Embed Size (px)
Citation preview

M O Ababneh, FRCA
Jordan Hospital
Amman
The Oxygen Dilemma!
Can Too Much O2 Kill?


• A science and health writer and editor in Stratford-upon-
Avon, UK.
• Main interests are Medicine, Neuroscience and
Psychology.
Without it, cells die.
With too much, they die even faster
Victoria Stern | Oct 1, 2008
Works as a contributing editor and, a freelance writer, in.

• Oxygen is Vital for Life — without it, severe brain
damage may occur in as little as 3 minutes.
So doctors routinely treat traumas such as heart attack or
stroke by providing victims with more oxygen.
Mounting Evidence suggests, however, that
resuscitating with too much of the gas may actually have a Harmful effect.
• Researchers at the University of Texas Southwestern
Medical Center at Dallas reported in the Journal of Cerebral
Blood Flow and Metabolism (March. 2008), that resuscitating babymice with pure oxygen caused more brain damage
and Cerebral Palsy–Like problems, as compared with
mice that breathed air during resuscitation.“Our results are contrary to what one would expect,” “Many think oxygen doesn’t hurt and you can give as
much as possible to make up for a deficiency.
Our study shows this notion is wrong !.”
Steven G. Kernie, M.D.
Associate Professor of Pediatrics, Pathology and Cell Biology
Director, Pediatric Critical Care Medicine

• It raises the important Possibility that doctors are
treating patients the Wrong Way, says Lance
Becker, who similarly showed that cells were muchmore likely to die after being reexposed tooxygen than they were when deprived.
Professor of emergency medicine at the University of Pennsylvania School of Medicine and director of its Center for Resuscitation Science*,
In fact;Physicians do not know how much is too much.
Or whether administering extra amounts actually benefits patients at all.

• That oxygen mask they strap on patients rushed to
the ER after a heart attack or a stroke?
It could be doing more Harm than good in many
cases, Dutch researchers say in a new report.
• VUMC research group found no support for
routinely giving critically ill patients high-dose
oxygen, a common practice among paramedics and
emergency physicians.
Health | Wed Jan 11, 2012Report;
Extra oxygen may harm
emergency patients
• "There is NOT a single study that points to beneficial effects !"Dr. Yvo Smulders.
Read more at Reutershttp://www.reuters.com/article/2012/01/11/us-oxygen-patients-
Prof Dr. Yvo Smulders theme leader of ICaR-VU.Professor in Internal medicine for Vascular diseases.
"All of the evidence that we found points to “Detrimental Effects.”

• Most doctors believe extra oxygen is life-savingand many guidelines recommend it.
• "What you would expect is that oxygen is healthy,”.
“But it seems that god didn’t introduce 20%
oxygen in room air FOR NOTHING.”

• All the human research I could find on supplementaloxygen after Heart attacks, Strokes, Cardiacarrest and Acute attacks COPD.
Came up with; all had the same grim message:
Supplemental Oxygen doesn't work, and there issome evidence that it might be Harmful.
“I think it is about time that you step away from your instinct approach and look at the EVIDENCE.”
• One trial found 9 out of 80 (11%) heart attack
patients who got oxygen died.
Compared to just 3 out of 77 (4%) who got
compressed air.
Although that difference could have been a statistical
fluke, it was still bad news for oxygen.
“Another trial, in stroke patients, had to be
stopped early because too many patients who got extra oxygen died.
• A high flow oxygen to achieve high oxygen
concentration in inspired air has been a central part of
the standard treatment for suspected MI.
The infamous MONA treatment.
Is 100% oxygen good for you?
OXYGEN.
ENOUGH, ALREADY
Posted on April 11, 2015 by Thomas D
But hyper-oxygenation does have an effect. A negative effect.
That was shown already back in the 50s.
So why are we still giving high flow oxygen to
patients ?

Richard Beasley1, Sarah Aldington1, 1Medical Research Institute of New Zealand, PO Box 10055, Wellington, New Zealand 2University of Southampton, Southampton, UK
OXYGEN THERAPY IN MI
Posted on April 11, 2015 by Thomas D

• The AHA currently recommends giving supplementaloxygen to people with cardiac arrest Until theheart is Restarted.
They urges doctors and paramedics to use
measurements to ensure that oxygen levels in the
blood is not too high.
What often happens is that providers just leave the
oxygen on full blast.
"They don't realize they are giving too much oxygen,”.
"It's just not something they are paying attention to."

