Embed Size (px)
Citation preview

353
THE MANAGEMENT OF THE QUINIZARINSWEAT TEST (Q.S.T.)
By L. GUTTMANN, M.D.Neurological Surgeon in Charge, Head and Spinal Injuries Centre, Ministry of Pensions' Hospital,
Stoke Mandeville, near Aylesbury, Buckinghamshire
The investigation of sweating represents aspecial and relatively new approach to clinicaland physiological research on cutaneous fupc-tion.- The recent war has afforded greatopportunities for investigating the phenomenaresulting from injuries of the nervous systemaffecting the sweat mechanisms, and theQuinizarin method (L. Guttmann, 1937, '38,'40, '4I, '46; Highet, I942; Lewin, 1943;Seddon, 1942) has proved a reliable and themost simple method of studying these pheno-mena in detail. Disturbances of the centraland peripheral sudomotor pathwavs can beaccurately revealed and the purely physio-logial activity of sweat glands estimated. TheQuinizarin Sweat Test (Q.S.T.) is objectiveand, unlike sensory tests, does not dependupon statements made by the patient. In fact,in certain types of peripheral nerve lesions,such as incomplete or dissociated lesions, andfor the localization of plexus lesions and thedifferentiation between pure cauda equinalesions and those complicated by superimposeddamage to peripheral nerves or sympatheticcolumn, the Q.S.T. has yielded informationallowing accurate diagnosis, which could notbe obtained by mere consideration of the dis-turbances of the motor and sensory functionsalone. Moreover, the success of operationsinvolving the removal of portions of thesympathetic nervous system can be determinedaccurately by this method.The more widespread the use of the Q.S.T.
as a supplement to other diagnostic methodsand, in particular, for clinical and physiologicalresearch, the more essential it is to employ anadequate and standardized technique toguarantee optimum conditions for accurateresults. The purpose of this paper is topresent a full description of the author'stechnique in the management of the Q.S.T.,as developed during the last ten years.
The Quinizarin CompoundThe sodium salt of quinizarin (2-6-disul-
phonic acid) is the colour indicator. It isa red-brown dye and a derivative of anthro-quinon similar to alizarin, purpurin and.anthraruphin, all of which are used in the dyeindustry. For application to the human skinthe quinizarin must be mixed with sodiumcarbonate in order that the colour change withmoisture shall take place whatever the pH ofthe sweat secretion; rice starch is also addedto economize in the amount of dye that has tobe used. The following mixture is mostsuitable:
Quinizarin 2-6-disulphonic acid...... 35 g.Sodium carbonate (powdered) ........ 30 g.Rice starch .................... 60-70 g.This compound is obtainable as a powder
ready for use in containers of .250 gm. fromBurroughs Wellcome and Co., London.On occasions it has proved useful to change
these proportions, and the powder has evenbeen mixed with olive or paraffin oils forspecial investigations. The powder form,however, has proved satisfactory for all clinicalpurposes. On account of the affinity ofquinizarin for water the test powder must bestored in absolutely dry and air-tight con-tainers. When performing a test the necessaryquantity of powder should be removed fromthe container, which should be resealed atonce. It has been found that a slight changein colour from red-grey to blue-grey whichoccurs after a time does not interfere with theusefulness of tte mixture.
Investigation Room-Sweat CabinetAll tests are carried out in a room. set out
apart for the purpose, in order to provide.standard conditions. This is essential if theQ.S.T. is combined with measurements of
by copyright. on A
ugust 12, 2021 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.23.262.353 on 1 A
ugust 1947. Dow
nloaded from

