Embed Size (px)
Citation preview

The Management of Alzheimer’s Disease and Related Dementias
The Treatment of Alzheimer’s Disease and Disease Progression Modification

Alzheimer’s Disease (AD): Overview
Progressive, degenerative CNS disorder Characterized by memory impairment plus one or
more additional cognitive disturbances Gradual decline in three key symptom domains
– Activities of daily living (ADL)
– Behavior and personality
– Cognition Most common cause of dementia in people
aged 65 and over

Evans DA, Scherr PA, Smith LA, et al. Aging (Milano). 1990(Sept);2(3):298-302; Ernst RL, Hay JW. Am J Public Health. 1994(Aug);84(8):1261-1264; Alzheimer’s Association, 2002
Alzheimer’s Disease: Economic Consequences
Third most expensive disease in the US Costs over $100 billion/year Further $33 billion in lost productivity
and other employer costs 3/4 of patients admitted to residential care
within 5 years of diagnosis

Adapted from Brookmeyer et al, 1998.
8
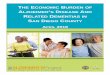
Delay (Years)
US
Pre
vale
nce
of
AD
(Mil
lio
ns)6
4
2
0204720372027201720071997
0 1 5
Potential Impact of Interventions to Delay Onset of Alzheimer’s Disease

Potential to Increase Diagnosis and Treatment Across Disease Stages
AChE = acetylcholinesterase1Mattson Jack; 2MMI MDAD, 2001; 3On CHeI—midpoint of last year’s treatment by severity rates and rates reported in Reminyl uptake, 2001; 4Decision Resources.
0
200,000
400,000
600,000
800,000
1,000,000
1,200,000
1,400,000
Mild4 Moderate4 Severe4
Number of patients1
Diagnosed2
Treated with AChE inhibitor3
Nu
mb
er o
f P
atie
nts
Disease Stages

Knopman D, Scheider L, Davis K et al. Neurology. 1996(July);47(1):166-177.
Pro
bab
ilit
y o
f R
emai
nin
g a
t H
om
e
Time (Weeks)
80 mg
>80 to 120 mg
>120 to 160 mg
11410085715742281200.4
0.6
0.8
1.0
Long-term Effects of Tacrine on Nursing Home Placement

Hill JW, Futterman R, Duttagupta S, et al. Neurology. 2002(Jan 8);58(1):62-70.
0 5 10 15 20 25
Renal Disease
Cerebrovascular Disease
Peripheral Vascular Disease
Chronic Pulmonary Disease
Diabetes
Diabetes withChronic Complications
Congestive Heart Failure
Annual Cost (Thousands)
Nondemented19,300 matched
ADRD 3,934
Dementia Increases the Costs of Caring for Common Comorbidities in Managed Medicare Settings

Haley WE, Levine EG, Brown SL, et al. Am J Geriatr Soc. 1987(May);35(5):405-411Shaw et al., J Psychosom Res 2003; 54:293-302vonKanel et al., Am J of Cardiol 2001(June);87:1405-1408Grant I, Psychosom Med 1999; 61:420-423
Caregiver Burden in AD
Compared with noncaregiver controls matched by age, gender, race and marital status, caregivers of persons with AD or related disorders require– 46% more physician visits
– 71% more prescribed medications
– Higher diastolic blood pressure
– Hypercoagulable state
– Higher plasma norepinephrine

5% 10% 65% 5% 7% 8%
Dementia with Lewy bodies Parkinson’s disease
Diffuse Lewy body disease Lewy body variant of AD
Vascular dementias and AD
Other dementias Frontal lobe dementia
Creutzfeldt-Jakob disease Corticobasal degeneration
Progressive supranuclear palsy Many others
AD and dementia with Lewy bodies
Vascular dementiasMulti-infarct dementiaBinswanger’s disease
AD
Small et al, 1997; APA, 1997; Morris, 1994.
Differential Diagnosis of Dementia

AP=amyloid plaques; NFT=neurofibrillary tanglesCourtesy of George Grossberg M.D.; St. Louis University.
Normal AD
AP NFT
Neuropathologic ChangesCharacteristic of AD

