Embed Size (px)
Citation preview
The North Carolina AHEC Program and Partnerships in Practice
Transformation
1
2
Mission Statement ofMission Statement of North Carolina AHEC Program North Carolina AHEC Program
• The mission of the North Carolina AHEC Program is to meet the state’s health and health workforce needs by providing educational programs in partnership with academic institutions, health care agencies, and other organizations committed to improving the health of the people of North Carolina.
3
Area Health Education Centers Program
• AHEC History and Background– 1970 Carnegie Report - “Higher Education and
The Nation’s Health”– 1972 Federal funding for initial 11 programs– Federal funds for start up– State and local support to sustain AHEC Programs long-term
• AHEC Program Today– AHEC Programs in 47 states– Over 240 regional AHEC centers
4
Area Health Education Centers Program
• AHEC in North Carolina– One of original 11 states– 1974 state funding– Strong support of General Assembly– Close links to Office of Rural Health and other rural
initiatives– NC AHEC largest and most comprehensive in the country
North Carolina AHEC Core Programs
• Community-Based Student Training– To provide students opportunities to learn from preceptors
in the community and to have experiences that focus on community health, primary care and prevention
• Community-Based Residency Training– To prepare primary care physicians, general surgeons,
psychiatrists and other needed specialties for practice in communities in the state
• Support for Practicing Health Professionals– To keep providers up-to-date, enhance the practice
environment, and improve quality and patient safety through continuing education programs and direct support for community practices
5
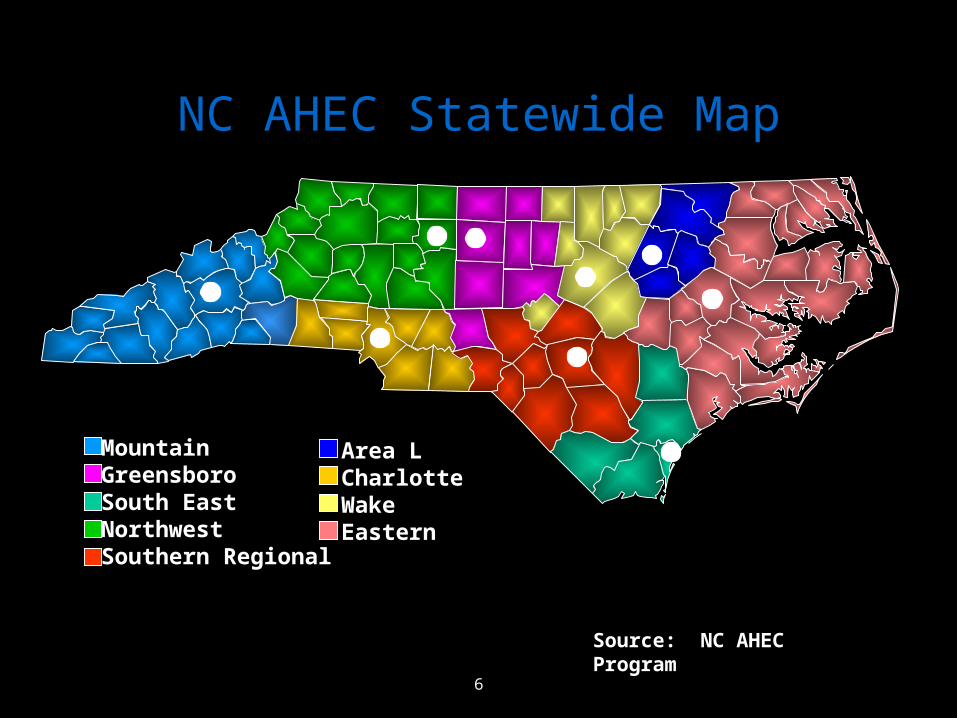
NC AHECAHEC Statewide Map
Source: NC AHEC Program
MountainGreensboroSouth EastNorthwestSouthern Regional
Area LCharlotteWakeEastern
6
AHEC Quality Initiative: Support for Practicing Health Professionals
• Improved quality is part of our mission• QI work complements our CE/CME programming• QI gives us clear measures to demonstrate outcomes
based on clinical data
• AHEC already in thousands of practices statewide– Placing students– Offering continuing education– Providing library resources– Many MDs are grads of AHEC residencies
7
Improving Performance in Practice: A National Quality Initiative
• NC one of two initial pilot states
• AHEC employs QIC (Quality Improvement Consultant)
• CCNC Network and AHEC selected M.D. practices to participate
