Embed Size (px)
Citation preview

1Journal ofNeurology, Neurosurgery, and Psychiatry 1993;56:1046-1054
NEUROLOGICAL EMERGENCY
The management of acute spinal cordcompression
Robin A Johnston
A wide variety of pathological lesions causespinal cord compression. The clinical presen-tation may indicate the nature of the lesionalthough with modem imaging techniques theimportance of making a clinical diagnosis ofpathology has diminished. The importantdiagnostic aspect of acute spinal cord com-pression is that it should be recognised asearly as possible and the patient referred withthe urgency that each particular case merits.The over-riding reason for this is to enhancethe chances of reversing the neurologicaldamage by appropriate decompressionsurgery. Prognosis for recovery dependsmainly on two factors: a) the severity of theneurological deficit and b) the duration of thedeficit before decompression. There will beother factors taken into consideration whenplanning surgical management including gen-eral fitness, life expectancy, tumour pathol-ogy, and the extent of any metastatic spread.Successful spinal cord decompression meansreturn of normal function in affected limbsand a stable, painless spine. Generally thismeans restoring independent walkingalthough both patient and surgeon may haveto settle for lesser degrees of functional recov-ery.
Spinal cord compression implies a "struc-tural" lesion of the vertebral column compro-mising the spinal canal and producing amyelopathy. The signs and symptoms ofspinal cord compression are those of motorand sensory deficit, but the common featureof "structural" lesions is pain. Spine pain ornerve root pain, occurring in the presence ofmyelopathic symptoms strongly implies asurgically remediable aetiology. The greatmajority of patients presenting with spinalcord compression reach hospital by referralthrough their general practitioner or throughan Accident and Emergency Department andare usually admitted to general medical orsurgical wards. In the early stages it may bedifficult to detect abnormal neurologicalsigns, especially if these are subtle and thepain component is large. For a variety of rea-sons, including late self-referral to any med-ical practitioner, delays can and do occur inthe referral of such a patient to a specialistspinal unit. This was the subject of a candidand disturbing report by Maurice-Williamsand Richardson in which they illustrate thediverse causes for delayed referral and theconsequences of this.' Any neurosurgeon ororthopaedic surgeon who carries out spinaldecompression, will have experience ofpatients who are referred having been para-plegic for several days, well beyond the time
of useful surgical treatment. Recognition ofsigns and symptoms of spinal cord compres-sion may be difficult without a neuroscienceenvironment and it is important that bothneurosurgeons and neurologists take the trou-ble to facilitate referral from physicians andgeneral surgeons at an early stage. Thisincludes an ongoing educational element ofwhich a most important aspect is to encour-age colleagues to recognise the early signs ofmyelopathy. Easier access to spinal imagingshould help.
TraumaThe most acute form of spinal cord compres-sion is caused by trauma of which 50%occurs in the cervical spine and the greatmajority of the remainder in the thoraco-lumbar junction and lumbar spine. Patientsare usually young males involved in road traf-fic accidents, falls and occasionally sportrelated activities.2 The forces involved can beresolved into flexion, extension, compressionand rotation, although usually more than oneis involved to produce the variety of differentfracture patterns and subluxations seen in thecervical spine. In about 10% of cases, twonon-contiguous levels of the cervical spine aredamaged, separated by several normalsegments.3The management of acute spinal cord
injury is the subject of many text books andpublications and may be intimidating to thoseunfamiliar with this clinical problem. In factthe major components of management ofspine trauma are analogous to the manage-ment of a fracture of a long bone. The man-agement steps involved are recognition,immobilisation, investigation, reduction, fixa-tion and rehabilitation. The cervical fractureshould be recognised for what it is and in thegreat majority of cases the combination ofneurological deficit, plus a painful and tendercervical region will indicate at least the possi-bility of cervical spine damage. Situations dooccur where a patient is unable to provide ahistory because of decreased consciousnessand in these it is better to make the assump-tion that cervical damage is present untilproved otherwise. The cervical spine can beimmobilised simply by holding the headfirmly between two hands and maintainingthe cervical spine in a neutral position untilbetter facilities are available. Depending onthe circumstances the patient may be fittedwith an appropriate sized Philadelphia stylecollar, or be placed in cervical traction. Thefrequently used soft, spongy cervical collars
Department ofNeurosurgery,Institute ofNeurological Sciences,Glasgow GS1 4TF,UK.R A Johnston
1046 on January 15, 2020 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.56.10.1046 on 1 O
ctober 1993. Dow
nloaded from

The management of acute spinal cord compression
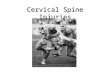
are particularly ineffective in restricting cervi-cal movements. One study indicates that thistype of collar prevents only 25% of flexionand extension movements. A Philadelphiastyle collar rises to the occiput, spreads overthe shoulders, rises over the chin and pro-vides more effective immobilisation. Cervicaltongs may be applied in the CasualtyDepartment within a matter of seconds if theGardner-Wells variety are used. Theserequire only a little local anaesthetic and areplaced 4cms above the external auditory mea-tus. They are simply hand-screwed throughthe anaesthetised scalp into the outer skullcortex to a pre-set tension. The doctor thenhas full control of the patient's cervical spine.Definitive investigations at an early stagemust include a lateral plain x-ray of all cervi-cal vertebrae. So many cases of missed frac-ture in the cervical spine are the result ofinadequate x-rays which omit the lower verte-brae. Flexion/extension views can be particu-larly revealing. If carried out carefully thepatient will come to no harm and the filmsmay show abnormal movement. Cervicalspine x-rays are difficult to read, especially forinexperienced junior staff and recourseshould be had to experienced staff beforemanagement decisions are made on thesepatients. More definitive investigation is car-ried out by CT scanning, which almostalways reveals more damage than was initiallyexpected from plain x-rays. If C7 is unavail-able through ordinary x-rays it is alwaysaccessible through CT scanning. MRI isbeginning to be made available to patientswith acute spinal injuries.4 It is particularlyhelpful in recognising damage to ligaments,discs and pre-vertebral tissues which haveclearly altered signals with this form of scan-ning, but which may not be recognised usingx-rays (fig 1).
Figure 1 MRI (1 -5Tesla Seimens Magnetom,T2 weighted scan) 24 hoursafter acute spinal trauma.The altered signalffrom theanterior longitudinalligament opposite C2 andC3 is clearly seen. Thiscervical spine has lost asubstantial degree ofstability.
