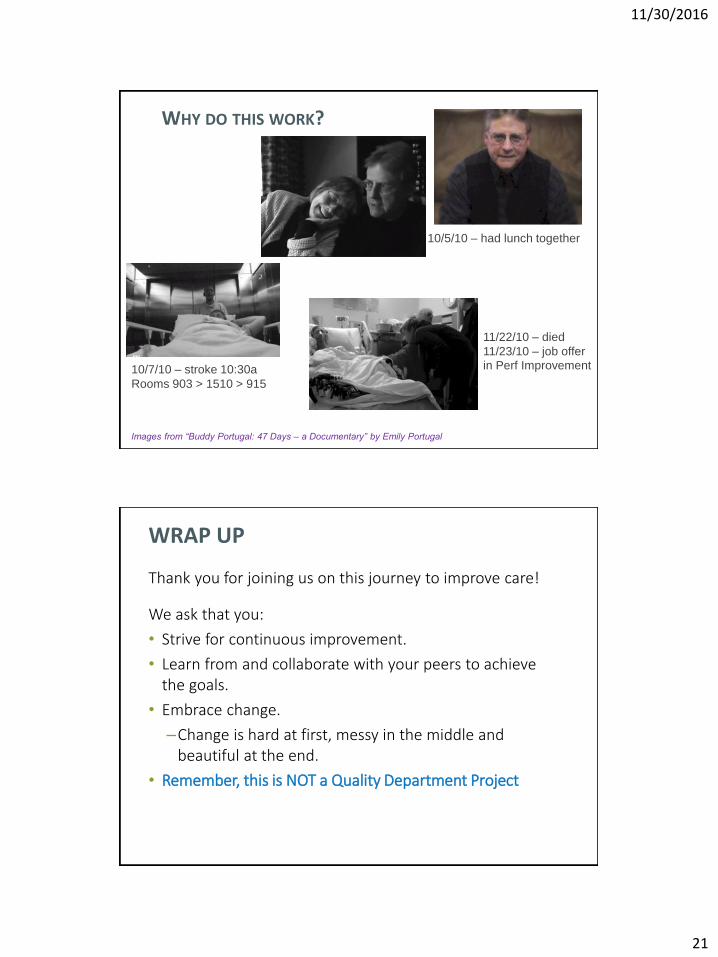
WHY DO THIS WORK?
41
10/5/10 – had lunch together
10/7/10 – stroke 10:30a
Rooms 903 > 1510 > 915
11/22/10 – died
11/23/10 – job offer
in Perf Improvement
Images from “Buddy Portugal: 47 Days – a Documentary” by Emily Portugal
WRAP UP
Thank you for joining us on this journey to improve care!
We ask that you:
• Strive for continuous improvement.
• Learn from and collaborate with your peers to achieve the goals.
• Embrace change.
–Change is hard at first, messy in the middle and beautiful at the end.
• Remember, this is NOT a Quality Department Project

11/30/2016
22
QUESTIONS?
Thank you – we look forward to supporting you on your HIIN journey





























