Embed Size (px)
Citation preview

A S I A H E A L T H P O L I C Y P R O G R A M S E M I N A R
The Performance and Driving Force of Government Health Expenditure in China:Government Health Expenditure in China:
Evidences From Provincial Panel Data 1991-2007
Qiulin Chen1,2, Ling Li21 Walter H. Shorenstein Asia-Pacific Research Center, Stanford University
2 National School of Development, Peking University
Presented by Qiulin [email protected]
May 5th , 2011
1

Contents
1 Backgrounds and stylized facts1. Backgrounds and stylized facts2. Research questions with literature review3. Empirical strategy and data4. Empirical results of hypothesis 1 & 2p yp5. Conclusions and discussions
2

1. Backgrounds & Stylized Facts
Chinese Health Care System
g y
Chinese Health Care System• During the period from 1950 to 1978, China had many
achievements in health sector to be proud ofachievements in health sector to be proud of– rapid and large reductions in mortality rate, despite China’s low income
per capita at that time– create a low cost, wide coverage primary health care system
• After 30 years of economic reform, China’s healthcare system h i d ll i did d i hhas not improved as well as its economy did. Instead, it has deteriorated in many aspects– Accessibility and affordability are both decreasedAccessibility and affordability are both decreased– Patients, providers and government are all unsatisfied
“Kan Bing Gui, Kan Bing Nan ”(看病贵、看病难)g g (
3

4

1. Backgrounds & Stylized Facts (cont.)
Current Health Care Reform in China
g y ( )
Current Health Care Reform in China• The state has withdrawn abruptly from its previously
predominant role in health China is a case in point and apredominant role in health. China is a case in point and a warning to the rest of the world. (WHO, 2008)
• The SARS crisis pushed the Chinese government to realize that it is necessary and urgent to solve the unbalance between economic and social development (“一条腿长 一条腿短”) (economic and social development ( 条腿长、 条腿短 ). ( Wen Jiabao, 2010)
• The key tasks to deepen the health care reform started in 2009 are to increase and secure the government health expenditure (“加大资金投入 保障资金安全”) (Li Keqiang 2009)( 加大资金投入,保障资金安全 ). (Li Keqiang, 2009)
5

1. Backgrounds & Stylized Facts (cont.)g y ( )
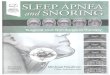
Structure of Total Health Expenditure : 1978 2008
The GHE decreased since the late 1980s and has returned to increase 59.97
70.00
Structure of Total Health Expenditure : 1978-2008
1980s and has returned to increase since the early 2000s ( SARS in 2003).
59.97
50.00
60.00
38.70
30.00
40.00
15.69
20.00
0.00
10.00
8 9 0 1 2 3 4 5 6 7 8 9 0 1 2 3 4 5 6 7 8 9 0 1 2 3 4 5 6 7 8
Market reform in health sector: 1985 SARS, New govt. (NCMS): 2003
Source: Chinese Health Statistics Yearbook 2009
197
197
198
198
198
198
198
198
198
198
198
198
199
199
199
199
199
199
199
199
199
199
200
200
200
200
200
200
200
200
200
Out‐of‐pocket Social Health Exp. Government Health Exp.6

1. Backgrounds & Stylized Facts (cont.)g y ( )
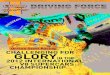
Inter-province Inequality of Health Outcome and Input
Heilong
jiang
吉林
辽宁Inner
新疆
Per Capita GDP 2000
Life Expectancy 2000 Heilong
jiang
吉林
辽宁新疆
河北
山东
安徽湖北
上海
河南
山西
Inner
Mongolia
陕西
宁夏
甘肃
Qinghai
Sichuan
西藏 江苏
浙江
天津北京
重庆
宁
河北
山东
安徽湖北
上海
河南
山西
Inner
Mongolia
陕西
宁夏
甘肃
Qinghai
Sichuan
西藏 江苏
天津北京
Shanghai:78.1Yunnan: 65.5
海南
福建
江西湖南
广
东
Guangxi
贵州云南
浙江重庆
What are the factors of the big gap? Only economic status?
海南
福建
江西湖南
广
东
Guangxi
贵州云南
浙江重庆
海南
Heilong
jiang
吉林
辽宁Inner
Mongolia甘肃
新疆
天津北京
黑龙江
吉林
辽宁
内蒙古甘肃
新疆
天津北京
2000 2007
河北
山东
江西
安徽湖北
湖南
上海
河南
山西
Mongolia
陕西
宁夏Qinghai
Sichuan
西藏 江苏
浙江
天津
重庆
河北
山东
江西
安徽湖北
湖南
上海
河南
山西
陕西
宁夏青海
四川
西藏 江苏
浙江
天津
重庆
Share of GHE as Total Govt. Exp.
What are the driving forces of this change in the 21st century?
海南
福建湖南
广
东
Guangxi
贵州云南
海南
福建湖南
广
东
广西
贵州云南 Highest 1/3
Middle 1/3Lowest 1/3

