Embed Size (px)
Citation preview
THE PIERRE-ROBIN SYNDROME: A SURGICAL EMERGENCY
IN THE NEONATAL PERIOD
By R. T. ROUTLEDGE, F.R.C.S.
Department of Plastic and Jaw Surgery, Frenchay Hospital, Bristol
A CONGENITAL abnormality, which can provide eighteen major examples in one plastic surgery department over a period of five years, may reasonably be considered to be uncommon, but hardly rare enough to account for the dearth of clinical papers written on the subject in British medical literature. An exhaustive search through the literature has revealed two short papers in the Lancet, one written in I937 and the other in I947, and one rather more comprehensive paper in the British Journal of Plastic Surgery, though the last: concerned only two such cases. It would seem reasonable to suppose that the Pierre-Robin syndrome, though well recognised in this country, is not sufficiently well known as the killer it can be in the neonatal period. A glance at the statistics, in this department shows that the number of cases admitted annually has increased each year, and I believe that this mirrors an increasing awareness of the condition, particularly amongst pa:diatricians in the region. What success we have had in the treatment of this condition will, we hope, encourage the belief that something active can be done to help these unfortunate infants, and it is to be expected that, as a result, more cases will be referred. It seemed to be time, therefore, to collect what data we had on the subject, and to analyse our own experiences and results.
The syndrome of congenital, small, recessive mandible, usually associated with a cleft of the soft palate, and manifesting itself by respiratory embarrassment and difficulty in feeding, seems to have been referred to as the Pierre-Robin syndrome since that French clinician first published a paper on the subject in z923. In point of fact, the condition was described by Shukowsky twelve years earlier, and he mentioned surgical relief of symptoms by a method of tongue fixation. Pierre-Robin later published additional papers in the American literature and these appeared to stimulate considerable interest in the problem. A fair amount has been written about the condition in the medical literature of the United States, and most of our information stems from this source.
Pierre-Robin's case descriptions give the impression that the majority o f the infants under his care were relatively minor examples of the deformity, and the picture is clouded by references to the importance of adenoidal hypertrophy on the future of the children. He was the first, however, to stress the importance of the effect of gravity in relieving respiratory embarrassment. Lapage, writing in the Lancet in I937, paints a gloomy picture of surgical procedures on micrognathic infants, holding that bronchopneumonia inevitably follows the operation. He recommended postural treatment with the employment o f cumbersome wire splints to hold the mandible in a forward position. Such splints had been devised and used in America, and it had been claimed that this therapy was highly efficacious in the control of respiratory crises. A careful study of
204
THE P I E R R E - R O B I N S Y N D R O M E 205
micrognathic infants in this department makes it reasonably certain that, in order to control respiratory difficulty due to a small recessive mandible, by traction on the mandible itself, the condyles would need to be dislocated forward well out of the glenoid fossa~, and it is not reasonable to suppose that the inefficient, over-large wire contraptions fortunately ever did anything of the sort.
It was Beverley Douglas (I946, z95 o) who first presented a clear picture of the syndrome and its effects, and offered certain carefully considered ideas as to the cause of such effects. He, too, described an operation for the anterior fixation of the tongue which has been widely used by surgeons ever since, both in the United States and in this country. Douglas emphasises a feature of the condition that we have rarely observed. He found vomiting to be a pronounced symptom and mentions that sudden death, due to inhaled vomitus, occurs quite frequently. We have not had a death due to this cause, and have not found vomiting to be a frequent or a distressing complication. It is possible that the so-called vomiting attack is, in reality, an episode of choking during a feed with rejection of milk which has never got as far as being swallowed. Douglas reports a very low mortality in cases treated by operation. Indeed, in a second paper, he reports that none of a series of some twelve cases died.
Sweet and Kemsley, in a paper written in I947, present some interesting embryological theories, and they mention a fact which we too have noted--that not all cases of extreme micrognathos are associated with a cleft palate.
A comprehensive article by Kiskadden and Dietrich summarised the position up to z953. These writers report but few deaths in all cases treated in hospitals in the United States by operation, and no cases of pneumonia post-operatively. The impression given is that the Douglas operation is the complete answer to the problem, a conclusion which our own experiences have been unable to substantiate. Rather more mixed success with the Douglas operation was reported in ~958 by Benavent and Ramos-Oller.
Champion (I956) attacked the problem from another angle, and rather than attempt to control the tongue itself, he prefers to close the palatal cleft, believing that this is the key factor in the production of symptoms of respiratory distress. That it is a factor is unquestionable, but observations made in this department suggest that it is not the only factor. Champion does mention, as did May and Chun (z948), the presence in some cases of a tongue-tie, and this feature will be further elaborated, as we believe it can be of great importance.
