Embed Size (px)
Citation preview
THE NEED for the
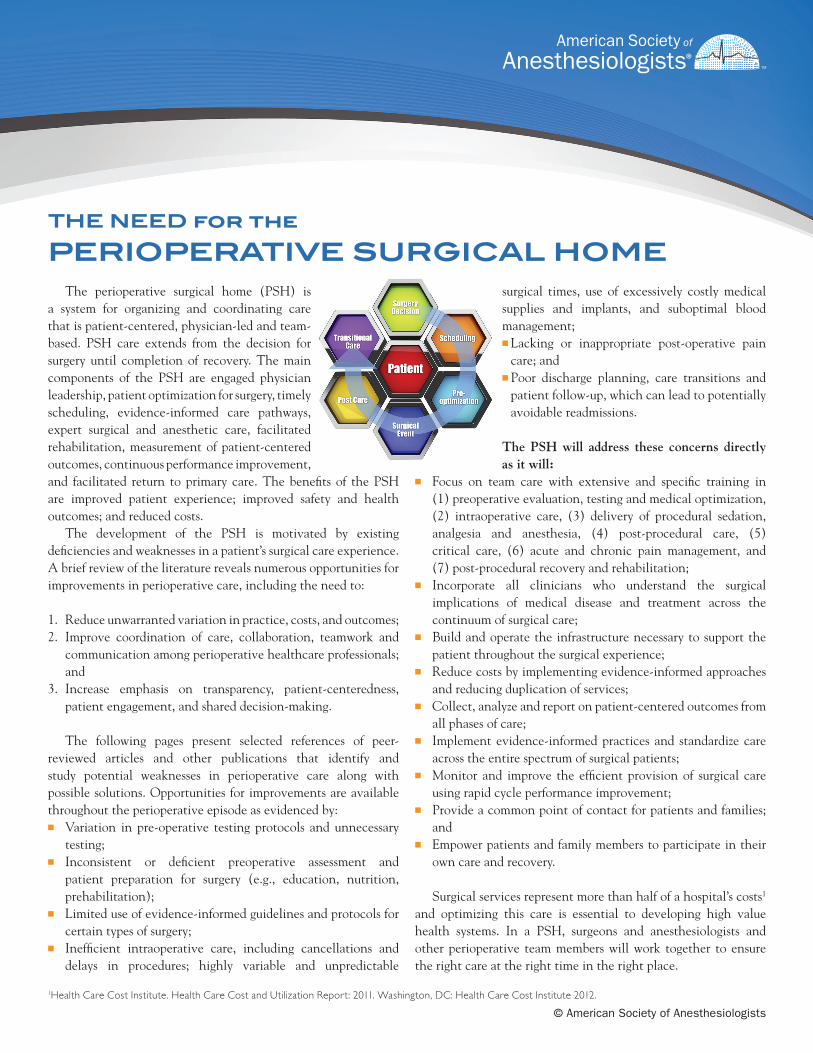
PERIOPERATIVE SURGICAL HOME The perioperative surgical home (PSH) is a system for organizing and coordinating care that is patient-centered, physician-led and team-based. PSH care extends from the decision for surgery until completion of recovery. The main components of the PSH are engaged physician leadership, patient optimization for surgery, timely scheduling, evidence-informed care pathways, expert surgical and anesthetic care, facilitated rehabilitation, measurement of patient-centered outcomes, continuous performance improvement, and facilitated return to primary care. The benefits of the PSH are improved patient experience; improved safety and health outcomes; and reduced costs. The development of the PSH is motivated by existing deficiencies and weaknesses in a patient’s surgical care experience. A brief review of the literature reveals numerous opportunities for improvements in perioperative care, including the need to:
1. Reduce unwarranted variation in practice, costs, and outcomes;2. Improve coordination of care, collaboration, teamwork and
communication among perioperative healthcare professionals; and
3. Increase emphasis on transparency, patient-centeredness, patient engagement, and shared decision-making.
The following pages present selected references of peer-reviewed articles and other publications that identify and study potential weaknesses in perioperative care along with possible solutions. Opportunities for improvements are available throughout the perioperative episode as evidenced by:n Variation in pre-operative testing protocols and unnecessary
testing;n Inconsistent or deficient preoperative assessment and
patient preparation for surgery (e.g., education, nutrition, prehabilitation);
n Limited use of evidence-informed guidelines and protocols for certain types of surgery;
n Inefficient intraoperative care, including cancellations and delays in procedures; highly variable and unpredictable
surgical times, use of excessively costly medical supplies and implants, and suboptimal blood management; n Lacking or inappropriate post-operative pain
care; and n Poor discharge planning, care transitions and
patient follow-up, which can lead to potentially avoidable readmissions.
