Embed Size (px)
Citation preview

FALL 2018
FLCANCER.COM
Back On Track: FCS Helps Former Patient Overcome Latest Hurdle
340B Drug Program Needs Reform
Dedicated Team Brings Cancer Care To Palatka
T H E M A G A Z I N EFCS

For more information, visit FASLODEXHCP.com
MAKE EVERY STEP COUNT
FASLODEX is a registered trademark of the AstraZeneca group of companies. ©2018 AstraZeneca. All rights reserved. US-23240 8/18
You are encouraged to report negative side effects of prescription drugs to the FDA. Visit www.FDA.gov/medwatch or call 1-800-FDA-1088.
US-23240 Faslodex FCS The Magazine.indd 1 8/23/18 9:15 AM

Fall 2018 3
Fall 2018Contents
In This Issue
DEPARTMENTS 6 FCS News36 Patient Letters
SPOTLIGHTS32 Doctor Spotlight: Dr. David Wenk 34 Office Spotlight: Palatka Office38 Senior Management Team Spotlight: Jeff Esham
FEATURES22 Plan B for 340B24 Cool Running 26 Pearls of Wisdom for Leadership and Succcess
FCS Physician Dr. David Wenk, son Kolbe, wife Chrissy, and daughters Abby and Lily.
For more information, visit FASLODEXHCP.com
MAKE EVERY STEP COUNT
FASLODEX is a registered trademark of the AstraZeneca group of companies. ©2018 AstraZeneca. All rights reserved. US-23240 8/18
You are encouraged to report negative side effects of prescription drugs to the FDA. Visit www.FDA.gov/medwatch or call 1-800-FDA-1088.
US-23240 Faslodex FCS The Magazine.indd 1 8/23/18 9:15 AM
For all photos, article suggestions, and information to be included, content must be provided to [email protected] by the following due dates:
Spring Issue - Nov 1 for articles; Dec 15 for photosSummer Issue - Feb 1 for articles; Mar 15 for photos
Fall Issue - May 1 for articles; Jun 15 for photosWinter Issue - Aug 1 for articles; Dec 15 for photos
**Please include full names for all photos, in order from left to right. Photos must be high resolution or they will not be included.

4 FCS The Magazine
DR. LUCIO GORDON: FCS was founded in 1984, and we continue to believe we must do the best for our patients. It truly takes a team effort to provide the finest care available. As a physician, I rely on my team of both clinicians and non-medical personnel to ensure that every patient, and every family member, has the best possible experience when they come to FCS at the worst possible time in their lives.
Both our medical treatment and our personal treatment makes a difference in patients’ lives. We can administer the latest, greatest therapies, but without the human touch… without the “caring,” our patients may not feel they are receiving our best. It is truly gratifying when patients tell me how much they appreciate the entire FCS staff; in fact, they often tell me they feel like family…and that’s because of the very special teams of people we have at FCS.
BRAD PRECHTL: Florida Cancer Specialists provides a great example of teamwork for other community oncology practices nationwide. At this year’s Community Oncology Alliance (COA) Conference, for example, conference co-chair Dr. Lucio Gordan, of FCS Gainesville Cancer Center, stated, “At FCS, we approach patient care as a team, keeping in mind that nobody knows it all. Our administrators have
a different set of skills, and encounter different challenges in their day-to-day jobs than our physicians, or our nurses, or our pharmacists. But we need every member of our team at their best to provide the best care.”FCS often sets a benchmark for oncology best practices and that extends beyond clinical practice to the incredible job our administrative employees do. It’s very gratifying to be a part of our great team! Thanks to each and every one of you who continues to make a difference for our patients and their families.
COMMUNITY ONCOLOGYTAKES A TEAM EFFORTBY DR. LUCIO GORDON, PRESIDENT & MANAGING PHYSICIAN AND CEO BRAD PRECHTL, MBA
Editor'sLetter
PRESIDENT EMERITUS & FOUNDER DR. WILLIAM N. HARWIN
PHYSICIAN LEADERSHIPPRESIDENT & MANAGING PHYSICIAN
LUCIO GORDAN, M.D.
ASSISTANT MANAGING PARTNER, DIRECTOR, EXECUTIVE BOARD
STEPHEN V. ORMAN, M.D.
DIRECTOR OF PATIENT ADVOCACY, DIRECTOR, EXECUTIVE BOARD
MICHAEL DIAZ, M.D.
