Embed Size (px)
Citation preview
lable at ScienceDirect
Geriatric Nursing 35 (2014) S11eS16
Contents lists avai
Geriatric Nursing
journal homepage: www.gnjournal .com
Feature Article
The nursing assistants’ communication style and the behavioralsymptoms of dementia in Korean-American nursing home residents
Haesook Kim, PhD, RN, GNP-BC a,*, Diana Lynn Woods, PhD, RN, GNP-BC b,Janet C. Mentes, PhD, RN, ACNP-BC a, Jennifer L. Martin, PhD c, Ailee Moon, PhD d,Linda R. Phillips, PhD, RN, FAAN a
a School of Nursing, University of California, Los Angeles, USAb School of Nursing, Azusa Pacific University, USAcDavid Geffen School of Medicine, University of California, Los Angeles, USAdDepartment of Social Welfare, School of Public Affairs, University of California, Los Angeles, USA
Keywords:Communication styleBehavioral symptoms of dementiaKorean American older adults
* Corresponding author. Tel.: þ1 510 648 5358.E-mail address: [email protected] (H. Kim).
0197-4572/$ e see front matter � 2014 Mosby, Inc. Ahttp://dx.doi.org/10.1016/j.gerinurse.2014.02.016
a b s t r a c t
Few studies examined the association between communication style and behavioral symptoms of de-mentia (BSD). The communication style of Nursing Assistants’ (NAs), whose ethnic background is differentfrom the residents, may contribute to BSD. The purpose of this study was to explore the relationshipbetween non-KoreanNAs’ communication style and BSD in Korean-American (KA) nursing home residentswith dementia. Twenty eight NAs and 20 KA residents were recruited from an ethno-specific nursinghome. Research assistants observed and recorded NAs’ communication style and residents’ behaviorsimultaneously during routine care for 3 days. This study shows a trend that NAs’ dementia and culturallyappropriate communication style influenced the decreased behavioral symptoms. This finding suggeststhe need for training for NAs in dementia and culturally appropriate communication.
� 2014 Mosby, Inc. All rights reserved.
Introduction may experience communication challenges such as misinterpreta-
The population of older adults living in the United States (US) isbecoming more racially and ethnically diverse. The number ofethnic minorities over age 65 years is projected to increase up to28% of all older adults residing in the US by 2030.1 Consistently, theracial composition of ethnic minority nursing home (NH) residentsis rapidly growing. From 2000 to 2007, Hispanic and Asian NHresidents increased 43.3% and 44.7%, respectively.2 Although theprevalence of dementia in ethnic minority NH residents in theUnited States (US) is unknown, this estimation coupled with theincrease in the number of older adults with dementia,3 will likelylead to a corresponding increase in the number of ethnic minorityNH residents with dementia. Among the ethnic minorities, 1.7million Korean Americans (KA) represent the fifth largest Asiangroup, with a population increase of 42% from 2000 to 2010.4
Although the number of KA-NH residents is unknown, it willlikely increase with KA population growth.
The KA-NH residents may have different cultural and languagebackground from nursing assistants (NAs), who frequently providedirect care activities, such as bathing and dressing. If the NAs use adifferent language with different cultural experiences, KA residents
ll rights reserved.
tion of the verbal and non-verbal expressions of NAs.5,6 The needfor culturally familiar communication may be pronounced for KA-NH residents who have lower levels of English proficiency andtend to retain their language and culture.7,8 For example, when NAsinstruct in Korean to KA residents, KA residents expect culturallyappropriate linguistic and behavioral expressions.9 In Korean, thereare two types of words or phrases with the same meaning whichare used differently based on age, which is incorporated in a deep-seated respect for older adults.10 In other words, the Korean lan-guage is spoken in a casual manner (i.e., Yesamal) or in a morerespectful manner (i.e., Jondaemal). When NAs speak to KA resi-dents, the residents expect to hear the polite Jondaemal form(words or phrases), otherwise the KA residents may interpret theNAs communication style as disrespectful and impolite. The KAresidents with dementia may experience further frustration due tothe language and cultural barriers, in addition to their cognitiveimpairment, that in turn, might elicit or increase behavioralsymptoms of dementia (BSDs).11 The BSDs become a concern forcaregivers, and may result in higher rates of staff turnover andmedication overuse.12,13
Despite the increasing attention to culturally and linguisticallyappropriate care,14,15 there is a dearth of studies that have exploredculturally appropriate verbal and non-verbal expressions and theresulting influences on BSDs. Only a single case study16 was available

H. Kim et al. / Geriatric Nursing 35 (2014) S11eS16S12
in the literature to support the influence of native language onbehavioral symptoms of an immigrant residentwith dementia. Sincelanguage is only one aspect of culturally familiar communication,further studies are needed to examine other aspects of communi-cation (i.e., verbal and non-verbal style, communication traditions,and generational language rules) in ethnically diverse residents.
