Embed Size (px)
Citation preview

NI
TA[
Ch
J
A
1A
PEER-REVIEW REPORTS
The Nervus Intermedius: A Review of Its Anatomy, Function, Pathology, and Rolein Neurosurgery
R. Shane Tubbs1, Dominik T. Steck1, Martin M. Mortazavi1, Aaron A. Cohen-Gadol2A
Tdwtlngrdpotonpemts
wvnmrmg
cnttclmgplHp
PAIN
INTRODUCTION
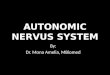
The nervus intermedius was first identifiedin 1563, and it was Heinrich August Wris-berg who named it the “portio media intercomunicantem faciei et nervum auditorium” in1777 (1). This nerve (Figure 1), often re-ferred to as the Wrisberg nerve, carriesparasympathetic fibers to the lacrimal andnasopalatine glands and transmits sensoryinformation from the tongue and variousskin areas of the nose and concha of theear (8, 20, 22, 28). A cutaneous brancharises near the origin of the chorda tym-pani nerve and joins with the auricularbranch of the vagus nerve to supply theexternal auditory canal and concha of theexternal ear. It is this innervation that al-lows herpetic vesicles to be identified inthe ear with viral infection of the genicu-late ganglion, the so-called Ramsay-Hunt
Key words� Anterior inferior cerebellar artery� Cranial nerve� Facial nerve� Intermediate nerve� Microvascular decompression� Neuralgia� Nervus intermedius� Vestibulocochlear nerve� Wrisberg nerve
Abbreviation and AcronymMRI: Magnetic resonance imaging
From 1Pediatric Neurosurgery, Children’sHospital, Birmingham, Alabama; and
2Goodman Campbell Brain and Spine, Department ofeurological Surgery, Indiana University, Indianapolis,
ndiana, USA
o whom correspondence should be addressed:aron A. Cohen-Gadol, M.D., M.Sc.
E-mail: [email protected]]
itation: World Neurosurg. (2013) 79, 5/6:763-767.ttp://dx.doi.org/10.1016/j.wneu.2012.03.023
ournal homepage: www.WORLDNEUROSURGERY.org
vailable online: www.sciencedirect.com
878-8750/$ - see front matter © 2013 Elsevier Inc.ll rights reserved.
syndrome (20). (
WORLD NEUROSURGERY 79 [5/6]: 763-7
NATOMY AND FUNCTIONS
he nervus intermedius consists of fiberserived from the superior salivary nucleushose stimulation results in secretion of
he lacrimal and submandibular and sub-ingual glands (4). Traveling along thiserve are sensory fibers derived from theustatory receptors destined for the supe-ior pole of the solitary nucleus in the me-ulla and fibers for cutaneous sensation ofarts of the ear destined for the dorsal partf the trigeminal tract (31). The course of
he nervus intermedius and the motor rootf the facial nerve can be divided into cister-al, meatal, labyrinthal, and extracranialarts. Rhoton et al. (20) found that, on av-rage, the length of all 3 segments was 22m. The nerve takes its name from its in-
ermediate position between the facial anduperior portion of the vestibular nerves
� BACKGROUND: Geniculate neuralgtating pathology. Unfortunately, a thoroclinical anatomy, function, and patholothe nervus intermedius, is lacking in taimed to further elucidate the diagnotreatment based on a review of the li
� METHODS: Using standard searchgermane reports regarding the nervussummary of this body of literature is p
� RESULTS: Since 1968, only approximpublished regarding the nervus intereports and in reference to geniculateliterature.
� CONCLUSIONS: Neuralgia involvingwhen present, can be life altering.effective as a treatment. Along its cistdistinguish from the facial nerve. Blong-term pain control can be seendecompression, but no prospective stsary to shed light on the efficacy ofneuralgia.