SCIENTIFIC DIRECTOR OF CLINICAL RESEARCH, DIRECTOR, DRUG DEVELOPMENT PROGRAM
LOWELL L. HART, M.D.
DIRECTOR OF RESEARCH OPERATIONS JAMES A. REEVES, JR., M.D.
EXECUTIVE MANAGEMENTCHIEF EXECUTIVE OFFICER
BRAD PRECHTL
CHIEF OPERATING OFFICERTODD SCHONHERZ
GENERAL COUNSELTOM CLARK
CHIEF MARKETING & SALES OFFICER SHELLY GLENN
CHIEF REVENUE CYCLE OFFICER SARAH CEVALLOS
SENIOR MANAGEMENTMARK MOCH RICH DYSON JEFF ESHAM
MICHAEL ESSIK INGA GONZALEZ JOYCE NELSON JEFFREY RUBIN
TARA RUSKA DAN FARRAR
FRANK NUNZIATO RAY BAILEY
CHRISTY BANACH LOIS BROWN
DON CHAMPLAIN MELISSA CHANDLER
MELODY CHANG DIANE G. COPE DAVID CURRY
ANDREW FISHER CLAUDIA FRENCH KATIE GOODMAN
SUE KEARNEY LEVESTER JONES
ROSE ANN MEYERS NICOLE PICAZIO ANNE RONCO LYNN SAWYER
SIERRA TOMLINSON SAMANTHA WATKINS
DENICE VEATCH KATHERINE HOGAN
JILL HAMMERICH ANNIE PIGUE JODI LOHNES LAURA SPERRY
PUBLISHED BYIN PARTNERSHIP WITH
TH
E M
AG
AZ
INEFCS

Fall 2018 5
This is more than just lip-service.
As the pioneers of performance-based contracting, we have
always been focused on the future of community oncology. That
long-standing commitment remains as the healthcare landscape
evolves due to changing regulations and industry standards.
Your success is our success.
Our purpose is to ensure your viability as an independent
practice and to help you grow. That can’t be fulfilled if we are
not providing the results and resources that you need-
and that forges lasting partnerships.
Care for you, so that you can care for patients.
As patient needs evolve, so do the tools and resources you
depend upon to meet those needs. We do our part by
investing in technology, research and other resources to
help you elevate the quality of patient care.
The True Purpose of your GPO
True partners in service.
True leaders in industry.
True innovators in care.
www.iononline.com

6 FCS The Magazine
FCSNews
✚ Senior Management | PromotionA Florida native, Rose Ann Meyers worked at the Fort Myers-based financial services organization for GE
for 18 years as a leader in Payroll and Accounts Payable. Rose Ann was tasked with leading customer service teams, managing acquisitions and transitions for the respective departments, and focusing on process improvement for productivity and savings. In April 2009, she joined FCS as a Procurement Auditor and was assigned to audit drug inventory at all locations. In November 2010, she was promoted to Procurement Manager and became a member of the Clinical Directions Team. As the Director of Procurement, she continues to manage the daily operations of Procurement, management of various medical supply vendors and contract negotiations. Rose Ann is Six Sigma GreenBelt and BlackBelt certified. Outside of work, Rose Ann loves to spend time with family, travel and scrapbook her memories!
✚ Promotion | Senior Director of Construction & Facilities ManagementFrank Nunziato joined FCS in 2016 as Construction
Development Manager and has now been promoted to Senior Director of Construction & Facilities Management. Frank attended Empire State College in Saratoga Springs, New York, and graduated with a degree in Science. Frank started his career in 1988 as an “A” Journeyman Electrician in New York City and has over 30 years of experience in Construction/Facilities Management. He is also an I.F.M.A. Certified Facility Manager. In 2000, he relocated to Naples, Florida, to accept a position as the Director of Facilities for a software company and was promoted to the Senior Director of Global Facilities in 2004. In 2008, he joined a private school in Naples as a Facility Manager that was responsible for Operations across the campus. In 2013, Frank accepted a position at EMCOR as a Senior Facility Manager and was responsible for 180 banking centers in Florida. In his spare time, Frank enjoys traveling, fishing, watching football and spending time with his wife of 25 years, Liz, and their three children.