Considering that ethnic minority NH residents prefer to receivecare from those who have familiar cultural background and/or areable to use residents’ native language,17,18 it becomes critical tounderstand appropriate communication style and its associationwith BSDs for the residents. The purpose of this study was toexplore and describe the association between non-Korean NAs’communication style and behavioral symptoms in KA-NH residentswith dementia. The findings may help family caregivers and healthprofessionals to better understand BSDs within the context of socialinteractions in an ethnically diverse community. It will ultimatelyimprove quality of life of KA-NH residents with dementia.
Methods
Sample and setting
After approval from Institutional Review Board, the study wasconducted in a single NH, where more than 90% residents were KAolder adults. This study used a descriptive longitudinal design.
ResidentsA total of 20 KA-NH residents participated in this study. Inclu-
sion criteria for residents were 1) Korean-American immigrants; 2)�65 years; 3) a diagnosis of dementia according to their medicalrecord and score less than 24 on the Korean version of the Mini-Mental State Examination (K-MMSE)19,20; 4) resident in the NHfor at least 2 months; 5) anticipated residency in the NH for theduration of the study; and 6) no dose adjustment of the followingmedications for at least 1 month: anti-psychotics, anti-depressants,anti-anxiety, neuroleptics or sedative-hypnotics. The principalinvestigator (PI) obtained written informed consent from thefamily members of 20 among 54 potential participants (35%). Seven(13%) refused to participate and 27 (50%) could not be reached.
Nursing assistantsA total of 28 NAs were observed in the study. Among 32 po-
tential participants, the PI recruited 28 individuals (87.5%). Four(12.5%) NAs declined participation. Inclusion criteria for NAs were:1) non-Korean, 2) non-fluent Korean speaker, and 3) anticipatedworking in the NH through the duration of the study.
Procedures
The PI reviewed the residents’ medical records and adminis-tered K-MMSE. NAs were individually interviewed to obtain de-mographic information.
Direct observationThe modified Agitated Behavior Rating Scale (mABRS)21,22 and
social interaction coding schemas (Dementia Social Interaction,Culture Social Interaction)23 were installed on the observationalcomputer software, the Pocket Observer 3.0 (Noldus) in hand-helddevices (Panasonic�; Japan). The maximum number of observationper resident could be six over three days (2/day � 3days ¼ 6).Trained RAs observed NAs/resident dyad interactions duringmorning care between 8 am and 10 am (e.g., dressing, bathing,combing, grooming, oral care, and transferring out of bed) and af-ternoon care (e.g., undressing, incontinence care, and transferringto bed) between 3 pm and 5 pm. Three RAs independently observed
and recorded NAs’ communication style and residents’ BSDs, asunobtrusively as possible. They simultaneously started codingwhen an NA entered a resident’s room to provide care andcontinued whenever the target behaviors (i.e., communication,BSDs) occurred. While one RA recorded the NA’s dementiacommunication style using the DSI coding schema, the other RArecorded the NA’s cultural communication style using the CSIcoding schema. The third RA observed and recorded the resident’sBSDs using the mABRS. The two RAs, who observed the NAs’communication style, stopped observation when the NA left aresident after completing her/his tasks. The third RA continued toobserve and record BSDs for 1 h after the NA left the resident’sroom. Data were downloaded from the hand-held device to TheObserver 5.0 (Noldus) and then transferred to Microsoft Excel tomanage the dataset. The cleaned dataset was exported to SPSS 20.0and/or STATA 12.0 for data analysis.
Reliability of observationsThe RAs had an intensive 8 h training session in standard pro-
tocols for using the hand-held device, the coding schemas, and themABRS until they demonstrated proficiency. RAs were trained for6 h away from the NH, using videotaped behavior, followed by a 2 hpractice observation session at the NH. Definitions for BSDs andcommunication style codes were clarified using examples. If therewere coding differences, they were resolved by group discussionunder the direction of the PI. To ensure the inter-rater reliability ofbehavioral observations, 2 RAs simultaneously recorded commu-nication style (DSI, CSI) for the same NA. The other 2 RAs simul-taneously recorded BSDs for the same resident. The inter-raterreliability between 2 RAs reached 0.70 or higher, using Cohen’skappa24,25 for both communication style and BSDs.
Measures
Demographic information about residents and NAsDemographic data for residents were abstracted from each resi-
dent’s medical records including medications, co-morbid medicalconditions, age, gender, and marital status. The K-MMSEwas used toassess cognitive status. Demographic information was obtaineddirectly from NAs including age, gender, race/ethnicity, primarylanguage, education, and length of time working in the facility.
