Embed Size (px)
Citation preview

The PCL in TKR:
to preserve or to cut ??
Francesco Giron
SOD Traumatologia e Ortopedia Generale AOU Careggi –FirenzeDirector: Prof. R Buzzi

…a 25 years old dilemma !

Aglietti’s last 25 years:
PS: 90%
MBK (CR-mobile): 10%
P. Aglietti J. Insall

Kinematics Roll-back Flexion
Gait Strength Proprioception
Exposure Balancing Joint line
Patella Instability Loosening Wear
CR vs PS: Controversy
Results
Surgical
Clinical

Kinematics Roll-back Flexion
Gait Strength Proprioception
Patella Instability Loosening Wear
Results
Surgical
Clinical
CR vs PS: Controversy
Exposure Balancing Joint line

W. Müller, 1982
Roll -back
Motion is guided along a unique
path by constant tension
fascicles of ACL & PCL
Four-bar linkage

Posterior Cruciate Ligament
Provides 95% of total restraint to posterior displacement of the tibia on the femur
Tensile forces increase with knee flexion

Posterior Cruciate Ligament
Allows femoral condyles to glide and rotate
posteriorly.

Posterior Cruciate Ligament
Roll back occurs during knee flexion which benefits:
Posterior clearance
Increased quadriceps moment arm

Tibial internal rotation in flexion
Freeman, JBJS-B 2000
Medial Condyle Lateral Condyle
Dynamic MRI studies

Lateral mobility:
1) Mobility of
lateral meniscus

Lateral mobility:
1) Mobility of
lateral meniscus
2) Lateral plateu
convex and downsloped

Lateral mobility:
1) Mobility of
lateral meniscus
2) Lateral plateu
convex and downsloped
3) Longer distal radius LFC
LFC
MFC

1) Fixed medial meniscus
Medial stability:

1) Fixed medial meniscus
2) Medial plateu
cup-shaped & “upsloped”
Medial stability:

1) Fixed medial meniscus
2) Medial plateu
cup-shaped & “upsloped”
3) Ligament colums in
tension
MFCLFC
MCLPCL
Medial stability:

Freeman, NOV-BVOT 2002Kadoya, in press
0
5
10
15
20
25PCL elongation (%)
20° 40° 60° 80° 100° 120°
PCL tightens from 45° to more flexion
PCL tension
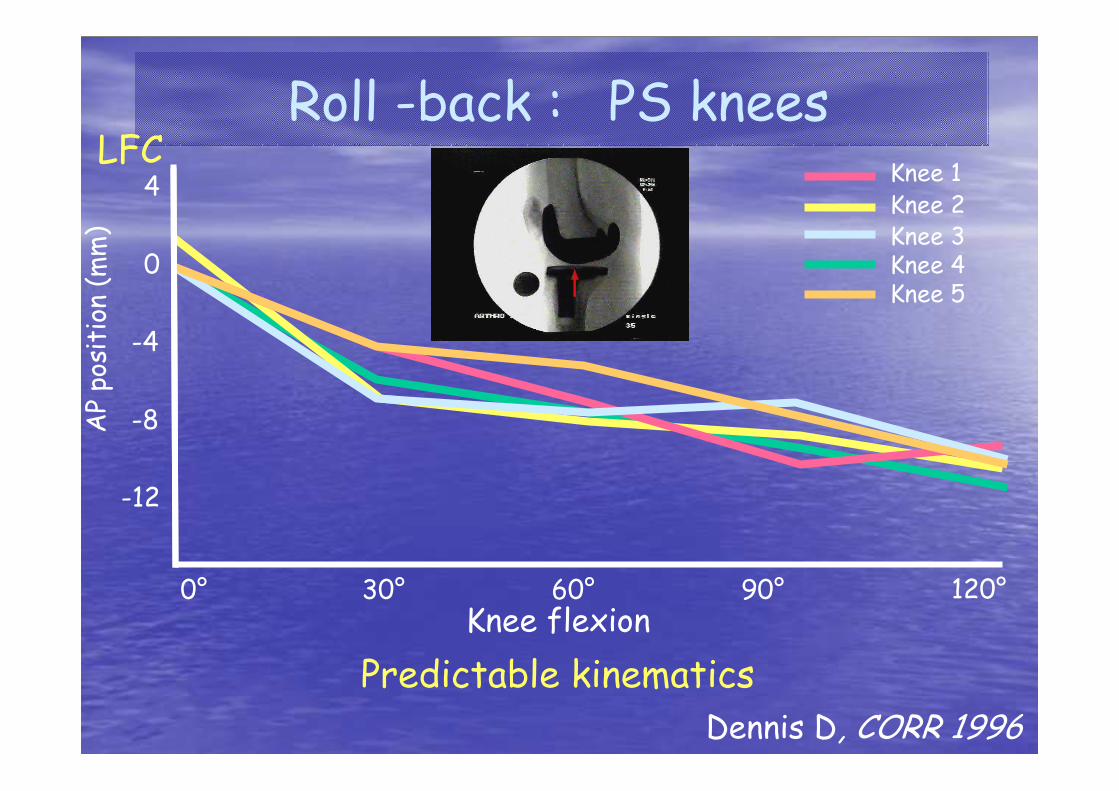
Roll -back : PS knees
Knee flexion
Dennis D, CORR 1996
Predictable kinematics
0° 30° 60° 90° 120°
0
4
-4
-8
-12
AP position (mm)
Knee 1Knee 2Knee 3Knee 4 Knee 5
LFC

