Embed Size (px)
Citation preview
Sports Med 2005; 35 (3): 235-256REVIEW ARTICLE 0112-1642/05/0003-0235/$34.95/0
2005 Adis Data Information BV. All rights reserved.
The Mechanisms of Massage andEffects on Performance, MuscleRecovery and Injury PreventionPornratshanee Weerapong,1 Patria A. Hume1 and Gregory S. Kolt2
1 New Zealand Institute of Sport and Recreation Research, Division of Sport and Recreation,Faculty of Health and Environmental Sciences, Auckland University of Technology,Auckland, New Zealand
2 Faculty of Health and Environmental Sciences, Auckland University of Technology,Auckland, New Zealand
ContentsAbstract . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2351. Types of Massage . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2372. The Possible Mechanisms of Massage . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 237
2.1 Biomechanical Mechanisms . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2382.1.1 Passive Stiffness . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2382.1.2 Active Stiffness . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2382.1.3 Joint Range of Motion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 238
2.2 Physiological Mechanisms . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2402.2.1 Increased Skin and Muscle Temperature . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2402.2.2 Increased Blood Flow . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2402.2.3 Hormones . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2422.2.4 Parasympathetic Activity . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 242
2.3 Neurological Mechanisms . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2422.3.1 Neuromuscular Excitability and the Hoffman Reflex . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2422.3.2 Pain and Muscle Spasm . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 243
2.4 Psychophysiological Mechanisms . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2432.4.1 Anxiety . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2432.4.2 Relaxation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2452.4.3 Recovery from Fatigue . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 245
2.5 Summary of the Mechanisms of Massage . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2453. The Evidence for Massage on Performance, Recovery or Muscular Injury Prevention . . . . . . . . . . . . 246
3.1 The Effects of Massage on Performance . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2463.2 The Effects of Massage on Recovery . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 247
3.2.1 Performance Recovery . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2473.2.2 Blood Lactate Removal . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 247
3.3 The Effects of Massage in Preventing Muscular Injury . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2473.3.1 Delayed-Onset Muscle Soreness . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 247
3.4 Summary of the Evidence for Massage Improving Performance, Enhancing Recovery orPreventing Muscular Injury . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 252
4. Conclusions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2535. Recommendations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 253
Many coaches, athletes and sports medicine personnel hold the belief, based onAbstractobservations and experiences, that massage can provide several benefits to thebody such as increased blood flow, reduced muscle tension and neurological
236 Weerapong et al.
excitability, and an increased sense of well-being. Massage can produce mechani-cal pressure, which is expected to increase muscle compliance resulting inincreased range of joint motion, decreased passive stiffness and decreased activestiffness (biomechanical mechanisms). Mechanical pressure might help toincrease blood flow by increasing the arteriolar pressure, as well as increasingmuscle temperature from rubbing. Depending on the massage technique, mechan-ical pressure on the muscle is expected to increase or decrease neural excitabilityas measured by the Hoffman reflex (neurological mechanisms). Changes inparasympathetic activity (as measured by heart rate, blood pressure and heart ratevariability) and hormonal levels (as measured by cortisol levels) followingmassage result in a relaxation response (physiological mechanisms). A reductionin anxiety and an improvement in mood state also cause relaxation (psychologicalmechanisms) after massage. Therefore, these benefits of massage are expected tohelp athletes by enhancing performance and reducing injury risk. However,limited research has investigated the effects of pre-exercise massage on perform-ance and injury prevention.
Massage between events is widely investigated because it is believed thatmassage might help to enhance recovery and prepare athletes for the next event.Unfortunately, very little scientific data has supported this claim. The majority ofresearch on psychological effects of massage has concluded that massage produc-es positive effects on recovery (psychological mechanisms). Post-exercise mas-sage has been shown to reduce the severity of muscle soreness but massage has noeffects on muscle functional loss. Notwithstanding the belief that massage hasbenefits for athletes, the effects of different types of massage (e.g. petrissage,effleurage, friction) or the appropriate timing of massage (pre-exercise vspost-exercise) on performance, recovery from injury, or as an injury preventionmethod are not clear. Explanations are lacking, as the mechanisms of eachmassage technique have not been widely investigated. Therefore, this articlediscusses the possible mechanisms of massage and provides a discussion of thelimited evidence of massage on performance, recovery and muscle injury preven-tion. The limitations of previous research are described and further research isrecommended.
Massage has been used for rehabilitation and ty, and an increased sense of well-being. There isrelaxation for thousands of years around the world. limited scientific evidence, however, to support theRecent research from the UK showed that in the past use of massage for enhancing performance, enhanc-11 years, massage treatment was administered for ing recovery from injury, or for preventing muscularapproximately 45% of the total time in physiothera- injury. There is a relative lack of good studies orpy treatment.[1] Massage is used in general ap- information on massage and its potential to influ-proaches, such as preparation for competition, be- ence muscle recovery, injury prevention and physi-tween competitions and in assisting recovery from
cal performance. Many claims are made about mas-competition, rather than treatment for specificsage, but few have any empirical data to back themproblems.[1] The large proportion of massage appli-up, and what little data there are tend to point morecation in sports events is due to many coaches andto the limitations of massage than to any significantathletes holding the belief, based on observationseffects. Rather, the possible mechanisms and theand experiences, that massage can provide severaleffects of massage usually result from authors’ spec-benefits to the body such as increased blood flow,
reduced muscle tension and neurological excitabili- ulations based on general biomechanical, physiolog-
2005 Adis Data Information BV. All rights reserved. Sports Med 2005; 35 (3)

The Mechanisms and Effects of Massage 237
ical or psychological knowledge. More scientific • The article may have discussed the possiblemechanisms of massage in relation to biome-data on the benefits of massage are required.chanical and/or neuromuscular properties ofThis literature review outlines possible mecha-muscle, sport performance, rate of injury andnisms of massage (biomechanical, physiological,muscle soreness.neurological and psychophysiological), and evalu-
• The article may have been a review of previousates the evidence for the benefits of massage inresearch.improving performance, enhancing recovery or
preventing muscular injury. 1. Types of MassageLiterature was located using three computer
Massage has been defined as “a mechanical ma-databases (PubMed, SPORT Discus and ProQuestnipulation of body tissues with rhythmical pressure5000 International) in addition to manual journaland stroking for the purpose of promoting health andsearches. The computer databases provided accesswell-being”.[2] Classic Western massage, or Swed-to biomedical and sport-oriented journals, serialish massage, is the most common form of massagepublications, books, theses, conference papers andcurrently used around the world for athletes withrelated articles published since 1964. The key searchpurported clinical advantages (see table I). There arephases used included: ‘sport massage’, ‘massage’,a number of techniques in existence, and their use
‘performance’, ‘sport injury’, ‘delayed onset muscledepends on the experience of the therapist and the
soreness’, ‘injury prevention’, ‘range of motion’ and intended clinical advantage desired. The majority of‘muscle stiffness’. Articles not published in English research has used a combination of Western tech-nor in scientific journals, nor articles that focused on niques to investigate the effects of massage, with aa specific type of massage (such as connective tissue few studies having used other techniques such asmassage, accupressure), nor articles that focused on myofascial trigger point massage.the effects of massage in special populations, werenot included in this review. The criteria for inclusion 2. The Possible Mechanisms of Massagewere:
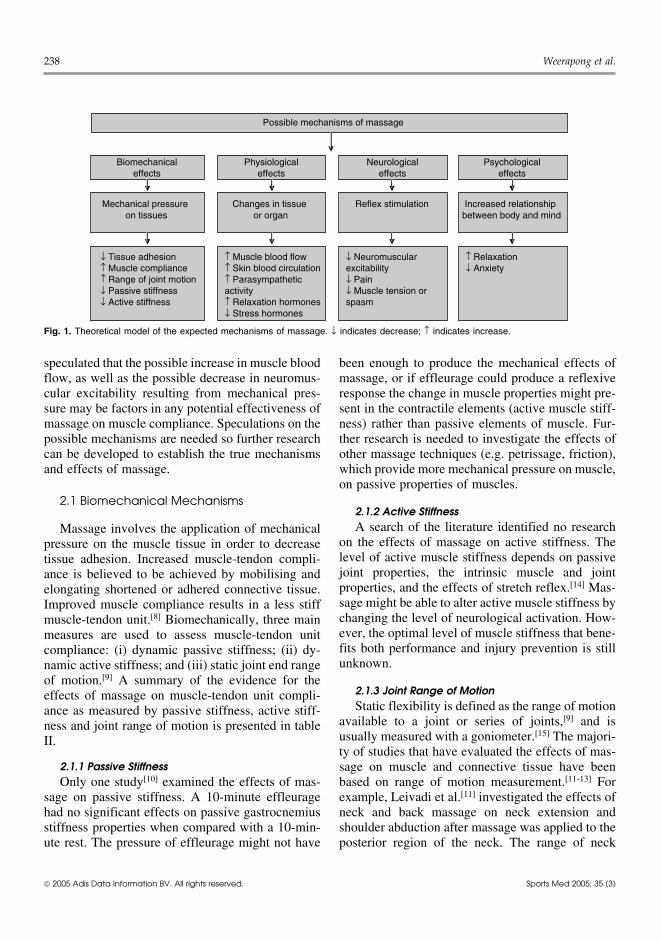
The effects of massage are most likely produced• The article must have used normal, healthy par- by more than one mechanism.[3-6] A theoretical
ticipants. Age, sex and fitness differences were model of how biomechanical, physiological, neuro-not excluding factors. logical and psychological mechanisms[6,7] may be
• The article must have used Swedish-type mas- affected by massage is presented in figure 1. Assage as an intervention. The massage technique stated earlier, the majority of these mechanisms aresuch as effleurage and petrissage were not ex- speculated by the authors with little empirical datacluding factors. to support the statement. For example, it has been
Table I. Summary of classic Western massage techniques
Technique Definition Application Suggested clinical advantageEffleurage Gliding or sliding movement over Beginning of a session Stimulate the parasympathetic
the skin with a smooth continuous During a break after applying nervous system and evoke themotion[3] a specific technique relaxation response
End of each session Enhance venous return
Petrissage Lifting, wringing, or squeezing of soft Following effleurage Mobilise deep muscle tissue ortissues in a kneading motion, or the skin and subcutaneous tissuepressing or rolling of the tissues Increase local circulationunder or between the hands[3] Assist venous return
Friction An accurately delivered penetrating Used for a specific purpose Treat muscle spasm or break uppressure applied through the such as to reduce muscle spasm adhesions from old injuriesfingertips[4]
Tapotement Various parts of the hand striking Finishing a section of the body Stimulate the tissues either bythe tissues at a fairly rapid rate[5] Before and during a competition direct mechanical force or by
reflex action
2005 Adis Data Information BV. All rights reserved. Sports Med 2005; 35 (3)
238 Weerapong et al.
Possible mechanisms of massage
Biomechanicaleffects
Mechanical pressure on tissues
↓ Tissue adhesion↑ Muscle compliance ↑ Range of joint motion ↓ Passive stiffness↓ Active stiffness
Physiologicaleffects
Changes in tissue or organ
↑ Muscle blood flow↑ Skin blood circulation ↑ Parasympathetic activity↑ Relaxation hormones↓ Stress hormones
Neurologicaleffects
Reflex stimulation
↓ Neuromuscular excitability↓ Pain↓ Muscle tension or spasm
Psychologicaleffects
Increased relationship between body and mind
↑ Relaxation↓ Anxiety
Fig. 1. Theoretical model of the expected mechanisms of massage. ↓ indicates decrease; ↑ indicates increase.
