Embed Size (px)
Citation preview
Journal ofsurgical Oncology 3(3): 309-315 (1971)
The Metabolism and Pharmacology of 5 -Fluorouracil
Edward Miller, M.D.’
5-Fluorouracil(5-FU) is a chemotherapeutic agent, which is administered systemically for the palliative treatment of certain neoplastic diseases. Because 5-FU is a potent antimetabolite, i t is recommended that the drug be given only by physicians experi- enced in the use of antimetabolites. Now that 5-FU is being applied topically for the treatment of skin neoplasms, it would be useful to review the metabolism and pharma- cology of this compound. In this paper, the metabolic pathways, the antineoplastic mechanism of action, and the effects on normal tissues are discussed.
INTRODUCTION In this symposium some of the papers describe the treatment of skin neoplasms with chemotherapy. The need for chemotherapy is evident because it is recognized today that this must be one of the means of completely controlling the neoplastic cell. This will be possible when medical science produces chemicals capable of altering- either permanently or continuously-the mechanism that controls the division of the neoplastic cell. The knowledge of the etiology of neoplasms, while desirable, is not necessarily a prerequisite to successful treatment, as has been illustrated in the past with other disease processes.
The greater part of the malignant cell function is cell division and growth, accompanied by a loss of its specialized function. Antimetabolite research therefore has been aimed a t the nucleic acids because of their major role in cell division and growth. An ‘antimetabolite’ is defined as a substance which acts by competing with normal metabolites for particular enzymes. By displacing the normal metabo- lite, the antimetabolite prevents normal function of the enzyme.
Because the antimetabolites are concerned with DNA synthesis, their action occurs during the S phase of cell division. The duration of these phases shows con-
This paper was presented at a symposium entitled ‘Recent Advances in the Management of Skin
* Director, Clinical Oncology, Department of Medical Research, Hoffmann-LaRoche, Inc., Nutley,
309
Neoplasms’held April 11-12,1969, New York, New York.
New Jersey.

310 Miller
siderable variation in different types of cells and in different species (Merkle et al., 1965).
If we do not consider the hormone as chemotherapy in the strict sense, then we can assume that the era of cancer chemotherapy began with nitrogen mustard, the prototype of the present-day alkylating agents. This compound was observed t o have an antitumor effect in animals and subsequently was shown to retain this activity against certain malignancies in man (Rhoads, 1946). In 1947, the anti- folate aminopterin was synthesized for use against acute leukemia in children, after Farber observed tha t the administration of folic acid to leukemic children accelerated the disease process. He therefore reasoned tha t a compound which would block folic acid might have some effect against leukemia. As we all know, this became a clinical reality and so ushered in the era of antimetabolites in cancer chemotherapy (Farber et al., 1948).
In 1954, Rutman observed that, in the rat, more uracil was utilized for nucleic acid synthesis in a liver tumor than in normal liver tissue (Rutman et al., 1954). I n 1956, Cohen and Barner reported their studies of ‘thymineless death’ in bacteria and suggested that compounds which would inhibit DNA synthesis might be of value in cancer chemotherapy. Heidelberger et al. (1957) demonstrated i n vitro tha t a synthesized antipyrimidine, 5-fluorouracil, inhibited the conversion of CI4-labeled formate into the methyl group of thymine. This was then shown t o have significant effect in the inhibition of animal tumor growth (Heidelberger et al., 1958). Fluorine was chosen because i t has an atomic weight close t o hydrogen and is therefore bound tightly to the molecule (Heidelberger et al., 1957).