Residents’ BSDsThe Modified Agitated Behavior Rating Scale (mABRS)21,22 was
used to measure frequency and intensity of BSDs using directobservation. The mABRS includes 6 six categories of behavior:vocalization, restlessness, escaping restraints, searching/wander-ing, tapping/banging, and pacing/walking. The ratings are coded ona four-point Likert-type scale for each point, ranging from notpresent (0) to high intensity (3). For example, intensity ratings forrestlessness are: 0 ¼ not present; 1 ¼ low intensity, rhythmicpurposeless movements of hands; 2 ¼ medium or moderate in-tensity, repetitive manipulation of an object, facial distress;3 ¼ high intensity, large amplitude rubbing or picking. The percentagreement for the presence or absence of BSDs ranged from 85.5%to 96.8% for frequency with kappa values ranging from 0.71 to 0.93and from 83 to 89.5% for intensity with kappa values ranging from0.60 to 0.64.21
NAs’ communication styleThe Dementia Social Interaction (DSI) coding schema23 con-
sists of 27 behavioral codes, including 12 dementia appropriateand 15 inappropriate communication styles (Table 1). Inter-raterreliability of the DSI coding scheme varied from 0.73 to 0.83 for
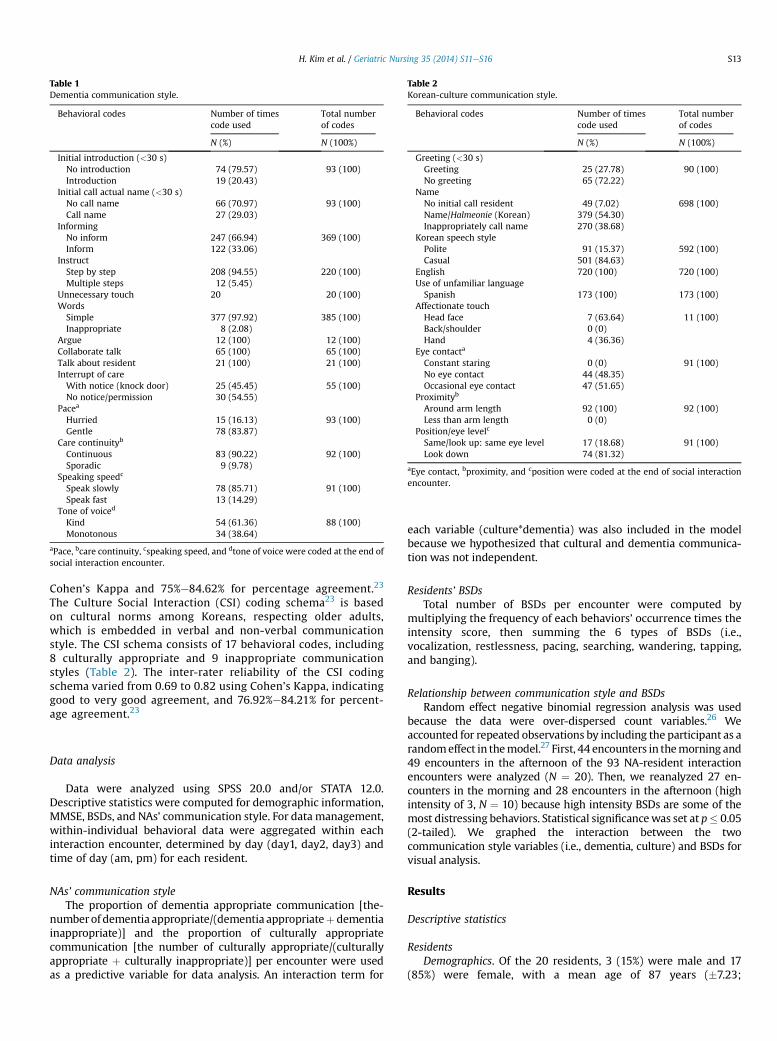
Table 2Korean-culture communication style.
Behavioral codes Number of timescode used
Total numberof codes
N (%) N (100%)
Greeting (<30 s)Greeting 25 (27.78) 90 (100)No greeting 65 (72.22)
NameNo initial call resident 49 (7.02) 698 (100)Name/Halmeonie (Korean) 379 (54.30)Inappropriately call name 270 (38.68)
Korean speech stylePolite 91 (15.37) 592 (100)Casual 501 (84.63)
English 720 (100) 720 (100)Use of unfamiliar languageSpanish 173 (100) 173 (100)
Affectionate touchHead face 7 (63.64) 11 (100)Back/shoulder 0 (0)Hand 4 (36.36)
Eye contacta
Constant staring 0 (0) 91 (100)No eye contact 44 (48.35)Occasional eye contact 47 (51.65)
Proximityb
Around arm length 92 (100) 92 (100)Less than arm length 0 (0)
Position/eye levelc
Same/look up: same eye level 17 (18.68) 91 (100)Look down 74 (81.32)
aEye contact, bproximity, and cposition were coded at the end of social interactionencounter.