354 POST GRADUATE MI
vasomotor activity by thermocouples andplethysmographs, or if combined with cysto-metrography for studying the correlations ofsweating and other autonomic responses tobladder activity-also for sensory tests afterthe thermoregulatory sweat test. Standardconditions are especially valuable forsensory tests in cases of peripheral nerve,-spinal root and spinal cord lesions, in whichstudies of recovery of sweating in relation tosensibility are carried out at regular intervals.The room is equipped with adequate lighting
arrangements for photographic purposes.A small bathroom adjoins the research room,
where the patient can be cleaned after theQ.S.T., and the spreading of the dye to otherrooms is thus avoided. The dye is easilyremovable with soap and water.The two most common methods of produc-
ing thermoregulatory sweating used are immer-sion of limbs in hot water and exposure ofparts of the body under hot air cradles.Immersion of limbs in hot water certainlyprovides useful information in certaininstances, e.g., for inducing reflex dilatationand sweating, but often finer details, especiallyin recovering peripheral nerve lesions, are notsatisfactorily revealed. If ordinary heat cradlesare used, apart from the danger of suffocatingthe patient and of burning anaesthetic areas ofskin, it is often very difficult for the patient toadopt the most suitable position for theinvestigation. These difficulties have beenobviated by specially designed sweatingcabinets. In a previous paper (I941), descrip-tion was given of a sweat box designed by theauthor for the work at the Peripheral NerveInjury Unit at the Wingfield-Morris Ortho-paedic Hospital, Oxford, consisting of twowooden sections, which fit into a standardhospital bed. Either section of the box canbe readily removed, and the box is portable.The box is fitted with two glass windows oneither side, to allow careful observation fromall directions throughout the test. They canbe opened for changing the patient's positionor for the application of fresh powder duringthe test, if some of the powder has come off orit is necessary *to investigate a greater areathan was indicated by previous clinical signs(Fig. i). The temperature within the box is
-DICAL JOURNAL August 19479
regulated by Iz electric lamp bulbs of 25 wattseach.During the last three years, the author has
designed several improved types of sweatcabinets, which are more comfortable for thepatients and, in particular, more suitable forthe investigation of patients with extensiveparalysis due to spinal cord or brain lesions.They are also equipped with thermocouples,and these allow combined studies of sweatingand vasomotor function. The latest model,which was built by the Engineering Depart-ment of the Ministry of Works (the author isespecially grateful to Mr. G. Smith and hisstaff for their co-operation), is demonstratedin Figs. 2a, b and c.The construction of the sweat cabinet is as
follows:Dimensions:
Length.. 6 ft. 9 in.Width .. 3 ft. 3 in.Height .. 3 ft. 9 in.
The patient lies on a trolley within thecabinet, i ft. 8 in. above the floor, and can bemoved on this trolley to the bath after the test.The cabinet is timber framed and the wallsand ceilings are formed of two thicknesses ofplywood separated by 2 in. air space.
Ventilation. By an electrically driven centri-fugal fan, mounted in a separate control deskwith 4I in. bore flexible air connection to thecabinet. The fan delivers 6oo cubic ft. of airper hour, the air being delivered into thecabinet in an upward direction to avoidimpinging on the patient; the volume isadjustable by a small damper. A small,75-watt electric heater is fitted in the fandischarge to preheat the air to.between goo andI00° F. before admission to the cabinet. Airis discharged from the cabinet through a smalladjustable grill.
Heating. The cabinet is heated by banks ofcarbon filament lamps and tubular heaterswhich are mounted on the ceiling of thecabinet, which is fitted with a chromium-plated reflector; 24-32 candle-power, I30-watt carbon filament lamps are provided andcontrolled in banks of three lamps by switchesmounted on the outside of the cabinet. Inaddition, four tubular heaters, each 6 ft. long,loaded at 6o watts per ft., are installed.Experience has shown'that the tubular heaters
by copyright. on A
ugust 12, 2021 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.23.262.353 on 1 A
ugust 1947. Dow
nloaded from