1. Backgrounds & Stylized Facts (cont.)
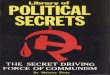
Government Expenditures & Revenues Among 5 tier Govt
g y ( )
Government Expenditures & Revenues Among 5-tier Govt.
Local govt., especially the county/ district 22 04%
Total Revenue: 2007the county/ district levels bear most of the govt. health exp..
22.04%(93.3%)
54.07%
24.72%
Central Govt.
18.24%(69.3%)
15 68%
%
45.93%
%
75.28%
Transfe
Province / Autonomous Region
15.68%(36.2%)
42 81%
Local Govt.
T t l E 2007
ersPrefecture / Autonomous Prefecture
42.81%(28%)
1.23%
Total Exp.: 2007
Central govt. transfers:•More to the West
Rural County / Urban District
T / T hi / U b C it
Source: National Health Financial Annual Report , 2007
(51%)GHE through Health Dept.: 2007
•Most through special projects (跑部钱进)
Town / Township / Urban Community
8

1. Backgrounds & Stylized Facts (cont.)g y ( )
Inter-department Distribution of Gov. Health Exp.: 2007
Did the govt. health exp. through healthGHE through health department (incl. operating expenses on health care and
Did the govt. health exp. through health dept. and other dept. perform equally?
40%30%
30%60%
on health care and TCM) GHE through other departments
ghe dhe
30% (especially subsidies to social health insurance)Other GHE (inclOther GHE (incl. family planning, medical education, capital construction
fheCentral govt.: <4%
Source: National Health Financial Annual Report 2007, MOH.
and so on)
Source: National Health Financial Annual Report , 2007; Chinese Financial Statistical Yearbook, 20089

2. Research Questions
• The new health reform started in 2009 showed the determination of
Q
• The new health reform started in 2009 showed the determination of the Chinese governments, especially the central government, to increase responsibilities in the health sector. The most obvious action of this commitment is to increase government healthaction of this commitment is to increase government health expenditure (GHE).
• But there is still a hot debate about whether the government should allocate more public funds to health or just deepen the marketization of the health sector.
• Two questions may have to be answered:Two questions may have to be answered:
1. Why? Why should the government increase health care dit ?expenditures?
2. How? How could the government, especially the local g p ygovernments be encouraged to increase health care expenditures?
10

• Question 1: Why?
• Perspective 1: health care delivery public or private
• Empirically, we should know what did the GHE perform in the past years?
• Perspective 1: health care delivery, public or private providers
• Perspective 2: health care financing public• Perspective 2: health care financing, public (government) or private
A t f bli h lth fi iArguments for public health financing− Particularity of health care goods (Gupta and Dasgupta 2002)− Equality objective of health care system (Richardson and McKie 2007)Equality objective of health care system (Richardson and McKie 2007)− Transaction cost (“The Economics of Public and Private Roles in Health
Care”, HNP )Problems caused by private financing (Freyens 2008)− Problems caused by private financing (Freyens 2008)
Hypothesis 1 (H1): The GHE did improve health outcomes (positive effects) in Chinaoutcomes (positive effects) in China.
11

• Question 1: Why?
Empirical studies on effects of health financing
• Literature review
p g− Outcomes of private health financing (user fees):
About 1980s (Akin, Birdsall et al. 1987; Griffin 1988)About late 1990s (Sepehri and Chernomas 2001; Yisa Fatiregun et alAbout late 1990s (Sepehri and Chernomas 2001; Yisa, Fatiregun et al. 2004; Deininger and Mpuga 2005)
− Outcomes of public health financing : p gFocus on mortality (Gupta, Verhoeven et al. 2002; Hanmer, Lensink et al. 2003; Mayer and Sarin 2005)Focus on less developed countries (Bidani and Ravallion 1997; IssaFocus on less developed countries (Bidani and Ravallion 1997; Issaand Ouattara 2005)Econometric method does matter! (Issa and Ouattara 2005)
− Outcomes of China’s public financing : See Du lexun,2005; Zhao & Tao et al, 2005 ; Wang Jun, 2007
Few studies addressed the effects of GHE on Chinese
3
Few studies addressed the effects of GHE on Chinese health outcomes, especially by newly developed methods.
12

