Embed Size (px)
Citation preview

Gynecologic Oncology 130 (2013) 346–349
Contents lists available at SciVerse ScienceDirect
Gynecologic Oncology
j ourna l homepage: www.e lsev ie r .com/ locate /ygyno
The Patient Protection and Affordable Care Act: Impact on the careof gynecologic oncology patients in the absence of Medicaid expansionin Central Virginia☆
Madeleine Courtney-Brooks a,⁎, Elizabeth B. Pelkofski a, Carolyn L. Engelhard b, Linda R. Duska a
a Thornton Gynecology Oncology Service, Department of Obstetrics and Gynecology, University of Virginia Health System, Charlottesville, VA 22908, USAb Health Policy Analyst, University of Virginia Health System, Charlottesville, VA 22908, USA
H I G H L I G H T S
• Medicaid expansion opt-out may decrease access to care for low income uninsured and under-insured gynecologic oncology patients in Central Virginia.• Minority women and women with cancer will be disproportionately affected.
☆ This paper was presented as an oral presentation atAngeles, CA, March 2013.⁎ Corresponding author at: University of Virginia Health
Oncology, Department of Obstetrics and Gynecology, PO22908, USA. Fax: +1 434 982 3271.
E-mail address: [email protected] (M. Courtney
0090-8258/$ – see front matter © 2013 Elsevier Inc. Allhttp://dx.doi.org/10.1016/j.ygyno.2013.04.468
a b s t r a c t
a r t i c l e i n f oArticle history:
Received 25 February 2013Accepted 27 April 2013Available online 3 May 2013Keywords:Medicaid expansionAffordable Care Act
Objective.Many gynecologic oncology (GO) patients inVirginia are low income and their care is supplementedbyDisproportionate ShareHospital (DSH) funds. Our objective is to estimate howmany newGOpatientsmay loseaccess to care if the state forgoes Medicaid expansion.
Methods.New patients referred to the GO service between July 1, 2010 and July 1, 2012 were identified. Datawere collected regarding age, race, referral diagnosis, payor, and state pay scale. Pay scale 1 (PS1) is equal to thefederal poverty level (FPL). Assumptions included the following: (1) pay scale is a surrogate for income, (2) PS1patients will be ineligible for discounted insurance through the exchanges, and (3) decreasing DSH funds will re-
sult in a reduction of the free-care pool.Results. There were 1623 referrals to the GO service and the majority (83%) was Caucasian. The payor distri-bution was 44% commercial insurance, 5.6% Medicaid, 31% Medicare, and 10.4% uninsured. Among the 361womenwhowere PS1, 32% were uninsured. Thirty percent of PS1 patients wereminorities and 47.4% had ama-lignancy. Of note, 52% of new patients with cervical cancer were PS1.
Conclusion. Seven percent of new GO patients are PS1 and uninsured. This population contains a dispropor-tionate number of minorities and women with cancer. These women will have difficulty affording care as DSHfunding decreases, particularly in states with lean Medicaid that opt out of Medicaid expansion. The burden oflack of access to care will be shouldered by an unfortunate few.
© 2013 Elsevier Inc. All rights reserved.
Introduction
In 2010 Barack Obama signed into law the Patient Protection and Af-fordable Care Act (ACA) [1,2]. This historic act ultimately aims to increaseaccess to health care for all Americans and decrease the cost of healthcare but has other equally important goals inmind. For example, with re-spect to cancer patients, the ACA aims to increase access to cancer care,improve quality of care, examine the causes for cancer care disparities,
the SGO Annual Meeting, Los
System, Division of GynecologicBox 800712, Charlottesville, VA
-Brooks).
rights reserved.
and investigate differences in cancer care across the country [3,4]. The ul-timate goal is affordable, comprehensive, and quality cancer care.
Since its passage in 2010, the constitutionality of the ACA has beenchallenged in a number of state and federal courts. The most frequenttarget of the challenges was the individual mandate as many felt thatfining individuals for failing to purchase insurance was not within thescope of Congressional power [5]. Many of these separate cases weremerged into a single case heard by the Supreme Court, entitled NationalFederation of Independent Business v. Sebelius, in June 2012. The SupremeCourt upheld the crucial individual mandate, requiring that all Ameri-cans have health insurance or suffer tax penalties. However, the Su-preme Court also declared that the states were not required toparticipate in the Medicaid expansion, an essential component of theACA in terms of improving access to care for low income patients [6].