GUTTMANN: The Management of Quinizarin Sweat Test
are not so effective as carbon filament lampsfor promoting rapid sweating of the patient.A' Cambridge' direct-reading, dial-type ther-mometer is provided to indicate air tempera-tures adjacent to the patient.
Cabinet humidity. A Negretti and Zambrahair-type, direct-reading hydrometer is pro-vided for indicating relative humidity near thepatient.
Bodv Temperature Measurement(a) Skin temperatures. Ten plug-in type
thermocouples are provided for the measure-ment of skin temperatures. Permanent copperconstantan compensating leads are connectedbetween plugs in the cabinet and the controldesk. Flexible compensating leads are takenfrom the ten plugs in the cabinet to withini ft. of the hot junctions, the remainingcouples being of No. 32 S.W.G. copper con-stantan, terminating on a circular silver plateabout 3 in. diameter which, in turn, is mountedon a sponge rubber and bakelite finger. Thesponge rubber ensures good contact betweenthe hot junction of the thermocouple and thepatient's body.
(b) Rectum temperatures. Couples are pro-vided for taking rectum temperatures. Thehot junction is inserted into and soldered toa silver tube about 2-1 in. long by 3 in.diameter. The couple leads are suitablyinsulated for sterilizing.
(c) Mouth temperatures. Couples are alsoprovided for obtaining mouth temperatures.Again the hot junction is inserted into a silvertube of oval section. The length of the tubeis 31 in. and the cross section axes 3/32 in.by 1 in.
(d) Potentiometer and cold junction. ANegretti and Zambra nul-point, quick-readingpotentiometer calibrated to read in degreesFahrenheit is provided on the control cabinet,together with a melting ice-cold junction anda multi-way change-over switch.
Control desk. The control desk, in additionto housing the fresh air in-put fan, potentio-meter, etc., is provided with a main powercontrol switch, switches controlling tubularheaters and banks of lamps, together withindicator lamps.Thermocouples and main wiring connections
between the control desk and the cabinet are
carried via' Plessey' multi-pin connectors andflexible conduit.
Position of the PatientThe position of the patient is important.
He must lie comfortably in such a manner thatthe area to be investigated may be inspectedeasily and the running of sweat from normalor hyperhidrotic areas into anhidrotic orhypohidrotic areas is avoided. The limbs aresupported on sandbags or on slings, asrequired. In peripheral nerve lesions, themost suitable position of the patient varieswith the nerve under investigation and withthe associated contractures of the joints in thedamaged area. It is beyond the scope of thispaper to describe in detail the optimumposition for everv nerve, but a few examplesmay be given. In an isolated lesion of thevolar branch of the ulnar nerve, the hand andforearm should be placed in full supination,in order that sweating in the areas of themedian nerve and dorsal cutaneous branch ofthe ulnar cannot run into the denervated area.In an isolated lesion of the dorsal cutaneousbranch of the ulnar, or in a lesion of all ulnarbranches, the forearm should be pronatedand the wrist kept in dorsiflexion to preventthe running of sweat from the median andsuperficial radial nerve areas and from theareas of the medial and dorsal cutaneousnerves of the forearm. In testing the externalpopliteal nerve, the leg should be elevated byplacing a support underneath the heel, toensure full exposure of the posterolateraldistribution of the nerve in the middle andupper third of the leg. In certain instances,such as lesions of the whole sciatic nerve,sacral plexus or root lesions, the patient isplaced in the abdominal position, withsufficient support underneath the knees, inorder to outline the whole area involved. Inbrachial plexus lesions, the paralysed limbmust be supported by slings and occasionallyit will be necessary to perform two sweatingtests to get full information about the extentof the lesion.
Method of Study*When the patient has adopted a suitable
position in the box, the area of skin to be
August I 947 355
by copyright. on A
ugust 12, 2021 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.23.262.353 on 1 A
ugust 1947. Dow
nloaded from