New Physicians/Promotions/Retirements
✚ New Physician & Location | Dr. J. Wynn Sullivan Medical Oncologist Dr. J. Wynn Sullivan joined FCS in February
2018 and added a new location in Palatka, Florida, to the FCS network. Dr. Sullivan received his undergraduate degree in Microbiology at the University of Florida and received his Doctorate of Osteopathic Medicine at Nova Southeastern University. Dr. Sullivan finished his Residency and Fellowship in Jacksonville, Florida, at the University of Florida Health Science Center, training in Medical Oncology and Hematology. Dr. Sullivan is actively involved in the American Cancer Society, having served two terms as its president, and he has over 30 years of clinical experience, including industry and network trials. In his spare time, he enjoys spending quality time with his wife and four daughters.
✚ New Hospitalist Will Serve Lake and Sumter CountiesWe are proud to welcome our newest Hospitalist, Dr. Adewale
Fawole, to Lake and Sumter counties. With eight locations in these two Central Florida counties, Dr. Fawole will be a great addition to our Florida Cancer Specialists team.
✚ Promotion | Senior ManagementJodi Lohnes is the Associate Regional Director of Operations
for all FCS locations in Sarasota, Manatee, Polk and Highlands counties, and also supports FCS physicians Dr. Ross, and Dr. Avashia. Jodi has been with FCS for nearly four years and has over 20 years of healthcare experience. Jodi has provided managerial support to multiple offices and has been instrumental during transitions and training new incoming managers. She received a certification in Healthcare Green Belt Six Sigma from Villanova University in 2010. Jodi is an active member of the Professional Association of Health Care Office Management (PAHCOM). Jodi moved to Florida with her husband and son in 2003. She enjoys spending time with family and friends, reading and watching football (Go Pats!)
J. Wynn Sullivan, MD
Adewale Fawole, MD
Jodi Lohnes
Rose Ann Meyers
Frank Nunziato

Fall 2018 7
FCSNews
✚ Promotion | Regional Director of OperationsAs Regional Director for offices located in Charlotte, Lee, and
Collier counties, Anne Ronco oversees the daily operations of the clinical locations in these regions. Anne joined FCS as an Office Manager of the Summerlin office in 2015 and was promoted to Associate Regional Director in 2017. She began her career in the medical field as a Practice Administrator for a large hospitalist group, where she provided high-level support, as well as clinical and operational oversight, for the group in the Lee County area. Anne earned her Bachelor’s degree in Business Administration in 2015 and then completed her Masters in Healthcare during the summer of 2017. Anne enjoys spending time with her family, including following her two sons’ traveling baseball team, and boating.
✚ Retirement | Dr. Lee M. Zehngebot The staff and physicians of FCS would like to thank Dr. Lee M.
Zehngebot for his leadership and unwavering dedication to our patients.
FCS wishes Dr. Lee M. Zehngebot health and happiness in the next chapter of his life!
✚ Retirement | Dr. Eric T. Lubiner The physicians and staff of Florida Cancer Specialists thank Dr.
Eric T. Lubiner for his 18 years of serving patients! FCS recognizes Dr. Lubiner for his commitment to the communities of North Port and Port Charlotte and congratulating him on his retirement.
✚ New Radiologist | Dr. Keith A. FergusonWe are proud to welcome our newest Radiologist, Dr. Keith A.
Ferguson. With over 200 physicians across the state of Florida, Dr. Ferguson will be a great addition to our Florida Cancer Specialists team.
✚ New Physician | Gainesville Cancer CenterPlease join us in welcoming our newest Medical Oncologist, Dr.
Amy Nance, to the Gainesville Cancer Center. Dr. Nance is board-certified in internal medicine, medical oncology/hematology and has special interests in cancers of the breast, lung and colon. Dr. Nance earned her medical degree from the Mercer University School of Medicine (Macon, Georgia) and attended Emory University School of Medicine (Atlanta, Georgia) for her Internal Medicine Residency. After completion she relocated to Chapel Hill, North Carolina to complete her Fellowship in Hematology/Oncology at the University of North Carolina. In addition to her academic achievements, Dr. Nance received two research training grants for Hematology and Oncology from the University of North Carolina. As a cancer researcher, Dr. Amy Nance is actively engaged in clinical research and has been published in several peer-reviewed journals. Dr. Nance enjoys spending time with her family, running and traveling.