speculated that the possible increase in muscle blood been enough to produce the mechanical effects offlow, as well as the possible decrease in neuromus- massage, or if effleurage could produce a reflexivecular excitability resulting from mechanical pres- response the change in muscle properties might pre-sure may be factors in any potential effectiveness of sent in the contractile elements (active muscle stiff-massage on muscle compliance. Speculations on the ness) rather than passive elements of muscle. Fur-possible mechanisms are needed so further research ther research is needed to investigate the effects ofcan be developed to establish the true mechanisms other massage techniques (e.g. petrissage, friction),and effects of massage. which provide more mechanical pressure on muscle,
on passive properties of muscles.2.1 Biomechanical Mechanisms
2.1.2 Active StiffnessA search of the literature identified no researchMassage involves the application of mechanical
on the effects of massage on active stiffness. Thepressure on the muscle tissue in order to decreaselevel of active muscle stiffness depends on passivetissue adhesion. Increased muscle-tendon compli-joint properties, the intrinsic muscle and jointance is believed to be achieved by mobilising andproperties, and the effects of stretch reflex.[14] Mas-elongating shortened or adhered connective tissue.sage might be able to alter active muscle stiffness byImproved muscle compliance results in a less stiffchanging the level of neurological activation. How-muscle-tendon unit.[8] Biomechanically, three mainever, the optimal level of muscle stiffness that bene-measures are used to assess muscle-tendon unitfits both performance and injury prevention is stillcompliance: (i) dynamic passive stiffness; (ii) dy-unknown.namic active stiffness; and (iii) static joint end range
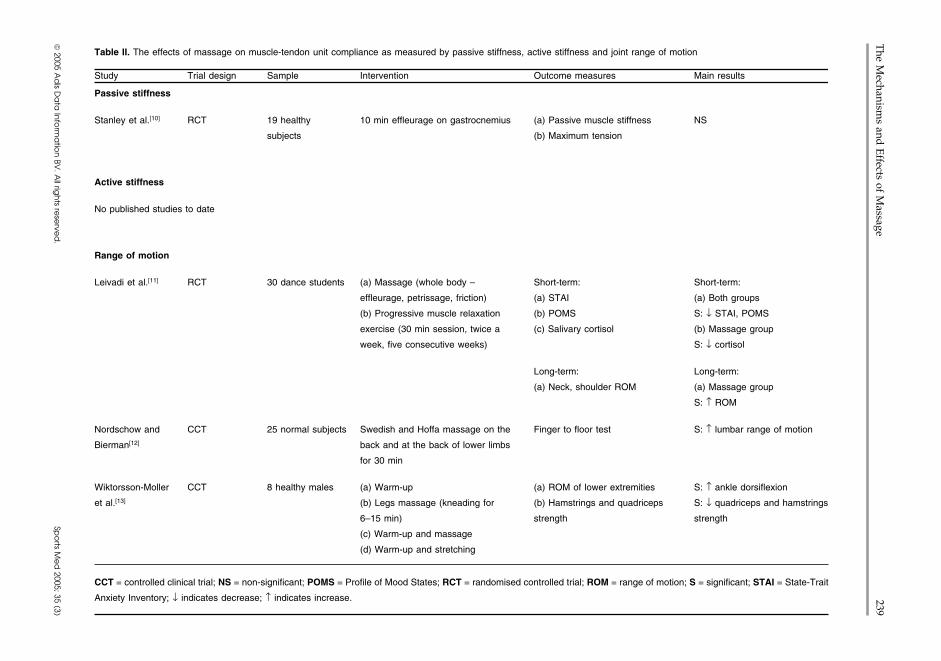
of motion.[9] A summary of the evidence for the2.1.3 Joint Range of Motioneffects of massage on muscle-tendon unit compli-Static flexibility is defined as the range of motionance as measured by passive stiffness, active stiff-
available to a joint or series of joints,[9] and isness and joint range of motion is presented in tableusually measured with a goniometer.[15] The majori-II.ty of studies that have evaluated the effects of mas-
2.1.1 Passive Stiffness sage on muscle and connective tissue have beenOnly one study[10] examined the effects of mas- based on range of motion measurement.[11-13] For
sage on passive stiffness. A 10-minute effleurage example, Leivadi et al.[11] investigated the effects ofhad no significant effects on passive gastrocnemius neck and back massage on neck extension andstiffness properties when compared with a 10-min- shoulder abduction after massage was applied to theute rest. The pressure of effleurage might not have posterior region of the neck. The range of neck
2005 Adis Data Information BV. All rights reserved. Sports Med 2005; 35 (3)
The M
echanisms and
Effects of M
assage239
2005 A
dis D
ata
Info
rma
tion
BV. A
ll righ
ts rese
rved
.Sp
orts M
ed
2005; 35 (3)
Table II. The effects of massage on muscle-tendon unit compliance as measured by passive stiffness, active stiffness and joint range of motion
Study Trial design Sample Intervention Outcome measures Main results
Passive stiffness
Stanley et al.[10] RCT 19 healthy 10 min effleurage on gastrocnemius (a) Passive muscle stiffness NS
subjects (b) Maximum tension
Active stiffness
No published studies to date
Range of motion
Leivadi et al.[11] RCT 30 dance students (a) Massage (whole body – Short-term: Short-term:
effleurage, petrissage, friction) (a) STAI (a) Both groups
(b) Progressive muscle relaxation (b) POMS S: ↓ STAI, POMS
exercise (30 min session, twice a (c) Salivary cortisol (b) Massage group
week, five consecutive weeks) S: ↓ cortisol
Long-term: Long-term:
(a) Neck, shoulder ROM (a) Massage group
S: ↑ ROM
Nordschow and CCT 25 normal subjects Swedish and Hoffa massage on the Finger to floor test S: ↑ lumbar range of motion
Bierman[12] back and at the back of lower limbs
for 30 min
Wiktorsson-Moller CCT 8 healthy males (a) Warm-up (a) ROM of lower extremities S: ↑ ankle dorsiflexion
et al.[13] (b) Legs massage (kneading for (b) Hamstrings and quadriceps S: ↓ quadriceps and hamstrings
6–15 min) strength strength
(c) Warm-up and massage
(d) Warm-up and stretching
CCT = controlled clinical trial; NS = non-significant; POMS = Profile of Mood States; RCT = randomised controlled trial; ROM = range of motion; S = significant; STAI = State-Trait
Anxiety Inventory; ↓ indicates decrease; ↑ indicates increase.

240 Weerapong et al.
extension motion was limited by anterior muscles temperature quickly returned to baseline level[17]
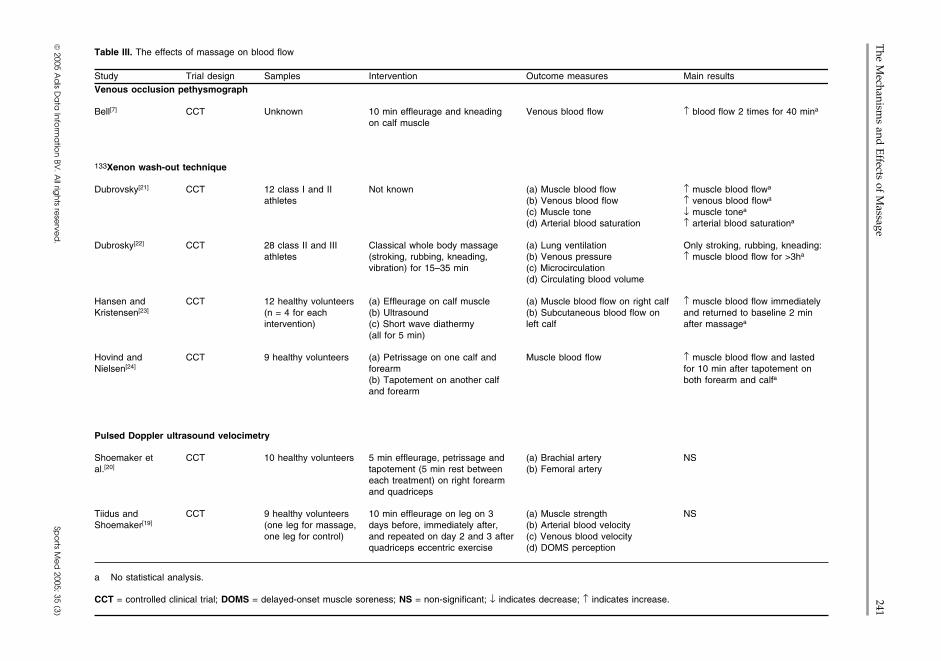
and ligaments and bony contact between spinous and muscle temperature did not increase in deepprocesses,[15] therefore, neck extension was not a muscle temperature (deeper than 2.5cm).[18] Thisgood outcome measure for the effectiveness of mas- leads to the implication that massage (effleuragesage in this study. In another study,[12] finger to floor technique) may not be suitable as a preparation and/distances increased significantly after massage of or preventative strategy for exercise.the back and lower extremities; however, this studydid not provide an appropriate control group and did 2.2.2 Increased Blood Flownot blind the examiner to whether the subject had One expected benefit of massage with respect tomassage or control. The massage therapist measured enhancement of athletic performance is the increasethe distance between the fingers and the floor, which in blood circulation. A variety of controlled clinicalmay have caused bias during measurement. When trials have used venous occlusion pethysmography,the effects of massage on lower extremity range of the 133Xenon wash-out technique, or pulsed Dop-motion were compared with the other pre-exercise pler ultrasound velocimetry to examine the effectsactivities such as warm-up and stretching,[13] mas- of massage on blood flow (see table III). Althoughsage increased only ankle dorsiflexion range of mo- several authors have agreed that massage could in-tion while stretching significantly increased all low- crease blood flow,[7,21-24] study results have beener extremity range of motion measurements. Thus, inconclusive largely because of their design limita-the effectiveness of massage on range of motion is tions. Besides small sample size[7,23,24] most of thesestill questioned, especially when compared with studies had no reported statistical analysis,[7,21-24]
more economical techniques like stretching. nor did they use a control group.[7,21-24] These limita-tions make it hard to differentiate the changes from
2.2 Physiological Mechanisms normal variations. More importantly, the venousocclusion pethysmograph and 133Xenon wash-out
2.2.1 Increased Skin and Muscle Temperature techniques used in these studies had their own limi-Superficial skin friction increases local heating, tations. The venous occlusion pethysmograph
and consequently, causes hyperaemia within the demonstrated underestimation of blood flow due tomassaged area. Local heating increases local blood the inflation of the cuff and was very sensitive tocirculation.[16] There is published evidence that skin movement artefacts.[19,20] The changes of blood flowand muscle temperature increased after massage ap- could not be expressed quantitatively.[23] Moreover,plication (effleurage technique). Longworth[17] re- the venous occlusion pethysmograph techniqueported an increase in skin temperature during a could not be used to measure blood flow during6-minute back massage, but skin temperature re- actual massage.[25] The 133Xenon wash-out tech-turned to baseline level after 10 minutes. Recently, nique overestimated blood flow because of the localDrust et al.[18] reported an increase in skin and trauma from injection of the tracer.[19,20,24,25] Pulsedintramuscular temperature (at 1.5 and 2.5cm) of the Doppler ultrasound has been used to investigatevastus lateralis muscle irrespective of massage dura- muscle blood flow and has indicated that manualtion (5, 10 and 15 minute of effleurage). Even massage did not affect blood flow in the muscle afterthough massage was shown to increase skin[17] and treatment of the muscle.[19,20] However, the ultra-intramuscular temperature,[18] such effects on skin sound used in these studies detected changes in theand intramuscular temperature might not be relevant large artery and vein but did not detect microcircula-to muscle blood flow. tion in muscle that could be affected by massage. In
It is still questionable whether increased skin and summary, there is a lack of confirming evidence thatintramuscular temperature[18] without increasing massage does anything significant (with a few ex-muscle blood flow[19,20] and muscle compliance[10] ceptions) for the blood flow physiological response.would be beneficial to enhance performance or pre- The only studies to look at blood flow with limitedvent injuries. The other limitations evident from technique problems[19,20] have shown no change ineffleurage technique administration were that skin total muscle blood flow. This indicates that there is
2005 Adis Data Information BV. All rights reserved. Sports Med 2005; 35 (3)
The M
echanisms and
Effects of M
assage241
2005 A
dis D
ata
Info
rma
tion
BV. A
ll righ
ts rese
rved
.Sp
orts M
ed
2005; 35 (3)
Table III. The effects of massage on blood flow
Study Trial design Samples Intervention Outcome measures Main resultsVenous occlusion pethysmograph
Bell[7] CCT Unknown 10 min effleurage and kneading Venous blood flow ↑ blood flow 2 times for 40 mina
on calf muscle
133Xenon wash-out technique
Dubrovsky[21] CCT 12 class I and II Not known (a) Muscle blood flow ↑ muscle blood flowa
athletes (b) Venous blood flow ↑ venous blood flowa
(c) Muscle tone ↓ muscle tonea
(d) Arterial blood saturation ↑ arterial blood saturationa
Dubrosky[22] CCT 28 class II and III Classical whole body massage (a) Lung ventilation Only stroking, rubbing, kneading:athletes (stroking, rubbing, kneading, (b) Venous pressure ↑ muscle blood flow for >3ha
vibration) for 15–35 min (c) Microcirculation(d) Circulating blood volume
Hansen and CCT 12 healthy volunteers (a) Effleurage on calf muscle (a) Muscle blood flow on right calf ↑ muscle blood flow immediatelyKristensen[23] (n = 4 for each (b) Ultrasound (b) Subcutaneous blood flow on and returned to baseline 2 min
intervention) (c) Short wave diathermy left calf after massagea
(all for 5 min)
Hovind and CCT 9 healthy volunteers (a) Petrissage on one calf and Muscle blood flow ↑ muscle blood flow and lastedNielsen[24] forearm for 10 min after tapotement on
(b) Tapotement on another calf both forearm and calfa
and forearm
Pulsed Doppler ultrasound velocimetry
Shoemaker et CCT 10 healthy volunteers 5 min effleurage, petrissage and (a) Brachial artery NSal.[20] tapotement (5 min rest between (b) Femoral artery
each treatment) on right forearmand quadriceps
Tiidus and CCT 9 healthy volunteers 10 min effleurage on leg on 3 (a) Muscle strength NSShoemaker[19] (one leg for massage, days before, immediately after, (b) Arterial blood velocity
one leg for control) and repeated on day 2 and 3 after (c) Venous blood velocityquadriceps eccentric exercise (d) DOMS perception
a No statistical analysis.