At or about this stage in management,referral should be made to a specialised spinalunit, preferably an acute spinal cord injuryunit. The newly opened National SpinalCord Injuries Unit for Scotland now receivespatients with spine trauma with and withoutcord injury within hours of injury in somecases. The pathophysiological consequencesof acute spinal cord injury on the cardio-vascular and respiratory symptoms and theintensive nursing requirements make earlyreferral of these patients to an appropriateunit imperative. Spinal cord damage resultsin loss of sympathetic neural control causinghypotension and bradycardia. These are nor-mal for the patient who has cord transectionand should not be the subject of volume load-ing in misplaced attempts to restore "normal"blood pressure. Loss of intercostal innerva-tion due to cranial cord trauma produces ven-tilatory insufficiency which is best managed inspecialised units.5
Fractures, subluxations or dislocationsrequire reduction into normal alignment.This may be relatively easily brought aboutusing simple cervical traction. In the 1970sthere was a vogue for using high loads of cer-vical traction, but this carries the risk of dam-age by traction on the spinal cord itself.Depending on the type and displacement ofthe injury, the position of the cervical spinecan be altered using a rolled up sheet to exag-gerate the lordotic curve. The vector of trac-tion may be varied to enhance the likelihoodof reducing the spine back to normal align-ment. These techniques require frequent x-ray assessment and management experience.Should appropriate cervical traction beunsuccessful in reducing the fracture/disloca-tion the options are for manipulation underanaesthesia, which should only be carried outby experienced staff, or more commonly now,by open reduction and internal fixation.These latter decisions should be made bythose experienced in dealing with spinetrauma. Those patients who have vertebraldamage but no spinal cord injury are to someextent vulnerable to secondary injury throughinadvertent or accidental mishandling of thespine and in some ways have considerablymore to lose than those patients who alreadyhave major spinal cord damage.
Fixation of the cervical spine may becarried out using external orthotic supportssuch as the halo fixator which is particularlyuseful for high cervical fractures. Even in thisdevice a small degree of flexion and extensioncan still occur. Methods of internal fixationhave evolved and improved, especially inrecent years. In the cervical spine theseinvolve plate and screw, wire or laminarclamp devices and do provide the patient withthe ability to begin mobilisation and rehabili-tation at an earlier stage.6 For thoracic andlumbar fractures the use of pedicle screw fixa-tion reduces the number of vertebral levelspermanently immobilised and allows per-operative fracture reduction and restorationof alignment in some cases.7 Malalignment ofvertebrae is reduced using internal fixation,
1047 on January 15, 2020 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.56.10.1046 on 1 O
ctober 1993. Dow
nloaded from

18ohnston
but longterm stability only comes throughbony union. There is, and will continue to be,great debate amongst specialists in the man-agement of patients with spinal cord injuryconcerning the merits and demerits of surgi-cal intervention. What is clear is that inselected circumstances internal fixation andfusion does have a role to play and doesimpart advantages to the patient, his rehabili-tation and his spine. What surgical interven-tion does not do, however, is improveneurological outcome. While there have beenspurious and isolated reports of this there isno generally recognised association betweensurgical decompression and fixation, andneurological recovery in patients with acutespinal trauma.The use of high doses of methylpred-
nisolone has become standard practice inNorth America for patients with acute spinaltrauma. This follows the results of studieswhich showed statistical improvement in limbfunction where these steroids were adminis-tered.8 This statistical improvement, however,may not be reflected in any significant func-tional or clinical gain by the patient. Whilethe use of high dose methylprednisolone has,for reasons other than those which areentirely medical, gained widespread use inAmerica this practice has not become estab-lished in the United Kingdom.
In patients who incur a severe head injury,the primary traumatic event is followed by aseries of microvascular and biochemicalchanges which are recognised as the meansby which secondary damage can compoundthe original injury. The same is true of spinalcord injury and it is possible that similarmechanisms are involved. The effect of theexcitotoxic glutamate which is releasedfollowing trauma to central neural tissue canbe modified using N-methyl D-aspartate(NMDA) receptor blockade. Considerableattention currently focuses on biochemicalmethods of preventing or modifying thesecondary damage produced following brainand spinal cord injury.9
Inflammatory conditionsThe most common surgically relevantinflammatory spinal condition is rheumatoiddisease which affects approximately 1% of thepopulation in Western Europe. The cervicalspine is involved in a substantial percentageof those patients who have rheumatoid dis-ease with the incidence and severity increas-ing with the duration of the disease. Themost common site of involvement is at theoccipito-C 1/C2 level, although all levels ofthe cervical spine may be involved.'0The fibrous inflammatory tissue mass is
generally referred to as pannus although bystrict definition pannus refers to the exudateoverlying the synovial membrane. The fluctu-ating progress of the condition graduallydestroys the joint tissues and articular sur-faces which will lead to subluxation or evendislocation. This is frequently seen in thefingers and wrist joints of patients withrheumatoid disease, but does also occur at
the occipito-Cl/C2 level. The most commonform of dislocation is anterior subluxation ofC1 on C2 and this may be fixed or mobiledepending on the activity of the inflammatoryprocess."1-"3 Eventually the condition will"burn out" and the joints may become anky-losed in an abnormal position. Loss of heightof the lateral masses of Atlas will result in ver-tical translocation of the odontoid processand this occurs in about 10% of the affectedpopulation. Less frequently occurring abnor-malities include posterior subluxation of Clon C2 where the odontoid is totally erodedand the atlas can move posteriorly relative tothe body of C2. Asymmetrical involvement ofthe lateral mass joints may lead to rotationaldeformities or lateral subluxations.'4 Thedemonstration of these different types ofatlanto-axial abnormalities has been enor-mously enhanced through the use of CTmyelography including sagittal plane recon-struction, and with magnetic resonance scan-ning, both carried out with the patient flexingand extending her neck.5' 16With any subluxation in this region, or in
