Embed Size (px)
Citation preview
The Postpartum Depression (PPD) Patient JourneyFirst in a Series of Articles on the Patient Journey and Management Challenges of PPD
Brought to you by Sage Therapeutics
SUPP
LEM
ENT
Supplement to
Volume 27, No. 6Supplement 1June 2018

2
THE POSTPARTUM DEPRESSION (PPD) PATIENT JOURNEY
This supplement was developed by MediMedia, an ICON plc company, with support from Sage Therapeutics. Sage Therapeutics is acknowledged for participating in the writing, review, and editing of this supplement.
3
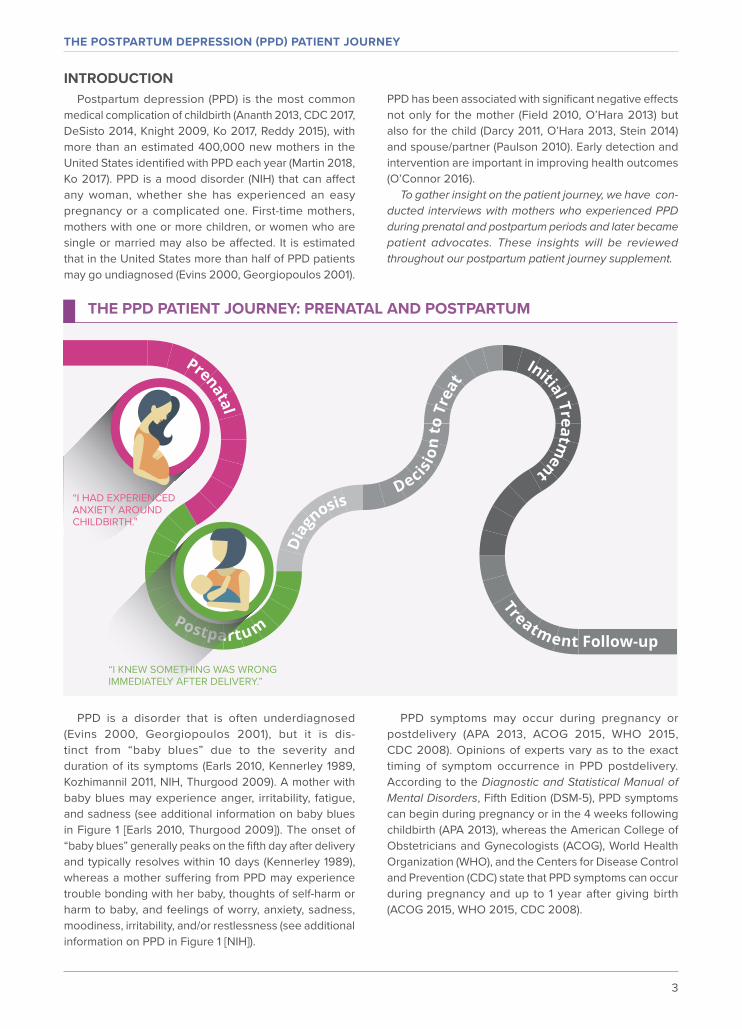
INTRODUCTIONPostpartum depression (PPD) is the most common
medical complication of childbirth (Ananth 2013, CDC 2017, DeSisto 2014, Knight 2009, Ko 2017, Reddy 2015), with more than an estimated 400,000 new mothers in the United States identified with PPD each year (Martin 2018, Ko 2017). PPD is a mood disorder (NIH) that can affect any woman, whether she has experienced an easy pregnancy or a complicated one. First-time mothers, mothers with one or more children, or women who are single or married may also be affected. It is estimated that in the United States more than half of PPD patients may go undiagnosed (Evins 2000, Georgiopoulos 2001).
PPD symptoms may occur during pregnancy or postdelivery (APA 2013, ACOG 2015, WHO 2015, CDC 2008). Opinions of experts vary as to the exact timing of symptom occurrence in PPD postdelivery. According to the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5), PPD symptoms can begin during pregnancy or in the 4 weeks following childbirth (APA 2013), whereas the American College of Obstetricians and Gynecologists (ACOG), World Health Organization (WHO), and the Centers for Disease Control and Prevention (CDC) state that PPD symptoms can occur during pregnancy and up to 1 year after giving birth (ACOG 2015, WHO 2015, CDC 2008).
PPD is a disorder that is often underdiagnosed (Evins 2000, Georgiopoulos 2001), but it is dis-tinct from “baby blues” due to the severity and duration of its symptoms (Earls 2010, Kennerley 1989, Kozhimannil 2011, NIH, Thurgood 2009). A mother with baby blues may experience anger, irritability, fatigue, and sadness (see additional information on baby blues in Figure 1 [Earls 2010, Thurgood 2009]). The onset of “baby blues” generally peaks on the fifth day after delivery and typically resolves within 10 days (Kennerley 1989), whereas a mother suffering from PPD may experience trouble bonding with her baby, thoughts of self-harm or harm to baby, and feelings of worry, anxiety, sadness, moodiness, irritability, and/or restlessness (see additional information on PPD in Figure 1 [NIH]).
