Embed Size (px)
Citation preview

Journal of Child and Family Studies (2018) 27:2161–2170https://doi.org/10.1007/s10826-018-1046-z
ORIGINAL PAPER
The Network Structure of Childhood Psychopathology inInternational Adoptees
Marko Elovainio 1,2● Christian Hakulinen1
● Laura Pulkki-Råback3 ● Hanna Raaska4 ● Helena Lapinleimu5
Published online: 28 February 2018© Springer Science+Business Media, LLC, part of Springer Nature 2018
AbstractInternational adoptees are at an increased risk of emotional and behavioral problems, especially those who are adopted at anolder age. We took a new approach in our study of the network structure and predictability of emotional and behavioralproblems in internationally adopted children in Finland. Our sample was from the on-going adoption study and comprised778 internationally adopted children (387 boys and 391 girls, mean age 10.5 (SD 3.4) years). Networks were estimated usingGaussian graphical models and lasso regularization for all the children, and separately for those who were adopted atdifferent ages. The results showed that anxiety/depressive symptoms, social problems, and aggressiveness were the mostcentral symptom domains. Somatic symptoms were the least central and had the weakest effect on the other domains.Similarly, aggressiveness, social problems, and attention problems were high in terms of predictability (73–65%), whereasinternalizing problems were relatively low (28–56%). There were clear but local age-group differences in network structure,symptom centrality, and predictability. According to our findings, network models provide important additional informationabout the centrality and predictability of specific symptom domains, and thus may facilitate targeted interventions amonginternational adoptees.
Keywords Network ● Adoption ● CBCL ● Behavioral problems
Introduction
Although most adopted children are well-adjusted (Jufferand van Ijzendoorn 2005), adoption has been identified asan independent risk factor for psychiatric and psychologicalproblems. Studies have reported that several factors inaddition to the individual genetic and biosocial background,such as social circumstances prior to adoption, the back-ground of the adoptive family, and relationships between
the adopted child and his or her family members, mayexacerbate developmental difficulties and psychologicalsymptoms (Merz and McCall 2010; O’Connor et al. 2003).It has been shown that a later age at adoption poses aspecific mental-health risk (Fensbo 2004), and that childrenwho are younger when they are adopted recover morequickly from the process of adoption and the potentialmental-health problems (Beckett et al. 2002). Moreover,girls adopted at more than 12 months of age have morepsychological problems than those adopted at a younger age(van Ijzendoorn et al. 2005).
Childhood psychiatric problems have traditionally beenclassified in terms of externalizing or internalizing beha-vioral and emotional problems (Achenbach et al. 1987).Internalizing symptoms reflect problems such as anxiety,depression, somatic complaints without a medical cause,and withdrawal from social contact. Externalizing symp-toms, on the other hand, manifest in conflicts with otherpeople and their expectations of the children’s behavior, andinclude aggression and rule breaking. The most stronglyestablished method for determining or characterizingbehavioral and emotional problems in children is the ChildBehavior Checklist questionnaire (CBCL). In terms of
* Marko [email protected]
1 Department of Psychology and Logopedics, University ofHelsinki, Helsinki, Finland
2 National Institute for Health and Welfare, Helsinki, Finland3 Collegium of Advanced Sciences, University of Helsinki,
Helsinki, Finland4 Department of Child Psychiatry, Helsinki University Central
Hospital, Helsinki, Finland5 Department of Pediatrics and Medicine, Turku University Central
Hospital, Turku, Finland
1234
5678
90();,:

output, the CBCL gives total scores and separates theinternalizing and externalizing symptom scores (second-order symptom domains), and produces different subscalesfor “thought”, “attention”, and “social” problems among6–18-year-olds (Achenbach and Dumenci 2001).
The common-cause hypothesis, which posits thatunderlying childhood disorders are dynamic and changedepending on the developmental stage, has not been wellascertained (Rutter et al. 2001). The new dynamic-networkhypothesis in the field of psychopathology has recentlychallenged the common-cause approach (Borsboom 2017;Borsboom and Cramer 2013), inspiring a rapidly expandingline of research (Boschloo et al. 2016; Fried et al. 2017).According to this new research stream, psychologicalsymptoms and behavioral problems should be con-ceptualized as nodes (symptoms or problems) in a networkthat are mutually dependent via causal associations (edges)(Borsboom and Cramer 2013). Feeling anxious, forinstance, could lead to problems with sleeping, which inturn may lead to concentration problems. Hence, psycho-logical symptoms may spread and activate other symptomsin a dynamic network (Boschloo et al. 2015; Epskamp et al.2012; Frewen et al. 2013; van Borkulo et al. 2014).
The theoretical underpinning in the network perspectiveis that symptoms are not assumed to be interchangeable,and that their importance, i.e., centrality, in the networkshould be estimated empirically. Centrality refers tosymptoms that have strong connections with many others,the activation of which they are likely to expand through thesymptom network once it is activated. Symptoms withfewer connections lie on the periphery of the network andare less important to the entity it describes (Cramer et al.2010; Cramer et al. 2016; Bringmann et al. 2015; vanBorkulo et al. 2015). This research approach has beenapplied to a range of phenomena in adults, includingdepression (Boschloo et al. 2016; Fried et al. 2015), anxietydisorders (Beard et al. 2016), psychotic disorders (Isvoranuet al. 2016; Isvoranu et al. 2017), substance abuse (Rhem-tulla et al. 2016), the general structure of psychiatricsymptomatology (Boschloo et al. 2015), health-relatedquality of life (Kossakowski et al. 2016), and personalitytraits (Constantini et al. 2015), but there are significantlyfewer studies regarding childhood problems.