The Medicaid program is jointly funded by states and the federalgovernment. Individual states have varying Medicaid eligibility criteria

347M. Courtney-Brooks et al. / Gynecologic Oncology 130 (2013) 346–349
within federal minimum standards, particularly with regard to non-disabled adults without dependent children [7]. The ACA, as it was orig-inally written, included the standardization of Medicaid eligibility re-quirements across the country in order to increase access to care; allUS citizens aged 18–65 years who live under 138% of the federal povertylevel (FPL) would be eligible for Medicaid under the expanded program.After the ACA was passed, estimates suggested that Medicaid expansionwould provide access to care for 16–18 million more Americans [8].Since states now have the ability to “opt-out” of Medicaid expansion,the number of new Americans that will be covered by theMedicaid pro-gram is unknown, but certainly will be lower than original estimates.
Currently the federal government provides funding to hospitalswhich provide care for patients who have low incomes and are under in-sured or uninsured via the Disproportionate Share Hospital (DSH) funds.These are also known as indigent care funds, or in Virginia as the “freecare pool.” As a result of the expectation that all states would participatein the Medicaid expansion, under the full institution of the ACA sched-uled for 2014 these funds will begin to be phased out [9]. While thefinal plan for this staged reduction has not been determined, it is veryclear that the DSH funds will significantly diminish. For states thatchoose to “opt out” of the Medicaid expansion, the same level of DSHfundswill no longer be available to cover the cost of caring for uninsuredpatients [9].
In Virginia, Medicaid eligibility requirements are particularly strict.Patients who are aged 18–65 years are not eligible for Medicaid regard-less of income unless they are disabled, pregnant, or have dependentchildren. At the University of Virginia (UVA) and at other state univer-sity teaching hospitals, pay scales have been developed based on in-come, assets, and number of dependents to determine the amount ofmoney a patient must pay for his or her care. These pay scales rangefrom a 0% co-pay to a 100% co-pay. For patientswhomeet criteria for in-digent care, the hospital and physicians are further reimbursed by theDSH funds. At the time of this writing, Virginia has declared that theCommonwealthwill “opt out” of theMedicaid expansion.What this de-cisionmeans is that with the impending decrease in the DSH funds, thehospitals caring for indigent patients may no longer be reimbursed atthe current rate for these patients' care.
In addition, a “coverage gap”will exist in Virginia. The insurance ex-changes created by the ACA were intended to serve patients who haveincomes greater than 100% of FPL, since patients making less would beeligible for Medicaid under the expanded eligibility criteria written intothe original ACA. Should Virginia opt out of Medicaid expansion, manypatients with an income b100% of FPL will not be covered by Medicaidand also will not be eligible to buy discounted insurance through theexchanges.
Currently the patient population at UVA includes a significant pro-portion of low income uninsured and under-insured patients. The hos-pital system is reimbursed for providing their care via DSH funds. Withthe possibility that Virginia may opt out of Medicaid expansion and thedecrease in DSH payments looming on the horizon, these low incomeuninsured and under-insured patients may lose access to free care butstill not qualify for Medicaid or be eligible for discounted health insur-ance. As providers we may lose the ability to provide care for this
Table 1State university teaching hospitals guidelines for medically indigent patients: annual incom
Pay scale 1 Pay scale 2 Pay sc
Number of dependents 0% co-pay 5% co-pay 20% co
1 0–11,170 11,171–12,287 12,2882 0–15,160 15,131–16,643 16,6443 0–19,090 19,091–20,999 21,0004 0–23,050 23,051–25,355 25,3565 0–27,010 27,011–29,711 29,7126 0–30,970 30,971–34,067 34,0687 0–34,930 34,931–38,423 38,4248 0–38,890 38,891–42,779 42,780
group of patients. Our objective in this study is to estimate how manynew referrals to the gynecologic oncology service at the University ofVirginia will no longer have access to care in the event the state forgoesMedicaid expansion.
