Embed Size (px)
Citation preview

The Open University
The marketisation of care before and during austerity
Susan Himmelweit
August, 2014
Paper for presentation at the IIPPE Annual ConferenceNaples 16 – 18th September 2014
DRAFT: PLEASE DO NOT CITE OR QUOTE WITHOUT PERMISSION
The author of this paper has given IIPPE permission to upload the present paper on IIPPE's website.
The work presented in this paper is entirely my own except where other authors have been referred to and acknowledged in the text. The views expressed in the paper are my own, and IIPPE, or any other member of IIPPE, cannot be held responsible for any statements made in this paper.

IntroductionFeminist economists, in using the term “provisioning” to define the appropriate subject matter of economics, include the provision of care within its domain, seeing it as one of the material processes required for people to thrive and societies to reproduce themselves (Nelson, 2006). Materialist accounts of the history and development of societies give a key role to how such material processes are organised but do not tend to include care within them. Instead they focus on how the surplus, mainly seen in terms of agricultural and industrial goods, is produced and distributed, using this to define economic classes. While feminist economists have made huge strides in analysing the specific features of care and their micro-economic implications, these insights have as yet hardly been integrated into theories of capitalist development, economic crises and policy responses to them. This paper is an attempt to start doing this by considering how changes in the provision of care, specifically the marketization of long-term care, have played a role in the imposition of austerity policies as a response to the recession consequent upon the financial crisis of 2008.
As has been noted for mainstream economics, times of crisis prove critical testing grounds for economic theories, throwing a spotlight on their ability both to explain what led to the crisis and to analyse policy responses to it. If how care is provided is to be integrated into such economic theories then it too should have bearing on such explanations. In this paper I will show how a particular materialist account of the causes and response to the crisis can be made more complete by considering the impact of how care is provided, especially long-term care. To do so requires recognising that economies rely on both paid and unpaid work, that gendered norms and practices allocate men’s and women’s labour differently to those two domains, and that care provision, although equally “economic”, has some specific features that distinguish it from how economists have traditionally analysed work in other production processes. These are the distinguishing features of a feminist economics approach.
There is some debate about how care should be defined, but for the purposes of this paper I will take it to mean the provision of hands-on services that enable others to have a socially agreed common set of capabilities. (I use that definition purposely to exclude the provision of such services to those who already have that set of capabilities, an activity that could be classified as mere “service”). Those social agreed sets of capabilities will vary across societies; thus, for example, being able to carry water might be deemed socially necessary in some societies, while being able to read might be in another - in both cases the services of others can provide substitute functionings for those who would not be strong enough or see well enough to have those capabilities without help.
In all societies, such care provision must include the enabling of children to grow into productive adult members of society and also some provision for the temporary illness or incapacity of normally productive members of society, though again there will be considerable variation in what exactly is seen as necessary for children to thrive and how the temporarily incapacitated are treated. However, care for those with permanent or increasing disabilities, both young and old, is often not seen as an investment in society and therefore practices with respect to their care may be much more subject to changing and variable norms, as accounts of the highly varied treatment of older people across different societies attest.
Over the past thirty years or so, we have seen the development of a human rights discourse in which those with disabilities have been increasingly seen as having rights to the support needed to give
1

them the same capabilities, or at least the same functionings in particular domains, as those of others without disabilities in their society. However, the argument of this paper is that, despite this, we have recently seen a counter-assault on what are seen as socially acceptable levels of capabilities for those who would need long term care to achieve them. This assault has been fuelled by two neo-liberal shibboleths, first that individual well-being is all that matters, second that individual rather collective choice and action is the best way to achieve this. As a result cutting state spending has been widely accepted as the only way to cope with government deficits in the aftermath of the financial crisis. If such cuts are to be permanent, public expectations about how long-term care is to be provided will have to change. Whether current austerity will be successful in lowering aspirations for care provision in the long-run remains to be seen; it has certainly been successful in the UK and some other European countries in lowering current standards of care provision, and in ensuring that care workers are employed under previously unacceptable conditions and for minimum pay.
Care and the Financial Crisis The immediate cause of the financial crisis was the unsustainable growth of household debt, particularly mortgage debt, fuelled on the demand side by rising inequality that kept wage rates stagnant or even falling, while the life styles of the rich fed rising consumer aspirations. The deregulation of financial markets, perverse incentives in the sector, combined with some sharp practices involved in securitisation to increase the supply of credit through irresponsible lending to those who had no hope of being able to meet their debt obligations. When the inevitable defaults occurred, they ricocheted through the financial system, paralysing it until huge government bailouts saved the banks from bankruptcy. Despite the bailouts, the banks took some time to start lending again, by which time the great recession, from which Europe has not yet recovered, had started.
To this economic account, a feminist analysis would add that, besides taking on increasing household debt, another tactic by which households had tried to mitigate the effect of a rising gap between stagnant wage levels and consumer aspirations, was to have two earners. Thus although income inequality between households also rose, it did not increase as fast as the inequality of earnings, because the earnings of second earners, largely women employed full- or part-time, partially made up the gap (at least below the top 1% of households, whose incomes from capital increased faster than their earnings). In many countries, rising employment for women went hand-in-hand with increasing public sector employment, so that in all developed economies women made up a substantial proportion of public sector employment and a larger proportion of women than men in employment worked for the state.
That for women the conditions of state employment were often better than those of private sector employment was both cause and consequence of this. In particular the public sector in many countries became a leader in family-friendly policies that enabled employees to combine caring responsibilities with employment, though still leaving a considerable second shift of caring and domestic work to be done unpaid, largely by women. In that sense, the rise in GDP and the state revenues generated by the increase in women’s employment were not the free lunch for the economy that they appeared to be. Instead they were paid for by women’s increased workload, whose rising employment hours were not matched by an equal drop in unpaid work. Economies relying on women’s employment to generate growth and mitigate the impact of falling wage levels on household income, were thus free-riding on, effectively extracting a surplus from, the excess working hours that women were putting in, through a failure of the mode of care provision to adapt
2

