Embed Size (px)
Citation preview
The NHLBI Division for the Application of Research Discoveries
(DARD): Translating Science into Practice
Karen A. Donato, S.M.Acting Deputy Director, Division for the Application of
Research DiscoveriesNational Heart, Lung, and Blood Institute
July 8, 2011Filippino Cardiovascular Summit

NHLBI Strategic Plan (2007): Three Goals
Goal 1 – From Form to FunctionTo improve understanding of the molecular and physiological basis of health and disease and to use that understanding to develop improved approaches to disease diagnosis, treatment, and prevention.
Goal 2 – From Function to CausesTo improve understanding of the clinical mechanisms of disease and thereby enable better prevention, diagnosis, and treatment.
Goal 3 – From Causes to Cures To generate an improved understanding of the processes involved in translating research into practice and use that understanding to enable improvements in public health and to stimulate further scientific discovery.
2

DARD Efforts In Translation in Clinical Health-care Settings
3
NHLBI Clinical Practice Guidelines
• Cardiovascular Dz prevention Hypertension (1976-
2003) Cholesterol (1988-2004) Obesity (1998) Integrated Pediatric CV
Risk Reduction (pending release 2011)
• Asthma (1991-2007)
• Sickle Cell Disease (in progress)
4
Joint National Committee on Prevention, Detection,
Evaluation, & Treatment of High Blood Pressure (JNC)
JNC 7: 2003 JNC 6: 1997 JNC 5: 1992 JNC 4: 1988 JNC 3: 1984 JNC 2: 1980 JNC 1: 1976
Detection, Evaluation, &Treatment of High Blood Cholesterol in Adults (ATP,
Adult Treatment Panel) ATP III Update: 2004 ATP III: 2002 ATP II: 1993 ATP I: 1988
Clinical Guidelines on the Identification, Evaluation,
& Treatment of Overweight and Obesity in
Adults Obesity 1: 1998
55
History of NHLBI CVD Adult Clinical Guidelines
Cardiovascular Prevention Guidelines New Directions
New directions for CV guidelines derived from recommendations by several groups:•NHLBI Cardiovascular Disease Thought Leaders
June 17, 2005
•NHLBI Clinical Guidelines Users and Developers March 7, 2006
•NHLBI Guidelines Leadership Group (Stakeholder Representation)
November 15, 2007
6

Update guidelines on BP, cholesterol, and obesity Use systematic evidence review process Use evidence & recommendations grading Standardize and coordinate approaches Develop consistent recommendations for lifestyle & risk assessment
Create an integrated CV risk reduction guideline Individual risk factor guidelines + lifestyle and risk assessment +
additional CVD prevention approaches Develop an improved approach to implementation Write guidelines clearly so they are more implementable Emphasize user needs: primary care, specialists, patients, Develop and disseminate materials & tools Develop an evidence-based implementation plan Create a National Program to Reduce Cardiovascular Risk
Cardiovascular Prevention Guidelines New Directions
7

888
New NHLBI Approach to CV Guideline Development
Evidence-based approach, using systematic reviews and graded recommendations
Standardized coordinated approach to blood pressure, cholesterol, and overweight/obesity guideline updates
Crosscutting work groups to develop consistent recommendations on lifestyle, risk assessment, and implementation
Development of an integrated CVD risk reduction guideline Integrate the individual risk factor guidelines + additional
CVD risk issues + lifestyle and risk assessment Evidence-based approach to implementation; emphasize user
needs and implementability Primary care, specialists, and patients/consumers User friendly with clear focused messages

99
Call for Nomination: Dec 17, 2007 to Feb 1, 2008
Over 440 nominations, 350 nominees
Major inputs from GLG organizations and their membership and general public
Expert Panel Composition Diversity and balance of expertise
Diversity of demographics
Conflict of interest management
9
New NHLBI Approach to CV Guideline Development

1010
NHLBI CVD Guidelines: Panels & Workgroups Chairs/Co-Chairs
• Panels: High blood cholesterol/dyslipidemia (ATP IV)
Neil Stone, MD; Alice Lichtenstein, DSc
High blood pressure (JNC-8) Paul James, MD; Suzanne Oparil, MD
Obesity/Overweight (Obesity II) Michael Jensen, MD; Donna Ryan, MD
Integrated clinical guideline for CVD risk reduction Sidney C. Smith, Jr., MD
• Workgroups: Risk Assessment
David Goff, Jr., MD, PhD; Donald M. Lloyd-Jones, MD, ScD
Lifestyle Robert Eckel, MD; John Jakicic, PhD
Implementation Thomas Pearson, MD, PhD; Wiley Chan, MD
10