PET and Genetic Risk forAlzheimer’s Disease
Small GW, Ercoli LM, Silverman DH. Proc Natl Acad Sci. USA. 2000(May) 23);97(11):6037-6042 .
Normal MemoryNormal Memory
No APOE -4
PET PET ImagingImaging
Genetic Genetic Risk:Risk:
DementiaDementia
APOE -4
-28% -31%-14%-6%

Alzheimer’s Disease Normal ControlDecreasedtemporoparietal
Occipitallobe
Cerebellum 0.00 19.36
Frontallobe
mg/100 g/min
UCI Brain Imaging Center

Silverman DH, Small GW, Chang CY, et al. JAMA. 2001 Nov 7;286(17):2120-2127
PET in the Evaluation of Dementia
284 dementia patients(138 autopsy-confirmed diagnosis)
Sensitivity 93%; specificity 76% Negative PET scan indicated chance of
cognitive progression <20% over 3 years

Rogers and Friedhoff, 1998; *Stern et al, 1994.
–6
0
6
12
180 6 12 14 26 38 50 62 74 85 98
AD
AS
-Co
g S
sco
reM
ean
Ch
ang
e fr
om
Bas
elin
e
Cumulative Weeks from Baseline of the Double-blind Study
Decline in ADAS-Cog scorebased on the natural history ofuntreated patients with moderateAD*
Improvement
DeclineN=133
Model-based Analysis: ADAS-Cog Score Mean Change from Baseline

Flynn et al, 1995; Perry et al, 1978; Rodriguez-Puertas et al, 1997; Whitehouse et al, 1982.
Major Cholinergic Changes in AD
Depletion of acetylcholine (ACh): especially in moderate to severe disease stages
Decline in choline acetyltransferase (ChAT) activity
Loss of cholinergic neurons– Loss of muscarinic (M2) receptors
– Loss of nicotinic receptors (nAChR) AChE Butylcholinesterase (BuChE)

AChE
AcetylCoA
CholineACh
Presynaptic neuron
Synaptic cleft
Postsynapticneuron Acetate
CholineCholine+
+
Glial cell
ACh
AChE
BuChE
BuChE
ChAT
CoA=coenzyme A; MR=muscarinic receptor; NR=nicotinic receptorAdapted from Adem, 1992.
MR1
MR2 NR
MR1 MR2 NR
Normal Cholinergic Function

Cholinesterase Inhibitors
Physicians’ Desk Reference, 2003.
AChCH3
O
ON
H3C
CH3
H 3C
+
Rivastigminemechanism: AChE/BuChE-I
NH3C
CH3
CH3
O N CH3
CH3
O
Donepezilmechanism: AChE-I
H3CO
H3CO
O
CH2
N CH2
.
Galantaminemechanism: AChE-I
O
N
HOOCH3
H3C
NEW

ChE Inhibitors: Overview
Enz et al, 1992, 1993; Samochocki et al, 2000; Svensson and Nordberg, 1997; Yamanishi et al, 1990; Cutler and Sramek, 1998; Inglis, 2002.
AChE Inhibitors
Dual AChE/BuChE Inhibitor
Characteristic Donepezil Galantamine Rivastigmine
Doses per day 1 2 2
Maximum dose (mg/d) 10 24 12
Brain region selectivity No No Yes
Reversibility Reversible Reversible Psuedo-reversible
Nicotinic allosteric modulation No Yes No
Cytochrome P450 metabolism Yes Yes No

Allosteric Nicotinic Receptor Modulation
Samochocki M, Zerlin M, Jostock R, et al. Acta Neurol Scand Suppl. 2000;176:68-73
Response amplitudeto 100 µM ACh
AC
h-I
nd
uce
d C
urr
ent
(pA
)
Concentration (µM)
GalantamineRivastigmineMetrifonateTacrineDonepezil
0
200
400
600
800
1,000
0.001 0.010 0.100 1.000 10.000
NEW