PPD has been associated with significant negative effects not only for the mother (Field 2010, O’Hara 2013) but also for the child (Darcy 2011, O’Hara 2013, Stein 2014) and spouse/partner (Paulson 2010). Early detection and intervention are important in improving health outcomes (O’Connor 2016).
To gather insight on the patient journey, we have con-ducted interviews with mothers who experienced PPD during prenatal and postpartum periods and later became patient advocates. These insights will be reviewed throughout our postpartum patient journey supplement.
“I HAD EXPERIENCED ANXIETY AROUND CHILDBIRTH.”
“I KNEW SOMETHING WAS WRONG IMMEDIATELY AFTER DELIVERY.”
THE PPD PATIENT JOURNEY: PRENATAL AND POSTPARTUM
THE POSTPARTUM DEPRESSION (PPD) PATIENT JOURNEY
THE POSTPARTUM DEPRESSION (PPD) PATIENT JOURNEY
4
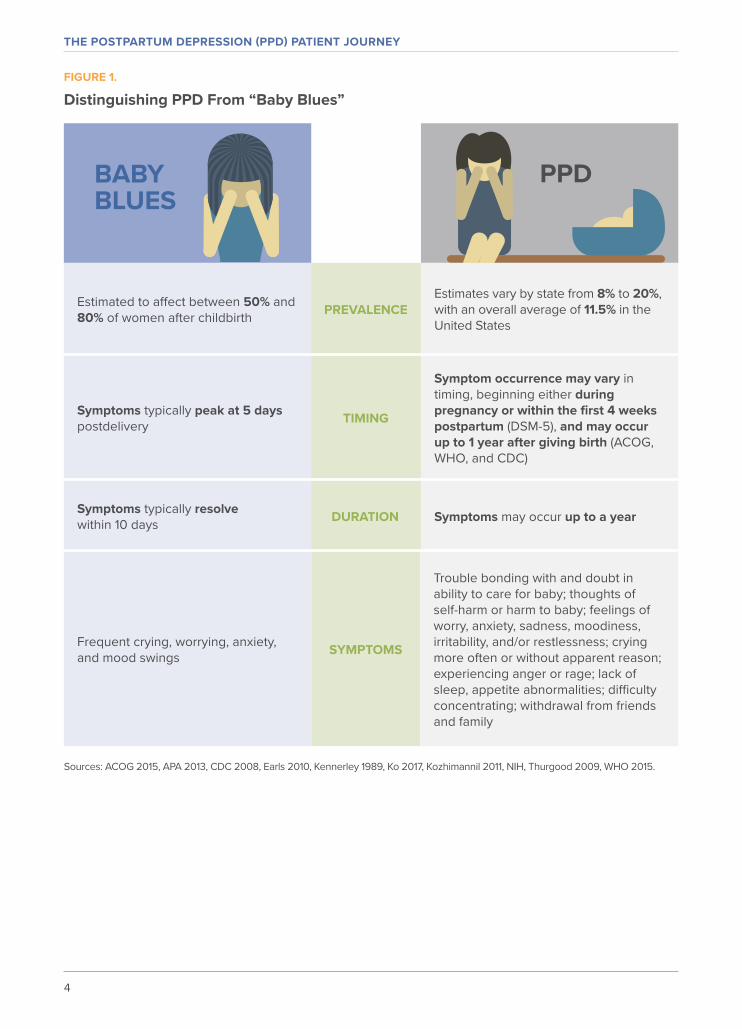
FIGURE 1.
Distinguishing PPD From “Baby Blues”
Sources: ACOG 2015, APA 2013, CDC 2008, Earls 2010, Kennerley 1989, Ko 2017, Kozhimannil 2011, NIH, Thurgood 2009, WHO 2015.
PREVALENCE
TIMING
DURATION
SYMPTOMS
Estimates vary by state from 8% to 20%, with an overall average of 11.5% in the United States
Symptom occurrence may vary in timing, beginning either during pregnancy or within the first 4 weeks postpartum (DSM-5), and may occur up to 1 year after giving birth (ACOG, WHO, and CDC)
Symptoms may occur up to a year
Trouble bonding with and doubt in ability to care for baby; thoughts of self-harm or harm to baby; feelings of worry, anxiety, sadness, moodiness, irritability, and/or restlessness; crying more often or without apparent reason; experiencing anger or rage; lack of sleep, appetite abnormalities; difficulty concentrating; withdrawal from friends and family
Estimated to affect between 50% and 80% of women after childbirth
Symptoms typically peak at 5 days postdelivery
Symptoms typically resolve within 10 days
Frequent crying, worrying, anxiety, and mood swings
BABY BLUES
PPD

5
FIGURE 2.
Additional PPD Risk Factors• Experienced stressful life events,
including child-care related stress • Difficult infant temperament• Mothers who are single or had an
unwanted pregnancy
While the exact cause of PPD is unknown, a combina-tion of factors may play a role (O’Hara 2014), including perinatal hormonal fluctuations, which may precipitate symptoms of PPD (Bloch 2000). Additionally, in animal models, data suggest links to the hypothalamic-pituitary-adrenal (HPA) axis and dysregulated γ-aminobutyric acid (GABA) signaling as underlying factors contributing to the pathophysiology of PPD (Melón 2017, Maguire 2008).