20). The average length of adherence, n
67, MAY/JUNE 2013 ww
hich is often crescent shaped, of the ner-us intermedius to the vestibulocochlearerve has been found to be approximately 8m (11, 20). Inside the meatus, the motor
oot of the facial nerve and the nervus inter-edius are usually bound together as a sin-
le structure.In the temporal bone, the facial nerve
ontinues its course through the facial ca-al. The nerve is supplied from branches of
he middle meningeal, maxillary, and pos-erior auricular arteries. Between the co-hlea and the semicircular canals, it runsaterally above the vestibule. Reaching the
edial wall of the epitympanic recess, theeniculum (external genu) is formed. Thisoint, above the base of the cochlea, is the
ocation of the geniculate ganglion (14).ere the nerve gives rise to the greateretrosal nerve (greater superficial petrosal
lthough uncommon, can be a debili-review of this pain syndrome and the
f its most commonly associated nerve,terature. Therefore, the present studyf this pain syndrome and its surgicalure.
nes, the literature was evaluated forrmedius and associated pathology. Anted.
y 50 peer-reviewed reports have beenius. Most of these are single-caseralgia. No report was a review of the
nervus intermedius is uncommon, butcrovascular decompression may bel course, the nerve may be difficult to
on case reports and small series,r nerve sectioning or microvascular
exist. Such studies are now neces-ical treatment of nervus intermedius
ia, aughgy ohe lisis oterat
engiinterese
atelrmedneu
theMi
ernaasedafte
udiessurg
erve), which carries parasympathetic fi-
w.WORLDNEUROSURGERY.org 763

dastaaurortniettmm
wminwcm
GS
AnntsT
PEER-REVIEW REPORTS
R. SHANE TUBBS ET AL. THE NERVUS INTERMEDIUS
PAIN
PAIN
bers supplying the lacrimal, nasal, and pal-atine glands (22, 29). The tympanic cavityand the nerve are separated only by a thinlayer of bone and this layer might be absent,so in some individuals, there is only the mu-cosa between the nerve and the cavity of themiddle ear, and therefore the nerve mightbe easily affected by infections of the middleear. Possible anomalies include the nervelying in the wall of the mastoid antrum withthe nerve emerging from the mastoid pro-cess and division of the nerve within thefacial canal (branches leave the temporalbone through different foramina in thiscase). An anterolateral turn toward the pa-rotid gland describes the extracranialcourse of the facial nerve after it emergesfrom the stylomastoid foramen (14, 31).
Rhoton et al. (20) and Oh et al. (16) foundup to 4 to 5 roots that made up the nervusintermedius, although a single root was themost common. Additionally, Rhoton et al.(20) stated that in approximately 20% ofcases, it is impossible to identify the nervusintermedius along its intracisternal coursebecause it is intimately attached to the ves-tibular part of the vestibulocochlear nerveand does not separate from it until the inter-nal acoustic meatus.
Preganglionic fibers from the superiorsalivatory nucleus in the pons travel to thepterygopalatine ganglion in the greaterpetrosal nerve, and the postganglionic fi-bers innervate the lacrimal gland as well asthe glands of the nose and palate. Pregan-glionic parasympathetic fibers from thepons travel to the submandibular ganglionin the chorda tympani and innervate thesubmandibular, the sublingual, and the ac-
Figure 1. Cadaveric dissection of the rightporus acousticus noting the facial, nervusintermedius, and vestibulocochlear nerves.
cessory salivary glands.
764 www.SCIENCEDIRECT.com
Section of the nervus intermedius mayecrease the cutaneous sensitivity in therea around the concha of the external ear,ensation from anterior nasopharynx andympanic membrane, part of the externaluditory canal, and the area behind the earnd over the mastoid process (11, 22). Stim-lation of the nervus intermedius can causeeferred pain to the ear, and the projectionf fibers from this nerve might also explaineferred pain to the face after irritation ofhe nervus intermedius (20). Therefore, theervus intermedius plays an important role
n the surgical treatment of neuralgia of thexternal auditory canal (see later) (20). In-erestingly, Ashram et al. (6) described elec-romyography activity in the orbicularis oris
uscle after stimulation of the nervus inter-edius.Burmeister et al. (8) conducted a study in
hich they tried to identify the nervus inter-edius with 3-T magnetic resonance imag-
ng (MRI). Their conclusion was that theervus intermedius can be depicted reliablyith MRI, which might be helpful, espe-
ially in the diagnosis of the source of tu-ors in this region.