to the new reality of women’s employment. How far that would have been sustainable, particularly as pressure built-up for women to work longer hours to contribute more to the “the economy”, is not clear.
Of course, there was some adaptation with some care provision being moved into the paid economy, through either direct public sector provision or market-provided care, the latter purchased by families and/or the state. Indeed, much of the newly generated employment was in the provision of services that, one way or another, enabled women to take employment including child, and to a lesser extent adult, care. In all developed economies, occupations and industries that have a caring component in their output have been the fastest growing of the past thirty years (Folbre and Nelson, 2000). In so far as they had to pay the costs of market provide care, financial pressures on families increased, reducing the gains of having a second earner.
An additional factor contributing to the crisis was the failure of most economies to adapt their care system to the increasing reality of households needing two incomes to keep up with aspirations generated by increasing inequality. In regimes providing insufficient public support for caring responsibilities, households’ dual-earning strategy was insufficient to maintain living standards; increasing and eventually unsustainable debt was still required. Thus, without a change in care regimes, the dual worker model proved insufficient to avert the crisis. Of course, even such a change rendering dual earning a more effective strategy might still only have delayed the inevitable if inequality between household incomes continued to increase and lending was deregulated. However countries with care regimes that do more to reduce the costs of care to individual families, notably the Nordic welfare states, also tend to be those in which inequality has not reached the levels of Anglo-Saxon regimes.
The “marketisation” of careIn the two or three decades before the financial crisis, many welfare states were going through processes that can be described generically as the “marketisation” of functions previously carried out, at least in part, by the state. Marketisation applied first to nationalised industries; these were particularly rapidly sold off by the Thatcher government in the UK, but were privatised also in other countries. Then previously publicly provided services began to be contracted out to private providers, and finally individuals with various needs began to be given control of their own publically-funded budgets with which to purchase for themselves the services they chose to use. Although this was an uneven process, and included some notable exceptions, such the survival of even the neo-liberal UK’s National Health Service, effectively a nationalised industry providing health care free at the point of use, the trend towards marketisation was present in nearly all OECD countries (Reed, 2011).
Only the last two stages of marketisation are relevant to long term care, since no country has ever made the provision of long-term care a fully nationalised industry; indeed in all countries the amount of care provided unpaid by relatives and friends dwarfs that provided by paid care workers. Although the Anglo-Saxon regimes were often the most enthusiastic promoters of markets, they were not always the first movers. Countries that had allowed or encouraged local authorities to contract out services to non-profit organisations for many years, began to allow private for-profit providers to compete for such contracts in the 1990s (Brennan et al, 2012). In the same decade, many countries introduced individualised personal budgets to allow care recipients to direct how the
3

public funds to which they were entitled were spent on their care. Some were even given direct payments, cash to spend directly themselves on employing their own care assistants and possibly for alternative purposes, with countries varying in how such payments could be used. These moves augmented the growing marketisation that was already happening through self-funding by those lacking family members able to provide care and whose eligibility for public support was insufficient to meet their needs. The need for such self-funding also rapidly increased as public funding failed to keep up with rising life expectancy (or rather the growing numbers of years that individuals would need support for disabilities), and women of the age bracket that had traditionally looked after aging parents and parents-in-law were increasingly in employment and/or lived too far away.
Table 1 shows how these trends had shaped the distribution of expenditure on long-term care around 2008, just before the financial crisis, for selected European countries for which data has been collected.
Table 1: Total public expenditure on long-term care (LTC) and its distribution between home care, residential care, and cash benefits (around 2008); European countries with available data
Country Total expenditure on LTC (% of GDP)
% of total expenditure on LTCResidential care Home care Cash benefits
Switzerland(5) 1.0% 73.9% 26.1% (0.7%)Denmark 2.7% 26.7% 73.3% -Germany 0.9% 57.7% 17.8% 24.4%Spain 0.3% 59.0% 27.0% 13.9%France(4) 1.2% 57.4% 42.6%Italy 1.7% 26.2% 31.7% 42.1%Netherlands(6) 2.2% 55.8% 33.6% 10.6%Austria(1) 1.3% 42.7% 57.3%Slovenia(5) 0.8% 25.7% 74.3% (27.5%)Slovakia(2) 0.5% 69.0% 4.9% 26.1%Finland(3) 1.8% 69.0% 31.0% -Sweden 3.9% 58.7% 38.1% 3.3%UK 1.2% 47.4% 24.2% 28.5%Source: Allen et al (2011) p12, Table 3.1, using Huber et al., 2009: 99; Office Fédéral des Assurances Sociales (OFAS), 2006; WP6 National Reports.Notes: (1) The Austrian LTC allowance is used by beneficiaries to also pay for residential care (about 20% of recipients) or home care services (about 25%) – or for informal care arrangements with migrant carers (about 10%) it is thus difficult to distinguish exact shares of expenditures; (2) 60+ population; (3) National Institute for Health and Welfare (2011); (4) Without specific surveys it is currently not possible to delineate the share of beneficiaries who choose services in- kind and those who choose purely cash benefits; ‐ (5) Due to differences in sources only residential care and home care add up to 100%; (6) CPB/ANCIEN data, including both the Exceptional Medical Expenses Act and the Social Support Act, as far as 65+ are concerned.
The European research consortium, ANCIEN, developed a typology of LTC systems in EU countries, covering their diverse arrangements for the organisation and financing of long term care provision, shown in Table 2 (Kraus et al., 2010). They note that this typology provides “surprising results as, for instance, the German and Slovak LTC systems result as similar, while countries as different as Austria, England, Finland, France and Spain seem to show the same pattern of LTC service use and financing. As a corollary, these results may yet again underline that LTC as a system is just emerging in most European countries” (Allen et al, 2011: p17).
4