CCT = controlled clinical trial; DOMS = delayed-onset muscle soreness; NS = non-significant; ↓ indicates decrease; ↑ indicates increase.

242 Weerapong et al.
likely little real effect of massage on muscle blood students in a nursing school.[17] The participantsflow (microcirculatory changes excepted). were massaged on the back for 6 minutes using a
slow stroke technique (effleurage). Heart rate, blood2.2.3 Hormones pressure and skin temperature increased after theMechanical pressure of massage might stimulate massage, indicating an increase in autonomic arous-
parasympathetic activity as shown by reducing sali- al level. The galvanic skin response increased, indi-va cortisol levels (an indirect measure of parasym- cating a lower level of sympathetic stimulation. Thepathetic activity). Changes in hormonal levels (sero- inconsistency in responses of the psychophysiologi-tonin and cortisol) after massage have been reported cal parameters might be due to individuals having amostly in specific conditions such as patients with unique response pattern. The participants in thelow back pain,[26] HIV positive patients[27] and de- study were healthy females and were not in a stress-pressed adolescent mothers,[28] which are beyond ful situation, so it may have been difficult to show athe scope of this literature review. A reduction of great relaxation response.saliva cortisol (stress hormones) in dance students In another study,[36] there were no significanthas also been reported.[11] The dancers, who were changes in blood pressure, pulse and temperaturerandomly assigned to massage or relaxation therapy after a 30-minute Swedish back massage in ninegroups, received treatment for five consecutive female medical students 1 day before an academicweeks. Saliva cortisol levels were investigated after examination. Only respiratory rate was significantlythe session on the first and last days of the study. reduced. These results might support the uniqueBoth groups reported less anxiety and depressed response pattern or simply mean that massage couldmood after their sessions, but only the massage activate only some parameters indicating parasym-group showed a decrease in cortisol levels. A re- pathetic responses in healthy female participants.duced pre-participation anxiety (nervousness) aftermassage may have large implications for perform-
2.3 Neurological Mechanismsance. The mechanisms responsible for reducing cor-tisol levels after massage application are still un-
2.3.1 Neuromuscular Excitability and theknown as the evidence for cortisol changes is weak.Hoffman Reflex
2.2.4 Parasympathetic Activity Massage is believed to stimulate sensory recep-Massage has shown some evidence of increasing tors and decrease muscle tension by reducing neuro-
parasympathetic activity by reducing heart rate, re- muscular excitability as measured by changes in theducing blood pressure,[17,29-32] increasing relaxation Hoffman reflex (H-reflex) amplitude.[37-40] H-reflexsubstances such as endorphins[33] and increasing is considered to be the electrical analogue of theheart rate variability.[34] The majority of research in stretch reflex.[41] In a study by Morelli et al.,[37] one-this area has been conducted in nursing using a hand petrissage for 3–6 minutes decreased H-reflexspecific sequence of massage called ‘back rub’, and amplitude, but the amplitude returned to baselinehas been performed in older people.[29-31] One study levels immediately after the termination of massage.investigated people with chronic pain,[33] while oth- The reduction of H-reflex amplitude was considereder studies used connective tissue massage[33] and to be due to a decrease in spinal reflex excitability[38]
myofascial trigger point massage.[34] Therefore, on- and showed specificity to the muscle group that hadly two studies that met the criteria (participants were received the massage.[40] The inhibitory effects ofhealthy people and Swedish massage was used as massage on the soleus H-reflex amplitude did notthe intervention) were reviewed. originate from mechanical stimulation of cutaneous
mechanoreceptors.[39] Therefore, the inhibitory ef-The effects of back massage on several psy-fects of massage might originate from muscle orchophysiological indices of arousal such as heartother deep tissue mechanoreceptors.rate, blood pressure, galvanic skin response, electro-
myography, skin temperature and psycho-emotional The potent inhibitory effects of massage on neu-response (using the State-Trait Anxiety Inventory romuscular excitability might be one of the explana-[STAI][35]) were examined in 32 female staff and tions for the reduction of muscle tension or spasm
2005 Adis Data Information BV. All rights reserved. Sports Med 2005; 35 (3)

The Mechanisms and Effects of Massage 243
after massage application. However, the reduction 2.4 Psychophysiological Mechanismsof H-reflex after massage (petrissage technique)
Various mechanisms for the cause of the relaxa-might not be the reason for reduction of muscletion response resulting from massage have beenstrength as reported by Wiktorsson-Moller et al.[13]
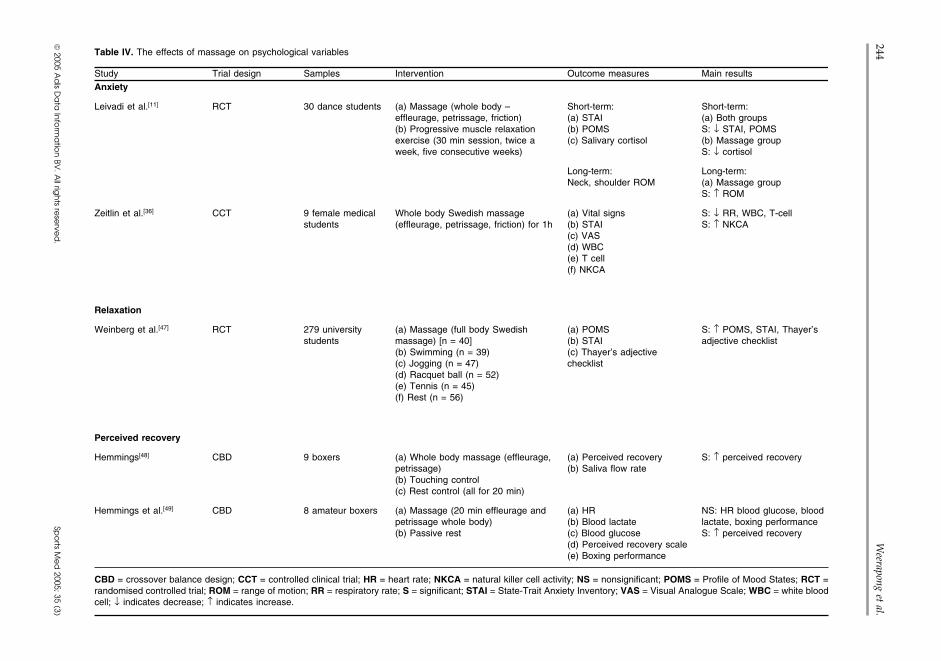
proposed. These include an increase of plasma en-(see section 3.1) because the H-reflex amplitude dorphins,[33] decreased arousal level,[17] decreasedreturned to baseline levels immediately after mas- stress hormone levels[11,26-28] or an activation of thesage termination.[37] Therefore, further research is parasympathetic response.[32,34,46] This section willneeded to investigate the relationship between the focus on the effects of Swedish massage on psycho-neurological effects of massage and performance, emotional responses in normal populations (see ta-and the effects of other types of massage application ble IV for a summary of studies).on neuromuscular excitability.
2.4.1 AnxietyThe majority of research in the psychological2.3.2 Pain and Muscle Spasm
area has reported that massage provided positiveMassage has been applied in order to relieve effects on anxiety. Most studies have used the
pain.[11,26,42-44] The possible responsible mechanisms STAI[35] to measure anxiety. Studies of the effects ofare neurological (gate-control theory), physiological massage on anxiety, however, had several limita-(biochemical substances) and mechanical (realign- tions such as no control group,[36] an inappropriatement of muscle fibres). Massage may reduce pain by control group[11] and small sample size.[36] For ex-
ample, the anxiety levels after being massaged onactivating the neural-gating mechanism in the spinalthe day before an academic examination were as-cord. Tactile information from massage might stim-sessed for nine medical students.[36] The mean STAIulate large fast nerve fibres and then, block thescore decreased significantly after the massage in-smaller, slower nerve fibres that detect pain. Thistervention and the respiratory rate was also signifi-effect presumably results from local lateral inhibi-cantly decreased between pre- and post-massagetion in the spinal cord[45] and explains why touchingmeasures. The small sample size and lack of athe painful area is an effective strategy for relievingcontrol group make the effectiveness of acute single
pain. However, there are no objective data to sup- massage treatments unclear.port this idea. Massage can increase biochemical The long-term effects of a 30-minute massage,substances such as serotonin,[11] which is a neuro- twice a week for four consecutive weeks were ex-transmitter that plays a role in reducing pain.[45]
amined in 30 dance students.[11] A progressive relax-Physiotherapists usually use massage to break the ation therapy group was used for comparison. Both
groups reported lower state anxiety levels and de-vicious cycle that causes muscle spasm, and conse-pressed mood subscale of the Profile of Mood Statesquently, muscle pain. Muscle spasm causes muscle(POMS);[50] however, only the massage group re-pain directly by stimulating mechanosensitive painvealed a significantly lower saliva cortisol levelreceptors or indirectly by compressing the bloodafter the massage session. The study did not state thevessels resulting in ischaemia.[45] Massage mighttime of blood collection, therefore, the cortisol levelhelp to rearrange muscle fibres and increaseshould be interpreted carefully because of the effectsmicrocirculation. The realignment of fibres helps toof circadian rhythm.[45] The progressive relaxation
reduce muscle spasm that stimulates pain receptors therapy was not an appropriate control group as itand helps to reduce the pressure on blood vessels. was an active relaxation technique that the partici-The increase in blood microcirculation helps to in- pants had to carry out by themselves, while massagecrease nutrition to the damaged area. However, there therapy was a passive relaxation technique appliedis no scientific evidence to support these ideas be- by the massage therapist. The relaxation group com-cause massage is unlikely to increase muscle blood pleted their exercises at home by following a record-flow and there is no published study on the effects of ed tape, which raises the issue of compliance to themassage on the realignment of fibres. intervention. Therefore, further studies on the ef-
2005 Adis Data Information BV. All rights reserved. Sports Med 2005; 35 (3)
244W
eerapong et al.
2005 A
dis D
ata
Info
rma
tion
BV. A
ll righ
ts rese
rved
.Sp
orts M
ed
2005; 35 (3)
Table IV. The effects of massage on psychological variables
Study Trial design Samples Intervention Outcome measures Main resultsAnxiety
Leivadi et al.[11] RCT 30 dance students (a) Massage (whole body – Short-term: Short-term:effleurage, petrissage, friction) (a) STAI (a) Both groups(b) Progressive muscle relaxation (b) POMS S: ↓ STAI, POMSexercise (30 min session, twice a (c) Salivary cortisol (b) Massage groupweek, five consecutive weeks) S: ↓ cortisol
Long-term: Long-term:Neck, shoulder ROM (a) Massage group
S: ↑ ROM
Zeitlin et al.[36] CCT 9 female medical Whole body Swedish massage (a) Vital signs S: ↓ RR, WBC, T-cellstudents (effleurage, petrissage, friction) for 1h (b) STAI S: ↑ NKCA
(c) VAS(d) WBC(e) T cell(f) NKCA
Relaxation
Weinberg et al.[47] RCT 279 university (a) Massage (full body Swedish (a) POMS S: ↑ POMS, STAI, Thayer’sstudents massage) [n = 40] (b) STAI adjective checklist
(b) Swimming (n = 39) (c) Thayer’s adjective(c) Jogging (n = 47) checklist(d) Racquet ball (n = 52)(e) Tennis (n = 45)(f) Rest (n = 56)
Perceived recovery
Hemmings[48] CBD 9 boxers (a) Whole body massage (effleurage, (a) Perceived recovery S: ↑ perceived recoverypetrissage) (b) Saliva flow rate(b) Touching control(c) Rest control (all for 20 min)
Hemmings et al.[49] CBD 8 amateur boxers (a) Massage (20 min effleurage and (a) HR NS: HR blood glucose, bloodpetrissage whole body) (b) Blood lactate lactate, boxing performance(b) Passive rest (c) Blood glucose S: ↑ perceived recovery
(d) Perceived recovery scale(e) Boxing performance
CBD = crossover balance design; CCT = controlled clinical trial; HR = heart rate; NKCA = natural killer cell activity; NS = nonsignificant; POMS = Profile of Mood States; RCT =randomised controlled trial; ROM = range of motion; RR = respiratory rate; S = significant; STAI = State-Trait Anxiety Inventory; VAS = Visual Analogue Scale; WBC = white bloodcell; ↓ indicates decrease; ↑ indicates increase.