Table 1Dementia communication style.
Behavioral codes Number of timescode used
Total numberof codes
N (%) N (100%)
Initial introduction (<30 s)No introduction 74 (79.57) 93 (100)Introduction 19 (20.43)
Initial call actual name (<30 s)No call name 66 (70.97) 93 (100)Call name 27 (29.03)
InformingNo inform 247 (66.94) 369 (100)Inform 122 (33.06)
InstructStep by step 208 (94.55) 220 (100)Multiple steps 12 (5.45)
Unnecessary touch 20 20 (100)WordsSimple 377 (97.92) 385 (100)Inappropriate 8 (2.08)
Argue 12 (100) 12 (100)Collaborate talk 65 (100) 65 (100)Talk about resident 21 (100) 21 (100)Interrupt of careWith notice (knock door) 25 (45.45) 55 (100)No notice/permission 30 (54.55)
Pacea
Hurried 15 (16.13) 93 (100)Gentle 78 (83.87)
Care continuityb
Continuous 83 (90.22) 92 (100)Sporadic 9 (9.78)
Speaking speedc
Speak slowly 78 (85.71) 91 (100)Speak fast 13 (14.29)
Tone of voiced
Kind 54 (61.36) 88 (100)Monotonous 34 (38.64)
aPace, bcare continuity, cspeaking speed, and dtone of voice were coded at the end ofsocial interaction encounter.
H. Kim et al. / Geriatric Nursing 35 (2014) S11eS16 S13
Cohen’s Kappa and 75%e84.62% for percentage agreement.23
The Culture Social Interaction (CSI) coding schema23 is basedon cultural norms among Koreans, respecting older adults,which is embedded in verbal and non-verbal communicationstyle. The CSI schema consists of 17 behavioral codes, including8 culturally appropriate and 9 inappropriate communicationstyles (Table 2). The inter-rater reliability of the CSI codingschema varied from 0.69 to 0.82 using Cohen’s Kappa, indicatinggood to very good agreement, and 76.92%e84.21% for percent-age agreement.23
Data analysis
Data were analyzed using SPSS 20.0 and/or STATA 12.0.Descriptive statistics were computed for demographic information,MMSE, BSDs, and NAs’ communication style. For data management,within-individual behavioral data were aggregated within eachinteraction encounter, determined by day (day1, day2, day3) andtime of day (am, pm) for each resident.
NAs’ communication styleThe proportion of dementia appropriate communication [the-
numberof dementia appropriate/(dementia appropriateþ dementiainappropriate)] and the proportion of culturally appropriatecommunication [the number of culturally appropriate/(culturallyappropriate þ culturally inappropriate)] per encounter were usedas a predictive variable for data analysis. An interaction term for
each variable (culture*dementia) was also included in the modelbecause we hypothesized that cultural and dementia communica-tion was not independent.
Residents’ BSDsTotal number of BSDs per encounter were computed by
multiplying the frequency of each behaviors’ occurrence times theintensity score, then summing the 6 types of BSDs (i.e.,vocalization, restlessness, pacing, searching, wandering, tapping,and banging).
Relationship between communication style and BSDsRandom effect negative binomial regression analysis was used
because the data were over-dispersed count variables.26 Weaccounted for repeated observations by including the participant as arandomeffect in themodel.27 First, 44 encounters in themorning and49 encounters in the afternoon of the 93 NA-resident interactionencounters were analyzed (N ¼ 20). Then, we reanalyzed 27 en-counters in the morning and 28 encounters in the afternoon (highintensity of 3, N ¼ 10) because high intensity BSDs are some of themost distressing behaviors. Statistical significancewas set at p� 0.05(2-tailed). We graphed the interaction between the twocommunication style variables (i.e., dementia, culture) and BSDs forvisual analysis.
