Embed Size (px)
Citation preview

The New Content and Format Requirements for
Prescription Drug Labeling
Leaner, Cleaner, More Precise
Rachel E. Behrman, MD, MPH
Office of Medical Policy
Center for Drug Evaluation and Research Food and Drug Administration

2
Learning objectives At the conclusion of this session, participants should be able to: 1. Describe the major content and format
changes to prescription drug labeling and the rationale for the changes
2. Summarize the essential concepts for developing specific labeling sections from the new final and draft labeling guidances
3. Describe general principles for developing and converting labeling as described in the draft “Implementation” guidance

3
Impetus and Rationale• Increasing length, detail and complexity of prescription
drug labeling• Research demonstrated that prescribers:
– Use labeling primarily to find a specific item of information or answer a specific question
– Found existing format difficult to use when looking for specific information
– Wanted easy access to certain labeling sections that they find more useful or important
– Would use labeling more if it included a short (maximum length one-half page) synopsis
• Result is more informative, accessible and memorable labeling, resulting in a better risk communication and management tool that will decrease errors due to misunderstood or incorrectly applied drug information

OverviewHighlights
– High level ½ page summary– Cited or concisely summarized information accompanied by identifying
numbers indicating where to find more detail
Contents – Allows easy reference to full prescribing information– Allows hyperlinks in electronic formats
Reorders and reorganizes sections– Frequently referenced information moved forward– Safety information remains consolidated
Establishes format requirements– Minimum 8-point font (trade labeling that accompanies drug product will
have minimum 6-point font)– Standardized bolding and “white space”
Clarifies and updates requirements

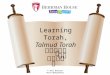
Example of Highlights for a Fictitious DrugHIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use Imdicon safely and effectively. See full prescribing information for Imdicon. IMDICON® (cholinasol) CAPSULES Initial U.S. Approval: 2000
WARNING: LIFE-THREATENING HEMATOLOGICAL ADVERSE REACTIONS
See full prescribing information for complete boxed warning. Monitor for hematological adverse reactions every 2 weeks for first 3 months of treatment (5.2). Discontinue Imdicon immediately if any of the following occur: Neutropenia/agranulocytosis (5.1) Thrombotic thrombocytopenic purpura (5.1) Aplastic anemia (5.1) ----------------------------RECENT MAJOR CHANGES-------------------------- Indications and Usage, Coronary Stenting (1.2) 2/200X Dosage and Administration, Coronary Stenting (2.2) 2/200X ----------------------------INDICATIONS AND USAGE--------------------------- Imdicon is an adenosine diphosphate (ADP) antagonist platelet aggregation inhibitor indicated for: Reducing the risk of thrombotic stroke in patients who have experienced
stroke precursors or who have had a completed thrombotic stroke (1.1) Reducing the incidence of subacute coronary stent thrombosis, when
used with aspirin (1.2) Important limitations: For stroke, Imdicon should be reserved for patients who are intolerant of
or allergic to aspirin or who have failed aspirin therapy (1.1) ----------------------DOSAGE AND ADMINISTRATION----------------------- Stroke: 50 mg once daily with food. (2.1) Coronary Stenting: 50 mg once daily with food, with antiplatelet doses
of aspirin, for up to 30 days following stent implantation (2.2) Discontinue in renally impaired patients if hemorrhagic or hematopoietic problems are encountered (2.3, 8.6, 12.3)
---------------------DOSAGE FORMS AND STRENGTHS---------------------- Capsules: 50 mg (3)
-------------------------------CONTRAINDICATIONS------------------------------ Hematopoietic disorders or a history of TTP or aplastic anemia (4) Hemostatic disorder or active bleeding (4) Severe hepatic impairment (4, 8.7) -----------------------WARNINGS AND PRECAUTIONS------------------------ Neutropenia (2.4 % incidence; may occur suddenly; typically resolves
within 1-2 weeks of discontinuation), thrombotic thrombocytopenic purpura (TTP), aplastic anemia, agranulocytosis, pancytopenia, leukemia, and thrombocytopenia can occur (5.1)
Monitor for hematological adverse reactions every 2 weeks through the third month of treatment (5.2)
------------------------------ADVERSE REACTIONS------------------------------- Most common adverse reactions (incidence >2%) are diarrhea, nausea, dyspepsia, rash, gastrointestinal pain, neutropenia, and purpura (6.1). To report SUSPECTED ADVERSE REACTIONS, contact (manufacturer) at (phone # and Web address) or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
------------------------------DRUG INTERACTIONS------------------------------- Anticoagulants: Discontinue prior to switching to Imdicon (5.3, 7.1) Phenytoin: Elevated phenytoin levels have been reported. Monitor
levels. (7.2) -----------------------USE IN SPECIFIC POPULATIONS------------------------ Hepatic impairment: Dose may need adjustment. Contraindicated in
severe hepatic disease (4, 8.7, 12.3) Renal impairment: Dose may need adjustment (2.3, 8.6, 12.3) See 17 for PATIENT COUNSELING INFORMATION and FDA-approved patient labeling
Revised: 5/200X