The PSH will address these concerns directly as it will:
n Focus on team care with extensive and specific training in (1) preoperative evaluation, testing and medical optimization, (2) intraoperative care, (3) delivery of procedural sedation, analgesia and anesthesia, (4) post-procedural care, (5) critical care, (6) acute and chronic pain management, and (7) post-procedural recovery and rehabilitation;
n Incorporate all clinicians who understand the surgical implications of medical disease and treatment across the continuum of surgical care;
n Build and operate the infrastructure necessary to support the patient throughout the surgical experience;
n Reduce costs by implementing evidence-informed approaches and reducing duplication of services;
n Collect, analyze and report on patient-centered outcomes from all phases of care;
n Implement evidence-informed practices and standardize care across the entire spectrum of surgical patients;
n Monitor and improve the efficient provision of surgical care using rapid cycle performance improvement;
n Provide a common point of contact for patients and families; and
n Empower patients and family members to participate in their own care and recovery.
Surgical services represent more than half of a hospital’s costs1
and optimizing this care is essential to developing high value health systems. In a PSH, surgeons and anesthesiologists and other perioperative team members will work together to ensure the right care at the right time in the right place.
1Health Care Cost Institute. Health Care Cost and Utilization Report: 2011. Washington, DC: Health Care Cost Institute 2012.
© American Society of Anesthesiologists
HPotentially avoidable adverse events occur too frequently in the perioperative setting.
“The 1999 Institute of Medicine report To Err Is Human put a spotlight on death from preventable medical errors. Surgically related errors are second only to medication errors as the most frequent cause of error-related death.”1
26% of adverse events identified among sample Medicare beneficiaries were events related to surgery and other procedures.2
“… findings suggest that local, regional, and national efforts aimed at improving surgical quality may ultimately reduce costs and improve outcomes.”3
1 Office of Inspector General (OIG), Department of Health and Human Services. Adverse events in hospitals: National incidence among Medicare beneficiaries. November 2010. http://oig.hhs.gov/oei/reports/oei-06-09-00090.pdf
2 Schimpff SC. Improving operating room and perioperative safety: background and specific recommendations. Surg Innov 2007;14:127-35.
3 Birkmeyer JD, Gust C, Dimick JB, Birkmeyer NJ, Skinner JS. Hospital quality and the cost of inpatient surgery in the United States. Ann Surg 2012;255:1-5.
HThere is substantial variability in surgical practice, costs, and outcomes.
“The mortality rate for patients undergoing inpatient non-cardiac surgery was higher than anticipated. Variations in mortality between countries suggest the need for national and international strategies to improve care for this group of patients.”4
“Our data suggest that many hospitals have considerable room to improve their cost efficiency for inpatient surgery and should look for patterns of excess utilization, particularly among surgical specialties, other inpatient specialist consultations, and various types of postdischarge care.”5
“The study showed substantial variations across the participating health care organizations in surgery times, hospital lengths-of-stay, discharge dispositions, and in-hospital complication rates.”6
“These findings led the consortium to test more coordinated management for medically complex patients, more use of dedicated teams, and a process to improve the management of patients’ expectations.”6
• Finks JF, Osborne NH, Birkmeyer JD. Trends in hospital volume and operative mortality for high-risk surgery. N Engl J Med 2011;364:2128-37.
• Kehlet H, Mythen M. Why is the surgical high-risk patient still at risk? Br J Anaesth 2011;106:289-91.
• McManus ML, Long MC, Cooper A, Mandell J, Berwick D, Pagano M, Litvak E. Variability in surgical caseload and access to intensive care services. Anesthesiology 2003;98:1491-6.
• Cowper PA, DeLong ER, Peterson ED, Hannan EL, Ray KT, Racz M, Mark DB: Variability in cost of coronary artery bypass surgery in New York State: Potential for cost savings. Am Heart J 2002; 143:130-9.
• Medbery RL, Perez SD, Force SD, Gillespie TW, Pickens A, Miller DL, Fernandez FG: Video-assisted thoracic surgery lobectomy cost variability: implications for a bundled payment era. Ann Thorac Surg 2014; 97:1686-92.
• Pasquali SK, Jacobs ML, He X, Shah SS, Peterson ED, Hall M, Gaynor JW, Hill KD, Mayer JE, Jacobs JP, Li JS: Variation in congenital heart surgery costs across hospitals. Pediatrics 2014;133:e553-60.
• Daffner S, Beimesch CF, Wang JC: Geographic and demographic variability of cost and surgical treatment of idiopathic scoliosis. Spine 2010; 35:1165-9.