Knee flexion
Roll -back : CR knees
0° 30° 60° 90° 120°
0
4
-4
-8
-12
AP position (mm)
Knee 1Knee 2Knee 3Knee 4 Knee 5
Symmetric condylar design
Erratic pattern
LFC

19/20 subjects experienced av. 4 mm lat. roll-back
Asymmetric condylar design
Bertin KC, Komistek RD, J. Arthropl 2002
MEDLAT
Roll -back : CR knees

Surgeon A
0° 30° 60° 90°
0
-5
-10
AP position (mm) Anterior
Posterior
Surgeon B
p<.05
Nozaki H, CORR 2002
Asymmetric condylar designLFC

Maximum flexion
CR PS
Tanzer M. Nexgen 112° Nexgen 111°J. Arthropl. 2002
Rorabeck C.H. AMK 108° AMK 108°CORR 2001
Dorr L.D. Apollo 120° Apollo 119°CORR 2000
Shoji H. * Y/S 114° Y/S 117°CORR 1994
Becker M.W. * AGC 111° IB-I 112°CORR 1991 *bilateral knees
Non weight-bearing

PFC CR 103°
PFC PS 113°p<.02
Dennis D. J. Arthropl 1998
Weight-bearing

Kinematics Roll-back Flexion
Gait Strength Proprioception
Patella Instability Loosening Wear
Results
Surgical
Clinical
CR vs PS: Controversy
Exposure Balancing Joint line

Gait analysis
CS knees were less normal than CR
Andriacchi, JBJS-A 1982
+

Wilson, J. Arthroplasty 1996Bolanos, J. Arthroplasty 1998
14 bilateral TKR: one CR, one PS
No difference
Knee flexion angle
Knee flexion moment
Gait analysis (stair climbing)
Percent of cycle
100%
100%
20°
40°
60°
0
-6
-4
-2
Degree
% Body weight
*leg length
PSCR

CR better
Warren, CORR 1993
No difference
Simmons, CORR 1996
Cash, CORR 1996
Lattanzio, J. Arthropl. 1998
Wada, CORR 2002
Position sense (electrogoniometer)
Proprioception

Huang, J. Arthropl. 1998Ishii, J. Orthop. Sci. 1998
Wada M, C0RR 2002
No differences
in isokinetic strength
Strength