the subaxial region, the spinal canal will becompromised and the patient may develop amyelopathy. One of the burning issues of epi-demiological investigation into rheumatoiddisease addresses the question of whichpatients with cervical spine involvement willgo on to develop spinal cord compression.Unfortunately despite considerable effortthere is no firm method of predicting whichpatients will deteriorate neurologically andwhich patients, with perhaps relatively severeradiological involvement, will never developneurological signs or symptoms. Clinicalmarkers have proved to be of little value, butmore recent work involving measurement ofcord diameter may prove to be of more valuein predicting those patients who will requiresurgical intervention.'7
Acute spinal cord compression is not com-mon in rheumatoid disease although there areanecdotal cases of patients suddenly collaps-ing with paralysis and succumbing due togross odontoid subluxation. Usually neuro-logical symptoms develop over a period ofweeks or even months, but a few patients dodevelop neurological signs and deterioratewith progressive myelopathy over a shortperiod of days. They present with deterior-ation in gait quality and complain of sensoryalteration or sensory loss, including loss ofmanual dexterity in the upper limbs. A clearclinical history is of paramount importance inconfirming a myelopathy, since severe andwidespread synovial joint involvement fre-quently precludes accurate assessment ofdeep tendon reflexes and muscle power. Thepatient will often be able to distinguishbetween new symptoms such as loss ofstrength or paraesthesia or significant gaitdeterioration and identify these separatelyfrom the symptoms of multiple joint involve-ment with which she is already very familiar.Isolated tendon reflexes may be elicitedalthough plantar responses are almost neverobtainable because of local joint involvement
1048 on January 15, 2020 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.56.10.1046 on 1 O
ctober 1993. Dow
nloaded from

The management of acute spinal cord compression
or previous surgery. Vertical subluxation ofthe odontoid process makes it possible thatthe patient will develop lower cranial nervesigns. In the past, speech difficulty, dysphoniaand nystagmus have been attributed to highspinal cord or low medullary compression bypannus around the odontoid process. Whilethis may be so in some cases, rheumatoid dis-ease in the temporo-mandibular and cricoary-tenoid joints may provide a more pragmaticcause.'819 In one of the largest series ofrheumatoid patients that have been studied,Crockard found that nystagmus onlyoccurred in those patients with pre-existingChiari I malformation.'7When an acute cervical myelopathy is con-
firmed in a patient with rheumatoid diseasethe most likely cause will be anterior atlanto-axial subluxation. This can easily and rapidlybe confirmed by a plain lateral x-ray of thecervical spine taken in flexion and extension.This will confirm only bone movement andposition whereas soft tissue involvement willrequire the use of CT myelography or MRI.The purpose of management in this situationis to reduce the compression on the cervicalcord and in the majority of cases this will beachieved by extending the upper cervicalspine and bringing into more normal align-ment the Cl and C2 vertebrae. However, itcannot be assumed that because vertebralalignment has been restored that spinal cordcompression has been reduced. This willbecome apparent once scanning of the regionhas been carried out. Restoration of normalvertebral alignment is achieved using lightcervical traction, preferably with titanium orcarbon fibre tongs so there is no interferencewith subsequent scanning. The simplest andeasiest type of cervical tong to apply is theGardner-Wells version which requires only aninjection of local anaesthesia into the scalp4cms directly above the external auditorymeatus. As the patient will most frequently befemale and small, the weight required willrarely exceed 3 or 4 kilograms. Over the next24 to 48 hours the patient will experience anyneurological improvement that is likely tooccur if reduction of cord compression hasbeen achieved. It is at this time that the inter-est of a spine surgeon must be engaged andappropriate imaging of the region carried out.It is also important to recall that patients withmultiple joint involvement due to rheumatoiddisease do not tolerate prolonged cervicaltraction. If neurological improvement is notobvious within 72 hours it is probablyunlikely to occur and traction should be dis-continued. Once appropriate scanning hasbeen carried out the surgical decision con-cerning continued immobilisation or inter-ventional decompression, fixation and fusionwill be made.
There are a variety of surgical proceduresfrom which the surgeon may select thosemost appropriate to individual patients. Theodontoid region can be approached directlyby the transpharyngeal route in order todirectly decompress the cervico-medullaryregion. It is recommended that this should be
followed by a posterior stabilising operationwhich will generate fusion of C1 and C2 oroccipital bone to C2.2>22 Subaxial cranialcompression is less common than at C1-2and usually also requires a combination ofanterior and posterior surgery. At all levelsthe aim is to directly decompress the spinalcord, to restore vertebral alignment and toprevent further malalignment. For manypatients a posterior C 1-C2 fixation andfusion will be sufficient but in others the sur-gical procedure may be more complex.23-28The postoperative mortality and morbidity
rates are greatest in those patients who arenot severely neurologically affected, that is,quadriparetic and unable to walk. The sys-temic effects of rhematoid disease, especiallyinterstitial pulmonary involvement, mayadversely affect postsurgical recovery. Inthose patients in whom the myelopathy isrecognised and treated in the early stages theoutlook for recovery is good and postopera-tive mortality is low.
Infective lesionsInfections of the spine are uncommon; butcan usefully be classified as either vertebralosteomyelitis or intraspinal infection. Theformer is the more common variety of infec-tion and can lead to the latter whereas "pure"intraspinal infection comprises extradural,subdural or intramedullary abscess indescending order of frequency and withoutconcomitant infection of the vertebral col-umn.2930 Intraspinal infections occur at a fre-quency of approximately one per million peryear in UK neurosurgical units and in the UKare predominantly caused by pyogenic organ-isms, usually Staphylococcus, whereas in Asiaor Africa Mycobacterium tuberculosis is thecommon infecting organism."