This, then, summarises the data available to us when we began to treat cases of the Pierre-Robin syndrome who presented as surgical emergencies.
Method of Product ion of Symptoms.lln most of the publications on the Pierre-Robin syndrome, glossoptosis is a frequently employed term, and great play is made of the so-called ball-valve action of the tongue in the production of respiratory distress. Both these conceptions imply a paralytic, or at best, a static, state of the tongue and do not, we submit, give a true picture of the role of the tongue in the production of the respiratory crises associated with this condition. Though the mandible is excessively small, the tongue is normal (or in some cases large) for the size of the infant, and it is a very active organ. The trigger to many an episode of respiratory obstruction seems to be the impaction of the tongue tip
206 B R I T I S H JOURNAL OF P L A S T I C SURGERY
in the cleft of the palate. These tiny babies seem to have considerable difficulty in disengaging the tongue from the cleft, and the violent muscular contractions which result from their efforts to free the tongue bulge this organ up out of the oral cavity so that it acts as a cork in the bottleneck of the nasopharynx. All the symptoms of suffocation are shown until a degree of anoxia is reached where the tongue becomes limp and flaccid, and drops out of the nasopharynx, so restoring the airway. It is the self-limiting aspect of these episodes of complete obstruction
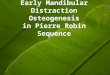
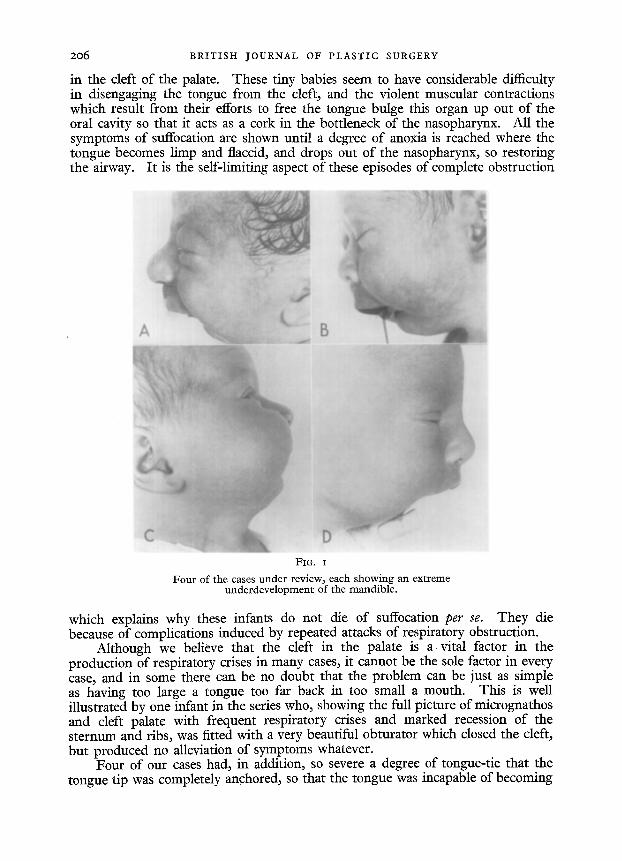
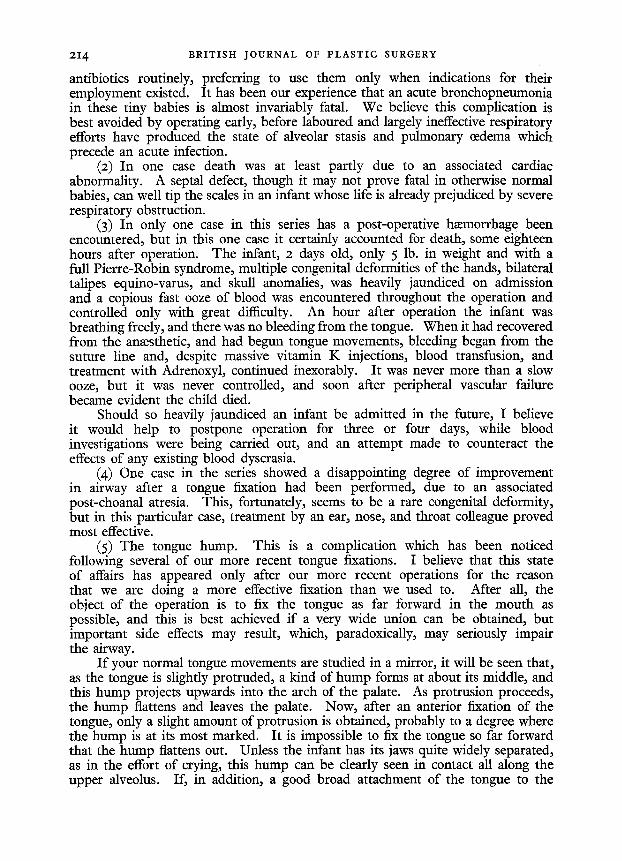
FIG. I
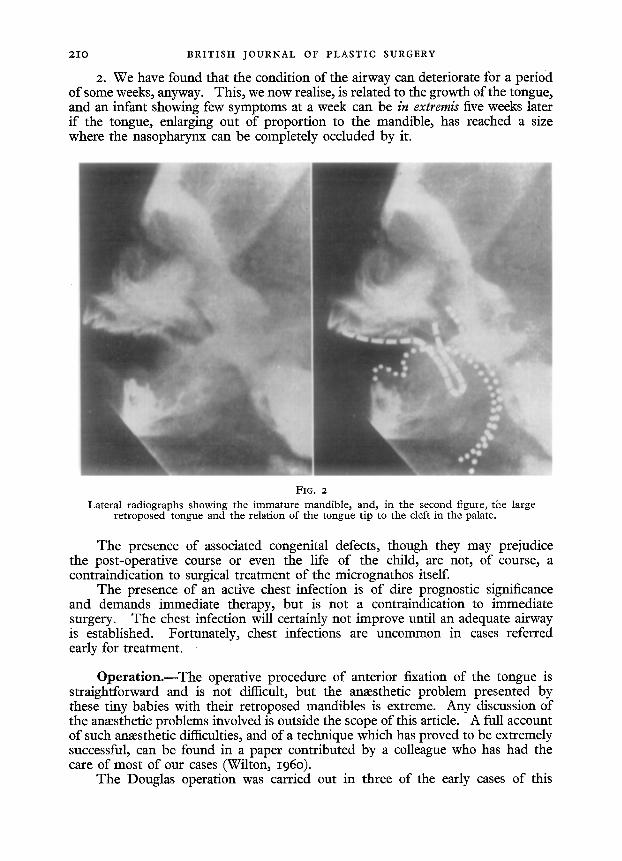
Four of the cases under review, each showing an cxtreme underdevelopment of the mandible.
which explains why these infants do not die of suffocation per se. They die because of complications induced by repeated attacks of respiratory obstruction.
Although we believe that the cleft in the palate is a vital factor in the production of respiratory crises in many cases, it cannot be the sole factor in every case, and in some there can be no doubt that the problem can be just as simple as having too large a tongue too far back in too small a mouth. This is well illustrated by one infant in the series who, showing the full picture of micrognathos and cleft palate with frequent respiratory crises and marked recession of the sternum and ribs, was fitted with a very beautiful obturator which dosed the cleft, but produced no alleviation of symptoms whatever.
Four of our cases had, in addition, so severe a degree of tongue-tie that the tongue t ip was completely anchored, so that the tongue was incapable of becoming
THE PIERRE-ROBIN SYNDROME 207
jammed in the cleft of the palate. Even so, all four cases exhibited episodes of severe respiratory obstruction.
It is mainly this uncertainty about the responsibility of the cleft palate in the production of respiratory obstruction in any particular case which has led us to believe that the focus of attention in surgical treatment should be on the tongue, and not on the palate. The tongue is always at fault ; the palate, often, but not always.
A further variable factor which profoundly affects the symptomatology is the relative size of the tongue. Pruzansky and Richmond (I954), basing their theories on careful X-ray cephalometric studies, postulated that a micrognathic deformity of itself is not sufficient to produce respiratory embarrassment unless the tongue is of normal or large size. A careful clinical study of our own cases leads us to the same conclusion, and one case in particular strongly supports such a theory. An infant, admitted at the age of one day, with a Pierre-Robin syndrome, remained perfectly well without any respiratory crises and with no feeding difficulties for over a fortnight. He was then transferred back to the maternity hospital, where he continued to progress satisfactorily for a little while. He was returned to this department at the age of 7 weeks, having repeated attacks of respiratory obstruction and cyanosis, with very marked sternal and costal recession, so that anterior fixation of the tongue became a matter of extreme urgency. It can only have been growth of the tongue that precipitated these severe symptoms. As far as the micrognathic deformity and cleft palate went, he was no worse off than when he was first admitted ; indeed, the jaw had probably grown a little. On his second visit, however, the tongue had grown to a size where it was now capable of causing a complete upper respiratory obstruction. It would appear probable, therefore, that an infant afflicted with this syndrome is better off if he happens to have a relatively small tongue.
Two of our patients had micrognathos without a cleft palate, but one had symptoms so slight that we were able to discharge her without treatment after a period of observation of a week, while the other infant, showing all the symptoms of a severe Pierre-Robin syndrome and operated on without relief of symptoms, was then discovered to have a congenital bilateral post-choanal atresia. Studies of a number of infants (not included in the present series) treated without operation at the Bristol Children's Hospital, who had congenitally small mandibles, but with intact palates, lead us to believe that symptoms of respiratory obstruction are unlikely to develop in such cases unless the deformity is of the most extreme degree.
Effect of Pos ture . - - I t is convenient to consider the effect of posture at this point, though it will entail anticipating some aspects which will be dealt with later.