Table 2: Typology based on organisation and financing of long--term care Nature of the system Countries CharacteristicsOriented towards informal care, low private financing
Belgium,* Czech Republic, Germany, Slovakia
Low spending, low private funding, high IC use, high IC support, cash benefits modest
Generous, accessible and formalised
Denmark, The Netherlands, Sweden
High spending, low private funding, low IC use, high IC support, cash benefits modest
Oriented towards informal care, high private financing
Austria, England, Finland, France, Spain
Medium spending, high private funding, high IC use, high IC support, cash benefits high
High private financing, informal care seems a necessity
Hungary, Italy Low spending, high private funding, high IC use, low IC support, cash benefits medium
Source: Kraus et al., 2010: 39, adapted from Allen et al (2011) p17, Table 3.7 Note: * medium spender.
The reasons given for introducing the marketization of public services varied across countries (see for example: Allen et al, 2011; Brennan et al., 2012; Da Roit and Le Bihan, 2010; Kraus et al, 2010; Ungerson and Yeandle, 2007). For the contracting-out of services to private providers, reasons included expected efficiency gains: either because private providers were believed to be inherently more efficient that managers in the public sector or, more often, that competition between providers would incentivise them to provide greater value for money. Value for money could mean higher quality but was more often cited in the context of cost containment in the face of rising demand.
Against this it was argued that because there are inherent difficulties in assessing and comparing care quality, in practice competition would be primarily over price and thus rely on cutting costs. However, care provision is highly labour intensive with little scope for real productivity improvements, so in practice costs reductions would be achieved only by employing less well-trained staff, in fewer numbers and/or under worse pay and conditions, with all of these methods of cutting costs likely to lead to reductions in the quality of care.
Private sector providers could often achieve such cost reductions more readily, since public sector employees were more likely to be unionised and able to hold their employers to account not only for their own wages and working conditions, but also the standard of care being provided to recipients (Francois and Vlassopoulos, 2007). Similarly for-profit providers could achieve lower costs than non-profits motivated by a professional or public service ethic who, along with their workers, might not be willing to provide care if they could not do it to an acceptable standard. A report by the Commission for Social Care inspection in the UK found that private provision of long term care for older people – both residential and non-residential – was less likely to be judged ‘good’ or ‘excellent’ and more likely to be judged ‘poor’ or ‘adequate’ by inspectors than either public or voluntary sector provision (CSCI, 2009). UK data also shows that provision of services in the private sector is associated with a greater workforce turnover, and of long-hours working practices, than either the public sector or the voluntary sector, which “raises clear worries about the quality of public services outsourced to the private sector compared with those provided in-house.” (Reed, 2011, p 18). Nevertheless, if cost containment in the face of rising demand was the main aim, “efficiency” gains in terms of reduced costs might result in the introduction of competitive tendering by for-profit providers being judged a success.
5

Giving care recipients their own personal budgets or direct payments to spend in “consumer- directed” care takes these arguments a step further. Making care recipients into consumers by allowing them to choose and purchase their own care, was seen as giving them more autonomy and fostering increased choice, both seen as desirable in their own right. Consumer choice was also expected to lead to yet greater efficiency and value for money from providers who would be responding directly to consumer demand, not having that mediated through local authority purchasers (though in practice it might be another third-party, such as a relative, who chose on behalf of care recipient.) The fear of customer exit should make providers more responsive to care recipients’ preferences and encourage their voice in improving services. It might also provoke innovation, by giving providers the incentive to seek out gaps in provision and develop new ways of meeting needs (Allen et al., 2011: 26)
Value for money might also be increased through unwanted services not being provided, but rather having services being “personalised” to an individual’s preferences (how far this could go depends on how recipients were allowed to use their personal budgets). Personalisation was also seen as desirable because it would encourage “co-production”, by which was meant the engagement of care recipients in their own care; keeping them actively engaged was seen as important in preventing or delaying further care needs developing.
Another argument was used was that of equity, that those who could pay for their own services had always been able to make such choices and this should be also be available to those dependent on state support. Further, while more articulate care recipients tend to get better service from public services, the market was said to give similar voice to all (in contrast to the traditional view that voice in the market depends on the resources that one has to spend) (ibid).
Again there were opposing arguments. For competition to work, customers have to have full information about available services, including the quality and prices charged by all potential providers. Information on quality is hard to acquire for long-term care and, for the very reason that they need care in the first place, purchasers may have particular difficulty in making such choices, which they often have to make in situations that are pressuring and stressful, when first discovering that they cannot manage without the help of others (Brennan, 2012). Market competition is also more effective when there are low costs to change. This is far from the case with long-term care, where the need to build up relationships favours familiarity and continuity of care, so that care recipients may well stick with unsatisfactory care out of fear that an unfamiliar alternative could be worse (ibid). A frequent complaint is that, by frequently changing the care workers allocated to a care recipient, care providers do not accommodate care recipients’ wishes for continuity, familiarity and security in having their specific needs met – this can hardly be rectified by changing providers and getting a completely new set of carers1.
Further, individual recipients do not have the market power that local authorities do. Providers who thrive in the market tend to be large ones who do well from clients needing a standardised service in densely populated areas. This leaves those with unusual needs or in remote places unable to
1 The author’s own experience, after contacting a private for-profit provider from a local authority recommended list, was of having six different carers in the first ten days of a period in which she needed care.
6