Results
Descriptive statistics
ResidentsDemographics. Of the 20 residents, 3 (15%) were male and 17
(85%) were female, with a mean age of 87 years (�7.23;
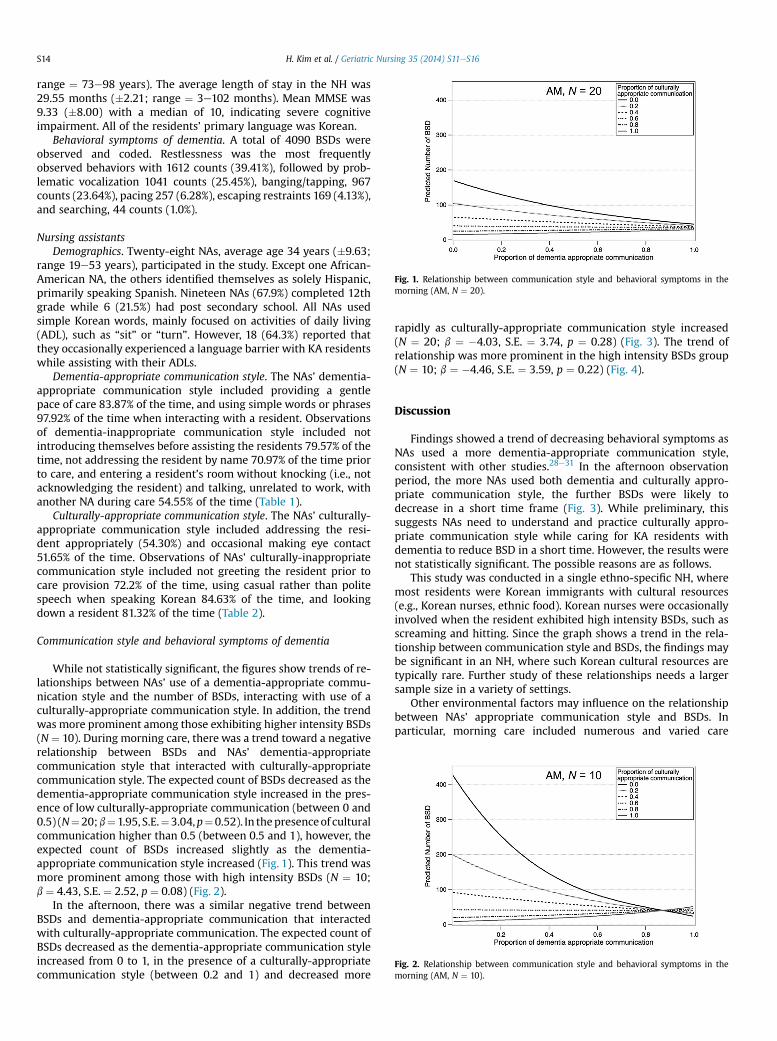
Fig. 1. Relationship between communication style and behavioral symptoms in themorning (AM, N ¼ 20).
Fig. 2. Relationship between communication style and behavioral symptoms in themorning (AM, N ¼ 10).
H. Kim et al. / Geriatric Nursing 35 (2014) S11eS16S14
range ¼ 73e98 years). The average length of stay in the NH was29.55 months (�2.21; range ¼ 3e102 months). Mean MMSE was9.33 (�8.00) with a median of 10, indicating severe cognitiveimpairment. All of the residents’ primary language was Korean.
Behavioral symptoms of dementia. A total of 4090 BSDs wereobserved and coded. Restlessness was the most frequentlyobserved behaviors with 1612 counts (39.41%), followed by prob-lematic vocalization 1041 counts (25.45%), banging/tapping, 967counts (23.64%), pacing 257 (6.28%), escaping restraints 169 (4.13%),and searching, 44 counts (1.0%).
Nursing assistantsDemographics. Twenty-eight NAs, average age 34 years (�9.63;
range 19e53 years), participated in the study. Except one African-American NA, the others identified themselves as solely Hispanic,primarily speaking Spanish. Nineteen NAs (67.9%) completed 12thgrade while 6 (21.5%) had post secondary school. All NAs usedsimple Korean words, mainly focused on activities of daily living(ADL), such as “sit” or “turn”. However, 18 (64.3%) reported thatthey occasionally experienced a language barrier with KA residentswhile assisting with their ADLs.
Dementia-appropriate communication style. The NAs’ dementia-appropriate communication style included providing a gentlepace of care 83.87% of the time, and using simple words or phrases97.92% of the time when interacting with a resident. Observationsof dementia-inappropriate communication style included notintroducing themselves before assisting the residents 79.57% of thetime, not addressing the resident by name 70.97% of the time priorto care, and entering a resident’s room without knocking (i.e., notacknowledging the resident) and talking, unrelated to work, withanother NA during care 54.55% of the time (Table 1).
Culturally-appropriate communication style. The NAs’ culturally-appropriate communication style included addressing the resi-dent appropriately (54.30%) and occasional making eye contact51.65% of the time. Observations of NAs’ culturally-inappropriatecommunication style included not greeting the resident prior tocare provision 72.2% of the time, using casual rather than politespeech when speaking Korean 84.63% of the time, and lookingdown a resident 81.32% of the time (Table 2).