Emotional and social factors, such as past history of depression or anxiety, lack of social support, low socio-economic status, or a poor spousal or partner relationship, have been reported as risk factors for PPD (see additional risk factors shown in Figure 2 [O’Hara 2013, Stewart 2003]).
Source: O’Hara 2013.
THE PPD PATIENT JOURNEY: DIAGNOSIS
“I JUST DIDN’T FEEL RIGHT. MY HUSBAND HAD NOTICED A CHANGE IN ME AND ENCOURAGED ME TO CALL MY OB.”
“I HAD EXPERIENCED ANXIETY AROUND CHILDBIRTH.”
“I KNEW SOMETHING WAS WRONG IMMEDIATELY AFTER DELIVERY.”
THE POSTPARTUM DEPRESSION (PPD) PATIENT JOURNEY
6
Perinatal women have been reported to experience barriers, such as fear of stigma or being judged as an unfit mother, when discussing their mental health concerns with family and providers (Byatt 2013). We asked the patients we interviewed what feelings or challenges they faced when they sought out help and support from family, friends, and providers during their postpartum journey, and they reported the following: • Not feeling blissful over the birth of the child• Fearing how family and friends may view them
as mothers• Uncertainty about when to seek professional help • Confiding in family who assured them it was normal
to feel this way• Thinking the symptoms would go away on their own• Lack of comfort or being reluctant to voice their con-
cerns and feelings with family, friends, or physicians
The findings of our interviews were similar to those from a prior study (Byatt 2013) in which women were recruited through community organizations that provided education and advocacy support for perinatal women. Each participant was asked a series of open-ended questions about her experiences with perinatal depres-sion screening, management in obstetric settings, and her opinion on strategies that could improve perinatal depression care in the obstetric setting (Byatt 2013).
The barriers they faced were similar to the barriers expressed by patients we interviewed. Women in the focus group study reported (Byatt 2013):• Reluctant or “terrified” to acknowledge mental
health concerns to family, friends, or healthcare professionals due to shame, guilt, and pressure to be a “super-mother” who can “do it all”
• Fear of potential consequences—including hospitalization—due to admitting thoughts of harming themselves or their children
• Lack of partner support and judgmental comments by partners, friends, or family
• Potential disapproval from family members or society, which decreased the participant’s likelihood of seeking help
• Lack of education for the mother and partner about perinatal depression during perinatal care
• Lack of access to treatment or knowledge about where to seek it
• Barriers to available treatment options; multiple participants felt they were offered very narrow treatment options
• Lack of communication on treatment options; participants who were screened for perinatal depression felt the screening had limited utility and did not encourage engagement in treatment
THE PPD PATIENT JOURNEY PERSPECTIVE: THE FEAR OF FAILING
Among the patients interviewed, there was a common theme of fear of failing as a mother, including:
Concerns that the birth plan was not aligning correctly, including having a safe delivery
Concerns regarding ability to successfully breastfeed
Concerns about the newborn’s failure to thrive
“MOTHERS CONSIDER THEMSELVES A FAILURE
IF THINGS DON’T GO ACCORDING TO PLAN”

7
Screenings have been recommended both during pregnancy and postpartum to help identify women with PPD so healthcare professionals can provide appropri-ate treatment at the optimal time (ACOG 2015, USPSTF 2016). To support postpartum follow-up care, there is a Physician Quality Reporting System (PQRS) measure, which is part of the National Quality Strategy Domain: Communication and Care Coordination. The measure evaluates the percentage of patients who gave birth during a 12-month period, who were seen for postpartum care within 8 weeks of giving birth, and who received postpartum care services. These care services include a breastfeeding evaluation and education, postpartum depression screening, postpartum glucose screening for gestational diabetes, and family and contraceptive planning. One option for potentially improving quality of
care for mothers during their postpartum care follow-up appointments is to implement this measure (PQRS 2016).
Opportunities for PPD screening can present at both the mother’s prenatal and postpartum visits (ACOG 2015). Postpartum visits are generally conducted by obstetricians, family physicians, and nurse midwives.
In the focus group that Byatt et al documented, women felt more empowered to speak about their feelings and experiences among healthcare professionals who were supportive. It helped the participants “feel strong, gave them a sense of relief, and allowed for healing” (Byatt 2013). Our findings echoed that conclusion —the patients we interviewed saw various providers within the first year of their child’s life and felt that they were more open to talking about their symptoms with providers with whom they felt most connected and comfortable.