All in all, the conceptualization of various psychiatricand psychological symptoms as networks have shed newlight on the interconnections of individual symptoms, andthereby on the symptoms that should be the focus ofinterventions. For instance, symptoms that were closer tothe center in the network of depressive symptoms (loss ofinterest and pleasure, depressed mood, fatigue) werestronger predictors of the onset of a depressive episode thanthose that were not as central (hypersomnia, decrease inappetite) (van Borkulo et al. 2015a, 2015b).
Although psychiatric symptoms in children have not beenexamined from a network perspective, a previous studyanalyzed psychiatric symptomology in adolescents inaccordance with the network approach using the Youth self-report scale on the symptom level (Boschloo et al. 2016).Our study will make a further contribution in testing thenetwork structure at the symptom-domain level in a sampleof international adoptees, who have been shown to face anincreased risk of psychiatric problems (Elovainio et al. 2015;Raaska et al. 2012). First, we examined the structure ofchildhood behavioral and emotional problems in terms of itsarchitecture, constructing a symptom-domain network in asample of international adoptees. Second, given the evidencethat older adoptees face an increased psychopathological risk(Raaska et al. 2012), we tested whether the network struc-tures of children who were adopted at an older as opposed toa younger age differed. Third, using the network metrics ofcentrality (indicating the relative importance of the symp-tom) and node strength (indicating the strength of its con-nection with other symptoms) we investigated which itemswere most significant to behavioral and emotional problemsin childhood. Fourth, we evaluated the predictability of theindividual symptom domains (how well each symptom inthe network is predicted by all the other symptoms). Pre-dictability gives an additional estimate of how relevant agiven symptom is, and how it would change after an inter-vention focused on other symptoms.
Method
Participants
This study is part of on-going research covering all children(634 boys and 816 girls, response rate 55.7%) (Raaska et al.2012) adopted internationally through the three legalizedadoption organizations in Finland between the years 1985and 2007. The children were from Asia (China, Thailand,the Philippines, India, Vietnam, Sri Lanka, Pakistan, Nepal,Taiwan, Southern Korea, Israel), Africa (Southern Africa,Ethiopia, Mozambique), America (Columbia, Guatemala,the Dominican Republic, USA, Canada) and Eastern Eur-ope (Russia, Romania, Estonia, Poland).
Procedure
Data were gathered via self-administered questionnairesboth from the adoptive parents and from adoptees aged over9 years (2007–2009). A subsample of children aged 6–15years with no missing values in the CBCL symptom-domain measures was used in the current study (N= 758).He participants were divided into two age groups (meanages 1.0 and 4.4 years at the time of the adoption).
2162 Journal of Child and Family Studies (2018) 27:2161–2170

The Ethics Review Committee of the Hospital District ofSouth-West Finland approved this study, and the partici-pating children and their parents gave their written consentfor their participation.
Measures
The Child Behavior Checklist (CBCL) was used to assessbehavioral and emotional problems. We grouped thesymptoms as internalizing vs. externalizing, each beingrated 0= “not true”, 1= “somewhat or sometimes true”, or2= “very true or often true”. The CBCL has previouslybeen used among internationally adopted children, withgood psychometric test results (Dedrick et al. 2008). Weused questionnaires compiled for those aged 6–18 andcontaining 113 questions (Hawk and McCall 2010). Fromthese we constructed the following symptom domains:anxiety/depression, withdrawal/depression, somatic com-plaints, rule-breaking behavior, social problems, thoughtproblems, attention problems, and aggressive behavior(Achenbach and Rescorla 2001). The Cronbach’s alphas ofthe individual domains were all above 0.97.
Data Analyses
The network structure of the CBCL symptom domains wasestimated as a Gaussian Graphical Model using the Rqgraph package (Epskamp et al. 2012). The least absoluteshrinkage and selection operator (graphical lasso) procedure(Tibshirani 1996) estimates a network in which the nodesare CBCL symptom domains (e.g., aggressiveness, rulebreaking, social problems) and the edges are partial corre-lation coefficients between the nodes. Thus, each edgerepresents the relationship between two nodes (symptom-domain variables), after controlling for all other relation-ships in the network. The Graphical lasso minimizes theprobability of detecting false positive edges by setting verysmall edges to zero. The shrinkage parameter is chosen tominimize the extended Bayesian Information Criterion(Chen and Chen 2008), and has been shown accurately torecover underlying network structures (van Borkulo et al.2014). The graphical representation of networks is based onthe Fruchterman–Reingold algorithm that places nodes withstronger and/or more connections closer together. Giventhat CBCL symptoms are ordered-categorical, the analyseswere based on polychoric correlation.