NHLBI Director
DARD Director
DARD Project Team
SAIC and RTI Support
Contracts
Clinical Guidelines Executive Committee
Expert Panel for the
Integrated CVD Guideline Development
Expert Panel for
Cholesterol Update
Expert Panel for
Hypertension Update
Expert Panel for Obesity Update
Risk Assessment
Lifestyle/Nutrition/PA
Implementation/System/IT/ Informatics
Cross-Cutting Workgroups
11
NHLBI Clinical Guidelines for CV Risk Reduction: Organizational Structure

Products:Evidence Reviews
*Same for all Guidelines
Products:
Updated RF Guidelines Implementation Plan
JNC 8
+
+
+ Approach to writing
guidelines (e.g., GLIA )
ATP IV
CVD Risk Factor List*
Risk Assessment Approach for Cholesterol
Heart Healthy Diet & Physical Activity*
Modifications for Chol.
+
+
+ Approach to writing
guidelines (e.g., GLIA)
OBESITY 2
CVD Risk Factors List*
Risk Assessment Approach for Obesity
Heart Healthy Diet & Physical Activity*
Modifications for Obesity
+
+
+ Approach to writing guidelines (e.g., GLIA)
CVD Risk Factor List*
Risk Assessment Approach for BP
Heart Healthy Diet & Physical Activity*
Modifications for BP
Implementation WG
Evidence Review on implementation approaches
Product:
Integrated CVD Risk Reduction Guideline
Product: Evidence-based
Implementation Plan
+Approach to patient: Risk assessment, Lifestyle, BP,
Chol, Obesity, Mult RFs, Other Risk Reduction Topics (e,g., Aspirin, Smoking, HRT)
Integrated Panel
Evidence Review on multiple RFs
Lifestyle WG
Evidence Review on Lifestyle
Issues
Risk Assessment WG
Evidence Review & Risk Prediction Model
Project Map
Implementation WG
Evidence-informed Guidance
Lifestyle WG
Evidence Review on Diet & Physical Activity
Risk Assessment WG
Evidence Review & Risk Prediction Model
Blood Pressure PanelEvidence Review on BP
Tx
Cholesterol PanelEvidence Review on
Cholesterol Tx
Obesity PanelEvidence Review on
Obesity Tx

131313
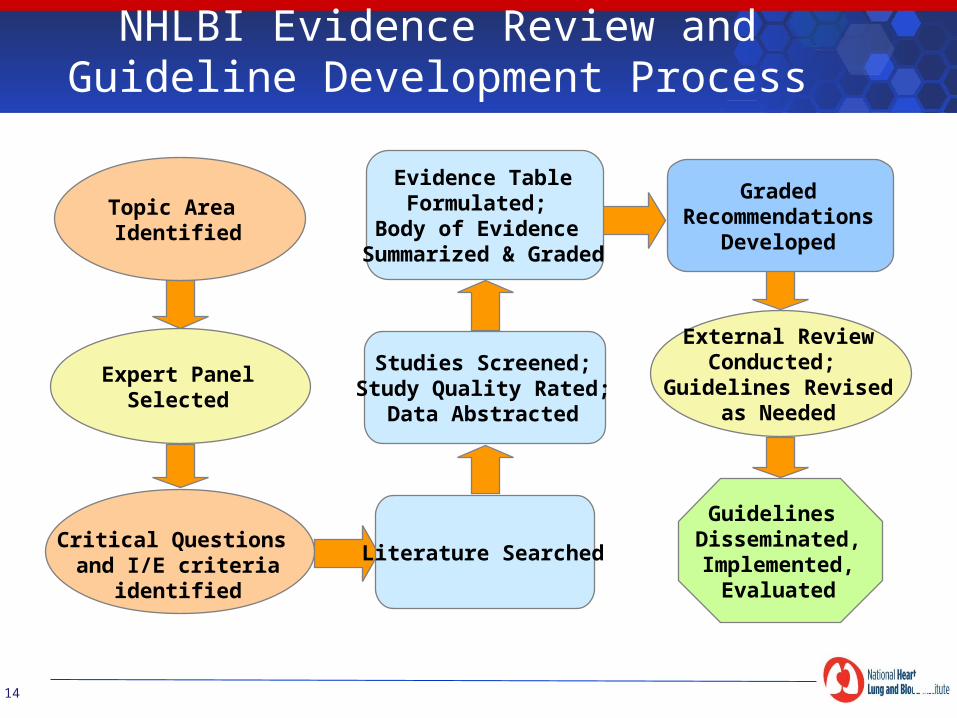
NHLBI Evidence Review and Guideline Development Process
14
Expert PanelSelected
External ReviewConducted;
Guidelines Revisedas Needed
Literature Searched
Studies Screened;Study Quality Rated;
Data Abstracted
Evidence TableFormulated;
Body of Evidence Summarized & Graded
Guidelines Disseminated,Implemented,
Evaluated
GradedRecommendations
Developed
Topic Area Identified
Critical Questions and I/E criteria
identified