exercise the choice that consumer-directed care is supposed to provide. “Personalisation” is not a cheap option for service delivery, as it involves a tailored solution for each public service client and therefore more “face time” between client and adviser than a standardised service (Unite, 2008). Individual needs might indeed be better met by a local authority mandated to ensure that all those needing care in their area receive at least a standard package. A study of direct payments recipients in the UK found that for older people using an agency to purchase services “the degree of user autonomy was not necessarily any greater” since they would need to go through the agency to resolve any issues that could not be resolved within their contract (Yeandle and Stiell, 2012).
The original model of consumer-directed care was of care recipients acting as employers, finding their own care assistants and training them to meet their specific needs (and occasionally using some of their direct payments to buy other things that would help them with other needs, such as tickets to a football match). However, in practice many care recipients purchase their care from agencies or care providers with many employees – they may have the choice between agencies and providers, but any provider will achieve cost efficiencies only by providing just as standardised a service as any local authority.
Many younger disabled people supported and welcomed the move to consumer-directed care, and in particular favoured direct payments by which they could employ and train their own care assistants to meet their specific needs, which were likely to be fairly constant. It was older care recipients with progressing needs who were more likely to find choice to be a burden rather than a liberation and did not want the responsibility of becoming their care assistants’ employer (Land and Himmelweit, 2010).
This paper, which is focused on the effects of austerity, will not evaluate these claims for and against the benefits of marketization for care recipients. Many studies of how the different stages of marketisation have worked out in practice have been carried out and others are still on-going (see eg Glendinning and Kemp, 2006; Ungerson and Yeandle, 2007; Glendinning and Moran, 2009; Da Roit and Le Behan, 2010; Kraus et all 2010; Lipszyc et al, 2012; Allen et al, 2014). However, while considering the effects of austerity, we do need to note that many of the non-financial benefits claimed for the use of the market to deliver care, particularly for consumer-directed care, depend on resources being less than minimal. For example, the argument that users would be empowered by being able to use their personal budgets in other ways than providing basic services depends on those budgets being sufficient to cover more than just those essential services. But in practice, even before the advent of austerity, studies showed that spending was being squeezed and social care was talked about as facing an underfunding crisis (Wanless, 2006).
Some of the biggest problems of consumer directed care are for the care workers. In the UK, particularly as local authority budgets have been cut, there has been widespread concern about the spread of zero hours contracts, in which workers have to be on call, and may be restricted form taking on any other employment but are not guaranteed any hours of employment (or income), yet may be called in for single widely separated hours with their travel time unpaid. In England, one in five social care workers are now employed on zero-hours (Kline, 2013). Further, such contracts can lead to bullying by employers as the allocation of work can be used to demand unacceptable conditions (op.cit). But an interview study found that it was “when care workers are employed directly by an older person (rather than via and agency) that the risks to both parties are likely to be
7

greatest” (Yeandle and Ungerson, p133). These risks include those arising from casual recruitment processes, misunderstandings of employment rights, job insecurity, changing care needs of the care recipient, and isolation and lack of support for care workers, including for their own health needs.
This is not surprising since the cost-savings of marketization arise primarily from employing fewer, less well-trained workers under less-costly conditions. For example, transferring the risk of whether work is available to employees has been a longstanding strategy to reduce costs: zero-hours contracts are just an extreme version of this; enforced self-employment is another. Marketisation should therefore be more effective at reducing costs in more “flexible” labour markets, like that of the UK, where there is less employment regulation to protect the most vulnerable from such risks by allocating them to those who can bear them better. But care recipient employers are in no better position than their employees to bear such risks. Further costs visited on care workers have effects on their employers too, since vulnerable workers provide worse care.
These considerations suggest that provision through the market may not only be a way of preventing costs rising for long-term care, but at the expense of quality; market provision may also make it easier to cut costs in times of austerity. Local authorities cutting spending on care may find it easier to reduce payments made to private contractors than to their own staff, who are likely to be unionised and vocal. Whether private contractors can resist such cuts will depend on how competitive the local market is, but where the local or national government is the main purchaser for care services, it will have considerable power to set the level of payments, though not necessarily to ensure what quality is delivered for those payments. Reductions in quality take time to be revealed and in a contracting out system providers can be blamed for them, rather than the lack of funding, making them a more politically palatable response to an insufficient budget than the direct implementation of cuts in a publically provided service.
Again the use of consumer-directed care, personal budgets or direct payments, allows this abrogation of responsibility to be taken a step further (Himmelweit and Land, 2010). Not letting personal budgets rise in line with costs, when those in receipt of them are isolated care recipients many of them employing their own care assistants, is a relatively easy way to restrain spending. In Germany in 2001, three-quarters of domiciliary care users took the option of a cash payment even though it was worth half the value of services in kind (Glendinning and Kemp, 2006: 236). Many used it to pay an informal carer. There is now evidence that more are changing back to opt for the service not least because the cash payment has not been increased since it was introduced (Glendinning and Moran, 2009). This was even without austerity measures.
Further the existence of personal budgets may make implementing cuts in general easier, even if relatively few have taken them up in the past. Those receiving direct services dissatisfied with diminishing quality, not realising that this is an effect of cuts in spending, may now believe they can do better themselves if they control how their personal budgets is spent.
Never let a good crisis go to wasteEven before the bailout of the banks, many European countries had a fiscal deficit. The financial crisis greatly increased those deficits, partly due to the costs of the bank bailout but more because of the increased spending on benefits and reduction in tax receipts consequent on the recession’s rise in unemployment and fall in GDP. Falling GDP not only reduced government revenues, it also cut the denominator against which deficits were measured, making them appear larger. A number of
8