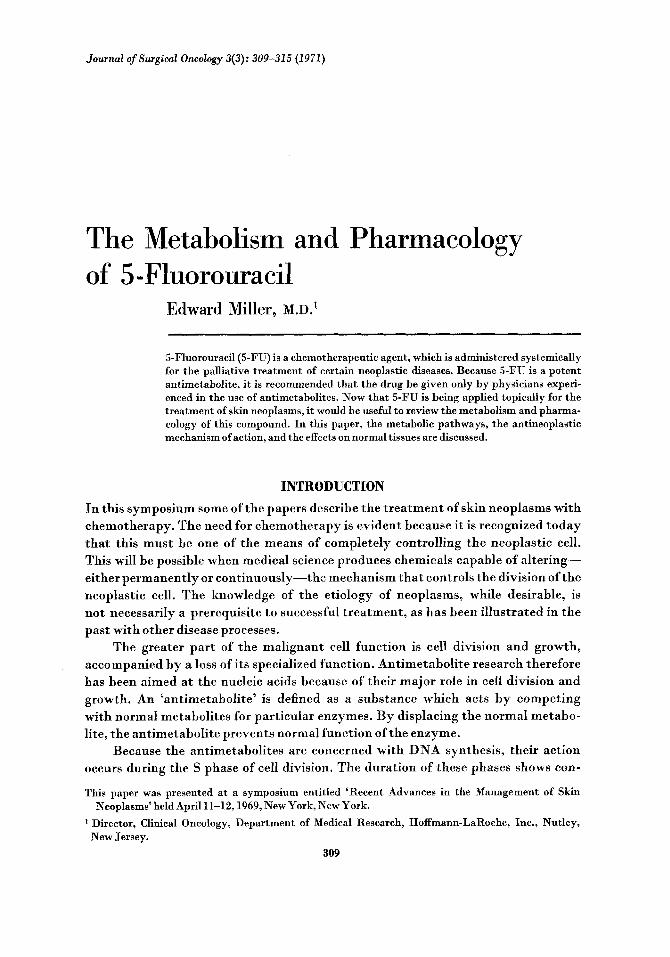
METABOLISM The structures of the pyrimidines uracil and thymine and the antipyrimidine
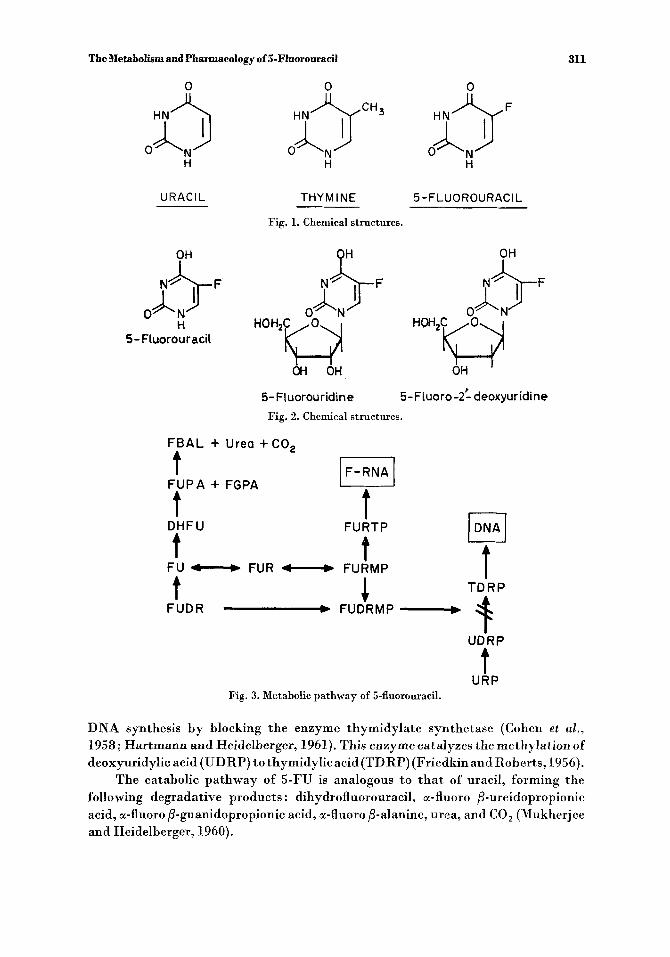
5-fluorouracil arc shown in Fig. 1. The nucleosides 5-fluorouridine (5-FUR) and 5-fluoro 2‘-deoxyuridine (5-FUDR) are shown in Fig. 2.