• Peterson ED, Coombs LP, Ferguson TB, Shroyer AL, DeLong ER, Grover FL, Edwards FH: Hospital variability in length of stay after coronary artery bypass surgery: results from the Society of Thoracic Surgeon’s National Cardiac Database. Ann Thorac Surg 2002;74:464-73.
• Ghaferi AA, Birkmeyer JD, Dimick JB. Variation in hospital mortality associated with inpatient surgery. N Engl J Med 2009;361:11368-75.
4 Pearse RM, Moreno RP, Bauer P, Pelosi P, Metnitz P, Spies C, Vallet B, Vincent J-L, Hoeft A, Rhodes A, et al. Mortality after surgery in Europe: a 7 day cohort study. Lancet 2012;380:1059-65.
• Brooke BS, Dominci F, Pronovost PJ, Makary MA, Schneider E, Pawlik TM. • Variations in surgical outcomes associated with hospital compliance with
safety practices. Surgery 2012;151:651-9. • Jan S, Slap G, Dai D,Rubin DM. Variation in surgical outcomes for adolescents
and young adults with inflammatory bowel disease. Pediatrics 2013;131: S81-9.
5 Miller DC, Gust C, Dimick JB, Birkmeyer N, Skinner J, Birkmeyer JD. Large variations in Medicare payments for surgery highlight savings potential from bundled payment programs. Health Affairs 2011;30:2107-15.
• Missios S, Bekelis K. The association of unfavorable outcomes with the intensity of neurosurgical care in the United States. PLoS One. 2014 Mar 19;9(3):e92057. doi: 10.1371/journal.pone.0092057. eCollection 2014.
6 Tomek IM, Sabel AL, Froimson MI, Muschler G, Jevsevar DS, Koenig KM, Lewallen DG, Naessens JM, Savitz LA, Westrich JL, Weeks WB, Weinstein JN. A collaborative of leading health systems finds wide variations in total knee replacement delivery and takes steps to improve value. Health Affairs 2012;31:1329-38.
HThere are opportunities to improve patient-centeredness.
“Meeting information needs are positively and significantly associated with both patient satisfaction measures (i.e., Ratings of Care Processes, p < 0.01; Global Satisfaction, p < 0.05, Perceived Health Benefit, p < 0.01) and one general health status measure (i.e. Quality of Life, p < 0.01).”7
“Patient-centered communication was correlated with the patients’ perceptions of finding common ground. In addition, positive perceptions (both the total score and the subscore on finding common ground) were associated with better recovery from their discomfort and concern, better emotional health two months later, and fewer diagnostic tests and referrals.”8
• Bakhtiari E. Patient-Centered Surgery. HealthLeaders (Vol. May 12): Institute for Healthcare Improvement. 2010.
• Ellison LM, Pinto PA, Kim F, et al. Telerounding and patient satisfaction after surgery. J Am Coll Surg 2004;199:523-30.
7 Larson CO, Nelson EC, Gustafson D, Batalden PB. The relationship between meeting patients’ information needs and their satisfaction with hospital care and general health status outcomes. Int J Qual Health Care 1996;8:447-56.
• Oates J, Weston WW, Jordan J. The impact of patient-centered care on outcomes. Fam Pract 2000;49:796-804.
EXHIBITSelected References Identifying Areas of Opportunity for Improvement through the Perioperative Surgical Home
© American Society of Anesthesiologists

8 Oshima Lee E, Emanuel EJ. Shared decision making to improve care and reduce costs. N Engl J Med 2013;368:6-8.
• Vetter TR, Downing ME, Vanlandingham SC, Noles KM, Boudreaux AM. Predictors of Patient Medication Compliance on the Day of Surgery and the Effects of Providing Patients with Standardized yet Simplified Medication Instructions. Anesthesiology 2014.
HThere are opportunities to improve coordination, communication, collaboration and teamwork.
Observational studies have demonstrated that higher ratings of collaboration and teamwork have been associated with better patient outcomes.9-12
“Patients with multiple, complex comorbidities that require attention from numerous providers with distinct areas of expertise frequently find themselves navigating through diagnoses and treatments from an often disjointed and loosely associated group of providers.”13
“High levels of relational coordination among care providers have been associated with shorter hospital stays, greater patient-perceived quality of care, and improved clinical outcomes.”13
• ACS Bulletin: Improved communication techniques enable residents to provider better care now and in the future. August 2013 Issue. http://bulletin.facs.org/2013/08/improved-communication-techniques-enable-residents-to-provide-better-care-now-and-in-the-future/
9 Baggs JG, Schmitt MH, Mushlin AI, Mitchell PH, Eldredge DH, Oakes D, Hutson AD. Association between nurse-physician collaboration and patient outcomes in three intensive care units. Crit Care Med. 1999;27:1991-1998.