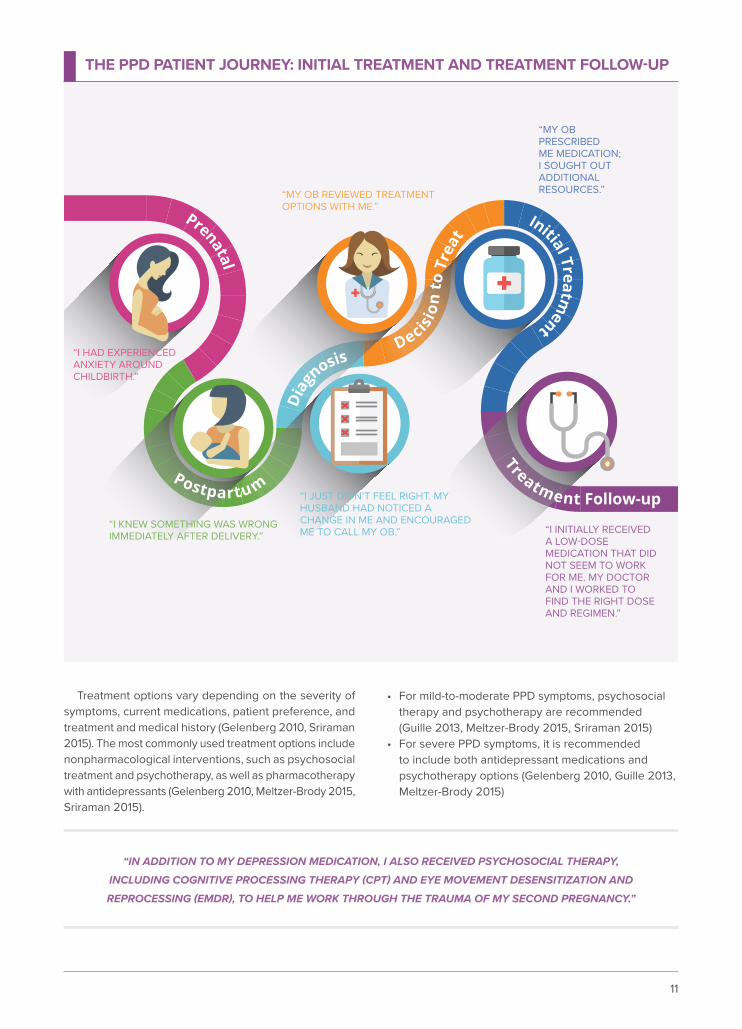
THE PPD PATIENT JOURNEY: DECISION TO TREAT
“MY OB REVIEWED TREATMENT OPTIONS WITH ME.”
“I JUST DIDN’T FEEL RIGHT. MY HUSBAND HAD NOTICED A CHANGE IN ME AND ENCOURAGED ME TO CALL MY OB.”
“I HAD EXPERIENCED ANXIETY AROUND CHILDBIRTH.”
“I KNEW SOMETHING WAS WRONG IMMEDIATELY AFTER DELIVERY.”
“WE NEED TO TELL WOMEN IT IS NOT A SIGN OF WEAKNESS TO ASK FOR HELP; IT’S A SIGN OF STRENGTH, THAT YOU CAN RECOGNIZE SOMETHING IS WRONG AND YOU NEED HELP TO TAKE CARE
OF YOUR BABY, AND THERE ARE STEPS YOU NEED TO TAKE IN ORDER TO DO THAT.”
– POSTPARTUM SUPPORT VIRGINIA
THE POSTPARTUM DEPRESSION (PPD) PATIENT JOURNEY
8
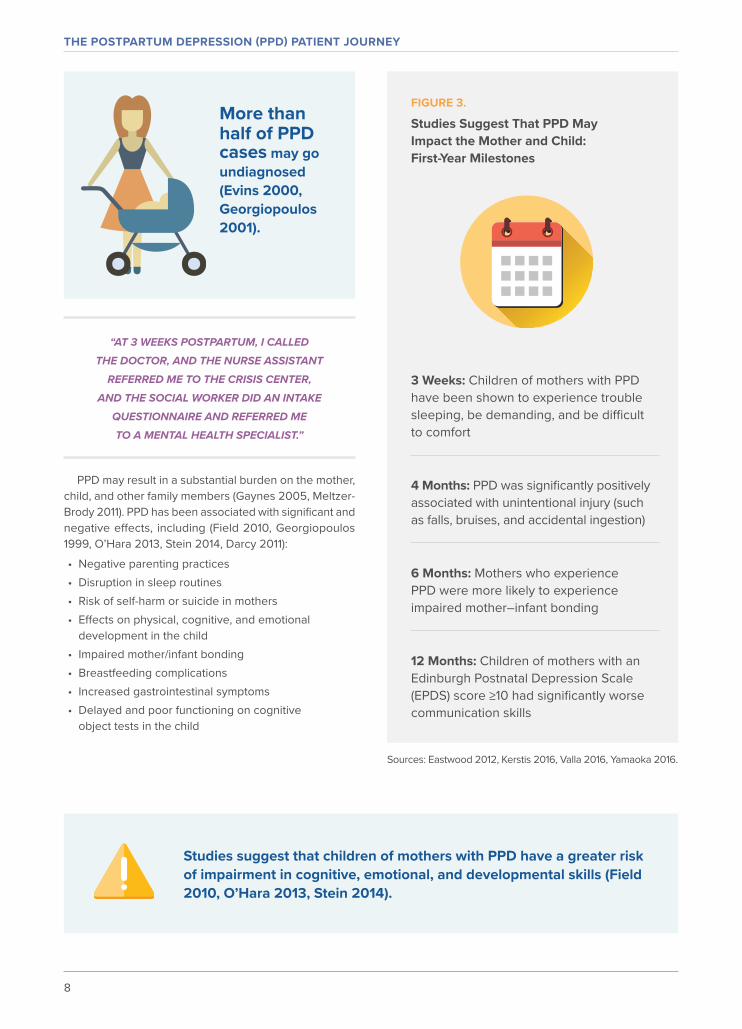
FIGURE 3.