We tested the robustness of the eight-symptom-domainnetwork and of the graph-theoretical measures derived fromit using the R-package “bootnet”, a bootstrap samplingprocedure (Epskamp 2015). We evaluated the stability ofthe centrality metrics by repeatedly correlating centralitymetrics of the original data set with those calculated fromsubsamples including less and less participants. We then
calculated the centrality stability correlation coefficient (CS-coefficient) to quantify stability. The CS-coefficient is themaximum number of participants that can be dropped whilemaintaining 95% probability that the correlation betweencentrality metrics from the full data set and the subset dataare at least 0.70. CS-coefficients above 0.50 indicate stablecentrality and above 0.25 is recommended for interpretingcentrality indices.
We then estimated the centrality of all the symptoms,which represents the connectedness of a given symptomwith all the others in the network. The centrality indicatorswere: (A) node-strength centrality defined as the sum of allassociations a given symptom exhibits with all other nodes;(B) betweenness centrality based on the concept that theshortest path length connects any two symptoms (a symp-tom with high betweenness lies along the shortest pathconnecting many other symptoms); and (C) closeness cen-trality as a measure of how close a symptom is to all theother symptoms (Opsahl et al. 2010). The difference inoverall connectivity (defined as the weighted sum of theabsolute connections (Barrat et al. 2004)) between the net-works of those who were adopted at a younger vs. an olderage was assessed statistically using the Network ConnectionTest (NCT), which is implemented in the R-package NCT(Van Borkulo 2015a, 2015b). The NCT is a two-tailedpermutation test involving the repeated (100,000 times)calculation of the difference between two groups of ran-domly regrouped individuals. It results in a distributionunder the null hypothesis (on the assumption that bothgroups are equal), which can be used to test the significanceof any difference between the groups. The observed dif-ference is considered significant at the threshold of 0.05.We assessed the predictability of the individual symptomsusing the R-package MGM, which was developed forestimating time-varying mixed graphical models (Haslbeck2016) version 1.1.-7. The MGMs were estimated via 1-regularized (lasso) neighborhood regression, the neighbor-hood of a node being the set of nodes connected to it.
Results
Table 1 shows the means and standard deviations of theCBCL symptom domains. The mean age of the participants(girls 50.3%) was 2.7 years (SD 2.1) at the time of adoptionand 10.5 years (SD 3.4 years) at the time of the data col-lection. The average age at the time of the adoption in theyounger group was 1.0 years (SD 0.7) and 4.4 years (SD(0.7) in the older group.
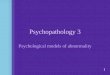
Figures 1a, b show the symptom networks of all theadoptees, and of the two age groups. The edges between thenodes within a network correspond to polychoric partialcorrelations between the CBCL domains, after controlling
Journal of Child and Family Studies (2018) 27:2161–2170 2163

for all other domains. The stronger the connection betweentwo nodes, the thicker and more saturated is the edge (theconnecting line between two nodes). Positive and negativeconnections are denoted by green and red edges, respec-tively. Each node corresponds to a CBCL symptom domain,as shown in Table 1, and is colored according to the second-order domain to which it is allocated (as shown in Fig. 1a,b). The Fruchterman–Reingold algorithm, which placesmore strongly connected nodes closer together, is used fornode placement in all the networks. The global structure ofeach one partly reflects the second-order-domain set-up.Domains belonging to the same second-order domain wereclosely connected and clustered (in predetermined second-order domains). For instance, aggressive behavior and rulebreaking were strongly connected, representing a second-order domain of externalizing symptoms. Withdrawal andanxiety were also connected, representing a second-orderdomain of internalizing symptoms, and of the second-order-domain “other symptoms”, attention problems and socialproblems were connected. Thought problems seemed to be abridging symptom between internalizing and externalizing.
Our person-dropping stability analysis produced CS-coefficients of 0.23, 0.62, and 0.74 for our betweenness,closeness, and strength centrality metrics, respectively. Thevalue for betweenness was below and the others were abovethe recommended minimum threshold of 0.25, suggestingthat the centrality estimates are somewhat unstable. Dif-ferences between those adopted at older as opposed toyounger ages seemed to relate to overall connectivity andedge strength. There were fewer but stronger connectionsbetween the nodes among those who were adopted at anolder age, and the connections more clearly reflect theunderlying second-order domain structure.
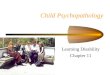
Figure 2 shows the centrality measures for all the domainnetworks. The networks of those adopted at an older vs. ayounger age differed in centrality on two items: accordingto all the measures of centrality, the anxiety/depressiondomain seemed to be the most central among younger but
not among the older adoptees, whereas aggressiveness wasthe most central item among children adopted at an olderage. On the other hand, thought problems were less pro-minent among those who were adopted at a younger age.These results indicate that among all the adoptees, anxiety/depression, social problems, and aggressiveness may be thesymptom domains that affected all the others, and thatsomatic symptoms had the least effect on the others.
We conducted the Network Comparison Test to examinethe differences in overall network structure between the agegroups, and could not reject the null hypothesis that thenetwork structure is invariant over subpopulations when theweighted network structures were compared (coefficient=0.192, p-value= 0.54). These results indicate that thedomain-network structure generalizes to different sub-populations quite well. However, it should be noted that thisdoes not rule out the existence of local differences given thelimited statistical power to detect them.