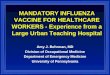
Example of Contents for a Fictitious DrugFULL PRESCRIBING INFORMATION: CONTENTS* WARNING – LIFE-THREATENING HEMATOLOGICAL ADVERSE REACTIONS 1 INDICATIONS AND USAGE
1.1 Thrombotic Stroke 1.2 Coronary Stenting
2 DOSAGE AND ADMINISTRATION 2.1 Thrombotic Stroke 2.2 Coronary Stenting 2.3 Renally Impaired Patients
3 DOSAGE FORMS AND STRENGTHS 4 CONTRAINDICATIONS 5 WARNINGS AND PRECAUTIONS
5.1 Hematological Adverse Reactions 5.2 Monitoring for Hematological Adverse Reactions 5.3 Anticoagulant Drugs 5.4 Bleeding Precautions 5.5 Monitoring: Liver Function Tests
6 ADVERSE REACTIONS 6.1 Clinical Studies Experience 6.2 Postmarketing Experience
7 DRUG INTERACTIONS 7.1 Anticoagulant Drugs 7.2 Phenytoin 7.3 Antipyrine and Other Drugs Metabolized Hepatically 7.4 Aspirin and Other Non-Steroidal Anti-Inflammatory Drugs 7.5 Cimetidine 7.6 Theophylline 7.7 Propranolol 7.8 Antacids 7.9 Digoxin 7.10 Phenobarbital 7.11 Other Concomitant Drug Therapy 7.12 Food Interaction
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy 8.3 Nursing Mothers 8.4 Pediatric Use 8.5 Geriatric Use 8.6 Renal Impairment 8.7 Hepatic Impairment
10 OVERDOSAGE 11 DESCRIPTION 12 CLINICAL PHARMACOLOGY 12.1 Mechanism of Action 12.2 Pharmacodynamics 12.3 Pharmacokinetics 13 NONCLINICAL TOXICOLOGY 13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility 14 CLINICAL STUDIES 14.1 Thrombotic Stroke 14.2 Coronary Stenting 16 HOW SUPPLIED/STORAGE AND HANDLING 17 PATIENT COUNSELING INFORMATION
17.1 Importance of Monitoring 17.2 Bleeding 17.3 Hematological Adverse Reactions 17.4 FDA-Approved Patient Labeling
*Sections or subsections omitted from the full prescribing information are not listed.

ImprovementsEmphasizes “Patient Counseling Information”
– Referenced in Highlights– New section in Full Prescribing Information (FPI)– Approved patient labeling, if available, is reprinted at end
Encourages AR reporting by including contact information (toll-free number and Internet address) for reporting both serious and nonserious ARs
Identifies and Dates “Recent Major Changes”– Captures Boxed Warning, Indications, D&A, Contraindications and
W&P– Referenced in Highlights; margin mark in FPI
Adds the established pharmacologic class, if known, to Highlights
Adds initial U.S. approval date

Format Changes
• Warnings and Precautions consolidated• Formerly in Precautions, now new sections
– Drug Interactions– Use in Specific Populations– Patient Counseling Information
• Formerly optional, now required– Clinical Studies– Nonclinical Toxicology
• Created Dosage Forms and Strengths and moved How Supplied to near end

Revision of Safety Requirements• Contraindications
– Risk of use clearly outweighs any possible benefit– Includes only known hazards (e.g., eliminate “allergic to any
component of drug”)
• Warnings and Precautions Expanded to include clinically significant adverse reactions
• Adverse Reactions – Retains, and clarifies, existing definition of what to include
(reasonable association = some basis for causal relationship)– Separates ARs from clinical trials and postmarketing
spontaneous reports– Revises requirements on how to classify and categorize ARs
and how to describe AR rates– Requires a description of AR profile based on entire database