Studies Suggest That PPD May Impact the Mother and Child: First‑Year Milestones
3 Weeks: Children of mothers with PPD have been shown to experience trouble sleeping, be demanding, and be difficult to comfort
4 Months: PPD was significantly positively associated with unintentional injury (such as falls, bruises, and accidental ingestion)
6 Months: Mothers who experience PPD were more likely to experience impaired mother–infant bonding
12 Months: Children of mothers with an Edinburgh Postnatal Depression Scale (EPDS) score ≥10 had significantly worse communication skills
“AT 3 WEEKS POSTPARTUM, I CALLED THE DOCTOR, AND THE NURSE ASSISTANT
REFERRED ME TO THE CRISIS CENTER, AND THE SOCIAL WORKER DID AN INTAKE
QUESTIONNAIRE AND REFERRED ME TO A MENTAL HEALTH SPECIALIST.”
More thanhalf of PPD cases may go undiagnosed (Evins 2000, Georgiopoulos 2001).
PPD may result in a substantial burden on the mother, child, and other family members (Gaynes 2005, Meltzer-Brody 2011). PPD has been associated with significant and negative effects, including (Field 2010, Georgiopoulos 1999, O’Hara 2013, Stein 2014, Darcy 2011):• Negative parenting practices• Disruption in sleep routines• Risk of self-harm or suicide in mothers• Effects on physical, cognitive, and emotional
development in the child• Impaired mother/infant bonding• Breastfeeding complications• Increased gastrointestinal symptoms• Delayed and poor functioning on cognitive
object tests in the child
Studies suggest that children of mothers with PPD have a greater risk of impairment in cognitive, emotional, and developmental skills (Field 2010, O’Hara 2013, Stein 2014).
Sources: Eastwood 2012, Kerstis 2016, Valla 2016, Yamaoka 2016.

9
A recent observational study published in JAMA Psychiatry of 9848 women with PPD and 8287 children found that children of women with persistent and severe depression are at an increased risk for behavioral prob-lems by 3.5 years of age and have a greater chance of developing depression during adolescence. Additionally,
the study found that women with persistent or unresolved PPD are more likely to experience depressive symptoms until at least 11 years after childbirth (Netsi 2018).
PPD also has a negative impact on the mental health of both the mother and her partner (Georgiopoulos 1999, Paulson 2010).
Among the patients interviewed, each had a different experience with her child and faced some internal challenges and issues within herself.
THE PPD PATIENT JOURNEY PERSPECTIVE: MOTHER AND BABY RELATIONSHIP
“ I did not feel connected to my child; I would often question why I had this other child, if I was unable to bond with him. I often found myself feeling that I did not like him, because he was constantly crying. I look back during his first year, and there are many milestones I can’t remember. ”
“ PPD did prevent me from bonding with my child; my symptoms would often prevent me from getting out of bed, bathing myself and my child, unable to communicate how I was feeling and how much I was struggling. ”
“ I felt confused on who this infant was to me, I had no joy after the birth. I felt feelings of rage, irritation, and agitation, just felt like I couldn’t keep it together. ”
“ I felt super protective over my daughter, but I often found myself having a sense of fear holding her and a constant disconnecting bond with her. My husband noticed and stepped in and took over the bonding relationship I was unable to give at the time. ”
“IT TOOK ME ABOUT 2 MONTHS BEFORE I FELT A CONNECTION
WITH MY SON. WHILE I STILL TOOK CARE OF HIM ALONG WITH CAREGIVERS, I JUST DIDN’T FEEL
THE JOY OR CONNECTION.”

THE POSTPARTUM DEPRESSION (PPD) PATIENT JOURNEY
10
Among the patients interviewed, there was a mixed response about returning to work or staying home with the baby; each respondent had a different experience.
THE PPD PATIENT JOURNEY PERSPECTIVE: RETURNING TO WORK VERSUS STAYING HOME
“I KNEW I HAD TO WORK, BUT I DID NOT WANT TO. I WAS
EXTREMELY FRUSTRATED AND TIRED, BUT I KNEW I HAD TO WORK FOR MY CHILDREN.”
“I DID NOT RETURN TO MY PREVIOUS EMPLOYER. AFTER MY DIAGNOSIS AND TREATMENT, I KNEW THIS WOULD BE LIFE-CHANGING IN MANY WAYS,
INCLUDING MY CAREER.”
“I RETURNED TO WORK AFTER MY FIRSTBORN, BUT WITH MY SECOND PREGNANCY, I DECIDED NOT TO RETURN. I FELT LIKE MY MEDICATION
WAS GETTING ON THE RIGHT TRACK, AND I DID NOT WANT TO RISK ANY SETBACK IN MY HEALTH. I KNEW BACK THEN IT WAS THE BEST DECISION
AT THE TIME FOR MY CHILD AND ME. I HAVE NO REGRETS.”