ENICULATE NEURALGIA AND ITSURGICAL TREATMENT
lthough nervus intermedius (geniculate)euralgia is rare and difficult to diagnose, aumber of different surgical treatment op-
ions have evolved, leading to more confu-ion about the most appropriate approach.he International Headache Society (10) de-
fines nervus intermedius neuralgia as inter-mittent episodes of pain located deep in theear that last for seconds or minutes; theposterior wall of the auditory canal may be atrigger zone. The pain can be accompaniedby disorders of lacrimation, salivation, andtaste (10). In 1909, Clark and Taylor (9) werethe first to report success in treating facialpain with resection of the geniculate gan-glion. Of note, some have advocated tran-section of the nervus intermedius forchronic cluster headaches (15, 22). In fact,Rowed (22) reported a 75% success rate us-ing this technique in such patients. Paren-thetically, this investigator found that hear-ing impairment was the most frequentserious complication after sectioning of thenervus intermedius (22).
Sachs (24) followed up four patients
after section of the nervus intermedius,WORLD NEUROSURGERY, http://d
two of them for more than 10 years. Thefirst patient, a 43-year-old woman, suf-fered from attacks of right-sided face andhead pain for 7 years that later becameassociated with severe pain in the rightear. During surgery and under local anes-thesia, the facial, vestibulocochlear, andglossopharyngeal nerves, including thenervus intermedius, were explored; stim-ulation of the nervus intermedius resultedin pain in the ear and right face. The samesymptoms could be produced when stim-ulating the vestibulocochlear nerve. Thefacial (inadvertently) and vestibuloco-chlear nerves and the nervus intermediuswere sectioned. No recurrence was notedat 15 years of follow up. The second pa-tient, a 56-year-old man with attacks ofleft-sided facial pain that were associatedwith ipsilateral lacrimation and nasalcongestion, underwent left greater petro-sal neurectomy, which brought relief for 3years. A third patient, a 65-year-old manwho suffered from attacks of pain on theleft side of the face without lacrimation,nasal congestion, or ear pain, also under-went sectioning of the nervus interme-dius. Lacrimation was lost, but no loss oftaste occurred, and the patient becamepain-free postoperatively. The fourth pa-tient, a 36-year-old man, complained ofdaily headaches for 6 to 8 weeks per year.The pain was in the right cheek, eye, fore-head, temple, and behind the right ear. Inthis case, a large internal auditory arterywas seen between the facial and vestibu-locochlear nerves. Sectioning of the ner-vus intermedius caused decrease of lacri-mation and loss of taste on the anteriortwo-thirds of the tongue and immediaterelief of pain (24). There is some variationin the distribution of pain among theabove patients (some suffering from fa-cial pain) making it difficult to assess whoreliably harbored geniculate neuralgia.
Lovely and Janetta (13) reported 14 casesof patients with the primary complaint ofdeep inner ear pain, often in combinationwith atypical facial pain or throat pain. Vas-cular compression of the trigeminal, glos-sopharyngeal, or vagus nerve or the nervusintermedius was observed in almost everycase and was assumed to be a cause of theprimary or secondary complaints in thesepatients (Figures 2 and 3A).
These cases emphasize the importance
of the nervus intermedius in otalgia. Fourx.doi.org/10.1016/j.wneu.2012.03.023

gicwrgct(tlPag
ytmtNtiagrihic
siaptDeftpocatf(cncitcrha
PEER-REVIEW REPORTS
R. SHANE TUBBS ET AL. THE NERVUS INTERMEDIUS
PAIN
PAIN
patients had to undergo multiple proce-dures, and in two of them, lasting relief wasnot obtained before the nervus intermediuswas sectioned. The sectioning of the nervusintermedius was well tolerated in all pa-tients, and no neurologic deficits or altera-tions in taste or lacrimation were reported(13). The efficacy of pain relief through mi-crovascular decompression or sectioning ofthe nervus intermedius cannot be reliablyestablished by this study. Some patientssuffered from atypical face pain as well, andtherefore, a heterogeneous group of pa-tients was analyzed.
Figure 3. Intraoperative images of the surgical apwith geniculate neuralgia. Note the surrounding
Figure 2. Schematic drawing of the surgicalapproach to the nervus intermedius formicrovascular decompression or sectioning.
pulled away (C) from the nerve and held in place with
WORLD NEUROSURGERY 79 [5/6]: 763-7
Rupa et al. (23) reported 14 patients witheniculate neuralgia who underwent nervus
ntermedius sectioning. This cohort was in-luded among 18 cases of primary otalgiaith additional procedures, including
esection of the geniculate ganglion,lossopharyngeal, vagus, tympanic, andhorda tympani nerves. Among all pa-ients, pain relief was achieved in 72.2%23). Reported side effects of nervus in-ermedius sectioning included decreasedacrimation, salivation, and taste (23).ulec (18) has also reported good resultsfter nervus intermedius sectioning foreniculate neuralgia.