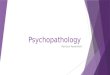
Finally, we considered how well the other nodes in thenetwork predicted the individual nodes (symptom domains),meaning that we computed the mean of the conditional dis-tribution of the node at hand with that of its neighbors.Because we were interested in how well a given node could bepredicted by all the other nodes in the network, we removedthe effects of the intercepts. The results of the predictabilityanalyses are presented in Fig. 3a, b and Table 2. The greenedges in Fig. 3a, b indicate positive relationships and the rededges indicate negative relationships. The circle of each colorindicates the proportion of explained variance for each node.As expected, there was a close relationship between theparameters of the network model and predictability: if a nodewas connected to only a few other nodes then the explainedvariance tended to be low, and the more edges that wereconnected to a node, the higher the predictability tended to be.Thus, the predictability of aggressiveness was relatively high(0.73), as was that of social problems (0.63) and attentionproblems (0.65). However, predictability was lower in thecase of second-order internalizing symptom domains such aswithdrawal (0.41), anxiousness (0.56), and somatic problems(0.28). There were some differences in symptom-domainpredictability between those who were adopted at older(Fig. 3b) vs. younger ages. In short, the predictability indomains representing externalizing symptoms (aggressivenessand rule breaking) was stronger among those who wereadopted at an older age, whereas internalizing symptoms suchas withdrawal and somatic symptoms were more predictableamong those adopted at a younger age (Table 2).
Discussion
We have demonstrated a state-of-the-art approach to model-ing the architecture of childhood psychiatric symptomology.
Table 1 The means and standard deviations of the CBCL symptomdomains (N= 784)
Mean SD
Anxiety/depressive symptoms 2.3 3.00
Withdrawal/depressive symptoms 1.5 2.12
Somatic complaints 1.6 2.00
Social problems 2.5 3.06
Thought problems 1.9 2.92
Attention problems 4.5 4.38
Rule-breaking behavior 2.6 4.01
Aggressive behavior 6.1 6.60
N 784
2164 Journal of Child and Family Studies (2018) 27:2161–2170

The network structure of international adoptees reflected thepredetermined clusters of externalizing and internalizingsymptoms relatively well. The connections became moredistinct as the child grew older, which is consistent withearlier findings showing that symptoms become more clearlydomain-specific at older ages (Dedrick et al. 2008). Externa-lizing symptoms, such as aggressive behavior, were posi-tioned centrally in the networks according to all the centralitymeasures, and their predictability was also high. These results
indicate that symptoms related to the aggressiveness domainpotentially affect all the other symptoms and are potentially agood target for interventions. There were local network dif-ferences between those adopted at older and younger ages,indicating the centrality of aggressiveness among the formerand anxiousness among the latter. According to these results,it would be reasonable to take the age at the time of adoptioninto account when planning interventions for internationaladoptees.
Fig. 1 The network of emotional and behavioral problems in inter-national adoptees as measured by the CBCL in all (a), in those adoptedat a younger age and those adopted at an older age (b). The color and
thickness of an edge represent the size of the absolute polychoricpartial correlation between two nodes. The node colors correspond tothe three domains (color figure online)
Journal of Child and Family Studies (2018) 27:2161–2170 2165

A number of studies have indicated that internationallyadopted adolescents have more mental-health problems thantheir non-adopted age-mates, adopted adolescents havingmore externalizing problems in particular (Askeland et al.2017). It is essential to offer efficient and targeted (treat-ment) intervention and prevention strategies for this high-risk population already in childhood. Due to increasednumber of severe attachment problems (disorganizedattachment) among adopted children, most of the interven-tion studies among adopted children have focused onattachment and parental sensitivity. These attachment-basedinterventions are shown to increase attachment security andwell-being of the children (Wright et al. 2015). However,there are findings that severe attachment problems may belinked with concurrent or later behavioral problems andaggression (Zeanah et al. 2016) and it has increased theneed to expand the focus of treatment programs also onbehavioral problems. Our findings about the centrality ofaggressiveness give support on this. In their study using acommunity sample of adolescents Boschloo and others(Boschloo et al. 2016) showed that externalizing problemshad a lot of connections within the same domain and notparticular amount connections with other domains. Thus,the centrality of externalizing problems may be typical forinternational adoptees, but future studies with acase–control design where international adoptees and otherchildren can be efficiently compared are needed.
These results would have been difficult to detect withoutusing the Gaussian Graphical Model (GGM) to determine
the network structure for emotional and behavioral pro-blems. Every pairwise interaction is evaluated while con-trolling for all the other variables, after which the network isregularized by means of lasso penalization. Edges that sur-vive the resulting process are likely to represent real asso-ciations. We did not determine the nature or the direction ofthese associations. Some relationships between symptomdomains may reflect potential causal effects, whereas othersmay be potentially bidirectional. It is highly likely that beingaggressive leads to rule-breaking behavior, but not viceversa, whereas aggressive behavior may cause social pro-blems and social problems may also provoke aggressive-ness. A similar approach was adopted in a previous study inwhich the Youth Self Report was used on the item level totest the network structure of emotional and behavioral pro-blems among adolescents (Boschloo et al. 2016).According to the results, the network structure correspondedwith the structure that had previously been identified inprincipal component analyses (symptom domains) (Achen-bach and Dumenci 2001). Our findings offer further supportfor the same theoretical structure in showing that symptomdomains within the same second-order domain have moreand stronger connections than those in different second-order domains. However, as in the above-mentioned study(Boschloo et al. 2016), the network-structure analyses alsoyielded new information about the complex associationsbetween emotional and behavioral problems.
