Embed Size (px)
Citation preview
The Michigan. Alcoholism Screening Test (Mast)BY MELVIN L. SELZER, M.D. AND JANE LOWENSTEHJ, M.S.W.*
There is a widely acknowledged need to develop reliable methods of identifying individuals who have chronic drinking problems. Granted this task is complicated by the current bewilderment about the etiology of alcoholism, progress can be made toward a more universal classification system provided that standardized instruments are used. Our own interest in developing a questionnaire to determine whether a respondent has a chronic and serious drinking problem stems frcm earlier traffic research where it was often difficult to make this determination.
Given research results indicating that alcoholics are responsible for a substantial majority of alcohol-related accidents, particularly those deemed serious, the need for a reliable detection instrument as a first step in efforts to reduce these traffic mishaps is obvious.Seme observers may consider the problem of detecting alcoholics among serious traffic offenders to be an academic one. Our response is that the alcoholics among such drivers must be identified since they are usually unable to alter their alcohol-related delinquent traffic pattern without treatment that will ameliorate their chronic drinking problem and thus lower their risk of causing serious or fatal traffic accidents.
The Michigan Alcoholism Screening Test (MAST) was devised to provide a consistent, quantifiable, easily administered interview instrument for the detection of alcoholism (Table 1). The MAST consists of a series of 25 questions, many of which have been used previously by investigators in alcoholism surveys. 3-6 The respondent is asked to tell whether he has had specific drinking- related experiences. The questions were designed to be straightforward and understandable to unsophisticated resporxJeafcs. In addition, it was hoped that
■»The University of Michigan Highway Safety Research Institute and Department of Psychiatry
seme of the questions would appear sufficiently neutral so that evasive alcoholics would betray their drinking problems.
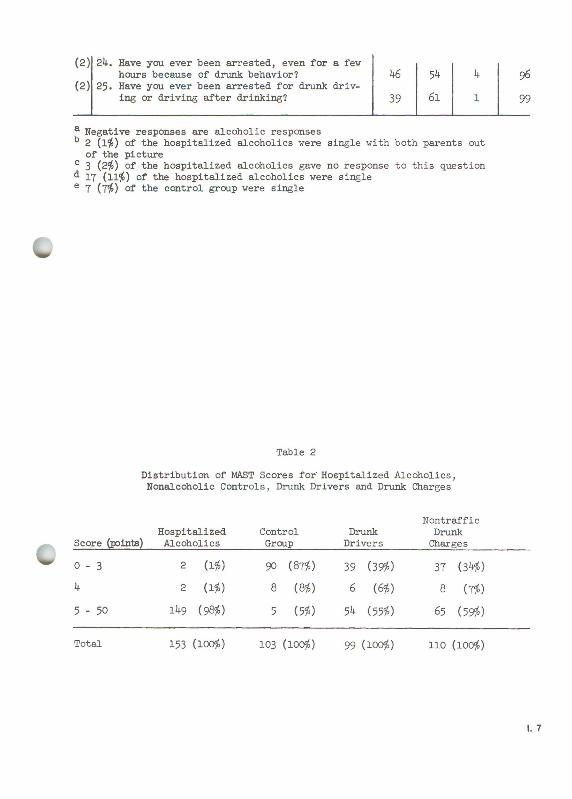
The MAST was first used with 153 known (hospitalized) alcoholics and a control group of 103 presumed non-alcoholics in order to obtain a sample of alcoholic and non-alcoholic responses to each question. The control group consisted of 67 non-academic University of Michigan employees and 36 patients at the University's Allergy Clinic; the control group was socioeconomically ccmparable to the hospitalized alcoholics. Any person in the control group with an obvious drinking problem was eliminated fron the study. Based on an analysis of the responses of the two groups and on the clinical importance of each item, a tentative scoring system was devised and a point value assigned to each question.(The above two groups' distribution of responses to the MAST and the point value for each question are given in Table 1.) A total of five or more points is considered presumptive evidence of alcoholism; four points is regarded as suggestive of alcoholism.
Although the scoring system as now used is relatively arbitrary, we are currently in the process of validating the reliability of the MAST as an instrument for the detection of alcoholism with an intensive search of social and medical agency records for alcohol-related information on all MAST respondents. When the validation process is completed, revisions of the MAST questions and scoring system can be undertaken to make it a more effective instrument.