✚ New Physician | Sarasota DowntownPlease join us in welcoming our newest Medical Oncologist,
Dr. Elizabeth Guancial, to the Sarasota Downtown location. Dr. Elizabeth Guancial is board-certified in internal medicine, medical oncology/hematology and has special interests in cancers of the bladder, kidney, testicle and prostate. Dr. Guancial earned her medical degree from the Harvard School of Medicine (Boston, Massachusetts) and completed her Internal Medicine Residency at the Massachusetts General Hospital. After her residency, Dr. Guancial was awarded a Fellowship in Hematology/Oncology at the world-renown Dana Farber Cancer Institute in Boston.
In addition to her academic achievements, Dr. Guancial received research grants from the Bladder Cancer Advocacy Network, University of Rochester Medical Center and the New York State Empire Clinical Research Investigator Program. As a cancer researcher, Dr. Elizabeth Guancial is actively engaged in clinical studies, has been published in several peer-reviewed journals and previously served as a peer reviewer for the European Oncology & Hematology Journal and the British Journal of Urology.
Eric T. Lubiner, MD
Lee M. Zehngebot, MD
Anne Ronco Amy Nance, MD
Keith A Ferguson, MD
Elizabeth Guancial, MD

8 FCS The Magazine
FCSNews
✚ New Physician | Naples Napa RidgeMedical Oncologist Dr. Simon Abi Aad joined FCS on Aug. 6 in
Naples. Dr. Simon Abi Aad is board-certified in internal medicine, medical oncology/hematology and has special interest in public policy and cancer care delivery to patients. Dr. Abi Aad earned his medical degree from the Université Saint Esprit de Kaslik Faculté de Médecine (Jounieh, Lebanon), did a research internship at the MD Anderson Cancer Center and completed his Internal Medicine Residency at the Icahn School of Medicine at Mount Sinai – St. Luke’s Roosevelt Hospital Center (New York, N.Y.) with extensive rotations at the Memorial Sloan Kettering Cancer Center. After his residency, Dr. Abi Aad was awarded a Fellowship in Hematology/Oncology at the University of Miami – Sylvester Comprehensive Cancer Center (Miami, Florida).
✚ New Physician | Fort MyersMedical Oncologist Dr. Magali Van den Bergh will join our Fort
Myers locations — Cape Coral Cay West, Cape Coral Cancer Center and Fort Myers Cancer Center. Dr. Van den Bergh graduated magna cum laude from Northwestern State University with a dual degree in Biology and Chemistry, while competing in Division 1 college tennis. After earning her medical degree (M.D.) with honors among the top five in her class at the American University of the Caribbean, she completed her internship and residency in internal medicine at the University of Connecticut. She was awarded a fellowship in hematology and medical oncology at H. Lee Moffitt Cancer Center and Research Institute/University of South Florida, where she was appointed as Chief Fellow.
FCS Events
✚ Advancing Quality in Oncology Care | AJMCThank you to all who attended the Institute
of Value-Based Medicine Program on April 5, with speakers FCS Physician Dr. Lucio Gordan and FCS Director of Care Management, Don Champlain.
Pictured left to right | FCS Physician Dr. Lucio Gordan and FCS Associate Director of Care Management Don Champlain.
✚ FCS Dedicates New SponsorshipOn March 4, at the International Polo Club Palm Beach, Florida Cancer Specialists dedicated its VIP Sponsorship
for the Leukemia & Lymphoma Society’s 2018 Man/Woman of Year (Palm Beach) in honor of The Leukemia & Lymphoma Society Palm Beach Area Brand Ambassador, Brandon Phillips.
Photo taken at the FCS Foundation’s second annual Polo Brunch. Pictured left to right | The Leukemia & Lymphoma Society-Suncoast Chapter Chair & FCS CMSO Shelly H. Glenn with International all-star polo player, cancer survivor and philanthropist Brandon Phillips.
✚ Conference | Digital Healthcare Transformation AssemblyFCS Chief Marketing and Sales Officer Shelly Glenn
participated in a panel discussion during the 2018 Digital Healthcare Transformation Conference: Using Digital Technology to Turn Employees into Brand Ambassadors.
Pictured in photo | Moderator | Brian Ahier, Aetna, Digital Health Evangelist. Panel participants | Florida Cancer Specialists’ Chief Marketing & Sales Officer Shelly H. Glenn, Centura SVP & Chief Marketing Officer Janell Moerer, HCA Assistant VP Marketing Deven Nongbri and Cancer Treatment Centers of America Chief Growth Officer Peter Yesawich.