Materials and methods
Study approval was obtained from the University of Virginia (UVA)institutional review board. We identified all women who presentedfor a new patient visit to a gynecologic oncology provider betweenJuly 1, 2010 and July 1, 2012.Womenwere identified using departmen-tal records of new patient referrals. UVA's Clinical Data Repository(CDR) was used to obtain additional information including age; race;place of residence; referring physician; referral diagnosis; payor; andstate pay scale assignment.
State pay scale assignment
Currently at the University of Virginia, patients who are uninsured,have income up to 200% of the FPL, and whose assets do not exceed agiven threshold qualify for the hospital's indigent care program. Thesepatients are assigned a pay scale based on income, number of depen-dents and assets. A patient's pay scale then determines the co-pay forwhich he or she will be responsible. The annual income ranges foreach pay scale level are presented in Table 1. In short, the incomelimit for pay scale 1 (0% co-pay) is ≤100% of the FPL and for pay scale7 (100% co-pay) is >200% of the FPL. The annual income limits for payscale 2 (5% co-pay), 3 (20% co-pay), 4 (45% co-pay), and 5 (70%co-pay) are between 100% and 200% of the FPL. The amount of assetsallowed is also based on the number of people in the household. Ahousehold of one person is allowed $2000 in assets, two people $3000in assets, and another $100 in assets is allowed for each additional per-son in the household. A patient must meet both income and assetcriteria to qualify for the indigent care program.
Study model
Assumptions in our study model include (1) state pay scale, calcu-lated using formulas that include income, number of dependents andassets, is a surrogate for income, (2) in Virginia, women who are cur-rently uninsured with an income b100% of the FPL will be ineligiblefor a health insurance subsidy to buy discounted insurance throughhealth care exchanges and (3) the reduction of the DSH funds will re-sult in a reduction of the current free care pool.
Results
There were 1623 new patient referrals to the UVA gynecologic on-cology clinic during the study time period. The demographic informa-tion for the entire population of new referrals is presented in Table 2.Themeanpatient agewas 56.4 years.Most patients (68.5%)were youn-ger than 65 years and therefore did not qualify forMedicare. Themajor-ity of women were Caucasian (83%) with smaller percentages of Black
e ranges for fiscal year 2013.
ale 3 Pay scale 4 Pay scale 5 Pay scale 7