The Mechanisms and Effects of Massage 245
fects of massage on anxiety need to provide more have been shown during the recovery phase of box-appropriate control groups. ing performances and after a training session.[49,53]
Despite no changes in physiological fatigue indica-2.4.2 Relaxation tors such as blood lactate and heart rate, nine boxersThe effects of massage on relaxation have been reported that massage positively affected the per-
investigated by using valid questionnaires such as ception of recovery following boxing performancethe POMS;[50] however, the use of the POMS for and seemed to be a useful recovery strategy. Theindicating the level of relaxation is questionable as Perceived Recovery scale is a useful questionnairethe questionnaire is composed of six scales: tension, to indicate recovery because it is short and easy todepression, anger, vigour, fatigue and confusion.[50]
understand. However, the Perceived Recovery scaleOnly the tension, vigour and fatigue subscales are has not been widely used in research studies. Toappropriate for relaxation measurement. POMS is date, there is no published article reporting the cor-also considered too long to complete[51] as there are relation between the Perceived Recovery scale and65 items in the original version and 72 items in the physiological markers of fatigue.bipolar version. Therefore, the POMS is not anappropriate questionnaire from which to measure
2.5 Summary of the Mechanisms of Massagerelaxation. Interestingly, there are no questionnairesavailable to allow a direct investigation of the level
Massage is believed to benefit athletes by en-of relaxation.hancing performance and recovery, as well as pro-Weinberg et al.[47] reported a preliminary studymoting relaxation through biomechanical, physio-on the effects of massage on mood enhancement inlogical, neurological and psychological mecha-183 physical education students. Massage interven-nisms. Despite the general belief of the benefits oftion was compared with several physical activitiesmassage, there are limited empirical data on possi-such as swimming, jogging, tennis and racquetball.ble mechanisms of massage. Mechanical pressureThe students completed a battery of psychologicalfrom massage is believed to increase muscle compli-questionnaires before and after each interventionance. Several studies reported an increase in staticincluding the POMS, the State Anxiety Inventoryflexibility, as measured by joint range of motion, but(SAI),[35] and the high and general activation sub-these studies were methodologically flawed.[11-13]
scales from Thayer’s adjective checklist.[52] Interest-One study reported poor effects of massage (effleu-ingly, only the massage and running groups reportedrage technique) on dynamic flexibility as measureda significant positive mood enhancement with sig-by passive stiffness.[10] Studies on physiologicalnificant decreases in tension, confusion, fatigue,mechanisms such as the changes of blood circula-anxiety, anger and depression. Only the massagetion,[19,20] hormonal levels[12] and psychophysiologi-group showed a significant decrease in the Thayer’scal parameters (e.g. blood pressure and hearthigh activation subscale and the SAI scores. In arate)[29-34] are still inconclusive. The explanationssimilar study, Hemmings[53] compared the psycho-might be due to the unique response pattern oflogical effects of massage, lying resting, or touchingindividuals and the variations of massage interven-control using the POMS during boxing training.tions (i.e. massage technique, duration of massageMassage application during training improved theand pressure of massage) used in each study. Thetension and fatigue subscales of the POMS, whicheffects of massage on neurological mechanismsare applicable to measurement of relaxation. Thehave been reported to reduce the amplitude of the H-studies by both Weinberg et al.[47] and Hemmings[53]
reflex;[37-40] however, results were limited to theshowed significant positive psychological effectspetrissage technique. Many studies have reportedattributable to massage despite the mood state of thethat massage can promote relaxation by improvingparticipants.psychophysiological response. Therefore, further
2.4.3 Recovery from Fatigue studies are needed to investigate the biomechanical,Positive perceived psychological benefits of physiological, neurological and psychological
massage using the Perceived Recovery linear scale mechanisms for each massage technique. The re-
2005 Adis Data Information BV. All rights reserved. Sports Med 2005; 35 (3)

246 Weerapong et al.
sults will help to provide appropriate massage appli- 3.1 The Effects of Massage on Performancecations for specific sports purposes.
Sport massage is used both pre- and post-event inan attempt to increase athletes’ performance, over-3. The Evidence for Massage oncome fatigue and help recovery.[54] An increase inPerformance, Recovery or Muscularmuscle blood flow would hasten the delivery ofInjury Preventionoxygen, increase muscle temperature and bufferblood pH, which would then aid in the performance
Sport massage has been used for centuries in an of exercise.[2] Increased muscle blood flow, theoreti-attempt to prevent and cure injuries.[4,6,54,55] Mas- cally, should help to remove waste products aftersage is considered to enhance muscle relaxa-
exercise and should enhance delivery of protein andtion,[12,13] reduce muscle tension[21] and sore-
other nutrients needed for muscle repair.[25] In-ness,[19,56] promote the healing process,[57] and con-creased lymph flow, could, in theory, reduce post-sequently, improve athletic performance.[58-60]
exercise swelling and stiffness by reducing muscleMassage is also thought to provide a soothing, seda-interstitial content and thereby reduce muscle dis-tive, invigorating feeling and can give the athletecomfort.[55] However, there are no data to supportconfidence by the positive reaction that takes placethese ideas, and the few studies on massage andwithin the body.[47-49,53] Massage might be an effec-
tive way to prevent acute injuries resulting from blood flow have shown no increases in blood flow.abnormal tissue conditions (e.g. muscle tears in tight A search of the literature identified only twomuscle) and chronic injuries caused by wear and studies on the effects of pre-exercise massage ontear (e.g. tendinosis)[61] by rearranging the muscle performance. Wiktorsson-Moller et al.[13] found thatfibres.[62] As a result of these suggested benefits,
6–15 minutes of petrissage, with the aim of promot-manual massage may be a useful modality to en-ing relaxation and comfort, reduced musclehance performance and prevent injury for athletesstrength. However, Wiktorsson-Moller et al.[13] usedwho use their muscles vigorously.isokinetic movement to test muscle strength. Re-
Sport massage may help to optimise positive- search has shown that the tests of muscular functionperformance factors such as healthy muscle and
were not suitable to monitor performance.[64] Thereconnective tissues and normal range of motion.[61]
were no relationships between the percentageMassage is used to minimise negative-performancechanges in the tests of muscular function (concentricfactors such as dysfunctional muscle and connectiveand eccentric contraction of isoinertial and isokinet-tissue, restricted range of motion, and pain andic tests) and the changes in performance (sprintinganxiety.[61] Therefore, preventive massage is com-and cycling) after an 8-week weight-training pro-monly recommended to help athletes prepare both
physically and mentally for a forthcoming event.[3] gramme.[64] Another study on the effects of 30 min-In addition, sports massage is believed to decrease utes of pre-exercise whole-body Swedish massageinjury-potential factors. Even though massage has (including effleurage, petrissage and tapotement) inbenefited several injury-risk factors such as in- 14 sprinters[65] showed that mean stride frequenciescreased range of motion,[11-13] reduced pain[42,63] and were not significantly different between massageanxiety,[11,47] there have been no intervention studies
and control groups. However, it should be noted thatto assess the effects of these possible injury preven-
the highest absolute stride frequency was obtainedtion strategies. There is no clear evidence that mas-in the trial immediately following massage. Stridesage can actually improve performance, enhancefrequency needs to be combined with stride lengthrecovery or prevent muscular injury. In addition, theto determine performance. Therefore, the effects ofcost to benefit ratio of massage compared with otherpre-exercise massage on performance are still in-methods such as jogging or stretching has not yet
been investigated. conclusive due to the lack of well controlled studies.
2005 Adis Data Information BV. All rights reserved. Sports Med 2005; 35 (3)

The Mechanisms and Effects of Massage 247
3.2 The Effects of Massage on Recovery a more normal alignment. Nevertheless, there are nodata to support these suggested mechanisms.
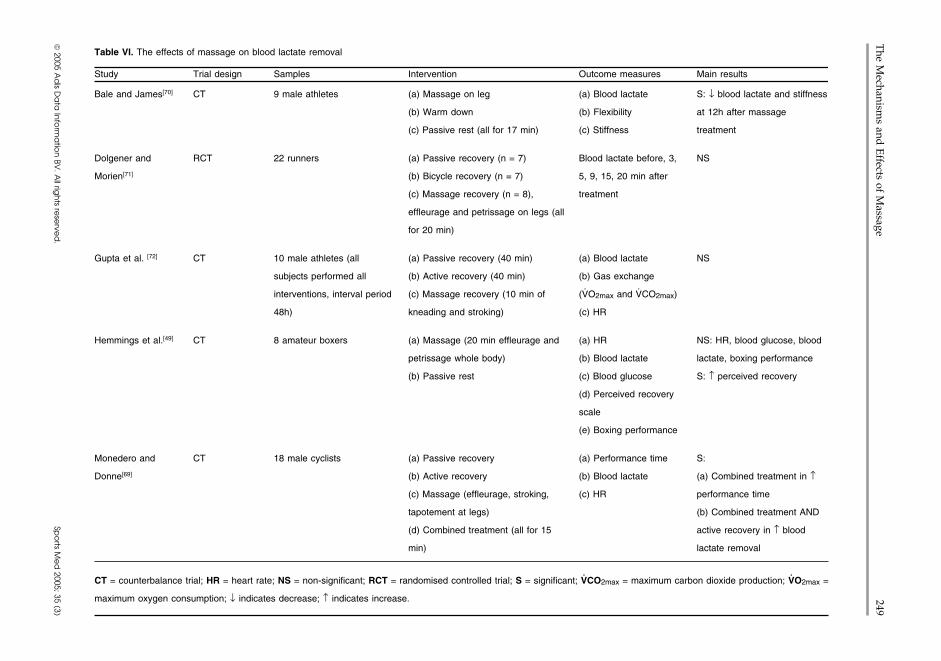
3.2.1 Performance Recovery 3.2.2 Blood Lactate RemovalIt is believed that one of the greatest advantages Blood lactate has been used as a marker for
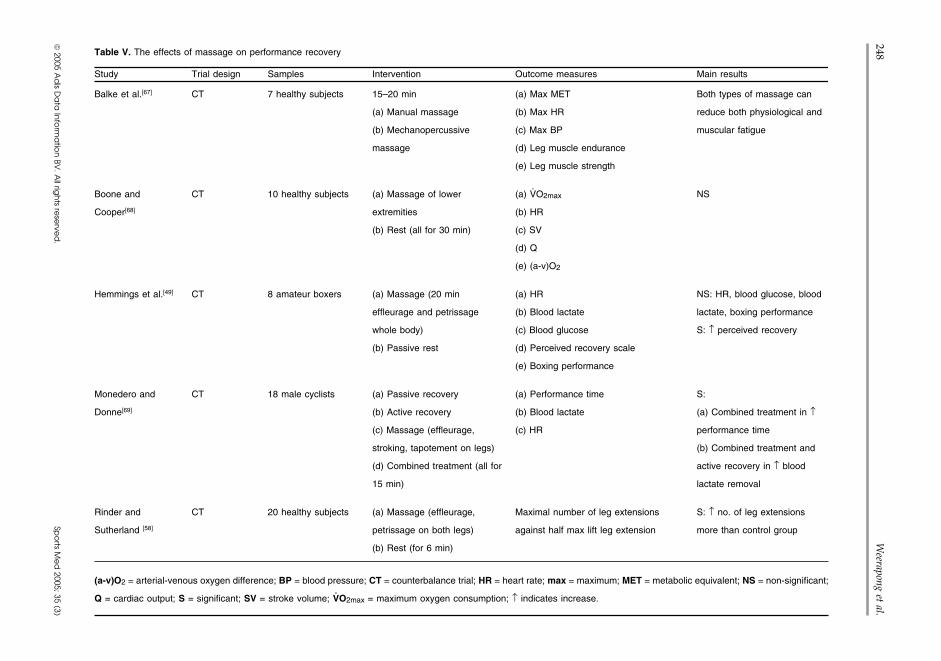
of sport massage is to overcome fatigue and reduce fatigue and recovery.[49,69-72] A summary of the ef-recovery time, especially during periods of competi- fects of massage on blood lactate removal istion, and consequently, enhance performance at the presented in table VI.next event. Even though many elite athletes believe Only one study has reported that massage treat-that massage is an important part of their suc- ment could increase blood lactate removal aftercess,[62,66] the effects of massage itself are still ques- strenuous exercise.[70] Cool-down, however, pro-tioned. Massage can improve some physiological duced a superior blood lactate removal rate thanmarkers[67] but some studies have shown no effect massage therapy. Other studies showed no benefiton any recovery parameters.[49] A summary of the from massage.[49,69,71,72] Therefore, there is little em-effects of massage on performance recovery is pirical evidence to support the effectiveness of mas-presented in table V. sage for blood lactate removal despite participants