Adverse Reaction DefinitionPrevious § 201.57 Revised § 201.57
An adverse reaction is an undesirable effect, reasonably associated with the use of the drug, that may occur as part of the pharmacological action of the drug or may be unpredictable in its occurrence.
For the purposes of prescription drug labeling, an adverse reaction is an undesirable effect, reasonably associated with use of a drug, that may occur as part of the pharmacological action of the drug or may be unpredictable in its occurrence. This definition does not include all adverse events observed during use of a drug, only those adverse events for which there is some basis to believe there is a causal relationship between the drug and the occurrence of the adverse event.

Other Clarifications• D&A and I&U
Dosing regimens and indications or uses not included in these sections must not be implied or suggested in other sections
• For approval based on a surrogate, I&U must– Include a succinct description of the limitation of use– Describe any uncertainty about the anticipated benefit – Refer to a description of available evidence in Clinical Studies
• Clinical Studies– Include detail about AWC studies pertinent to S&E use– Not an encyclopedic listing
• References – include only when labeling must rely on either– Recommendation by authoritative body– Standardized methodology, scale or technique

Affected Products
• New NDAs, BLAs and efficacy supplements (e.g., new indication, new dosage regimen, new route of administration)
• Applications and efficacy supplements approved up to 5 years prior to final rule
• Encourage voluntary compliance by older products
• All products must append FDA-approved patient labeling within 1 year

Implementation ScheduleNDA, BLA or efficacy
supplementLabeling must conform
Submitted on or after 6/30/06 At time of submission
Pending on 6/30/06
Approved 6/30/05-6/30/066/30/09 (3 years)
Approved 6/30/04-6/29/05 6/30/10 (4 years)
Approved 6/30/03-6/29/04 6/30/11 (5 years)
Approved 6/30/02-6/29/03 6/30/12 (6 years)
Approved 6/30/01-6/29/02 6/30/13 (7 years)
Approved Pre-6/30/01Voluntary at any time
(encouraged to conform)

Appending Patient Labeling
FDA-approved patient labeling must be reprinted at end of labeling or accompany labeling by June 30, 2007
– Includes MedGuides, approved “PPIs,” instructions for use, etc.
– Applies to all drugs, including “older” products that are not subject to the new requirements
– Can be submitted in the Annual Report

Labeling Supplement Regulations(§§ 314.70 and 601.12)
• Changes to Highlights require submission of a prior-approval labeling supplement
• Exceptions – changes to Highlights that may be submitted in the Annual Report– Removal of a listed section from “Recent
Major Changes” after 1 year– Changes to the revision date

Older Prescription Drug Products
• § 201.57 redesignated § 201.80• Modifications
– Ensure that statements currently appearing in labeling related to effectiveness or dosage and administration are sufficiently supported
– Require that FDA-approved patient labeling be attached or accompany prescription drug labeling (within 1 year of effective date)
– Limit References to cited authoritative report, methodology, scale or technique

21 CFR Changes
§ 201.56 General labeling requirements
§ 201.57 Specific requirements for “newer” drugs
§ 201.58 Waiver provision
§ 201.80 Specific requirements for “older” drugs
(formerly § 201.57)
§§ 314.70 and 601.12 Supplements – changes to Highlights require prior-
approval

Related Regulatory Initiatives
Electronic Labeling Rule required sponsors to submit e-labeling to FDA beginning 6/2004
Barcoding rule requires bar codes on labels of prescription drugs and OTC drugs
The Drug Listing Proposed Rule will require the electronic submission to FDA of drug registration and listing information for all marketed human and animal medical products
Modernizing MedWatch– Expanding communications– Unified AE reporting systems
Paperless labeling will eliminate requirement for insert

§ 201.56 General RequirementsLabeling must:
– Contain a summary of essential scientific information for the safe and effective use of the drug
– Be informative and accurate and neither promotional in tone nor false or misleading
– Be based whenever possible on data derived from human experience. No implied claims or suggestions of drug use may be made if there is inadequate evidence of safety or lack of substantial evidence of effectiveness
– Be updated when new information becomes available that causes the labeling to become inaccurate, false, or misleading