• Choromanski D, Frederick J, Mckelvey GM, Wang H. Intraoperative patient information handover between anesthesia providers. J Biomedical Research 2014;000:000-000.
• Cosgrove J, Gaughan M, Snowden C, Lees T. Decreasing delays in urgent and expedited surgery in a university teaching hospital through audit and communication between perioperative and surgical directorates. Anaesthesia 2008;63:599-603.
10 Davenport DL, Henderson WG, Mosca CL, Khuri SF, Mentzer RM, Jr. Risk-adjusted morbidity in teaching hospitals correlates with reported levels of communication and collaboration on surgical teams but not with scale measures of teamwork climate, safety climate, or working conditions. J Am Coll Surg. 2007;205:778-784.
13 Gittell JH. High Performance Healthcare: Using The Power of Relationships to Achieve Quality, Efficiency and Resilience. New York, NY: McGraw-Hill; 2009.
11 O’Leary KJ, Wayne DB, Haviley C, Slade ME, Lee J, Williams MV. Improving teamwork: Impact of structured interdisciplinary rounds on a medical teaching unit. J Gen Intern Med. 2010;25:826-832.
• Toscan J, Manderson B, Santi SM, Stolee P. “ Just another fish in the pond”: the transitional care experience of a hip fracture patient. International Journal of Integrated Care 2013;13:e023-e.
• Vashdi DR, Bamberger PA, Erez M. Can Surgical Teams Ever Learn? The Role of Coordination, Complexity, and Transitivity in Action Team Learning. Acad Manage J 2013;56:945-71.
12 Wheelan SA, Burchill CN, Tilin F. The link between teamwork and patients’ outcomes in intensive care units. Am J Crit Care. 2003;12:527-534.
• Wyler Von Ballmoos MC, Johnstone DW. Outcomes in thoracic surgical management on non-small cell lung cancer. J Surg Oncol 2014;online.
• Young J, Masya L, Solomon M, Shepherd H. Identifying indicators of colorectal cancer care coordination: a Delphi study. Colorectal Dis 2014;16:17-25.
HEffective preoperative assessment and patient preparation can improve quality and reduce costs.
“In the same-day surgery suite, 98 of 1,164 (8.4%) APMC-evaluated patients were cancelled, as compared with 366 of 2,252 (16.2%) in the non-APMC group (P < 0.001). In the general operating rooms, 87 of 1,631 (5.3%) APMC-evaluated patients were cancelled, as compared with 192 of 1,477 (13.0%) patients without a clinic visit (P < 0.001). For both operating areas, APMC patients had a significantly earlier room entry time than patients not evaluated in the APMC.”14
“Among adults, well-nourished patients were three times more likely to be discharged sooner than those who had some degree of malnutrition. Well-nourished patients with digestive tract diseases were also discharged sooner than malnourished patients with the same condition.”15
“In the postoperative phase, the patients who had improved during prehabilitation were also more likely to have recovered to their baseline walking capacity than those with no change or deterioration. Patients who deteriorated were at greater risk of complications requiring reoperation and/or intensive care management.”16
• Bilku D, Dennison A, Hall T, Metcalfe M, Garcea G. Role of preoperative carbohydrate loading: a systematic review. Ann R Coll Surg Engl 2014;96:15-22.
• Carrillo SR, Melody J.; Douglas, James R.; Rubiano, Andre’s; Schubert, Armin. Surgical Home: Anesthesiologist-Directed Preoperative Triage Reduces Unnecessary Testing and Associated Economic Burden. 2012.
• Correll D, Bader A, Hull M, Hsu C, Tsen L, Hepner D. Value of preoperative clinic visits in identifying issues with potential impact on operating room efficiency. Anesthesiology;105:1254-9.
14 Ferschl M, Tung A, Sweitzer B, Huo D, Glick D. Preoperative clinic visits reduce operating room cancellations and delays. Anesthesiology 2005;103:855-9.
• Fritsch G, Flamm M, Hepner D, Panisch S, Seer J, Soennichsen A. Abnormal preoperative tests, pathologic findings of medical history, and their predictive value for perioperative complications. Acta Anaesthesiol Scand 2012;56:339-50.
• Furze G, Dumville JC, Miles JN, Irvine K, Thompson DR, Lewin RJ. “Prehabilitation” prior to CABG surgery improves physical functioning and depression. Int J Cardiol 2009;132:51-8.