Simon Abi Aad, MD
Magali Van den Bergh, MD

Fall 2018 9
FCSNews
✚ FCS’ Dr. Lucio Gordan Co-Chairs COA ConferenceOn April 12th, FCS Physician Dr. Lucio Gordan served as one of the Conference Co-Chairs at this year’s
Community Oncology Alliance (COA) Conference.
Pictured left to right | VP Texas Oncology Debra Patt, MD, MPH, MBA, CEO Dayton Physicians Network Robert Baird, Jr., RN, MSA, CASC, Lake Norman Oncology Dr. David Eagle, FCS Physician Dr. Lucio Gordan and CEO for The Center for Cancer & Blood Disorders Barry Russo.
FCS COO Todd Schonherz Presents at the 2018 Community Oncology Alliance (COA) Conference
✚ FCS CEO Brad Prechtl Presents at ACCC On March 15, FCS CEO Brad Prechtl, MBA, spoke at the
Association of Community Cancer Centers (ACCC) 44th Annual Meeting & Cancer Center Business Summit in Washington, D.C. His topic was “Physician Practice Models that Succeed in a Value-Based World.”
✚ FCS Hosts Patient Advocacy Educational EventOn March 21, FCS hosted a Patient Advocacy Educational Event at the FCS Cattleman location in
Sarasota, Florida. Patients were invited to learn about updates from the FCS CPAN Chapter and CPAN National Advocacy efforts. Guest speakers included: Associate Director of Care Management Don Champlain, RN, MHA, FCS Physician and Director of Patient Advocacy Dr. Michael Diaz, Care Management Manager, Beth Wittmer, RN, OCN, and COA Director of Patient Advocacy & Education Rose Gerber.
Front Row - left to right | FCS Physician Dr. Michael Diaz; Physician Liasion Mary Ellen Woska; Care Management Manager Beth Wittmer; and FCS Foundation Lead Volunteer Terri Prechtl.Back Row - left to right | Patient Point Dan Branch, Care Manager Karen Yoder, RN; Care Manager Stacey Jacovina, LPN; Director of Care Management; Don Champlain RN MHA; FCS Patient Wes; Janus Representative Chiquita Bonds; Director of Patient Advocacy and Education with COA Rose Gerber.
✚ Sarah Cannon Research Institute Annual Leadership Retreat in Nashville
Pictured left to right | Susan Modugno Sr., Clinical Quality Specialist; Jenifer Bar-Nur, Research Manager, East; Lynn Bentz, Sr. Research Coordinator, South; Margie Simonetta, Sr. Research Coordinator, North; Katie Goodman, Director of Clinical Research; Dinah Barnes, Study Manager, North; Patty Wright, Sr Research Coordinator, Panhandle; Patrice Rosser, Study Manager, South.
Brad Prechtl, MBA

10 FCS The Magazine
FCSNews
✚ Pharmacy Operations and Regional Pharmacy Trainers at the 2018 Annual Pharmacy Trainers Conference
Pictured left to right | Melody Chang Director of Pharmacy Operations, Terri Ertley Regional Pharmacy Trainer, Michelle Middleton Regional Pharmacy Trainer, Stephanie Sabillon Pharmacy Operations Manager, Tamer Morghem Regional Pharmacy Trainer, Dawn Furdock Regional Pharmacy Trainer, Lori Whatton Regional Pharmacy Trainer, April Wilson Regional Pharmacy Trainer, Jana Kutzko Regional Pharmacy Trainer, April Arredondo Regional Pharmacy Trainer, Camilo Rodriguez, Associate Director of Pharmacy Operations, Tracy Wuerth Regional Pharmacy Trainer
✚ Fort Myers Cancer Center Hosts Team Building Paint Party to Raise Funds for the FCS Foundation
Pictured left to right | Back Row: Russell Shaw MLT GLO , Kria Welliver PSS GLO, Marcie Jacobs Lead Nurse GLO, Nicole Kruse PSS GLO, and Deaudria Allen Assistant Office Manger GLO.Front Row: Roberto Guajardo Cytogenetics technologist – Pathology lab, Jeri Alexander FISH technologist – Pathology lab, Lindsay Wood Office Manager GLO, Anne Ronco Regional Director, Tiffany Schaffner Lead Medical Assistant, Nicole Askew (instructor), and Lauren Frosh LPN GLO.
✚ GoPro Donation | Light the Way FoundationElijah Burgess, son of Dr. Harris’ patient, Lisa Burgess, wanted to record his mom’s fight against metastatic
breast cancer. They try to have “adventures” together, as he calls them, and Elijah wanted a way to capture them. Dr. Harris and Florida Hospital Social Worker, Vanessa Hill with Light The Way Foundation made his wish come true.