There are pros and cons in testing networks of symptomdomains rather than individual symptoms. It is implied in
Betweenness Closeness Strength
−1 0 1 2 −2 −1 0 1 2 −2 −1 0 1
aggressive
anxious
attention
rulebreaking
social
somatic
thought
withdrawn
typeAllOlderYounger
Fig. 2 Centrality measures of symptom domains in all, in those adopted at a younger age and in those adopted at an older age
2166 Journal of Child and Family Studies (2018) 27:2161–2170

some findings that potentially important information is lostwhen items are summed to establish scale scores. As Bos-chloo and others (2016) showed, for instance, depressive
symptoms that had strong connections with other symptomsin the network more strongly predicted the onset of severedepression than symptoms with few or weak connections.
a
b
Fig. 3 The Mixed Graphical Model estimated on the symptom networkin all adoptees (a), in those adopted at a younger age and thoseadopted at an older age (b). The green edges indicate positive
relationships and the red edges negative relationships. The blue ring inall the nodes shows the proportion of explained variance (color figureonline)
Journal of Child and Family Studies (2018) 27:2161–2170 2167

We, therefore, believe that both research and clinical practicecould benefit from an approach that specifically focuses onindividual problems and their unique role in the network.However, very few scales reflect this thinking, and someindividual items measuring individual symptoms are notmeant to have any other role than to increase the reliability ofthe given scale or subscale. Thus, some items may just addnoise in the network structure and the analyses may produceartificially complex results. It may nevertheless be reasonableto test the structure on the level of theoretically meaningfulmeasures, in this case on the symptom-domain level. At leastthese approaches are complementary, as suggested in theabove-mentioned study testing the network structure ofhealth-related quality of life (Kossakowski et al. 2016).
In any case, the network approach yields importantinformation about specific associations between symptomdomains. One advantage is its capacity to identify the mostimportant nodes in the structure. This type of informationmay facilitate the formation of hypotheses on the etiologicalmechanisms underlying the onset and course of psycho-pathology. Associating symptoms with other symptoms inthe network could help in targeting interventions to thosechildren at highest risk. Our centrality analyses revealed thatsymptoms of aggressiveness and anxiety were the mostprominent in all the network structures, particularly amongthose who were adopted at older and younger ages,respectively. There were no differences between the twogroups in overall network connectivity, however. Aggres-siveness, problems with social relations, attention problems,rule breaking and anxiety/depression were the symptomdomains that the other symptoms in the network predictedmost strongly. Factors not included in the network seemed topredict somatic symptoms and withdrawal, especially amongthose who were adopted at an older age. Thus, it seems thatinterventions targeted at counteracting aggressiveness
should focus on rule-breaking behavior and thought pro-blems. Interventions aimed at reducing anxiety should focuson withdrawn behavior, thought problems and social pro-blems, although there were clear differences between thosewho were adopted at older as opposed to younger ages.
The network structure in the older group clearly reflectedthe second-order domain structure, and the predictorsprobably also belonged to the same second-order domain.Thought problems seemed to be associated with anxiety inboth groups. The network structure of those who wereadopted at younger age did not reflect the second-orderdomain structure as clearly, and multiple symptom domainswere related. It is thus reasonable to assume that interven-tions should also focus on multiple or even all symptomdomains. A further implication is that the networks of thosewho were adopted at an older age may be more solid andmore difficult to change: according to our findings, most ofthe symptom domains of those in this group were wellexplained by the other symptoms domains in the network.Prolonged adverse experiences, or simply getting older,may affect this structuring process, and studies following upinternational adoptees are needed to assess the differences.Factors that were outside of the network clearly explainedmore of the symptom domains of those who were adoptedat a younger age, hence it would be easier to bring aboutchanges by changing the environment.
Limitations
A major limitation of this study is the lack of a real prognosticdesign, which prevented us from drawing any causal con-clusions or offering any interpretations related to the temporalorder of the associations between the symptom domains.CBCL is an established and widely used measure of child-hood psychopathology (Hawk and McCall 2010; Trillings-gaard et al. 2004; Verhulst and Versluis-den Bieman 1995).However, all the information in our study was reported by theparents, and more reliability would have been achieved hadwe used multiple informants. The CBCL scores we obtainedcould be considered relatively low compared to the results ofprevious cross-cultural studies (Viola et al. 2011), especiallygiven that we were focusing on a risk group. Thus, there maybe cultural differences in reporting symptoms. Our studyfocused exclusively on internationally adopted children.Comparisons with non-adopted children in future researchcould enhance understanding about the pathophysiology ofpsychiatric symptoms in adoptees. However, even if thelevels differ, the associations between the various constructsmay not, hence the CBCL may well be a good measure ofbehavioral problems in Finland and elsewhere.