The metabolic pathway of 5-FU is presented schematically in Fig. 3. The biochemical effects of 5-FU in the anabolic pathway are (1) the inhibition of RNA synthesis by inhibiting the incorporation of uracil and orotic acid (not shown), (2) the incorporation of F U into a fraudulent RNA (shown in the upper right), (3) the inhibition of DNA synthesis (shown in the lower right) (Danneberg et al., 1953). The inhibition of DNA synthesis is considered t o be chiefly responsible for the antineoplastic activity of FU in man, since concentrations which inhibit DNA synthesis may still permit RNA synthesis (Heidelberger et al., 1960). 5-Fluorouracil is converted to 5-fluorouridine (5-FUR) and then t o the mono-, di-, and triphos- phates of 5-FUR. This is then incorporated into the fraudulent RNA. 5-Fluorouri- dine monophosphate (5-FURMP) is also reduced t o 5-fluoro 2-deoxyuridine monophosphate (5-FUDRMP). 5-FUDRMP may also be formed directly from 5-FUDR. There is no further anabolism t o the di- and triphosphate nucleotides of 5-FUDR. The formation of 5-FUDRMP is considered t o be the basis for the anti- neoplastic action of 5-FU. 5-FUDRMP, the so-called lethal nucleotide, inhibits
The Metabolism and Pharmacology of 5-Fluorouracil 311
URACIL THYM IN€ 5 -FLUOROURACI L
Fig. 1. Chemical structures.
0 H
5- Fluorouracil
5- FLuorou r idin e 5- F Luoro -2: deoxyur idi ne Fig. 2. Chemical structures.
FBAL + Urea +CO,
FUPA + FGPA t
t t t t t 4
JDNAI t 9
FURTP DHFU
FU - FUR FURMP TDRP
FUDR - FUDRMP-
UDRP
t URP
Fig. 3. Metabolic pathway of 5-fluorouracil.
DNA synthesis by blocking the enzyme thymidylate synthetase (Cohen et al., 1958; Hartmann and Heidelberger, 1961). This enzyme catalyzes the methylation of deoxyuridylic acid (UDRP) t o thymidylicacid(TDRP) (Friedkinand Roberts, 1956).
The catabolic pathway of 5-FU is analogous to tha t of uracil, forming the following degradative products: dihydrofluorouracil, a-fluoro /3-ureidopropionic acid, a-fluoro P-guanidopropionic acid, a-fluoro /3-alanine, urea, and CO, (Mukherjee and Heidelberger, 1960).

312 Miller
The liver is the principal site of catabolism of 5-FU (Chaudhuri et al., 1958). It is apparently entirely catabolized up t o a threshold dose, above which the liver can no longer handle it and anabolism then proceeds. A lack of catabolic activity has been observed in certain tumors and has been suggested as the explanation for the localization of 5-FU in these tumors. The degradative products of 5-FU are ineffective against malignant disease and are nontoxic to normal tissue (Mukherjee et al., 1963).
Following an intravenous injection of 15 mg/kg of 5-FU in man, the plasma levels fall off rapidly. In 3 hr no intact drug can be detected in the plasma (Clarkson e t a l . , 1964).
About 15 percent of the intravenous dose is excreted in the urine in 6 hr as intact 5-FU, with over 90 percent of this amount (the 15 percent) excreted in the first hour. Patients with impaired renal function excrete less 5-FU. However, this has little or no effect on toxicity, since the normal urinary excretion is already so low (Clarkson et al., 1964).
About 60-80 percent of the intravenous dose is excreted as respiratory CO, in 8-12 hr-the product of catabolism (Mukherjee et al., 1963). It is obvious tha t very little of the dose administered follows the anabolic pathway.
There is considerable variation in the uptake of 5-FU in tumors of different organs. The vascularity and the cellularity of the tissue play a large role-not only in tumors, but also in normal tissue. In general, however, the conversion into the nucleotide 5-FUDRMP-i.e., the anabolism of 5-FU-is greater in tumors than in normal tissue (Mukherjee et al., 1963).
PHARMACOLOGY It has been stated that 5-FU may exert antitumor effects by inhibiting DNA
synthesis. Clinically, the systemic administration of 5-FU has its greatest effect in adenocarcinoma of the large bowel and the breast. Frequently, there is also some effect in other solid tumors. This correlates fairlywell with theuptake of 5-FUinthese tissues. By this mechanism 5-FU also interferes with the metabolism of the normal, rapidly proliferating cells-e.g., the gastrointestinal mucosa, the bone marrow, the hair follicles, and the nail beds (Milles et al., 1962; Brennan et al., 1960; Stalzer et al., 1965; Falkson and Schulz, 1962; Vaitkevicius et aE., 1961).
In approximately three quarters of the patients treated with systemic 5-FU, the first sign of toxicity is a stomatitis which appears after four t o eight doses. This can vary from mild erythema to hemorrhagic ulceration of the oral cavity. The classic site of this manifestation is inside the lower lip. This early sign of toxicity is useful in monitoring the administration of the drug. Frequently accompanying the stomatitis is diarrhea, which occurs in approximately half of the patients treated. Nausea and vomiting may occur a t any time during the course of therapy in about 30 percent of the patients. These are apparently of central origin due t o the effect of 5-FU on the brain stem.