151515
Step 1 – Develop critical questions (CQs)
Step 2 – Establish study inclusion & exclusion criteria
Step 3 – Search literature for relevant studies
Step 4 – Rate the quality of each included study
Step 5 – Abstract study data
Step 6 – Create evidence tables for each study
Step 7 – Summarize the evidence for each CQ
Evidence Review and Guideline Development Process

Critical Questions and I/E Criteria
Critical Question in PICOTS format Population Intervention/Exposure Control/Comparator Outcomes Time frame Setting
Inclusion/ Exclusion criteria: Selecting types of studies (e.g., observational, RCTs) Identifying subgroups Defining specific outcomes
16
Systematic search of the literature for each critical question using inclusion/exclusion criteria
Initial screen of citations by title and abstracts, followed by full-text review
All articles reviewed for inclusion independently by two trained reviewers
If the reviewers do not agree about inclusion status, a 3rd reviewer with content and methodological expertise reviews and adjudicates. If uncertainty remains, the article is included.
17
Literature Review Process
Rating the Quality of Individual Studies
The quality of each “included” study is rated by two independent reviewers
Good, Fair, Poor If the raters do not agree, a 3rd rater with content and
methodological expertise reviews and adjudicates Standardized NHLBI rating instruments with pre-specified criteria: Controlled intervention studies (e.g., RCTs) Observational studies (cohort, cross-sectional, case-control) Systematic reviews and meta-analyses
18
1919
Evidence-Based Review and Guideline Development Process
Step 8 – Review and grade the body of evidence for each critical question (or subquestion)
Step 9 – Draft graded recommendations (assure grade is aligned with quality and strength of evidence)
Step 10 – Release draft recommendations for public comment, with invitations for review
Step 11 – Review comments and revise recommendations as needed
Step 12 – Combine recommendations into guidelines Step 13 – Disseminate and implement guidelines
19

Type of EvidenceQuality Rating
• Well-designed, well-executed RCTs that adequately represent populations to which results are applied and directly assess effects on health outcomes• Well conducted meta-analyses of such studiesHighly certain about the estimate of effect.
High
• RCTs with minor limitations affecting confidence in, or applicability of, results;• Well-designed, well-executed nonrandomized controlled studies and well- designed, well-executed observational studies• Well conducted meta-analyses of such studiesModerately certain about the estimate of effect.
Moderate
• RCTs with major limitations• Nonrandomized controlled studies and observational studies with major limitations affecting confidence in, or applicability of, the results• Uncontrolled clinical observations without an appropriate comparison group (e.g., case series, case reports)• Physiological studies in humans• Meta-analyses of such studiesLow certainty about the estimate of effect.
Low
20
NHLBI Evidence Quality Rating System