Kinematics Roll-back Flexion
Gait Strength Proprioception
Patella Instability Loosening Wear
Results
Surgical
Clinical
CR vs PS: Controversy
Exposure Balancing Joint line

MIS surgery
More difficult PS stemmed component insertion

Easier insertion with unstemmed CR tibial components

Modular PS stemmed component

PCL balancing is difficult
Normal PCL strain
Lotke PA, Am. J. Knee Surg. 1993 10%
Mahoney OM, J. Arthropl 1994 37%
Incavo SJ, CORR 1994 25%

PCL too tight
Limited flexionExcessive posterior poly contact stress and shear forces due to exaggerated rollback
Rocking movement of the tibial component may precipitate loosening, especially in uncemented cases.

Poly lift-off in flexion

Increased femoral rollback in flexion with posterior 1/3 contact rather than mid 1/3 contact of the tibiofemoral articulation

PCL too lose
Flexion instabilityPagano, CORR, 1998
May occur in the CR TKAs with prior patellectomyLaskin, JBJS, 1995
Possible increase in poly wear due to cyclic slidingWalker, ORS, 1991
PCL deficiency in rheumatoid patients with recurrent synovitisLaskin, CORR, 1997
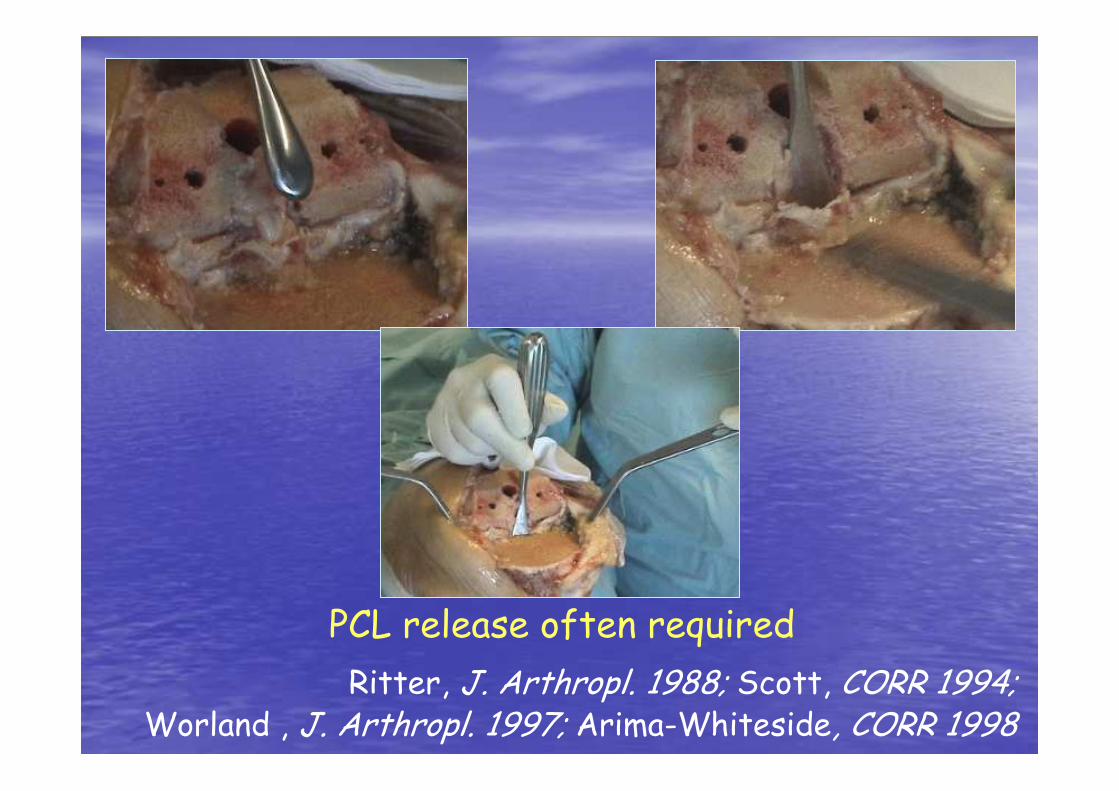
PCL release often required
Ritter, J. Arthropl. 1988; Scott, CORR 1994; Worland , J. Arthropl. 1997; Arima-Whiteside, CORR 1998