Pictured left to right | Florida Hospital Andina Robeas, Florida Hospital Social Worker Vanessa Hill, FCS ARNP Amy Youman, Lisa Burgess-Patient of Dr. Harris’s, Elijah Burgess- son and GoPro recipient, FCS Physician Dr. Eric Harris, Physician Liasion Kay Simpkins and Jenifer Labonte from Light The Way Foundation.
✚ Light the Night Kick-off
FCS CMSO and The Leukemia & Lymphoma Society Suncoast Chapter Board Chair, Shelly H Glenn was a guest speaker at the Light the Night kick off event for 2018!
✚ Blanket Warmer Donation | PasadenaPassing along the gift of warmth to our patients, Dave and Bobbi Norris of the Make a Difference Foundation
donated a new blanket warmer to our Pasadena office, located in St. Petersburg.
Pictured left to right | Physician Liaison Manager, Maria Ramos-Person, VP of Practice Operations Jeff Rubin, Dave and Bobbi Norris, FCS Physician Dr. Vu Tran Ho, CMSO Shelly Glenn, and Physician Liaison Sandy Brooks.

Fall 2018 11
FCSNews
✚ FCS Leadership Program | 2018 GraduatesThe Leadership Program goal is simple — share strategies we think are key to creating future leaders
at FCS. We introduce the leadership and the business side of Florida Cancer Specialists that few people see. At the same time, we focus on strategies that are applicable for success. We challenge leaders to make the connection back to their area and learn to adapt and apply the philosophy.
The instructor-led leadership curriculum is two and a half days and includes courses such as Healthcare Law, Financial Literacy, Understanding FLMA, ADA and Workers’ Compensation and more.
Pictured left to right | First row: Sara Jones, FCS U Administrator/Mgr. Customer Experience; Patrice Rosser, Study Mgr.; Shari Duncan, Revenue Mgr.; Maria Ramos-Person, Physician Liaison Manager; Dan Baxter, Information Security Officer; Julie Briggs, Mgr. Radiation Services; Kelli Mendoza, Office Mgr.; Stephanie Sabillon, Pharmacy Operations Mgr.; Pam Venneri, Office Mgr.; Cathy Ruck, Prior Auth Nurse Mgr. Second row: Nicole Siaba, Accred & Regulatory; James Earley, Operational Excellence Mgr.; Dinah Welsh-Barnes, Study Manager; Jenean Fletcher, Office Mgr.; Kelly Staten, Revenue Mgr.; David McBreen, Dispensing & Distribution; Holly Stephens, Office Mgr.; Jodi Lohnes, Office Manager; Deidre Jenkins, Central Scheduling Mgr. Third row: Francine Ulrich, HR Mgr.; Diane Ducharme, Sup C&D Compliance; Sandy Leahy, Head Nurse; Anne Ronco, Regional Director; Barbara Scott, Office Mgr.; Todd Schonherz, COO; Eric Bush, IT Service Desk Mgr.
✚ Artist Donation at Orange Avenue LocationGinae Lee Scott, local artist and a former FCS patient of Dr. Lee Zehngebot, donates one of her paintings to the
treatment room at our Orange Avenue location.
Pictured left to right | Regional Director of Operations Lynn Sawyer, FCS former patient and local artist Ginae Lee Scott and Dr. Lee Zehngebot.
✚ LLS Woman of the Year 2018 | Rhonda WebsterFCS Senior Physician Liaison, Rhonda Webster was named the 2018 Leukemia & Lymphoma Society’s
Woman of the Year for Central Florida. She raised $131,739 for blood cancer services.
Pictured left to right | Nick Honingford, Denise Bennett-Walls, Patty Geddie, Anthony Cortes, FCS Senior Physician Liaison Rhonda Webster, Dr. Oludapo Soremi and Grayson Zrelack.
Pictured left to right | Trigg Webster, Quenton Fontaine, Rhonda’s husband David Webster, FCS Senior Physician Liaison and 2018 Woman of the Year Rhonda Webster, Aiden Fontaine, Tres Fontaine, Tori Cutlip, Chad and Joanna Walling. Front row - grandmother, Melva Patterson.