Communication style and behavioral symptoms of dementia
While not statistically significant, the figures show trends of re-lationships between NAs’ use of a dementia-appropriate commu-nication style and the number of BSDs, interacting with use of aculturally-appropriate communication style. In addition, the trendwas more prominent among those exhibiting higher intensity BSDs(N ¼ 10). During morning care, there was a trend toward a negativerelationship between BSDs and NAs’ dementia-appropriatecommunication style that interacted with culturally-appropriatecommunication style. The expected count of BSDs decreased as thedementia-appropriate communication style increased in the pres-ence of low culturally-appropriate communication (between 0 and0.5) (N¼20;b¼1.95, S.E.¼3.04,p¼0.52). In thepresenceof culturalcommunication higher than 0.5 (between 0.5 and 1), however, theexpected count of BSDs increased slightly as the dementia-appropriate communication style increased (Fig. 1). This trend wasmore prominent among those with high intensity BSDs (N ¼ 10;b ¼ 4.43, S.E. ¼ 2.52, p ¼ 0.08) (Fig. 2).
In the afternoon, there was a similar negative trend betweenBSDs and dementia-appropriate communication that interactedwith culturally-appropriate communication. The expected count ofBSDs decreased as the dementia-appropriate communication styleincreased from 0 to 1, in the presence of a culturally-appropriatecommunication style (between 0.2 and 1) and decreased more
rapidly as culturally-appropriate communication style increased(N ¼ 20; b ¼ �4.03, S.E. ¼ 3.74, p ¼ 0.28) (Fig. 3). The trend ofrelationship was more prominent in the high intensity BSDs group(N ¼ 10; b ¼ �4.46, S.E. ¼ 3.59, p ¼ 0.22) (Fig. 4).
Discussion
Findings showed a trend of decreasing behavioral symptoms asNAs used a more dementia-appropriate communication style,consistent with other studies.28e31 In the afternoon observationperiod, the more NAs used both dementia and culturally appro-priate communication style, the further BSDs were likely todecrease in a short time frame (Fig. 3). While preliminary, thissuggests NAs need to understand and practice culturally appro-priate communication style while caring for KA residents withdementia to reduce BSD in a short time. However, the results werenot statistically significant. The possible reasons are as follows.
This study was conducted in a single ethno-specific NH, wheremost residents were Korean immigrants with cultural resources(e.g., Korean nurses, ethnic food). Korean nurses were occasionallyinvolved when the resident exhibited high intensity BSDs, such asscreaming and hitting. Since the graph shows a trend in the rela-tionship between communication style and BSDs, the findings maybe significant in an NH, where such Korean cultural resources aretypically rare. Further study of these relationships needs a largersample size in a variety of settings.
Other environmental factors may influence on the relationshipbetween NAs’ appropriate communication style and BSDs. Inparticular, morning care included numerous and varied care
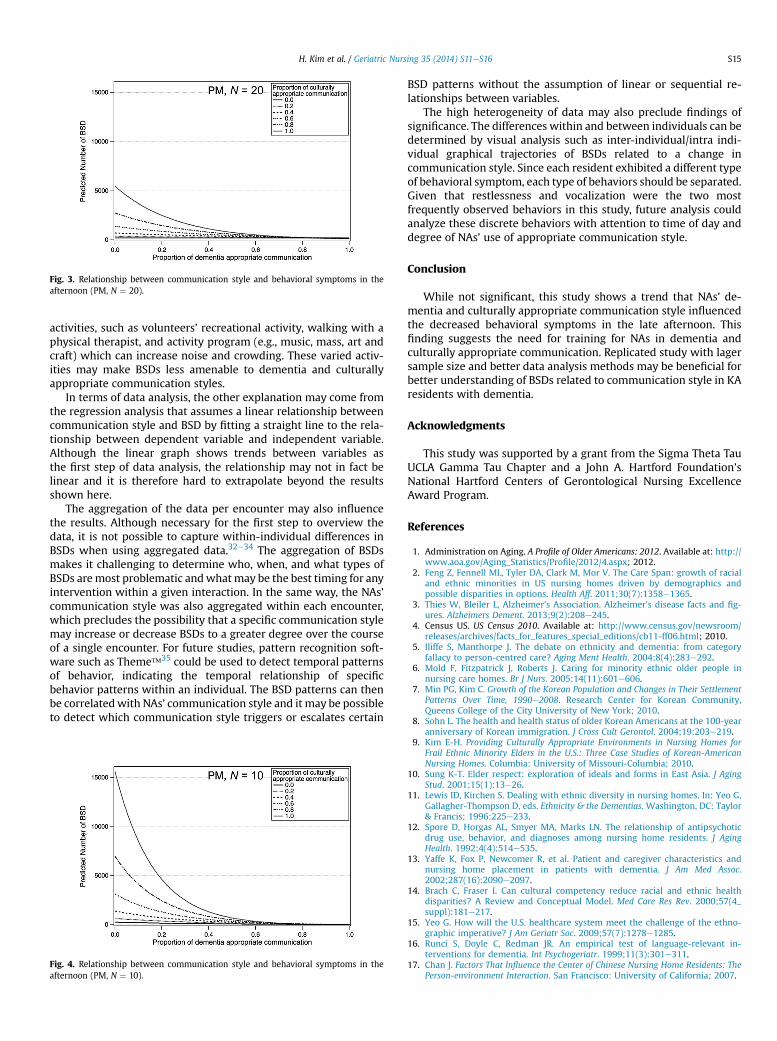
Fig. 3. Relationship between communication style and behavioral symptoms in theafternoon (PM, N ¼ 20).