Severe deformity (varus>15°)
65 Tricon-CR vs 50 IB-PS
Laskin, CORR 1996
CR showed worse
clinical results &
higher revision rate

Joint line
Possible problem in PS knees

Mihalko-Krackow, CORR 1999
Cadaveric measurementsGap increase (mm)
2
4
6
8
Extension Flexion
p<0.05
F/E gaps changes after PCL section
Kadoya, CORR 2001

Intraoperative measurements
Baldini-Scuderi, J Arthropl in press
F/E gaps changes after PCL section
Gap increase (mm)
0.5
1.0
p>0.05
Extension Flexion
1.5
2.0

Cope-O’Brien, J. Arthroplasty 2002
PS CR
Preop. 2.2 2.2
Postop. 2.4 2.5
Joint line height
J.L. (cm)

Kinematics Roll-back Flexion
Gait Strength Proprioception
Patella Instability Loosening Wear
Results
Surgical
Clinical
CR vs PS: Controversy
Exposure Balancing Joint line

Hozack, CORR 1989
Patellar problemsPS knees

Original IB-I Modified IB-I
Patellar clunkRoundededge
21 % 5 %

Deep and prolonged throclea
IB-II
LPS
Deepened and prolonged throclea
Less prominentshoulder

Distally prolonged throclea
Synovial entrapment
Incidence 13.5% 3.8% 0%p<0.01
Pollock D.C., Engh G.A., JBJS-A 2002
AMK-PS AMK-PScongruency
PFC-PS

Flexion instability
More of a problem with old design CRs
202 AMK (FU: 4 yrs)8% AP instability
Waslewski, J. Arthropl. 1998
Persistent pain
Sense of instability
Recurrent effusions
Pes and retinacular tenderness
Posterior drawer sign
Above average range of motion
Clinical features

Healthy
Alexiades, Scott, AJKS 1989Hagena, Int Orthop 1989
Reduced PCL strength
OA
300
600
Rupture force (N)
p<.0001

Rheumatoid arthritis
F.U. (yrs) Flexion instability
Laskin, Tricon-M 8.2 40% CORR 1997
Schai-Scott, PFC 11.0 2% CORR 1999
Archibeck, MG-I 10.5 3%JBJS-A 2001