• Numerous QIC visits to practices according to level of need a) Learn measurement b) PDSA’s c) Quarterly Regional Collaboratives – expert and peer sharing
8
Services Evolution
• QI focus / Registry / Population management DM and asthma (18 practices)
• PCMH and informatics added with emphasis on care algorithms and self-management teaching
• Full REC buffet
9
AHEC Onsite Practice-Based Services
• Health Information Technology - EHR’s
• Patient-Centered Medical Home Recognition
• QI / Workflow Redesign using rapid practice based measurement
10
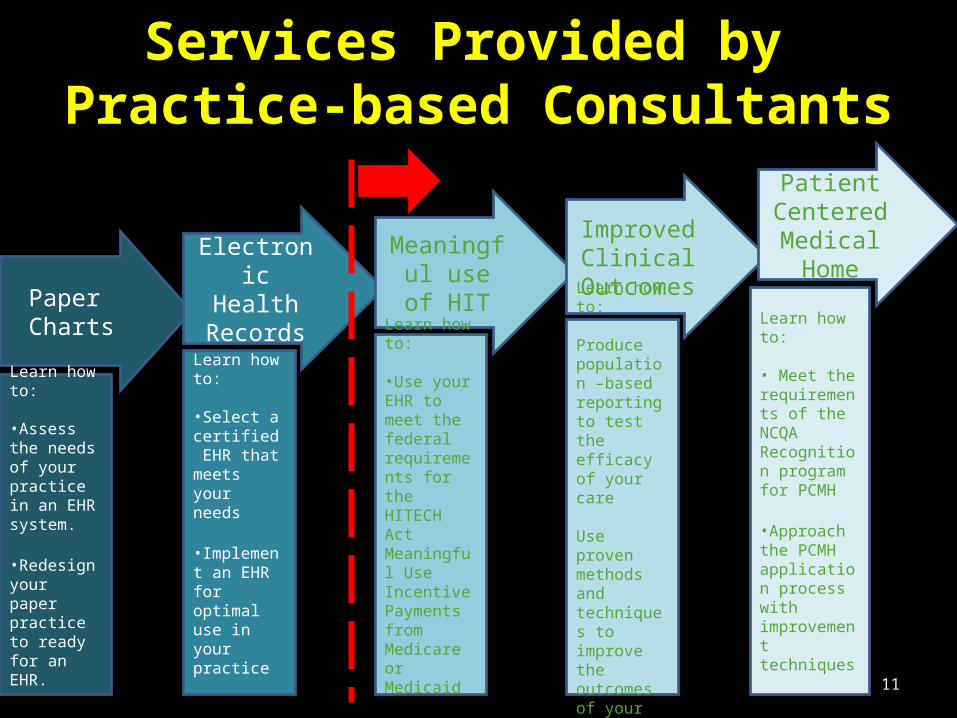
Paper Charts
Electronic Health
Records
Meaningful use of HIT
Improved Clinical
Outcomes
Patient Centered Medical Home
Learn how to:
•Select a certified EHR that meets your needs
•Implement an EHR for optimal use in your practice
Learn how to:
•Assess the needs of your practice in an EHR system.
•Redesign your paper practice to ready for an EHR.
Learn how to:
•Use your EHR to meet the federal requirements for the HITECH Act Meaningful Use Incentive Payments from Medicare or Medicaid
Learn how to:
Produce population –based reporting to test the efficacy of your care
Use proven methods and techniques to improve the outcomes of your patients
Learn how to:
• Meet the requirements of the NCQA Recognition program for PCMH
•Approach the PCMH application process with improvement techniques
11
Services Provided by Practice-based Consultants
• Priority primary care practices (10 or less docs or rural or urban safety net) receive services at no charge
• Developing a program for other specialties that will be fee based
12
Practical Implications
• 113,000 diabetic patients
• Strong diabetic control improved from a baseline of 24% to 47% of diabetic patients
• Translates to 1900 lives saved over 10 years
13
Current Enrollment
• 1020 practices
• 3742 primary care providers
• 3.8 million patients
• 900,000 with HTN; 400,000 Diabetics 320,000 asthmatics; 700,000 smokers
14
Conclusions
• Key to success of AHEC – CCNC partnership - Trusted entities known to collaborate well with others - Statewide presence BUT Local personnel and offices (infrastructure) - Solutions are bottom up; NOT top down edicts - Boots on the ground
• THE MESSAGE: - Care Management, PCMH, EHR’s, and QI are all tools to help practices help patients have the absolute best chance to live a better and longer lives – practices can enlist help in building these systems
15
























![AHEC 6408D+ Users Guide[1]](https://img.pdfslide.us/doc/110x75/577d26531a28ab4e1ea0dfe0/ahec-6408d-users-guide1.jpg)