POST GRADUATE MEDICAL JOURNAL
investigated is dabbed with quinizarin com-pound on a swab of cotton wool and sufficientpressure is employed to ensure that the orificesof the sweat glands are filled with powder.The area must be thoroughly covered withthe powder and the powder evenly distributed.Application of the powder with an atomizerwas found to be unsatisfactory, owing to thelack of pressure and the unnecessary sprayingof powder all over the room. It should bementioned that the powder is quite harmlessand tests can be carried out repeatedly atshort intervals. 'Ihis is a special advantagethat the quinizarin method has over other dyetests-for instances, iodine starch methods(V. Minor, I927), and especially the ferro-sulphate-ether-alcohol method- (Rieder andNeumann, 1932). Special care should betaken in powdering the face, to avoid any dustsetting up mucosal irritation during theapplication of the powder. Droplets fromsneezes or tears may moisten the powder andspoil the test. Therefore, when the face ispowdered the patient's eyes must be keptclosed. In many cases, it will be necessary topowder larger areas of the body in order tostudy the cutaneous reflex phenomena causedby the lesion. In brachial plexus'lesions oneshould always remember the possibility ofthere being an associated lesion of portions ofthe cervical sympathetic and therefore theface should be powdered on both sides. Incases in which 'insufficient powder has beenapplied, or in patients with a skin so smooththat the powder has not adhered, repeatedpowdering is necessary during the test to bringabout clear contrast>.
'The Thermoregulatorv Sweat TestWhen the powdering is completed, the
doors of the sweat cabinet are closed and thetemperature within the box is raised gradually.As a rule, the temperature within the box israised from room temperature to i I00 or1200 F. The duration of heating required toproduce sweating is subject to individualvariations (r5-35 minutes) and the onset and-the intensity of the sweating is influenced byvarious extrinsic and intrinsic factors, such asatmospheric conditions (especially humidity),age, sex, endocrine metabolic factors, thelevel and completeness of the nerve lesion.
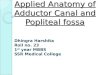
Onset of sweating can be facilitated, and itsintensity promoted, by a hot drink andaspirin grs. 5-I0 given five to ten minutesbefore the test. The following recordcorrelates the changes in skin and rectaltemperatures to sweating at various stages ofthe test (Fig. 3).When the secretion of visible sweat com-
mences, the hidrotic areas of skin take. on adark, blue-violet colour, whilst the anhidroticareas remain unchanged in colour. Theopening of the individual sweat ducts appearas small, dark dots. These details are shownin a close-up photograph in Fig. 4, whichdemonstrates complete anhidrosis in themedian nerve distribution, with scatteredindividual sweat ducts in the border zonesdemonstrating the intermediate zone of theinterrupted median nerve with its neighbours,the ulnar and the radial.
It is essential to observe 'the details ofsweating throughout the various stages of thetest. Unless the progress is carefully observed,the results may be quite fallacious, especiallyin incomplete lesions of peripheral nerves.Placing the patient under hot air cradles,powdering him and then leaving him aloneuntil the termination of the test is a haphazardmethod, which' is to be condemned moststrongly. In the course of the test, one mustnote the onset, distribution' and amount ofsweating, not only in the area supplied by theinjured peripheral nerve, sympathetic gangliaor spinal segment, but also in the areas suppliedby the neighbouring normal parts of the bodyand even in corresponding areas on theopposite side of the body. Some reflexphenomena, such as perilesionary hyper-hidrosis (Guttmann and List, I928), or borderzone reflexes (Guttmann, I933, I9401) althoughobvious in a great 'number of cases at thecommencement of the test, may be obscuredlater on when sweating is profuse. This isshown in a case of complete lesion of thespinal cord at Th. Io/II, where at the begin-ning of the test the level of the lesion iswell-marked by the early onset of sweatingand hyperhidrosis in the border zone abovethe level (Fig. sa), whilst at the end thehyperhidrotic zone is obscured by profusesweating in all areas above the level of thelesion (Fig. sb). Thus, it is often necessary
356 A4ugust I1947by copyright.
on August 12, 2021 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.23.262.353 on 1 August 1947. D
ownloaded from

August 1947 GUTTMANN: The Managemlent of Quiniizarin Sweat Test 357
FIG. I.
t.-
!4
FiG. 2a.
by copyright. on A
ugust 12, 2021 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.23.262.353 on 1 A
ugust 1947. Dow
nloaded from