In the untreated case posture alone has little effect in preventing attacks of respiratory distress, or in alleviating an attack which has already begun. Even when lying prone it is, of course, quite possible for an infant to get its tongue impacted in a cleft palate with consequent obstruction of the airway. However, with the tip of the tongue controlled, e.g., by an anterior fixation operation or with a tongue suture if operation has not yet been performed, postural treatment is of the utmost importance. It is, of course, of equal importance in the nursing of those cases of micrognathos which have an intact palate, where the milder
208 B R I T I S H JOURNAL OF P L A S T I C SURGERY
symptoms are due to reduction of the airway by a normal-sized tongue in a very small oral cavity. Here, the balance between an inadequate and an adequate airway is so fine that the slight gravity effect on the tongue, produced by turning the child, can make all the difference. We recommend, therefore, that these children are better nursed in a prone or semi-prone position.
Typical History of such a Case.--As a rule, these cases are referred for treatment once the diagnosis has been firmly established. Now that p~ediatricians xealise that something can be done for such infants, surgically, in the way of relief of symptoms, cases tend to be referred very early in life. Our youngest patient was aged 4 hours and the oldest was 6 weeks, but the average age of the infants on admission was around 7 to 9 days.
It should be noted, though, that three of the infants were first referred at the age of 6 weeks and we believe that these " late starters " can be explained by a disproportionate tongue growth producing a progressive increase in the severity of the symptoms during the first few weeks of life.
The story is fairly straightforward. There i s a history of cyanotic attacks with laboured respiration and marked recession of the sternum and ribs. Quite often, nursing staff or parents handling the child relate these attacks to feeds, and the question of a congenital tracheo-oesophageal fistula has then to be considered. The reason that the attacks appear to be related to feeds seems to be that extra muscular activity is demanded of the tongue during sucking, and the chance of an actively mobile tongue becoming fixed in thec le f t is much greater. The frequency with which these cyanotic attacks recur varies considerably from case to case and appears to bear little relation to the degree o f micrognathos. (It probably does bear a direct relation to the size of the tongue, however.)
First-aid Precautions during Transfer of Patients.mOnce the diagnosis is made and the decision taken to transfer the infant, it is sound policy to insert a stitch so that control of the tongue is maintained at all times. A suture of any fairly heavy non-absorbable material is passed through the full thickness of the tongue as far back as is possible. The usual experience is that when a stitch has been inserted, it is then possible to draw the tongue far enough forward to pass yet another suture even farther back. This suture is left long and anchored with artery forceps, and the first one may be removed.
In four cases we have encountered a complication which negatived effective action of a tongue suture. In cases where a severe degree of tongue-tie exists, the tip of the tongue is so tightly bound down to the lingual surface of the lower alveolus that pulling on the tongue stitch merely draws up the bulk of the tongue into the mouth and, if anything, only serves further to diminish the airway. In these cases it is essential to divide the tongue-tie. It is only necessary to split the tight band with a pair of scissors, completing the division by gentle digital pressure on the under surface of the tongue in a backward direction.
It is essential to transport the infant in the company of an experienced nurse, preferably one who has had training in the management of such small surgical patients. An oxygen tent may be needed on the ambulance trip.
Mouth-to-mouth inflation is the only effective method of artificial respiration, should the infant suffer an anoxic episode serious enough to demand this.
THE P I E R R E - R O B I N SYNDROME 209
Management on Arrival at Hospi ta l . - -A full clinical examination is carried out to assess the extent and type of deformity, and to determine the presence of associated congenital defects. Six of the patients in this series had associated defects, including congenital heart disease, bilateral talipes equino-varus, congenital anomalies of the skull, syndactyly of the fingers, and cerebral turnout. One case exhibited all the stigmata of achondroplasia. X-rays of the skull and iaw are of academic interest only, and the severity of the deformity is more accurately determined by clinical observation and assessment of the freedom of the airway in various postures of the child. I f any doubt exists as to the presence of a congenital tracheo-oesophageal fistula a simple and accurate check is provided by passing a soft rubber catheter through the nose into the oesophagus. I f a catheter can be so passed, it is highly unlikely that a tracheo-oesophageal fistula exists.
Associated post-choanal atresia is difficult to spot. The diagnosis is not usually considered until a good deal later when, anterior fixation of the tongue having been successfully obtained, a residual degree of upper respiratory obstruction persists. I f the condition is suspected, a few drops of lipiodol may be instilled into the nose and the child then X-rayed in the supine position. A post-choanal block will be evident if the lipiodol does not flow freely out of the nasal cavity into the nasopharynx.
It has been noted that, in those cases with more than moderate respiratory embarrassment, the infant takes up a typical posture. It will lie on its side with the head very considerably retracted, making convulsive movements of the tongue and all the accessory muscles of respiration. Costal and sternal recession is marked, and in one case which came to us after a lapse of some weeks, an actual moulding of the ribs had begun. In severe cases a degree of cyanosis persists, even when an acute respiratory crisis has passed.
Indications for Operat ion.- -Our ideas have changed as regards the indications for operation. At first it was believed that surgery should be withheld until, after a period of observation, sometimes of a few days' duration, it became evident that careful nursing by itself was not going to control sufficiently the tendency to severe cyanotic episodes. The reasons for such a belief were, ill the main, the following : - -
I. Any general anmsthetic and operative interference in such tiny, poorly ventilated infants carries a severe risk, and should not be lightly undertaken.
2. It was known that the symptoms were self-righting in time, and we felt that the infants would show a gradual improvement and must be at their very worst when we first saw them.
Now we believe that so long as the deformity is present and there is a reliable history of repeated cyanotic attacks, an operation is best performed at the earliest possible opportunity. Two factors have occasioned this reversal in procedure : - -
I. The longer these infants are exposed to repeated attacks of respiratory obstruction and what amounts, at the best, to subcyanotic intervening periods, the more likely they are to develop an acute chest infection, which then tips the scales very heavily against them. Even with babies fortunate enough to avoid this complication it has been our experience that they fail to gain in weight and fail to thrive in spite of apparently adequate feeding.
3 B
.210 BRITISH JOURNAL OF PLASTIC SURGERY
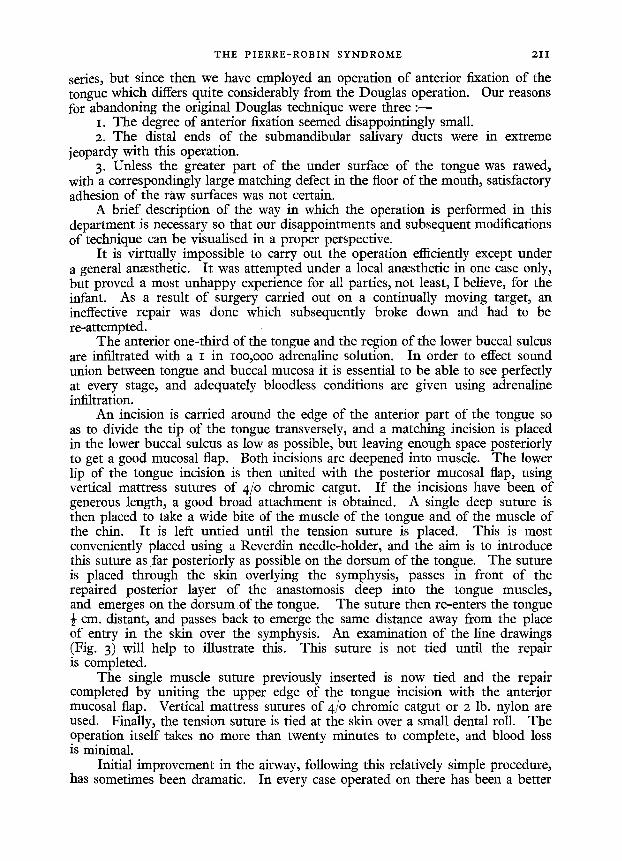
2. We have found that the condition of the airway can deteriorate for a period of some weeks, anyway. This, we now realise, is related to the growth of the tongue, and an infant showing few symptoms at a week can be in extremis five weeks later if the tongue, enlarging out of proportion to the mandible, has reached a size where the nasopharynx can be completely occluded by it.