In addition to the two criterion groups, the MAST was given to several other groups in which a high incidence of drinking problems was suspected and in which respondents might have reason to hide their problem. Two of these groups were 99 persons convicted of drunk driving and 110 persons convicted of drunk and disorderly charges. Both groups were interviewed at court immediately after their convictions. It was anticipated that a considerable proportion of the latter two groups would obtain alcoholic scores to the MAST - if the respondents were being truthful. It was also expected that a larger proportion of alcoholics
2
would be found among those convicted of drunk and disorderly charges than among those found guilty of drunk driving. This expectation was derived from common stereotypes of the "drunk and disorderly" offender.
Table 2 indicates that more than half of the persons in each of these two groups obtained alcoholic scores when given the MAST. Fifty-four (55$) of the drunk drivers and 65 (59$) °f the drunk and disorderly offenders obtained scores of five or more. There was no significant difference between the two groups in the proportions falling within the alcoholic, suggestive, and non-alcoholic categories. However, 3̂- (63$) of the 'ÿh alcoholic drunk drivers scored within the lowest alcoholic range of five to ten points, as compared to only 25 (38$) of the 65 alcoholic drunk and disorderly offenders. Thus the MAST responses for the two groups provide some substantiation for the idea that there are more severe alcoholics among the drunk and disorderly offenders.
The ability of the MAST to categorize as alcoholic over half of the persons in two groups in which high proportions of undisclosed, but problematic drinking were expected, is encouraging. However, we were surprised that only 59$ of the drunk and disorderly offenders obtained alcoholic scores. This may be a function of the relatively youthful population of Ann Arbor; exactly half of the Drunk and Disorderly group were under 30 and of these only 1+4$ scored 5
or more points contrasted to 75$ of those who were 30 years and older. Since the questionnaire is based on certain drinking behavior and its consequences, younger persons often have not yet developed the complications necessary to place them in the "alcoholic" range.
That an effective program for detecting and actively treating alcoholic traffic offenders will come about is a certainty. How long it will take to evolve is problematic. Perhaps a Ralph Hader is needed to arouse the public in this area of traffic safety. At any rate, such programs will be of far more value than the current movement to lower the legal permissible blood alcohol level from 0 .15$ to 0.10$. The claim that such a purely legal maneuver would lower
accident rates should be regarded as frivolous and resembles nothing as much as the voodoo practice based on the premise that one can destroy an enemy by sticking pins through a doll resembling him. Clearly an approach more fruitful than incantation is needed and cannot begin to evolve until methodology is developed to reveal those problem drivers who have a chronic drinking problem.
Identification of drivers with drinking problems is an essential part of any program aimed at treating the alcoholic and hopefully modifying his problematic behavior, including his driving behavior. In addition to its potential utility for traffic safety programs, the MAST can be of use to medical, legal, and psychiatric personnel seeking an objective and universal method of establishing a diagnosis of alcoholism.
4
R e fe re n ce s
Selzer, M.L.: Alcoholism, Mental Illness, and Stress in 96 Drivers CausingFatal Accidents. Behav. Sei. lU:l, 1969.
Selzer, M.L.; Rodgers, J.; and Kern, S.: Fatal Accidents: The Role of Psychopathology, Social Stress and Acute Disturbance. Amer. J. Psychiat. 124:1028, February, 1968.
Guze, S.B. et. al.: Psychiatric Illness and Crime with Particular Referenceto Alcoholism: A Study of 223 Criminals. J. Nerv. Ment. Pis. 134:512, 1962.
Bailey, M.D.; Haberman, P.W.j and Alksne, H.: The Epidemiology of Alcoholismin an Urban Residental Area. Quart. J. Alcohol 26:19, 1965.
Mulford, H.A., and Wilson, R.W.: Identifying Problem Drinkers in a Household Survey. Public Hlth. Svce. Pub. No. 1000, Series 2 - No. 16, May, 1966.
Selzer, M.L., and Ehrlich, N.J.: A Screening Program to Detect Alcoholismin Traffic Offenders. In: The Prevention of Highway Injury. (Selzer, M.L.,Gikas, P.W., and Huelke, D.F., Editors). Ann Arbor: University of MichiganHighway Safety Research Institute, 1967, pp. 44-50.
