Embed Size (px)
Citation preview
The Ontario Stroke Strategy
Southeastern Ontario (SEO) May 2005
Cally Martin, BScPT, MSc(Rehab)Regional Stroke Coordinator, SEO
Ontario Stroke Strategy
• Stroke = leading cause of death and disability with high health care and human costs (1994 study: direct and indirect cost of stroke care in Ontario approached $964 million a year)
• Report of MOH and HSFO: “Towards an Integrated Stroke Strategy for Ontario”
• May 2000 MOHLTC announced budget for a Provincial Integrated Stroke Strategy
Based on demonstration phase spear-headed by the HSFO
3 components:
• public awareness
• professional education
• systems change
Ontario Stroke Strategy - Funding• KGH designated a Regional Stroke Centre with a
Stroke Prevention Clinic in 2001 (after 3 year demonstration phase)
• Community Stroke Prevention Clinics designated in Perth, Brockville, Belleville in 2003
• QHC designated a District Stroke Centre in 2004
• Funding from MOHLTC Hospitals Branch to hospitals
• Funding from MOHLTC Health Promotion Branch to promote health - this includes funding to HSFO for BP action plan and public awareness campaign.
System Change, Professional Education, Public Awareness
• Regional Stroke Centres• District Stroke Centres• Prevention Clinics• Links with Rehab, Community, LTC• Links with Health Promotion, Primary Care• Access to Best Practice; Build Stroke
Expertise / Professional Education
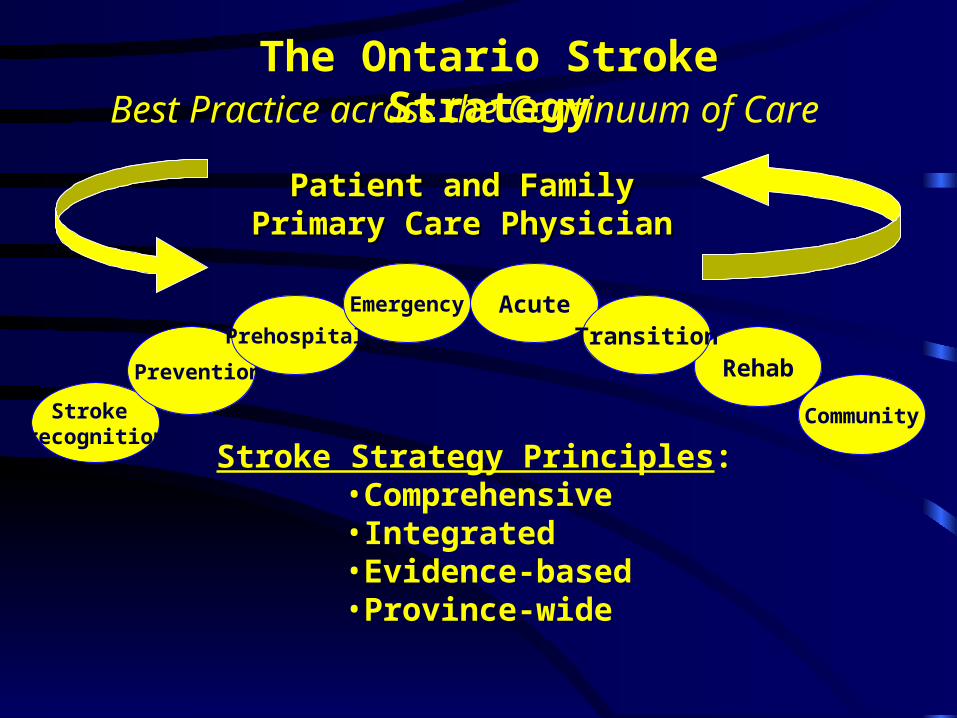
Patient and FamilyPatient and FamilyPrimary Care PhysicianPrimary Care Physician
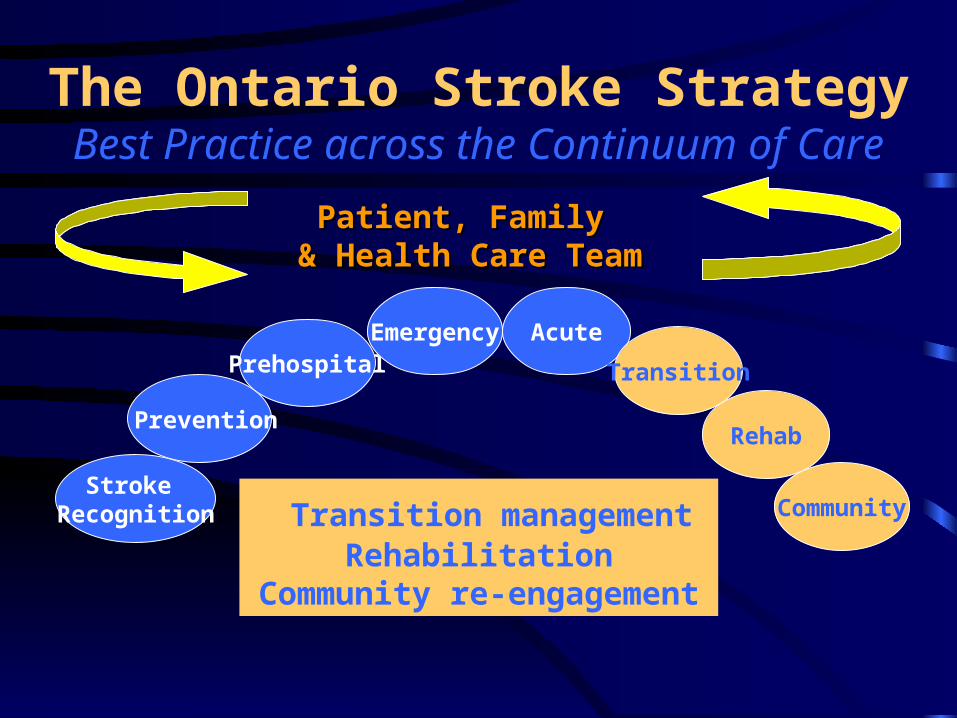
Best Practice across the Continuum of Care
The Ontario Stroke Strategy
Stroke Strategy Principles:•Comprehensive•Integrated•Evidence-based•Province-wide
Stroke recognition
Prevention
Prehospital
Emergency Acute
Rehab
Community
Transition
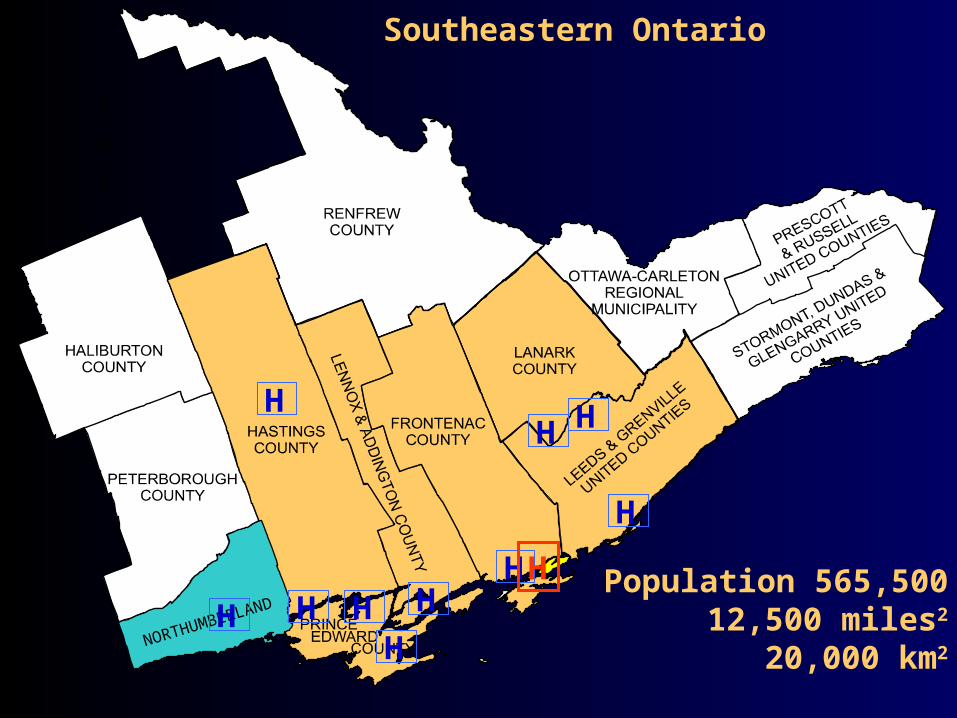
NORTHUMBERLAND