To conclude, the network structure of emotional andbehavioral problems supported the second-order domainstructure of the CBCL. Furthermore, the network analyses
Table 2 The variance explained of each individual symptom domainin all the adoptees, those who were adopted as older children and thosewho were adopted as younger children
Symptom domain All Adopted asolder
Adopted asyounger
(N= 778) (N= 385) (N= 392)
Anxiety/depressivesymptoms
0.56 0.54 0.56
Withdrawal/depressivesymptoms
0.41 0.29 0.51
Somatic complaints 0.28 0.26 0.32
Social problems 0.63 0.62 0.62
Thought problems 0.53 0.58 0.48
Attention problems 0.65 0.66 0.58
Rule-breaking behavior 0.58 0.59 0.48
Aggressive behavior 0.73 0.75 0.67
2168 Journal of Child and Family Studies (2018) 27:2161–2170

gave potentially important information about the uniquerole of individual symptom domains and their complexassociations, both within and outside the second-orderdomain. Perceiving emotional and behavioral problems ascomplex networks may help clinicians to shape theirthinking about the various mechanisms and treatment stra-tegies. The differences between the age groups also impliesthe need for treatment strategies focusing more on thosewho were adopted at an older age.
Acknowledgements This study was funded by The Foundation forPediatric Research in Finland, and EVO Grants from Turku UniversityHospital and the Academy of Finland. We thank the children andfamilies who participated in the study and the Finnish adoptionorganizations Save the Children Finland and Interpedia, and the city ofHelsinki.
Author Contributions M.E.: designed and executed the study, ana-lyzed the data, and wrote the paper. L.P.-R.: collaborated with thedesign and writing of the study. C.H., H.R., and H.L.: collaboratedwith the design and writing of the study.
Funding This study was funded by The Foundation for PediatricResearch in Finland, and EVO Grants from Turku University Hospitaland the Academy of Finland.
Compliance with Ethical Standards
Conflict of Interest The authors declare that they have no conflict ofinterest.
Ethical Approval The Ethics Review Committee of the Hospital Dis-trict of South-West Finland approved this study.
Informed Consent The participating children and their parents gavetheir informed written consent for their participation.
References
Achenbach, T.M., & Dumenci, L. (2001). Advances in empiricallybased assessment: revised cross-informant syndromes andnew DSM-oriented scales for the CBCL, YSR, and TRF: com-ment on Lengua, Sadowksi, Friedrich, and Fischer (2001).Journal of Consulting and Clinical Psychology, 69(4),699–702.
Achenbach, T.M., McConaughy, S.H., & Howell, C.T. (1987). Child/adolescent behavioral and emotional problems: Implications ofcross-informant correlations for situational specificity. Psycholo-gical Bulletin, 101, 213–232.
Achenbach, T.M., & Rescorla, L.A. (2001). Manual of the ASEBAschool_age forms & profiles. Burlington: University of Vermont,Research Center for Children, Youth & Families.
Askeland, K.G., Hysing, M., La Greca, A.M., Aaro, L.E., Tell, G.S., &Sivertsen, B. (2017). Mental Health in Internationally AdoptedAdolescents: A Meta-Analysis. Journal of American Academy ofChild and Adolescence Psychiatry, 56(3), 203–213. https://doi.org/10.1016/j.jaac.2016.12.009. e201.
Barrat, A., Barthelemy, M., Pastor-Satorras, R., & Vespignani, A.(2004). The architecture of complex weighted networks. Pro-ceedings National Academy of Science United States A, 101(11),3747–3752. https://doi.org/10.1073/pnas.0400087101.
Beard, C., Millner, A.J., Forgeard, M.J., Fried, E.I., Hsu, K.J.,Treadway, M.T., & Bjorgvinsson, T. (2016). Network analysis ofdepression and anxiety symptom relationships in a psychiatricsample. Psychological Medicine, 46(16), 3359–3369. https://doi.org/10.1017/S0033291716002300.
Beckett, C., Bredenkamp, D., Castle, J., Groothues, C., O’Connor, T.G., & Rutter, M., Romanian Adoptees Study, T. (2002). Behaviorpatterns associated with institutional deprivation: a study ofchildren adopted from Romania. Journal of Developmental andBehavioral Pediatrics, 23(5), 297–303.
Borsboom, D. (2017). A network theory of mental disorders. WorldPsychiatry, 16, 5–13.
Borsboom, D., & Cramer, A.O. (2013). Network analysis: an inte-grative approach to the structure of psychopathology. AnnualReview of Clinical Psychology, 9, 91–121. https://doi.org/10.1146/annurev-clinpsy-050212-185608.
Boschloo, L., Schoevers, R.A., van Borkulo, C.D., Borsboom, D., &Oldehinkel, A.J. (2016). The network structure of psycho-pathology in a community sample of preadolescents. Journal ofAbnormal Psychology, 125(4), 599–606. https://doi.org/10.1037/abn0000150.
Boschloo, L., van Borkulo, C.D., Borsboom, D., & Schoevers, R.A.(2016). A Prospective study on how symptoms in a networkpredict the onset of depression. Psychotherapy and Psychoso-matics, 85(3), 183–184. https://doi.org/10.1159/000442001.
