Embed Size (px)
Citation preview
7/28/2019 The Medical Context of Parental Coping With Childhood Cancer 1
http://slidepdf.com/reader/full/the-medical-context-of-parental-coping-with-childhood-cancer-1 1/15
American Journal of Community Psychology, VoL 14, No. 2, 1986
T h e M e d ic a l C o n t e x t o f P a r e n t a l C o p i n g W i th
C h i l d h o o d C a n c e r 1
O s c a r A . B a r b a ri n 2 a n d M a r k C h e s l e r
University of Michigan
This research as ses sed the ex ten t to w h ich con tex tua l fac to r s , e spec ia l ly theme d ica l con tex t , a re r e la ted to the use o f spec i f i c cop ing s t ra teg ies by 74p a r e n t s o f s u r v i v i n g c h i ld r e n w i t h ca nc er. P a r e n t s r e p o r t e d t h a t t h e y c o p e dreasonab ly w e l l by us ing in format ion - seek ing , p rob lem-so lv ing , he lp -seek ing ,main ta in ing emot iona l ba lance , r e ly ing on r e l ig ion , be ing op t im is t i c , deny-
ing , a nd accep ting . M or e h igh ly educa ted pare n t s t en ded to use pro b le m so lv -
ing, optimism , an d inform ation seeking s ignificantly m or e an d denial s ignificant-
ly less than less wel l -educated parents . H ow eve r , g ende r an d incom e w ereunre la ted to cop ing . The use o f spec i f i c cop ing s tra teg ies was no t r e la ted to
s e v e r it y o f t h e c h i l d 's m e d i c a l c o n d i t io n , s t re s s le v e l o r p a r e n t s " o w n e v a lu a -
t i o n s o f t h e i r c o p i n g e f fe c t iv e n e s s . H o w e v e r , t h e q u a l it y o f re l a ti o n s w i t ht h e m e d i c a l s t a f f w a s s t r o n g l y r e l a t e d t o c o p i n g s t ra t eg i es . U s e o f p a s s i v e
c o p i n g s t ra t e g ie s w a s p o s i t i v e l y r e l a te d t o g o o d r e l a ti o n s w i t h t h e m e d i c a l
s t a f f .
Most s tudies of s t ress fu l l i fe events indicate that i l lness or loss of a loved
o n e r e p re s e n ts a m a j o r s t r es s o r ( D o h r e n w e n d & D o h r e n w e n d , 1 97 4; D o h r e n -
w e n d , K r a s n o f f , A s k e n a s y , & D o h r e n w e n d , 1 9 78 ; H o l m e s & R a h e , 1 96 7).
A l t h o u g h d i a g n o s i s a n d t r e a t m e n t o f a c h i l d w i t h a s e r i o u s a n d c h r o n i c i l l -
ness se ldom app ears in such s tudies , i t a l so represents a s igni f ican t l i fe d i s rup-
t i o n w h i c h t h r e a t e n s p e r s o n a l e q u i l i b r i u m a n d f a m i l y w e l l- b e in g . T h e i n it ia l
i m p a c t o f t h e d i a g n o s i s is il l u s tr a t e d i n th e f o l l o w i n g re p o r t s f r o m p a r e n t s .
~ P r e p a r a ti o n o f t h i s p a p e r w a s g r e a t l y f a c il i ta t e d b y t h e a w a r d o f a p o s t d o c t o r a l f e l lo w s h i p
b y t h e P s y c h o l o g y D e p a r t m e n t a t S t a n f o r d U n i v e r s i ty a n d b y a g r a n t f r o m t h e U n i v e r si t y o f
M i c h i g a n ' s C o m m i t t e e o n t h e I n t e rn a t i o n a l Y e a r o f t h e C h i ld . T h a n k s a r e d u e t o P r o f e s s o r sP h i l i p Z i m b a r d o a n d E w a r t T h o m a s .
2 A ll c o r r e s p o n d e n c e s h o u l d b e a d d r e s s e d t o O s c a r A . B a r b a r i n , D e p a r t m e n t o f P s y c h o l o g y ,
U n i v e r s it y o f M i c h i g a n , A n n A r b o r , M i c h i g a n 4 81 0 9.
221
0091-0562/86/0400-0221505.00/0 © 1986 Plenum Pub lishingCorporation
7/28/2019 The Medical Context of Parental Coping With Childhood Cancer 1
http://slidepdf.com/reader/full/the-medical-context-of-parental-coping-with-childhood-cancer-1 2/15
222 Barbarin and Chesler
It tore me up. I didn't know from one minute to the next whether he was going tobe with us. You know I worried a lot. I felt bad. I was hurt. He is my only boy.I didn't know if I was there myself.I felt like my heart had been torn right out o f me. I was terribly despondent at first.I was bitter and asked myself why it had happened.
Al though med ica l p rogress has inc reased the l i ke l ihood tha t a ch i ld
diagnosed wi th cancer wi ll surv ive and resume a norm al l i fe (Am erican Canc er
Socie ty , (1982) , many chi ldren s t i l l d ie f rom the d isease . Painfu l medica l
t rea tm ents (perhaps surgery) and the i r s ide effec ts , repe ated hospi ta l iza t ions ,
and the un ce r t a in ty o f rec overy o r re l apse , o f l ife o r dea th seve rely t e st s
pa ren t s ' emot iona l s tab i li t y (Fu t t e rm an & Ho ffm an , 1973) . Mo reove r , man y
paren t s ' l ack o f fami l i a r i t y w i th the d i sease and i ts t rea tmen t , conce rn abo u t
insu rance coverage and f inances , and the un remi t t i ng dem ands o f ca ring fo r
a ser iously i l l ch i ld a l l c rea te s t ress (Desmond, 1980) . The effor t requi red
to deve lop and nu r tu re re l a t ionsh ips wi th fami ly , f r i ends , and med ica l p ro -
fess ionals ma y fur th er tax parents ' psychologica l reserves (Binger e t a l. , 1969;
Cass i le th & Ham i l ton 1979) . A l th oug h some o f t hese s tre sses m ay d imin i sh
over t ime , t hey se ldom van i sh en t i re ly .
S T R E SS A N D C O P I N G S T R A T E G I E S
Severa l scholars suggest tha t var ia t io ns in fam i l ies ' experie nce of s t ress
is re la ted to d i f feren ces in the i r use of copin g s t ra tegies (B arba r in , 1983;
Brehm, 1965; Kubler-Ross , 1978; Lazarus , 1966; Sel igman, 1975; Taylor ,
1983) . Ou r unde rs t and ing o f pa ren t s ' s t ra teg ies fo r cop ing w i th the s tre sses
o f ch i ldhood cance r has been advanced subs t an t i a l ly by seve ra l p ionee r ing
s tu d ie s . F o r i n s ta n c e , F r ie d ma n , C h o d o f f , M a s o n , a n d H a m b u r g (19 77 )
docu me n ted the use o f accep tance , re s igna t ion , re lig ious fa i th , ho pe and op -
t imism, denial , and ant icipatory grief by famil ies of chi ldren with cancer.
Spinet ta , Swa rner , and S hep0 sh (1981) obse rved severa l o th er Copings t ra t eg ies among such fami l i e s : a cons i s t en t ph i losophy / theo logy , suppor t
from a s igni f icant o ther , communicat ion wi th the chi ld , communicat ion wi th
s ib l ings, and ma in tenance o f no rm al fa mi ly func t ion ing . Ku ps t e t a l. (1982)
ca t egor i zed the cop ing s t ra teg ies t hey obse rved s om ewh a t d i f fe ren t ly : open
com mu nica t ion , l iv ing in the present , a ff i rm ing l i fe , t rea t ing the child as nor-
ma l , and deve lop ing a ph i losoph ica l ou t look on the d i sease .