European policy makers asserted that government deficits were the underlying cause of the crisis or, at any rate, that without tackling those deficits the crisis could not be resolved, because it would no longer be possible to finance increasing government debt. The justification for austerity was thus to reduce government deficits; within the Eurozone because there was no mechanism by which exchange rates could be adjusted to prevent a run on any individual country’s public debt, and for more ideological reasons for the UK’s newly elected right leaning coalition government.
An alternative Keynesian view was that deficits could only be tackled by making full use of a country’s resources, in particular by reducing unemployment and thus, rather than spending cuts, a further stimulus was needed, which would ultimately reduce the deficit by generating increased revenues. Although supported by evidence from the past when efforts to cut spending directly had only led to increased deficits, this approach was not adopted by any European government, nor formally by the United States. However, greater willingness in practice by the US government to introduce stimulus measures, and a domestic economy capable of generating the majority of its own demand, led to growth resuming faster in the US than in Europe, though unemployment remained high.
One explanation of the unwillingness of European governments to find a way around the architecture of the Eurozone that made applying a stimulus difficult, is that the German government was seizing the crisis as an opportunity to reform the spending patterns of their European partners and make them conform to the economic model adopted in Germany in the early 2000s that had reduced working-class social benefits and living standards in pursuit of export-led growth. Similarly the UK government, although unconstrained by Eurozone rules, was of its own volition seizing the crisis as an opportunity to shrink the state in line with its own neo-liberal views. In other words, it was not so much that these governments thought that austerity was the only way out of the crisis, but it was the only way acceptable to them given their long-term aims.
Another related, but more class-based, view recognises that in modern capitalism finance capital is internationally mobile and has little stake in any domestic economy. It is therefore ultimately interested only in opportunities for profitable investment and not in generating growth or full employment in any particular economy. Capital had done well with the share of profits rising as the global economy expanded, providing new and cheaper labour markets. However in this globalised world, the costs of reproduction of the metropolitan working class, taking account of both wage levels and the contribution of state spending, as state benefits were increasingly used to top-up wage levels which had stagnated or even fallen in the years before the crisis, had become uncompetitive.
The solution favoured by finance capital was to lower these costs of reproduction further, and the crisis provided an opportunity to do so in two ways. The first was to ensure that real wages continued to fall; for that to happen levels of unemployment had to remain high for a sustained period. Cuts in the so called “social wage”, expenditure on the benefits and public services used by the working class, to lower the social costs of reproduction provided the second route. Austerity could be used to move along both routes, with un- and under-employment frightening the working class into accepting wages cuts and inferior working conditions, and cuts in social spending enabling taxes on capital to be reduced. Without both these conditions being met, cuts in both real wages and in public spending, international finance would not invest in such “uncompetitive” economies,
9

preferring cheap labour economies and tax havens, and the crisis would continue. So in this view, the explanation of austerity is not that there was no alternative or more effective route out of the crisis, but that finance capital had the power to ensure that crisis conditions remained until its “solution” was adopted. Austerity was its weapon of choice.
Thus according to this view, the falls in working class living standards that have undoubtedly taken place, are not the unintended by-products of the crisis itself or of policies to resolve it, but rather the measure of success of those policies themselves. The imposition of austerity can be seen as directed directly at changing norms concerning acceptable living standards, in terms of both household incomes and social provision, including a reduction in what are seen as acceptable minimum standards of care.
European evidenceWhile countries varied in what was happened to wage levels before and during the crisis, by 2010 average real wages were falling in all the major countries on which austerity measures had been imposed as conditions of Eurozone bailouts, Greece, Italy, Ireland, Spain and Portugal, several Eastern European countries, Hungary, Slovenia, the Slovak Republic and in the UK, where austerity was self-imposed, and to a lesser extent and with a less severe effects in Austria, the Netherlands and Denmark (OECD (2014). OECD data also shows that it was in these countries that household disposable income fell most and absolute poverty rates increased the most sharply.
However, the effects of cuts in public services on working class living standards are less frequently taken into account. In the period 2010-2013, expenditures on “benefits in kind”, directly delivered social services, fell in many European countries as table 3 shows.
Table 3: Real public social expenditure, real GDP and various categories of social expenditure as % of GDP, % change 2009 -2013: European OECD countries and OECD total
% change 2009 -2013
Country public social expenditure as % of GDP
real GDPreal public
social expenditure
on cash benefits
on benefits in kind
on long-term care*
Austria 0.3% 5.9% 6.2% 2.7% -4.6% 1.5%Belgium 8.6% 4.2% 12.8% 6.1% 13.0% 6.8%Czech Republic 6.2% 2.3% 8.5% 3.2% 11.0% 8.9%Denmark 7.6% 2.5% 10.2% 4.5% 10.7% -3.9%Estonia -10.4% 17.8% 7.4% -12.8% -4.9% -14.4%Finland 7.1% 3.8% 10.9% 8.0% 5.9% 1.7%France 6.2% 4.0% 10.2% 3.4% 10.5% -26.6%Germany -2.3% 8.7% 6.4% -6.2% 3.2% 0.7%Greece -7.2% -21.0% -28.2% -1.5% -18.3% 16.5%Hungary -8.3% 2.0% -6.2% -1.1% -22.7% -Iceland -6.9% 3.1% -3.8% -5.7% -7.8% -3.1%Ireland -4.9% 0.9% -4.0% 2.6% -16.4% -Italy 3.8% -2.1% 1.7% 2.1% 7.6% -Luxembourg 1.2% 7.1% 8.3% 2.0% -0.1% 7.4%Netherlands 10.4% 0.4% 10.8% 4.6% 16.7% 11.0%Norway 0.4% 5.5% 5.8% 5.3% -4.8% -2.3%Poland 0.2% 12.4% 12.6% -4.5% 12.8% 10.9%Portugal 6.4% -4.0% 2.4% 8.2% 2.4% -
10