Southeastern Ontario
Population 565,50012,500 miles2
20,000 km2
H
H
HH
H
HHH
H
H
H
Regional Stroke Steering Committee
Full representation:
• across region
• across continuum of care
Subcommittees (prevention, acute, rehab, LTC)
Local area stroke workplans• Perth, Brockville, Kingston/Napanee, Quinte
Regional Stroke Team• Medical Director• Regional Stroke Program Manager• District Stroke Coordinator (Quinte)• Regional and Community Prevention Clinic Staff
(Kingston, Belleville, Brockville, Perth)• Regional Advanced Practice Nurse• Regional Education Coordinator• Administrative support• Enhanced KGH Acute Stroke Unit Team• Long-term Care and Community Specialist• Regional Tele-stroke Pilot Project Leader• ?? in 05/06 Regional Rehabilitation Coordinator
Stroke Best Practice Guidelines
19 Best Practice Guidelines Care Guides Protocols & Guidelines Assessment & Outcome
Measurement Tools Resource Listing CD ROM
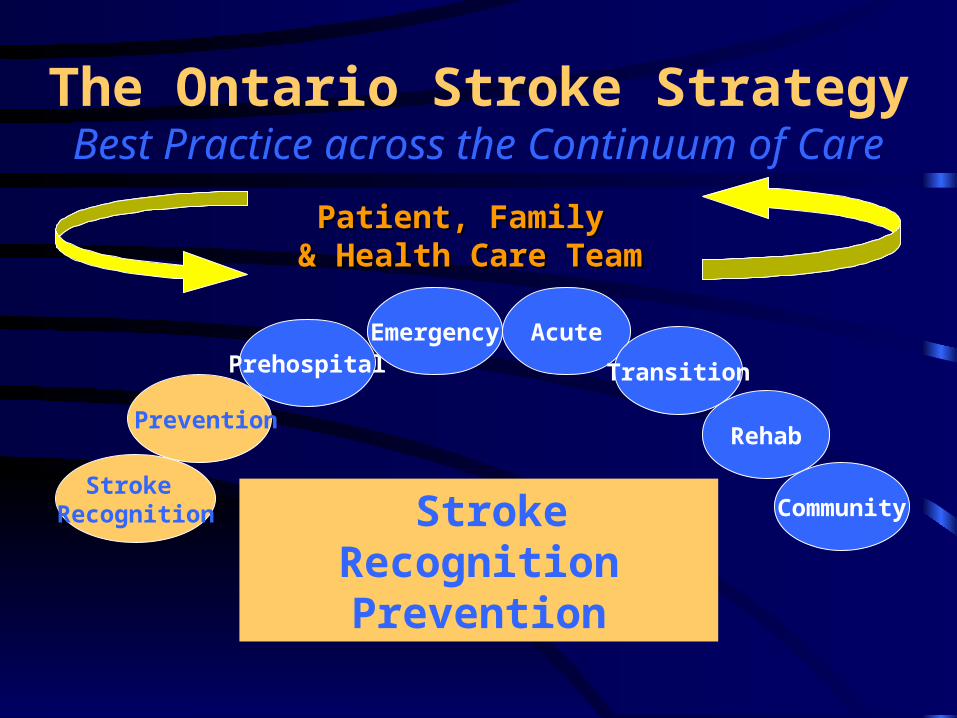
Patient, Family Patient, Family & Health Care Team& Health Care Team
Stroke Recognition
Prevention
PrehospitalEmergency Acute
Rehab
Community
Transition
The Ontario Stroke StrategyBest Practice across the Continuum of Care
Stroke RecognitionPrevention
Health Promotion & Stroke Prevention
• Health Promotion
• Risk Factor Management in Primary care (e.g. Blood pressure control)
• Stroke Prevention Clinics– Regional Stroke Centre, KGH – Community hospital prevention clinics in
Belleville, Brockville, Perth
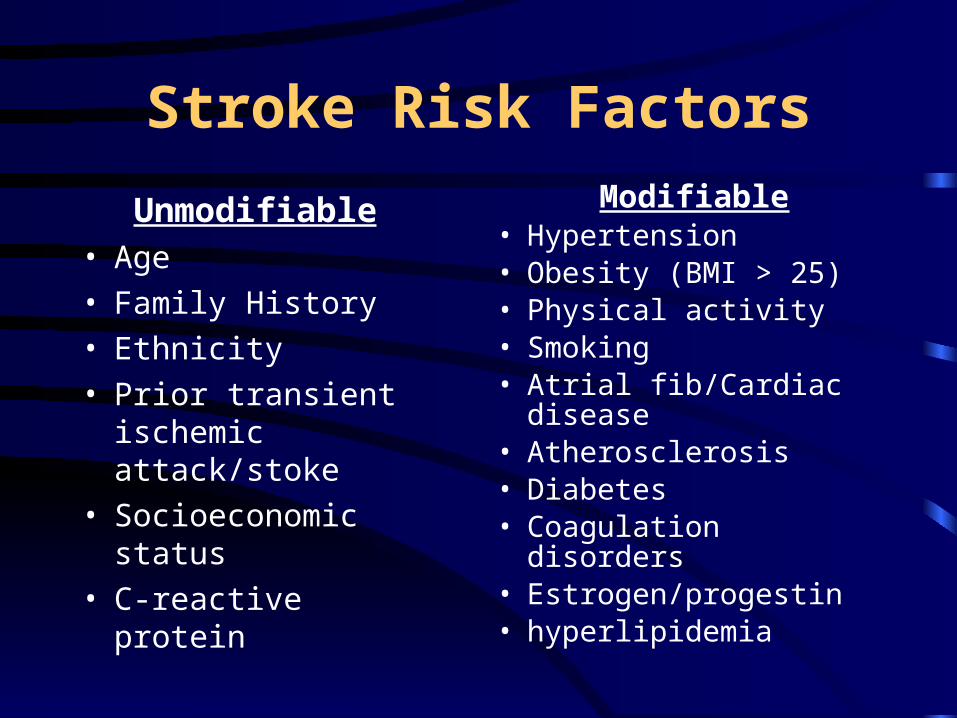
Stroke Risk Factors
Unmodifiable• Age
• Family History
• Ethnicity
• Prior transient ischemic attack/stoke
• Socioeconomic status
• C-reactive protein
Modifiable• Hypertension• Obesity (BMI > 25)• Physical activity• Smoking• Atrial fib/Cardiac disease• Atherosclerosis• Diabetes• Coagulation disorders• Estrogen/progestin• hyperlipidemia
1) What % of Canadians have high blood pressure?