H. Kim et al. / Geriatric Nursing 35 (2014) S11eS16 S15
activities, such as volunteers’ recreational activity, walking with aphysical therapist, and activity program (e.g., music, mass, art andcraft) which can increase noise and crowding. These varied activ-ities may make BSDs less amenable to dementia and culturallyappropriate communication styles.
In terms of data analysis, the other explanation may come fromthe regression analysis that assumes a linear relationship betweencommunication style and BSD by fitting a straight line to the rela-tionship between dependent variable and independent variable.Although the linear graph shows trends between variables asthe first step of data analysis, the relationship may not in fact belinear and it is therefore hard to extrapolate beyond the resultsshown here.
The aggregation of the data per encounter may also influencethe results. Although necessary for the first step to overview thedata, it is not possible to capture within-individual differences inBSDs when using aggregated data.32e34 The aggregation of BSDsmakes it challenging to determine who, when, and what types ofBSDs aremost problematic andwhatmay be the best timing for anyintervention within a given interaction. In the same way, the NAs’communication style was also aggregated within each encounter,which precludes the possibility that a specific communication stylemay increase or decrease BSDs to a greater degree over the courseof a single encounter. For future studies, pattern recognition soft-ware such as Theme�35 could be used to detect temporal patternsof behavior, indicating the temporal relationship of specificbehavior patterns within an individual. The BSD patterns can thenbe correlatedwith NAs’ communication style and it may be possibleto detect which communication style triggers or escalates certain
Fig. 4. Relationship between communication style and behavioral symptoms in theafternoon (PM, N ¼ 10).
BSD patterns without the assumption of linear or sequential re-lationships between variables.
The high heterogeneity of data may also preclude findings ofsignificance. The differences within and between individuals can bedetermined by visual analysis such as inter-individual/intra indi-vidual graphical trajectories of BSDs related to a change incommunication style. Since each resident exhibited a different typeof behavioral symptom, each type of behaviors should be separated.Given that restlessness and vocalization were the two mostfrequently observed behaviors in this study, future analysis couldanalyze these discrete behaviors with attention to time of day anddegree of NAs’ use of appropriate communication style.
Conclusion
While not significant, this study shows a trend that NAs’ de-mentia and culturally appropriate communication style influencedthe decreased behavioral symptoms in the late afternoon. Thisfinding suggests the need for training for NAs in dementia andculturally appropriate communication. Replicated study with lagersample size and better data analysis methods may be beneficial forbetter understanding of BSDs related to communication style in KAresidents with dementia.
Acknowledgments
This study was supported by a grant from the Sigma Theta TauUCLA Gamma Tau Chapter and a John A. Hartford Foundation’sNational Hartford Centers of Gerontological Nursing ExcellenceAward Program.
References
1. Administration on Aging. A Profile of Older Americans: 2012. Available at: http://www.aoa.gov/Aging_Statistics/Profile/2012/4.aspx; 2012.
2. Feng Z, Fennell ML, Tyler DA, Clark M, Mor V. The Care Span: growth of racialand ethnic minorities in US nursing homes driven by demographics andpossible disparities in options. Health Aff. 2011;30(7):1358e1365.
3. Thies W, Bleiler L, Alzheimer’s Association. Alzheimer’s disease facts and fig-ures. Alzheimers Dement. 2013;9(2):208e245.
4. Census US. US Census 2010. Available at: http://www.census.gov/newsroom/releases/archives/facts_for_features_special_editions/cb11-ff06.html; 2010.
5. Iliffe S, Manthorpe J. The debate on ethnicity and dementia: from categoryfallacy to person-centred care? Aging Ment Health. 2004;8(4):283e292.
6. Mold F, Fitzpatrick J, Roberts J. Caring for minority ethnic older people innursing care homes. Br J Nurs. 2005;14(11):601e606.
7. Min PG, Kim C. Growth of the Korean Population and Changes in Their SettlementPatterns Over Time, 1990e2008. Research Center for Korean Community,Queens College of the City University of New York; 2010.
8. Sohn L. The health and health status of older Korean Americans at the 100-yearanniversary of Korean immigration. J Cross Cult Gerontol. 2004;19:203e219.
9. Kim E-H. Providing Culturally Appropriate Environments in Nursing Homes forFrail Ethnic Minority Elders in the U.S.: Three Case Studies of Korean-AmericanNursing Homes. Columbia: University of Missouri-Columbia; 2010.