*Darvesh S, Grantham DL, Hopkins DA. J Comp Neurol. 1998(April 13);393(3):374-390. †Mesulam, 2000.
BuChE neurons are less abundant than AChE neurons BuChE is very rich in cortical and limbic areas (amygdala and
hippocampus) BuChE accumulations in neuritic plaques
Amygdala
Figure 1* Figure 2†
AChEBuChE Hippocampus
Distribution of Cholinesterases in the Healthy Human Brain

Darvesh S, Hopkins DA. J Comp Neurol. 2003;463(1):25-43.
Distribution of Cholinesterases in the Healthy Human Thalamus

Rivastigmine Inhibition of CSF BuChE/AChE: Correlation with CNTB Scores
Cutler et al, 1998; Costa et al, 1999;Giacobini et al, 2002.
*P<.01; **P<.05CNTB=computerized neurophysiological test batteryCSF=cerebrospinal fluid
AUC
Cognitive Performance CNTB BuChE Activity AChE ActivityCNTB summary score -0.65* -0.56*Paired assoc. learning -0.53** -0.22Paired assoc. learning/delayed recall -0.69* -0.36Visual memory -0.52** -0.42
BuChE in CSF
0 2.5 5.0 7.5 10.0 12.5
150
100
50
0
Time (Hours)
Per
cen
tag
e o
f B
asel
ine
mea
n ±
SE
M
Rivastigmine 3 mg po
AChE in CSF
0 2.5 5.0 7.5 10.0 12.5
150
100
50
0
Time (Hours)
Per
cen
tag
e o
f B
asel
ine
mea
n ±
SE
M
Rivastigmine 3 mg po

Relation between Activity and Numbers of Senile Plaques in the Cerebral Cortex
Perry, 1978.
0
20
40
60
80
100
120
140
160
180
200
0 1-5 6-10 11-20 21-30 30-42
Mean Plaque Count
Per
cen
tag
e o
f ac
tivi
ty i
n
gro
up
wit
h n
o p
laq
ues
BuChE
AChE
ChAT

Guillozet et al, 1997.
Compact Plaque Formation

BuChE
Arendt et al, 1992.
0 50 100 150 200
1.50
1.25
1.00
0.75
0.50
Density of A Deposition
G1
nm
ol/
Min
. x
mg
Pro
tein
AChE
Activity of ChEs and -amyloid (A) Deposition in AD Cortex

Davidsson et al, 2001.
50
40
30
20
10
0 Baseline 12 months
AC
hE
Act
ivit
y m
mo
l/m
L/M
in.
P=.0013
800
700
600
500
400
300
200
100
0
10 mg 5 mg 32 mg 24 mg
CS
F A
Ch
E
Pro
tein
Donepezil Galantamine PlaceboTacrine (80–160 mg/day)
0 12 0 12 0 6 0 6 0 12 months
Nordberg et al, 1999.
Long-term CSF Inhibition: Upregulation of AChE by Tacrine, Donepezil, and Galantamine

High-dose rivastigmineLow-dose rivastigmine
Darreh-Shori et al, 2002.
Treatment Length (Months)
Inh
ibit
ion
of
CS
F A
Ch
E (
%)
60
50
40
30
20
10
0
-100 3 6 9 12 0 3 6 9 12
Inh
ibit
ion
of
CS
F B
uC
hE
(%
)
8070605040302010
0-10
Treatment Length (Months)
Long-term CSF Inhibition: Sustained Inhibition of AChE and BuChE by Rivastigmine

Rogers and Friedhoff, 1998; *Stern et al, 1994.
–6
0
6
12
180 6 12 14 26 38 50 62 74 85 98
AD
AS
-Co
g S
core
mea
n C
han
ge
fro
m B
asel
ine
Cumulative Weeks from Baseline of the Double-blind Study
Decline in ADAS-Cog scorebased on the natural history ofuntreated patients with moderateAD*
Improvement
Decline
Model-based Analysis: ADAS-Cog Score Mean Change from Baseline