Al tho ugh these descr ip t ive typologies advance ou r unde rs tanding of how
fami li e s ac tua l ly dea l w i th se r ious an d ch ron ic ch i ldh ood i ll ness, t hey do no t
t ake adv an tage o f recen t concep tua l i za t ions o f t he cop ing p rocess . La za rusand Laun ie r (1978) p ro pos ed a typ o log y o f cop ing s t ra teg ies based o n the
d i s t inc t ion be tween ac t ive o r p rob lem focused (e .g . , d i rec t ac t ion a imed a t
e l iminat ing or m i t iga ting ant ic ipa ted s tresses) and pass ive or em ot ion- focu sed

7/28/2019 The Medical Context of Parental Coping With Childhood Cancer 1
http://slidepdf.com/reader/full/the-medical-context-of-parental-coping-with-childhood-cancer-1 3/15
T h e C o n t e x t o f C o p i n g 223
(e.g., cognitive or emotional maneuvers aimed at moderat ing the impact of
stress by reinterpreting or avoiding it). Although Billings and Moos (1981)
made finer discriminations between the method (active/direct vs. passive/in-
direct) and the target (problem vs. emotions) their ways of classifying discrete
coping strategies are consistent. In these terms, both the list developed byFriedman et al. (1977) and Kupst et al. (1982) emphasized relatively passive
strategies. Spinetta et al. (1981) included some strategies that are more ac-
tive in nature: For example, support, communication, and maintenance of
family functioning. Unfor tunately, there are few data available from these
and other sources to assess the factors that may predispose parents to use
various active or passive strategies. Most importantly, few studies have ex-
amined the relationship between the medical factors and coping process.
The Medical Context of Parental Coping
Early analyses of the relationship between parental coping strategies
and the medical context relied primarily on observations of parents of dying
children and took the form of prescriptive reports. More recent studies that
have explored medical context effects typically have examined only the child's
medical condition (Spinetta et al., 1982). Attention to the child's medi-
cal condition is understandable. Indeed, parents' coping responses can
be expected to vary with the child's diagnosis and medical status because thelatter are associated with differential stress, prospects for survival, and in-
trusiveness of treatment (Chesler, Barbarin, Chesler, Hughes, & Lebo, 1981).
For example, children with Wilms tumors now have a 2-year survival rate
of over 85%0, whereas children with brain tumors have a 2-year survival rate
of under 50% (American Cancer Society, 1982). Varied treatment procedures
such as surgery, radiation, or chemotherapy create quite different concerns
and require somewhat different adaptations by parents and children. Similar-
ly, uncontrollable events such as relapse usually creates additional severe stress
and uncertainty. Learned helplessness theory (Seligman, 1975) predicts thatthe more severe and uncontrollable the stressor the more likely individuals
are to adopt passive and emotion-focused coping strategies such as accep-
tance, optimism, and religious beliefs. This prediction is consistent with the
emphasis on passive strategies observed by Friedman et al. (1977) and Kupst
et al. (1980).
However, the child's medical situation is only part of a more complex
medical context which includes evolving relations with a medical care
organization. Although the link between coping and transactions with im-
portant others has been noted elsewhere (Brickman et al., 1982; Coyne &Holroyd, in press; McCubbin & Patterson, 1982, 1983; Wortman & Dunkel-
Schetter, 1979), few studies have explicitly examined the interaction between
parents' ways of coping and their relationship with medical staff. Much of

7/28/2019 The Medical Context of Parental Coping With Childhood Cancer 1
http://slidepdf.com/reader/full/the-medical-context-of-parental-coping-with-childhood-cancer-1 4/15
224 Barbarin and Chesler
the prior research has been conducted by staff responsible for the medical
or psychological care of children with cancer. As such, the staff's impact
on stress and coping has been taken as a given and not examined
systematically.
In general, the role structure of bureaucratized medical care systemspress for compliant and relatively passive patient/parent roles (Antonovsky,
1980; DiMatteo, 1979; Friedson, 1970; Stone, 1979; Taylor, 1979). In this
context, passive strategies such as deference, optimism, and denial, and
reliance on religious faith may be regarded by the sta ff as most appropriate
or convenient behaviors for patients and their families. The use of active
coping strategies by patients and their guardians, such as information seek-
ing and participation in decision-making, may be construed as acting-out
responses or as intrusions on the medical staff's responsibilities. In addition,
medical staff may avoid constantly depressed or hopeless parents, just asthey appear to withdraw emotionally from their young patients and families
as death approaches (Binger et al., 1969; Vaux, 1977). Since the causal direc-
tion of the relation between parental coping and sta ff behaviors is unclear,
it is also possible that parents' coping choices may influence the ways in which
medical staff relate to parents.
An examination of the relations between parent-staf f transactions and
parents use of particular coping styles may offer valuable insights into why
parents respond they way they do in chronically stressful situations. In this
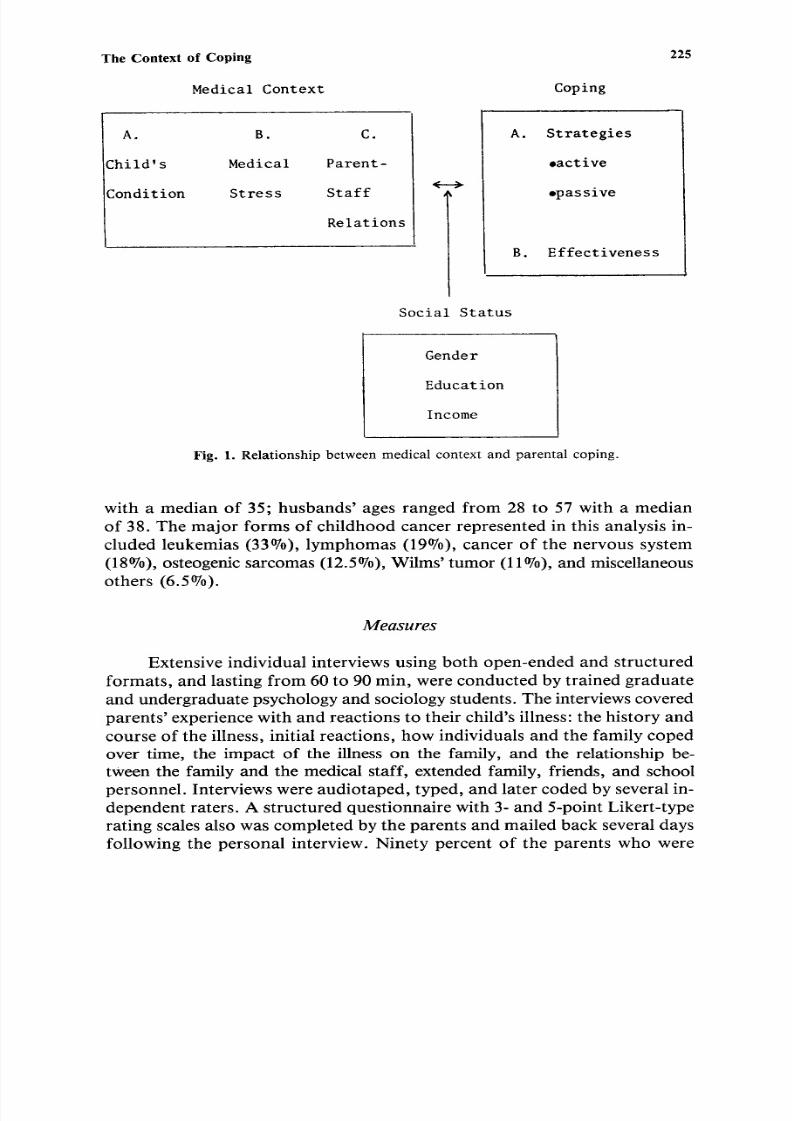
paper we examine how the various coping strategies covary with aspects ofthe medical context. The medical context is conceived in terms o f the child's
medical condition, parental stress from the illness, and the quality of parent's
relationships with the medical staff. Figure 1 presents the variables and the
relationships explored in this study.
This research is part of a larger study of stress and coping in families
of children with cancer. In the larger study, a total of 94 parents (55 families)
were sampled from a pool of 265 families of children with cancer treated
within the previous 5 years at a major university medical center. This sam-
ple population was selected randomly, after stratificat ion by the age and life
status of the child at the time of the study and by the type of cancer sus-
tained by the child. In all, 70 families were contacted and 15 declined to par-
ticipate.