358 POST GRADUATE MEDICAL JOURNAL August 1947
*(
t.........
FiG. 2b.
|ww-
*|d-.::.:;e I'll"'
FIG. 2C.
by copyright. on A
ugust 12, 2021 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.23.262.353 on 1 A
ugust 1947. Dow
nloaded from

August I947 GUTTMANN: The Management of Quinizarin Sweat Test 359
130 F
120
/ / t110 oo
00 -s)x X Saxt Recta/l emp.
X*x1x A xERtiA X
90 Left<;e0Hndlx/ngel
B x8Ou Temo. x Commencement of sweating
s0 / ' &ekfootf(dorsom) xx Profuse sweating
x xx xxx xxx Maximal sweating
705 ,0 Is 20 2S 30 35 40 45 50 55 60 65 70
Time in Minutes
FIG. 3.
FIG. 4
by copyright. on A
ugust 12, 2021 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.23.262.353 on 1 A
ugust 1947. Dow
nloaded from

360 POST GRADUATE MEDICAL JOURNAL August 1947
..
-..: .... ... .. :. .::: ....:.:;;
FIG. 5a.
by copyright. on A
ugust 12, 2021 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.23.262.353 on 1 A
ugust 1947. Dow
nloaded from

Aiagqust 1947 OUTTMANN: The Management of Quinizarin Sweat Test 3b6
---
|
|-'ty' 1| || |*1 ||
g1 iI-s
..
XX1
:: ^ ;; |%.:.:...
...
*:
*X:f
*:t
FIG. 5b.
area of anaesthesia
. o o : area of analgesia
by copyright. on A
ugust 12, 2021 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.23.262.353 on 1 A
ugust 1947. Dow
nloaded from

362 POST GRADUATE MEDICAI, JOURNAL August 1947
:/
FIG. 6.
..... .... ....--.o°... .;...I
:R:C~~ ....|.... P..!Y
m&.,=°fi.,.t.i'& ;° .,.l2?r.
b;r°4 .:
FIG. 7.
*.... ..:: ... :.. .......
:: ::.:
XN. .:ZNX:N{Qh*;..: :.
... ....: .:.; : .: : :i .:.... .... . .. .:
:.....
.....*:.::* .: :.;:; .::.;: :. . .. : .X:<t... : .: .. : : ..... . :X...:NX
:: .. ... ;:.X |: XFIG. 8a
by copyright. on A
ugust 12, 2021 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.23.262.353 on 1 A
ugust 1947. Dow
nloaded from

August I947 GUTTMANN: The Management of Quinizarin Sweat Test 363
.IG
FIG. Fb.
by copyright. on A
ugust 12, 2021 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.23.262.353 on 1 A
ugust 1947. Dow
nloaded from

364 POST GRADUATE MEDICAL JOURNAL August 1947
FIG. I 0.
wi..
FIG. I1I.
FIG. 12.
......
by copyright. on A
ugust 12, 2021 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.23.262.353 on 1 A
ugust 1947. Dow
nloaded from