12 FCS The Magazine
✚ Run Amuck with a Duck | Gainesville, FLOn March 3, FCS physicians and staff joined the ninth annual Run Amuck with the Duck in Gainesville,
Florida. Thousands of participants walked, jogged or ran to raise awareness and critical funds for patient services and clinical research projects in the local community.
Pictured left to right | Front row: Tiffany Gorenburg Townsend, Jamie Gorenburg, Aidan Gorenberg Screwvala (duck), Hayley Gorenberg, Zoe Gorenberg Screwvala, Caren Gorenberg. Back row: Dick Gorenberg, George Sands, Mike Gorenberg, Pete Gorenberg, Dr. Lucio Gordan, and Mayor of Gainesville, Lauren Poe.
✚ FCS Supports the Tampa Bay Lightning Thank you to FCS Staff and Physicians — Dr. Michael Scott, Dr. David Wright, Dr. Christopher George, Dr.
Hafeez Chatoor and Dr. R. Waide Weaver — at the Tampa Cancer Center for showing your support. #GOBOLTS.
FCSNews
✚ Regional Cancer Center | Colon Cancer Awareness EventOn March 1, FCS physicians and staff participated in the Colon Cancer Awareness event at the Regional Cancer
Center located in Fort Myers, Florida.
✚ FCS VP of Practice Operations Inga Gonzalez Awarded Oviedo Winter Springs Trustee Award
Pictured left to right | Past President of the Oviedo-Winter Springs Regional Chamber of Commerce Todd Sykes, FCS VP of Practice Operations Inga Gonzalez, Chair of the Board of Directors Dawn Ofodile and Senior Office Manager Kristy Meeks.
✚ FCS Pathologist Scales KilimanjaroFCS Pathologist Dr. Gina Elhammady climbed Mount Kilimanjaro in Tanzania, and she made sure to take FCS
to the top with her!
✚ Courage Through Cancer WalkFCS Tallahassee office associates distributed FCS items at the Courage Through Cancer Walk at Tom Brown
Park, Tallahassee.
Pictured left to right | Shon Bennett, Letitia Owens, Suzanne Harrison, Patty Wright and Janet Shepard.

Fall 2018 13
✚ Fleming Island | Kentucky Derby Fundraiser On April 26, staff at the FCS Fleming Island location dressed up in honor of the Kentucky Derby for an
office fundraiser.
Pictured left to right | 1st row- Sheila Gagne, BSN, RN, Laura Sperry Associate Director, Tiara Wilds, PSS, 2nd row- Sherri Greene, BSN, RN, Holly Stephens Senior Office Manager, Sharrie Bauer LPN, Lori Stellar PSS, Jennifer Bailey Social Worker, Paulesha Gibson MA Back row- Samantha Hiller FC, Betty Geyer PSS, and Madeline Ribot Lead PSS.
✚ Sailing Heals 2018 | NaplesDr. Susan Morgan (now retired), of Florida Cancer Specialists, has participated in Sailing Heals over the years,
along with several of her patient guests. This year, Dr. Morgan made the day even more special by personally sponsoring a lunch for the patients, along with a few Naples Sailing & Yacht Club host captains.
“Sailing Heals offers our patients, who are going through one of the greatest challenges in life, a chance to get away from it all and enjoy a healing day on the water with family and friends. The joy and memories that result can last forever. It’s become a sort of field trip that I look forward to sharing with my patients every year. Even more than treatment plans, I like to ‘prescribe’ a day with Sailing Heals!” Dr. Morgan said.
✚ Kaitlin Hill, RN, OCN, BSN | Sun City CenterOne year ago, Kaitlin Hill enrolled
in the accelerated RN to BSN program at the University of South Florida knowing that she had a fast approaching deadline because of her husband’s pending deployment, just four days following her pinning on May 3. She approached her studies as she does everything else — with a positive, hard-working attitude while balancing her family and work.
Unknown to Kaitlin, she was the only recipient of the Academic Nursing Excellence Award in her graduating class. This award is bestowed upon a graduating student from the undergraduate program for overall excellence in nursing coursework. The recipient is selected on the basis of their academic achievements while enrolled in the USF College of Nursing. Kaitlin’s hard work and success not only reflects the Florida Cancer Specialists’ C.A.R.E. values, but also the very best of the nursing profession, as well.
✚ FCS Announces New Location in The VillagesOn May 10 in The Villages, Anchor Health and AHC Hospitality broke ground on the new Center of
Advanced Healthcare at Brownwood. In attendance were local dignitaries, executives from The Villages Health, Florida Cancer Specialists physicians and staff and guest speaker, Gov. Rick Scott. FCS’ new Brownwood office will be located at 2925 Traverse Trail, Villages, Florida 32163.