PS knees
Lombardi, J. Arthropl. 1993
IB I 0.6 %
IB II 0.2 %
Dislocation
2 mm2 mm
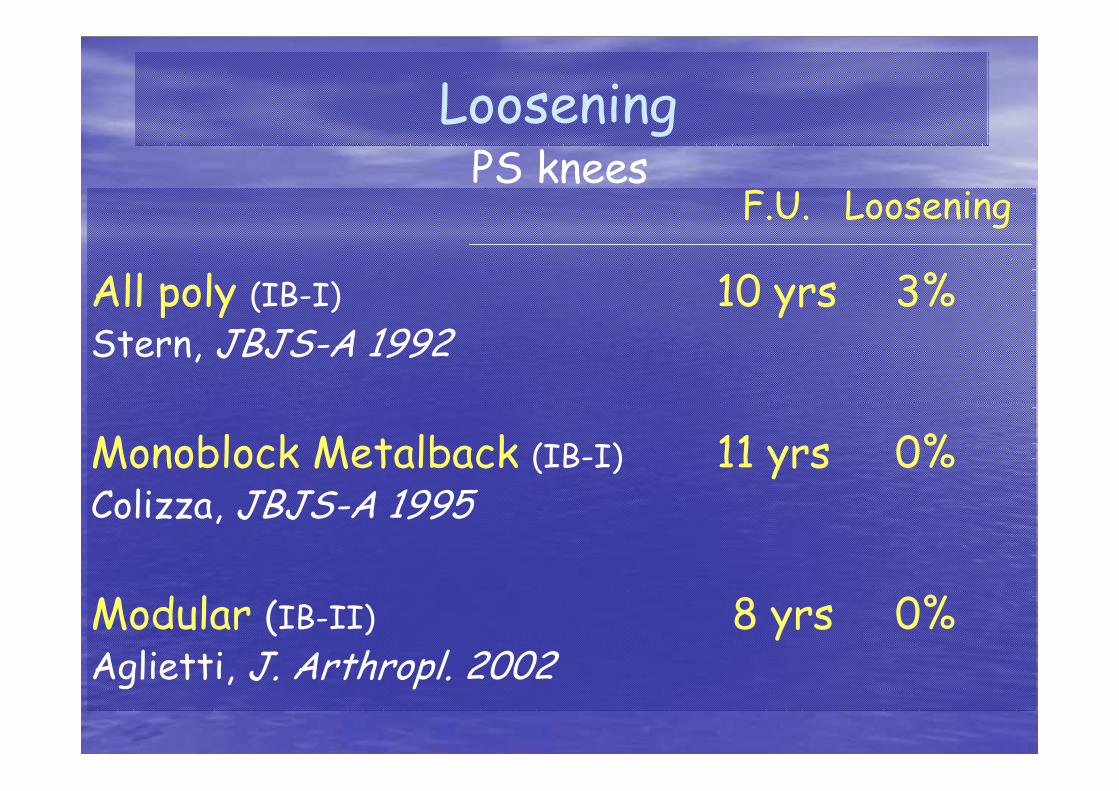
F.U. Loosening
All poly (IB-I) 10 yrs 3%Stern, JBJS-A 1992
Monoblock Metalback (IB-I) 11 yrs 0%Colizza, JBJS-A 1995
Modular (IB-II) 8 yrs 0%Aglietti, J. Arthropl. 2002
LooseningPS knees

F.U. Loosening
Monoblock Metalback (AGC) 15 yrs 0.4%Ritter, CORR 2001
Monoblock Metalback (Kinematic-I) 16 yrs 1.7%Rand, CORR 2001
Modular (MG-I) 11 yrs 0.0%Berger, CORR 2001
CR knees

Flat on flat
Thin poly
Heat compression
PCL tension
CR old mistakes
Wear

If the PCL is retained the tibial component needs to be flat in AP plane.

Posterior impingement occurs with PCL retention and dished tibial component
Kinetic Conflict

PCl retention see-saw effect

Flat tibial tray, poor articular conformity, leads to increased contact stresses and
increased wear

Andriacchi, 1993
Increasing conformity reduces stresses
4
Contact stress (MPa)
3
2
1
5 10 15 20 25Radius ratio R2/R1
1
1
1
1
5
1.5

Benjamin, CORR 2001
Retrieved CR inserts
Length of implantation (yrs) 4.5 8.5
Linear wear (mm/year) 0.4 0.2
Volumetric wear (mm3/year) 959 356
Flat Curved

Meniscal Bearing Knee
Constant posterior
condylar radius
(spherical condyles)
Full conformity