To investigate the effects of massage on recov- reporting less fatigue after massage applica-ery, several studies provided massage between sport tion.[48,49,53,69,71,72] If an elevated muscle blood flowsessions. However, there were some limitations in is the aim of treatment then light exercise would bethese studies leading to inconclusive data. For ex- more beneficial than massage.[20,25,55] If psychologi-ample, Monedero and Donne[69] administered com- cal effects of fatigue are to be considered thenbination treatments (active exercise and massage) so massage might provide some benefit. However, nothe true benefits of individual massage treatments studies have compared the psychological effects ofare still unclear. Some studies had problems with massage and cool-down.credible data including small sample size[49,68] andlack of statistical analysis.[67] An appropriate design 3.3 The Effects of Massage in Preventing(such as a crossover design), use of a control group Muscular Injury(placebo treatment), and maximisation of motiva-tion of participants in both control and massage 3.3.1 Delayed-Onset Muscle Sorenessgroups are factors that need to be considered in Delayed-onset muscle soreness (DOMS) is amassage studies in order to minimise psychological very important problem for coaches and athleteseffects. because it causes chronic pain and diminishes mus-
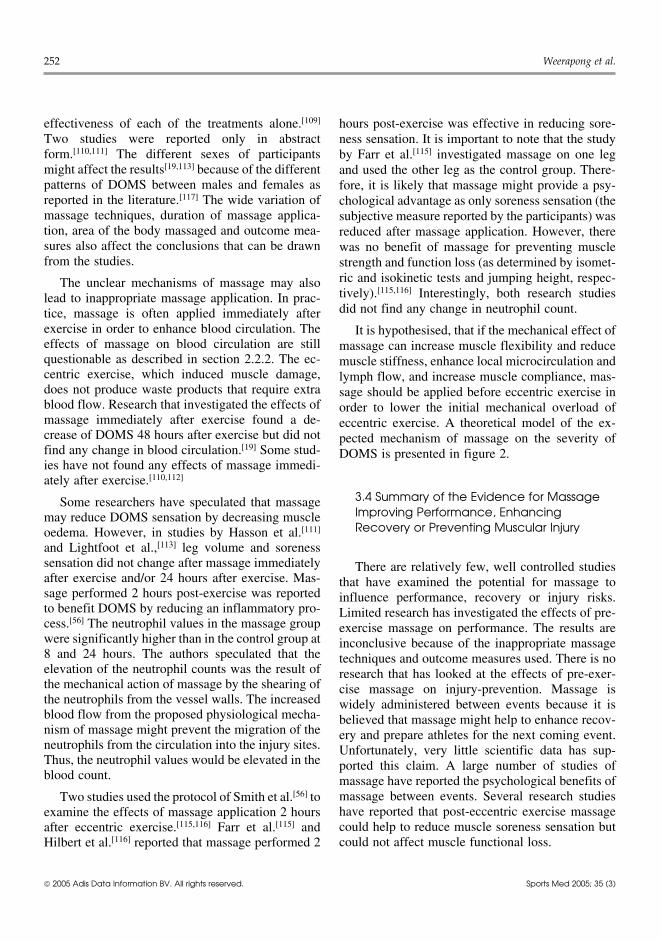
cle function and ability to participate in sport.[73]Curative massage can facilitate soft tissue heal-DOMS commonly occurs between 24 and 72 hoursing in a number of ways. Massage may help reduceafter unaccustomed eccentric exercise.[74-77] Theboth primary oedema and the possibility of seconda-consequences of damage to muscle function includery oedema caused by the pressure of increased fluidprolonged loss of muscle strength,[76,78-81] sorenessin the area of trauma.[6,57] Starkey[57] found thatsensation,[77,80,81] decreased range of motion,[79] in-combination treatments including cold, exercise andcreased muscle stiffness,[77,78] increased resting met-mechanical massage could reduce total time lostabolic rate[82] and perturbed athletic perform-from practice by approximately 2 days when com-ance.[83-86] These changes might increase the risk ofpared with the normal ice, compression and eleva-sports injury.tion treatment. Unfortunately, the published report
showed neither the results section nor the statistical The sequence of DOMS events consists of theanalysis. Therapists apply massage to the injured mechanical stress of exercise on muscle fib-area because they expect massage to improve blood res,[74,75,87-90] causing sarcomeres to rupture[91] fol-circulation to the injured area and, consequently, to lowed by calcium homeostasis disturbance. Thehelp enhance healing. The mechanical pressure from damage of sarcoplasmic reticulum or muscle mem-massage is generally used to treat adherent or con- brane can increase intracellular calcium and triggertracted connective tissue in order to restore fibres to calcium-sensitive pathways.[92,93] Calpain, the calci-
2005 Adis Data Information BV. All rights reserved. Sports Med 2005; 35 (3)
248W
eerapong et al.
2005 A
dis D
ata
Info
rma
tion
BV. A
ll righ
ts rese
rved
.Sp
orts M
ed
2005; 35 (3)
Table V. The effects of massage on performance recovery
Study Trial design Samples Intervention Outcome measures Main results
Balke et al.[67] CT 7 healthy subjects 15–20 min (a) Max MET Both types of massage can
(a) Manual massage (b) Max HR reduce both physiological and
(b) Mechanopercussive (c) Max BP muscular fatigue
massage (d) Leg muscle endurance
(e) Leg muscle strength
Boone and CT 10 healthy subjects (a) Massage of lower (a) V̇O2max NS
Cooper[68] extremities (b) HR
(b) Rest (all for 30 min) (c) SV
(d) Q
(e) (a-v)O2
Hemmings et al.[49] CT 8 amateur boxers (a) Massage (20 min (a) HR NS: HR, blood glucose, blood
effleurage and petrissage (b) Blood lactate lactate, boxing performance
whole body) (c) Blood glucose S: ↑ perceived recovery
(b) Passive rest (d) Perceived recovery scale
(e) Boxing performance
Monedero and CT 18 male cyclists (a) Passive recovery (a) Performance time S:
Donne[69] (b) Active recovery (b) Blood lactate (a) Combined treatment in ↑
(c) Massage (effleurage, (c) HR performance time
stroking, tapotement on legs) (b) Combined treatment and
(d) Combined treatment (all for active recovery in ↑ blood
15 min) lactate removal
Rinder and CT 20 healthy subjects (a) Massage (effleurage, Maximal number of leg extensions S: ↑ no. of leg extensions
Sutherland [58] petrissage on both legs) against half max lift leg extension more than control group
(b) Rest (for 6 min)
(a-v)O2 = arterial-venous oxygen difference; BP = blood pressure; CT = counterbalance trial; HR = heart rate; max = maximum; MET = metabolic equivalent; NS = non-significant;
Q = cardiac output; S = significant; SV = stroke volume; V̇O2max = maximum oxygen consumption; ↑ indicates increase.
The M
echanisms and
Effects of M
assage249
2005 A
dis D
ata
Info
rma
tion
BV. A
ll righ
ts rese
rved
.Sp
orts M
ed
2005; 35 (3)
Table VI. The effects of massage on blood lactate removal
Study Trial design Samples Intervention Outcome measures Main results
Bale and James[70] CT 9 male athletes (a) Massage on leg (a) Blood lactate S: ↓ blood lactate and stiffness
(b) Warm down (b) Flexibility at 12h after massage
(c) Passive rest (all for 17 min) (c) Stiffness treatment
Dolgener and RCT 22 runners (a) Passive recovery (n = 7) Blood lactate before, 3, NS
Morien[71] (b) Bicycle recovery (n = 7) 5, 9, 15, 20 min after
(c) Massage recovery (n = 8), treatment
effleurage and petrissage on legs (all
for 20 min)
Gupta et al. [72] CT 10 male athletes (all (a) Passive recovery (40 min) (a) Blood lactate NS
subjects performed all (b) Active recovery (40 min) (b) Gas exchange
interventions, interval period (c) Massage recovery (10 min of (V̇O2max and V̇CO2max)
48h) kneading and stroking) (c) HR
Hemmings et al.[49] CT 8 amateur boxers (a) Massage (20 min effleurage and (a) HR NS: HR, blood glucose, blood
petrissage whole body) (b) Blood lactate lactate, boxing performance
(b) Passive rest (c) Blood glucose S: ↑ perceived recovery
(d) Perceived recovery
scale
(e) Boxing performance
Monedero and CT 18 male cyclists (a) Passive recovery (a) Performance time S:
Donne[69] (b) Active recovery (b) Blood lactate (a) Combined treatment in ↑
(c) Massage (effleurage, stroking, (c) HR performance time
tapotement at legs) (b) Combined treatment AND
(d) Combined treatment (all for 15 active recovery in ↑ blood
min) lactate removal
CT = counterbalance trial; HR = heart rate; NS = non-significant; RCT = randomised controlled trial; S = significant; V̇CO2max = maximum carbon dioxide production; V̇O2max =
maximum oxygen consumption; ↓ indicates decrease; ↑ indicates increase.
250W
eerapong et al.
2005 A
dis D
ata
Info
rma
tion
BV. A
ll righ
ts rese
rved
.Sp
orts M
ed
2005; 35 (3)
Table VII. The effects of massage on muscle soreness
Study Trial design Samples Intervention Outcome measures Main resultsFarr et al.[115] CT 8 healthy males (one leg 30 min leg massage (effleurage (a) Muscle strength S: ↓ soreness and tenderness
massage, one leg control) and petrissage) 2h after 40 min (b) Plasma CK at 48h post-eccentric exercisetreadmill walk (c) Vertical jump
(d) Soreness(e) Tenderness
Hasson et al.[111] RCT 16 healthy subjects (no (a) Retrograde massage (n = 6) (a) Max isotonic KE NSspecific sex) (b) Placebo massage (n = 5) (b) Max concentric KE
(c) Control (n = 5) (c) Max eccentric KE(treatment 24h post-exercise) (d) Max 1-leg jump
(e) Max 2-leg jump(f) Soreness perception
Hilbert et al. [116] RCT 18 healthy volunteers (a) Swedish massage (7 min of (a) POMS S: ↓ soreness at 48h post-effleurage, 1 min of tapotement, 12 (b) ROM eccentric exercisemin of petrissage) (c) Peak torque (eccentric(b) control (placebo lotion applied contraction)and rest for 20 min) (d) DDSIntervention performed 2h after (e) Neutrophilshamstrings eccentric exercise
Lightfoot et al.[113] RCT 31 healthy volunteers (a) Massage (10 min of petrissage) (a) DOMS scale NS(12M, 19F) [n = 10 for immediately and 24h post-exercise (b) Lower leg volumeeach group] on the left calf muscle (c) CK level
(b) Stretching(c) Control
Rodenburg et al.[109] RCT 50 untrained males (n = 27 (a) Warm-up, stretching, massage (a) DOMS scale S: ↓ DOMS (extensorfor experimental group) (15 min of effleurage, tapotement, (b) Maximal isotonic force muscles), CK, flexed arm
petrissage) (c) Flexion angle of elbow angle(b) Control (d) Extension angle of S: ↑ maximal isotonic force
elbow(e) CK level(f) Mb concentration
Smith et al.[56] RCT 14 untrained males (n = 7 (a) 30 min of effleurage, shaking, (a) Muscle soreness rating S: ↓ DOMS and CKfor each intervention) petrissage, cross-fibre (b) Blood CK, neutrophils, S: ↑ neutrophils
(b) Control cortisolIntervention performed 2h afterbiceps and triceps eccentricexercise
Continued next page
The Mechanisms and Effects of Massage 251
um-activated neutral protease, plays a role in theultrastructural muscle damage.[76] The inflammatoryresponse to damaged muscle fibres causes a transferof fluid and cells to the damaged tissue.[94] Theincreased fluid produces swelling after injury. Neu-trophils and macrophages migrate to the inflam-matory sites and play a role in both the damage andrepair processes.[76] The exact mechanisms to ex-plain how soreness develops and why there is adelay in pain sensation is not fully under-stood.[15,87,95,96]
Several treatments that aim to prevent and/orreduce the severity of muscle damage have beeninvestigated including acupuncture,[97] ultra-sound,[98,99] cryotherapy,[100] compression,[78,101]
anti-inflammatory drugs,[102,103] hyperbaric oxygentherapy,[104] warm-up,[105,106] stretching[106-108] andmassage.[19,56,109-113] These treatments have been ap-plied as a prophylactic and/or a therapeutic interven-tion. However, the benefits of these treatments arestill inconclusive. From a clinical point of view, thetreatment given prophylactically is more desirablefor reducing or preventing injury, and consequently,for producing a reduction in further injuries, chronicpain, cost of injury treatment and time lost fromtraining activities.