Extradural spinal abscess may be foundanywhere within the spinal extradural spacebut this does not communicate with theintracranial extradural space because the twoare separated at the foramen magnum wherethe outer, endosteal layer of the intracranialdura adheres to bone. The spinal dura is asingle layer with the extradural space mostprominent posteriorly and it is here thatmost extradural abscesses are found, the greatmajority being in the thoracic or lumbarspine. Cervical extradural abscess is uncom-mon and is usually associated with vertebralosteomyelitis. The abscess may extend over afew or many vertebral levels and it is wellrecognised that non-contiguous abscessesmay occur.'233A spinal extradural abscess is a neuro-
surgical emergency and is one of the fewinstances where the history and clinical exam-ination may provide an instant pathologicaldiagnosis. The patient may, or may not, pre-sent with systemic signal illness, but as theabscess enlarges and compression of thespinal cord occurs then myelopathic symp-toms gradually develop, usually over thecourse of a small number of days.'F36 Theoutstanding clinical feature is spinal pain and
1049 on January 15, 2020 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.56.10.1046 on 1 O
ctober 1993. Dow
nloaded from

10ohnston
the marked local tenderness of the spine atthe level of abscess formation. Tapping thespinous processes lightly with a tendon ham-mer may elicit this and indicate the patho-logical diagnosis. Several studies havereported the high frequency of misdiagnosisof this condition in its early stages. The com-plaint of spinal pain, particularly in youngerpatients and of thoracic pain in all patientsshould be regarded seriously enough to makea definitive pathological diagnosis rather thanto assume the symptom is due to minor"mechanical dysfunction". By the timeneurological symptoms are present, even inthe absence of neurological signs, the proba-bility of some form of surgically remediablestructural spinal lesion increases consider-ably. Should the patient present with a para-plegia this should be regarded as a failure ofdiagnosis, as symptoms are frequently presentfor several days before this end stage.The most valuable diagnostic exercise is
high grade MRI scanning.37 This will confirmthe diagnosis of extradural abscess, indicateits upper and lower limits, demonstratewhether or not there is an associated, andtherefore probably primary osteomyelitis andin most cases differentiate between extraduralabscess and subdural abscess. Myelographywith CT scanning is the next best diagnosticinvestigation although the distinction betweenabscess, haematoma, or even in some casesmetastatic tumour is not possible.
Investigations should be carried out with-out delay and the management of choice is byimmediate surgical decompression. Since theabscesses are very commonly located in theposterior extradural space, albeit extendinglaterally on either side, this is one occasionwhere a decompressive laminectomy is theoperation of choice. Attention should be paidto the upper and lower limits of the abscessalthough the laminectomy may not require tobe taken to these extremes should the pus beof a liquid nature. On other occasions thelaminectomy may need to be taken to thelimits if the compressive material is semi-solidinfected granulation tissue.The results of surgery tell their own story
and indicate that when patients are severelyaffected or paraplegic the likelihood of neuro-logical recovery is poor. The mortality ratefor this condition has diminished over theyears with improving diagnosis, but is never-theless substantial for a spinal condition andis variously reported at between 17% and36%.31 38
Vertebral osteomyelitis is a relativelyuncommon condition, but familiar to spinesurgeons in the United Kingdom. The com-monest causes are staphylococci, strepto-cocci, E coli and occasionally unusualorganisms such as salmonella or brucella. Forthe most part the spinal cord is not affectedand the problem is one of structural integrityof the vertebral column.39 However, bothpyogenic and tuberculous osteomyelitis maylead to the formation of an extradural abscesslying anterior to the spinal cord, which maycause acute spinal cord compression in a
fashion not dissimilar to a "pure" extraduralabscess. The gradual progressive nature ofbone infection will produce a more protractedpreceding history, including spinal pain,aches, malaise, discomfort and system signsof infection culminating in an acute neurolog-ical deterioration.
Plain x-rays of the spine may give the diag-nosis by revealing erosion and loss of heightin contiguous vertebrae with destruction ofthe intervertebral disc. The coexistence of anextradural abscess is made by MRI or by CTmyelography and is done as a matter of someurgency. It requires only a few millilitres oflocalised liquefied pus in the anterior cervicalspinal canal to cause substantial tetraparesis,recovery from which is entirely possible withexpeditious decompression. Scanning alsoreveals the extent of vertebral and para-vertebral infection and can usually bedistinguished from metastatic disease.40
For pyogenic osteomyelitis which predomi-nates in the UK, direct ventral spinal canaldecompression is often required. In the cervi-cal spine this will involve an anterior cervicaldecompression procedure which can be car-ried out through an intervertebral disc spaceby a medial vertebrectomy. Division of theposterior longitudinal ligament usually resultsin the egress of a small volume of liquefiedpus which is sometimes less than impressiveconsidering the degree of paralysis which ithas produced. In these acute situations thesurgeon is best advised not to incorporatespinal reconstruction, but rather to return thepatient to a period of external spinal stabilisa-tion, usually by cervical traction, accompa-nied by appropriate intravenous antibiotictherapy. Once the infection has been treatedin such a way for a period of several days,then more definitive means of stabilising thespine can be employed. In these situationswhere the pyogenic infection is under control,bone grafting almost always results in a solidfusion and in selected cases it is becomingaccepted practice to use one or more of theforms of internal metal fixation while contin-uing antibiotic treatment.
In the thoracic and lumbar spine surgicaldecompression involves more difficult access,either by costo-transversectomy or posteriorthoracotomy in the thoracic region and by theextra-peritoneal route in the lumbar region.In tuberculous osteomyelitis a limitedpostero-lateral decompression by costo-transversectomy to release indolent purulentmaterial is a satisfactory means of decompres-sion with reconstruction and stabilisingsurgery reserved for later if necessary.4
Degenerative pathologyDegenerative change within the spine onlycauses acute spinal cord compression in asmall group, but usually has a more pro-longed course involving progressive neurolog-ical symptoms.42 Protrusion of intervertebraldisc into the spinal canal, whether this be inthe presence of existing osteophyte or not,can produce a rapidly developing myelopathy.
1050 on January 15, 2020 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.56.10.1046 on 1 O
ctober 1993. Dow
nloaded from

The management of acute spinal cord compression
Acute disc protrusions most commonly occurin the lumbar spine with 80% being locatedeither at L4/5 or L5/S1. Central compressionof the spinal theca at this level causes anacute cauda equina syndrome which is aspinal emergency. Isolated or "pure" cervicalintervertebral disc protrusion is much lesscommon than compression due to osteophyteformation although it is common to find acombination of both. "Pure" cervical discprolapse can occur at any age and it maybe that a pre-existing and relatively mildmyelopathy rapidly becomes much worsebecause of protrusion of cervical disc a fewmillimetres further into the spinal canal.Acute myelopathy will present in olderpatients who have degenerative changessuperimposed on a developmentally narrowcervical spinal canal (<10 mm AP diameter).In these patients the usual mechanism is vio-lent hyperextension of the neck.43 "Pure"thoracic disc protrusion is uncommon andthese patients present to neurosurgical unitsat a frequency of one per million per year.44 Itis more common to find that the so calledthoracic 'disc' is in fact a combination ofosteophyte and calcified disc material, ratherthan degenerate nucleus pulposus which hasprolapsed into the spinal canal.