Baseline 3 6 9 12 18 24 30 36
–6–4–2
02468
1012141618202224
AD
AS
-Co
g S
core
Mea
n C
han
ge
fro
m B
asel
ine
Time (Months)
Estimated decline: Stern equation12 months placeboGalantamine 24–32/24 mg/d
Truyen and Kershaw, 2002; Stern et al, 1994.
ADAS-Cog: Mean Change from Baseline during up to 36 Months’ Treatment with Galantamine
Time (Months)
Baseline 3 6 9 12 24 36
Number of Patients 165 165 165 165 160 124 81

Withdrawal Design Staggered-start Design
Time
Per
form
ance
Time
Per
form
ance
Randomizedphase
Randomizedphase
Placebophase
Placebophase
Placebo
Active
Placebo
Active
Symptomatic effect
Disease-modifyingeffect
Disease-modifyingeffect
Symptomatic effect
Leber, 1997.
Discrimination between Disease Modification and Symptomatic Benefit

*P<.0012; **P<.0007; ***P<.0001 vs placebo; mean MMSE score=19Rogers SL, Farlow MR, Doody RS, Mohs R, Friedhoff LT. Neurology. 1998(Jan);50(1):136-145
Baseline 6 12 18 Endpoint 30Decline
Improvement
Placebowashout
Weeks on Therapy
AD
AS
-Co
g M
ean
Ch
ang
e fr
om
B
asel
ine
-3
-2
-1
0
1
2
3
4
10 mg/day (n=157)5 mg/day (n=154)Placebo (n=162)
***
***
******
** *
Effects of Donepezil on Cognition

Galantamine 24 mg/ Galantamine 32 mg/ Placebo/Galantamine 24 mg (n=116) Galantamine 24 mg (n=102) Galantamine 24 mg (n=135)
OC analysis; *P=.03 vs placebo/galantamine 24 mgRaskind et al, 2000.
–4
–3
–2
–1
0
1
2
3
4 Baseline 13 26 39 52
AD
AS
-Co
g m
ean
(±
SE
M)
Ch
ang
e fr
om
Bas
elin
e
Double-blind Open-label
Time (Weeks)
*
Improvement
DeclineAll patients receive galantamine
Long-term Effects of Galantamine on Cognition: ADAS-Cog Change from Baseline

Rivastigmine 6–12 mg
Rivastigmine 1–4 mg
Placebo
Projected placebo
*P<.05 vs projected placeboFarlow et al, 2000.
0 12 18 26 38 44 52
Study Week
210
–1–2–3–4–5–6–7–8–9
AD
AS
-Co
g M
ean
Ch
ang
e (±
SE
M)
fro
m B
asel
ine
All patients taking rivastigmine
Long-term Effects of Rivastigmine on Cognition: ADAS-Cog

Doraiswamy et al, 2000.
All patients taking rivastigmine 2–12 mg/d
Study Week
0 26 38 44 52 78 104
–5
0
5
10
15
20
25
30
***
AD
AS
-Co
g M
ea
n C
ha
ng
efr
om
Ba
se
lin
e (
± S
EM
)
*P<.05; ***P<.001 vs projected placeboOC data set Baseline GDS 5
*
*** ***
***
*
*
******
*
Projected placebo
Rivastigmine 6–12 mg/d Placebo treatment up to 26 weeks
Rivastigmine 1–4 mg/d
****** ***
***
*
Effect of Long-term Rivastigmine Therapy on Cognition in Patients GDS ≥5

RDO Population
Mea
n C
han
ge
in A
DA
S-C
og
*
*P<.05
–2
–1
0
1
2
3
4
5
6
7
8
9
6–12 mg/day 1–4 mg/day Placebo
Farlow et al, 2003.
Rivastigmine Effect on Cognitive Function: Return Dropouts at Week 26

Potkin SG et al., Int J Neuropsychopharmacol. 2001;4(3):223-230
Increased frontal cortex
Increased hippocampus
Rivastigmine responders
minus baseline
Increase
Decrease
No change
Placebo
Natural Progression of AD over 6 Months vs the Effects of Rivastigmine