Boschloo, L., van Borkulo, C.D., Rhemtulla, M., Keyes, K.M.,Borsboom, D., & Schoevers, R.A. (2015). The Network structureof symptoms of the diagnostic and statistical manual of mentaldisorders. PLoS ONE, 10(9), e0137621 https://doi.org/10.1371/journal.pone.0137621.
Bringmann, L.F., Lemmens, L.H., Huibers, M.J., Borsboom, D., &Tuerlinckx, F. (2015). Revealing the dynamic network structureof the Beck Depression Inventory-II. Psychological Medicine, 45(4), 747–757. https://doi.org/10.1017/S0033291714001809.
Chen, J., & Chen, Z. (2008). Extended Bayesian information criteriafor model selection with large model spaces. Biometrika, 95,759–771.
Constantini, G., Epskamp, S., Borsboom, D., Perugini, M., Möttus, R.,Wldorp, L., & Cramer, A.O. (2015). State of the aRt personalityresearch: A tutorial on network analysis of personality data in R.Journal of Research in Personality, 54, 13–29.
Cramer, A.O., van Borkulo, C.D., Giltay, E.J., van der Maas, H.L.,Kendler, K.S., Scheffer, M., & Borsboom, D. (2016). Majordepression as a complex dynamic system. PLoS ONE, 11(12),e0167490 https://doi.org/10.1371/journal.pone.0167490.
Cramer, A.O., Waldorp, L.J., van der Maas, H.L., & Borsboom, D.(2010). Comorbidity: a network perspective. Behavioral BrainSciences, 33(2-3), 137–150. https://doi.org/10.1017/S0140525X09991567.
Dedrick, R.F., Tan, T.X., & Marfo, K. (2008). Factor structure of theChild Behavior Checklist/6-18 in a sample of girls adopted fromChina. Psychological Assessment, 20(1), 70–75. https://doi.org/10.1037/1040-3590.20.1.70.
Elovainio, M., Raaska, H., Sinkkonen, J., Makipaa, S., & Lapinleimu,H. (2015). Associations between attachment-related symptomsand later psychological problems among international adoptees:results from the FinAdo study. Scand Journal of Psychology, 56(1), 53–61. https://doi.org/10.1111/sjop.12174.
Epskamp, S. (2015). bootnet: Bootstrap methods for various networkestimation routines. R-package. Repository CRAN. https://www.r-project.org.
Epskamp, S., Cramer, A.O., Waldorp, L.J., Schmittmann, V., &Borsboom, D. (2012). qgraph: network visualizations of rela-tionships in psychometric data. Journal of Statistical Softwares,12, 1–18.
Journal of Child and Family Studies (2018) 27:2161–2170 2169

Fensbo, C. (2004). Mental and behavioural outcome of inter-ethnicadoptees: a review of the literature. European Child and Ado-lescence Psychiatry, 13(2), 55–63. https://doi.org/10.1007/s00787-004-0358-2.
Frewen, P.A., Schmittmann, V.D., Bringmann, L.F., & Borsboom, D.(2013). Perceived causal relations between anxiety, posttraumaticstress and depression: extension to moderation, mediation, andnetwork analysis. European Journal of Psychotraumatology, 4.https://doi.org/10.3402/ejpt.v4i0.20656
Fried, E.I., Bockting, C., Arjadi, R., Borsboom, D., Amshoff, M.,Cramer, A.O., & Stroebe, M. (2015). From loss to loneliness: Therelationship between bereavement and depressive symptoms.Journal of Abnormal Psychology, 124(2), 256–265. https://doi.org/10.1037/abn0000028.
Fried, E.I., van Borkulo, C.D., Cramer, A.O., Boschloo, L., Schoevers,R.A., & Borsboom, D. (2017). Mental disorders as networks ofproblems: a review of recent insights. Social Psychiatry andPsychiatric Epidemiology, 52(1), 1–10. https://doi.org/10.1007/s00127-016-1319-z.
Haslbeck, J. (2016). mgm:Estimating Time-Varying MixedGraphicalModels. R-package. Repository CRAN. https://www.r-project.org.
Hawk, B., & McCall, R.B. (2010). CBCL behavior problems of post-institutionalized international adoptees. Clinical Child andFamily Psychology Review, 13(2), 199–211. https://doi.org/10.1007/s10567-010-0068-x.
Isvoranu, A.M., Borsboom, D., van Os, J., & Guloksuz, S. (2016). Anetwork approach to environmental impact in psychotic disorder:Brief theoretical framework. Schizophrenia Bulletin, 42(4),870–873. https://doi.org/10.1093/schbul/sbw049.
Isvoranu, A.M., van Borkulo, C.D., Boyette, L.L., Wigman, J.T.,Vinkers, C.H., Borsboom, D., & Group, I. (2017). A networkapproach to psychosis: pathways between childhood trauma andpsychotic symptoms. Schizophrenia Bulletin, 43(1), 187–196.https://doi.org/10.1093/schbul/sbw055.
Juffer, F., & van Ijzendoorn, M.H. (2005). Behavior problems andmental health referrals of international adoptees: a meta-analysis.JAMA, 293(20), 2501–2515. https://doi.org/10.1001/jama.293.20.2501.