More stresses if conforming
0
5
10
15
20
25
30
35
40
0 1 2 3 4 5 6 7 8 9 10
Axial rotation
MPa
CONFORMING
FLAT
Malrotation in fixed CR
D’Lima-Colwell, CORR 2001
Implant stresses
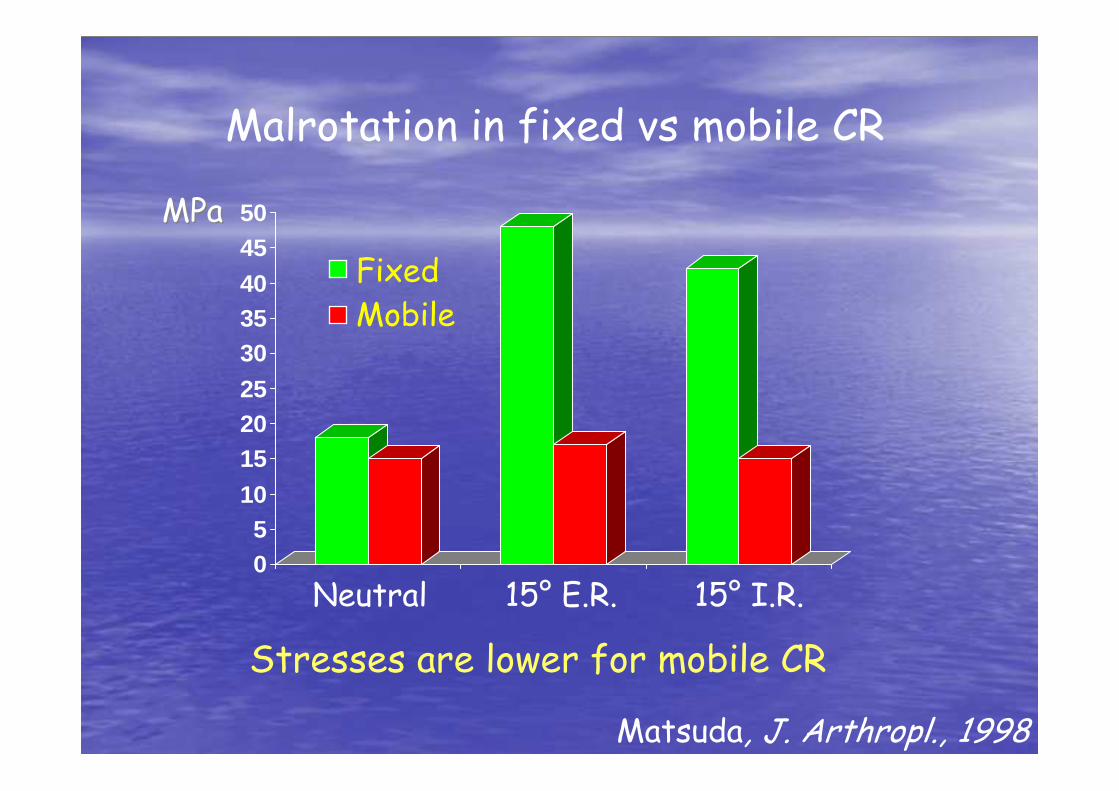
Stresses are lower for mobile CR
05
10
152025
303540
4550
FixedMobile
MPaMPa
Neutral 15° E.R. 15° I.R.
Matsuda, J. Arthropl., 1998
Malrotation in fixed vs mobile CR

0,0000,0100,0200,0300,0400,0500,0600,0700,0800,0900,1000,1100,1200,1300,1400,150
1 2 3 4 5
cycles in the lab (million)
wea
r (g
r)
Wear in PS
Traditionally less of a problem due to improved conformity
Walker, Proc Inst Mech Eng, 1998Walker, CORR, 2000
IB-IIB-II