Grade Strength of Recommendation
AStrong recommendation High certainty that the net benefit is substantial. Benefits are much greater than risks/harms.
BModerate recommendation Reasonable certainty that the net benefit is moderate to substantial or there is high certainty that the net benefit is moderate. Benefits are greater than risks/harms.
CWeak recommendation At least moderate certainty that the net benefit is small. Benefits may slightly outweigh risks/harms.
DRecommendation against At least moderate certainty that it has no net benefit or that risks/harms outweigh benefits.
E
Expert opinion Net benefit is unclear. Balance of benefits and harms cannot be determined because of no evidence, insufficient evidence, or conflicting evidence, but the panel thought it was important to provide clinical guidance and make a recommendation. Further research is recommended.
N
No recommendation for or against Net benefit is unclear. Balance of benefits and harms cannot be determined because of no evidence, insufficient evidence, or conflicting evidence, and the panel thought no recommendation should be made. Further research is recommended.
21
NHLBI Recommendation Strength
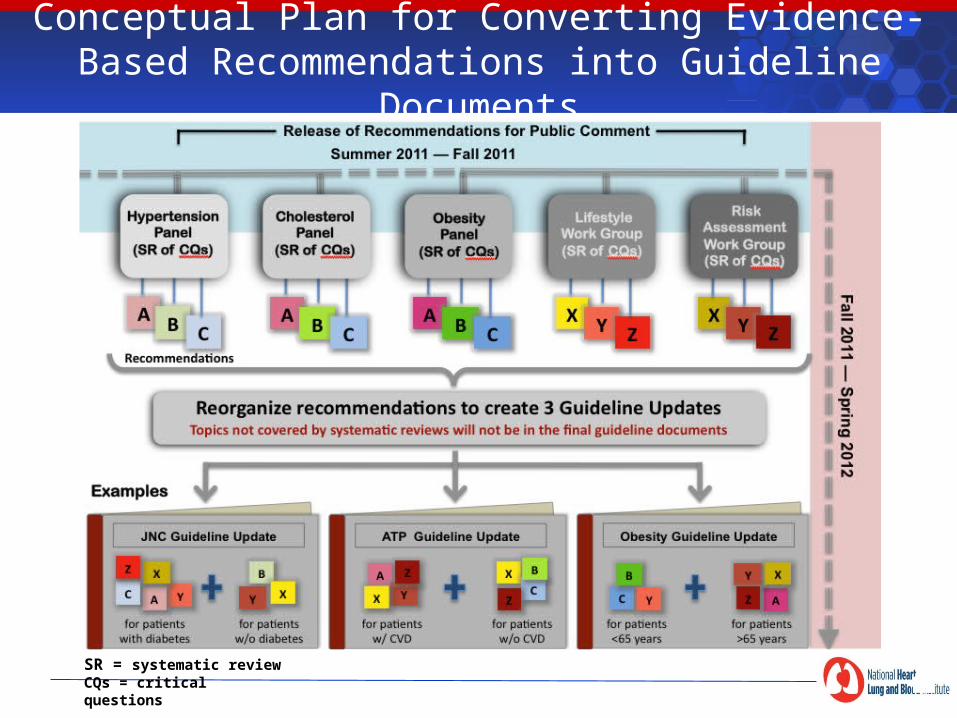
Conceptual Plan for Converting Evidence-Based Recommendations into Guideline Documents
SR = systematic reviewCQs = critical questions

Integrated Guideline on CV Risk Reduction in Children and Adolescents
• Topics: Screening for risk factors Family history Nutrition and diet
Physical activity
Tobacco exposure
High blood pressure
Lipids and lipoproteins
Overweight and obesity
Diabetes and other conditions Risk factor clustering and the metabolic syndrome
• To be released in 2011
23
CVD Risk Reduction Guideline in Children/Adolescents: Implementation
Purpose: To facilitate maximal adoption of the pediatric CV guideline to integrate assessment and treatment of CV risk factors into routine care by pediatric care providers
Approaches: Understand the needs of pediatric care providers through
formative research Create strategies and tools to facilitate application of the
guideline in the care of children and adolescents Evaluate strategies and tools in practice settings to determine
effectiveness and to enhance the tool kit Embed the tool kit into practice improvement projects to produce
large-scale practice adoption