-pay 45% co-pay 70% co-pay 100% co-pay
–14,893 14,894–18,617 18,618–22,340 22,341–over–20,173 20,174–25,217 25,218–30,260 30,261–over–25,453 25,454–31,817 31,818–38,180 38,181–over–30,733 30,734–38,417 38,418–46,100 46,101–over–36,012 36,013–45,018 45,019–54,020 54,021–over–41,292 41,293–51,618 51,619–61,940 61,941–over–46,572 46,573–58,218 58,219–69,860 69,861–over–51,852 51,853–64,818 64,819–77,780 77,781–over
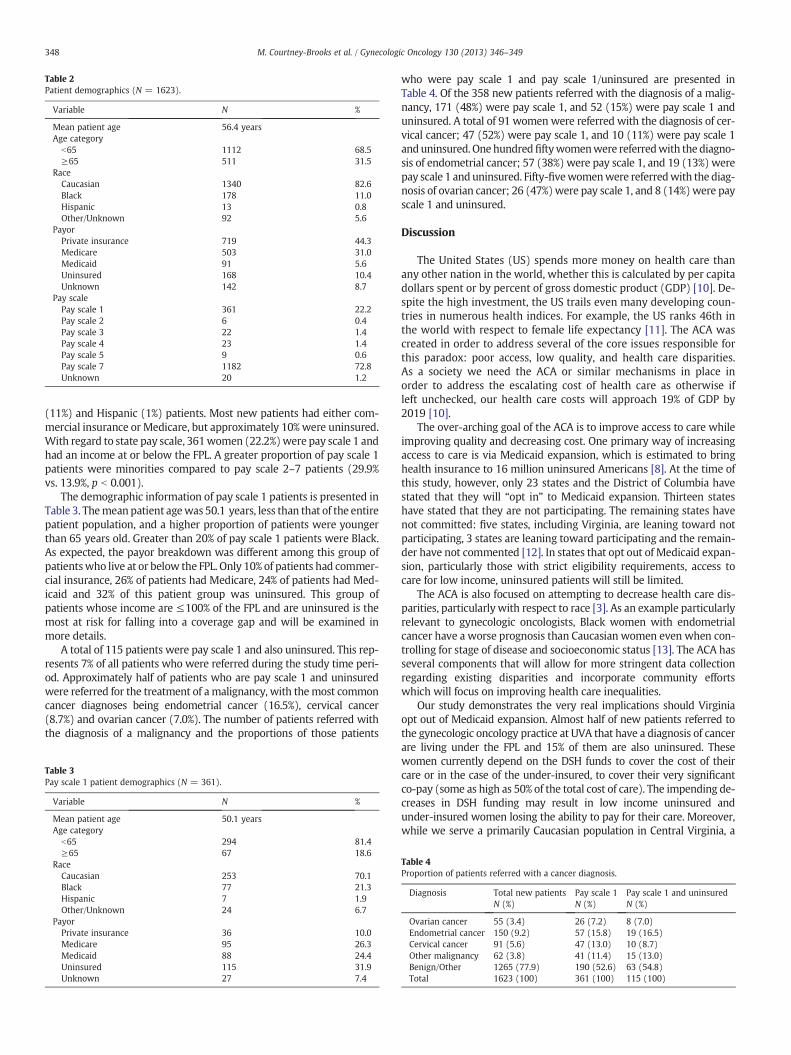
Table 2Patient demographics (N = 1623).
Variable N %
Mean patient age 56.4 yearsAge category
b65 1112 68.5≥65 511 31.5
RaceCaucasian 1340 82.6Black 178 11.0Hispanic 13 0.8Other/Unknown 92 5.6
PayorPrivate insurance 719 44.3Medicare 503 31.0Medicaid 91 5.6Uninsured 168 10.4Unknown 142 8.7
Pay scalePay scale 1 361 22.2Pay scale 2 6 0.4Pay scale 3 22 1.4Pay scale 4 23 1.4Pay scale 5 9 0.6Pay scale 7 1182 72.8Unknown 20 1.2
348 M. Courtney-Brooks et al. / Gynecologic Oncology 130 (2013) 346–349
(11%) and Hispanic (1%) patients. Most new patients had either com-mercial insurance or Medicare, but approximately 10% were uninsured.With regard to state pay scale, 361women (22.2%)were pay scale 1 andhad an income at or below the FPL. A greater proportion of pay scale 1patients were minorities compared to pay scale 2–7 patients (29.9%vs. 13.9%, p b 0.001).
The demographic information of pay scale 1 patients is presented inTable 3. Themean patient agewas 50.1 years, less than that of the entirepatient population, and a higher proportion of patients were youngerthan 65 years old. Greater than 20% of pay scale 1 patients were Black.As expected, the payor breakdown was different among this group ofpatientswho live at or below the FPL. Only 10% of patients had commer-cial insurance, 26% of patients had Medicare, 24% of patients had Med-icaid and 32% of this patient group was uninsured. This group ofpatients whose income are ≤100% of the FPL and are uninsured is themost at risk for falling into a coverage gap and will be examined inmore details.
A total of 115 patients were pay scale 1 and also uninsured. This rep-resents 7% of all patients who were referred during the study time peri-od. Approximately half of patients who are pay scale 1 and uninsuredwere referred for the treatment of amalignancy, with themost commoncancer diagnoses being endometrial cancer (16.5%), cervical cancer(8.7%) and ovarian cancer (7.0%). The number of patients referred withthe diagnosis of a malignancy and the proportions of those patients
Table 3Pay scale 1 patient demographics (N = 361).