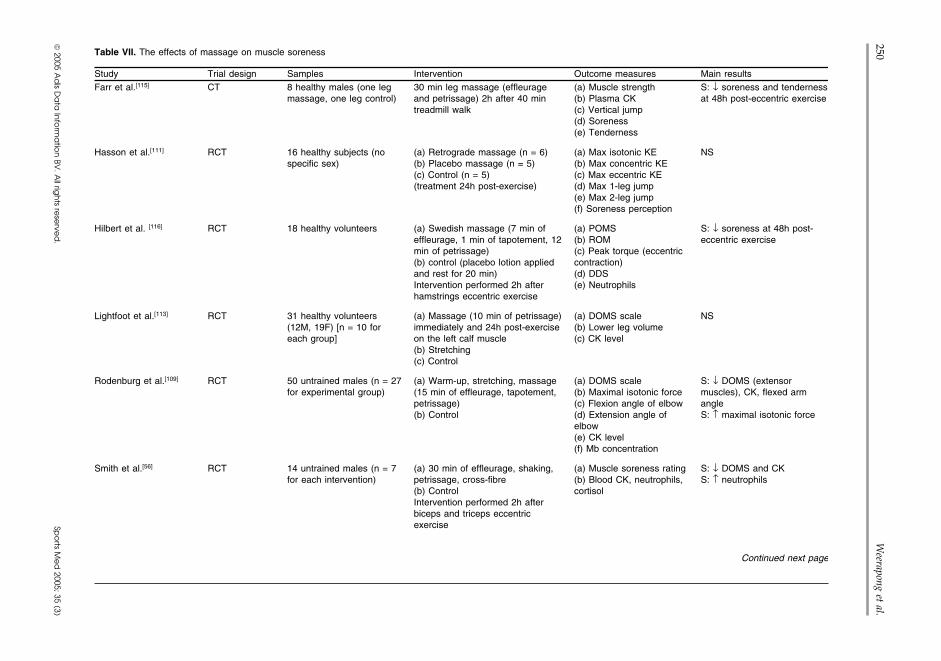
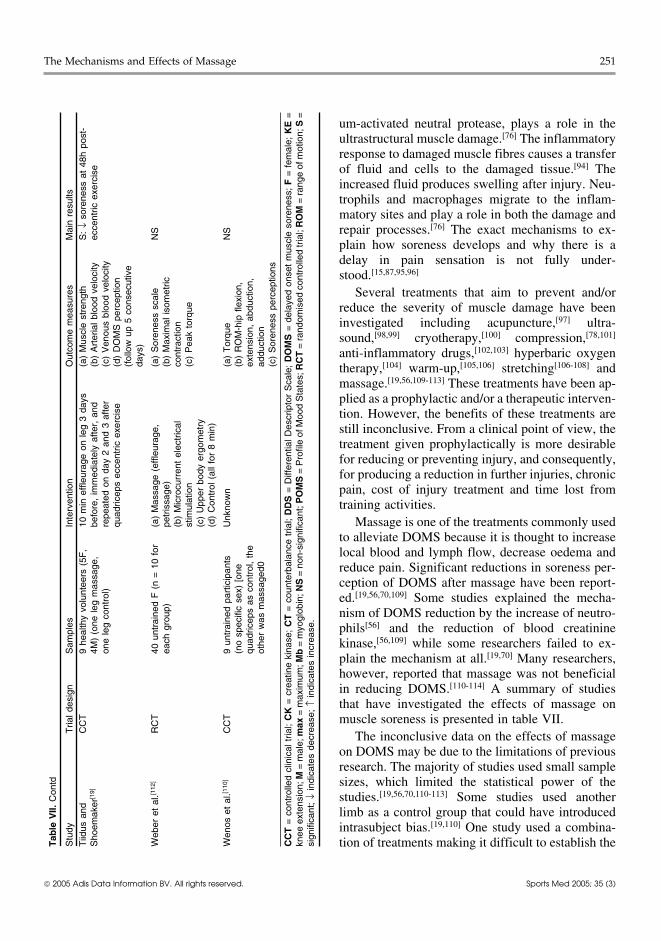
Massage is one of the treatments commonly usedto alleviate DOMS because it is thought to increaselocal blood and lymph flow, decrease oedema andreduce pain. Significant reductions in soreness per-ception of DOMS after massage have been report-ed.[19,56,70,109] Some studies explained the mecha-nism of DOMS reduction by the increase of neutro-phils[56] and the reduction of blood creatininekinase,[56,109] while some researchers failed to ex-plain the mechanism at all.[19,70] Many researchers,however, reported that massage was not beneficialin reducing DOMS.[110-114] A summary of studiesthat have investigated the effects of massage onmuscle soreness is presented in table VII.
The inconclusive data on the effects of massageon DOMS may be due to the limitations of previousresearch. The majority of studies used small samplesizes, which limited the statistical power of thestudies.[19,56,70,110-113] Some studies used anotherlimb as a control group that could have introducedintrasubject bias.[19,110] One study used a combina-tion of treatments making it difficult to establish the
2005 Adis Data Information BV. All rights reserved. Sports Med 2005; 35 (3)
Tab
le V
II. C
ontd
Stu
dyT
rial d
esig
nS
ampl
esIn
terv
entio
nO
utco
me
mea
sure
sM
ain
resu
ltsT
iidus
and
CC
T9
heal
thy
volu
ntee
rs (
5F,
10 m
in e
ffleu
rage
on
leg
3 da
ys(a
) M
uscl
e st
reng
thS
: ↓
sore
ness
at
48h
post
-S
hoem
aker
[19]
4M)
(one
leg
mas
sage
,be
fore
, im
med
iate
ly a
fter,
and
(b)
Art
eria
l blo
od v
eloc
ityec
cent
ric e
xerc
ise
one
leg
cont
rol)
repe
ated
on
day
2 an
d 3
afte
r(c
) V
enou
s bl
ood
velo
city
quad
ricep
s ec
cent
ric e
xerc
ise
(d)
DO
MS
per
cept
ion
(fol
low
up
5 co
nsec
utiv
eda
ys)
Web
er e
t al
.[112
]R
CT
40 u
ntra
ined
F (
n =
10
for
(a)
Mas
sage
(ef
fleur
age,
(a)
Sor
enes
s sc
ale
NS
each
gro
up)
petr
issa
ge)
(b)
Max
imal
isom
etric
(b)
Mic
rocu
rren
t el
ectr
ical
cont
ract
ion
stim
ulat
ion
(c)
Pea
k to
rque
(c)
Upp
er b
ody
ergo
met
ry(d
) C
ontr
ol (
all f
or 8
min
)
Wen
os e
t al
.[110
]C
CT
9 un
trai
ned
part
icip
ants
Unk
now
n(a
) T
orqu
eN
S(n
o sp
ecifi
c se
x) [
one
(b)
RO
M-h
ip f
lexi
on,
quad
ricep
s as
con
trol
, th
eex
tens
ion,
abd
uctio
n,ot
her
was
mas
sage
d0ad
duct
ion
(c)
Sor
enes
s pe
rcep
tions
CC
T =
con
trol
led
clin
ical
tria
l; C
K =
cre
atin
e ki
nase
; C
T =
cou
nter
bala
nce
tria
l; D
DS
= D
iffer
entia
l Des
crip
tor
Sca
le;
DO
MS
= d
elay
ed o
nset
mus
cle
sore
ness
; F
= f
emal
e; K
E =
knee
ext
ensi
on; M
= m
ale;
max
= m
axim
um; M
b =
myo
glob
in; N
S =
non
-sig
nific
ant;
PO
MS
= P
rofil
e of
Moo
d S
tate
s; R
CT
= r
ando
mis
ed c
ontr
olle
d tr
ial;
RO
M =
ran
ge o
f mot
ion;
S =
sign
ifica
nt;
↓ in
dica
tes
decr
ease
; ↑
indi
cate
s in
crea
se.
252 Weerapong et al.
effectiveness of each of the treatments alone.[109] hours post-exercise was effective in reducing sore-Two studies were reported only in abstract ness sensation. It is important to note that the studyform.[110,111] The different sexes of participants by Farr et al.[115] investigated massage on one legmight affect the results[19,113] because of the different and used the other leg as the control group. There-patterns of DOMS between males and females as fore, it is likely that massage might provide a psy-reported in the literature.[117] The wide variation of chological advantage as only soreness sensation (themassage techniques, duration of massage applica- subjective measure reported by the participants) wastion, area of the body massaged and outcome mea- reduced after massage application. However, theresures also affect the conclusions that can be drawn was no benefit of massage for preventing musclefrom the studies. strength and function loss (as determined by isomet-
ric and isokinetic tests and jumping height, respec-The unclear mechanisms of massage may alsotively).[115,116] Interestingly, both research studieslead to inappropriate massage application. In prac-did not find any change in neutrophil count.tice, massage is often applied immediately after
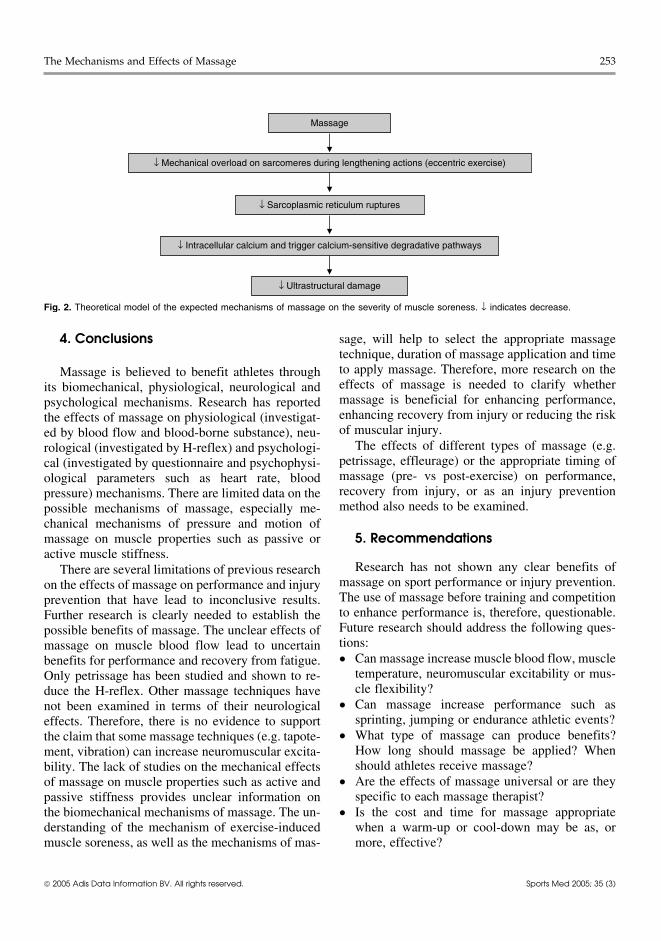
exercise in order to enhance blood circulation. The It is hypothesised, that if the mechanical effect ofeffects of massage on blood circulation are still massage can increase muscle flexibility and reducequestionable as described in section 2.2.2. The ec- muscle stiffness, enhance local microcirculation andcentric exercise, which induced muscle damage, lymph flow, and increase muscle compliance, mas-does not produce waste products that require extra sage should be applied before eccentric exercise inblood flow. Research that investigated the effects of order to lower the initial mechanical overload ofmassage immediately after exercise found a de- eccentric exercise. A theoretical model of the ex-crease of DOMS 48 hours after exercise but did not pected mechanism of massage on the severity offind any change in blood circulation.[19] Some stud- DOMS is presented in figure 2.ies have not found any effects of massage immedi-ately after exercise.[110,112]
3.4 Summary of the Evidence for MassageSome researchers have speculated that massageImproving Performance, Enhancingmay reduce DOMS sensation by decreasing muscleRecovery or Preventing Muscular Injuryoedema. However, in studies by Hasson et al.[111]
and Lightfoot et al.,[113] leg volume and sorenesssensation did not change after massage immediately There are relatively few, well controlled studiesafter exercise and/or 24 hours after exercise. Mas- that have examined the potential for massage tosage performed 2 hours post-exercise was reported influence performance, recovery or injury risks.to benefit DOMS by reducing an inflammatory pro- Limited research has investigated the effects of pre-cess.[56] The neutrophil values in the massage group exercise massage on performance. The results arewere significantly higher than in the control group at inconclusive because of the inappropriate massage8 and 24 hours. The authors speculated that the techniques and outcome measures used. There is noelevation of the neutrophil counts was the result of research that has looked at the effects of pre-exer-the mechanical action of massage by the shearing of cise massage on injury-prevention. Massage isthe neutrophils from the vessel walls. The increased widely administered between events because it isblood flow from the proposed physiological mecha- believed that massage might help to enhance recov-nism of massage might prevent the migration of the ery and prepare athletes for the next coming event.neutrophils from the circulation into the injury sites. Unfortunately, very little scientific data has sup-Thus, the neutrophil values would be elevated in the ported this claim. A large number of studies ofblood count. massage have reported the psychological benefits of
massage between events. Several research studiesTwo studies used the protocol of Smith et al.[56] tohave reported that post-eccentric exercise massageexamine the effects of massage application 2 hourscould help to reduce muscle soreness sensation butafter eccentric exercise.[115,116] Farr et al.[115] andcould not affect muscle functional loss.Hilbert et al.[116] reported that massage performed 2
2005 Adis Data Information BV. All rights reserved. Sports Med 2005; 35 (3)
The Mechanisms and Effects of Massage 253
Massage
↓ Mechanical overload on sarcomeres during lengthening actions (eccentric exercise)
↓ Sarcoplasmic reticulum ruptures
↓ Intracellular calcium and trigger calcium-sensitive degradative pathways
↓ Ultrastructural damage
Fig. 2. Theoretical model of the expected mechanisms of massage on the severity of muscle soreness. ↓ indicates decrease.