Slovakia -3.0% 10.5% 7.5% 4.0% -14.0% -6.8%Slovenia 6.6% -1.7% 4.9% 6.9% 6.1% 7.0%Spain 9.3% -3.0% 6.3% 10.2% 7.7% -Sweden -0.2% 12.5% 12.3% -1.8% 1.2% -2.0%Switzerland1 -7.08% 8.0% 0.02% -0.08% -14.63% 5.8%United Kingdom -0.1% 4.9% 4.8% 3.2% -3.4% -OECD - Total 2.5% 7.9% 10.5% 3.0% 1.9% -1Figures for Switzerland are for % change 2010-2013 *All figures for long-term care are for % change 2009-2012
The first column gives the relative change from 2009-2013 in total social spending as a proportion of GDP. It shows that various countries were prepared to allow their social expenditure fall behind any growth in GDP. However their situations differed. The only country cutting expenditure faster than GDP, whose GDP was fell between 2009 and 2013 was Greece; these cuts were effectively imposed from outside as a condition of Greece’s continued membership of the Eurozone. Other countries whose GDP fell, including Italy, Spain, Portugal and Slovenia did not cut social spending relative to GDP. The UK, Sweden, Germany, Switzerland, Slovenia and Estonia cut the proportion of GDP that went on social spending despite their GDP rising over that period.
The numbers in the fourth and fifth columns of Table 3 show any shifts between services delivered in kind and cash benefits, including any increase in the use of direct payments for long-term care. Ireland, Greece and, outside the Eurozone, several Eastern European countries, cuts in social services were very severe but cuts in cash benefits more limited, though cuts per recipient may have been much higher, given the likely increase in their numbers. For those countries where unemployment rose between 2010 and 2013, automatic stabilisers will have contributed to an increase in expenditure on cash benefits and thus on total public social expenditure. Falls in discretionary social spending on services and on cash benefits not related to unemployment were therefore greater than Table 3 shows.
Estonia and Poland stand out as the sole countries deciding to cut cash benefits rather than social services, while Germany cut cash benefits while increasing total social spending. Other countries, such as Norway and Switzerland, imposed cuts in social service expenditure without having suffered any particularly severe effects of the financial crisis. Estonia, Germany, Poland and Sweden also recovered fast from the crisis in terms of GDP but cut cash benefits nevertheless. And finally the UK, despite its self-imposed austerity, kept its social expenditure roughly in line with its slow growing GDP, and failed to cut cash benefits at all until 2012-13, so until then the cuts came almost entirely from social services (though some of these, including for long-term care may have turned into cash benefits during that period).
The final column shows growth in general government expenditure for long-term care in the period 2009-2012. It excludes expenditure through a country’s social security system and therefore cannot distinguish between total cuts and a shift in expenditures towards direct benefits. For example, France has a system of support for long-term care that is delivered largely through its APA (Allocation Personnalisée à l’Autonomie), a social security benefit. A further shift towards this system might explain why a country that did not cut state expenditure in general in 2009-2012, apparently imposed a particularly large cut in expenditure long-term care. In most countries
11

expenditure on long term care increased as a percentage of GDP, though less fast that the population at risk of needing it.
Despite this complexity, a pattern emerges with some outliers. The countries classified in Table 2 as making modest use of cash benefits to deliver long-term care divide into two: those where expenditure was already high, Sweden and Denmark, cut their expenditure on long-term care more than on social spending in general, while those where expenditure was low or medium, Belgium, Czech Republic, Germany and the Netherlands, cut or increased their spending on social care roughly in line with their social expenditure in general. Of those for which we have data who made high use of cash benefits to deliver care, Finland and France cut spending on long term social care more than other social spending, France spectacularly so by changing to a cash benefit system, as noted above, while Austria slightly bucked the trend by increasing spending on long term social care slightly more than on social spending in general.
This provides rather weak evidence to support the idea that governments had more difficulty cutting spending on long term care on services that were delivered directly in kind than those that were delivered through cash benefits. Currently, I could find no further data available at the European level to test this hypothesis.
Evidence from the UKOne country for which the OECD does not have data on expenditure on long-term care is the UK, because it is funded separately for its constitutive nations England, Wales, Scotland and Northern Ireland. A study of trends in expenditure on long-term care in England provides a telling case-study of how one economy has used personal budgets to manage long term care in a period of austerity.
In England, local authorities are responsible for providing publicly funded social care, but do so mainly on the basis of revenue allocations from the central UK government. In 2010, the Comprehensive Spending Review of the incoming right-leaning coalition government cut its grant to local authorities by 26% in real terms, which lead to a projected fall of 14% in local authority spending. Three years later in June 2013, another 10% cut in the grant to local authorities was announced for 2015/6.
Local authorities in theory could allocate those cuts where they chose, but in practice cuts of that size meant that all major categories of local government spending were reduced. Providing social care for adults and children represents the largest category of spending for local councils. In 2012/3, the reductions made to adult social care budgets accounted for over 52 per cent of the total reductions in local government spending (Audit Commission, 2013).
The 2014 report for QualityWatch on social care for older people examined the scope and scale of cuts in spending on services for older people from 2009/10 to 2012/13 and found significant variation in how local authorities responded in terms of their spending on social care, with around a third of local authorities reducing their net current expenditure by 20 % or more in real terms between 2009/10 and 2012/13, a very few showing increases in spending, and the remainder implementing cuts of between zero and 20 per cent. The average was a cut of 15%. Cuts were implemented by tightening eligibility criteria to concentrate resources on those with the greatest needs, increasing user fees, reducing fees paid to providers and administrative costs. These cuts took place against a backdrop of increasing demand for social care among older people, as their numbers
12