Variable N %
Mean patient age 50.1 yearsAge category
b65 294 81.4≥65 67 18.6
RaceCaucasian 253 70.1Black 77 21.3Hispanic 7 1.9Other/Unknown 24 6.7
PayorPrivate insurance 36 10.0Medicare 95 26.3Medicaid 88 24.4Uninsured 115 31.9Unknown 27 7.4
who were pay scale 1 and pay scale 1/uninsured are presented inTable 4. Of the 358 new patients referred with the diagnosis of a malig-nancy, 171 (48%) were pay scale 1, and 52 (15%) were pay scale 1 anduninsured. A total of 91 women were referred with the diagnosis of cer-vical cancer; 47 (52%) were pay scale 1, and 10 (11%) were pay scale 1anduninsured. Onehundredfiftywomenwere referredwith the diagno-sis of endometrial cancer; 57 (38%) were pay scale 1, and 19 (13%) werepay scale 1 anduninsured. Fifty-fivewomenwere referredwith the diag-nosis of ovarian cancer; 26 (47%)were pay scale 1, and 8 (14%)were payscale 1 and uninsured.
Discussion
The United States (US) spends more money on health care thanany other nation in the world, whether this is calculated by per capitadollars spent or by percent of gross domestic product (GDP) [10]. De-spite the high investment, the US trails even many developing coun-tries in numerous health indices. For example, the US ranks 46th inthe world with respect to female life expectancy [11]. The ACA wascreated in order to address several of the core issues responsible forthis paradox: poor access, low quality, and health care disparities.As a society we need the ACA or similar mechanisms in place inorder to address the escalating cost of health care as otherwise ifleft unchecked, our health care costs will approach 19% of GDP by2019 [10].
The over-arching goal of the ACA is to improve access to care whileimproving quality and decreasing cost. One primary way of increasingaccess to care is via Medicaid expansion, which is estimated to bringhealth insurance to 16 million uninsured Americans [8]. At the time ofthis study, however, only 23 states and the District of Columbia havestated that they will “opt in” to Medicaid expansion. Thirteen stateshave stated that they are not participating. The remaining states havenot committed: five states, including Virginia, are leaning toward notparticipating, 3 states are leaning toward participating and the remain-der have not commented [12]. In states that opt out of Medicaid expan-sion, particularly those with strict eligibility requirements, access tocare for low income, uninsured patients will still be limited.
The ACA is also focused on attempting to decrease health care dis-parities, particularly with respect to race [3]. As an example particularlyrelevant to gynecologic oncologists, Black women with endometrialcancer have a worse prognosis than Caucasian women even when con-trolling for stage of disease and socioeconomic status [13]. The ACA hasseveral components that will allow for more stringent data collectionregarding existing disparities and incorporate community effortswhich will focus on improving health care inequalities.
Our study demonstrates the very real implications should Virginiaopt out of Medicaid expansion. Almost half of new patients referred tothe gynecologic oncology practice at UVA that have a diagnosis of cancerare living under the FPL and 15% of them are also uninsured. Thesewomen currently depend on the DSH funds to cover the cost of theircare or in the case of the under-insured, to cover their very significantco-pay (some as high as 50% of the total cost of care). The impending de-creases in DSH funding may result in low income uninsured andunder-insured women losing the ability to pay for their care. Moreover,while we serve a primarily Caucasian population in Central Virginia, a
Table 4Proportion of patients referred with a cancer diagnosis.
Diagnosis Total new patientsN (%)
Pay scale 1N (%)
Pay scale 1 and uninsuredN (%)
Ovarian cancer 55 (3.4) 26 (7.2) 8 (7.0)Endometrial cancer 150 (9.2) 57 (15.8) 19 (16.5)Cervical cancer 91 (5.6) 47 (13.0) 10 (8.7)Other malignancy 62 (3.8) 41 (11.4) 15 (13.0)Benign/Other 1265 (77.9) 190 (52.6) 63 (54.8)Total 1623 (100) 361 (100) 115 (100)

349M. Courtney-Brooks et al. / Gynecologic Oncology 130 (2013) 346–349
disproportionate number of our patients who live under the FPL are mi-norities. Should Virginia opt out of Medicaid expansion, disparities incancer care may increase further.