2) Of these, what % are unaware of their BP?
3) Of those who are aware of their condition, what % have their BP treated and controlled ?
Stroke Prevention QUIZ
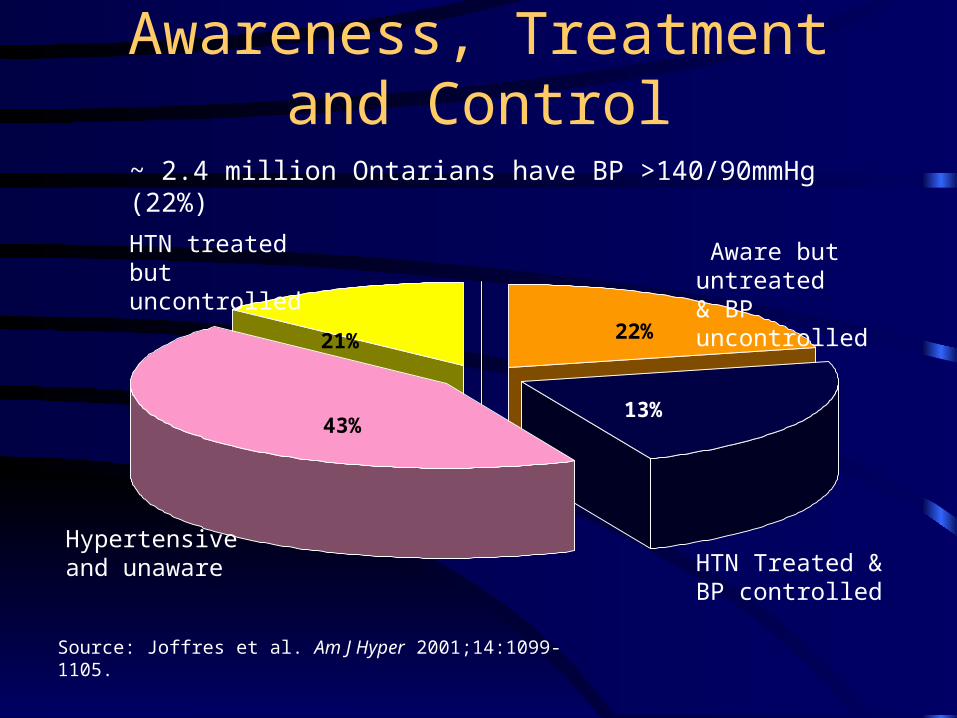
Awareness, Treatment and Control
22%
Source: Joffres et al. Am J Hyper 2001;14:1099-1105.
43%13%
21%
HTN treated but uncontrolled
Aware but untreated& BP uncontrolled
Hypertensiveand unaware HTN Treated & BP
controlled
~ 2.4 million Ontarians have BP >140/90mmHg (22%)
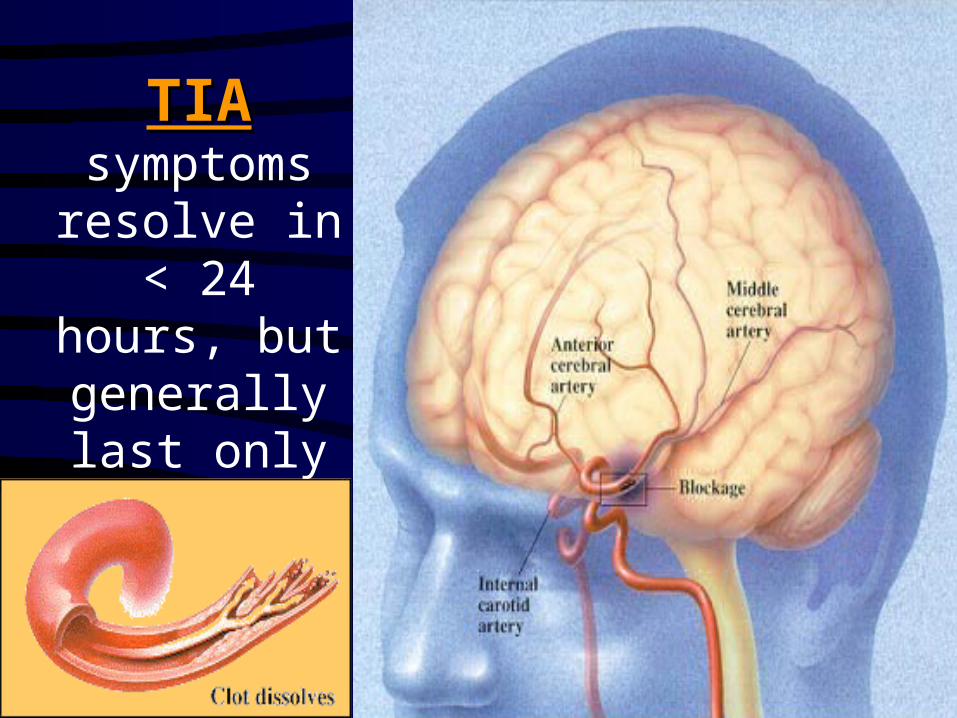
TIATIAsymptoms
resolve in < 24 hours,
but generally last only a few min
What percentage of those who have a TIA will have a
stroke within the next 48 hours?
a) .01%
b) .1%
c) 2.5%
d) 5%
What percentage of those who have a TIA will have a
stroke within the next 48 hours?
a) .01%
b) .1%
c) 2.5%
d) 5%
Why is there an Urgent Need for TIA Care?