“I HAD POSTPONED MY RETURN TO WORK. WHEN I DID RETURN WITH SUPPORT FROM MY FAMILY AND MY EMPLOYER, I RETURNED AS A PART-TIME EMPLOYEE. I NEEDED MORE TIME TO ADJUST BACK
INTO THE ROLE AND PROPERLY HEAL MYSELF, AS I WAS STILL SUFFERING FROM PPD.”
11
Treatment options vary depending on the severity of symptoms, current medications, patient preference, and treatment and medical history (Gelenberg 2010, Sriraman 2015). The most commonly used treatment options include nonpharmacological interventions, such as psychosocial treatment and psychotherapy, as well as pharmacotherapy with antidepressants (Gelenberg 2010, Meltzer-Brody 2015, Sriraman 2015).
“MY OB PRESCRIBED ME MEDICATION; I SOUGHT OUT ADDITIONAL RESOURCES.”
“I INITIALLY RECEIVED A LOW-DOSE MEDICATION THAT DID NOT SEEM TO WORK FOR ME. MY DOCTOR AND I WORKED TO FIND THE RIGHT DOSE AND REGIMEN.”
THE PPD PATIENT JOURNEY: INITIAL TREATMENT AND TREATMENT FOLLOW-UP
“IN ADDITION TO MY DEPRESSION MEDICATION, I ALSO RECEIVED PSYCHOSOCIAL THERAPY, INCLUDING COGNITIVE PROCESSING THERAPY (CPT) AND EYE MOVEMENT DESENSITIZATION AND REPROCESSING (EMDR), TO HELP ME WORK THROUGH THE TRAUMA OF MY SECOND PREGNANCY.”
• For mild-to-moderate PPD symptoms, psychosocial therapy and psychotherapy are recommended (Guille 2013, Meltzer-Brody 2015, Sriraman 2015)
• For severe PPD symptoms, it is recommended to include both antidepressant medications and psychotherapy options (Gelenberg 2010, Guille 2013, Meltzer-Brody 2015)
“MY OB REVIEWED TREATMENT OPTIONS WITH ME.”
“I JUST DIDN’T FEEL RIGHT. MY HUSBAND HAD NOTICED A CHANGE IN ME AND ENCOURAGED ME TO CALL MY OB.”
“I HAD EXPERIENCED ANXIETY AROUND CHILDBIRTH.”
“I KNEW SOMETHING WAS WRONG IMMEDIATELY AFTER DELIVERY.”

A 2014 Cochrane review assessed the effectiveness of antidepressants in comparison with other treatment (pharmacologic and nonpharmacologic), placebo, or treat-ment as usual for postnatal depression. While the review found that women with postnatal depression who were treated with selective serotonin reuptake inhibitors (SSRIs) were more likely to improve or recover than those given placebo, the quality of evidence was determined to be low,
partially due to the small number of studies and the risk of bias identified in the included studies. The review also reports a lack of long-term safety data. Similar acknowledg-ments are made by multiple treatment guidelines, which state that the evidence for the safety of current PPD phar-macotherapies, particularly SSRIs, during breastfeeding is limited (Molyneaux 2014, APA 2001, ADAA, Hirst 2010).
FIGURE 4.
Current Pharmacologic Therapy Options for PPD
MAOIs=monoamine oxidase inhibitors; SNRIs=serotonin-norepinephrine reuptake inhibitors; SSRIs=selective serotonin reuptake inhibitors. Sources: Gelenberg 2010, Molyneaux 2014.
Currently, there are no FDA‑approved treatments for PPD.
12
THE POSTPARTUM DEPRESSION (PPD) PATIENT JOURNEY
While data to support antidepressants in PPD are limited, SSRIs are the most commonly used pharmacologic treatment for PPD

13
In August, our next installment of the Patient
Journey and Management Challenges of PPD
will focus on the obstetrician–gynecologist
perspective. This supplement will highlight the
needs for systematic screening and diagnosis,
as well as more timely and appropriate treatment
for patients with PPD.
We would like to thank the patient advocacy groups for their insights on
the patient journey perspective. These contributors include: A Mother’s
Sanctuary (AMS), Moms Mental Health Initiative, Postpartum Support
Charleston, and Postpartum Support Virginia.
CONCLUSIONIn summary, PPD is the most common medical
complication of childbirth (Ananth 2013, CDC 2017, DeSisto 2014, Knight 2009, Ko 2017, Reddy 2015), is associated with significant negative effects not only on the mother but the whole family (Darcy 2011, Field 2010, O’Hara 2013, Paulson 2010, Stein 2014), and diagnosis rates still remain low (Evins 2000, Georgiopoulos 2001). There is still an unmet need in PPD education; this need for increased awareness for PPD is reinforced by our patient interviews.
It is important to reduce the social stigma of PPD; as a final interview question we asked the patients, “if they could change their experience with PPD, what would they have done differently?”
• “I would have taken medication a lot sooner.”• “Be more prepared, know the risk factors, have
more education on PPD, and be more aggressive when to seek better care.”
• “I would not have secluded myself as much, and I would have communicated my feelings much sooner.”
Encouraging communication, education, and awareness of PPD may help improve patient outcomes as patients navigate their postpartum journey.
THE POSTPARTUM DEPRESSION (PPD) PATIENT JOURNEY
14
REFERENCESAnxiety and Depression Association of America. Postpartum depression. https://adaa.org/living-with-anxiety/women/postpartum-depression. Accessed February 7, 2018.