4. Conclusions sage, will help to select the appropriate massagetechnique, duration of massage application and timeto apply massage. Therefore, more research on theMassage is believed to benefit athletes througheffects of massage is needed to clarify whetherits biomechanical, physiological, neurological andmassage is beneficial for enhancing performance,psychological mechanisms. Research has reportedenhancing recovery from injury or reducing the riskthe effects of massage on physiological (investigat-of muscular injury.ed by blood flow and blood-borne substance), neu-
The effects of different types of massage (e.g.rological (investigated by H-reflex) and psychologi-petrissage, effleurage) or the appropriate timing ofcal (investigated by questionnaire and psychophysi-massage (pre- vs post-exercise) on performance,ological parameters such as heart rate, bloodrecovery from injury, or as an injury preventionpressure) mechanisms. There are limited data on themethod also needs to be examined.possible mechanisms of massage, especially me-
chanical mechanisms of pressure and motion of5. Recommendationsmassage on muscle properties such as passive or
active muscle stiffness.Research has not shown any clear benefits ofThere are several limitations of previous research
massage on sport performance or injury prevention.on the effects of massage on performance and injuryThe use of massage before training and competitionprevention that have lead to inconclusive results.to enhance performance is, therefore, questionable.Further research is clearly needed to establish theFuture research should address the following ques-possible benefits of massage. The unclear effects oftions:massage on muscle blood flow lead to uncertain• Can massage increase muscle blood flow, musclebenefits for performance and recovery from fatigue.
temperature, neuromuscular excitability or mus-Only petrissage has been studied and shown to re-cle flexibility?duce the H-reflex. Other massage techniques have
• Can massage increase performance such asnot been examined in terms of their neurologicalsprinting, jumping or endurance athletic events?effects. Therefore, there is no evidence to support
• What type of massage can produce benefits?the claim that some massage techniques (e.g. tapote-How long should massage be applied? Whenment, vibration) can increase neuromuscular excita-should athletes receive massage?bility. The lack of studies on the mechanical effects
• Are the effects of massage universal or are theyof massage on muscle properties such as active andspecific to each massage therapist?passive stiffness provides unclear information on
the biomechanical mechanisms of massage. The un- • Is the cost and time for massage appropriatederstanding of the mechanism of exercise-induced when a warm-up or cool-down may be as, ormuscle soreness, as well as the mechanisms of mas- more, effective?
2005 Adis Data Information BV. All rights reserved. Sports Med 2005; 35 (3)
254 Weerapong et al.
11. Leivadi S, Hernandez-Reif M, Field T, et al. Massage therapyIn order to overcome limitations of previous re-and relaxation effects on university dance students. J Dance
search, massage studies should consider these Med Sci 1999; 3 (3): 108-1212. Nordschow M, Bierman W. The influence of manual massagepoints:
on muscle relaxation: effect on trunk flexion. J Am Phys Ther• An appropriate control group should be provided. 1962; 42 (10): 653-7The ideal control group for a massage study 13. Wiktorsson-Moller M, Oberg B, Ekstrand J, et al. Effects of
warming up, massage, and stretching on range of motion andshould be passive therapy where the participantsmuscle strength in the lower extremity. Am J Sports Medreceive the same attention in terms of time from 1983; 11 (4): 249-52
the therapists as the massage group. However, 14. McNair P, Stanley S. Effect of passive stretching and jogging onthe series muscle stiffness and range of motion of the anklethe therapists should not apply any pressure onjoint. Br J Sports Med 1996; 30: 313-8
the muscle. Some physiotherapy equipment 15. Clarkson H. Musculoskeletal assessment: joint range of motionmight be appropriate such as a sham shortwave and manual muscle strength. 2nd ed. Philadelphia (PA): Lip-
pincott Williams & Wilkins, 2000diathermy.16. Black C, Vickerson B, McCully K. Noninvasive assessment of• Studies should be designed as a counterbalance vascular function in the posterior tibial artery of healthy
humans. Dyn Med 2003; 2 (1): 1design in order to minimise the different re-17. Longworth J. Psychophysiological effects of slow stroke backsponses of individual participants.
massage in normotensive females. Adv Nurs Sci 1982; 4:• Appropriate outcome measures and massage 44-61
18. Drust B, Atkinson G, Gregson W, et al. The effects of massagetechniques should be used in the study.on intra muscular temperature in the vastus lateralis in humans.Int J Sports Med 2003; 24 (6): 395-9
19. Tiidus P, Shoemaker J. Effleurage massage, muscle blood flowAcknowledgementsand long term post-exercise recovery. Int J Sports Med 1995;16 (7): 478-83
The authors would like to acknowledge Huachiew 20. Shoemaker J, Tiidus P, Mader R. Failure of manual massage toChalermprakiet University (Thailand), New Zealand Institute alter limb blood flow: measures by Doppler ultrasound. Med
Sci Sports Exerc 1997; 29 (5): 610-4of Sport and Recreation Research (Division of Sport and21. Dubrosky V. Changes in muscle and venous blood flow afterRecreation, Auckland University of Technology, New Zea-
massage. Soviet Sports Rev 1982; 4: 56-7land) and the American Massage Therapy Association Foun-22. Dubrosky V. The effect of massage on athletes’ cardiorespirato-dation, for funding assistance in the preparation of this manu-
ry systems. Soviet Sports Rev 1983; 5: 48-9script. The authors have no conflicts of interest that are23. Hansen T, Kristensen J. Effect of massage, shortwave diathermydirectly relevant to the content of this review. and ultrasound upon 133Xe disappearance rate from muscle
and subcutaneous tissue in the human calf. Scand J Med SciSports 1973; 5: 179-82
24. Hovind H, Nielsen S. Effect of massage on blood flow inReferencesskeletal muscle. Scand J Med Sci Sports 1974; 6: 74-71. Galloway S, Watt J, Sharp C. Massage provision by physiother-
apists at major athletics events between 1987 and 1998. Br J 25. Tiidus P. Massage and ultrasound as therapeutic modalities inSports Med 2004; 38 (2): 235-7 exercise-induced muscle damage. Can J Appl Physiol 1999; 24
2. Cafarelli E, Flint F. The role of massage in preparation for and (3): 267-78recovery from exercise. Sports Med 1992; 14 (1): 1-9 26. Hernandez-Reif M, Field T, Krasnegor J, et al. Lower back pain
3. Tappan F, Benjamin P. Tappan’s handbook of healing massage is reduced and range of motion increased after massage ther-techniques: classic, holistic, and emerging methods. Stamford: apy. Int J Neurosci 2001; 106: 131-45Appleton & Lange, 1998 27. Ironson G, Field T, Scafidi F, et al. Massage therapy is associat-
4. Goats GC. Massage-the scientific basis of an ancient art: part 1. ed with enhancement of the immune system’s cytotoxic capac-The techniques. Br J Sports Med 1994; 28 (3): 149-52 ity. Int J Neurosci 1996; 84: 205-17
5. De Domenico G, Wood E. Beard’s massage. 4th ed. Philadel- 28. Field T, Grizzle N, Scafidi F, et al. Massage and relaxationphia (PA): WB Saunders Company, 1997 therapies’ effects on depressed adolescent mothers. Adoles-
6. Braverman D, Schulman R. Massage techniques in rehabilita- cence 1997; 31 (124): 903-1003tion medicine. Phys Med Rehabil Clin N Am 1999; 10 (3): 29. Corley M, Ferriter J, Zeh J, et al. Physiological and psychologi-631-49 cal effects of back rubs. Appl Nurs Res 1995; 8 (1): 39-43
7. Bell A. Massage and physiotherapist. Physiotherapy 1964; 50:30. Fraser J, Kerr J. Psychological effects of back massage on406-8
elderly institutionalized patients. J Adv Nurs 1993; 18: 238-458. Magnusson S. Passive properties of human skeletal muscle31. Groer M, Mozingo J, Droppleman P, et al. Measures of salivaryduring stretch manoeuvres. Med Sci Sports Exerc 1998; 8:
secretary immunoglobulin A and state anxiety after a nursing65-77back rub. Appl Nurs Res 1994; 7 (1): 2-69. Gleim GW, McHugh MP. Flexibility and its effects on sports
32. Labyak S, Metzger B. The effects of effleurage backrub on theinjury and performance. Sports Med 1997; 24 (5): 289-99physiological components of relaxation: a meta-analysis. Nurs10. Stanley S, Purdam C, Bond T, et al. Passive tension and stiffnessRes 1997; 46 (1): 59-62properties of the ankle plantar flexors: the effects of massage
[abstract]. XVIIIth Congress of the International Society of 33. Kaada B, Torsteinbo O. Increase of plasma beta-endorphins inBiomechanics; 2001 Jul 8-13; Zurich connective tissue massage. Gen Pharmacol 1989; 20 (4): 487-9
2005 Adis Data Information BV. All rights reserved. Sports Med 2005; 35 (3)
The Mechanisms and Effects of Massage 255
34. Delaney J, Leong K, Watkins A, et al. The short-term effects of 58. Rinder A, Sutherland C. An investigation of the effects ofmyofascial trigger point massage therapy on cardiac autonom- massage on quadriceps performance after exercise fatigue.ic tone in healthy subjects. J Adv Nurs 2002; 37 (4): 364-71 Complement Ther Nurs Midwifery 1995; 1: 99-102
35. Spielberger CD, Gorsuch RL, Lushene RE. The State-Trait 59. Viitasalo J, Niemela K, Kaapola R, et al. Warm under waterAnxiety Inventory. Palo Alto (CA): Consulting Psychologists water-jet massage improves recovery from intense physicalPress, 1970 exercise. Eur J Appl Physiol 1995; 71: 431-8
36. Zeitlin D, Keller S, Shiflett S, et al. Immunological effects of 60. Zelikovski A, Kaye C, Fink G, et al. The effects of the modifiedmassage therapy during academic stress. Psychosom Med intermittent sequential pneumatic device (MISPD) on exercise2000; 62: 83-7 performance following an exhaustive exercise bout. Br J
37. Morelli M, Seaborne D, Sullivan S. Changes in H-reflex ampli- Sports Med 1993; 27 (4): 255-9tude during massage of triceps surae in healthy subjects. J 61. Benjamin P, Lamp S. Understanding sports massage. Cham-Orthop Sports Phys Ther 1990; 12 (2): 55-9 paign (IL): Human Kinetics, 1996
38. Morelli M, Seaborne D, Sullivan S. H-reflex modulation during 62. Cinque C. Massage for cyclists: the winning touch. Phys Sport-manual muscle massage of human triceps surae. Arch Phys smed 1989; 17 (10): 167-70Med Rehabil 1991; 72: 915-9
63. Danneskiold-Samsoe B, Christiansen E, Lund B, et al. Regional39. Morelli M, Chapman C, Sullivan S. Do cutaneous receptors muscle tension and pain (fibrositis): effects of massage and
contribute to the changes in the amplitude of the H-reflex myoglobin in plasma. Scand J Med Sci Sports 1982; 15: 17-20during massage? Electromyogr Clin Neurophysiol 1999; 39:
64. Murphy A, Wilson G. The ability of tests of muscular function441-7to reflect training-induced changes in performance. J Sports40. Sullivan S, Williams L, Seaborne D, et al. Effects of massage onSci 1997; 15 (2): 191-200alpha motoneuron excitability. Phys Ther 1991; 71 (8): 555-60