Unfortunately this is likely to be a problem that is not isolated toVirginia. At the time of this study 13 states have declared that theyare not going to participate in Medicaid expansion: Alabama, Georgia,Idaho, Louisiana, Maine, Mississippi, North Carolina, Oklahoma, Penn-sylvania, South Carolina, South Dakota, Texas and Wisconsin [12].Many of these states also have strict Medicaid eligibility requirementsand will also likely have a significant number of patients who fall intothe coverage gap without Medicaid expansion.
The most common argument against Medicaid expansion is cost.Many states have expressed concern that increasing the Medicaidpool will result in a huge financial burden placed on the states. The fed-eral government has stated that it will cover the full cost of most of thenewly eligible Medicaid patients. In later years federal matching ratewill decline slightly but will still remain above the regular Medicaidmatching rate at 90%. For example, from 2014 to 2016 the federal gov-ernmentwill pay 100%of newly eligible adults; this ratewill decrease to95% in 2017, 94% in 2018, and ultimately 90% in 2020 and future years[14]. Several states such as Pennsylvania and Florida have hired inde-pendent organizations to assess the economic implications of partici-pating in Medicaid expansion [15,16]. A recent report by RANDexamined the economic implications of the ACA in Pennsylvania witha particular focus on the state's decision to expand Medicaid. As onewould expect, they found that expanding Medicaid would decreasethe number of uninsured and would also decrease uncompensatedcare costs. Expanding Medicaid would also bring in substantial govern-ment funds and in the initial years of Medicaid expansion, the statewould see a net surplus. However “in 2017 and beyond the state costsfor the expansion will grow. Beginning in 2017, there will be a netflow of money out of the state regardless of how the Medicaid expan-sion is handled; however, Pennsylvania will see much larger outflowswithout the expansion of eligibility [15].”While at first glance the con-cept of Medicaid expansion may seem to likely result in increased costsfor states, the bulk of the expansion will be federally funded for the firstseveral years and may actually decrease net state expenditures as sug-gested by the work by RAND in Pennsylvania. We encourage objectiveassessment by states questioning the economic feasibility of Medicaidexpansion prior to claiming that the cost is prohibitive.
The causes of disparities in cancer arise from a complicated interplayof social, economic, cultural, and health system factors and have been ex-amined by two recent Institute of Medicine reports as well as a numberof studies specifically exploring gynecologic cancers [17–21]. The ACA at-tempts to address health care disparities primarily by increasing accessto care via Medicaid expansion. However, we recognize that expandingMedicaid will not address all sources of health care disparities. Otherpossible interventions include those directed at increasing cancerscreening rates, improving the stability of the patient–physician relation-ship in publicly funded health plans and instituting multi-disciplinarycare teams including patient navigators for cancer screening and treat-ment [22]. A recent commentary in the Journal of Clinical Oncology dis-cusses the success of a recent attempt to eliminate disparities incolorectal cancer (CRC) in the state of Delaware. Using the combinationof a comprehensive screening program, patient navigation for screeningand care coordination and case management, over a 7 year period CRCscreening disparities were eliminated, incidence rates were equalizedand mortality differences were nearly eliminated [23].
At UVA we are one of the larger providers of care for uninsured andunder-insured women in Central Virginia with gynecologic cancer. Inorder to continue to provide care to these women, we will need tolobby the Commonwealth to participate in the Medicaid expansion.
The ACA stands to impart many benefits to women with cancer: it willincrease access to care, attempt to identify and address disparities,allow patients with pre-existing conditions (such as gynecologic cancer)to obtain health insurance, and mandate payment for all phases of clini-cal trials. However, in order tomaximize the number ofwomenwhowillbenefit from the ACA,wewill need to encourage our governors to partic-ipate fully in the Medicaid expansion. If not carefully evaluated, in statesopting out of Medicaid expansion, society's most vulnerable groups maycontinue to bear the disproportionate share of poor access to care.
Conflict of interest statement
The authors have no conflicts of interest to report.
References
[1] Patient Protection and Affordable Care Act. Public Law 111-148.http://www.gpo.gov/fdsys/pkg/PLAW-111publ148/html/PLAW-111publ148.htm . [Accessed February 17,2012].
[2] Health Care and Education Reconciliation Act of 2010. Public Law 111-152.http://www.gpo.gov/fdsys/pkg/PLAW-111publ152/html/PLAW-111 . [Accessed February17, 2012].