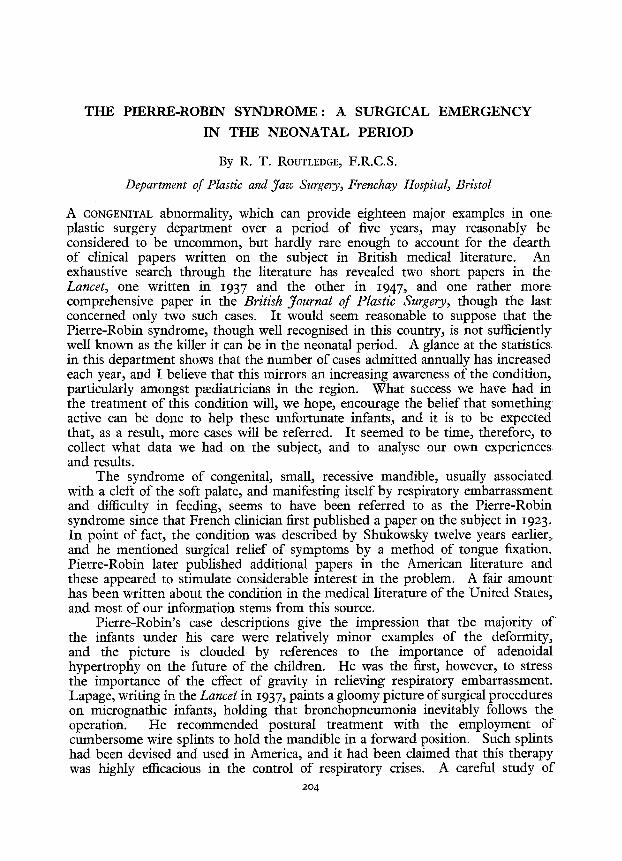
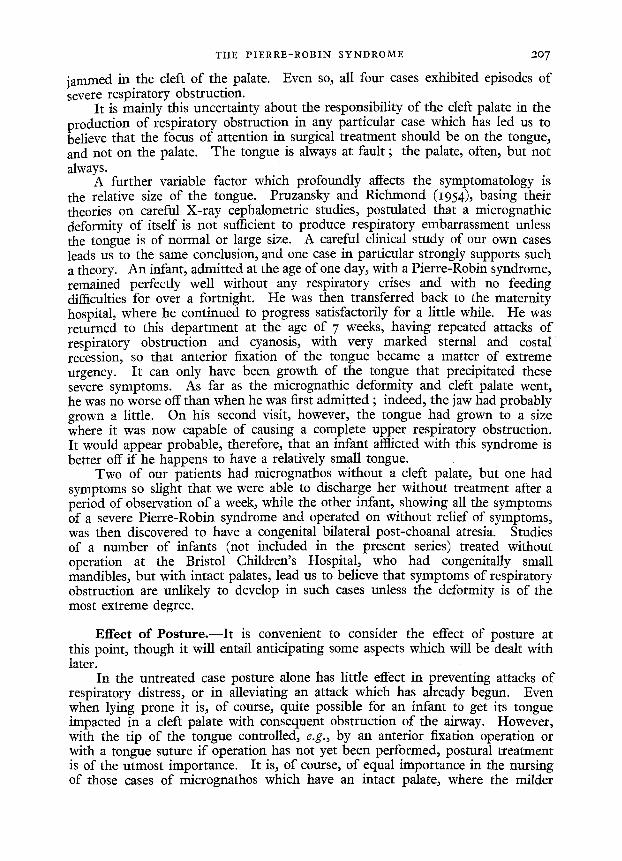
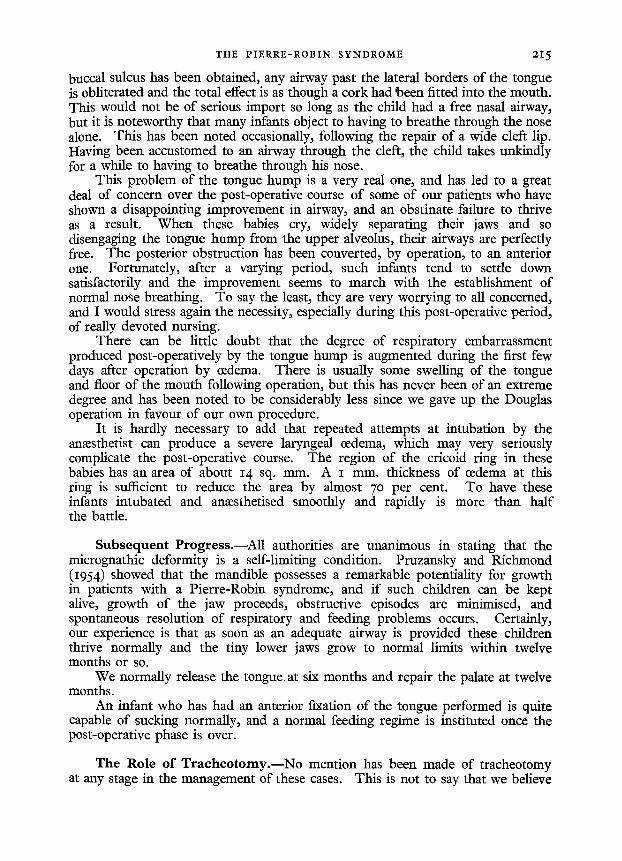
FIG. 2 Lateral radiographs showing the immature mandible, and, in the second figule~ the large
retroposed tongue and the relation of the tongue tip to the cleft in the palate.
The presence of associated congenital defects, though they may prejudice the post-operative course or even the life of the child, are not, of course, a contraindication to surgical treatment of the micrognathos itself.
The presence of an active chest infection is of dire prognostic significance and demands immediate therapy, but is not a contraindication to immediate surgery. The chest infection will certainly not improve until an adequate airway is established. Fortunately, chest infections are uncommon in cases referred early for treatment.
Operat ion.--The operative procedure of anterior fixation of the tongue is straightforward and is not difficult, but the anaesthetic problem presented by these tiny babies with their retroposed mandibles is extreme. Any discussion of the anaesthetic problems involved is outside the scope of this article. A full account of such anaesthetic difficulties, and of a technique which has proved to be extremely successful, can be found in a paper contributed by a colleague who has had the care of most of our cases (Wilton, 196o ).
The Douglas operation was carried out in three of the early cases of this
T H E P I E R R E - R O B I N S Y N D R O M E 2 I I
series, but since then we have employed an operation of anterior fixation of the tongue which differs quite considerably from the Douglas operation. Our reasons for abandoning the original Douglas technique were three : - -
I. The degree of anterior fixation seemed disappointingly small. 2. The distal ends of the submandibular salivary ducts were in extreme
jeopardy with this operation. 3. Unless the greater part of the under surface of the tongue was tawed,
with a correspondingly large matching defect in the floor of the mouth, satisfactory adhesion of the raw surfaces was not certain.