• Glick DB, Tung A, Ferschl MB, Sweitzer B. Anesthesia preoperative medicine clinic: beyond surgery cancellations. Anesthesiology 2006;105: 225-6.
• Jones S, Alnaib M, Kokkinakis M, Wilkinson M, Gibson ASC, Kader D. Pre-operative patient education reduces length of stay after knee joint arthroplasty. Ann R Coll Surg Engl 2011;93:71.
• Kim S-w, Han H-S, Jung H-w, et al. Multidimensional Frailty Score for the Prediction of Postoperative Mortality Risk. JAMA Surgery 2014.
• Knox M, Myers E, Wilson I, Hurley M. The impact of pre-operative assessment clinics on elective surgical case cancellations. Surgeon 2009;7:76-8.
15 Leandro-Merhi VA, de Aquino JL, Sales Chagas JF. Nutrition status and risk factors associated with length of hospital stay for surgical patients. JPEN J Parenter Enteral Nutr 2011;35:241-8.
16 Mayo NE, Feldman L, Scott S, et al. Impact of preoperative change in physical function on postoperative recovery: argument supporting prehabilitation for colorectal surgery. Surgery 2011;150:505-14.
EXHIBITSelected References Identifying Areas of Opportunity for Improvement through the Perioperative Surgical Home
© American Society of Anesthesiologists

• Pattakos G, Johnston DR, Houghtaling PL, Nowicki ER, Blackstone EH. Preoperative prediction of non-home discharge: A strategy to reduce resource use after cardiac surgery. J Am Coll Surg 2012;214:140-7.
• Pollard JB, Garnerin P. Outpatient preoperative evaluation clinic can lead to a rapid shift from inpatient to outpatient surgery: a retrospective review of perioperative setting and outcome. Journal of Clinical Anesthesia 1999;11:39-45.
• Putwatana P, Reodecha P, Sirapo-ngam Y, Lertsithichai P, Sumboonnanonda K. Nutrition screening tools and the prediction of postoperative infectious and wound complications: comparison of methods in presence of risk adjustment. Nutrition 2005;21:691-7.
• Robinson TN, Wu DS, Stiegmann GV, Moss M. Frailty predicts increased hospital and six-month healthcare cost following colorectal surgery in older adults. Am J Surg 2011;202:511-4.
• Swank AM, Kachelman JB, Bibeau W, et al. Prehabilitation before total knee arthroplasty increases strength and function in older adults with severe osteoarthritis. The Journal of Strength & Conditioning Research 2011;25:318-25.
• Thilen S, Treggiari M, Weaver E. An opportunity for anesthesiologists to add value by controlling preoperative resources. ASA Practice Management Meeting, Orlando, FL; 2012.
• Topp R, Swank AM, Quesada PM, Nyland J, Malkani A. The effect of prehabilitation exercise on strength and functioning after total knee arthroplasty. PM&R 2009;1:729-35.
• Vetter TR. Tighten your belts! Reduce your transfusion costs with pre-operative management of anemic patients. Review Course Lectures 2013;3:52.
• Wong J, Lam D, Abrishami A, Chan MV, Chung F. Short-term preoperative smoking cessation and postoperative complications: a systematic review and meta-analysis. Canadian Journal of Anesthesia/Journal canadien d’anesthésie 2012;59:268-79.
HEffective preoperative assessment to reduce unnecessary tests can improve quality and will reduce costs.
“Selective test ordering by staff anesthesiologists reduces the number and cost of preoperative investigations. Educational efforts should be directed towards improving resident and staff preoperative test ordering practices.”17
“In a 5% sample of Medicare claims data, 2803 patients underwent preoperative stress testing without any indications. When these results were applied to the entire Medicare population, we estimated that there are over 56,000 patients who underwent unnecessary preoperative stress testing. The rate of testing in patients without cardiac indications has increased significantly over time.”18
• Brown SR, Brown J. Why do physicians order unnecessary preoperative tests? A qualitative study. Family Medicine-Kansas City 2011;43:338.
• Bryson G. Preoperative testing is inconsistent with published guidelines and rarely changes management. Can J Anesth 2006;53:236-41.
• Cooper M, Newman N, Ibrahim A, Lam E, Herman J, Singh V, Wolfgang C, Pawlik T, Cameron J, Makary M. Unnecessary tests and procedures in patients presenting with solid tumors of the pancreas. J Gastrointest Surg 2013;17:1218-23.