25
Professional Education Materials

http://healthyweight. nhlbi.nih.gov

DARD Efforts in Translation for Community Settings and
Reducing Health Disparities
27
Goal: To employ the Community Health Worker (CHW) model to improve CV health in low-income and high-risk communities to reduce health disparities
Objectives:• To train and equip CHWs to conduct culturally
sensitive heart health education • To use evidence-based curricula and other
resources developed by NHLBI
• To improve knowledge and attitudes, and promote health behaviors and adherence that promote CV health
CHW Initiative – Goal and Objectives
28
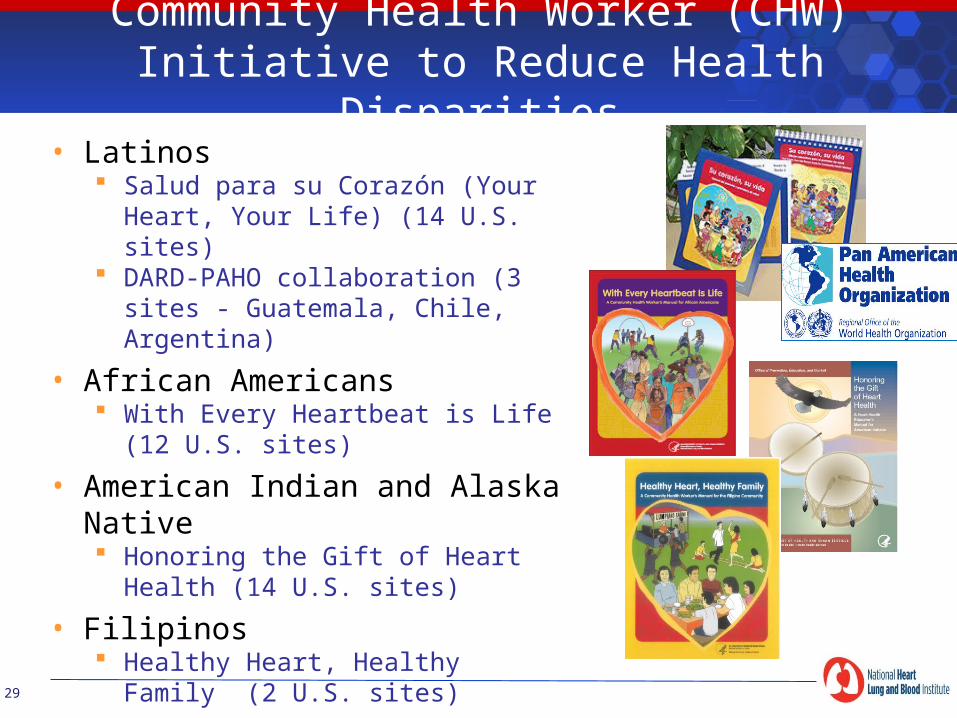
Community Health Worker (CHW) Initiative to Reduce Health Disparities
• Latinos Salud para su Corazón (Your
Heart, Your Life) (14 U.S. sites) DARD-PAHO collaboration (3 sites -
Guatemala, Chile, Argentina)
• African Americans With Every Heartbeat is Life (12
U.S. sites)
• American Indian and Alaska Native Honoring the Gift of Heart
Health (14 U.S. sites)
• Filipinos Healthy Heart, Healthy Family
(2 U.S. sites)29

History and Status of CHW Initiative
Background Created in 1994 to promote heart health and reduce disparities First curriculum was for Spanish-speaking Latinos
Strategies CHW training, community education, screening, lifestyle, and
clinical management (in some sites) Engagement of community partners to sustain the projects
Evaluations Process evaluation of 7 sites in 2001 Current evaluations to:
• Determine program effectiveness• Evaluate specific strategies• Determine future directions
30

We Can!® A National Education Program to Help Children and Families Maintain a Healthy Weight!
31
S.M.A.R.T
NIH Science Curricula Local Partnerships Local Media Outreach Events
Communities
Federal Clinical• Non-profit Media Corporate
Partnerships
Media
Web Print Television
We Can!™ media coverage: estimated reach of 1.4 billion
4 NIH Institutes (NHLBI, NIDDK, NICHD, NCI)
43 partners including CDC, HRSA, PCPFS, DOI (NPS,
FWS), Action for Healthy Kids, Subway, et al.
About 1500 Community Sites in 50 states, District of Columbia, Puerto Rico, Northern Mariana
Islands, 11 countries

We Can!® Sites
32
43 We Can! Partners
33

Implementing Clinical Guidelines: Improving Patient Outcomes
Guideline Implementation
(Simons-Morton, 2005)
Patient Health
Insurance & Government• Performance measures (e.g.,HEDIS)• Accreditation (JCAHO)• Insurance reimbursement (p4p)
Clinical Institutions• CME, academic detailing• Services & appointments• Patient monitoring & feedback• Reminders, charting cues, eHR• Provider incentives
Patients• Knowledge• Behaviors• Tx Adherence• Risk Factors
Clinicians• Screening & diagnoses• Treatments & procedures• Advice & counseling• Referrals
34
Phone: (301) 592-8573 Fax: (301) 592-8563 E-mail: [email protected] Internet: http://www.nhlbi.nih.gov Address: P.O. Box 30105 Bethesda, MD 20824-0105
Online Catalog: http://emall.nhlbihin.net
NHLBI Health Information Center

Thank you for your attention
36