A brief description of the way in which the operation is performed in this department is necessary so that our disappointments and subsequent modifications of technique can be visualised in a proper perspective.
It is virtually impossible to carry out the operation efficiently except under a general anaesthetic. It was attempted under a local anaesthetic in one case only: but proved a most unhappy experience for all parties, not least, I believe, for the infant. As a result of surgery carried out on a continually moving target, an ineffective repair was done which subsequently broke down and had to be re-attempted.
The anterior one-third of the tongue and the region of the lower buccal sulcus are infiltrated with a I in Ioo,ooo adrenaline solution. In order to effect sound union between tongue and buccal mucosa it is essential to be able to see perfectly at every stage, and adequately bloodless conditions are given using adrenaline infiltration.
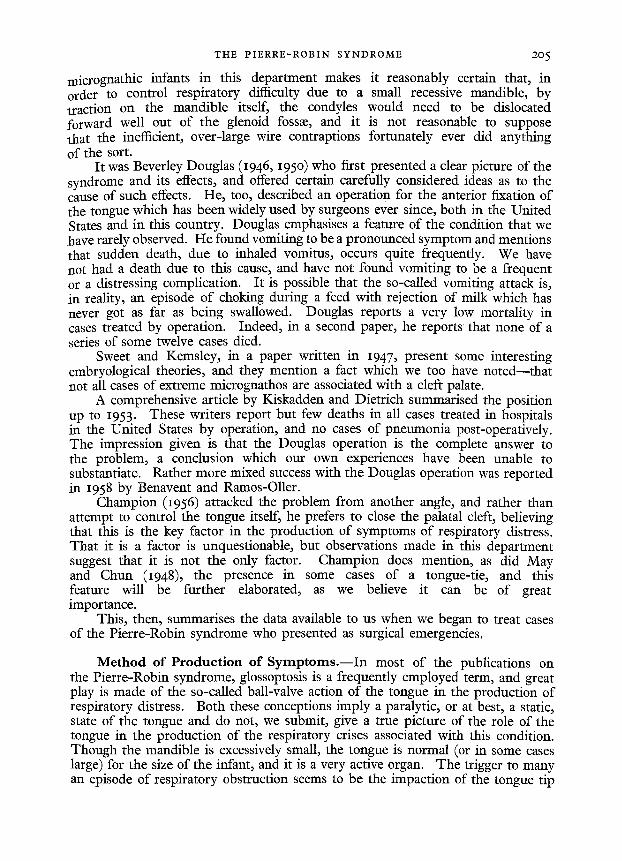
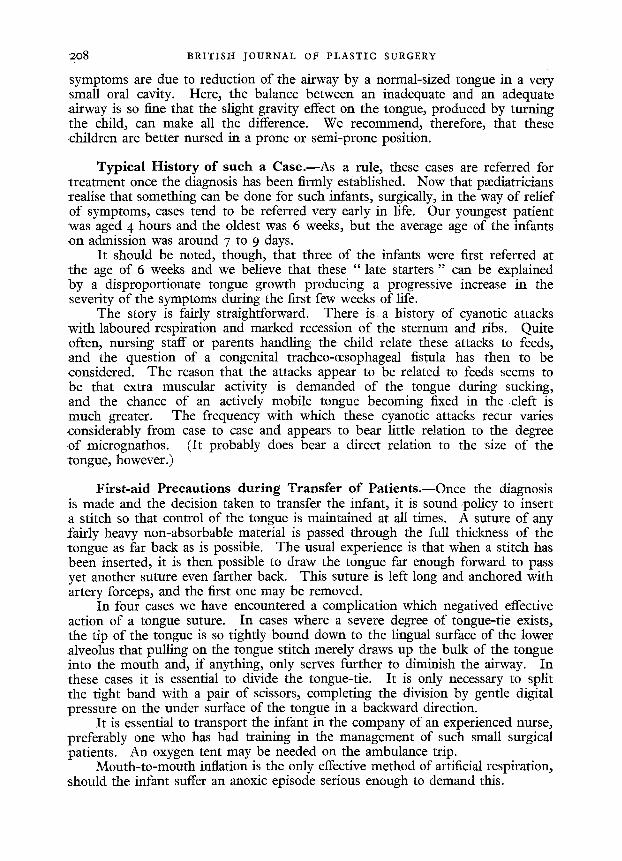
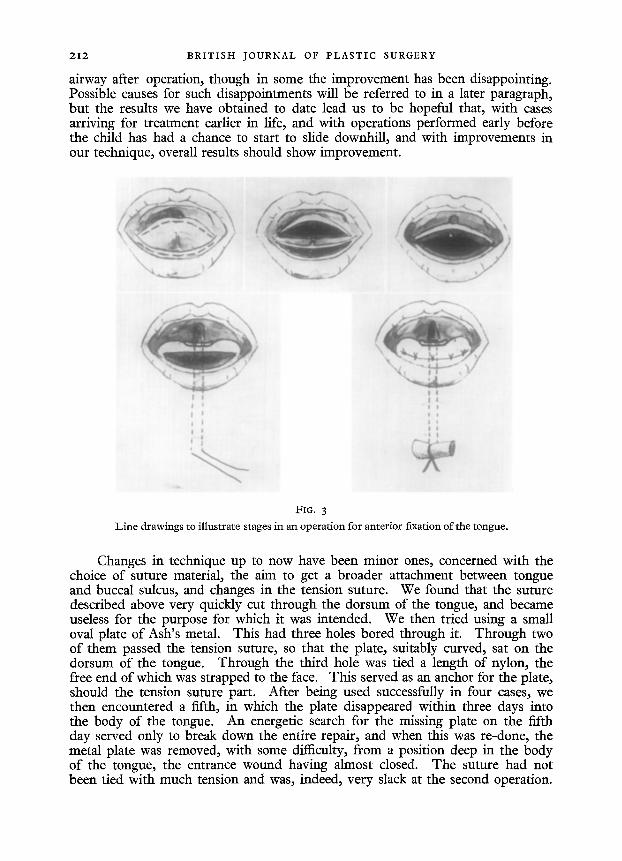
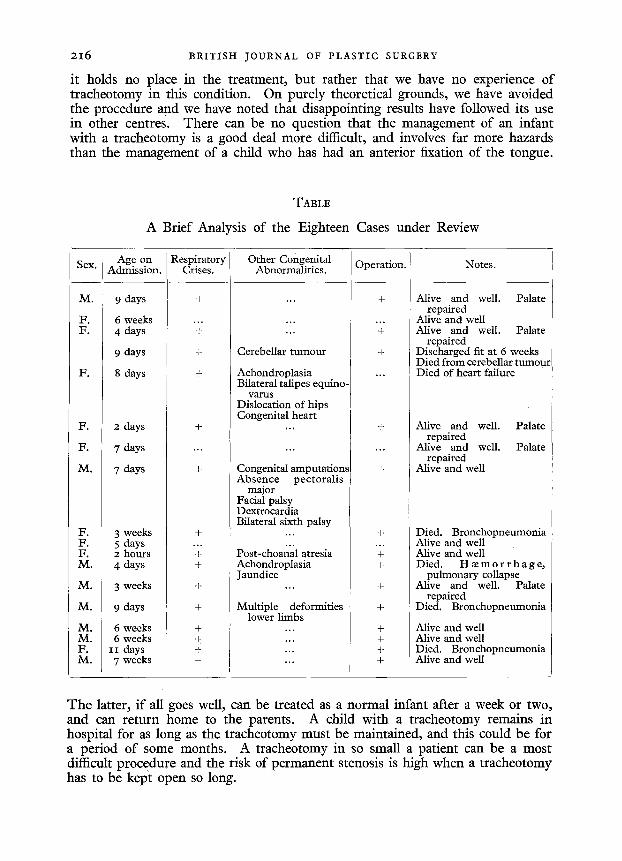
An incision is carried around the edge of the anterior part of the tongue so as to divide the tip of the tongue transversely, and a matching incision is placed in the lower buccal sulcus as low as possible, but leaving enough space posteriorly to get a good mucosal flap. Both incisions are deepened into muscle. The lower lip of the tongue incision is then united with the posterior mucosal flap, using vertical mattress sutures of 4/o chromic catgut. I f the incisions have been of generous length, a good broad attachment is obtained. A single deep suture is then placed to take a wide bite of the muscle of the tongue and of the muscle of the chin. It is left untied until the tension suture is placed. This is most conveniently placed using a Reverdin needle-holder, and the aim is to introduce this suture as far posteriorly as possible on the dorsum of the tongue. The suture is placed through the skin overlying the symphysis, passes in front of the repaired posterior layer of the anastomosis deep into the tongue muscles, and emerges on the dorsum of the tongue. The suture then re-enters the tongue ½ cm. distant, and passes back to emerge the same distance away from the place of entry in the skin over the symphysis. An examination of the line drawings (Fig. 3) will help to illustrate this. This suture is not tied until the repair is completed.