Sakas et al. (26) reported a case of a 52-ear-old woman with episodes of pain ofhe right auditory canal, pinna and retro-
astoid area, as well as right-sided tinni-us, hearing loss, imbalance, and vertigo.
euroimaging demonstrated a tortuous an-erior inferior cerebellar artery compress-ng the facial and vestibulocochlear nervest the internal auditory meatus. During sur-ery, the artery was mobilized and sepa-ated from the nerves. All symptoms,ncluding pain, tinnitus, vertigo, andearing loss, improved during the follow-
ng months (26). Belloti et al. (7) dis-ussed a 65-year-old patient who pre-
h (A) to the nervus intermedius in a patients (B). An offending vessel was identified and
a Teflon implant (D).67, MAY/JUNE 2013 ww
ented with both trigeminal and nervusntermedius neuralgia (touching the nosend the external auditory meatus causedain in the second/third divisions of the
rigeminal nerve and ear, respectively).uring surgery, the anterior inferior cer-
bellar artery was found adherent to theacial and vestibulocochlear nerves andhe root of the trigeminal nerve was com-ressed by three large veins and a branchf the superior cerebellar artery. After de-ompressing the nerves from the vesselsnd rhizotomy of the sensory root of therigeminal nerve, the patient became painree (7). Saers et al. (25), Younes et al.30), and Özer et al. (17) reported similarases of suspected nervus intermediuseuralgia in which the anterior inferiorerebellar artery compressed the nervusntermedius and mobilization of the ar-ery cured the pain. Such neurovascularompression led to demyelination at theoot entry zone (25). Interestingly, someave questioned vascular compression ascause of geniculate neuralgia (5).Alfieri et al. (2) found that the mean dis-
tance laterally from the brain stem of cen-tral myelin for the nervus intermedius was0.5 mm on the medial side of the nerve and0.33 on its lateral side. The Obersteiner-Redlich zone or glial-Schwann cell junctionfor the medial and lateral sides of the nervewas 0.279 mm and 0.33 mm, respectively(2). With these data, it appears that the ner-vus intermedius is closer to the brain stemcompared with other cranial nerves (2).
Riederer et al. (19) described an inter-esting case of familial geniculate neural-gia and concluded that an X-linked domi-nant inheritance was most likely the causeof the occurrence of nervus intermediusneuralgia in the family. In some cases, agenetic susceptibility for cranial neural-gias might be present (32), and one theorysuggested a mutation of the Nav 1.7 so-dium channel with resultant nerve hyper-excitability (3).
PERSPECTIVES ON SURGICALTREATMENT OF GENICULATENEURALGIA
The previously discussed studies regard-ing the surgical treatment of geniculateneuralgia suffer from similar limitations.The studied patients suffered from heter-
proacnerve
ogeneous pain syndromes that included
w.WORLDNEUROSURGERY.org 765

acmowsc
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
PEER-REVIEW REPORTS
R. SHANE TUBBS ET AL. THE NERVUS INTERMEDIUS
PAIN
PAIN
poorly described face pain. The numberof patients mentioned in the individualstudies and the follow-up durations arealso limited.
The efficacy of exploratory surgery withtransection of nervus intermedius for long-term relief of geniculate neuralgia remainsunconvincing. Therefore, patient selectionremains especially important, and the riskof vestibulocochlear nerve dysfunction andresultant persistent dizziness and balancedysfunction should be carefully consideredduring manipulation of the VII/VIII com-plex. Glossopharyngeal neuralgia with aprimarily otitic component may mimicgeniculate neuralgia; this overlap in presen-tation should be considered during explora-tion of the posterior fossa cranial nervesbecause the glossopharyngeal nerve may beinvolved in vascular compression.
TUMORS INVOLVING THENERVUS INTERMEDIUS
Scheller et al. (27) reported a possible caseof case of nervus intermedius schwannomathat presented with progressive left-sidedhearing loss and dizziness. Rizer et al. (21)reported a 38-year-old man with left-sidedhearing loss and tinnitus. MRI demon-strated a lesion in the lateral end of the leftinternal auditory canal. During surgery, atumor was found that attached only to partof the facial nerve and was removed withnervus intermedius sectioning. Kudo et al.(12) reported a patient who presented withleft hemifacial spasm. A small mass (laterfound to be a schwannoma) arising fromthe nervus intermedius, adhering to andcompressing the facial nerve, was found.The nervus intermedius was sectioned andthe patient was free of spasms after surgeryand at long-term follow-up.