Kossakowski, J.J., Epskamp, S., Kieffer, J.M., van Borkulo, C.D.,Rhemtulla, M., & Borsboom, D. (2016). The application of anetwork approach to Health-Related Quality of Life (HRQoL):introducing a new method for assessing HRQoL in healthy adultsand cancer patients. Quality of Life Research, 25(4), 781–792.https://doi.org/10.1007/s11136-015-1127-z.
Merz, E.C., & McCall, R.B. (2010). Behavior problems in childrenadopted from psychosocially depriving institutions. Journal ofAbnormal Child Psychology, 38(4), 459–470. https://doi.org/10.1007/s10802-009-9383-4.
O’Connor, T.G., Caspi, A., Defries, J.C., & Plomin, R. (2003).Genotype-environment interaction in children’s adjustment toparental separation. Journal of Child Psychology and Psychiatry,44(6), 849–856.
Opsahl, T., Agneessens, F., & Skvoretz, J. (2010). Node centrality inweighted networks: Generalizing degree and shortest paths.Social Networks, 32, 245–251.
Raaska, H., Elovainio, M., Sinkkonen, J., Matomaki, J., Makipaa, S.,& Lapinleimu, H. (2012). Internationally adopted children inFinland: parental evaluations of symptoms of reactive attachment
disorder and learning difficulties - FINADO study. Child Careand Health Development, 38(5), 697–705. https://doi.org/10.1111/j.1365-2214.2011.01289.x.
Rhemtulla, M., Fried, E.I., Aggen, S.H., Tuerlinckx, F., Kendler, K.S.,& Borsboom, D. (2016). Network analysis of substance abuseand dependence symptoms. Drug and Alcohol Dependence, 161,230–237. https://doi.org/10.1016/j.drugalcdep.2016.02.005.
Rutter, M., Pickles, A., Murray, R., & Eaves, L. (2001). Testinghypotheses on specific environmental causal effects on behavior.Psychological Bulletin, 127(3), 291–324.
Tibshirani, R. (1996). Regression shrinkage and selection via the lasso.Journal of Royal Statistical Society, B58, 267–288.
Trillingsgaard, A., Damm, D., Sommer, S., Jepsen, J.R., Ostergaard,O., Frydenberg, M., & Thomsen, P.H. (2004). Developmentalprofiles on the basis of the FTF (Five to Fifteen) questionnaire-clinical validity and utility of the FTF in a child psychiatricsample. European Child and Adolescence Psychiatry, 13(Suppl3), 39–63. https://doi.org/10.1007/s00787-004-3006-y.
Van Borkulo, C. (2015). Network comparison test:permutation-basedtest of differences in strength of networks. https://github.com/cvborkulo/NetworkComparisonTest.R-package
van Borkulo, C., Borsboom, D., Epskamp, S., Blanken, T.F., Bos-chloo, L., Schoevers, R.A., & Waldorp, L.J. (2014). A newmethod for constructing networks from binary data. ScientificReports, 4, 5918 https://doi.org/10.1038/srep05918.
van Borkulo, C., Boschloo, L., & Borsboom, D., et al. (2015a).Association of symptom network structure with the course ofdepression. JAMA Psychiatry, 72, 1219–1226.
van Borkulo, C., Boschloo, L., Borsboom, D., Penninx, B., Waldorp,L., & Schoevers, R.A. (2015b). Association of symptom networkstructure with the course of depression JAMA. Psychiatry, 72(12), 1219–1224.
van Ijzendoorn, M.H., Juffer, F., & Poelhuis, C.W. (2005). Adoptionand cognitive development: a meta-analytic comparison ofadopted and nonadopted children’s IQ and school performance.Psychological Bulletin, 131(2), 301–316. https://doi.org/10.1037/0033-2909.131.2.301.
Verhulst, F.C., & Versluis-den Bieman, H.J. (1995). Developmentalcourse of problem behaviors in adolescent adoptees. Journal ofAmerican Academy of Child and Adolescence Psychiatry, 34(2),151–159. doi:S0890-8567(09)63753-9 [pii]10.1097/00004583-199502000-00010.
Viola, L., Garrido, G., & Rescoria, L. (2011). Testing multiculturalrobusteness of the child behavior checklist in a national epide-miological sample in Uruguai. Journal Abnormal Child Psy-chology, 39, 897–908.
Wright, B., Barry, M., Hughes, E., Trepel, D., Ali, S., Allgar, V., &Gilbody, S. (2015). Clinical effectiveness and cost-effectivenessof parenting interventions for children with severe attachmentproblems: a systematic review and meta-analysis. Health Tech-nology Assessment,, 19(52), vii–xxviii. https://doi.org/10.3310/hta19520. 1-347.
Zeanah, C.H., Chesher, T., & Boris, N.W. (2016). Practice parameterfor the assessment and treatment of children and adolescents withreactive attachment disorder and disinhibited social engagementdisorder. Journal of American Academy of Child and Adoles-cence Psychiatry, 55(11), 990–1003. https://doi.org/10.1016/j.jaac.2016.08.004.
2170 Journal of Child and Family Studies (2018) 27:2161–2170