In cases of acute disc protrusion, whicheverthe level, spinal pain usually accompanied byroot pain is a common clinical symptom. Thelevel of root pain provides a good indicationof which intervertebral disc is the culprit.When the disc protrudes sufficiently into thespinal canal to cause spinal (or cauda equina)compression then neurological symptoms andsigns accompany the pain. In the cervical andthoracic region these will lead to a myelopa-thy commensurate with the level of compres-sion. Clinical determination of the sensorylevel gives a good indication of the level ofthoracic disc prolapse. The distribution ofpain, numbness, or "dropped" reflexes in theupper limbs provides a good clinical indicatorto the level of cervical disc disease. When thepatient produces symptoms which illustrateloss of manual dexterity it is often the casethat compression is at the level of the C3/4intervertebral disc. In the lumbar spine, com-pression of the cauda equina produces lossof sensation across the sacral dermatomes,either unilaterally or bilaterally, associatedwith root pain in both legs and with loss ofbladder sphincter function. The clinical diag-nosis of an acute disc prolapse in the cervicaland lumbar spine is relatively straightforward,but misdiagnosis often occurs in the thoracicregion. There may be a background history ofthoracic spine pain and several studies haveconfirmed that probably because of the rarityof thoracic disc disease, other pathologicaldiagnoses are given prior consideration."The diagnosis is of disc prolapse confirmed
radiologically by MRI of the appropriatespinal region. The alternative is CT myelog-raphy but with modern CT scanners contrastis usually not required to confirm lumbar discprolapse although it is still required in thethoracic and cervical spine.45
The management of acute myelopathy oran acute cauda equina syndrome due to inter-vertebral disc prolapse involves urgent surgi-cal decompression. In the lumbar spine this iscarried out through a micro-discectomyapproach and in the majority of cases thisgives adequate access to the disc prolapse onboth sides. Occasionally the access has to beincreased by either a hemilaminectomy or onoccasions by a full laminectomy. For thosepatients with coexisting lumbar canal stenosisit is recommended by some that a lamin-ectomy is used to reduce the risk of a post-surgical cauda equina syndrome which occursat a frequency of 1 in 500 lumbar discoperations.46
In the cervical spine disc prolapse causingmyelopathy is removed through an anterioraccess route between the carotid sheath later-ally and the pharynx/larynx medially. This isan approach to the subaxial spine and whenthe compression is due to disc prolapse alonea simple disc excision is satisfactory. This iscarried out using an operating microscopewith excision of the disc material and the car-tilaginous end-plates down to the level of theposterior longitudinal ligament and laterallyto the medial part of the unco-verterbraljoints. It is necessary to open the posteriorlongitudinal ligament to directly visualise andexplore the extradural space as disc materialcan find its way through the longitudinallyorientated fibres of this ligament into theextradural space. It is not necessary to carryout a fusion procedure although this can becarried out either by the Smith-Robinson orCloward technique if preferred. The use of abone fusion does not confer additional neuro-logical recovery, although it may be required(or preferred) if spinal stability is significantlydegraded. Those patients in whom a fusionprocedure is not carried out may be moresusceptible to cervical pain for the first fewweeks following the decompression and theuse of a cervical collar is recommended.Laminectomy is not indicated for a patientwith myelopathy due to acute cervical discprolapse as this would involve unacceptablecord retraction to remove the disc.
For those patients who develop an acutemyelopathy due to hyperextension forcessuperimposed on a narrow spinal canal thereis little, if any, convincing evidence that surgi-cal decompression improves neurologicalrecovery. In those few patients who have anarrow cervical spinal canal and who developan acute non-traumatic myelopathy, alaminectomy or a multiple level anteriordecompression and fusion are the surgicalalternatives although the presumed ischaemicpathogenesis does not incline to thefavourable outcome associated with slowlydeveloping spondylitic myelopathy.4'
For a thoracic disc protrusion the surgicalaccess must be either lateral or anterior or acombination of both. The approaches to thethoracic spinal canal are those which giveaccess to the disc prolapse without requiringany retraction of the thoracic spinal cord andare such that the disc material may be
1051 on January 15, 2020 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.56.10.1046 on 1 O
ctober 1993. Dow
nloaded from

12ohnston
removed in a direction away from the spinaltheca. The recommended approaches arepediculectomy, costo-transversectomy ortransthoracic partial vertebrectomy.444748 Alaminectomy is only indicated for thoracicdisc prolapse if the disc material is entirelyfree and is located in a position lateral to thespinal cord. This does happen, but not com-monly. A laminectomy for an anteriorlyplaced thoracic disc prolapse invites majorneurological deterioration.
For patients who present with an acutedisc prolapse causing cauda equina syndromeprognosis for recovery is based on the severityof the pre-decompression neurological deficitrather than the duration of neurologicalsymptoms, although it is difficult to entirelyseparate these two components.49 The same islikely to apply to prognosis for recovery fol-lowing cervical and thoracic disc inducedmyelopathy. Full recovery for expeditiouslydiagnosed and optimally managed patients isto be expected.