The single muscle suture previously inserted is now tied and the repair completed by uniting the upper edge of the tongue incision with the anterior mucosal flap. Vertical mattress sutures of 4jo chromic catgut or 2 lb. nylon are used. Finally, the tension suture is tied at the skin over a small dental roll. The operation itself takes no more than twenty minutes to complete, and blood loss is minimal.
Initial improvement in the airway, following this relatively simple procedure, has sometimes been dramatic. In every case operated on there has been a better
212 B R I T I S H JOURNAL OF P L A S T I C SURGERY
airway after operation, though in some the improvement has been disappointing. Possible causes for such disappointments will be referred to in a later paragraph, but the results we have obtained to date lead us to be hopeful that, with cases arriving for treatment earlier in life, and with operations performed early before the child has had a chance to start to slide downhill, and with improvements in our technique, overall results should show improvement.
. t !
t
FIG. 3
Line drawings to illustrate stages in an operation for anterior fixation of the tongue.
Changes in technique up to now have been minor ones, concerned with the choice of suture material, the aim to get a broader attachment between tongue and buccal sulcus, and changes in the tension suture. We found that the suture described above very quickly cut through the dorsum of the tongue, and became useless for the purpose for which it was intended. We then tried using a small oval plate of Ash's metal. This had three holes bored through it. Through two of them passed the tension suture, so that the plate, suitably curved, sat on the dorsum of the tongue. Through the third hole was tied a length of nylon, the free end of which was strapped to the face. This served as an anchor for the plate, should the tension suture part. After being used successfully in four cases, we then encountered a fifth, in which the plate disappeared within three days into the body of the tongue. An energetic search for the missing plate on the fifth day served only to break down the entire repair, and when this was re-done, the metal plate was removed, with some difficulty, from a position deep in the body of the tongue, the entrance wound having almost closed. The suture had not been tied with much tension and was, indeed, very slack at the second operation.
THE P I E R R E - R O B I N S Y N D R O M E 213
It must be remembered, however, that even after anterior fixation the tongue is capable of a good deal of movement, and the tension suture should be tied quite slackly to allow for this.
Most recently we have used, instead of a metal plate, a common shirt button of the pearl variety, anchored in a similar way. This has proved satisfactory to date.
Post-operative Care.--The infant is placed in an oxygen tent to recover from the anmsthetic, but this is removed as soon as it is seen that respiratory excursions are full and free, and that costal and sternal recession and any evidence
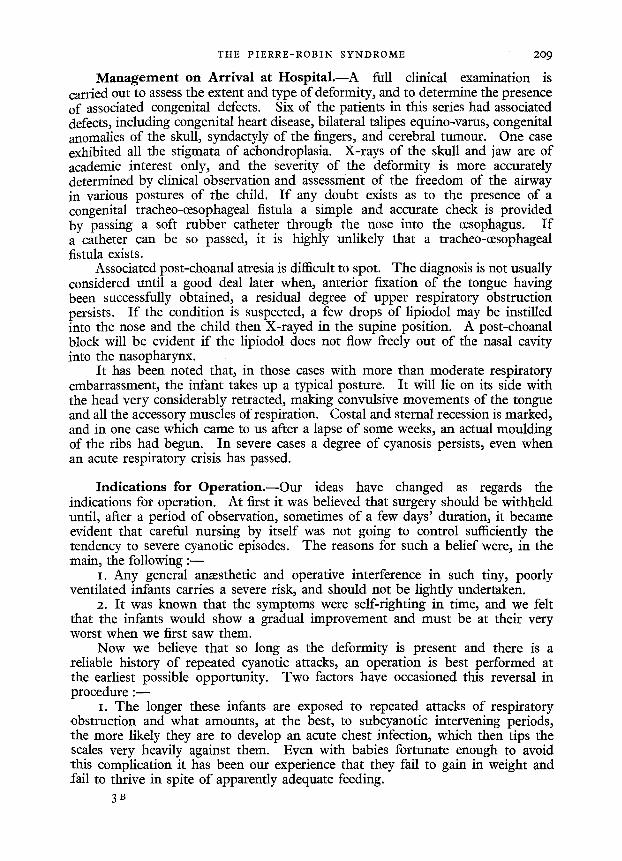
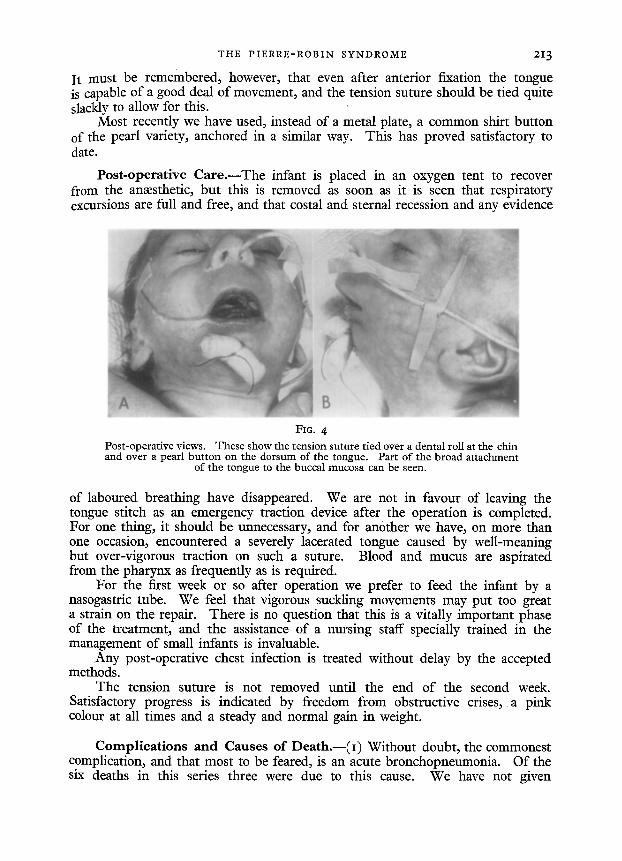
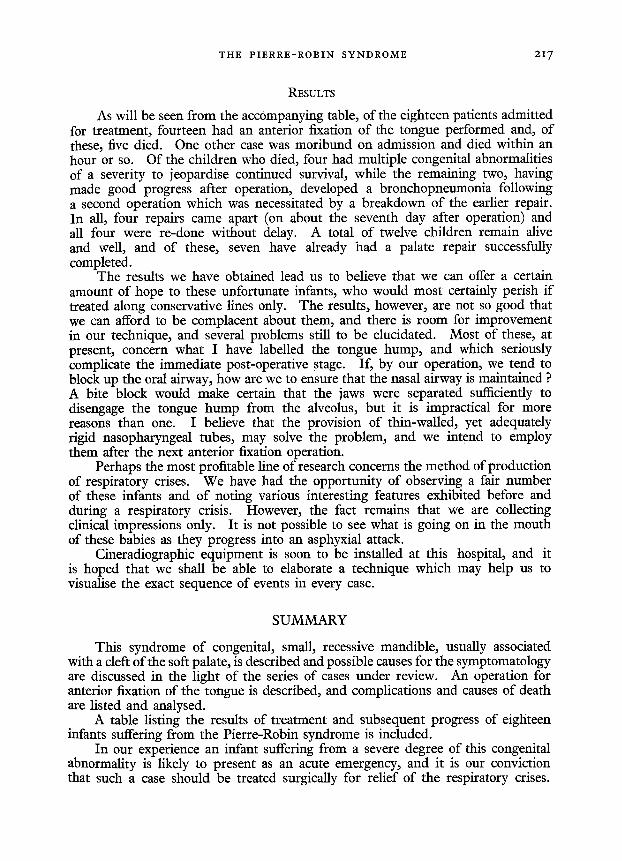
FIG. 4
Pos t -opera t ive views. These show the tens ion suture t i ed over a denta l roll at the chin and over a pear l b u t t o n on the dorsum of the tongue. Par t of the b road a t tachment
of the tongue to the buccal mucosa can be seen.