• Short term risk of stroke – 10.5 % stroke risk within 90 days
• half < 48hrs • First stroke/TIA
40% have subsequent stroke within 5yrs• 15 - 30% stroke patients had previous TIA
Secondary Stroke Prevention
• Best Practice: Timely identification and management of those at highest risk of stroke
• Process: – TIA Collaborative Care Plans in ER’s– Stroke Prevention Clinics with Case Management by
Advanced Practice Nurse or RN– Full medical management – Education re lifestyle change (e.g. diet)– Timely revascularization
Medications for Secondary Stroke Prevention
• Antihypertensives• Antihyperlipidemic agents• Antiplatelets
– Aggrenox (ASA + ER Dipyridamole) or
– ASA and Plavix (Clopidogrel)• ACE Inhibitors• Anticoagulation, if indicated
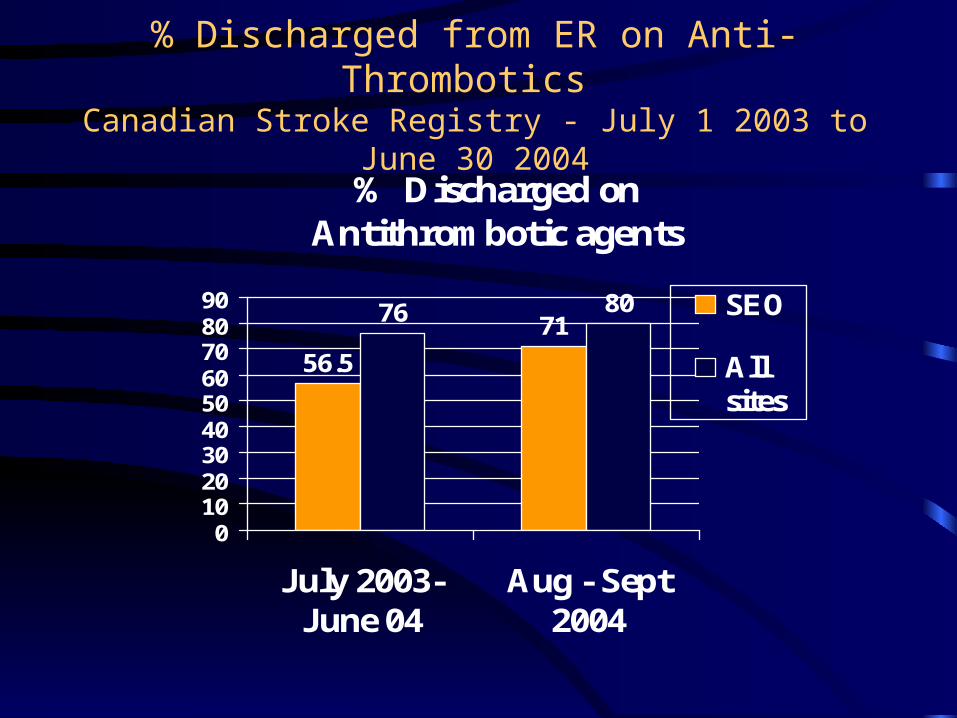
% Discharged from ER on Anti-Thrombotics Canadian Stroke Registry - July 1 2003 to June 30 2004
% Discharged on Antithrombotic agents
7176 80
56.5
0102030405060708090
July 2003-June 04
Aug - Sept2004
SEO
Allsites
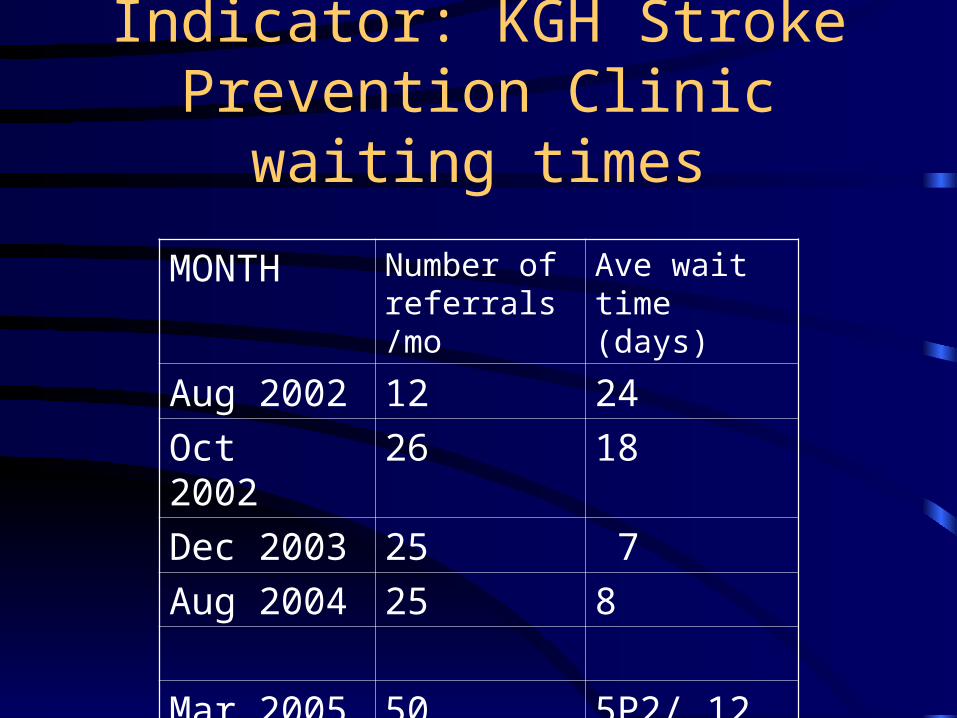
Indicator: KGH Stroke Prevention Clinic waiting times
MONTH Number of referrals/mo
Ave wait time (days)
Aug 2002 12 24
Oct 2002 26 18
Dec 2003 25 7
Aug 2004 25 8
Mar 2005 50 5P2/ 12 P3
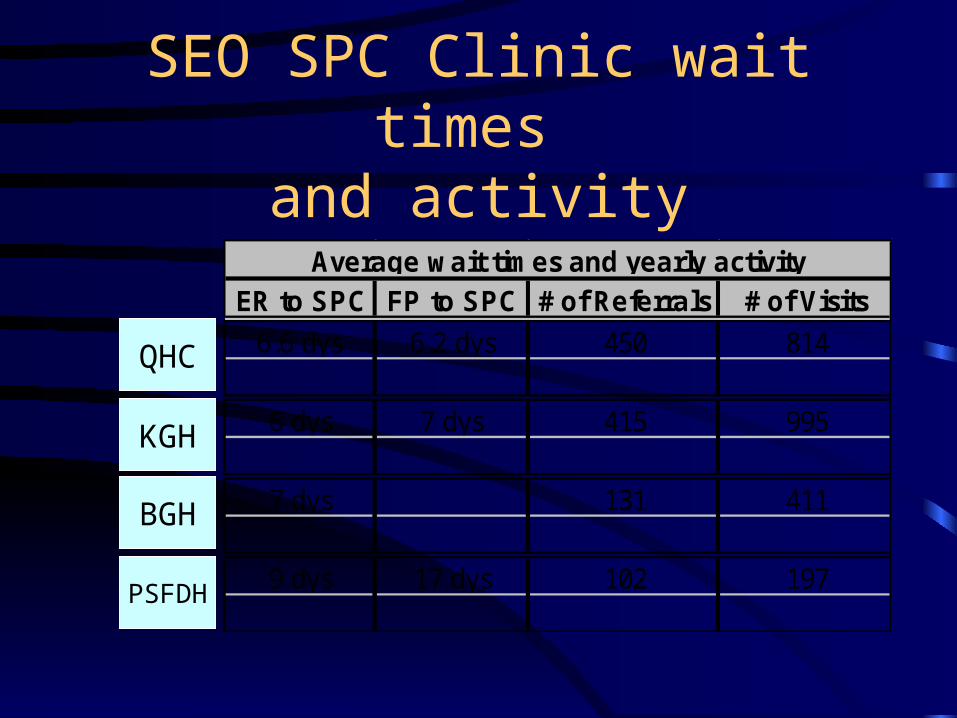
SEO SPC Clinic wait times and activity
ER to SPC FP to SPC # of Referrals # of Visits
6.6 dys 6.2 dys 450 814
6 dys 7 dys 415 995
7 dys 131 411
9 dys 17 dys 102 197
Average wait times and yearly activity
QHC
KGH
BGH
PSFDH
Patient, Family Patient, Family & Health Care Team& Health Care Team
Stroke Recognition
Prevention
Emergency Acute
Rehab
Community
Transition
The Ontario Stroke StrategyBest Practice across the Continuum of Care
EMS
Pre-hospital
Regional Acute Stroke Protocol Southeastern Ontario
For those with Signs and Symptoms of Stroke: A Coordinated system response