• Question 2: How?
P ibilit 1 I ffi i t fi l
• Empirically, we should know why did the local govt. under invest on health in the past years?
• Possibility 1: Insufficient fiscal resourcesIf so, why did it not happened in the before-reform era and
not happened in education sector?not happened in education sector?
13

• Question 2: How?
100
Fiscal Exp. Decentralization and Govt. Health Exp. Decentralization : 1957-2008
70
80
90
Government health expenditure decentrali ation has a long histor
40
50
60
70 decentralization has a long history.
10
20
30
40
0
10
Local share in total GHE (%) Local share in total govt. outlay (%)
Source: National Health Financial Annual Report; Chinese Financial Statistical Yearbook 14

• Question 2: How?
Share of govt. education Share of GHE
in the expenditure of science, education, culture
gexpenditure
in the expenditure of science, education, culture
YearYear Total Central Local Total Central Local
19911991 21 %% 4 %% 23%% 58 %% 44 %% 60 %%D
19921992 21 %% 4 %% 23 %% 57 %% 46 %% 59 %%
19941994 20 %% 4 %% 22 %% 60 %% 48 %% 62 %%
Decreasi19941994
19961996 20 %% 4 %% 22 %% 61 %% 48 %% 62 %%
19981998 19 %% 4 %% 21 %% 62 %% 51 %% 64 %%
ng
19981998 19 %% 4 %% 21 %% 62 %% 51 %% 64 %%
20002000 18 %% 3 %% 20 %% 64 %% 49 %% 66 %%
20022002 16 %% 4 %% 17%% 66 %% 47 %% 69 %%
Increasi
20022002 16 %% 4 %% 17%% 66 %% 47 %% 69 %%
20052005 17 %% 4 %% 18 %% 65 %% 42 %% 68 %%
ng
Source: Chinese Financial Statistical Yearbook 15

• Question 2: How?
P ibilit 1 I ffi i t fi l
• Empirically, we should know why did the local govt. under invest on health in the past years?
• Possibility 1: Insufficient fiscal resourcesIf so, why did it not happened in the before-reform era and
not happened in education sector?not happened in education sector?• Possibility 2: Insufficient incentive
Effect of “Chinese-style Decentralization”: y
fiscal exp. decentralization(Local govt. takes most
political centralization(performance evaluation:
(See Montinola, Qian et al,1995; Blanchard & Shleifer, 2001; Tsui & Wang, 2004; Zhang Yongsheng 2005; Fu Yong & Zhang Yan 2007; Yao Jijun 2008)
( gresponsibilities on exp.)
(peconomic growth)
Zhang Yongsheng, 2005; Fu Yong & Zhang Yan, 2007; Yao Jijun, 2008)
Hypothesis 2 (H2): Local govt. under invested on health due yp ( ) gto regional economic competition.
16

• Question 2: How?
“ They (local officials) know well about how many They (local officials) know well about how many chickens or sheep died, but may not know how many people died in the area .”
—— A director from Qinghai Provincial Health Department
“ The main resistance to health care reform are from th l l t ”the local government.”
—— Chen Zhu, Minister of Chinese MOH (2009)
“ Whether the CMS is organized well or not dependsWhether the CMS is organized well or not, depends on whether the local officials weigh in on it or not. Whether the local officials weigh in on it or not, depends on whether they realize the importance of it or not”.
—— “How to Organize the CMS Well (III)” People's MedicalHow to Organize the CMS Well (III) , People s Medical Publishing House (1975)
17