of laboured breathing have disappeared. We are not in favour of leaving the tongue stitch as an emergency traction device after the operation is completed. For one thing, it should be unnecessary, and for another we have, on more than one occasion, encountered a severely lacerated tongue caused by well-meaning but over-vigorous traction on such a suture. Blood and mucus are aspirated from the pharynx as frequently as is required.
For the first week or so after operation we prefer to feed the infant by a nasogastric tube. We feel that vigorous suckling movements may put too great a strain on the repair. There is no question that this is a vitally important phase of the treatment, and the assistance of a nursing staff specially trained in the management of small infants is invaluable.
Any post-operative chest infection is treated without delay by the accepted methods.
The tension suture is not removed until the end of the second week. Satisfactory progress is indicated by freedom from obstructive crises, a pink colour at all times and a steady and normal gain in weight.
Complications and Causes of Death.--( i) Without doubt, the commonest complication, and that most to be feared, is an acute bronchopneumonia. Of the six deaths in this series three were due to this cause. We have not given
2 1 4 B R I T I S H J O U R N A L OF P L A S T I C SURGERY
antibiotics routinely, preferring to use them only when indications for their employment existed. It has been our experience that an acute bronchopneumonia in these tiny babies is almost invariably fatal. We believe this complication is best avoided by operating early, before laboured and largely ineffective respiratory efforts have produced the state of alveolar stasis and pulmonary oedcma which precede an acute infection.
(2) In one case death was at least partly due to an associated cardiac abnormality. A septal defect, though it may not prove fatal in otherwise normal babies, can well tip the scales in an infant whose life is already prejudiced by severe respiratory obstruction.
(3) In only one case in this series has a post-operative hmmorrhage been encountered, but in this one case it certainly accounted for death, some eighteen hours after operation. The infant, 2 days old, only 5 lb. in weight and with a full Pierre-Robin syndrome, multiple congenital deformities of the hands, bilateral talipes eqnino-varus, and skull anomalies, was heavily jaundiced on admission and a copious fast ooze of blood was encountered throughout the operation and controlled only with great difficulty. An hour after operation the infant was breathing freely, and there was no bleeding from the tongue. When it had recovered from the anmsthetic, and had begun tongue movements, bleeding began from the suture line and, despite massive vitamin K injections, blood transfusion, and treatment with Adrcnoxyl, continued inexorably. It was never more than a slow ooze, but it was never controlled, and soon after peripheral vascular failure became evident the child died.
Should so heavily jaundiced an infant be admitted in the future, I believe it would help to postpone operation for three or four days, while blood investigations wcrc being carried out, and an attcmpt made to countcract the effects of any existing blood dyscrasia.
(4) One case in the series showed a disappointing degree of improvement in airway after a tongue fixation had bccn performed, due to an associated post-choanal atresia. This, fortunately, seems to bc a rare congenital deformity, but in this particular case, treatment by an ear, nose, and throat colleague proved most effective.
(5) The tongue hump. This is a complication which has been noticed following several of our more recent tongue fixations. I believe that this state of affairs has appeared only after our more recent operations for the reason that we arc doing a more effective fixation than we used to. After all, the object of the operation is to fix the tongue as far forward in the mouth as possible, and this is best achieved if a very wide union can be obtained, but important side effects may result, which, paradoxically, may seriously impair the airway.
I f your normal tongue movements arc studied in a mirror, it will bc sccn that, as the tongue is slightly protruded, a kind of hump forms at about its middle, and this hump projects upwards into the arch of the palate. As protrusion proceeds, the hump flattens and leaves the palate. Now, after an anterior fixation of the tongue, only a slight amount of protrusion is obtained, probably to a degree where the hump is at its most marked. It is impossible to fix the tongue so far forward that the hump flattens out. Unless the infant has its jaws quite widely separated, as in the effort of crying, this hump can be clearly seen in contact all along the upper alveolus. If, in addition, a good broad attachment of the tongue to the
THE P I E R R E - R O B I N SYNDROME 2I 5
buccal sulcus has been obtained, any airway past the lateral borders of the tongue is obliterated and the total effect is as though a cork had been fitted into the mouth. This would not be of serious import so long as the child had a free nasal airway, but it is noteworthy that many infants object to having to breathe through the nose alone. This has been noted occasionally, following the repair of a wide cleft lip. Having been accustomed to an airway through the cleft, the child takes unkindly for a while to having to breathe through his nose.
This problem of the tongue hump is a very real one, and has led to a great deal of concern over the post-operative course of some of our patients who have shown a disappointing improvement in airway, and an obstinate failure to thrive as a result. When these babies cry, widely separating their jaws and so disengaging the tongue hump from the upper alveolus, their airways are perfectly free. The posterior obstruction has been converted, by operation, to an anterior one. Fortunately, after a varying period, such infants tend to settle down satisfactorily and the improvement seems to march with the establishment of normal nose breathing. To say the least, they are very worrying to all concerned, and I would stress again the necessity, especially during this post-operative period, of really devoted nursing.
There can be little doubt that the degree of respiratory embarrassment produced post-operatively by the tongue hump is augmented during the first few days after operation by oedema. There is usually some swelling of the tongue and floor of the mouth following operation, but this has never been of an extreme degree and has been noted to be considerably less since we gave up the Douglas operation in favour of our own procedure.