Bypass Protocol Implemented July 1999
Access to thrombolytics within a 3-hour time window
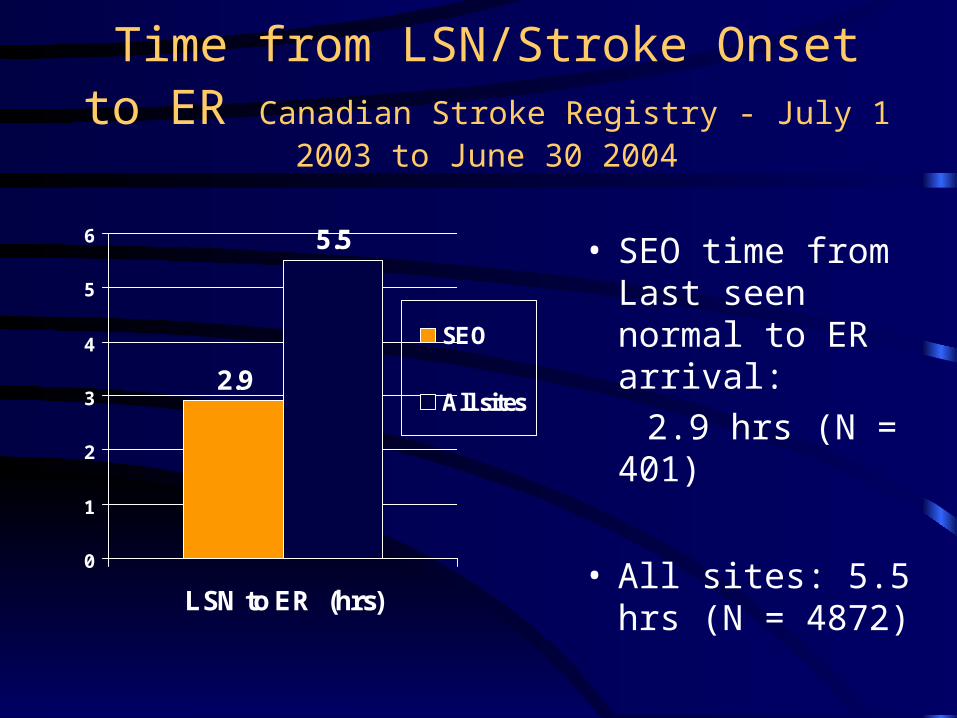
Time from LSN/Stroke Onset to ER Canadian Stroke Registry - July 1 2003 to June 30 2004
5.5
2.9
0
1
2
3
4
5
6
LSN to ER (hrs)
SEO
All sites
• SEO time from Last seen normal to ER arrival:
2.9 hrs (N = 401)
• All sites: 5.5 hrs (N = 4872)
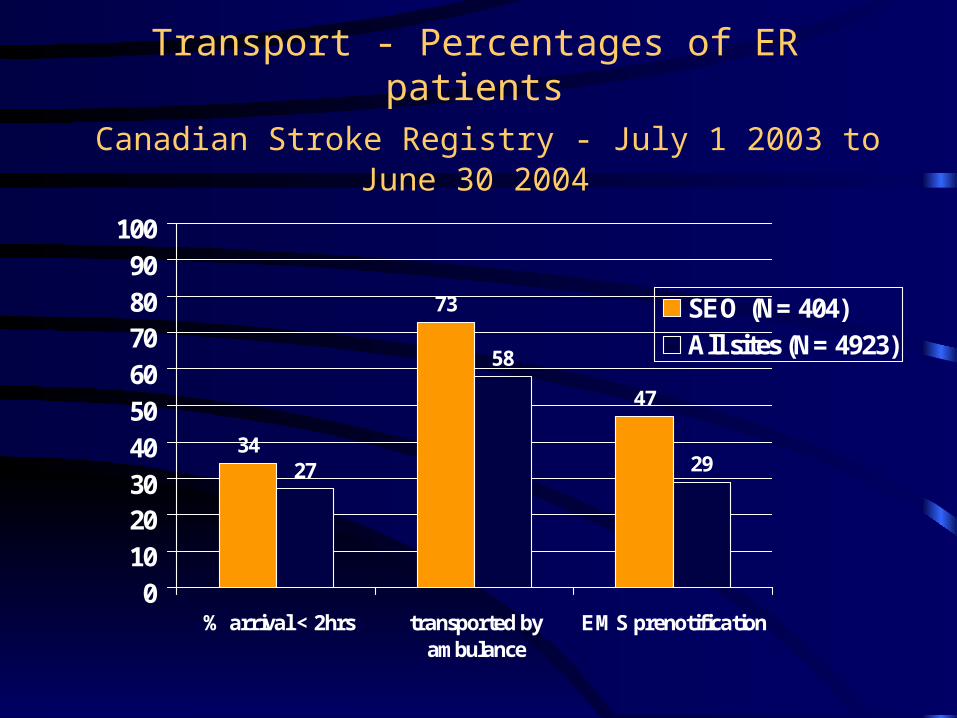
Transport - Percentages of ER patients Canadian Stroke Registry - July 1 2003 to June 30 2004
34
73
27
58
29
47
0102030405060708090
100
% arrival < 2hrs transported byambulance
EMS prenotification
SEO (N= 404)All sites (N= 4923)
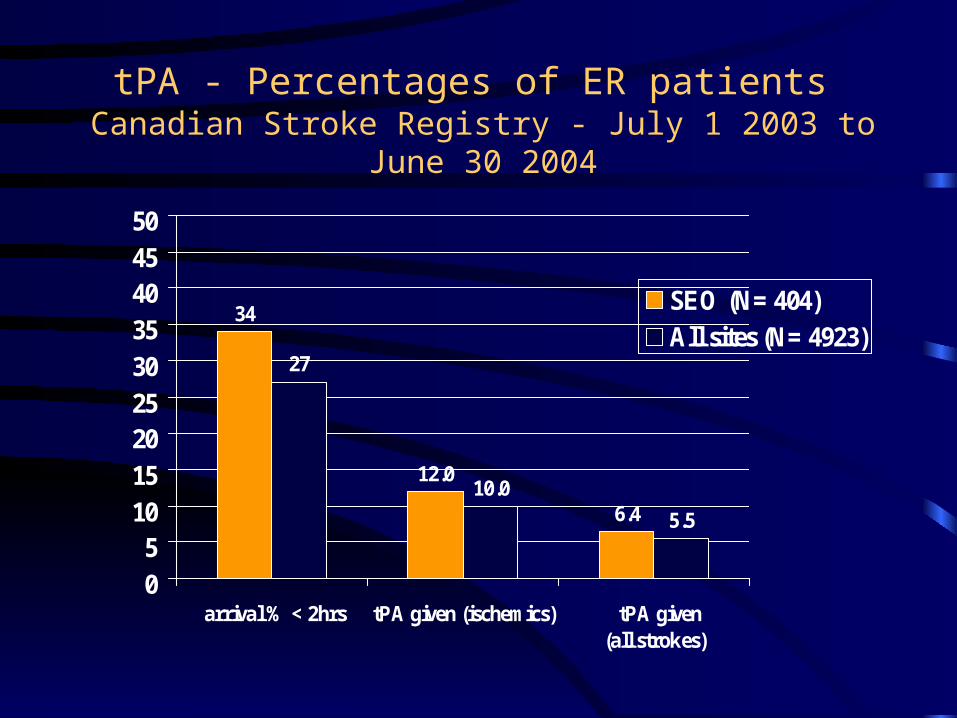
tPA - Percentages of ER patients Canadian Stroke Registry - July 1 2003 to June 30 2004
34
12.0
27
10.0
5.56.4
05
101520253035404550
arrival % < 2hrs tPA given (ischemics) tPA given (all strokes)
SEO (N= 404)All sites (N= 4923)
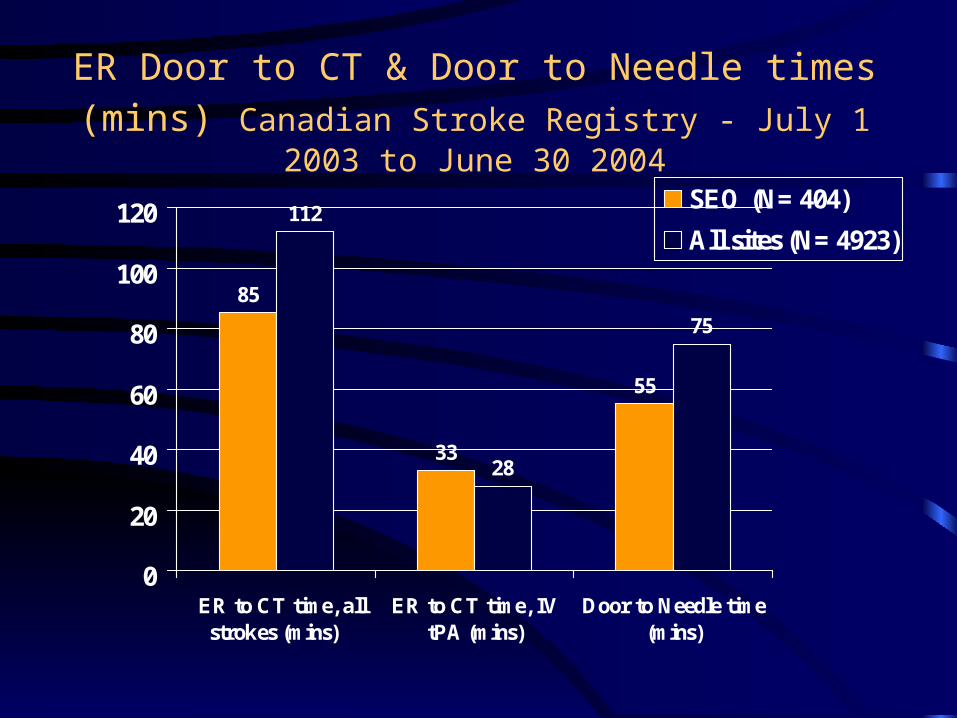
ER Door to CT & Door to Needle times (mins) Canadian Stroke Registry - July 1 2003 to June 30 2004
85
33
112
28
75
55
0
20
40
60
80
100
120
ER to CT time, allstrokes (mins)
ER to CT time, IVtPA (mins)
Door to Needle time(mins)
SEO (N= 404)
All sites (N= 4923)
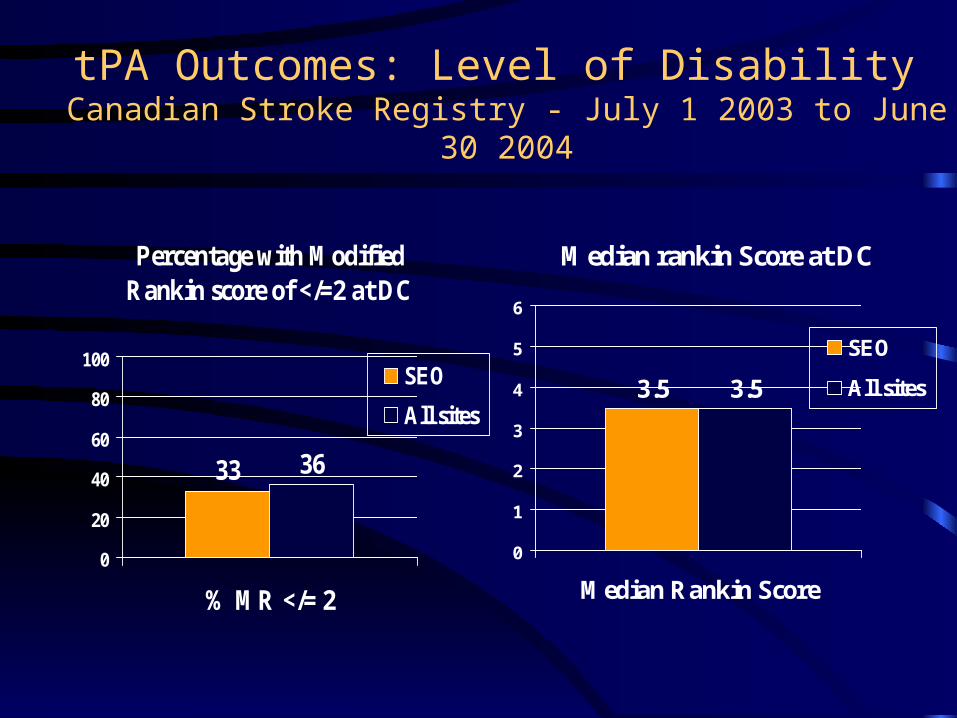
tPA Outcomes: Level of Disability Canadian Stroke Registry - July 1 2003 to June 30 2004
Percentage with Modified Rankin score of </=2 at DC
3633
0
20
40
60
80
100
% MR </= 2
SEO
All sites
Median rankin Score at DC
3.53.5
0
1
2
3
4
5
6
Median Rankin Score
SEO
All sites
Patient, Family Patient, Family & Health Care Team& Health Care Team
Stroke Recognition
Prevention
PrehospitalEmergency Acute
Rehab
Community
Transition
The Ontario Stroke StrategyBest Practice across the Continuum of Care
Acute
Inpatient Acute Stroke Care
• Regional Patient Flow
• Inter-disciplinary teams
• Organised stroke units