65. Harmer P. The effect of pre-performance massage on stride41. Zehr E. Considerations for the use of the Hoffmann reflex infrequency in sprinters. J Athl Train 1991; 26: 55-8exercise studies. Eur J Appl Physiol 2002; 86: 455-68
66. Samples P. Does ‘sport massage’ have a role in sport medicine?42. Gam A, Warming S, Larsen L, et al. Treatment of myofascialPhys Sportsmed 1987; 15 (3): 177-83trigger-points with ultrasound combined with massage and
67. Balke B, Anthony J, Wyatt F. The effects of massage treatmentexercise: a randomized controlled trial. Pain 1998; 77: 73-9on exercise fatigue. Clin Sports Med 1989; 1: 189-9643. Pope M, Phillips R, Haugh L, et al. A prospective randomized
68. Boone T, Cooper R. The effect of massage on oxygen consump-three-week trial of spinal manipulation, transcutaneous muscletion at rest. Am J Chin Med 1995; 13 (1): 37-41stimulation, massage and corset in the treatment of subacute
low back pain. Spine 1994; 19 (22): 2571-7 69. Monedero J, Donne B. Effect of recovery interventions on44. Puustjarvi K, Airaksinen O, Pontinen P. The effects of massage lactate removal and subsequent performance. Int J Sports Med
in the patients with chronic tension headache. Acupunct Elec- 2000; 21: 593-7trother Res 1990; 15: 159-62 70. Bale P, James H. Massage, warmdown and rest as recuperative
45. Guyton A, Hall J. Textbook of medical physiology. 10th ed. measures after short term intense exercise. Physiother SportPhiladelphia (PA): WB Saunders Company, 2000 1991; 13: 4-7
46. Lund I, Lundberg T, Kurosawa M, et al. Sensory stimulation 71. Dolgener F, Morien A. The effect of massage on lactate disap-(massage) reduces blood pressure in unanaesthesized rats. J pearance. J Strength Cond Res 1993; 7 (3): 159-62Auton Nerv Syst 1999; 78: 30-7 72. Gupta S, Goswami A, Sadhukhan A, et al. Comparative study of
47. Weinberg R, Jackson A, Kolodny K. The relationship of mas- lactate removal in short term massage of extremities, activesage and exercise to mood enhancement. Sport Psychol 1988; recovery and a passive recovery period after supramaximal2: 202-11 exercise sessions. Int J Sports Med 1996; 217 (2): 106-10
48. Hemmings B. Psychological and immunological effects of mas- 73. Ernst E. Does post-exercise massage treatment reduce delayedsage after sport. Br J Ther Rehabil 2000; 7 (12): 516-9 onset muscle soreness? A systemic review. Br J Sports Med
49. Hemmings B, Smith M, Gradon J, et al. Effects of massage on 1998; 32: 212-4physiological restoration, perceived recovery, and repeated 74. Appell H, Soares J, Durate J. Exercise, muscle damage andsports performance. Br J Sports Med 2000; 34: 109-15 fatigue. Sports Med 1992; 13 (2): 108-15
50. McNair DM, Lorr M, Droppleman LF. Profile of mood state75. Ebbeling C, Clarkson P. Exercise-induced muscle damage andmanual. San Diego (CA): Educational and Industrial Testing
adaptation. Sports Med 1989; 7: 207-34Service, 197176. Clarkson P, Sayers S. Etiology of exercise-induced muscle51. Terry P, Lane A, Lane H, et al. Development and validation of a
damage. Can J Appl Physiol 1999; 24 (3): 234-48mood measure for adolescents. J Sports Sci 1999; 17: 861-7277. Howell J, Chleboun G, Conaster R. Muscle stiffness, strength52. Thayer RE. Measurement through self-report. Psychol Rep
loss, swelling and soreness following exercise-induced injury1967; 20: 663-78in humans. J Physiol 1993; 464: 183-9653. Hemmings B. Sports massage and psychological regeneration.
78. Chleboun G, Howell J, Baker H, et al. Intermittent pneumaticBr J Ther Rehabil 2000; 7 (4): 184-8compression effect on eccentric exercise-induced swelling,54. Callagan M. The role of massage in the management of thestiffness, and strength loss. Arch Phys Med Rehabil 1995; 76:athlete: a review. Br J Sports Med 1993; 27 (1): 28-33744-955. Tiidus P. Manual massage and recovery of muscle function
79. Clarkson P, Nosaka K, Braun B. Muscle function after exercise-following exercise: a literature review. J Orthop Sports Physinduced muscle damage and rapid adaptation. Med Sci SportsTher 1997; 25: 107-12Exerc 1992; 24 (5): 512-2056. Smith L, Keating M, Holbert D, et al. The effects of athlete
80. McHugh M, Connolly D, Eston R, et al. Electromyographicmassage on delayed onset muscle soreness, creatine kinase andanalysis of exercise resulting in symptoms of muscle damage.neutrophil count: a preliminary report. J Orthop Sports PhysJ Sports Sci 2000; 18: 163-72Ther 1994; 19 (2): 93-9
57. Starkey J. Treatment of ankle sprains by simultaneous use of 81. McHugh MP, Connolly D, Eston R, et al. Electromyographicintermittent compression and ice packs. Am J Sports Med analysis of repeated bouts of eccentric exercise. J Sports Sci1976; 4 (4): 141-4 2001; 19: 163-70
2005 Adis Data Information BV. All rights reserved. Sports Med 2005; 35 (3)
256 Weerapong et al.
82. Dolezal B, Potteiger J, Jacobsen D, et al. Muscle damage and 103. Hasson S, Daniels J, Divine J, et al. Effects of ibuprofen use onresting metabolic rate after acute resistance exercise with an muscle soreness, damage, and performance: a preliminaryeccentric overload. Med Sci Sports Exerc 2000; 32 (7): 1202-7 investigation. Med Sci Sports Exerc 1993; 25 (1): 9-17
83. Smith L. Causes of delayed onset muscle soreness and the 104. Mekjavic I, Exner J, Tesch P, et al. Hyperbaric oxygen therapyimpact on athletic performance: a review. J Appl Sport Sci Res does not affect recovery from delayed onset muscle soreness.1992; 6 (3): 135-41
Med Sci Sports Exerc 2000; 32 (3): 558-6384. Glesson M, Blannin A, Zhu B, et al. Cardiorespiratory, hormo-
105. Nosaka K, Clarkson P. Influence of previous concentric exercisenal and haematological responses to submaximal cycling per-on eccentric exercise-induced muscle damage. J Sports Sciformed 2 days after eccentric or concentric exercise bouts. J
Sports Sci 1995; 13 (6): 471-9 1997; 1997 (15): 477-83
85. Hone L, Siler W, Schwane J. Does delayed muscle soreness 106. High D, Howley E, Franks B. The effects of static stretching andaffect oxygen consumption and selected gait parameters dur- warm-up on prevention of delayed-onset muscle soreness. Resing running [abstract]? Med Sci Sports Exerc 1990; 22: s34 Q Exerc Sport 1989; 60 (4): 357-61
86. Harris C, Wilcox A, Smith G, et al. The effect of delayed onset107. Johansson P, Lindstrom L, Sundelin G, et al. The effects ofmuscular soreness (DOMS) on running kinematics. Med Sci
preexercise stretching on muscular soreness, tenderness andSports Exerc 1990; 22: s34force loss following heavy eccentric exercise. Scand J Med Sci87. Cheung K, Hume P, Maxwell L. Delayed onset muscle sore-Sports 1999; 9: 219-25ness: treatment strategies and performance factors. Sports Med
2003; 33 (2): 145-64 108. Lund H, Vestergaard-Poulsen P, Kanstrup I, et al. The effects ofpassive stretching on delayed onset muscle soreness, and other88. Armstrong R. Mechanisms of exercise-induced delayed onset
muscular soreness: a brief review. Med Sci Sports Exerc 1984; detrimental effects following eccentric exercise. Scand J Med16: 529-38 Sci Sports 1998; 8: 216-21
89. Evans WJ, Cannon JG. The metabolic effects of exercise- 109. Rodenburg J, Steenbeek D, Schiereck P, et al. Warm-up,induced muscle damage. In: Holloszy J, editor. Exerc Sport Sci stretching and massage diminish harmful effects of eccentricRev. Baltimore (MD): William & Wilkins, 1991: 99-125 exercise. Int J Sports Med 1994; 15: 414-9
90. Faulkner J, Brooks S, Opiteck J. Injury to skeletal muscle fiber110. Wenos J, Brilla L, Morrison M. Effect of massage on delayedduring contractions: conditions of occurrence and prevention.
onset muscle soreness [abstract]. Med Sci Sports Exerc 1990;Phys Ther 1993; 73: 911-2122: s3491. Friden J, Lieber R. Structural and mechanical basis of exercise-
induced muscle injury. Med Sci Sports Exerc 1992; 24 (5): 111. Hasson S, Cone M, Ellison C, et al. Effect of retrograde massage521-30 on muscle soreness and performance [abstract]. Phys Ther
92. Armstrong R. Initial events in exercise-induced muscular injury. 1992; 72 (6): s100Med Sci Sports Exerc 1990; 22 (4): 429-35
112. Weber M, Servedio F, Woodall W. The effects of three modali-93. Armstrong R, Warren G, Warren J. Mechanisms of exercise- ties on delayed onset muscle soreness. J Orthop Sports Phys
induced muscle fibre injury. Sports Med 1991; 12 (3): 184-207 Ther 1994; 20 (5): 236-4294. Smith L. Acute inflammation: the underlying mechanism in
113. Lightfoot J, Char D, McDermont J, et al. Immediate post-delayed onset muscle soreness? Med Sci Sports Exerc 1991;exercise massage does not attenuate delayed onset of muscle23: 542-51soreness. J Strength Cond Res 1997; 11 (12): 119-2495. Clarkson P, Hubal M. Exercise-induced muscle damage in
humans. Am J Phys Med Rehabil 2002; 81 (11 Suppl.): s52-69 114. Yackzan L, Adams C, Francis K. The effects of ice massage ondelayed muscle soreness. Am J Sports Med 1984; 12 (2):96. deVries H, Housh T. Physiology of exercise: for physical educa-159-65tion, athletics and exercise science. Madison (WI): Brown &
Benchmark, 1996115. Farr T, Nottle C, Nosaka K, et al. The effects of therapeutic
97. Barles P, Robinson J, Allen J, et al. Lack of effect of acupunc- massage on delayed onset muscle soreness and muscle func-ture upon signs and symptoms of delayed onset muscle sore- tion following downhill walking. J Sci Med Sport 2002; 5 (4):ness. Clin Physiol 2000; 20 (6): 449-56 297-306
98. Ciccone C, Leggin B, Callamaro J. Effects of ultrasound and116. Hilbert J, Sforzo G, Swensen T. The effects of massage ontrolamine salicylate phonophoresis on delayed-onset muscle
delayed onset muscle soreness. Br J Sports Med 2003; 37: 72-5soreness. Phys Ther 1991; 71 (9): 675-8
99. Craig J, Bradley J, Walsh D, et al. Delayed onset muscle 117. MacIntyre D, Reid W, Lyster D, et al. Different effects ofsoreness: lack of effect of therapeutic ultrasound in humans. strenuous eccentric exercise on the accumulation of neutro-Arch Phys Med Rehabil 1999; 80 (3): 318-23 phils in muscle in women and men. Eur J Appl Physiol 2000;
81 (1-2): 47-53100. Eston RG, Peters D. Effects of cold water immersion on thesymptoms of exercise induced muscle damage. J Sports Sci1999; 17 (3): 231-8
101. Kraemer W, Bush J, Wickham R, et al. Influence of compres- Correspondence and offprints: Assoc. Prof. Patria A. Hume,sion therapy on symptoms following soft tissue injury from New Zealand Institute of Sport and Recreation Research,maximal eccentric exercise. J Orthop Sports Phys Ther 2001; Division of Sport and Recreation, Faculty of Health and31 (6): 282-90
Environmental Sciences, Auckland University of Technolo-102. Bourgois J, MacDougall D, MacDonald J, et al. Naproxen does
gy, Private Bag 92006, Auckland, New Zealand.not alter indices of muscle damage in resistance-trained men.Med Sci Sports Exerc 1999; 31 (1): 4-9 E-mail: [email protected]
2005 Adis Data Information BV. All rights reserved. Sports Med 2005; 35 (3)