Participants in this study include 74 parents from 45 families with
children living with cancer; 42 mothers and 32 fathers. With the exception
of one black family all participants were white. Twenty-three percent of the
parents o f children living with cancer reported an annual family income of
less than $15,000, 29°7o had an annual income between $15,000 and $25,000,
and 36O/o an annual income over $25,000; 11% of the informants did not
report their annual income. Ages of the wives ranged from 23 to 54 years
7/28/2019 The Medical Context of Parental Coping With Childhood Cancer 1
http://slidepdf.com/reader/full/the-medical-context-of-parental-coping-with-childhood-cancer-1 5/15
T h e C o n t e x t o f C o p i n g
Medical Context Coping
2 2 5
A. go
Child's Medical
Condition Stress
C.
Parent-
Staff
Relations
<.- ..~
A. Strategies
oactive
opassive
B . E f f e c t i v e n e s s
Social Status
Gender
Education
Income
Fig. 1. Rel~ionship between medicalcontext and parentalcoping.
with a median of 35; husbands' ages ranged from 28 to 57 with a median
of 38. The major forms of childhood cancer represented in this analysis in-
cluded leukemias (33%0), lymphomas (19%0), cancer o f the nervous system
(18%0), osteogenic sarcomas (12.5%0), Wilms' tumor (11%0), and miscellaneous
others (6.5%).
Measures
Extensive individual interviews using both open-ended and structured
formats, and lasting from 60 to 90 min, were conducted by trained graduate
and undergraduate psychology and sociology students. The interviews covered
parents' experience with and reactions to their child's illness: the history and
course of the illness, initial reactions, how individuals and the family coped
over time, the impact of the illness on the family, and the relationship be-
tween the family and the medical staff, extended family, friends, and school
personnel . Interviews were audiotaped, typed, and later coded by several in-
dependent raters. A structured questionnaire with 3- and 5-point Likert-typerating scales also was completed by the parents and mailed back several days
following the personal interview. Ninety percent of the parents who were
7/28/2019 The Medical Context of Parental Coping With Childhood Cancer 1
http://slidepdf.com/reader/full/the-medical-context-of-parental-coping-with-childhood-cancer-1 6/15
226 Barbarin and Chesler
interviewed completed and returned the questionnaire. The high return rate
is due in part to the strong endorsement of the study by Share, a Candlelighter-
afffliated self-help group for families of children with cancer and by the parents'
view that information about their experiences might be helpful to newly
diagnosed families.Medical Context. The child's medical condition was assessed by parents'
interview reports of the number o f hospitalizations experienced after diagnosis
and initial treatment induction. Parents" medically related stress was assessed
by a composite index consisting of four items rated on a 3-point scale
indicating the degree of stress resulting from (a) the fact that my child has
cancer, (b) my child's reactions to drugs, (c) my fear of the child's death and,
(d) my fear of relapse. The correlations among these items range from .47
to .63. The estimate of internal consistency is high (Cronbach's alpha = .83).
Parents' assessment of the quality of relations with medical staff wasa composite measure developed by combining structured questionnaire ratings
of relationship qualities such as respect, tenseness, anger, liking, and sup-
port. This index includes (a) Respect for Medical Staff, a 5-point rating of
the effect of the illness on respect for medical staff (1 = much less, 5 =
much more); (b) Tension in Relations with Medical Staff, a 3-point rating
of stress resulting from tense relations with medical staff, (c) Support From
Medical Staf, a composite of two 5-point ratings indicating support received
from doctors and from nurses (Pearson r = .61, p < .001); (d) Anger Toward
the Medical System, a 5-point rating indicating the extent to which the ex-perience of childhood cancer resulted in more or less anger toward the medical
care systems; and (e) Liking the Medical Staff, a 5-point rating of change
in feelings about medical staff resulting from the illness experience. This in-
dex represents parents evaluation of the relationship quality along several
related but distinct lines. The combination of static ratings such as those of
tension and support with change measures of liking, anger, and respect is
justified by the strong correlations among these ratings (range -- - .35 to
+ .71). These correlations show that individuals who report increases in lik-
ing and respect and decreases in anger are also likely to make favorable static
ratings of support and tension. The static ratings and parents view of the
change resulting from the intensive interaction during the t reatment phase
provide slightly different slants on parents' evaluations of the relationship.
Moreover, the estimate of internal consistency supports the reduction of these
ratings into a single index (Cronbach's alpha = .76).
Coping. Guided by earlier work on stress and coping, a typology of
coping strategies was developed inductively from parents' actual feelings and
behaviors reported in the interviews. Specific measures of coping techniques
were generated from parents' responses to interview questions about how
they coped with the diagnosis, treatment, treatment side effects, and the en-
tire illness situation. A score for each of eight coping strategies was obtained

7/28/2019 The Medical Context of Parental Coping With Childhood Cancer 1
http://slidepdf.com/reader/full/the-medical-context-of-parental-coping-with-childhood-cancer-1 7/15
The Context of Coping 227
by tabulating each instance in which a parent indicated use of a particular
strategy. The range of scores on each strategy is 0-4 except for religious faith
(range = 0-10), which has several additiona l items specifically addressing
the role of religion in coping. The interr ater agre ement for the coding of
the strategies incl uded in the ty polo gy is .83. The eight copi ng strategies a ndtwo coping styles are as follows:
1. In fo rm at io n seeking involves parents seeking and using inf orm a-
tion to help them understand the meaning of the diagnosis, to place their
emot ional reactions to the illness in perspective, or to reduce uncert ainty and
fear regarding their child 's survival.
I tried to find out everything I could about it. I read everything I could about it.The things I read about medical technology and its advances have helped me throughthe hard times. I keep some of these articles close at hand whenever I feel down.
2. Prob lem solving refers to the use of behaviorall y oriented solutions
for specific problems, such as increased work hour s to raise mon ey to meet
medical expenses, re arra nging schedules to be with the child in the hospital,
or pl an ni ng with teachers for the child's retur n to school.
Its like solving a problem. I am going to solve that problem, and I will not allowcertain things to happen. I don't know how to describe the strength within a humanindividual except that I said I was stronger than whatever that problem is and I willprevail.
She was in great pain, and I didn't think they cared very much. I got their attentionand they finally did something for the pain.
3. Inf orm al help seeking refers to the self-initiated use of inf orm al
helping networks of family members and friends for inst rumenta l aid or emo-
t ional support .
Friends and family are very important. I don't know if we could have handled it aswell without the support of our friends and family. Other people are not quite asinvolved, and sometimes you need to talk with them. It was too much of a burdenfor me so I turned to my family, I turned to my friends, I turned to my co-workers.
4. Main tai nanc e of emot ional balance refers to active efforts de-
signed to moderate emotional reactions and to avoid extreme mood swings,
especially thr ough cognitive self-control and related be haviors. In some sense
it means trying to retain or recapture some degree of previous normality in
one's personal style and social relations.
I try to see that the hustle and bustle of life is not important. I'm trying to take eachday as it comes and to experience each day more. I've often practiced hypnotherapyand relaxation techniques, and I also use a little rationalization.
5. Reliance on religious beli efs/ fait h refers to the use of prayer and
religious interpretations for emotional comfort or to evolve an acceptable
explanation for the illness.
7/28/2019 The Medical Context of Parental Coping With Childhood Cancer 1
http://slidepdf.com/reader/full/the-medical-context-of-parental-coping-with-childhood-cancer-1 8/15
2 2 8 B a r b a r in a n d C h e s l e r
I th ink pray ing had done m ore than anything else. I practice m y belief mo re. I feelthat was the on ly place I co uld turn to get help when I really needed i t . M y religiousbeliefs have helped me.