• Evidence-Based Stroke Care Pathways
• Regional Acute Stroke APN and stroke case manager
Good Nursing Care Improves Survival & Outcome
• Blood pressure
In ER, do not treat BP
(SBP 220, DBP 140)
• Fever >37.5• Blood glucose > 8.5
– Rx aggressively
• Hypoxia
• DVT / PE– DVT 20-70%– PE 10% mortality– Heparin prophylaxis DVT
50%
• UTI/Incontinence UTI ~40% Urinary Incontinence 32%-
79%
• Dysphagia • Depression
Patient, Family Patient, Family & Health Care Team& Health Care Team
Stroke Recognition
Prevention
PrehospitalEmergency Acute
Rehab
Community
Transition
The Ontario Stroke StrategyBest Practice across the Continuum of Care
Transition managementRehabilitationCommunity re-engagement
Transition Management
• Transition protocols• Documented standardized team
approach– include client centred goals
• Plan with primary provider• Ongoing access to rehabilitation
and community services
Transition
Rehabilitation Management
• Evaluate rehab potential of each client– team assessment and planning
• Access to appropriate rehab intensity across the continuum
• Assess and address caregiver burden
• Timely discharge from rehab units
Rehabilitation

Community Re-engagement
• Family centred care planning & follow-up• Develop stroke expertise in community
and LTC• Support caregivers
– community programs– respite care– Education
• Social support networks
Community
Rehabilitation: Key Points
• Start early
• Team approach– Expert assessment
• Patient/family centered
• Goal Oriented
• Communication
> 80% benefit from rehab
Rehabilitation: Start Early
• Acute Care– Early rehab in acute care prevents
• Skin breakdown• Falls• Pain/spasticity/contractures• Injuries
• Inpatient Rehab– Early admission to rehab improves
functional outcomes (level 2 evidence)
Rehabilitation Assessment
EXPERT REHAB ASSESSMENT
Who Should Receive Inpatient Rehab?