Neoplastic cord compressionBy far the commonest type of neoplasticspinal cord compression is that caused by sec-ondary tumour deposits and up to one thirdof patients with malignant disease havedeposits in the spine.50 51 These are most com-monly found in the vertebral body and pedi-cles with direct spread into the spinal canal.In about 5% of cases, metastatic tumour isconfined to the spinal extradural space.52 Theusual and most common primary tumours arebronchus, breast, gastrointestinal tract,prostate, kidney, myeloma and lymphoma.Most secondary deposits are found in thethoracic spine and multiple lesions may benon-contiguous. The reasons for this arelikely to be related to the venous drainage ofaffected primary organs being routed throughthe spinal extradural venous plexus. The rela-tive size of the thoracic spine clearly also hasan effect. Secondary deposits are less com-mon in the lumbar and cervical spine. Theyare uncommon or even rare in the sacralspine.As the tumour enlarges and encroaches on
the spinal cord the signs and symptoms ofmyelopathy progressively develop. This isassociated with spinal pain in over 90% ofpatients and in retrospect these patients areoften found to have complained of pain in theaffected region for many weeks before thedevelopment of clinical myelopathy.53 In themajority of cases the myelopathy progressesgradually, usually over a period of days orweeks. As the compression increases the abil-ity of the spinal canal to accommodate theextra volume is exhausted and the rate ofneurological deterioration increases rapidly.The typical patient will have complained ofthoracic spinal pain for perhaps four or sixweeks with gradual development of fatigue inthe lower limbs followed by decreased gaitquality and finally with rapid development ofweakness and loss of sensation. The apparentacute presentation is therefore usually only
the final stage of a more gradual process.54Acute spinal cord compression due to sec-
ondary tumour does occur when the tumourenlarges very rapidly due to haemorrhage orwhere a vertebral body suddenly collapsesbecause its structure has been extensivelyinfiltrated by the neoplastic process.The clinical features of presentation are
not sufficiently characteristic to permit anaccurate pathological diagnosis. Other causesof acute cord compression may present in asimilar clinical fashion. The diagnosis mustbe confirmed by appropriate spinal imaging,initially by plain x-ray of the relevant spinalregion although the whole spine needs to bemanaged as up to 17% of patients have multi-ple lesions.5' The typical features of metasta-tic involvement include loss of vertebralheight, an irregular lucent appearance withinthe fine architecture of the bone, preservationof the intervertebral disc space and the possi-bility of multiple lesions. Spinal x-rays shouldbe taken in combination with chest x-rays andthe clinical examination, either or both ofwhich may reveal evidence of a primarylesion. The optimal form of spinal imaging isby MR scan, or by CT myelography.55 All therelevant information can be obtained fromMRI including the number of levels affected,the extent of any local extravertebral infiltra-tion and soft tissue involvement. CT scan-ning gives a clear indication of the extent ofbone involvement and makes surgical plan-ning of the route of access and the achievableextent of excision more easy.
It may be that the pathological nature ofthe secondary tumour is circumstantiallyidentified by locating the primary tumour.When no primary can be found it is impor-tant to identify the histopathological type ofthe tumour by biopsy. In the spine betweenT5 and L5 this can be achieved through per-cutaneous vertebral body biopsy carried outunder biplanar image intensifier control.56 Analternative method is to use CT guided nee-dle biopsy at almost any level, although thistechnique does not as readily provide samplesof bone tissue, but rather of infiltrated softtissue immediately adjacent to the vertebra.Either technique is safe in experienced handsand yields a high rate of positive diagnosis.The subsequent management usually takes
account of a number of factors, each with avarying influence on the management in dif-ferent circumstances.57 The histopathology ofthe tumour must be taken into account withthe overall tumour load, that is, the numberof secondary deposits and the best estimate ofthe patient's life expectancy. The severity ofthe neurological deficit probably has themajor influence on the neurological recoveryfollowing decompression surgery. The mostseverely affected patients and those who areparaplegic have the lowest chance of regain-ing the ability to walk independently. Lesserlevels of recovery, which do not permit thepatient to either transfer, stand or walk, are oflittle practical benefit although return of sen-sation is of great importance to someone whois confined to a wheelchair.
1052 on January 15, 2020 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.56.10.1046 on 1 O
ctober 1993. Dow
nloaded from

The management of acute spinal cord compression
The first surgical decision to be made iswhether or not a surgical procedure is indi-cated. Surgery will provide the most rapidmeans of cord decompression, in contrast toradiotherapy which may take several days tohave its optimum effect as a decompressingagent. Even patients with highly radiosensi-tive tumours such as myeloma or lymphomaoccasionally require urgent surgical manage-
ment where the compression is due to a col-lapsed vertebra rather than to tumour tissuesurrounding the spinal cord.The route of access should then be decided
and at all spinal levels the surgeon has a
choice of posterior, lateral or anterior routes.In general where the compression and major
disease lies anterior to the spinal cord thisshould be the preferred route to decompres-sion. This may be transoral, transcervical,transthoracic or retroperitoneal depending on
the level of the spine affected. Lateral access
can be achieved through a laminectomyextended laterally to include the pedicle andfacet joint, a true costo-transversectomy or a
lateral extra-cavity approach which is in effectan extended multiple level costotransversec-tomy. Where the spinal cord is primarilycompressed posteriorly then a laminectomystill has a role to play. However, the days ofsimply carrying out a laminectomy for any
form of neoplastic spinal cord compressionare long since past. Studies from the late 70sand early 80s clearly showed how ineffective a
laminectomy is in the presence of vertebralbody disease. In this situation 20% of patientsare made neurologically worse and a similarnumber are made unstable. The decompres-sion process may entail removal of consider-
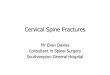
Figure 2 MRI (1 5Tesla Seimens Magnetom)showing a cervico-thoracicextradural haematoma ofspontaneous onset andunknown cause. Thehaematoma lies posterior tothe spinal cord.
able amounts of bone from the spine andrequire replacement using internal metallicfixation, bone graft, or in some cases methylmethacrylate in combination with metalfixation.
Surgical decision making in these situa-tions is complex and preparing contingencyplans for every clinical situation is not a prac-tical proposition. The over-riding aims are toprovide the most effective form of decom-pression of the spinal cord to leave the patientwith a pain-free, stable spine, with return offunction of the spinal cord. In some situa-tions, such as a patient with widespreadmetastatic bronchogenic tumour, it is entirelyinappropriate to carry out a transthoracicspinal decompression. In a patient who hasmultiple non-contiguous spinal lesions majorsurgery on any one of these is likely to befollowed by further cord compression at a dif-ferent level. In selected patients, however,even relatively major surgery to access anddecompress the spinal cord is indicatedbefore further treatment with radiotherapy orchemotherapy.