increased as a proportion of the population and they themselves became on average older and in more need of care.
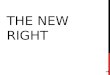
As Figure 1 shows, spending on most categories of services for older people had already begun to fall by 2009/10, but this was counteracted by a roughly equal increase in direct payments to carers (these figures do not include personal budgets or direct payments to care recipients, which are included in the category on which they are spent). From 2009/10, the rise spending on direct payments to carers did little to compensate for the falls in other categories, particularly residential care placements and home and day care, where spending fell by 13% and 23% respectively by 2012/13, to result in a net fall of over £1billion.
Figure 1: Change in real net spending on older people’s services, 2005/6 – 2012/3
Source: Ismail et al. 2014.
These significant reductions in expenditure on older adults impacted on both the numbers receiving support with their care needs and the amount and quality of care those still receiving such support state got. There were relatively small overall reductions from 2009/10 to 2012/13 in the numbers of residential care and nursing care recipients (Ismail et al, 2014). For them the cuts were implemented more in the form of reduced payments to providers. The Care Quality Commision’s analysis of unit costs of supporting adults in residential homes, nursing homes or intensively in their own home, notes that local authorities paid 5% less in real terms in 2011/12 than in 2011/12 and noted that ‘there is concern around the ability of the sector to maintain quality standards if there are further funding reductions’ (CQC, 2013).
Another way to restrict spending is to tighten the eligibility criteria for receiving public funded care services. The proportion of local authorities restricting public funding to those people with needs that are judged to be ‘substantial’ or ‘critical’ grew steadily from 65 % in 2006/07 to just over 70% in 20091/0 and then climbed to 87 % in 2013/14. The number of publicly supported older people receiving community-based services included a 35% reduction in those attending day-care centres and a 15% fall in the numbers receiving domiciliary care services (Ismail et al, 2014). The 2012 Health
13

Survey for England found that a third of women and one fifth of men over the age of 65 had unmet needs with respect to some activities of daily living (Whalley, 2012).
As a result, an increasing number of older people were having to use their own resources to support themselves or do without care. Nearly one quarter of a million fewer people received publicly funded service in 2012/13 than in 2009/10, a reduction of 26%. The numbers receiving direct payments increased by 20% but this amounted to only an increase of just over 10,000 in that period. One effect was an increased number of unpaid carers reporting that they cared for people for more than 20 hours a week (Ismail et al, 2014).
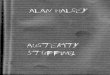
Figure 2: Numbers receiving care services in the community, numbers doing so through personal budgets and numbers whose personal budgets are received as direct payments: UK, 2005/6 – 2012
Figure 2, from a different source, shows how at the same time that the number of people receiving services in the community fell in that period, the number doing so in through personal budgets rose, and of these the number receiving direct payments increased slightly. Thus the implementation of severe cuts in social spending, which reduced the numbers of receiving care, happened at the same time as the proportion of care recipients on personal budgets rose substantially. This gives some support to the idea that under austerity personal budgets became a means by which cuts in long-term care expenditure could be implemented more readily. The evidence is consistent with an interpretation that faced with falling budgets, local authorities saved money on social care by
14

restricting eligibility, and insisting that any new care recipients, and perhaps existing one, were given personal budgets of lower value than similar services had previously cost the local authorities themselves.
ConclusionThis paper has argued that the imposition of austerity in times of recession can be seen as directed at changing norms concerning acceptable levels of provisioning and thus promoting conditions for more profitable expansion. In terms of material levels of consumption this has been clear, with what are seen as acceptable minimum standards falling as real levels of household incomes dropped in most countries that adopted austerity policies. Such policies have also resulted in less care being provided and financed by the state, at least in relation to increasing needs, with marketization in some cases the tool by which this is managed and rendered politically acceptable.
This paper has provided a little evidence to support the idea that marketisation, in particular the provision of individualised personal budgets that turned care recipients into consumers, has made the imposition of austerity easier, by shifting more costs onto families, lowering standards of state-financed care, restricting who is eligible to receive care and, perhaps above all, imposing casualised labour market conditions on care workers that would have been unacceptable a few years ago. Whether it is effective in the long-term in changing norms depends on whether the responsibility for such falling standards is successfully individualised onto individual care recipients and their families and what political and other limits there are to this process.
15