6 . O p t i m i s m i n v o l v es t h e u se o f i d e a t i o n s o r s e l f - s ta t e m e n t s t h a t t h in g s
w i l l t u r n o u t w e l l a n d r e p r e s e n t s a n e f f o r t t o f o c u s o n p o s i t i v e r a t h e r t h a nn e g a t i v e p o s s i b i l i t i e s .
After the init ial shock and everything we looked to the brighter side. Now we arenot the scared of i t .
I th ink positively . I th ink in terms of her growing up and going to school and gett ingbet ter and do ing the th ings tha t a norma l ch i ld would do . W e' re p repar ing her fo rthe future.
7 . D e n i a l r e f e rs t o d i s b e l i e f o f t h e d i a g n o s i s o r i ts n e g a t i v e i m p l i c a -
t i o n s , r e f u s a l t o f o c u s o n i l ln e s s - r e l a t e d i s s ue s a n d w i t h d r a w a l f r o m s i t u a -t i o n s r e m i n i s c e n t o f t h e i l ln e s s . I n t h e a b s t r a c t i t m a y b e d i f f i c u l t t o d r a w
t h e l i n e b e t w e e n o p t i m i s m a n d d e n i a l b u t m o s t r e p o r t s d o p e r m i t s u ch
d i s t i n c t i o n s .
M y husband doe sn ' t wan t to know abou t our son hav ing to go to the hosp i ta l p r io rto when he has to go. I t was 2 weeks befo re he could pronounc e the word leukemia.
I try to keep my m ind off i t . I d on ' t watch TV shows or anything pertaining to i t .I shut it off. I don 't want to hear ab out it. W hy hurt yourself by watching that garbage?
8 . A c c e p t a n c e r e f e r s t o a r e s p o n s e c h a r a c t e r i z e d b y a s o m e w h a tf a t a l i s t ic p e r c e p t i o n o f a s i t u a t i o n a s i n e v i ta b l e a n d u n c o n t r o l l a b l e . I t
r e p r e s e n t s c o m i n g t o t e r m s w i t h a p r o b l e m w i t h o u t a c t i n g d i r e c t ly o n i t .
I 've a lways sa id that ' I f i t 's gonna happen , i t ' s gonna happe n . '
W hy shou ld I cry? I jus t hand led i t and accep ted i t and that was that .
9 . A c t i v e c o p i n g st y le s r e p r e s e n t a c o m p o s i t e in d e x f o r m e d b y s u m -
m i n g t h e s c o r e s o f c o p i n g s t r a t e g ie s j u d g e d t o b e a c t i v e i n o r i e n t a t i o n ( n o s .
1 - 4 a b o v e ) ,
1 0. P a s s i v e c o p i n g s t y le s r e p r e s e n t a c o m p o s i t e i n d e x f o r m e d b y s u m -
m i n g t h e s c o r e s o f c o p i n g s t r a t e g ie s j u d g e d t o b e p a s s i v e in o r i e n t a t i o n ( n o s .
5 - 8 a b o v e ) .
C o p i n g e f f e c t i v e n e s s w a s b a s e d o n a 4 - p o i n t r a t in g m a d e b y i n f o r m a n t s
o f h o w w e l l t h e y f e l t t h e y h a n d l e d t h e i r c h i l d 's i l ln e s s (1 = p o o r l y , 4 - - v e r y
w e l l ) .
Social Status. T h e s o c i a l d e m o g r a p h i c v a r i a b l e s u s e d in t h is s t u d y i n -
c l u d e g e n d e r , y e a r s o f f o r m a l e d u c a t i o n , a n d a n n u a l f a m i l y i n c o m e . F o r c h i -
s q u a r e a n a l y s e s p a r e n t s a r e d i v i d e d i n to t h r e e i n c o m e g r o u p s b a s e d o n t h e i r
r e p o r t e d t o t a l f a m i l y i n c o m e ( < $ 1 0 , 0 0 0 , n = 1 3; $ 1 0 - $ 2 5, 0 0 0 , n = 2 6; a n d
> $ 25 , 00 0 , n = 2 3) a n d i n t o t h r e e g r o u p s b a s e d o n y e a r s o f f o r m a l e d u c a -
7/28/2019 The Medical Context of Parental Coping With Childhood Cancer 1
http://slidepdf.com/reader/full/the-medical-context-of-parental-coping-with-childhood-cancer-1 9/15
T h e C o n t e x t o f C o p i n g 2 2 9
tion (high schoo l educ atio n or less, n = 24; some college, n = 20; and col-
lege graduate or more, n = 23).
RESULTS
Most parents felt that they coped reasonably well. Of the 74 parents
in the sample only one gave herself a poo r rating, 13 (17.6%) gave themselves
fair ratings, 42 (56.8%) gave themselves good ratings, and 18 (24.3%) gave
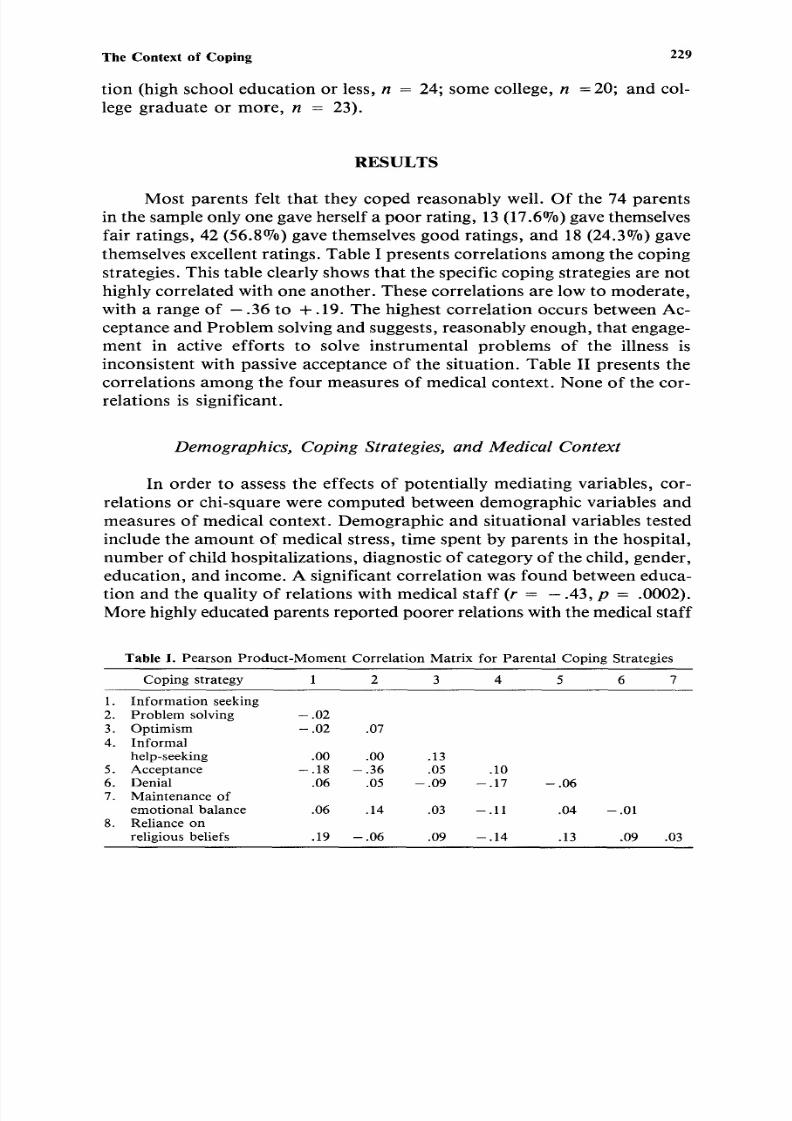
themselves excellent ratings. Table I presents correlations among the coping