It is hardly necessary to add that repeated attempts at intubation by the ana:sthetist can produce a severe laryngeal (edema, which may very seriously complicate the post-operative course. The region of the cricoid ring in these babies has an area of about 14 sq. mm. A I mm. thickness of (edema at this ring is sufficient to reduce the area by almost 7o per cent. To have these infants intubated and anmsthetised smoothly and rapidly is more than half the battle.
Subsequent Progress.--All authorities are unanimous in stating that the micrognathic deformity is a self-limiting condition. Pruzansky and Richmond (I954) showed that the mandible possesses a remarkable potentiality for growth in patients with a Pierre-Robin syndrome, and if such children can be kept alive, growth of the jaw proceeds, obstructive episodes are minimised, and spontaneous resolution of respiratory and feeding problems occurs. Certainly, our experience is that as soon as an adequate airway is provided these children thrive normally and the tiny lower jaws grow to normal limits within twelve months or so.
We normally release the tongue, at six months and repair the palate at twelve months.
An infant who has had an anterior fixation of the tongue performed is quite capable of sucking normally, and a normal feeding regime is instituted once the post-operative phase is over.
The Role of T raeheo tomy . - -No mention has been made of tracheotomy at any stage in the management of these cases. This is not to say that we believe
2 1 6 BRITISH JOURNAL OF PLASTIC SURGERY
it holds no place in the treatment, but rather that we have no experience of tracheotomy in this condition. On purely theoretical grounds, we have avoided the procedure and we have noted that disappointing results have followed its use in other centres. There can be no question that the management of an infant with a tracheotomy is a good deal more difficult, and involves far more hazards than the management of a child who has had an anterior fixation of the tongue.
TABLE
A Brief Analysis of the Eighteen Cases under Review
S e x .
M.
F. F.
F.
F .
F.
M.
F .
F. F. M.
M.
M.
M .
M. F. M.
Age on Admission.
9 days
6 weeks 4 days
9 days
8 days
2 days
7 days
Respiratory Crises.
÷
. . .
+
+
+
+
7 days +
3 weeks 5 days 2 hours 4 days
3 weeks
9 days
6 weeks 6 weeks
x i days 7 weeks
+ . . .
+ +
+
+
+ + + +
Other Congenital Abnormalities.
° . .
Cerebellar turnout
Achondroplasia Bilateral talipes equino-
varus Dislocation of hips Congenital heart
Congenital amputations Absence pectoralis
major Facial palsy Dextrocardia Bilateral sixth palsy
Post-choanal atresia Achondroplasia Jaundice
Multiple deformities lower limbs
Operation.
+
°° ,
+
+
÷
÷
+
+ +
÷
+
+ + + +
Notes.
Alive and well. Palate repaired
Alive and well Alive and well. Palate
repaired Discharged fit at 6 weeks Died from cerebellar tumour Died of heart failure
Alive and well. Palate repaired
Alive and well. Palate repaired
Alive and well
Died. Bronchopneumonia Alive and well Alive and well Died. H m m o r r h a g e ,
pulmonary collapse Alive and well. Palate
repaired Died. Bronchopneumonia
Alive and well Alive and well Died. Bronchopneumonia Alive and well
The latter, if all goes well, can be treated as a normal infant after a week or two, and can return home to the parents. A child with a tracheotomy remains in hospital for as long as the tracheotomy must be maintained, and this could be for a period of some months. A tracheotomy in so small a patient can be a most difficult procedure and the risk of permanent stenosis is high when a tracheotomy has to be kept open so long.
THE P I E R R E - R O B I N S Y N D R O M E 2 I 7
RESULTS
As will be seen from the accompanying table, of the eighteen patients admitted for treatment, fourteen had an anterior fixation of the tongue performed and, of these, five died. One other case was moribund on admission and died within an hour or so. Of the children who died, four had multiple congenital abnormalities of a severity to jeopardise continued survival, while the remaining two, having made good progress after operation, developed a bronchopneumonia following a second operation which was necessitated by a breakdown of the earlier repair. In all, four repairs came apart (on about the seventh day after operation) and all four were re-done without delay. A total of twelve children remain alive and well, and of these, seven have already had a palate repair successfully completed.
The results we have obtained lead us to believe that we can offer a certain amount of hope to these unfortunate infants, who would most certainly perish if treated along conservative lines only. The results, however, are not so good that we can afford to be complacent about them, and there is room for improvement in our technique, and several problems still to be elucidated. Most of these, at present, concern what I have labelled the tongue hump, and which seriously complicate the immediate post-operative stage. If, by our operation, we tend to block up the oral airway, how are we to ensure that the nasal airway is maintained ? A bite block would make certain that the jaws were separated sufficiently to disengage the tongue hump from the alveolus, but it is impractical for more reasons than one. I believe that the provision of thin-walled, yet adequately rigid nasopharyngeal tubes, may solve the problem, and we intend to employ them after the next anterior fixation operation.
Perhaps the most profitable line of research concerns the method of production of respiratory crises. We have had the opportunity of observing a fair number of these infants and of noting various interesting features exhibited before and during a respiratory crisis. However, the fact remains that we are collecting clinical impressions only. It is not possible to see what is going on in the mouth of these babies as they progress into an asphyxial attack.
Cineradiographic equipment is soon to be installed at this hospital, and it is hoped that we shall be able to elaborate a technique which may help us to visualise the exact sequence of events in every case.
SUMMARY
This syndrome of congenital, small, recessive mandible, usually associated with a cleft of the soft palate, is described and possible causes for the symptomatology are discussed in the light of the series of cases under review. An operation for anterior fixation of the tongue is described, and complications and causes of death are listed and analysed.
A table listing the results of treatment and subsequent progress of eighteen infants suffering from the Pierre-Robin syndrome is included.
In our experience an infant suffering from a severe degree of this congenital abnormality is likely to present as an acute emergency, and it is our conviction that such a case should be treated surgically for relief of the respiratory crises.
218 BRITISH JOURNAL OF PLASTIC SURGERY
We believe that in many cases this line of treatment offers the only hope for continued survival.
I acknowledge with gratitude my debt to M r G. M . FitzGibbon and M r D. C. Bodenham, and I wish also to thank Dr N. C. Petersen of Copenhagen for the line drawings and M r L. G. Banham of the Medical Photographic Department for the clinical photographs.
REFERENCES
BENAVENT, W. J., and RAMOS-OLLER, A. (1958). Plast. reconstr. Surg., 22, 486. CHAMPION, R. (1956). Brit. ft. plast. Surg., 8, 283. DOtr~LAS, B. (1946). Plast. reconstr. Surg., 1, 3o4.
(195o). Plast. reconstr. Surg., 5, 113. KISKADDEN, W. S., and DIETRICH~ S. R. (1953)- Plast. reconstr. Surg., I2, 364. LAPAGE, C. P. (1937). Lancet, i, 323 . MaY, H., and CHUN, L. T. (1948). Pediatrics, 2, 685. PRtIZANSKY, S., and RICHMOND, J. B. (1954). Amer. ft. Dis. Child., 88, 29. SHUKOWSKY, W. P. (1911). fib. Kinderheilk., 73, 459. SWEET, A. M., and KEMSLEY, M. (1947). Lancet, 2, io. WILTON, T. N. P. (196o). Brit. ft. Ancesth., 3, 116.