• When a reliable measurement of oxygen saturation of
arterial blood (e.g. Pulse Oximetry (SpO2)) can be
achieved, titrate the inspired oxygen concentration toachieve an SpO2 of 94–98%.
McNulty PH, et al. Effects of supplemental oxygen administration on coronary blood flow in patients undergoing cardiac
catheterization. Am J Physiol Heart Circ Physiol 2005; 288: H1057-H1062.
5 minutes of Oxygen by non-rebreather Decreasescoronary blood flow by 30%, Increases coronary resistance by 40%, and Blunts the effect of vasodilator medications like Nitroglycerine.
Consider this:

• Habre et al, highlighting the importance of thebalance between risk and benefit for perioperative
oxygen administration.
• They propose that the Risk–Benefit of inspired
oxygen is higher in higher concentrations of inspired
oxygen and being more Harmful.
•D. Martin1,* M. Grocott2•1London, UK 2Southampton, UK
Recommendations for
perioperative oxygenation

• A long-term follow-up of this large RCT (1386 patients)
comparing the effect of 30% vs 80% oxygen during
and after abdominal surgery.
The 80% inspired oxygen group had an Increased long-
term mortality, specifically in those patients with cancer,and a shorter Cancer-free Survival.
Meyhoff CS, Jorgensen LN, Wetterslev J, Siersma VD, Rasmussen LS . Risk of new or recurrent cancer after a high perioperative inspiratory oxygen fraction during
abdominal surgery. Br J Anaesth 2014; 113(Suppl 1): i74–81
This Harm signal, a new recommendations
are warranted
Cancer patients!

Can oxygen hurt our patients?
PediatricsSeptember 2012, VOLUME 110 / ISSUE 3
Oxygen Therapy: 50 Years of Uncertainty
Win Tin
Crit Care Med. 2013;41(2):423-432
More Oxygen Can’t Hurt…Can It?by William E. "Gene" Gandy, JD, LP and Steven "Kelly" Grayson, NREMT-P, CCEMT-P On May 1, 2013

• Drug we use most often in EMS can cause harm if
we give it without good reason.
• EMS providers began giving oxygen not because it
had medically or scientifically demonstrated benefits
for patients, But Because They Could.
Yet, inarguably, hypoxia is bad.
Can oxygen hurt our patients?
Mike McEvoy
Jul 1, 2012 Updated June 5, 2015
More recent studies suggest that Hyperoxia, can be Equally Dangerous.
Hence the drug EMS providers administer most often may not be as safe as originally
thought.

• We’ve known since 1999 that oxygen worsenedsurvival in patients with minor to moderate strokesand made no difference for patients with severestroke.
In fact, the AHA recommended in 1994 againstsupplemental oxygen for non-hypoxemic strokepatients.
Ronning OM, Guldvog B. Should Stroke Victims Routinely Receive Supplemental
Oxygen? A Quasi-Randomized Controlled Trial. Stroke 1999;30:2033-2037.
Mike McEvoy

• First Aid – like any body of knowledge - changes and so
it should as new evidence emerges.
• CPR ratios have changed over the years as new evidence
gains enough credence and popularity to justify new ways
of thinking.
• Where 2 L of IV Fluid were routinely given to trauma
casualties, we now apply a more measured approach.
• Because of the long term complications which may arise
from prolonged immobilisation, a view of spinal
management is evolving rather than collaring and boarding
all casualties suspected of spinal injury.
Oxygen –
Sometimes less is more.
Hughes S. (2011) “Oxygen for MI: More harm than good?” http://www.medscape.com/viewarticle/748764.
• While change can be Frustrating, change in
response to developing knowledge and
understanding is the Only way we can ensure we
are providing the best possible care.
We wouldn’t administer any other drug with impunity
so why are we so happy to automatically put so
many casualties on High Flow Oxygen?
Make no mistake:
Oxygen is LIFE SAVING.
But oxygen, like all drugs, affects the body.

• So why would treating injuries with a molecule thatfuels life actually do the reverse?
Evidence suggests that pumping in too much oxygen
too quickly can strip the molecule of a single electron,creating a Free Radical.
Free radicals, are highly reactive with other
molecules, including vital DNA and proteins, theDestruction of which can damage or Kill cells.