Spinal cord compression by haematomaExtradural and subdural haematomas arecommon and well known conditions in cra-nial neurosurgery, but are distinctly uncom-mon in the spine. Subdural haematomas inparticular are rare, with few cases beingreported.58 Epidural haematomas, whileuncommon, are a recognised cause of cordcompression and about one third are associ-ated with patients receiving anticoagulanttherapy. Lumbar puncture in this group ofpatients may lead to the formation of a spinalepidural haematoma. A substantial propor-tion occur for no particular reason althoughin the literature they are associated with, oreven causally related to, what might otherwisebe described as minor traumas of everydayliving.5960 It seems more likely that these arecoincidental factors rather than causal. Thereis little evidence that arteriovenous abnormal-ities in the vertebra or other form of angioma-tous malformation are causally related tomore than a small number of spinal epiduralhaematomas.61 62
Their clinical presentation is similar to sev-eral other forms of structural spinal cordcompression. Haematomas produce a combi-nation of spinal pain and root pain, followedby a progressive myelopathy, whose featureswill depend on the level of compression.Occasionally the process develops over sev-eral days and there are documented cases inwhom the myelopathy has developed overseveral weeks.6' The majority present rela-tively rapidly, within one or two days, and thediagnosis is confirmed by MRI or CT myel-ography.64 (fig 2). The appearances are thoseof an extradural compressive lesion althoughwith MR scanning it is possible to distinguishhaematoma from pus or extradural tumour insome cases. Treatment is by laminectomy atthe level of compression.65
1053 on January 15, 2020 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.56.10.1046 on 1 O
ctober 1993. Dow
nloaded from

14ohnston
1 Maurice-Williams RS, Richardson PL. Spinal cord com-pression: delay in the diagnosis and referral of a com-mon neurosurgical emergency. Br J Neurosurg 1988;2:55-60.
2 Meyer PR. Acute injury retrieval and splinting techniques.In: Meyer PR, ed. Surgery of spine trauma. New York:Churchill Livingstone, 1989:1-21.
3 Vaccaro AR, An HS, Lin S, et al. Noncontiguous injuriesof the spine. JSpinalDis 1992;5:320-9.
4 Schaefer DM, Flanders AE, Osterholm JL, Northrup B.Prognostic significance of magnetic resonance imagingin the acute phase of cervical spine injury. J Neurosurg1992;76:218-23.
5 Cane RD, Shapiro BA. Pulmonary effects of acute spinalcord injury: assessment and management. In: MeyerPR, ed. Surgery of spine trauma. New York: ChurchillLivingstone, 1989:173-83.
6 Aldrich EF, Weber PB, Crow WN. Halifax interlaminarclamp for posterior cervical fusion: a long term followup review.Jf Neurosurg 1993;78:702-8.
7 McNamara MJ, Stephens GC, Spengler DM.Transpedicular short segment fusions for treatment oflumbar burst fractures. JSpinalDis 1992;5:183-7.
8 Bracken MB, Shephard MJ, Collins WF, et al.Methylprednisolone or naloxone treatment after acutespinal cord injury: 1 year follow up data. Results of thesecond national acute spinal cord injury study. J7Neurosurg 1992;76:23-31.
9 Tator CH, Fehlings MG. Review of the secondary injurytheory of acute spinal cord trauma with emphasis on
vascular mechanisms.Jf Neurosurg 199 1;75: 15-26.10 JohnstonRA, KelvinIG. Surgery of the rheumatoid cervi-
cal spine. Ann Rheum Dis 1990;49:845-50.11 SantavirtaS, Kottinen YT, Laasonen E, Honkanen V,
Antti-Poika I, Kauppi M. Ten year results of operationfor rheumatoid cervical spine disorders. J Bone JIointSurg 1991;73-B:1 16-20.
12 Mathews JA. Atlanto-axial subluxation in rheumatoidarthritis. Ann Rheum Dis 1974;33:526-31.
13 Pellicci PM, Ranawat CS, Tsairis P, Bryan WJ. Aprospective study of the progression of rheumatoidarthritis of the cervical spine. J Bone Joint Surg 1981;63-A:342-50.
14 SantavirtaS, Kankaanpaa U, Sandelin J, Laasonen E,Kottinen Y, Slatis P. Evaluation of patients withrheumatoid cervical spine. Scand J Rheumatol 1987;16:9-16.
15 Bell GR, Steams KL. Flexion-extension MRI of the upper
rheumatoid cervical spine. Orthopaedics 1991;14:969-74.
16 Krodel A, Refior HJ, Westermann S.Theimportance offunctional magnetic resonance imaging in the planningof stabilizing operations on the cervical spine in rheuma-toid patients. Arch Orthop Trauma Surg 1989;109:30-3.
17 DvorakJ, Grob D, Baumgartner H. Gschwent N, GraverW, Larsson S. Functional evaluation of the spinal cordby magnetic resonance imaging in patiehts withrheumatoid arthritis and instability of the upper cervicalspine. Spine 1989;14:1057-64.
18 Rogers MA, Crockard HA. Nystagm us and joint positionsensation; theirimportance in posterior occipito-cervicalfusion in rheumatoid arthritis. Presented in part, 19thAnnual Meeting, Cervical Spine Research Society,December 1991, Philadelphia PA.
19 Toolaner G. Cutaneous, sensoryimpairment in rheuma-toid atlanto-axial subluxation assessed quantitatively byelectrical stimulation. Scand J Rheumatol 1987;16:27-32.
20 Dickman CA, Locantro J, Fessler RG. The influence oftransoral odontoid resection on stability of the cran-
iovertebral junction. J Neurosurg 1992;77:525-30.21 Crockard HA, Calder I, Ransford AO. One stage transoral
decompression and posterior fixation in rheumatoidatianto-axial subluxation. J BoneJoint Surg 1990;72-B:682-5.
22 HadleyMN, Spetzler RF, Sonntag, VKH. The transoralapproach to the superior cervical spine. J7 Neurosurg1989;71: 16-23.
23 Wertheim SB, Bohiman HH. Occipitocervical fusion. JBone joint Surg 1987;69-A:833-6.
24 Ranawat CS, O'Leary P, Pellicci P, Tsairis P, MarchiselloP, Dorr L. Cervical spine fusion in rheumatoid arthritis.JBone Joint Surg 1979;61-A: 1003-00.
25 Chan CP, Ngian KS, Cohen L. Posterior upper cervicalfusion in rheumatoid arthritis. Spine 1992;17:268-72.
26 Ferlic DC, Clayton, MI, Leidholt JD, Gamble WE.Surgical treatment of the symptomatic unstable cervicalspine in rheumatoid arthritis. J Bone Joint Surg 1975;57-A:349-54.
27 Brattstr6m H, Granhoim L. Atlanto-axial fusion inrheumatoid arthritis. Acta Orthop Scand 1976;47:619-28.
28 Grob D, Dvorak J, Gschwend N, Froehlich M. Posterioroccipito-cervical fusion in rheumatoid arthitis. ArchOrthop Trauma Surg 1990;110:38-44.