[3] Moy B, Polite BN, Halpern MT, Stranne SK, Winer EP, Wollins DS, et al. AmericanSociety of Clinical Oncology policy statement: opportunities in the Patient Protec-tion and Affordable Care Act to reduce cancer care disparities. J Clin Oncol Oct 12011;29:3816–24.
[4] Moy B, Abernethy AP, Peppercorn J. Core elements of the Patient Protection and Af-fordable Care Act and their relevance to the delivery of high-quality cancer care;2012.
[5] Hodge Jr JG, Brown EC, Orenstein DG, O'Keefe S. Congress, courts, and commerce:upholding the individual mandate to protect the public's health. J Law Med EthicsFall 2011;39:394–400.
[6] Rosenbaum S, Westmoreland TM. The Supreme Court's surprising decision on theMedicaid expansion: howwill the federal government and states proceed? HealthAff (Millwood) Aug 2012;31:1663–72.
[7] Where are States Today? Medicaid and CHIP Eligibility Levels for Children andNon-Disabled Adults—Kaiser Family Foundation. http://www.kff.org/medicaid/7993.cfm.
[8] Foundation KF. Financing newMedicaid coverage under health reform: the role ofthe federal government and states. FOCUS on Health Reform; 2010.
[9] Davis C. National health Law, Program; 2012.[10] Braveman PA, Egerter SA, Mockenhaupt RE. Broadening the focus: the need
to address the social determinants of health. Am J Prev Med Jan 2011;40:S4–S18.
[11] Muennig PA, Glied SA. What changes in survival rates tell us about us health care.Health Aff (Millwood) Nov 2010;29:2105–13.
[12] Where each state stands on ACA's Medicaid expansion. http://www.advisory.com/Daily-Briefing/2012/11/09/MedicaidMap.
[13] Olson SH, Atoria CL, Cote ML, Cook LS, Rastogi R, Soslow RA, et al. The impact ofrace and comorbidity on survival in endometrial cancer. Cancer Epidemiol Bio-markers Prev May 2012;21:753–60.
[14] Newly Eligible Medicaid Recipients Under Health Care Reform and FederalMatching Funds (§2001) - Eff. Date: 1/1/2014. http://www.ahcancal.org/advocacy/Pages/NewlyEligibleMedicaidRecipientsHCR.aspx.
[15] The Economic Impact of Medicaid Expansion on Pennsylvania. http://www.rand.org/content/dam/rand/pubs/research_reports/RR200/RR256/RAND_RR256.pdf.
[16] Florida's Medicaid Choice: Understanding Implications of Supreme Court Rulingon Affordable Health Care Act. http://hpi.georgetown.edu/floridamedicaid/pdfs/florida-medicaid-choice-nov-2012.pdf.
[17] Institute of Medicine. The unequal burden of cancer. Washington, DC: NationalAcademy Press; 1999.
[18] Institute of Medicine. Unequal treatment: confronting racial and ethnic dispar-ities in healthcare. Washington, DC: National Academy Press; 2003.
[19] Farley J, Risinger JI, Rose GS, Maxwell GL. Racial disparities in Blacks with gyneco-logic cancers. Cancer Jul 15 2007;110:234–43.
[20] Bristow RE, Powell MA, Al-Hammadi N, Chen L, Miller JP, Roland PY. Disparities inovarian cancer care quality and survival according to race and socioeconomicstatus.J Natl Cancer Inst Apr 4 2013 [Epub ahead of print, in press].
[21] Bristow RE, Zahurak ML, Ibeanu OA. Racial disparities in ovarian cancer sur-gical care: a population-based analysis. Gynecol Oncol May 1 2011;121:364–8.
[22] Natale-Pereira A, Enard KR, Nevarez L, Jones LA. The role of patient navigators ineliminating health disparities. Cancer Aug 2011;117:3543–52.
[23] Grubbs SS, Polite BN, Carney Jr J, Bowser W, Rogers J, Katurakes N, et al. Eliminat-ing racial disparities in colorectal cancer in the real world: it took a village.J ClinOncol Apr 15 2013 [Epub ahead of print, in press].