CONCLUSIONS
Neuralgia involving the nervus intermediusis uncommon, but when present, it can belife altering. Microvascular decompressionmay be effective as a treatment. Along itscisternal course, the nerve may be difficultto distinguish from the facial nerve. Basedon case reports and small series, long-termpain control can be seen after nerve section-ing or microvascular decompression, but
no prospective studies exist. Such studies1
766 www.SCIENCEDIRECT.com
re now necessary to shed light on the effi-acy of surgical treatment of nervus inter-edius neuralgia. A thorough knowledge
f the anatomy of this nerve is necessaryhen treating patients presenting with
ymptoms due to pathology along itsourse.
REFERENCES
1. Alfieri A, Strauss C, Prell J, Peschke E: History of thenervus intermedius of Wrisberg. Ann Anat 192:139-144, 2010.
2. Alfieri A, Fleischhammer J, Strauss C, Peschke E:The central myelin-peripheral myelin transitionalzone of the nervus intermedius and its implicationsfor microsurgery in the cerebellopontine angle. ClinAnat 2011 Dec 20. [Epub ahead of print]
3. Alfieri A, Strauss C: Familial occipital neuralgia withsporadic nervus intermedius neuralgia (NIN). JHeadache Pain 12:657, 2011.
4. Alfieri A, Fleischhammer J, Prell J: The functions ofthe nervus intermedius. AJNR Am J Neuroradiol 32:E144; author reply E145, 2011.
5. Alfieri A, Strauss C: Microvascular decompressionmay be an effective treatment for nervus interme-dius neuralgia. J Laryngol Otol 125:765; author reply765, 2011.
6. Ashram YA, Jackler RK, Pitts LH, Yingling CD: In-traoperative electrophysiologic identification of thenervus intermedius. Otol Neurotol 26:274-279,2005.
7. Bellotti C, Medina M, Oliveri G, Ettorre F, BarraleS, Sturiale C, Melcarne A: Neuralgia of the inter-mediate nerve combined with trigeminal neural-gia: case report. Acta Neurochir (Wien) 91:142-143, 1988.
8. Burmeister HP, Baltzer PA, Dietzel M, Krumbein I,Bitter T, Schrott-Fischer A, Guntinas-Lichius O,Kaiser WA: Identification of the nervus intermediususing 3T MR imaging. AJNR Am J Neuroradiol 32:460-464, 2011.
9. Clark LP, Taylor AS: True tic douloureux of thesensory filaments of the facial nerve. I. Clinicalreport of a case in which cure was effected byphysiological extirpation of the geniculate gan-glion. I1. Report of surgical treatment. JAMA 53:2144-2146, 1909.
0. Headache Classification Committee of the Interna-tional Headache Society: Classification and diag-nostic criteria for headache disorders, cranial neu-ralgias and facial pain. Cephalalgia 8(Suppl 7):1-96,1988.
1. Jordan DR: The nervus intermedius. Arch Ophthal-mol 111:1691-1692, 1993.
2. Kudo A, Suzuki M, Kubo N, Kuroda K, Ogawa A,Iwasaki Y: Schwannoma arising from the intermedi-
WORLD NEUROSURGERY, http://d
ate nerve and manifesting as hemifacial spasm. Casereport. J Neurosurg 84:277-279, 1996.
3. Lovely TJ, Jannetta PJ: Surgical management ofgeniculate neuralgia. Am J Otol 18:512-517, 1997.
4. Monkhouse WS: The anatomy of the facial nerve.Ear Nose Throat J 69:677-683, 686-687, 1990.
5. Morgenlander JC, Wilkins RH: Surgical treatment ofcluster headache. J Neurosurg 72:866-871, 1990.
6. Oh CS, Chung IH, Lee KS, Tanaka S: Morphologicalstudy on the rootlets comprising the root of the inter-mediate nerve. Anat Sci Int 78:111-113, 2003.
7. Özer FD, Duransoy YK, Camlar M: Atypic geniculateneuralgia: atypic anatomic correlation of cranialnerve roots and AICA. Acta Neurochir (Wien) 151:1003-1004; discussion 1004, 2009.