Impairment type & severity Moderate to severe
Ability to learn
Physical endurance (3hr/day)
• 6 Ontario Stroke Rehab Pilot projects approved by MOHLTC May 2002
• SEO pilot: – transition from rehab unit to own home– Stroke Care Diary
Stroke Rehabilitation Pilots
The Discharge Link Project (DLP)
GoalTo investigate best practice related to stroke client transition from inpatient rehabilitation to the community by:
• enhancing therapy• augmenting provider
communication
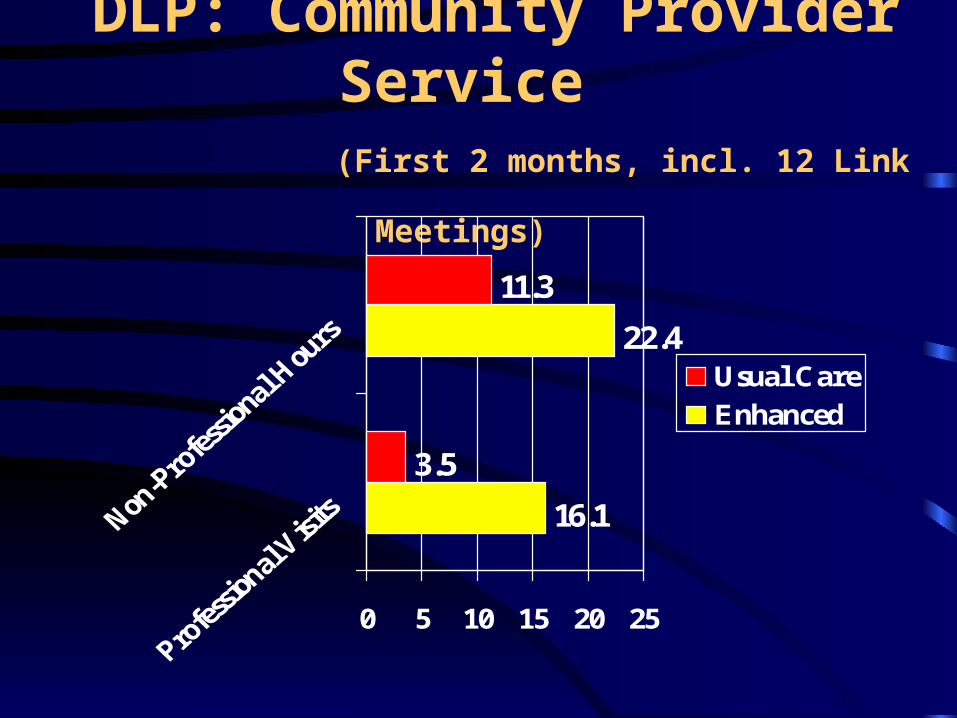
DLP: Community Provider Service (First 2 months, incl. 12 Link Meetings)
16.1
22.4
3.5
11.3
0 5 10 15 20 25
Usual CareEnhanced
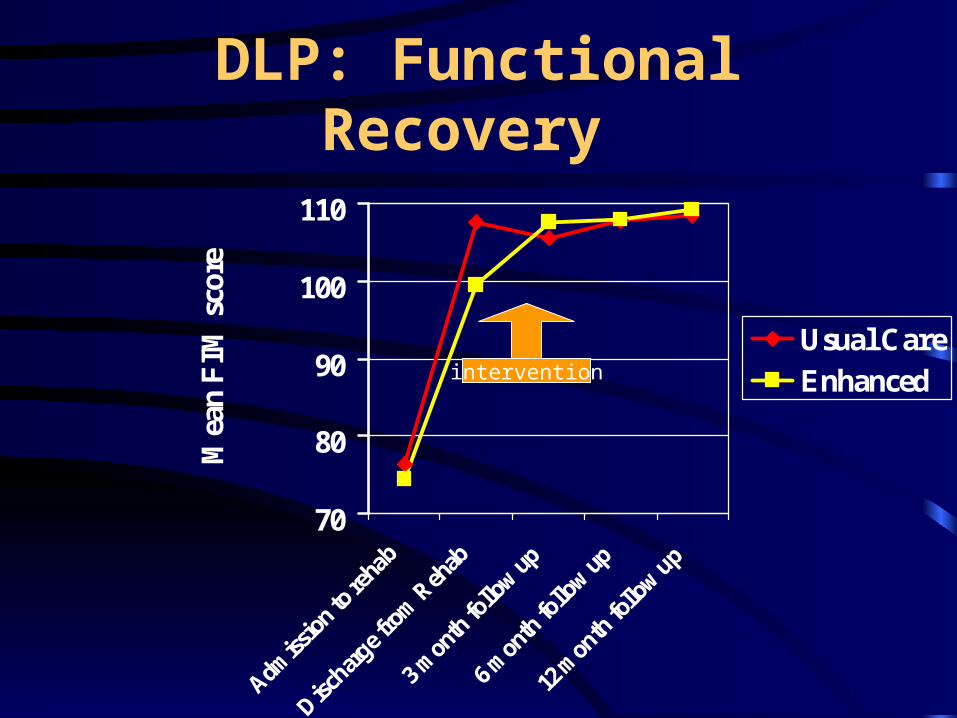
DLP: Functional Recovery
70
80
90
100
110
Admiss
ion t
o reh
ab
Discha
rge f
rom Reh
ab
3 mon
th fo
llow up
6 mon
th fo
llow up
12 m
onth fo
llow up
Mea
n FIM
sco
re
Usual CareEnhancedintervention
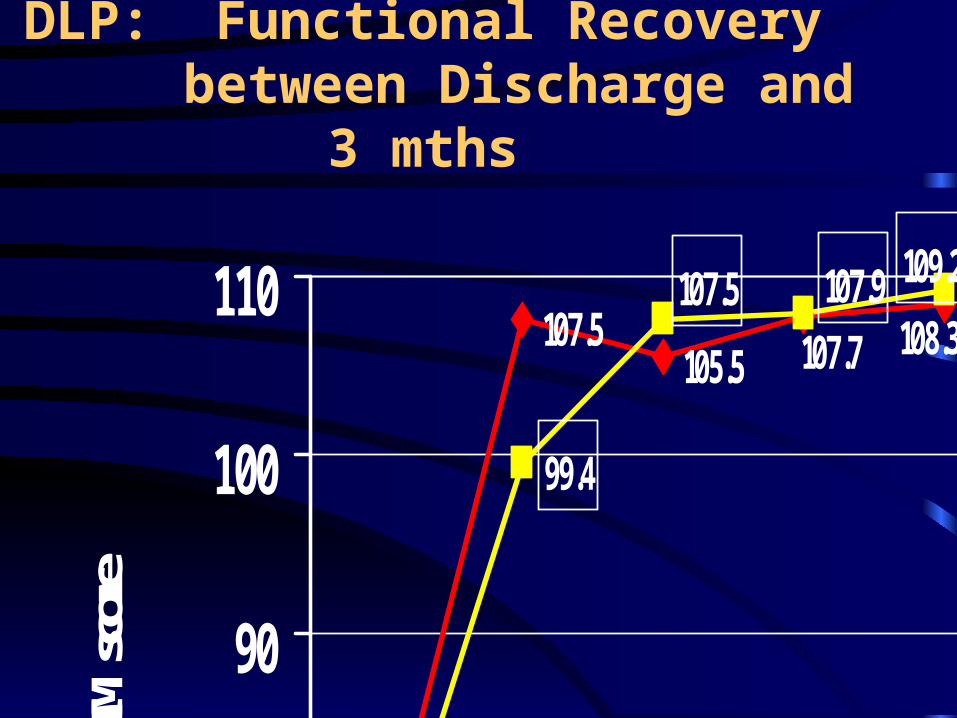
DLP: Functional Recoverybetween Discharge and 3 mths
76.3
107.5105.5
74.4
99.4
108.3107.7
109.2107.9107.5
70
80
90
100
110
Mean
FIM
score N
E
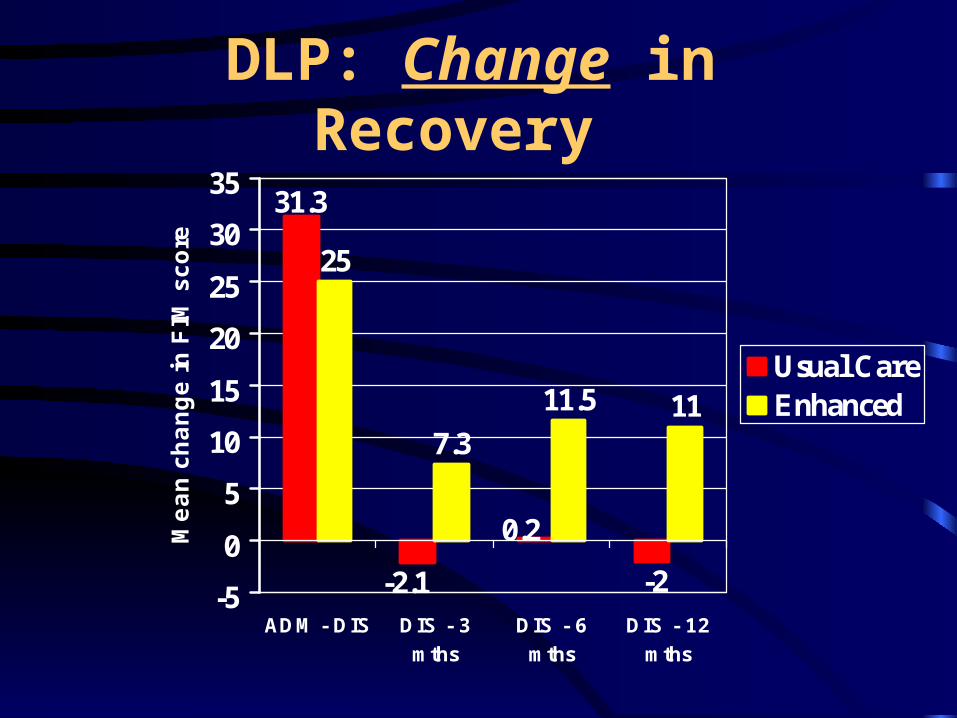
DLP: Change in Recovery
25
7.3
11.5 11
31.3
-2.1
0.2
-2-5
0
5
10
15
20
25
30
35
ADM - DIS DIS - 3mths
DIS - 6mths
DIS - 12mths
Mean c
hange in
FIM
sco
re
Usual CareEnhanced
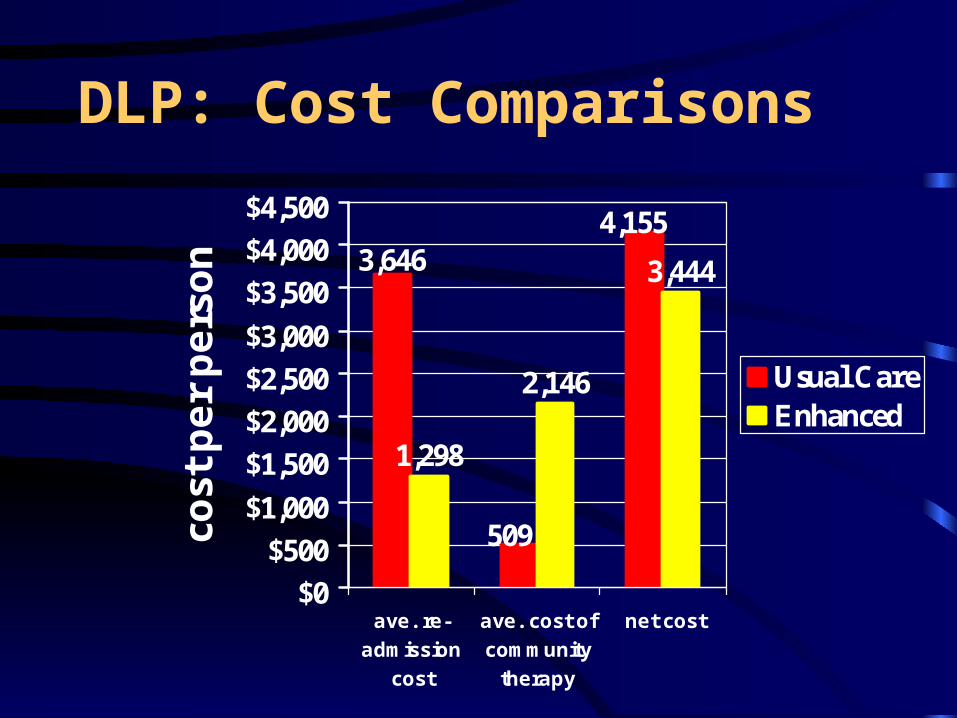
DLP: Cost Comparisons
1,298
2,146