Bibliography
Allen, K. et al. (2011) Governance and finance of Long Term Care across Europe: Overview report, Interlinks http://www.birmingham.ac.uk/Documents/college-social-sciences/social-policy/HSMC/research/interlinks-wp6-final.pdf
Audit Commission (2013) Tough Times 2013: Councils’ responses to financial challenges from2010/11 to 2013/14. http://www.audit-commission.gov.uk/wp-content/uploads/2013/11/Tough-Times-
2013-Councils-Responses-to-Financial-Challenges-w1.pdf.
Brennan D., Cass, B. Himmelweit, S. and Szebehely, M.(2012) 'The Marketisation of Care: Rationales and Consequences in Nordic and Liberal Care Regimes', Journal of European Social Policy, 22(4): pp. 377–391
CQC (Care Quality Commission) (2013) The State of Health Care and Adult Social Care in England: Technical Annex 2: Adult social care funding data collection. http://www.cqc.org.uk/sites/default/files/media/documents/state_of_care_annex2.pdf
CSCI (Commission for Social Care Inspection) (2009) The State of Social Care in England: 2007-08, http://www.cqc.org.uk/_db/_documents/SOSC08%20Report%2008_Web.pdf
Da Roit, B. and Le Bihan, B. (2010) Similar and Yet So Different: Cash-for-Care in Six European Countries' Long-Term Care, The Milbank Quarterly, Vol. 88, No. 3, pp. 286-309
European Commission (2012), The 2012 Ageing Report: Economic and budgetary projections for the27 EU Member States (2010-2060), European Economy 2, http://ec.europa.eu/economy_finance/publications/european_economy/2012/pdf/ee-2012-2_en.pdf
Folbre, N. and Nelson, J. (2000) ‘For love or money – or both? ’, Journal of Economic Perspectives, vol.14, no.4, pp.123 - 40
Franklin, B. (2014) The Future Care Workforce, International Longevity Centre - UK http://www.ilcuk.org.uk/index.php/publications/publication_details/the_future_care_workforce
Glendinning, C and Kemp, P eds (2006) Cash and Care. Policy Press
Glendinning, C and Moran, B (2009) Reforming Long-term Care: Recent Lessons from Other Countries, University of York social Policy Research Unit Working Paper No. DHP 2318 http://www.york.ac.uk/inst/spru/research/pdf/LTCare.pdf
Ismail, S., Thorlby, R. and Holder, H. (2014) Focus On: Social care for older people: Reductions in adult social services for older people in England, QualityWatch, http://www.qualitywatch.org.uk/focus-on/social-care-older-people
Kline, R. (2013) Zero-hours contracts are inappropriate in the field of social care work http://www.theguardian.com/social-care-network/2013/aug/21/zero-hours-contracts-social-care
16

Kraus, M., Riedel, M., Mot, E., Willemé, P., Röhrling, G., Czypionka, T (2010) A Typology of Long-Term Care Systems in Europe. Brussels: CEPS (Social welfare policies, ENEPRI Research Reports, http://www.ceps.eu/book/typology-long-term-care-systems-europe
Land, H. and Himmelweit, S. (2010). Who Cares: Who Pays? A Report on Personalisation in Social Care. Unison, London.
Lipszyc, B., Sail, E. and Xavier, A. (2012) Long-term care: need, use and expenditure in the EU-27, European Economy, Economic Papers 469, http://ec.europa.eu/economy_finance/publications/economic_paper/2012/ecp469_en.htm
Martin, B. (2013) Thatcher had a level of care that local authority workers simply can't provide, http://www.theguardian.com/society/2013/apr/16/thatcher-home-care-workers-standards
Martin, C. and Le Bihan, B., (2007) ‘Cash for Care in the French Welfare State: A skilful Compromise?’ in C. Ungerson and S. Yeandle (eds) Cash for Care in Developed Welfare States, Palgrave, Macmillan, pp 32-59.
The National Audit Office (2014) Adult social care in England: overview, HC 1102
Nelson, J. A. (2006) Economics for Humans, University of Chicago Press
OECD (2013), Health at a Glance 2013: OECD Indicators, OECD Publishing. http://dx.doi.org/10.1787/health_glance-2013-en
OECD (2014), Average wages (indicator). doi: 10.1787/cc3e1387-en (Accessed on 30 July 2014)
Pennycook, M., Cory, G., and Alakeson, V. (2013) A Matter of Time: The rise of zero-hours contracts, Resolution Foundation, http://www.resolutionfoundation.org/media/media/downloads/A_Matter_of_Time_-_The_rise_of_zero-hours_contracts_final_1.pdf
Howard Reed (2011) The Shrinking State: Why the rush to outsource threatens our public services, Unite theUnion, http://classonline.org.uk/docs/Unite_The_shrinking_state_2011.pdf
Ungerson, C. and Yeandle, S. (2007) ‘ Conclusion: Dilemmas, Contradictions and Change’ in C. Ungerson and S. Yeandle (eds) Cash for Care in Developed Welfare States, Palgrave, Macmillan, pp 187-206.
C. Ungerson and S. Yeandle (eds) (2007) Cash for Care in Developed Welfare States, Palgrave, Macmillan
Wanless D (2006) Securing Good Care for Older People: Taking a long-term view. The King’s Fund. www.kingsfund.org.uk/publications/securing-good-care-older-people
Whalley R (2012) ‘Social care: need for and receipt of help’, in Health and Social Care InformationCentre, Health Survey for England 2012, Health and Social Care Information Centre. http://healthsurvey.hscic.gov.uk/media/1019/chpt-8_social-care-need-and-receipt.pdf
17

Yeandle , S. and Stiell, B. (2012) ‘Issues in the Development of the Direct Payments Scheme for Older People in England’, in C. Ungerson and S. Yeandle (eds) Cash for Care in Developed Welfare States, Palgrave, Macmillan, pp 104-136.
Vlassopoulos, M. and Francois, P. (2008) ’Pro-social Motivation and the Delivery of Social Services’, CESifo Economic Studies, 54(1), 22-54, 2008
18