10. Sung K-T. Elder respect: exploration of ideals and forms in East Asia. J AgingStud. 2001;15(1):13e26.
11. Lewis ID, Kirchen S. Dealing with ethnic diversity in nursing homes. In: Yeo G,Gallagher-Thompson D, eds. Ethnicity & the Dementias. Washington, DC: Taylor& Francis; 1996:225e233.
12. Spore D, Horgas AL, Smyer MA, Marks LN. The relationship of antipsychoticdrug use, behavior, and diagnoses among nursing home residents. J AgingHealth. 1992;4(4):514e535.
13. Yaffe K, Fox P, Newcomer R, et al. Patient and caregiver characteristics andnursing home placement in patients with dementia. J Am Med Assoc.2002;287(16):2090e2097.
14. Brach C, Fraser I. Can cultural competency reduce racial and ethnic healthdisparities? A Review and Conceptual Model. Med Care Res Rev. 2000;57(4_suppl):181e217.
15. Yeo G. How will the U.S. healthcare system meet the challenge of the ethno-graphic imperative? J Am Geriatr Soc. 2009;57(7):1278e1285.
16. Runci S, Doyle C, Redman JR. An empirical test of language-relevant in-terventions for dementia. Int Psychogeriatr. 1999;11(3):301e311.
17. Chan J. Factors That Influence the Center of Chinese Nursing Home Residents: ThePerson-environment Interaction. San Francisco: University of California; 2007.

H. Kim et al. / Geriatric Nursing 35 (2014) S11eS16S16
18. Shin D-S. Residential and caregiver preferences of older Korean Americans.J Gerontol Nurs. 2008;34(6):48e54.
19. Folstein MF, Folstein SE, McHugh PR. “Mini-mental state.” A practical methodfor grading the cognitive state of patients for the clinician. J Psychiatr Res.1975;12(3):189e198.
20. Kang Y, Na D, Hahn S. A validity study on the Korean mini-mental state ex-amination (K-MMSE) in dementia patients. J Korean Neurol Assoc. 1997;15(2):300e308.
21. Woods DL, Dimond M. The effect of therapeutic touch on agitated behaviorand cortisol in persons with Alzheimer’s disease. Biol Res Nurs. 2002;4(2):104e114.
22. Bliwise DL, Lee KA. Development of an Agitated Behavior Rating Scale fordiscrete temporal observations. J Nurs Meas. 1993;1(2):115e124.
23. Kim H, Woods DL. The development of direct-care staff social interactioncoding schemas for nursing home residents with dementia. Geriatr Nurs.2012;33(2):113e117.
24. Altman DG. Inter-rater agreement. In: Practical Statistics for Medical Research.London, England: Chapman & Hall; 1991:404.
25. Cohen J. A coefficient of agreement for nominal scales. Educ Psychol Meas.1960;20:37e46.
26. Cameron AC, Trivedi PK. Regression Analysis of Count Data. New York: Cam-bridge Press; 1998.
27. Hedeker D, Gibbons RD. Longitudinal Data Analysis. New York: John Wiley &Sons, Inc; 2006.
28. Burgener S, Jirovec M, Murrell L, Barton D. Caregivers and environmentalvariables related to difficult behaviors in institutionalized demented elderlypersons. J Gerontol. 1992;47(4):242e249.
29. Hart BD, Wells D. The effects of language used by caregivers on agitation inresidents with dementia. Clin Nurse Spec. 1997;11(1):20e23.
30. Graneheim U, Norberg A, Jansson L. Interaction relating to privacy, identity,autonomy and security. An observational study focusing on a woman withdementia and “behavioural disturbances,” and on her care providers. J AdvNurs. 2001;36(2):256e265.
31. Skovdahl K, Kihlgren AL, Kihlgren M. Dementia and aggressiveness: videorecorded morning care from different care units. J Clin Nurs. 2003;12(6):888e898.
32. Garre-Olmo J, López-Pousa S, Vilalta-Franch J, de Gracia Blanco M, Vilarrasa AB.Grouping and trajectories of neuropsychiatric symptoms in patients withAlzheimer’s disease. Part II: two-year patient trajectories. J Alzheimers Dis.2010;22(4):1169e1180.
33. Mohs RC, Schmeidler J, Aryan M. Longitudinal studies of cognitive, functionaland behavioural change in patients with Alzheimer’s disease. Stat Med.2000;19(11e12):1401e1409.
34. Robert PH, Verhey FR, Byrne J, et al. Grouping for behavioral and psychologicalsymptoms in dementia: clinical and biological aspects. Consensus paper of theEuropean Alzheimer disease consortium. Eur Psychiatry. 2005;20:490e496.
35. Magnusson M. Discovering hidden time patterns in behavior: T-patterns andtheir detection. Behav Res Methods Instrum Comput. 2000;32(I):93e110.