Tibial post wear: a new entity
Pulosky, JBJS-A, 2001

Hyperextension

Hyperextension
Flexed femoral component

Hyperextension
Flexed femoral component
Malrotation

Hyperextension
Flexed femoral component
Femoral component lift-off
Malrotation
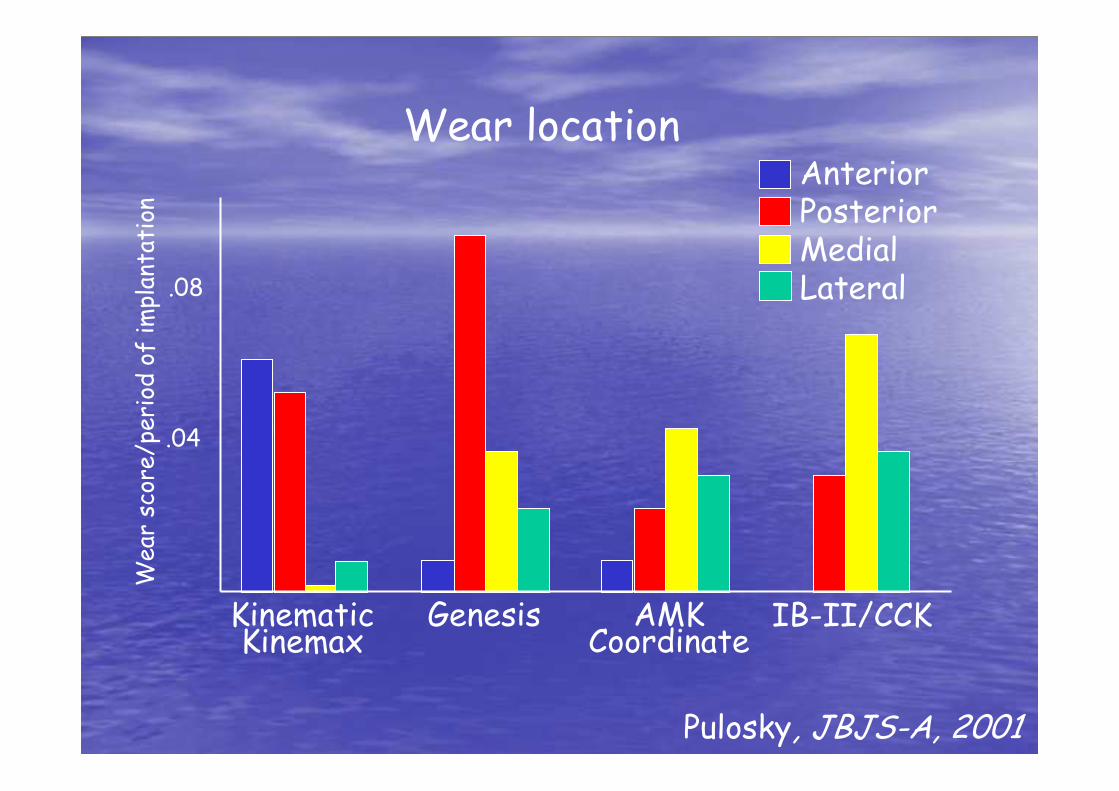
Wear location
.04
.08
Wear score/period of implantation
KinematicKinemax
Genesis AMKCoordinate
IB-II/CCK
AnteriorPosteriorMedialLateral
Pulosky, JBJS-A, 2001

Backside wear: CR & PS
Axial load
MicromotionElastic
deformation
Shear forces
Wasielewski, CORR 2002Parks-Engh, CORR 1998

Implant sources of micromotion
Locking mechanism
Conformity
Cam & post
Common to both prostheses:
PS specific:

F.U.(yrs) E/G Survivorship
Aglietti, 1999 IB-I 10 83% 92%
Li-Bentley, 1999 IB-II 10 94% 92%
Vince, 2000 IB-I 12 84% 92%
Insall, 2001 IB-I 10 96% 96%
IB-II 10 95% 98%
PS knees
Long-term results

F.U.(yrs) E/G Survivorship
Rand, 1995 Kinematic 10 87% 96%
Schai-Scott, 1998 PFC 10 -- 90%
Berger, 2001 MG-I 11 84% 84%
MG-II 9 92% 100%
Ritter, 2001 AGC 11 -- 99%
CR knees

Conclusions
After 25 years of Socratic debate, there is no
clear advantage of one solution to the other.

Keep in mind that not all designs
are the same, in both types

If the results are equal, it is preferable to use
the easier technique

My suggestion: use what you know best.

“Excellence is not a singular act, but a habit: you are what you repeatedly do.”
Aristotle





