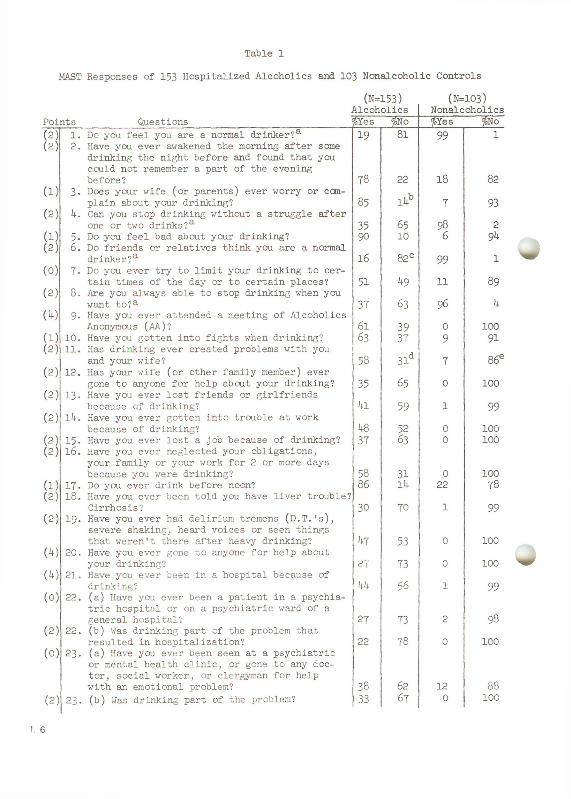
Table 1MAST Responses of 153 Hospitalized Alcoholics and 103 Nonalcoholic Controls
(N=153) (N=103)Alcoholics Nonalcoholics
Points Questions $Yes $>No $Yes %No(2 )(2 )
1. Do you feel you are a normal drinker?8,2. Have you ever awakened the morning after some
drinking the night before and found that you could not remember a part of the evening
19 81 99 1
(X)before?
3. Does your wife (or parents) ever worry or com78 22
. h18 82
(2)plain about your drinking?
4. Can you stop drinking without a struggle after85 nr 7 93
one or two drinks?a 35 65 98 2(1)(2 )
5- Do you feel bad about your drinking?6. Do friends or relatives think you are a normal
90 10 6 9k
(0 )drinker?a
7. Do you ever try to limit your drinking to cer16 82c 99 1
(2)tain times of the day or to certain places?
8 . Are you always able to stop drinking when you51 h9 11 89
wwant to?a
9. Have you ever attended a meeting of Alcoholics37 63 96 1+
Anonymous (AA)? 61 39 0 100(1)(2 )
10. Have you gotten into fights when drinking?11. Has drinking ever created problems with you
63 37 9 91
(2)and your wife?
12. Has your wife (or other family member) ever58 31d 7 86e
(2 )gone to anyone for help about your drinking?
13. Have you ever lost friends or girlfriends35 65 0 100
(2 )because of drinking?
lU. Have you ever gotten into trouble at work1+1 59 1 99
because of drinking? 48 52 0 100(2 )(2 )
15. Have you ever lost a job because of drinking?16 . Have you ever neglected your obligations,
your family or your work for 2 or more days37 63 0 100
because you were drinking? 58 31 0 100(1)(2 )
17. Do you ever drink before noon?18. Have you ever been told you have liver trouble?
86 14 22 78
(2)Cirrhosis?
1 9. Have you ever had delirium tremens (D.T.'s), severe shaking, heard voices or seen things
30 70 1 99
(*0that weren't there after heavy drinking?
20. Have you ever gone to anyone for help abouth i 53 0 100
Wyour drinking?
21. Have you ever been in a hospital because of27 73 0 100
(0 )drinking?
22. (a) Have you ever been a patient in a psychiatric hospital or on a psychiatric ward of a
kk 56 1 99
(2 )general hospital?
22. (b) Was drinking part of the problem that27 73 2 98
(o)resulted in hospitalization?
2 3. (a) Have you ever been seen at a psychiatric or mental health clinic, or gone to any doctor, social worker, or clergyman for help
22 78 0 100
with an emotional problem? 38 62 12 88(2 ) 2 3. (b) Mas drinking part of the problem? 33 67 0 100
(2 ) 2 k . Have ycru ever been arrested, even for a few hours because of drunk behavior? k6 51* k 96
(2 ) 25. Have you ever been arrested for drunk driving or driving after drinking? 39 61 1 99
a Negative responses are alcoholic responses13 2 (l$) of the hospitalized alcoholics were single with both parents out of the picture
c 3 (2$) of the hospitalized alcoholics gave no response to this question d 17 (11$) of the hospitalized alcoholics were single e 7 (7$) °f the control group were single
Table 2Distribution of MAST Scores for' Hospitalized Alcoholics, Nonalcoholic Controls, Drunk Drivers and Drunk Charges
NontrafficHospitalized Control Drunk Drunk
Score (points) Alcoholics______ Group_______Drivers_______Charges0 - 3 2 (1$) 90 (87$) 39 (39$) 37 (3̂ $)
2 (1$) 8 (8$) 6 (6$) 8 (7$)5 - 50 I k s (98$) 5 m 5k (55$) 65 (59$)
Total 153 (ioc$) 103 (ioc$) 99 (100$) 110 (100$)