American Academy of Pediatrics Committee on Drugs. The transfer of drugs and other chemicals into human milk. Pediatrics. 2001;108(3):776-789.
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. Arlington, VA: American Psychiatric Association; 2013.
Ananth CV, Keyes KM, Wapner RJ. Pre-eclampsia rates in the United States, 1980-2010: age-period-cohort analysis. BMJ. 2013;347:1-9.
Bloch M, Schmidt PJ, Danaceau M, Murphy J, et al. Effects of gonadal steroids in women with a history of postpartum depression. Am J Psychiatry. 2000;157(6):924-930.
Byatt N, Biebel K, Friedman L, Debordes-Jackson G, Ziedonis D, Pbert L. Patient’s views on depression care in obstetric settings: how do they compare to the views of perinatal health care professionals? Gen Hosp Psychiatry. 2013;35(6):598-604.
Centers for Disease Control and Prevention. Pregnancy mortality surveillance system. https://www.cdc.gov/reproductivehealth/maternalinfanthealth/pmss.html. Accessed February 7, 2018.
Centers for Disease Control and Prevention. Prevalence of self-reported postpartum depressive symptoms—17 states, 2004-2005. https://www.cdc.gov/Mmwr/preview/mmwrhtml/ mm5714a1.htm. Accessed February 7, 2018.
Committee on Obstetric Practice. The American College of Obstetricians and Gynecologists Committee opinion no. 630: screening for perinatal depression. Obstet Gynecol. 2015;125(5):1268-1271. https://www.acog.org/-/media/Committee-Opinions/Committee-on-Obstetric-Practice/co630.pdf?dmc=1. Accessed February 7, 2018.
Darcy JM, Grzywacz JG, Stephens RL, Leng I, Clinch CR, Arcury TA. Maternal depressive symptomatology: 16-month follow-up of infant and maternal health-related quality of life. J Am Board Fam Med. 2011;24(3):249-257.
DeSisto CL, Kim SY, Sharma AJ. Prevalence estimates of gestational diabetes mellitus in the United States, Pregnancy Risk Assessment Monitoring System (PRAMS), 2007-2010. https://www.cdc.gov/pcd/issues/2014/13_0415.htm. Accessed February 7, 2018.
Earls MF; Committee on Psychological Aspects of Child and Family Health, American Academy of Pediatrics. Incorporating recognition and management of perinatal and postpartum depression into pediatric practice. Pediatrics. 2010;126(5):1032-1039.
Eastwood JG, Jalaludin BB, Kemp LA, Phung HN, Barnett BEW. Relationship of postnatal depressive symptoms to infant temperament, maternal expectations, social support and other potential risk factors: findings from a large Australian cross-sectional study. BMC Pregnancy Childbirth. 2012;12(148):1-11.
Evins GG, Theofrastous JP, Galvin SL. Postpartum depression: a comparison of screening and routine clinical evaluation. Am J Obstet Gynecol. 2000;182(5):1080-1082.
Field T. Postpartum depression effects on early interactions, parenting, and safety practices: a review. Infant Behav Dev. 2010;33(1):1-6.
Freeman MP, Joffe H, Cohen LS. Postpartum depression: help patients find the right treatment. Current Psychiatry. 2012;11(11):14-21.
Gaynes BN, Gavin N, Meltzer-Brody S, et al. Perinatal depression: prevalence, screening accuracy, and screening outcomes. Evid Rep Technol Assess (Summ). 2005:(119):1-8.
Gelenberg AJ, Freeman MP, Markowitz JC, et al. Practice Guideline for the Treatment of Patients With Major Depressive Disorder. 3rd ed. Arlington, VA: American Psychiatric Association; 2010. https://psychiatryonline.org/pb/assets/raw/sitewide/practice_guidelines/guidelines/mdd.pdf. Accessed February 7, 2018.
Georgiopoulos AM, Bryan TL, Wollan P, Yawn BP. Routine screening for postpartum depression. J Fam Pract. 2001;50(02):117-122.
Georgiopoulos AM, Bryan TL, Yawn BP, Houston MS, Rummans TA, Therneau TM. Population-based screening for postpartum depression. Obstet Gynecol. 1999;93(5):653-657.
Guille C, Newman R, Fryml LD, Lifton CK, Epperson CN. Management of postpartum depression. J Midwifery Womens Health. 2013;58(6):643-653.
Hirst KP, Moutier CY. Postpartum major depression. Am Fam Physician. 2010;82(8):926-933.
Kennerley H, Gath D. Maternity Blues. I. Detection and measurement by questionnaire. Br J Psychiatry. 1989;155:356-362.
Kerstis B, Aarts C, Tillman C, et al. Association between parental depressive symptoms and impaired bonding with the infant. Arch Womens Ment Health. 2016;19(1):87-94.
Knight M, Callaghan WM, Berg C, et al. Trends in postpartum hemorrhage in high resource countries: a review and recommendations from the International Postpartum Hemorrhage Collaborative Group. BMC Pregnancy Childbirth. 2009;9(55):1-10.