8. Pulec JL: Geniculate neuralgia: long-term results ofsurgical treatment. Ear Nose Throat J 81:30-33,2002.
9. Riederer F, Sédor PS, Linnebank M, Ettlin DA: Fa-milial occipital and nervus intermedius neuralgia ina Swiss family. J Headache Pain 11:335-338, 2010.
0. Rhoton AL Jr, Kobayashi S, Hollinshead WH: Ner-vus intermedius. J Neurosurg 29:609-618, 1968.
1. Rizer FM, Guthikonda M, Lippy WH, Schuring AG:Simultaneous presentation of facial nerve neuromaand otosclerosis. Am J Otol 15:427-430, 1994.
2. Rowed DW: Chronic cluster headache managed bynervus intermedius section. Headache 30:401-406,1990.
3. Rupa V, Saunders RL, Weider DJ: Geniculate neural-gia: the surgical management of primary otalgia. JNeurosurg 75:505-511, 1991.
4. Sachs E Jr: The role of the nervus intermedius infacial neuralgia. Report of four cases with observa-tions on the pathways for taste, lacrimation, andpain in the face. J Neurosurg 28:54-60, 1968.
5. Saers SJ, Han KS, de Ru JA: Microvascular decom-pression may be an effective treatment for nervusintermedius neuralgia. J Laryngol Otol 12:1-3, 2011[Epub ahead of print]
6. Sakas DE, Panourias IG, Stranjalis G, StefanatouMP, Maratheftis N, Bontozoglou N: Paroxysmalotalgia due to compression of the intermediatenerve: a distinct syndrome of neurovascular conflictconfirmed by neuroimaging. Case report. J Neuro-surg 107:1228-1230, 2007.
7. Scheller C, Rachinger J, Prell J, Kornhuber M,Strauss C: Schwannoma of the intermediate nerve. JNeurosurg 109:144-148, 2008.
8. Smith JJ, Breathnach CS: Functions of the seventhcranial nerve. Ear Nose Throat J 69:688-691, 694-695, 1990.
9. Thomsen J, Borum P, Tos M, Zilstorff K: Nervusintermedius in acoustic neuromas: a critical evalua-tion of intermedius nerve testing, with special refer-
ence to the nasolacrimal reflex. Am J Otol 3:21-27,1981.x.doi.org/10.1016/j.wneu.2012.03.023

3
Ca
R
Ch
J
A
1A
as
PEER-REVIEW REPORTS
R. SHANE TUBBS ET AL. THE NERVUS INTERMEDIUS
LN
ER
VE
LN
ER
VE
30. Younes WM, Capelle HH, Krauss JK: Microvasculardecompression of the anterior inferior cerebellarartery for intermediate nerve neuralgia. StereotactFunct Neurosurg 88:193-195, 2010.
31. Walker HK: Cranial nerve VII: the facial nerve andtaste. In: Walker HK, Hall WD, Hurst JW, editors.Clinical Methods: The History, Physical, and Labora-
tory Examinations. 3rd edition. Boston: Butterworths,1990.cc
P. Sarat Chandra, Pankaj Kumar Singh, V
isting symptoms; however, the treatment
ovw
lpsantiSvt1wir
fsge
�
Ic
WORLD NEUROSURGERY 79 [5/6]: 767-7
2. Wang Y, Yu CY, Huang L, Riederer F, Ettlin D: Fa-milial neuralgia of occipital and intermedius nervesin a Chinese family. J Headache Pain 12:497-500,2011.
onflict of interest statement: The authors declare that therticle content was composed in the absence of any
ommercial or financial relationships that could beonstrued as a potential conflict of interest.inay Goyal, Avnish Kumar Chauhan, Nir
ation, resulting in better patient compli-
abss
atglsaobu
sis
72, MAY/JUNE 2013 ww
eceived 17 November 2011; accepted 29 March 2012
itation: World Neurosurg. (2013) 79, 5/6:763-767.ttp://dx.doi.org/10.1016/j.wneu.2012.03.023
ournal homepage: www.WORLDNEUROSURGERY.org
vailable online: www.sciencedirect.com
878-8750/$ - see front matter © 2013 Elsevier Inc.ll rights reserved.