44
42
40
38
36
34
32
30
28
26
24
22
44
42
40
38
36
34
32
30
28
26
24
22
Glu
cose
met
abo
lism
R_FrM
gL_
FrM
gR_C
ingA
L_Cin
gAR_F
rSg
L_Fr
SgR_A
ngL_
Ang
R_Sup
r/Ang
L_Sup
r/Ang
R_Tem
p/M
g
R_Tem
p/M
g
R_FrM
gL_
FrM
gR_C
ingA
L_Cin
gAR_F
rSg
L_Fr
SgR_A
ngL_
Ang
R_Sup
r/Ang
L_Sup
r/Ang
R_Tem
p/M
gR_T
emp/
Mg
Untreated (n=12) Treated (n=11)
Baseline
Brain region Brain region
P<0.05all brain regions
12 months
Nordberg.
Glucose Metabolism in Cortical Association Areas for AD Patients with and without Rivastigmine Treatment

Cortex Hippocampus Cortex Hippocampus0
100
200
Ch
E A
ctiv
ity
% o
f R
esp
ecti
ve
Co
ntr
ol
Val
ues
±
SE
M
AD Brain Region
AChE BuChE
AChE and BuChE Activities in Human Postmortem AD Brain
Perry EK, et al. Neuropathol Appl Neurobiol. 1978;(4):273-277

BuChE staining in plaques, tangles, dystrophic neurites, and glia in AD
BuChE staining primarily glial in nondemented
Guillozet AL, Smiley JF, Mash DC, Mesulam MM. Ann Neurol. 1997(Dec);42(6):909-918
Selective Association of BuChE with Amyloid Plaques in Cortex AD

200
150
100
50
0Sec
rete
d
-AP
P L
evel
s in
R
at
CS
F (
Co
ntr
ol
± S
EM
%)
Nonlesion Nucleus basalis lesion
Control Phenserine CymserineBuChEIAChEI
Haroutunian V, et al. Brain Res Mol Brain Res. 1997;46(1-2):161-168
AChE and BuChE Inhibitors Decrease Endogenous -APP Levels in Rats

12
10
8
6
4
2
0
–20 0.7 0.8 0.9 1.0
MM
SE
Dec
lin
e/Y
ear
BuChE Level in Medial Temporal Cortex
R=0.88 P<.002
N=9Perry et al, in press.
Disease Progression: Rate of Cognitive Decline in DLB Correlated with BuChE Levels at Autopsy

Buerger et al, 2002.
10
0
–10
–20
An
nu
al
MM
SE
Dec
reas
e
CSF p-tau231 (pg/mL)
0 300 600 900 1,200 1,500 1,800 2,100RHO=-.30P<.01
Correlation between CSF [Phospho-tau] and MMSE Decrease in MCI

1,300
1,100
900
700
500
300
100
CS
F t
au L
evel
(pg
/mL
)
Control Tacrine Rivastigmine
Stefanova et al, 2003.
P=.005* P=.16
P=.04*
Baseline
Followup (12 months)
CSF Tau Levels in Treated and Untreated AD Patients

50% cases of moderate AD remain undiagnosed 70% cases of mild AD remain undiagnosed
Physician would have been consulted sooner if caregiver or others had known aboutprescription medication
Physician would have been consulted sooner if caregiver or others had known about early signs
Harris Interactive Inc., 2001.
Greater Awareness May Lead to Earlier Diagnosis and Treatment

Summary
Both AChE and BuChE can contribute to the loss of ACh, which underlies many of the symptoms in AD
Inhibition of CSF AChE and BuChE with rivastigmine correlates with clinical benefits
BuChE increases with severity of AD BuChE may play a role in plaque maturation and APP
processing Both AChE and BuChE are pharmacological targets Lack of upregulation with rivastigmine implies that cognitive
benefits are sustained during long-term treatment Increased AChE protein following galantamine and
donepezil is of uncertain clinical importance

Summary (cont’d)
AD is an expensive illness in human and economic terms for patient and care givers
Diagnosis is often not made, especially in early and mild AD Frequently treatment is not initiated or sustained Early treatment pays off; delaying treatment has long-term
consequences Functional imaging can aid in early diagnosis of dementia Moderately ill patients can robustly respond to tx Cholinesterase inhibitors attenuate symptomatic decline
and may modify disease progression