After a course of 5-FU the intestinal mucosa usually shows suppression of nor- mal cell growth resulting in atrophy of the glandular elements, followed by epithelial
The Metabolism and Pharmacology of 5-Fluorouracil 313
desquamation. The mucosa returns to normal after the cessation of therapy. In studies of the intestinal mucosa there was no correlation between the clinical toxicity of the gastrointestinal tract and the histologic appearance of the mucosa. Diarrhea sometimes occurred in the absence of any mucosal changes. In addition, there was no correlation between the bone marrow changes or the tumor response and the mucosal changes in the gastrointestinal tract (Milles et al., 1962).
I n bone marrow studies made while patients were receiving 5-FU therapy, characteristic changes have been observed which resemble those seen in pernicious anemia (Stalzer et al., 1965). Erythrocyte precursors are markedly decreased after four or five daily doses of 5-FU, resulting in a sharp rise in the mye1oid:erythroid ratio. Erythropoiesis is megaloblastic. About the eleventh to twelfth day, normal hematopoiesis results in the return of the M E ratio t o normal. During the twelfth t o the twenty-sixth day, there is a leukopenia in the peripheral blood, with occa- sionally a thrombocytopenia. The lowest point is usually around the twentieth day.
Although the red cell precursors are decreased in the marrow, there is usually no anemia because of the 3-month life span of the mature red cell. However, the short life span of the mature granulocyte results in leukopenia. The lymphocytes are not affected. The megaloblastic anemia which is sometimes seen is due to DNA deficiency while RNA synthesis continues. The DNA deficiency is due t o deficient thymine or thymidine synthesis. Either thymine or thymidine in appropriate doses can improve megaloblastic anemia (Brennan et at., 1960; Stalzer et al., 1965). However, this is not used clinically since the marrow will return t o normal in 1-2 weeks. Even in the presence of thrombocytopenia, bleeding and purpura have been rare. The hematopoietic depression can be independent of the stomatitis, hut this rarely occurs. We have seen marrow depression without stomatitis in those patients who have received prior radiotherapy of antineoplastic agents.
There have been two reports of an acute cerebellar syndrome after the admini- stration of 5-FU. These were characterized by ataxia, vertigo, dysphagia, slurred speech, and nystagmus. To a lesser extent there were also some signs of vestibular disturbance. This was apparently dose dependent since the same patients were able t o toIeratelower doses of F U (Riehl and Brown, 1964; Moertel et at., 1964).
On a weight basis, 5-FU is 10 to 20 times more antiandrogenic than progester- one. In the immature castrated rat, testosterone causes increased mitosis and in- creased RNA and protein synthesis, resulting in the growth of the seminal vesicles. 5-FU in adequate doses will reverse the testosterone by inhibiting the synthesis of DNA, RNA, and protein. However, increased doses of testosterone will cause increased incorporation of 5-FU into RNA with a decreased inhibition of DNA synthesis (Cantarow and Zagerman, 1964). There has been no direct study of the effect of 5-FU on spermatogenesis.
As with many other cytotoxic chemotherapeutic agents, 5-FU has been ob- served to be teratogenic in laboratory animals. The types of malformations included cleft palate and deformed paws and tail. In rats, the fetus is five times more sensi- tive than the adult to a lethal dose of 5-FU. I n the same animal, the tumor-inhibiting

314 Miller
dose is about 14 times greater than the minimal teratogenic dose (Chaube and Murphy, 1968). There has been no report of any teratogenic effect in humans.
The lymphocytes from cancer patients who had been treated with 5-FU were studied for chromosomal anomalies. The following aberrations were reported, some as early as after the first dose of 5-FU: chromosome fragmentation and deletion, chromatid breaks, translocations, segmental interchanges, and ring chromosomes (Amato et aE., 1966).
In several experimental studies 5-FU has suppressed the immune response in mice and in humans. This is influenced both by the dose of 5-FU given and by the timing of the drug administration in relation t o the antigenic challenge (Suhrland et al., 1966; Santos, 1967).