PER
IPH
ER
APER
IPH
ER
A
Early versus Delayed Endoscopic Surgery for Carpal Tunnel Syndrome: ProspectiveRandomized Study
mal Thakkur, Manjari Tripathi
INTRODUCTION
Carpal tunnel syndrome (CTS) is the mostcommon nerve entrapment syndrome oc-curring in the upper extremity, with a prev-alence of up to 9% (18). Classic symptomsof CTS include pain, paresthesia (character-istically worse during the night, termed bra-chialgia paresthetica nocturna), and hypoesthe-sia in the hand. Weakness and atrophy ofthe abductor pollicis brevis (APB) and mus-cles innervated by the median nerve mayalso be observed. The characteristic prolon-gation of distal motor latency confirms thediagnosis (1, 25). Initially, a conservative
pproach to treatment is preferred for per-
Key words� Carpal tunnel release� Carpal tunnel syndrome� Endoscopic surgery� Flexor retinaculum
Abbreviations and AcronymsAPB: Abductor pollicis brevisCTS: Carpal tunnel syndromeEP: ElectrophysiologyICMR: Indian Council for Medical ResearchNSAIDs: Nonsteroidal antiinflammatory drugs
Department of Neurosurgery, All India Instituteof Medical Sciences, New Delhi, India
To whom correspondence should be addressed:Manjari Tripathi, D.M.[E-mail: [email protected]]
Citation: World Neurosurg. (2013) 79, 5/6:767-772.http://dx.doi.org/10.1016/j.wneu.2012.08.008
Journal homepage: www.WORLDNEUROSURGERY.org
Available online: www.sciencedirect.com
1878-8750/$ - see front matter © 2013 Elsevier Inc.All rights reserved.
f choice is surgical dissection of the trans-erse carpal ligament (flexor retinaculum)ith decompression of the nerve (16, 18).Open dissection of the transverse carpal
igament has been the standard procedureerformed for �50 years (5, 21). Endo-copic surgical techniques were developednd introduced to ameliorate the inconve-iences and adverse events of open dissec-
ion. Endoscopic carpal tunnel release wasntroduced by Okutsu et al. in 1987 (15).ubsequently, several other clinicians de-eloped endoscopic techniques for dissec-ion of the transverse carpal ligament (3,2-23). These techniques were introducedith the presumed advantage of being min-
mally invasive with decreased surgical du-
� OBJECTIVE: To compare the effecsurgery in patients with moderately s
� METHODS: The study included 10ormed before surgery excluded secoevere CTS (grade 3– 4) were randorading scale for CTS was used to asndoscopic carpal tunnel release usin
RESULTS: Following a course of cwas offered in two groups: early surgedelayed surgery as per the usual waitinmprovement in both groups was signiompared, improvement was better
confidence interval 6.35–9.12).
� CONCLUSIONS: On the basis ofproposed in patients with moderately
nce. Generally, most reviews state thatoth endoscopic and open techniques areafe and equally effective in relieving theymptoms of CTS.
The timing of surgery (early or delayed) islso important. Most patients who are rou-inely considered for surgery are usuallyiven a trial of conservative treatment, fol-
owed by surgery after 3– 6 months. Earliertudies have shown that both conservativend surgical treatments lead to improvedutcomes. However, the improvement haseen shown to be better in patients whonderwent surgery (20, 21).
Treatment for moderately severe (Blandcore 3– 4 [defined subsequently]) (25) CTSs controversial. Few studies favored both
f early versus delayed endoscopiccarpal tunnel syndrome (CTS).
tients with CTS. Investigations per-ry causes. Patients with moderatelyassigned. Bland’s neurophysiologicthe patients. Patients underwent anindigenously designed instrument.
rvative treatment, surgical treatment� 51; <1 week after diagnosis) and
t (n � 49; >6 months after diagnosis).t (P < 0.001). When both groups werehe early surgery group (P < 0.001;
study, early endoscopic surgery isre CTS.
ts oevere
0 pandamlysessg an
onsery (ng lis
ficanfor t
thisseve
urgery and conservative treatment. How-
w.WORLDNEUROSURGERY.org 767











![· investigated 1, 12, 13, 14]. Among the 14 human isozymes of carbonic ... Nervus thoracicus Nervus lumbalis Nervus sacralis Control Cornea Humor vitreus](https://img.pdfslide.us/doc/110x75/5c7eee8809d3f2a53f8beca7/-investigated-1-12-13-14-among-the-14-human-isozymes-of-carbonic-nervus.jpg)