29 Dutton JEM, Alexander GL. Intramedullary spinalabscess. J Neurol Neurosurg Psychiatty 1954;17:303-7.
30 Fraser RAR, Ratzan K, Wolpert SM, et al. Spinal sub-dural empyema. Arch Neurol 1973;28:235-8.
31 Johnston RA. Intraspinal infection. In: Findlay G, Owen
R, eds. Surgery of the spine. London: Blackwell, 1992:621-8.
32 Dandy WE. Abscesses and inflammatory tumors in thespinal epidural space (so called pachymeningitisexterna). Arch Surg Chicago 1926;13:477-94.
33 Heusner AP. Non tuberculous spinal epidural infections.NEnglJMed 1948;239:845-54.
34 Statham P, Gentleman D. Importance of early diagnosisof acute spinal extradural abscess. Jf R Soc Med 1989;82:584-7.
35 Baker AS, Ojemann RG, Swartz MN, et al. Spinalepidural abscess. N EnglJ Med 1975;293:463-8.
36 Hakin RN, Burt AA, Cook JB. Acute epidural abscess.Paraplegia 1979;17:330-6.
37 Ross J. Inflammatory disease. In: Modic M, Masaryk T,Ross J, eds. Magnetic resonance imaging of the spine.Chicago: Year Book Medical, 1989:167-82.
38 Holme A, Dott NM. Spinal epidural abscess. BMJ1954;64:64-8.
39 Ho EKW, Leong JCY. Spinal osteomyelitis. In: FindlayG, Owen R, eds. Surgery of the spine. London: BlackwellScientific, 1992:621-8.
40 Modic MT, Feiglin DH, Piraino DW, et al. Vertebralosteomyelitis; assessment using MR. Radiology 1985;157:157-63.
41 Johnston RA, Hadley DM. Tuberculous infection of thethoracic spine. In: Tarlov EC, ed. Neurosurgical treat-ment of disorders of the thoracic spine. Illinois: AmericanAssociation of Neurological Surgeons, 1991:95-109.
42 Ferguson RJL, Kaplan LR. Cervical spondylitic myelopa-thy. Neurol Clin 1985;3:373-82.
43 Epstein N, Epstein J. Benjamin V, et al. Traumaticmyelopathy in patients with cervical spinal stenosiswithout fracture or dislocation. Spine 1980;5:489-96.
44 Russell T.Thoracic intervertebral disc protrusion: experi-ence of 67 cases and review of the literature. Br J7Neurosurg 1989;3:153-60.
45 Wesolowski DP, Wang AM. Radiologic evaluation. In:Rothman RH, Simeone FA, eds. The Spine.Philadelphia: WB Saunders, 1992:570-6.
46 McLaren AC, Bailey SI. Cauda equina syndrome: a com-plication of lumbar discectomy. Clin Orthop 1986;204:143-9.
47 Fidler MW, Goedhart ZD. Excision of prolapse of tho-racic intervertebral disc. J Bone Jt Surg 1984;66B:518-22.
48 Russell T. Thoracic intervertebral disc protrusion. In:Findlay G, Owen R, eds. Surgery of the spine. London:Blackwell Scientific, 1992:813-20.
49 O'Laoire SA, Crockard HA, Thomas DG. Prognosis forsphincter recovery after operation for cauda equinacompression owing to lumbar disc prolapse. BMJ 1981;282:1852-4.
50 Schaberg J, Gainor B. A profile of metastatic carcinoma ofthe spine. Spine 1985;10:19-20.
51 Wong D, Fornasier V, MacNab I. Spinal metastases: Theobvious, the occult and the imposters. Spine 1990;15:1-4.
52 Constans J, de Divitus E, Donzelli R, et al. Spinal metas-tases with neurological manifestations: review of 600cases. JNeurosurg 1983;59:111-18.
53 Gilbert R, Kim J, Posner J. Epidural spinal cord compres-sion from metastatic tumor: diagnosis and treatment.Ann Neurol 1978;3:40-51.
54 Shapiro W, Posner J. Medical versus surgical treatment ofmetastatic spinal cord tumour. In:Thompson R, GreenJ, eds. Controversies in Neurology. New York: RavenPress, 1983:57-65.
55 Godersky J, Smoker W, Knutzon R. Use of magneticresonanceimagingin the evaluation of metastatic spinaldisease. Neurosurgery 1987;21:676-80.
56 Findlay G, Sandeman D, Buxton P.The role of needlebiopsy in the management of malignant spinal compres-sion. BrJNeurosurg 1988;2:479-84.
57 Findiay GFG. Metastatic spinal disease. In: Findlay G,Owen R, eds. Surgery of the spine. London: BlackwellScientific, 1992:557-72.
58 Reinsel TE, Goldberg E, Granato DB, etal. Spinal sub-dural haematoma: A rare cause of recurrent postopera-tive radiculopathy. J Spinal Dis 1993;6:62-7.
59 Cowie RA. Acute spinal haematoma. In: Findiay G, OwenR, eds. Surgery of the spine. London: Blackwell Scientific,1992:621-8.
60 Bruyn GW, Bosma NJ. Spinal extradural haematoma. In:Vinken PJ, Bruyn GW, eds. Handbook of clinicalneurology. Amsterdam: Elsevier, 1976;1-30.
61 Harris DJ, Fornasier VL, Livingstone KE. Hae-mangiopericytoma of the spinal canal. Report of threecases. JNeurosurg 1978;49:914-20.
62 Stuart Lee K, McWhorter JM, Angelo IV. Spinal epiduralhaematoma associated with Pagets disease. Surg Neurol1988;30: 131-4.
63 Boyd HR, Pear BL. Chronic spontaneous spinal epiduralhaematoma: report of two cases. J Neurosurg 1972;36:239-42.
64 Larsson EM, Holtas 5, Cronqvist S. Emergency magneticresonance examination of patients with spinal cordsymptoms. Acta Radiol 1988;29:69-75.
65 Johnston RA, Bailey IC. Spinal extradural haematoma;report of two cases. Ulster Medical Joumnal 1983;52:157-61.
1054 on January 15, 2020 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.56.10.1046 on 1 O
ctober 1993. Dow
nloaded from