There have been many publications describing various toxic manifestations related to the skin. In 5-20 percent of the patients treated systemically with 5-FU, alopecia and dermatitis have been reported. These changes are apparently not on an allergic basis since they are dose dependent. Hyperpigmentation has been frequently observed and is usually manifested after a long period of treatment, giving the patient an addisonian appearance. Falkson, in South Africa, has reported the largest series of patients with photosensitivity, which is characterized by an erythema after short exposure t o the sun while receiving systemic 5-FU. There have been a few reports of abnormalities in the nail beds, but these are apparently in- frequent (Falkson and Schulz, 1962 ; Vaitkevicius et nl., 1961).
When 5-FU is applied topically t o intact skin, the amount absorbed is less than 10 percent. This is based on studies with CL4-labeled drug (Klein, unpublished data; Dillaha et al., 1965). I n addition, the rate of absorption carried out over the entire 24 hr, would tend t o simulate an intravenous infusion of the compound. This would also tend to lower the toxicity of 5-FU, which apparently follows the catabolic pathway when it is infused over a long period of time (Miller and Sullivan, 1967). However, when 5-FU has been administered topically to hemorrhagic ulcerated areas of the skin, the absorption has been so rapid tha t the classic toxic side-effects have appeared. Therefore, caution must be exercised in selecting the type of lesion for treatment with topical 5-FU.
REFERENCES Amato, R. S., Mitra, J., Kabakow, B., and Blinick, G. (1966). Effects of thio-tepa and 5-fluorouracil
on chromosomes of human lymphocytes in v i v a Lcvy Laboratories, Beth Israel Medical Center and Department of Biology, New York University, New York, N.Y. Federation Proc. 25: 561 (abst. No. 2101).
Bosch, L., Harbers, E., and Heidelberger, C. (1958). Studies on fluorinated pyrimidines. V. Effects on nucleic acid metabolism invitro. Cancer Res. 18: 335.
Brennan, M. J., Vaitkevicius, V. K., and Rebuck, J. W. (1960). Megaloblastic anemia associated with inhibition of thymine synthesis (observations during 5-fluorouracil treatment). Blood 16: 1535- 1545.
Cantarow, A., and Zagerman, A. J. (1964). Fluorouracil inhibition of testosterone-stimulated growth of seminalvesicles. Proc. Soc. Exptl. Biol. Med. 115: 1052-1054.
Chaube, S., and Murphy, M. L. (1968). The teratogenic effects of the recent drugs active in cancer chemotherapy. Advan. Teratol. 3: 181-237.

The Metabolism and Pharmacology of 5-Fluorouracil 315
Chaudhuri, N. I<., Mukherjee, K. L., and Heidelberger, C. (1958). Studies on fluorinated pyrimidines. VII. The degradative pathway. Biochem. Pharmacol. 1 : 328-341.
Clarkson, B., O’Connor, A,, Winst,on, L., and Hutchison, D. (1964). The physiologic disposition of 5-fluorouracil and 5-fluoro-2‘-deoxyuridinein man. Clin. Pharmacol. Therap. 5 : 581-610.
Cohen, S. S., and Barner, H. D. (1956). Studies on the induction of thymine deficiency on the effects of thymine and thymidine analogs in Escherichia coli. J. Bacteriol. 7 1 : 588.
Cohen, S. S., Flaks, J. G., Barner, H. D., Loeb, M. R., and Lictenstein, J. (1958). The mode of action of 5-fluorouracil andits derivatives. Proc. Natl. Acad. Sci. 44: 1004.
Danneberg, P. B., Montag, B. J., and Heidelberger, C. (1958). Studies on fluorinated pyrimidines. IV. Effects onnucleic acid metabolism in vivo. Cancer Res. 18 : 328-334.
Dillaha, C. J., Jansen, G. T., Honeycutt, W. M., and Holt, G. A. (1965). Further studies with topical 5-fluorouracil. Arch. Derrnatol. 92: 410.
Falkson, G., and Schulz, E. J. (1962). Skin changes in patients treated with 5-fluorouracil. Brit. J. Dermatol. 24: 229-236.
Farber, S., Diamond, L. K., Mercer, R. D., Sylvester, R., Jr., and Wolff, J. A. (1948). Temporary re- missions in acute leukemia in children produced by folic acid antagonist, 4-amino-ptero yl-glutamic acid (aminopterin). New Engl. J . Med. 238: 787.
Friedkin, M., and Roberts, D. (1956). Conversion of uracil deoxyrihoside to thymidine of deoxyribo- nucleic acid. J. B i d . Chem. 220: 653.