• Czoski-Murray C, Jones M, McCabe C, Claxton K, Oluboyede Y, Roberts J, Nichol J, Rees A, Reilly C, Young D, Fleming T. What is the value of routinely testing full blood count, electrolytes and urea, and pulmonary function tests before elective surgery in patients with no apparent clinical indication and in subgroups of patients with common comorbidities:
a systematic review of the clinical and cost-effective literature. Health Technol Assess 2012;16:1-159.
• Falcone R, Nass C, Jermyn R, Hale C, Stierer T, Jones C, Walters G, Fleisher L. The value of preoperative pharmacologic stress testing before vascular surgery using ACC/AHA guidelines: A prospective, randomized trial. J Cardiothorac Vasc Anesth;17:694-8.
17 Finegan BA, Rashiq S, McAlister FA, O’Connor P. Selective ordering of preoperative investigations by anesthesiologists reduces the number and cost of tests. Can J Anaesth 2005;52:575-80.
• Fischer JP, Shang EK, Nelson JA, Wu LC, Serletti JM, Kovach SJ. Patterns of Preoperative Laboratory Testing in Patients Undergoing Outpatient Plastic Surgery Procedures. Aesthet Surg J 2014;34:133-41.
• Garcia AP, Pastorio KA, Nunes RL, Locks GF, Almeida MCSd. Indication of preoperative tests according to clinical criteria: need for supervision. Rev Bras Anestesiol 2014;64:54-61.
• Kaplan EB, Sheiner LB, Boeckmann AJ. The usefulness of preoperative laboratory screening. JAMA 1985;253:3576-81.
• Katz R, Dexter F, Rosenfeld K, Wolfe L, Redmond V, Agarwal D, Salik I, Goldsteen K, Goodman M, Glass P. Survey study of anesthesiologists’ and surgeons’ ordering of unnecessary preoperative laboratory tests. Anesth Analg 2011;112:2017-12.
• Nepomnayshy D, Hesham W, Erickson B, MacDonald J, Iorio R, Brams D. Sleep apnea: Is routine preoperative screening necessary? Obes Surg 2013:1-5.
• Reynolds TM, National Institute for Health and Clinical Excellence guidelines on preoperative tests: the use of routine preoperative tests for elective surgery. Ann Clin Biochem 2006;43:13-6.
• Schein OD, Katz J, Bass EB, et al. The value of routine preoperative medical testing before cataract surgery. Study of medical testing for cataract surgery. New Engl J Med 2000;342:168-75.
18 Sheffield KM, McAdams PS, Benarroch-Gampel J, et al. Overuse of preoperative cardiac stress testing in Medicare patients undergoing elective noncardiac surgery. Ann Surg 2013;257:73-80.
• Sousa Soares Dd, Marques Brandão RR, Nogueira Mourão MR, Fernandes de Azevedo VL, Vieira Figueiredo A, Santana Trindade E. Relevance of routine testing in low-risk patients undergoing minor and medium surgical procedures. Brazilian Journal of Anesthesiology 2013;63:197-201.
• Wijeysundera DN, Austin PC, Beattie WS, Hux JE, Laupacis A. Variation in the practice of preoperative medical consultation for major elective noncardiac surgery: A population-based study. Anesthesiology 2012;116: 25-34.
HUse of clinical pathways such as enhanced recovery after surgery (ERAS) and other guidelines can improve quality and reduce costs.
“A ‘fast track’ protocol allows patients with high levels of co-morbidity undergoing complex colorectal and reoperative pelvic surgery to benefit from a rapid recovery and early discharge from hospital. The approach is safe and has low readmission rates.”19
“Clinical pathway regional anesthesia care for outpatient orthopedics may have a significant role in simultaneously containing costs and improving both process efficiency and patient outcomes.”20
• Aarts M-A, Okrainec A, Glicksman A, Pearsall E, Victor JC, McLeod RS. Adoption of enhanced recovery after surgery (ERAS) strategies for colorectal surgery at academic teaching hospitals and impact on total length of hospital stay. Surg Endosc 2012;26:442-50.
EXHIBITSelected References Identifying Areas of Opportunity for Improvement through the Perioperative Surgical Home
© American Society of Anesthesiologists

• Abraham N, Albayati S. Enhanced recovery after surgery programs hasten recovery after colorectal resections. World J Gastrointest Surg 2011;3:1-6.
• Cinello M, Nucifora G, Bertolissi M, Badano L, Fresco C, Gonano N, Floretti M. American College of Cardiology/American Heart Association perioperative assessment guidelines for noncardiac surgery reduces cardiologic resource utilization preserving a favourable clinical outcome. J Cardiovasc Med 2007;8:882-8.