Ko JY, Rockhill KM, Tong VT, Morrow B, Farr SL. Trends in postpartum depressive symptoms—27 states, 2004, 2008, and 2012. MMWR. 2017;66(6):153-156. https://www.cdc.gov/mmwr/volumes/66/wr/mm6606a1.htm. Accessed February 7, 2018.
Kozhimannil KB, Adams AS, Soumerai SB, Busch AB, Huskamp HA. New Jersey’s efforts to improve postpartum depression care did not change treatment patterns for women on Medicaid. Health Aff (Millwood). 2011;30(2):293-301.
Maguire J, Mody I. GABA(A)R plasticity during pregnancy: relevance to postpartum depression. Neuron. 2008;59(2):207-213.
Martin JA, Hamilton BE, Osterman MJK, Driscoll AK, Drake MS. Births: final data for 2016. Natl Vital Stat Rep. 2018;67(1):1-55. https://www.cdc.gov/nchs/data/nvsr/nvsr67/nvsr67_01.pdf. Accessed February 7, 2018.
15
Melón LC, Hooper A, Yang X, Moss SJ, Maguire J. Inability to suppress the stress-induced activation of the HPA axis during the peripartum period engenders deficits in postpartum behaviors in mice. Psychoneuroendocrinology. 2017;1-12.
Meltzer-Brody S. New insights into perinatal depression: pathogenesis and treatment during pregnancy and postpartum. Dialogues Clin Neurosci. 2011;13(1):89-100.
Meltzer-Brody S, Jones I. Optimizing the treatment of mood disorders in the perinatal period. Dialogues Clin Neurosci. 2015;17(2):207-218.
Molyneaux E, Howard LM, McGeown HR, Karla AM, Trevillion K. Antidepressant treatment for postnatal depression. Cochrane Database Systematic Revs. 2014;(9):CD002018.
National Institute of Mental Health (NIMH). Postpartum depression facts. https://www.nimh.nih.gov/health/publications/postpartum-depression-facts/postpartum-depression-brochure_146657.pdf. Accessed February 7, 2018.
Netsi E, Pearson RM, Murray L, Cooper P, Craske MG, Stein A. Association of persistent and severe postnatal depression with child outcomes. JAMA Psychiatry. 2018;75(3):247-253.
O’Connor E, Rossom RC, Henninger M, Groom HC, Burda BU. Primary care screening for and treatment of depression in pregnant and postpartum women: evidence report and systematic review for the US Preventive Services Task Force. JAMA. 2016;315(4):388-406.
O’Hara MW, McCabe JE. Postpartum depression: current status and future directions. Annu Rev Clin Psychol. 2013;9:379-407.
O’Hara MW, Wisner KL. Perinatal mental illness: definition, description, and aetiology. Best Pract Res Clin Obstet Gynaecol. 2014;28(1):3-12.
Paulson JF, Bazemore SD. Prenatal and postpartum depression in fathers and its association with maternal depression. JAMA. 2010;303(19):1961-1969.
Physician Quality Reporting System (PQRS). Measure #336: Maternity care: post-partum follow-up and care coordination—national quality strategy domain: communication and care coordination. https://pqrsregistry.clinicspectrum.com/2016/individual_measures/336.pdf. Accessed February 7, 2018.
Reddy UM, Murguia M, Grobman WA, et al. Serious maternal complications after early preterm delivery (24-33 weeks’ gestation). Am J Obstet Gynecol. 2015;213(4):538.e1-9.
Sriraman NK, Melvin K, Meltzer-Brody S; Academy of Breastfeeding Medicine. ABM clinical protocol #18: use of antidepressants in breastfeeding mothers. Breastfeed Med. 2015;10(6):290-299.
Stein A, Pearson RM, Goodman SH, et al. Effects of perinatal mental disorders on the fetus and child. Lancet. 2014;384(9956):1800-1819.
Stewart DE, Robertson E, Dennis CL, Grace SL, Wallington T. Postpartum depression: literature review of risk factors and interventions. http://www.who.int/mental_health/prevention/ suicide/lit_review_postpartum_depression.pdf. Accessed February 7, 2018.
Thurgood S, Avery DM, Williamson L. Postpartum depression (PPD). Am J Clin Med. 2009;6(2):17-22.
US Preventive Services Task Force. Depression in adults: screening. https://www.uspreventiveservicestaskforce.org/Page/Document/RecommendationStatementFinal/depression-in-adults-screening1. January 2016. Accessed February 7, 2018.
Valla L, Wentzel-Larsen T, Smith L, Skogbrott Birkeland M, Slinning K. Association between maternal postnatal depressive symptoms and infants’ communication skills: a longitudinal study. Infant Behav Dev. 2016;45:83-90.
World Health Organization. Maternal mental health. http://www.who.int/mental_health/maternal-child/maternal_mental_health/en/. Accessed February 7, 2018.
Yamaoka Y, Fujiwara T, Tamiya N. Association between maternal postpartum depression and unintentional injury among 4-month-old infants in Japan. Matern Child Health J. 2016;20(2):326-336.

16
THE POSTPARTUM DEPRESSION (PPD) PATIENT JOURNEY
© 2018 Sage Therapeutics, Inc. 05/18 PP-US-PPD-0001