strategies. This table clearly shows tha t the specific coping strategies are not
highly correlated with one another. These correlations are low to moderate,
with a range of -.36 to +. 19. The highest correlation occurs between Ac-
ceptance and Pr oble m solving and suggests, reasonably enough, that engage-
ment in active efforts to solve instrumental problems of the illness is
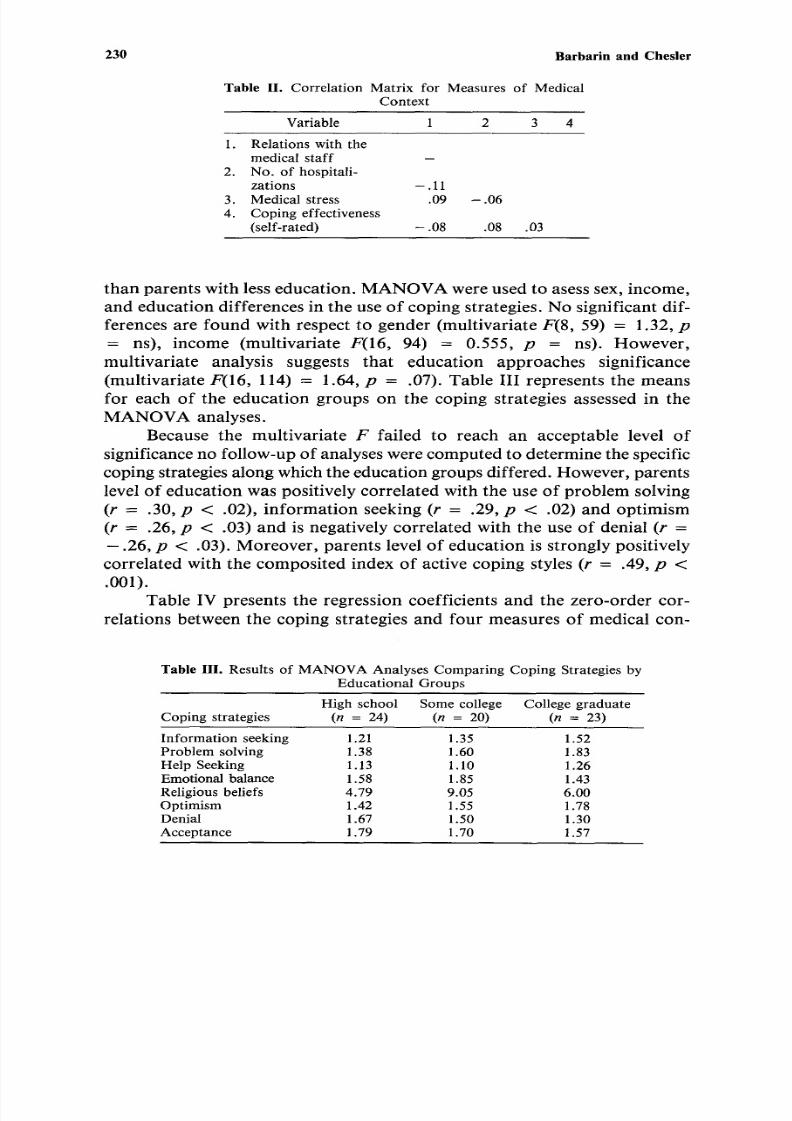
inconsistent with passive acceptance of the situation. Table II presents the
correlations among the four measures of medical context. None of the cor-
relations is significant.
Demographics, Coping Strategies, and Medical Context
In order to assess the effects of potentially mediating variables, cor-relations or chi-square were computed between demographic variables and
measures of medical context. Demographic and situational variables tested
include the amou nt of medical stress, time spent by parents in the hospital,
numbe r of child hospitalizations, diagnostic of ca tegory of the child, gender,
education, and income. A significant correlation was found between educa-
tion and the quality of relations with medical staf f (r = - . 4 3 , p = .0002).
More highly educated parents reported poo rer relations with the medical staff
Table I. Pearson Product-Moment Correlation Matrix for Parental Coping Strategies
Coping strategy 1 2 3 4 5 6 7
1. Informationseeking2. Problem solving -.023. Optimism - .02 .074. Informal
help-seeking .00 .00 .135. Acceptance -.18 -.36 .05 .106. Denial .06 .05 -.09 -.177. Maintenance of
emotional balance .06 .14 .03 - . 118. Relianceonreligious beliefs .19 -.06 .09 -.14
- .06
.04 - .01
.13 .09 .03
7/28/2019 The Medical Context of Parental Coping With Childhood Cancer 1
http://slidepdf.com/reader/full/the-medical-context-of-parental-coping-with-childhood-cancer-1 10/15
2 3 0 B a r b a r i n a n d C h e s l e r
T a b l e I I . C o r r e l a t i o n M a t r i x f o r M e a s u r e s o f M e d i c a l
C o n t e x t
V a r i a b l e 1 2 3 4
1 . R e l a t i o n s w i t h t h e
m e d i c a l s t a f f2 . N o . o f h o s p i t a l i-
z a t i o n s - . 11
3 . M e d i c a l s t r e s s . 0 9
4 . C o p i n g e f f e c t iv e n e s s
( se l f - r a t e d ) - . 08
- .0 6
.0 8 .0 3
t h a n p a r e n t s w i t h le ss e d u c a ti o n . M A N O V A w e r e u s e d t o a se ss s ex , in c o m e ,
a n d e d u c a t i o n d i f f e r e n c e s i n t h e u s e o f c o p i n g s t r a te g i es . N o s i g n i f ic a n t d i f-
f e r e n c e s a r e f o u n d w i t h r e s p e c t t o g e n d e r ( m u l t i v a r i a t e F ( 8 , 5 9 ) = 1 .3 2 , p- - n s ) , i n c o m e ( m u l t i v a r i a t e F ( 1 6 , 9 4 ) = 0 . 5 5 5 , p = n s ) . H o w e v e r ,
m u l t i v a r i a t e a n a l y s i s s u g g e s t s t h a t e d u c a t i o n a p p r o a c h e s s i g n i f i c a n c e
( m u l t i v a r i a t e F ( 1 6 , 1 1 4) = 1 .6 4 , p = . 0 7) . T a b l e I II r e p r e s e n t s t h e m e a n s
f o r e a c h o f th e e d u c a t i o n g r o u p s o n t h e c o p i n g s t r a te g i e s a ss e ss e d in t h e
M A N O V A a n a l y s e s .
B e c a u s e t h e m u l t i v a r i a t e F f a i l e d t o r e a c h a n a c c e p t a b l e l e v e l o f
s i g n if ic a n c e n o f o l l o w - u p o f a n a l y s es w e r e c o m p u t e d t o d e t e r m i n e t h e s p e ci fi c
c o p i n g s t ra t eg i e s a l o n g w h i c h t h e e d u c a t i o n g r o u p s d i f f e r e d . H o w e v e r , p a r e n t s
l ev e l o f e d u c a t i o n w a s p o s i t iv e l y c o r r e l a t e d w i t h t h e u s e o f p r o b l e m s o l v in g
( r = . 3 0 , p < . 0 2 ), i n f o r m a t i o n se e k i n g ( r = . 2 9 , p < . 0 2) a n d o p t i m i s m
( r = . 2 6 , p < . 0 3 ) a n d i s n e g a t i v e l y c o r r e l a t e d w i t h th e u s e o f d e n i a l ( r =
- . 26 , p < . 03 ). M o r e o v e r , p a r e n t s l e v el o f e d u c a t i o n i s s t r o n g l y p o s i t i v e l y
c o r r e l a t e d w i t h th e c o m p o s i t e d i n d e x o f a c ti v e c o p i n g s t y le s ( r = . 49 , p <
.001) .