19 Delaney C, Fazio V, Senagore A, Robinson B, Halverson A, Remzi F. ‘Fast track’postoperative management protocol for patients with high co-morbidity undergoing complex abdominal and pelvic colorectal surgery. Br J Surg 2001;88:1533-8.
• Dunne DJ, Yip VS, Jones RP, McChesny EA, Lythgoe DT, Psarelli EE, Jones L, Lacasia-Purroy C, Malik HZ, Poston GJ, Fenwick SW. Enhanced recovery in the resection of colorectal liver metastases. J Surg Oncol 2014;110:197-202.
• Eskicioglu C, Forbes SS, Aarts MA, Okrainec A, McLeod RS. Enhanced recovery after surgery (ERAS) programs for patients having colorectal surgery: a meta-analysis of randomized trials. J Gastrointest Surg 2009;13:2321-9.
• Favuzza J, Brady K, Delaney CP. Transversus abdominis plane blocks and enhanced recovery pathways: making the 23-h hospital stay a realistic goal after laparoscopic colorectal surgery. Surg Endosc 2013:1-6.
• Fleisher LA, Beckman JA, Brown KA, et al. ACC/AHA 2007 guidelines on perioperative cardiovascular evaluation and care for noncardiac surgery: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 2002 Guidelines on Perioperative Cardiovascular Evaluation for Noncardiac Surgery). Circulation 2007;116:e418-99.
• Hardt J, Schwarzbach M, Hasenberg T, Post S, Kienle P, Ronellenfi tsch U. The effect of a clinical pathway for enhanced recovery of rectal resections on perioperative quality of care. Int J Colorectal Dis 2013:1-8.
• Holm B, Thorborg K, Husted H, Kehlet H, Bandholm T. Surgery-Induced Changes and Early Recovery of Hip-Muscle Strength, Leg-Press Power, and Functional Performance after Fast-Track Total Hip Arthroplasty: A Prospective Cohort Study. PLoS One 2013;8:e62109. Kehlet H. Surgery: Fast-track colonic surgery and the’knowing–doing’gap. Nature Reviews Gastroenterology and Hepatology 2011;8:539-40.
• Kolozsvari NO, Capretti G, Kaneva P, et al. Impact of an enhanced recovery program on short-term outcomes after scheduled laparoscopic colon resection. Surg Endosc 2012.
• Lassen K, Coolsen MM, Slim K, et al. Guidelines for perioperative care for pancreaticoduodenectomy: Enhanced Recovery After Surgery (ERAS®) Society recommendations. Clin Nutr 2012.
• Mythen M, Swart M, Acheson N, et al. Perioperative fl uid management: Consensus statement from the enhanced recovery partnership. Perioperative Medicine 2012;1:2.
• Sammour T, Zargar-Shoshtari K, Bhat A, Kahokehr A, Hill AG. A programme of Enhanced Recovery After Surgery (ERAS) is a cost-effective intervention in elective colonic surgery. N Z Med J 2010;123:61-70.
• Varadhan KK, Lobo DN, Ljungqvist O. Enhanced recovery after surgery: the future of improving surgical care. Crit Care Clin 2010;26:527-47.
• Williams BA, DeRiso BM, Engel LB, et al. Benchmarking the perioperative process: II. Introducing anesthesia clinical pathways to improve processes and outcomes and to reduce nursing labor intensity in ambulatory orthopedic surgery. J Clin Anesth 1998;10:561-9.
20 Williams BA, DeRiso BM, Figallo CM, et al. Benchmarking the perioperative process: III. Effects of regional anesthesia clinical pathway techniques on process effi ciency and recovery profi les in ambulatory orthopedic surgery. J Clin Anesth 1998;10:570-8.
HImprovement in intraoperative blood management can improve quality and reduce costs.
“Variation in hemoglobin transfusion was signifi cant among surgical services, surgeons, and anesthesiologists. The use of erythrocyte salvage, fresh frozen plasma, and platelets varied threefold to fourfold among individual surgeons compared with their peers performing the same surgical procedure.”21
“We conclude that blood component usage for coronary artery bypass grafts differs widely among institutions. The variability in use of these components is accounted for in part by unnecessary transfusions in otherwise routine, uncomplicated coronary artery bypass graft procedures.”22
• Campbell Jr DA, Henderson WG, Englesbe MJ, et al. Surgical site infection prevention: The importance of operative duration and blood transfusion—results of the fi rst American College of Surgeons–National Surgical Quality Improvement Program Best Practices Initiative. J Am Coll Surg 2008;207:810-20.