GUTTMANN: The Management of Quinizarin Sweat Test
to make photographic records of the earlystages of the test. The test must be continueduntil maximal sweating has occurred in allparts of the body. Only in this way can onecompare findings in successive tests. This isof particular importance in testing peripheralnerve lesions in the various stages of regenera-tion. It must be remembered that the activityof recently reinervated sweat glands is charac-terized by a delayed onset, and diminisheddegree, of secretion and, therefore, a strongerand prolonged heat stimulus is necessary tobring these glands into action.At the termination of the test, the tem-
perature within the sweat cabinet is graduallyreduced. The powder, which has beenmoistened and discoloured by sweat secretion,adheres to the skin. Superfluous dry quini-zarin powder is removed by careful dustingwith a small piece of cotton wool. Areas ofnormal or excessive sweating are clearlyoutlined by a uniform deep purple staining.In areas of hypohidrosis, such as in incompletelesions, or in the intermediate zone of completelesions of peripheral nerves or areas of earlyregeneration, sweating is characterized by smallpatches or isolated pin-points of sweat, whichshow various degrees of colour intensity, thusdemonstrating the various degrees of sweatgland activity. The anhidrotic areas are notdiscoloured. Fig. 6 demonstrates a state ofrecovery of sweat glands in the distribution ofthe median nerve about 20 months after nervesuture in the middle of the forearm. Therewas recovery of pain and touch sensibilityalso, with the exception of the tips of indexand middle fingers, which were still anaesthetic(marked by uninterrupted line).The results of the sweat test and also of the
sensory examination are recorded photo-graphically. The fine pin-points of sweatingin hypohidrotic. tas, can be shown up satis-factorily oily by dwe..-up photography (Fig. 4).In naany cases, parficularly of regeneratingverve lesions, the fine pin-points of sweatingrequire accentuation by fine ink spots, toachieve accurate photographic records of themost distal distribution of sweat glands activity.
Correlation of Q.S.T. and Sensory TestThe Q.S.T. can be usefully employed as
a guide for sensory tests in peripheral nerve
and plexus lesions. Sensory tests are carriedout after the sweating test, when the patienthas adapted himself to the room temperature.This technique has been adopted by the authorsince 1939 as a routine in many hundreds ofperipheral nerve and spinal cord lesions.Generally speaking, in complete lesions ofperipheral nerves, the area of anhidrosiscorresponds closely to the area of analgesia inthe autonomous zone, i.e., that zone suppliedsolely by the interrupted nerve. In the inter-mediate zone, which is also supplied by theneighbouring nerves and where loss ofsensibility is partial, there is usually obviousreduced sweating. However, experience fre-quently has shown that there is dissociationbetween the areas of analgesia and anhidrosis.If pain sensibility is carefully tested and bothsuperficial and deep needle pricks are em-ployed, it will be found that anhidrosiscorresponds more closely to the area of anal-gesia to superficial or moderate needle pricks,and within the border of this superficialanalgesia there is an irregular zone in whichdeep needle pricks are appreciated. Moreover,sweating may also occur well within the borderof superficial analgesia. This extension ofsweating occurs usually in the form of irregularencroachments or indentations. Sometimes,in these encroachments of sweating, even adeep needle prick is not appreciated as pain.This is shown in Fig. 7, demonstrating a partof the area of sensory loss and of anhidrosisin a case of complete division of the externalpopliteal nerve. It shows the encroachmentsof sweating from either side into the dener-vated area and the dissociation betweenanaesthesia (uninterrupted line), analgesia,(dotted line} and anhidrosis. Figs. 8a and bdemonstrate a case of dissociated lesion of theexternal popliteal nerve, in which the branchesof the lateral cutaneous nerve of the leg andthe musculocutaneous nerve were completelyinterrupted, whereas the anterior tibial branchshowed an incomplete lesion only, i.e., markedweakness of the tibialis anticus and extensorhallucis longus, whereas sensibility and sweat-ing were not appreciably disturbed, as shownby the good sweating of the dorsum of thefirst and second toes and of their interspaces.In this case, there was a close correlationbetween analgesia (dotted line) and anhidrosis.
Augucst 1947 365by copyright.
on August 12, 2021 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.23.262.353 on 1 August 1947. D
ownloaded from