• Question 2: How?
Literatures on effects of Chinese-style Decentralization
• Literature review
− on economic growth: See Qian & Xu, 1993; Qian & Weingast, 1997; Qian and Roland, 1998( regional competition); Zhou Yean 2003; Zhou Li’an 2004; Li &1998( regional competition); Zhou Yean, 2003; Zhou Li an 2004; Li & Zhou 2005; Xu, Wang et al, 2007 (officials’ promotion); Wang, Zhang et al, 2007; Zhang Jun, 2007 (sustainable development)
− on social development (public goods provision): See Ping Xinqiao, 2006 (public goods); Fu & Zhang, 2007 (govt. exp. structure); Qiao, Fan et al, 2005; Zheng lei, 2008; Zhou & Wang, 2008 ); Q , , ; g , ; g,(education), Zhang Quan, 2008 (pollution)
− on social development (public goods provision): Pi & B i 2005 (h lth i bilit ) Qi b 2008 ( h lthPing & Bai, 2005 (health service capability); Qiao baoyun, 2008 ( health expenditure)
Few studies addressed the effects on both healthFew studies addressed the effects on both health expenditures and health outcomes; and structure effects.
18

3. Empirical Strategy and Data
• The econometric model
p gy
The econometric model
H : dependent variables0 1 2i t i t i t i t i tH K E Y Zα β β μ υ ω= + + + + +
– Hit : dependent variables• for H1: health outcome • for H2: health expenditure p
– KEYit : key variables• for H1: GHE• for H2: economic competition
– Zit :other control variables– ut : time effect– vi : regional effect– ώit : residual
19

• Basic regressions– Pooled OLS, random effect, fix effect: POLS, RE, FE (by Hausman test)– Robust regression (in case of heteroskedasticity)– Year fixed effect (in case of cross-sectional dependency): POLSYD, REYD, FEYD
• Possible bias and other problems – Autocorrelation in panel data– Variable omission bias– Endogeneityg y
• Dynamic Panel Data Model– First differenced GMM, DIF-GMM (Arellano and Bond 1991): DIF, DIFYD– System GMM SYS-GMM (Arellano and Bover 1995; Blundell and Bond 1998):System GMM, SYS GMM (Arellano and Bover 1995; Blundell and Bond 1998):
SYS, SYSYD
IV for Endogeneity (not applied in this study)Test StrategiesPassed
Autocorrelation of residuals : DW test, Woodridge test
Autocorrelation: first-order auto regression (xtregar)
Rejected Variable omission and endogeneity: Dynamic Panel Data Model –Dynamic GMM (xabond2)• 1. AR(1)、AR(2)、Sargan test• 2. Check whether the coefficient is between the coefficients estimated from OLS and FE with lagged dependant variable
20

3. Empirical Strategy and Data (cont.)
D t S
p gy ( )
• Data Sources– China Statistical Yearbook (1991-2007, NBS)– National Health Financial Annual Report (1991-2007, MOH)p ( , )– National Health Statistics Annual Report (1991-2001, MOH)– Chinese Health Statistics Yearbook (2002-2007, MOH)
China Financial Statistical Yearbook (1991 2007 MOF)– China Financial Statistical Yearbook (1991-2007, MOF)
• 28/30 provinces, 1991-2007T i H K M t i l d d• Taiwan, Hong Kong, Macau are not included
• Tibet is not included due to data quality• Si Chuan and Chongqing are not included due to their separation
in1996
• H1: 1991-2001/ 28 ( no reported data of under-5 mortality by province)• H2: 1991-2007/ 30
21

4. Empirical Results: Hypothesis 1
• Dependant variables
p yp
– Under-five mortality, maternal mortality, infectious disease incidence– Improvement of health: ln (H-min(H)) (Sen,1981; Govindaraj & Rannan-
Eliya (1994))y ( ))• Key variables
– Real GHE ( incl. total GHE, GHE through health department, the other GHE) with two measurements:GHE) with two measurements:
– 1) real per capita (1978 constant prices): lnrfheper, lnrgheper, lnrdheper– 2) share of GHE in total govt. outlay: fhefr, ghefr, dhefr
• Control variables (used often in other related studies)– Health care: hospital beds and doctors (per 1000 people), prenatal
examination and rural water improvement coveragep g– Education: Primary school students, middle school students, college
students (per 10000 people)– Income ( per capita real GDP)– Income ( per capita real GDP)– Urban population ratio, population and population density
22