21 Frank SM, Savage WJ, Rothschild JA, Rivers RJ, Ness PM, Paul SL, Ulatowski JA: Variability in blood and blood component utilization as assessed by an Anesthesia Information Management System. Anesthesiology 2012;117:99-106.
22 Goodnough LT, Jonston MFM, Toy PTCY: The variability of transfusion practice in coronary artery bypass surgery. JAMA 1991;265:86-90.
• Lako A, Bilali S, Memishaj S, et al. The impact of blood use on patients undergoing coronary artery bypass surgery: a prospective study. Il Giornale di chirurgia 2013;35:20-6.
EXHIBITSelected References Identifying Areas of Opportunity for Improvement through the Perioperative Surgical Home
© American Society of Anesthesiologists
HThere are important opportunities to improve postoperative care, transitions, and patient follow-up.
“The current study found signifi cant variability in the use of follow-up procedures, with the most striking differences apparent across geographic regions.”23
“Postoperative recovery after open colonic surgery may be accelerated by effective pain relief integrated into an accelerated rehabilitation programme.”24
“Patients would be more adequately prepared for their recovery period at home, by encouraging client-centered, interdisciplinary communication between health practitioners; adopting a fl exible, approach to discharge planning which is tailored to individual needs of postsurgical patients, particularly in relation to advice and information related to recovery; and encouraging and supporting adequate health literacy for self-management.”25
• Anthony MK, Hudson-Barr DC. Successful patient discharge: A comprehensive model of facilitators and barriers. J Nurs Adm 1998;28:48-55.
• 23Cooper GS, Yuan Z, Chak A, Rimm AA. Geographic and patient variation among Medicare benefi ciaries in the use of follow-up testing after surgery for nonmetastatic colorectal carcinoma. Cancer 1999;85:2124-31.
• Hebl JR, Dilger JA, Byer DE, et al. A pre-emptive multimodal pathway featuring peripheral nerve block improves perioperative outcomes after major orthopedic surgery. Reg Anesth Pain Med 2008;33:510-7.
• Joh YG, Lindsetmo RO, Stulberg J, Obias V, Champagne B, Delaney CP. Standardized postoperative pathway: accelerating recovery after ileostomy closure. Dis Colon Rectum 2008;51:1786-9.
24 Kehlet, Mogensen. Hospital stay of 2 days after open sigmoidectomy with a multimodal rehabilitation programme. Br J Surg 1999;86.
25 McMurray A, Johnson P, Wallis M, Patterson E, Griffi ths S. General surgical patients’ perspectives of the adequacy and appropriateness of discharge planning to facilitate health decision-making at home. J Clin Nurs 2007;16:1602-9.
HPerioperative leadership and models such as the perioperative surgical home will be required to succeed in the new accountable care environment.
“We found that ACOs have so far devoted little attention to surgical care.”26
“However, surgeons and other specialists have a large role to play in caring for ACOs’ patients.”26
“In the years to come, ACOs will likely focus more on surgical care.”26
26 Dupree JM, Patel K, Singer SJ, West M, Wang R, Zinner MJ, Weissman JS. Attention to surgeons and surgical care is largely missing from early Medicare accountable care organizations. Health Aff (Millwood) 2014;33:972-9.
• Garson L, Schwarzkopf R, Vakharia S, et al. Implementation of a total joint replacement-focused perioperative surgical home: A management case report. Anesth Analg 2014;118:1081-9 10.
• Krupka DC, Sandberg WS, Weeks WB. The impact on hospitals of reducing surgical complications suggests many will need shared savings programs with payers. Health Aff (Millwood) 2012;31:2571-8.
• Lee A, Kerridge RK, Chui PT, Chiu CH, Gin T. Perioperative systems as a
quality model of perioperative medicine and surgical care. Health policy 2011;102:214-22.
• Ravikumar TS, Sharma C, Marini C, Steele GD Jr, Ritter G, Barrera R, Kim M, Safyer SM, Vandervoort K, De Geronimo M, Baker L, Levi P, Pierdon S, Horgan M, Maynor K, Maloney G, Wojtowicz M, Nelson K. A validated value-based model to improve hospital-wide perioperative outcomes: adaptability to combined medical/surgical inpatient cohorts. Ann Surg 2010;252:486-96; discussion 496-8.
• Seim AR, Sandberg WS. Shaping the operating room and perioperative systems of the future: innovating for improved competitiveness. Current Opinion in Anesthesiology 2010;23:765-71.
Prepared September 2014 bythe Department of Health Policy Research
EXHIBITSelected References Identifying Areas of Opportunity for Improvement through the Perioperative Surgical Home
© American Society of Anesthesiologists





