366 POST GRADUATE MEDICAL JOURNAL August I947
The white line demonstrates the area ofanaesthesia. Fig. 9 demonstrates the anhid-rosis and sensory loss in a full thickness skingraft a few weeks after operation, in whichthe close correlation between analgesia andanhidrosis is obvious also (the crosses demon-strate the area of analgesia to deep pin prick,the uninterrupted line the area of anaesthesia).Certain types of plexus lesions and, in par-ticular, lesions of the spinal cord show pro-nounced dissociation between the disturbanceof sweating and the various modalities ofsensibility. In incomplete lesions of thecervical cord, for instance, the lesion mayselect sudomotor fibres only in certain seg-ments of the distal parts of the body. This isshown in Fig. io by the marked impairmentof sweating on the right side of the trunk andleg in a case of an incomplete lesion of thecervical cord due to fracture-dislocation ofthe sixth cervical vertebra. The analgesia(interrupted line) involves the whole leftside of the body below Th. 4 and on the rightside the fourth and fifth thoracic dermatomes.The thermoanaesthesia (dotted and crossedlines) involves both sides of the body belowthe first thoracic dermatomes. On the motorside, there was spasticity in both lower limbs,particularly in the right leg.
Local Factors in Influencing Sweat- SecretionThe Q.S.T. often reveals disturbances of
sweating which are produced by factors otherthan lesions of the nervous system. It isnecessary to refer here to at least the moreimportant of these factors, as they can besuperimposed on a nerve lesion and thusproduce an area of disturbance of sweatinglarger than one would expect from the nervelesion alone. It must first be rememberedthat sweating is already diminished undernormal conditions in areas of skin which are
exposed to permanent pressure and friction byunderlying bony prominences, such as tip ofthe shoulder and elbow, the lower end of theulnar, the knuckles of the fingers and toes,the trochanteric area, the patella, the medialand lateral malleoli and the fifth metatarsal.Classical examples of the patliologically in-creased impairment of sweating (often com-bined with sensory disturbance) due topressure by prominent bone, are seen -in casesof hallux valgus.
Sweating may be affected also by extrinsicfactors due to pressure, such as splints, plasterof paris, adhesive plaster and other dressings(Fig. X i shows a complete lesion of the caudaequina at the level of L.i/L2.). As one wouldexpect in such a case, there is good sweatingover both lower limbs. There is, however,a sharply defined quadrangular area of almostcomplete anhidrosis over the lower abdominalregion on either side, obviously produced byelastoplast strapping, which was used to fastenthe dressing over the suprapubic cystotomywound.
In numerous cases of peripheral nervelesion, an atypical large area of sweat distur-bance is found, provided by superimposedlocal damage to the skin due to pressure bysplints, plaster and other factors. For'instance, in an ulnar nerve lesion it mayinvolve the whole palmar aspect of the hand.In patients with certain occupations, such aslabourers or butchers, this local damage isdue to permanent pressure caused by theirtools, and the disturbance of sweating corres-ponds to the hyperkeratosis of the palm inthese cases. Fig. 12 demonstrates a case ofcomplete lesion of ulnar nerve withoutevidence of injury to the median- nerve.There was, however, poor sweating in themedian area in the palm of the hand, due tolocal hyperkeratinization, whereas sweatingover the palmar aspect of the fingers in themedian area was unimpaired and profuse.
BIBLIOGRAPHY
GU'TT'MANN, L., and LIST, L. F. (1928), Z. Neur., 1z6, 504. (1946), Br. Yourn. Phys. Med., 9, I35.GUTTMANN, L. (I933), Z. Neur., 147, 291. HIIGHET, B. W. (I942), J. Neurol. and Psychiat., S, Ioi.--(1937), Klin. Wschr., 1,6I292. LEWIN, W. (I1943), Lancet II,' 756.=- (1938), CYonfina Neurol. 8, 296. MINOR, V. (I928), Dtsch. Z. Nervhik., Ioi.
(1940), J. Neural, and Ptychiat., 3, S97 RIEDER, A.,,AND NEUMANN, L. (I932), Klin. Wschr., II.,-(I94I), Proceedings of the Royal Soctety of Medicine, vol. 35, SEDDON, 1. H. (I942), Surgery of Modern Warfare, 52 S6o.77. Publisher E. and S. Livingstone, Edinburgh.
by copyright. on A
ugust 12, 2021 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.23.262.353 on 1 A
ugust 1947. Dow
nloaded from