4. Empirical Results (cont.) : Hypothesis 1
Dependant Ln( u5mr-min (u5mr)): Improvement of under-5 mortality
p ( ) yp
Independent FE AR DIF SYS FEYD ARYD DIFDY SYSYDlnrgheper 0.296* 0.319* 0.645 0.541* 0.612*** 0.460** 1.499 0.657**
(0.174) (0.172) (0.428) (0.275) (0.164) (0.193) (0.976) (0.303)R2 0 699 0 688R2 0.699 0.688Wood p 0.2101 0.067Sargan p 0.146 0.164 0.0213 0.0159Hansen p 0.765 0.558 0.986 1.000par1 p 0.0184 0.0235 0.00682 0.0134ar2 p 0.904 0.222 0.536 0.580ghefr 0.0267 0.0716 0.0767 -0.0510 0.129** 0.0635 0.155** 0.00334
(0 0554) (0 0533) (0 0887) (0 0744) (0 0543) (0 0545) (0 0740) (0 0900)(0.0554) (0.0533) (0.0887) (0.0744) (0.0543) (0.0545) (0.0740) (0.0900)R2 0.694 0.682Wood p 0.2351 0.0662Sargan p 0.354 0.00196 0.525 0.00224gHansen p 0.494 0.374 0.857 0.993ar1 p 0.122 0.0253 0.0889 0.00421ar2 p 0.697 0.197 0.537 0.131observations 246 218 216 244 246 218 216 244observations 246 218 216 244 246 218 216 244Provinces 28 28 28 28 28 28 28 28*** p<0.01, ** p<0.05, * p<0.1
23

Department effect—inter-department difference on health outcomes Share of total GHE Effect on Health ImprovementShare of total GHE Effect on Health Improvement
Total Government Health Expenditure 100% undetermined
Incl.Govt. Health Exp. through health dept. 40% Positive
Other Govt Health Exp 60% Negative or undetermined
Regional effect—Nothing to loose in the central area (破罐子破摔)
Other Govt. Health Exp. 60% Negative or undetermined
Improvement of under-5 mortalityEast Central West
FEYD ARYD FEYD ARYD FEYD ARYDTotal GHE 0.396 1.784* -0.0450 0.00383 0.512*** 0.472*Total GHE 0.396 1.784 0.0450 0.00383 0.512 0.472GHE through health department 0.213 0.604* 0.474 0.0136 -0.551 -0.469**Other GHE -0.0270 -0.331 -0.0875* -0.114 0.181*** 0.185**
Time effect “SARS” effectImprovement of infectious disease incidence
before SARS after SARSGHE through FE AR SYS DIF FE AR SYS DIF
Time effect— SARS effect
ghealth department
-0.141*** -0.126** -0.263 -0.156*** 0.365*** 0.0879 1.004*** 0.436*
Observations 276 248 165 194 150 120 120 150R2 0.236 0.570Sargan p 0 000103 7 97e 07 0 0699 0 000479Sargan p 0.000103 7.97e-07 0.0699 0.000479Hansen p 0.0759 0.0931 0.467 0.157ar1 p 0.122 0.00154 0.0857 0.0118ar2 p 0.490 0.454 0.369 0.0941
824

4. Empirical Results (cont.) : Hypothesis 2
• Dependant variables
p ( ) yp
• Dependant variables– Real GHE ( incl. total GHE, GHE through health department, the other
GHE) 1) l it (1978 t t i ) l fh l h l dh– 1) real per capita (1978 constant prices): lnrfheper, lnrgheper, lnrdheper
– 2) share of GHE in total govt. outlay: fhefr, ghefr, dhefr
• Control variables (used often in other related studies)– Health care service facilities: hospital beds and doctors(per 1000
people)people),– Health service demand: Infectious disease incidence– Income ( per capita GDP)– Urbanization: ratio of urban population in total population– Aging: ration of the elderly (65+) in total population– population and population densityp p p p y
– Policy dummy variables: 1999-Social health insurance, 2003-SARS25

4. Empirical Results (cont.) : Hypothesis 2
• Key variables
p ( ) yp
• Key variables– Economic competition: fdishare
share of FDI in a specific province as national total FDI= Provincial FDIit / National FDIt
– Fiscal Decentralization: fsfdshare of local GHE as total GHE in a specific province = Local GHEit / (Local GHEit + Central GHEit )
– Fiscal resources1: fiscal: fiscal self-sufficiency= (local fiscal revenues / local fiscal outlays) it
2: transfer: central govt. transfer= (central govt. transfer / total local govt. outlay) it
3 tf fd t b d t i3: outfrfd: extra-budgetary income= (local extra-budgetary income / total local govt. revenue) it
26