3,4443,646
509
4,155
$0
$500
$1,000
$1,500
$2,000
$2,500
$3,000
$3,500
$4,000
$4,500
ave. re-admission
cost
ave. cost ofcommunity
therapy
net cost
cost
per pers
on
Usual CareEnhanced
““A cycle of discontinuity”A cycle of discontinuity”
“You get so used to working within a system that you … you forget that there might be something better out there...”
“I finally get to do real OT!”
Key informant interviews:Voices of Providers….
Key informant interviews:Voices of clients….
“I am totally overwhelmed”
““Horrific”Horrific”““Hell on earth”Hell on earth”“It was hard. It was tough”
“if spouses become therapists… it really degrades and demises the personal
relationship.”
“What do you do?”
Long Term and Community Care
•Education
•Communication: Need for better information at transition points
•Rehabilitation expertise
•Support Networks: community programs
Community/Long Term Care
• Tips and Tools for Everyday Living: A resource for Stroke Caregivers
• LTC Resource teams work with LTC Specialists
• Community Care Stroke Service Guidelines
• Educational opportunities
• Communication Tool for Acute to LTC: “Transition Information Plan”
• Building LTC stroke network via “Linkage Luncheons”

Professional education
HSFO Prof Ed Web site
www.heartandstroke.ca/profed
The Road AheadStroke Best Practice GuidelinesImplementation across Ontario