T a b l e I V p r e s e n t s th e r e g r e s s i o n c o e f f ic i e n t s a n d t h e z e r o - o r d e r c o r -
r e l a t io n s b e t w e e n th e c o p i n g s t r a te g i e s a n d f o u r m e a s u r e s o f m e d i c a l c o n -
T a b l e I II . R e s u l ts o f M A N O V A A n a l y s e s C o m p a r i n g C o p i n g S t r at e g ie s b y
E d u c a t i o n a l G r o u p s
H i g h s c h o o l S o m e c o l le g e C o l l e g e g r a d u a t e
C o p i n g s t r a t e g i e s ( n = 2 4 ) ( n = 2 0 ) ( n = 2 3 )
I n f o r m a t i o n s e e k i n g 1 .2 1 1 .3 5 1 .5 2
P r o b l e m s o l v i n g 1 .3 8 1 .6 0 1 .8 3
H e l p S e e k i ng 1 .13 1 .10 1 .26
Em ot i on a l ba l a nc e 1 .58 1 .85 1 .43
R e l i g i o u s b e l i e f s 4 . 7 9 9 . 0 5 6 . 0 0O pt i m i sm 1 .42 1 .55 1 .78
De nia l 1 .67 1 .50 1 .30
A c c e p t a n c e 1 . 7 9 1 .7 0 1 .5 7

7/28/2019 The Medical Context of Parental Coping With Childhood Cancer 1
http://slidepdf.com/reader/full/the-medical-context-of-parental-coping-with-childhood-cancer-1 11/15
T h e C o n t e x t o f C o p i n g
T a ble I V . R e g r e s s i o n C o e ff i c ie n t s a n d Z e r o - O r d e r C o r r e l a t i o n s B e t w e e n C o p i n g
S t r a t e g y , E d u c a t i o n , a n d M e a s u r e s o f M e d i c a l C o n t e x t
2 3 1
C r i t e r i o n m e a s u r e s
P a r e n t - C o p i n g
H o s p i t a l i - M e d i c a l s t a f f e f f e c t i v e-V a r i a b l e z a t i o n s t re s s r e l a t i o n s n e s s
C o p i n g s t r a te g y
I n f o r m a t i o n s e e k i n g . 05 . 01 - . 1 3 . 0 0
P r o b l e m s o l v in g - . 0 1 . 08 - . 2 4 a - . 0 5
H e l p s e e k i n g - . 1 8 . 0 4 - . 0 4 . 08
E m o t i o n a l b a l a n c e . 0 9 - . 0 6 - . 1 3 - . 05
R e l i g i o u s b e l i e f s - . 0 7 . 1 5 . 1 8 - . 1 7
O p t i m i s m - . 0 4 - . 0 6 - . 0 6 . 0 9
D e n i a l . 0 2 - . 0 8 . 0 3 .2 6 ~
A c c e p t a n c e - . 2 4 a . 0 6 . 4 8 b . 1 4
E d u c a t i o n - . 1 8 - . 1 7 - . 4 3 c . 0 8
M u l t i p l e r . 3 2 . 2 1 . 6 5 . 3 8
F v a l u e . 9 0 . 3 8 4 . 7 6 1 . 3 6
~ p _< .05 .
b p < . 0 1 .
~ p _ . 0 0 1 .
t e x t u s e d a s c r i t e r ia i n t h e m u l t i p l e r e g r e s s i o n a n a l y s e s . T h e c o p i n g s t r a t e g i e s
a s a g r o u p d o n o t s i g n i f ic a n t l y r e l a te to h o s p i t a l i z a t io n , F ( 8 , 6 5 ) = 0 . 9 0 ,
p = ns , pa ren ta l med ica l s t re ss , F (8 , 65) - - 0 .38 , p = ns) , o r se l f - ra ted co p-
i n g e f f e c t i v e n e s s , F ( 8 , 6 5 ) -- 1 . 36 . H o w e v e r , c o p i n g s t r a t e g i es a r e s t r o n g l y
r e l a t e d t o t h e q u a l i t y o f r e l a ti o n s w i t h m e d i c a l s t a f f , F ( 9 , 5 7 ) = 4 . 7 6 , p =
.0001 .
T h e s e d a t a p r o v i d e m o d e s t e v i d e n c e o f s o m e r e l a t i o n s h i p s b e t w e e n
m e a s u r e s o f t h e m e d i ca l c o n t e x t o f c o p i n g a n d p a r e n t s ' u s e o f s p e c if ic co p -
i n g s t r a t e g i e s . A l t h o u g h p a r e n t s ' r e p o r t s o f d i s e a s e - r e l a t e d s t r e s s d o e s n o t
d e m o n s t r a t e a s i g n i f ic a n t r e la t i o n s h i p w i t h a n y o f th e c o p i n g s t r at e g ie s , i t
a p p e a r s t h a t a s t h e n u m b e r o f h o s p i t a li z a t io n s i n c r e a s es , p a r e n t s a r e le ss li k e ly
t o e m p l o y a c c e p t a n c e a s a c o p i n g s t r a te g y . P a r e n t s r e p o r t s o f q u a l i ty o f r e la -
t i o n s w i t h m e d i c a l s t a f f is p o s i ti v e l y c o r r e l a t e d w i t h a c c e p t a n c e a n d n e g a t i v e l y
c o r r e l a t e d w i t h p r o b l e m - s o l v i n g .
T h e r e a l s o i s a s i g n i f ic a n t p o s i t iv e c o r r e l a t i o n b e t w e e n d e n i a l a n d s e lf -
e v a l u a t e d c o p i n g e f f e c t iv e n e s s . P e r h a p s p a r e n t s f e el t h e y a r e c o p i n g b e t t e r
-to t h e e x t e n t t h e y c a n d e n y t h e s e r i o u s n e s s o f t h e i r c h i l d 's i l ln e s s a n d i ts i m -
p l i c a t i o n s , b u f f e r i n g t h e m s e l v e s f r o m p a i n f u l r e a l i t i e s .
The r e su l t s o f t he mu l t ip l e r e g r e s s ion o f c op ing s t r a t e g ie s on r e l a t ions
w i t h m e d i c a l s t a f f a r e p r e s e n t e d i n T a b l e V . I n o r d e r t o c o n t r o l f o r t h e
m e d i a t i n g r o l e e d u c a t i o n m a y h a v e i n t h e r e l a ti o n s h i p b e t w e e n c o p i n g s ty le s
a n d r e l a ti o n s w i t h t h e m e d i c a l s ta f f , e d u c a t i o n w a s i n c l u d e d a m o n g t h e p r e d i c -
7/28/2019 The Medical Context of Parental Coping With Childhood Cancer 1
http://slidepdf.com/reader/full/the-medical-context-of-parental-coping-with-childhood-cancer-1 12/15
232 Barbarin and Chesler
Table V. Multiple Regressions using Quality of Relations with
Medical Staff as the Criterion and Coping Strategies and Educa-
tion as the Predictors
Partial Beta
Variable correl ation coefficients t value
Coping strategy
Info rmat ion seeking .10 0.90 0.73
Pro ble m solving .09 0.78 0.50
Help seeking -. 10 - 1.26 -0 .7 4
Em ot io na l bal anc e - .28 - 1.82 - 2.16 ~
Religi ous beliefs .10 0.25 0.79
Opti mism .09 0.60 0.65
Den ia l - . 06 -0 .46 -0 .46
Acce pta nce .45 3.99 3.83 b
Ed uc at io n - .44 - 2.11 - 3.68 b
ap ___ .05.
bp _< .01.