• Treating with too much oxygen, therefore, could
increase the production of free radicals and makea Bad Situation even Worse.
The key is to find that “Sweet Spot,”—the optimal
amount to give a person so he or she can recover
with minimal damage.
Lance Becker
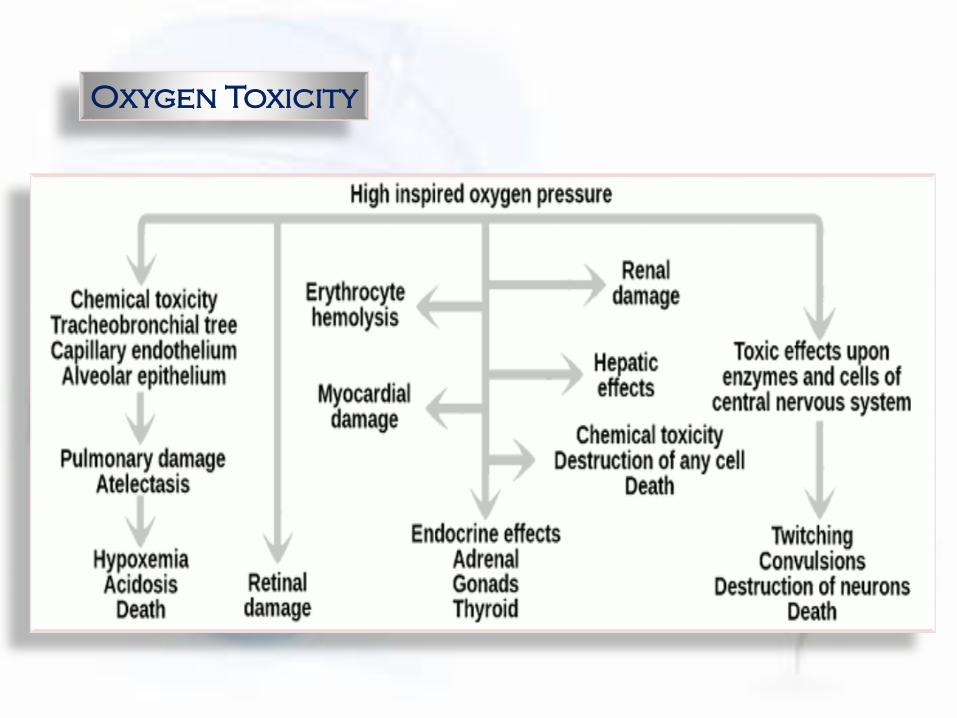
Oxygen Toxicity

• What is new are prehospital research studies comparing
outcomes of patients treated without oxygen or with
oxygen titrated to saturations versus patients routinely
given high flow oxygen.
These data are Frightening; they show impressive patient
harm from even Short periods of hyperoxia.
Research ?

• In a study of 5,549 trauma patients in Texas showed
prehospital supplemental oxygen administration
nearly Doubled mortality.
Stockinger ZT, McSwain NE. Prehospital Supplemental Oxygen in Trauma
Patients: Its Efficacy and Implications for Military Medical Care. Mil Med. 2014;169:609-612.
Other studies are showing a troubling pattern of
Worse outcomes associated with hyperoxia post
cardiac arrest.
Austin MA, Wills KE, Blizzard L, Walters EH, Wood-Baker R.
Effect of high flow oxygen on mortality in chronic obstructive pulmonary disease patients in prehospital
setting: randomised controlled trial. BMJ 2010;341:c5462.
Kilgannon JH, Jones AE, Parillo JE, at al. Emergency Medicine Shock Research Network
(EMShockNet) Investigators. Relationship between supranormal oxygen tension and outcome after
resuscitation from cardiac arrest. Circulation 2011;14:2717-2722.
It showed a Reduction in deaths during subsequent
hospitalization of 78% in COPD patients and 58% in all
patients.
Another study compared patients titrated tosaturations of 88 - 92 % vs Non-rebreather oxygenmasks.
• Knowing that both Hypoxia and Hyperoxia are
bad, EMS providers must stop giving oxygenroutinely.
Oxygen saturations should be measured on every patient.
• Protocols need to be aligned to reflect the 2015
guidelines:
Where do we go from here?
Administer oxygen to O2 Sats. between 94 and 96%.
No patient needs oxygen saturations above 97% and
in truth, there is little evidence suggesting any
clinical benefit of oxygen saturations above 90% in
any patient.

• Modifications (Protocols) in prehospital equipment in
controlling oxygen doses administered to patients
should be changed.
In all likelihood, the Venturi mask will make a
comeback, allowing EMS providers to deliver varied
concentrations of oxygen as needed to keep oxygensaturations between 94 - 96%.

• Few patients will require non-rebreather masks whichare prone to deliver too much oxygen (Hyperoxia).
CPAP devices will also need redesign as most
conventional EMS CPAP delivers 100% oxygen.
A study, found that prehospital CPAP using low oxygen
levels (28 - 30%) was highly effective and safe.
Bledsoe BE, Anderson E, Hodnick R, Johnson S, Dievendorf E. Low-Fractional Oxygen Concentration
Continuous Positive Airway Pressure Is Effective In The Prehospital Setting. Prehosp Emerg Care 2012;16:217-221.

• The drug we use most often can cause Harm if we
give it without good reason.
The Oxygen Dilemma!
Can Too Much O2 Kill?
This is more of an answer, too much oxygen can be harmful
While change can be Frustrating, change in
response to developing knowledge and understanding is the Only way we can ensure we are
providing the best possible care.