Hartmann, K.-U., and Heidelberger, C. (1961). Studies on fluorinated pyrimidines. XIII. Inhibition of thymidylate synthetase. J. Biol. Chem. 236: 3006-3013.
Heidelberger, C., Chaudhuri, N. K., Danneberg, P., Moorcn, D., Griesbach, L., Duschinsky, R., Schnitzer, R. J., Pleven, E., and Scheiner, J. (1957). Fluorinated pyrimidines: A new class of tumor-inhibitory compounds. Nature 179 : 663-666.
Heidelberger, C., Griesbach, L., Cruz, C., Schnitzer, R. J., and Grunberg, E. (1958). Fluorinated pyrimi- dines. VI. Effects of 5-fluorouridine and 5-fluoro-2’-deoxy-uridine on transplantable tumors. Proc. SOC. Exptl. Biol. Med. 97 : 470.
Heidelherger, C., Ghobar, A., Baker, R. K., and Mukherjee, K. L. (1960). Studies of fluorinated pyrimi- dines. X. Invivo studies on tumor resistance. Cancer Res. 20: 897.
Merkle, T. C., Stuart, R. N., and Gofman, J. W. (1965). The calculation oftreatment schedules for cancer chemotherapy. Lawrence Radiation Laboratory, University of California, Livermore, California, October 13.
Miller, E., and Sullivan, R. D. (1967). The alteration of biologic activity of cancer chemotherapy agents by prolonged infusion. Cancer Chemotherapy, Grune & Stratton, Inc., New York.
Milles, S. S., Muggia, A. L., and Spiro, H. M. (1962). Colonic histologic changes induced by 5-fluoroura- cil. Gastroenterology43: 391-399.
Moertel, C. G., Reitemeier, R. J., Bolton, C. F., and Shorter, R. G. (1964). Cerebellar ataxia associated with fluorinated pyrimidine therapy. Cancer Chemotherapy Rept. 41: 15-18.
Mukherjee, K. L., and Heidelberger, C. (1960). Studies on fluorinated pyrimidines. IX. The degradation of 5-fluoro~racil-6-C’~.J. Biol. Chem. 235: 433-437.
Mukherjee, K. L., Boohar, J., Wentland, D., Ansfield, F. J., and Heidelberger, C. (1963). Studies on fluorinated pyrimidines. XVI. Metabolism of 5-fluorouracil-2-CI4 and 5-fluoro-2’-deoxyuridine- 2-C14 in cancer patients. Cancer Res. 23: 49-77.
Rhoads, C. P. (1946). Nitrogen mustard in the treatment of neoplastic disease. J . A m . Med. Assoc. 131: 656.
Riehl, J.-L., and Brown, W. J. (1964). Acute cerebellar syndrome secondary to 5-fluorouracil therapy. Neurology14: 961-967.
Rutman, R. J., Cantarow, A., and Paschkis, K. E. (1954). Studies in 2-acetylaminofluorene carcino- genesis. 111. Utilization of uracil-2-C14 by preneoplastic rat liver and rat hepatoma. Cancer Res. 14: 119-123.
Santos, G. W. (1967). Immunosuppressive drugs I. Federation Proc. 26: 907-913. Stalzer, R. C., Kiely, J. M., Pease, G. L., and Brown, A. L., Jr. (1965). Effect of 5-fluorouracil on human
Suhrland, L. G., Benson, J. W., and LaBelle, E. (1966). Immunosuppression and tumor stimulation in
Vaitkevicius, V. K., Brennan, M. J., Beckett, V. L., Kelly, J. E., and Talky, R. W. (1961). Clinical
hematopoiesis. Cancer 18: 1071-1078.
mice with 5-fluorouracil. J. Lab. CZin. Med. 68: 992
evaluation of cancer chemotherapy with 5-fluorouracil. Cancer 14 : 131-152.










![PHARMACOLOGY · Web viewNone undergoes first pass metabolism D. All of it undergoes first pass metabolism GP05 [gjk] LD50 is: A. Median lethal dose B. Determined in phase I clinical](https://img.pdfslide.us/doc/110x75/5afc333d7f8b9a444f8bbee9/viewnone-undergoes-first-pass-metabolism-d-all-of-it-undergoes-first-pass-metabolism.jpg)


