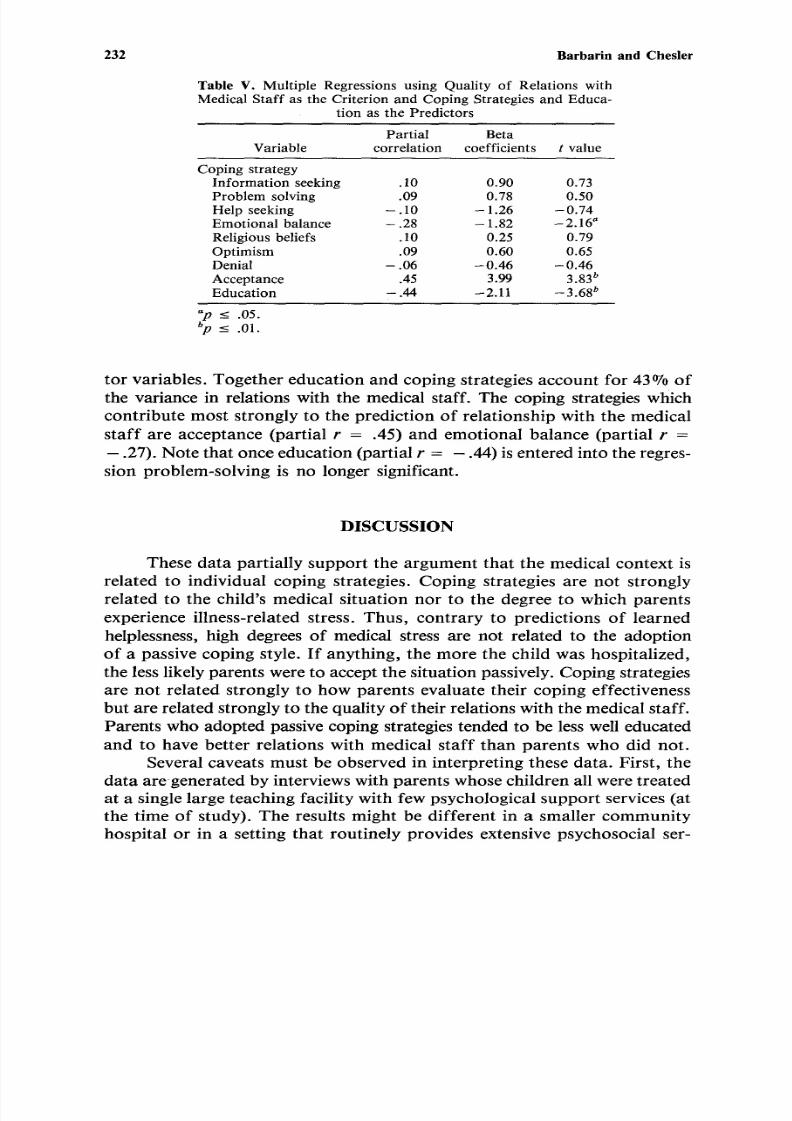
t o r v a r ia b le s . T o g e t h e r e d u c a t i o n a n d c o p i n g s tr a te g ie s a c c o u n t f o r 4 3 % o f
the variance in relat ions with the medical staff. The coping strategies which
con t r ib u te m os t s t rong ly to the p red ic t ion o f re l a t ionsh ip wi th the med ica l
s t a f f a re accep tance (pa r t ia l r = .45 ) and em ot iona l ba l ance (pa rt i a l r =
- .27). No te tha t once edu cat i on (part ial r = - .44) is entere d into the regres-
s ion problem-solv ing i s no longer s igni f icant .
D I S C U S S I O N
These da t a pa r t i a l ly suppor t t he a rgumen t t ha t t he med ica l con tex t i s
re la ted to indiv idual coping s t ra tegies . Coping s t ra tegies are not s t rongly
re l a t ed to the ch i ld ' s med ica l s i t ua t ion no r t o the deg ree to wh ich pa ren t s
exper i ence i l lness - re l a ted s t ress . T hus , con t ra r y to p red ic t ions o f l ea rned
helplessness, high degrees of medical st ress are not related to the adoption
of a pass ive cop ing s ty l e. I f any th ing , t he mo re the ch i ld was hosp i t a l i zed ,
the less l ikely pare nts were to ac cept the si tuat io n passively. Cop ing strategies
a re no t re l a t ed s t rong ly to how pa ren t s eva lua t e the i r cop ing e f fec t iveness
but are re la ted s t rongly to the qual i ty of the i r re la tions wi th the medica l s ta ff .
Parents who adopted passive coping strategies tended to be less well educated
and to have be t t e r re l a t ions wi th med ica l s t a f f t han pa ren t s w ho d id no t .
Severa l cavea t s mus t be obse rve d in in t e rp re t ing these da t a . F i r s t, t he
da ta a re gene ra t ed by in t erv i ews w i th pa ren t s whose ch i ld ren a l l were t rea t ed
at a s ingle la rge teaching fac i l i ty wi th few ps ycho logica l sup po rt serv ices (a t
the t ime o f s tudy) . The re su l t s migh t be d i f fe ren t i n a sma l l e r communi tyhosp i t a l o r i n a se t t i ng tha t rou t ine ly p rov ides ex tens ive psychosoc ia l se t -
7/28/2019 The Medical Context of Parental Coping With Childhood Cancer 1
http://slidepdf.com/reader/full/the-medical-context-of-parental-coping-with-childhood-cancer-1 13/15
The Contex t o f Coping 233
vices. Thus as the medical context itself varies, parents' reactions to the con-
text may vary as well.
Second, the coping indices are derived inductively from clusters of
parents's responses to open-ended questions rather than from explicitly struc-
tured ratings of coping. The approach adopted has the advantage ofphenomenological validity, insofar as parents described what they did.
However it imposes a degree of structure that parents did not bring to their
self-descriptions. It also relies upon retrospective reports o f how parents felt
and what they did. These reports may well involve selective memory and
distortion.
In spite of these cautions, it is important to explain why relatively passive
or acquiescent coping strategies may be associated with favorable relation-
ships with the medical care staff. Perhaps parents with good medical rela-
tionships have less need or desire to exert active control over the medicalsituation and thus view acceptance of what cannot be changed as an effec-
tive coping strategy. For their part, doctors and other medical staff may find
it easier to be supportive of parents who are passive rather than active (Taylor,
1979) and may subtly reinforce passive styles through contingent approval
and attention. It is especially interesting that parents with higher levels of
education report poorer relations with the medical staff than parents with
lesser levels of education. To be sure, these same parents reported greater
use of precisely those coping strategies that broke from passive patient norms
(more information seeking, more problem solving, and less denial). Perhaps
parents with higher status and more active coping strategies are more threaten-
ing to medical staffs, harder to deal with, harder to control, harder to relate
with harmoniously. Because parents with higher levels of education are closer
to the professional status of the medical staff they may be less willing to be
compliant and to "sit still" in the face of questionable staff behaviors
and attitudes. Perhaps too they are more likely to see clearly and discuss
openly the uncertain grounds on which all treatment for cancer rests.
These findings on coping effectiveness indicate that parents' evalua-
tions of their own coping are most highly associated with the use of denial
as a strategy. In highly stressful situations parents may feel satisfied if they
are simply able to keep on going and to ward off excessive pessimism by
moderate amounts of denial. Interpreted in this light, moderate amounts of
denial can be a healthy and functional response. Lazarus (1981) noted that
denial can be detrimental when it reduces vigilance to imminent threats and
delays adaptive responding but it may also preserve morale and hope through
selective avoidance of pessimistic information. The ability to put things out
of their mind may permit parents to return to apparent normality and to
triumph over continual worry and despair. Moreover, Featherstone (1980)
and Wortman and Dunkel-Schetter (1979) observed that medical staf f

7/28/2019 The Medical Context of Parental Coping With Childhood Cancer 1
http://slidepdf.com/reader/full/the-medical-context-of-parental-coping-with-childhood-cancer-1 14/15
234 Barbarin and Ches ler
m e m b e r s a n d c lo s e f r i e n d s o f t e n p r e f e r p e o p l e w i t h c a n c e r t o b e u p b e a t a n d
t o h a n d l e t h e c ri s i s w i t h e q u a n i m i t y . P a r e n t s w h o a r e p r e o c c u p i e d m a y d i s a p -
p o i n t t h e ir f r ie n d s a n d e x p e r ie n c e d i s a p p r o v a l a n d w i t h d r a w a l f r o m t h e m .
T h e m e d i c a l s t a f f 's p r e f e r e n c e f o r p a s s iv e p a r e n t / p a t i e n t c o p i n g s ty le s
m a y n o t b e c o n d u c i v e t o e f f e c t i v e l o n g - t e r m a d j u s t m e n t f o r s o m e p a t i e n t sa n d t h e i r f a m i l i e s . B r i c k m a n e t a l . ( 19 8 2) a n d o t h e r s c r i t ic i z e d t h e t r a d i t i o n a l
m e d i c a l m o d e l b e c a u s e o f t h e a s y m m e t r i c a l s t a f f - p a t i e n t r e l a t i o n s h i p s i n
w h i c h t h e s t a f f u n i l a t e r a l l y e s t a b l is h t h e r u l es g o v e r n i n g b e h a v i o r i n t h a t s e t -
t i n g a n d p a t i e n t s a r e e x p e c t e d t o a d o p t p a s s i v e ro l e s ( A n t o n o v s k y , 1 98 0) .