4. Empirical Results (cont.) : Hypothesis 2
Dependant Share of GHE through health departments as total GHE- ghefr
p ( ) yp
Dependant Share of GHE through health departments as total GHE ghefr
Independent FE AR DIF SYS FEYD ARYD DIFYD SYSYD
fdishare 0 110*** 0 0633* 0 0110 0 0862* 0 0914*** 0 0415 0 0190 0 0654*fdishare -0.110*** -0.0633* -0.0110 -0.0862* -0.0914*** -0.0415 -0.0190 -0.0654*
fdishare2 0.00242*** 0.00160 -7.86e-05 0.00260* 0.00204** 0.00110 0.000293 0.00194*
fsfd -0.0281** -0.0114 -0.0288** -0.00576 -0.0499*** -0.0404* -0.0373** -0.00249
dum1999 -0.882*** -0.673*** -0.808*** -0.704***
dum2003 0.351*** 0.264*** 0.340*** 0.284***
R2 0 716 0 736R2 0.716 0.736
Sargan p 0.142 0.308 0.401 0.598
ar1p 0.00896 0.00650 0.0142 0.00868
ar2p 0.133 0.107 0.234 0.187
382 352 349 381 382 352 349 381
30 30 30 30 30 30 30 30*** p<0.01, ** p<0.05, * p<0.1
27

Department effect—inter-department difference on health outcomes
Effects on GHETypes of GHE Effects on GHEEconomic Competition (fdishare)2 1999
1. Total GHE -0.0774** 0.00201*** -0.345***2. GHE through health department -0.0654* 0.00194* -0.779***
Regional effect Weakness in the Central (中部塌陷)
department3. Other GHE 0.0220 -0.000947 0.409**
Regional effect—Weakness in the Central (中部塌陷)
Effects on GHE through health department-ghefrEast Central West
E i C titi 0 0190 0 154** 0 204
Time effect “SARS” effect
Economic Competition 0.0190 -0.154** -0.204Fiscal Decentralization -0.0462 -0.115 -0.113**
Time effect— SARS effect
Effects on Total GHE- fhefrBefore 2003 After 2003
Economic Competition (significant) --Economic Competition --(significant) --Fiscal Decentralization --(significant) --(significant)
Effects on GHE through health department- ghefrBefore 2003 After 2003Before 2003 After 2003
Economic Competition --(significant) --(significant)Fiscal Decentralization --(significant) --(significant)
28

5. Conclusions & Discussions
Main findingsMain findings• (1) Increasing GHE did improve health performance, and this
improvement was mainly driven by the GHE through the health d t t di tl H liti l titi idepartment directly. However, political competition on economic performance lowered local governments’ GHE, mainly by cutting GHE through local health departments.
• (2) Compared with the eastern and western China, this health improvement was not significant in the middle where the regionalimprovement was not significant in the middle, where the regional economic competition led to much less GHE through health departments.
• (3) After SARS in 2003, the positive effect on health outcomes from GHE through health departments was enhanced, while the effectGHE through health departments was enhanced, while the effect from GHE through other departments was not equally significant.
29

5. Conclusions & Discussions (cont.)
Policy Implications
( )
y pAll these results suggest that
① adjusting the structure of public health financing, ② reforming the fiscal system, ③ and improving the performance evaluation system for local
governmentsgovernments are critical for the success of China’s on-going health reform.
The structure does matter!The system does matter!
This is only one of the aspect s of China’s 3rd Development Transition1 t1st (1949-1952): Socialist transformation2nd (Since 1978): Market reform 3rd (Since 2003; especially with the current “twelfth five-year plan”)
Balance economic development and social developmentBalance economic development and social developmentImprove people‘s lives and happiness
30

5. Conclusions & Discussions (cont.)
Limitations
( )
1. FDI share might not be a suitable measurement for regional economic competition in more recent years due to the economic restructuring. (My conclusion might be over pessimistic or there is other mechanism, recall the h f i l diff tt )change of regional difference pattern)
2. This study mainly discussed the quantity of health outcomes, while the quality of health outcomes have not been addressed.
3. It would be better to compare the public and private health financing directly, that is to study the effects of private health expenditure.
4. Sichuan and Chongqing are not included in the analysis.
Further work• Look for more suitable proxies for regional economic competition.
gq g y
p g p• Separate Sichuan and Chongqing in the early year or analyze for shorter
period ( after 1997)• Discuss the mechanism of high outcomes from GHE through health dept• Discuss the mechanism of high outcomes from GHE through health dept.. • Discuss the reasons of decreasing share of GHE through health dept..
31