E m e r g i n g t r e n d s i n th e t r e a t m e n t o f c h i l d h o o d c a n c e r , s u c h a s t h e
s k y r o c k e t i n g f i n a n c ia l b u r d e n o n p a r e n t s , i n c r e a s e d li f e e x p e c t a n c y , a n d
r e l i a n c e o n o u t p a t i e n t t r e a t m e n t , a r e l ik e l y t o i n c r e a s e t h e n e e d f o r p a r e n t s
t o m o n i t o r m e d i c a l a n d p s y c h o s o c i a l se r v i c e s a n d t o p r o v i d e a d d i t i o n a l c a r e
o v e r a n e x t e n d e d t i m e p e r io d . N e w p a r t n e r s h i p s a m o n g p a r e n t s a n d m e d i c a lp r o f e s s i o n a l s r e q u i r e b o t h t o e x p e r i m e n t w i t h c o m p a t i b l e f o r m s o f s u p p o r t
a n d e d u c a t i o n f o r a c t i v e p a r e n t r o l e s i n t h e m e d i c a l c a r e o f i ll c h i l d r e n .
R E F E R E N C E S
American Cancer Society. (1982). Cancer fac t s and f igures . New York : Author .Antono vosky , A. (1980). Health, stress and coping. San Francisco: Jossey-Bass.Barbarin, O. (1983). Coping with ecological transitions by blac k families: a psychosocial model.
J o u r n a l o f C o m mu n i t y P s y c h o lo g y , 1 1, 308-322.Billings, A ., & M oos, R. (1981). The r ole of coping responses and social resources in attenuating
the stress of life events. Journa l o f Behaviora l Medicine, 4 , 139-157.Binger, C., Ab lin, A., Feuerstein, R., K ushner, J ., Zu ker, S., & Mikelsen, C. (1969). Childhood
leukemia emot iona l impac t on pa t ien t and family . New Eng land Journa l o f Med ic ine ,280, 44-418.
Brehm, S. (1965). Th e application o f social ps ych olo gy to clinical practice. Washing ton , DC:Hemisphere Press.
Brickman, P. , Rabinowitz , V ., Karuza, J . , Coates , D ., Cohn , E. , & Kidder, L. (1982). Modelsof helping and coping. Amer ican Psycho log is t , 32 , 368-384.
Cassile th , B. , & Ham ilton, J . (1979). Learning to care for the cancer patient: the s tudent dilem -
ma. In B. Cassileth (Ed.), The canc er patient: social and m edical aspects o f care.Phi lade lph ia : Lea & Feb iger .Chesler, M ., B arbarin , O., Chesler, J . , Hughes , D., & Lebo , J . (1981). Roles of inform al net-
works and medical care organizations . In Help ing fam i l ie s cope wi th ch i ldhood cancer :prosp ects fo r collaboration. An n A rbo r: Univers ity of Michigan, Center for Researchon Social Organizations, CRSO W orking pap er #243, 1981.
Coyne, J., & Holroyd, K. (1982). Stress, coping and illness: a transactional perspective. InT. M illon, C. Green, & R. M eagher (Eds.), Ha ndb ook o f c linica l hea lth psycho logy .New York: Plenum Press .
DiM atteo, M . R. (1979). A socia l-psychological analysis o f phy sic ian-patient rapp ort . Journa l
of Social Issues, 35(1), 12-23.Desmo nd, H . (1980). Two families: an intensive obse rvatio n study . In J. Kellerman (Ed.),
Psychological aspects o f cancer. Springfie ld: C C Thomas.Dohrenwend, B., & Dohrenwend, B. (1974). Stressful life events. New York: Wiley.Dohrenwend, B . S., Krasnoff, L ., Askenasy, A. R ., & Dohrenwend, B. P. (1978). Exemplification
of a me thod for scaling l ife events : the P ER I l ife events scale . J o u r n a l o f He a l th a n dSoc ial Behavior, 19, 205-229.
7/28/2019 The Medical Context of Parental Coping With Childhood Cancer 1
http://slidepdf.com/reader/full/the-medical-context-of-parental-coping-with-childhood-cancer-1 15/15
The Context of Coping 235
Featherstone, H. (1980). A dif ference in the family• New York: Basic Books.Fried man , S. B. , Chodo ff , P . , M ason, J . , & Ha mb urg , D. (1977). Behavioral observ at ions on
parents ff-nticipating the death of a child. In A. Monat & R. Lazarus (Eds.), Stress and
coping (pp. 349-374). New York: Co lum bia Universi ty Press .
Friedson, E. (1970). Profession al dominance: the social s tructure o f m edical care. New York:
Ather ton Press .Futter man , E. , & Hoff ma n, I . (1973). Cris is and adapta t ion in the famil ies of fatal ly i ll children.
In J . A ntho ny & C. Koupern ick (Eds) . The ch i ld in h i s fami ly : the impact o f death and
disease (Vol. 2). New York: Wiley.Holmes, T. H. , & Rahe, R. H. (1967). The social readjustment rat ing scale . J ourna l o f
Psych osom atic Research, 11, 213-218.
Kubler-Ross, E. (1978). On death and dying. New York: Macmil lan.Kupst , M., Schulm an, J . , Honig, G. , Ma urer , H. , Mo rgan , E. , & Foc htm an, D. (1982). Fami-
ly coping with chi ldhood leukemia: one year af ter diagnosis . Journal o f Pedia tr ic
Psychology, 7, 157-67.Lazarus, R., (1966). Psychological s tress and the coping process. New York: McGraw-Hil l .Lazarus, R. (1981). The costs and bene fi ts of denial . In J . Spinet ta & P. Deasy-Spinet ta (Eds.),
Liv ing wi th ch i ldhood cancer (pp. 50-67). St. Louis: MO: C. V. Mosby.Lazarus, R. S. , & Launier , R. (1978). Stress-related t ransac t ions between persons and environ-
ment . In L. S. Perum & M. Lewis (Eds.) , Perspect ives in interact ionalpsychology (pp.
287-327)• New York: Plenum Press.McCubbin, H. , & Pat terson, J . M. (1982). Family adaptat ion to cr ises . In H. I . McCubbin,
A. E. Cauble, & J . M. Pat terson (Eds.) , Family s tress coping and social support .
Springfield, IL: C C Thomas.
McC ubbin, H. I . , & Pat terson, J . M . (1983). The fam ily s tress process: the double AB CX model
of ad jus tment and adapta t ion . In H. I . McCub bin , M. B. Sussman, & J . M. P a t te rson
(Eds.), Social stress and the fam ily . New York: Hawor th Press .
Seligman, M. (1975,). Helplessness. San Franc isco: F reeman.Spinet ta , J . , Swarner , J . , & Sheposh, J . (1981). Effect ive parenta l coping following the death
of a chi ld from cancer . Journal o f Pedia tr ic Psychology , 6 , 251-263.Stone, G. (1979). Pat ie nt comp liance and the role of the expert . Journa l o f Social lssues, 35(1) ,
34-59.Taylor, S. (1979). Ho spital-pa tient beh avio r reactance, helplessness, or control? Journal o f Soc ia l
Issues, 35(1), 156-184.Taylor , S. (1983). A djustm ent to threa tening events: a theory o f cognitive adaptat io n. American
Psychologist , 38, 1161-1163.Vaux, K. (1977). Life threatening disease in children. In J. Van Eyes (Ed.), The truly cured
child. Balt imore: Universi ty Park Press .
W ort ma n, C . B., & Dunkel-Schetter, C. (1979). Interp erson al relationships in cancer: A the oretical
analysis• Journa l o f Social Issues, 35, 120-154.