Pictured left to right | Jane Johansson, MSN, ARNP; Adewale Fawole, MD; Shannon Porterfields, RN, BSN; Jennifer Cultrera, MD; Jeff Esham, Vice President of Radiation Oncology and Radiology, Todd Schonherz, COO; Governor Rick Scott; Marays Veliz, MD; Inga Gonzalez, Vice President of Practice Operations; Annie Pigue, Associate Regional Director of Operations; Danielle Spears, Senior Physician Liaison.
FCSNews
Kaitlin Hill, RN, OCN, BSN

14 FCS The Magazine
FCSNews
✚ Evening with the Doctors in Fort MyersOn April 30, FCS hosted an “Evening with the Doctors” in Fort Myers at our Fort Myers Cancer
Center located in Gladiolus. Patients and the local community were invited to hear the latest on the initiatives and studies from FCS physicians and ask questions. Guests enjoyed hors d’oeuvres and light refreshments.
Pictured left to right | Dr. Gamini S. Soori, Dr. Michael J. McCleod, Dr. Faithlore Gardner, Dr. Silvia Romero, Dr. Liliana Bustamante, Dr. Raymond Esper, Dr. Syed F. Zafar and Dr. Frank Rodriguez.
✚ FCS Hosts Ribbon Cutting & Open House in Sun CityFCS physicians and staff welcomed patients, volunteers and local community leaders to a ribbon cutting
ceremony and open house on April 25 to unveil the newly renovated Sun City location. With nearly 100 attendees, the event celebrated the new and larger facility that provides greater access and convenience for patients in the Hillsborough area. Following the ceremony, guests enjoyed refreshments and a tour of the cancer center.
Pictured left to right | FCS CMSO Shelly Glenn, Ceci Garcia, Office Manager, Stacey Cowder, RN, Sam Watkins, Director of Operations, Anne Marie Neumann, Head Nurse, Wanda Howard, PSS, Shanise Guy, RN, Dr. Mark Robbins, Pam Sevalia, ARNP, Dr. Renjitha Ignatius, Alyssa Arnaud, RN, Monica Tyler, Senior Physician Liaison, Tiffany Gregory, MA.
✚ FCS Hosts Patient Appreciation BBQ in Spring HillOn April 21, FCS hosted the first annual Venice/Englewood Patient Appreciation BBQ! With more than
500 attendees, patients, family members, FCS Physicians and staff enjoyed great food, music and laughter!
Pictured left to right | First Row: Jennifer Nazario PSS, Beth Jensen OM, Amber Wright PSS, Ryan Howes PSS, Sylvie Cerami Head Nurse, Mehnaz Junagadhwalla MD, Robin Lifton MD, Shelly Glenn Chief Marketing & Sales Officer.Second Row: Pamy Owen PSS, Lilian Jerome PSS, Michelle Jones Head Nurse, Russ Laureno volunteer (Cate Husband) Cate Laureno OM, Patricia LeDuc PSS, Shelia Mattos PSS, Kysa Medina Financial Counselor, Jodi Lohnes Associate Regional Medical Director, Tabatha Brown Assistant OM, Back row behind Jodi, Jeffrey Richard, volunteer (with Jodi) and Jeffrey Rubin VP of Operations.
✚ Sebring | Blanket Warmer DonationOn May 9, Dave and Bobbi Norris of the Make a Difference Foundation passed along the gift of
warmth to our patients by donating a new blanket warmer to our Sebring location.
Pictured left to right | CMSO Shelly Glenn, FCS Physician Dr. Amit Shah, FCS Physician Dr. Syed Ahmed, Bobbi Norris, Dave Norris and Regional Director Anne Ronco.
Fall 2018 15
FCSNews
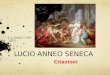
✚ Groundbreaking | OcalaAt a groundbreaking ceremony May 16, FCS celebrated a new state-of-the-art cancer center that will be located
on S.W. 48th Ave., Ocala, Florida 34474. With shovels in hand, FCS Executive Management, staff and Marion County physicians, Drs. Patrick Acevedo, Shilpa Oberoi, Vipul Patel, Craig Reynolds, Sachin Kamath and Mohammad Kamal, kicked off the transformation of an empty field into the new $10 million comprehensive center, which is scheduled to open in the fall of 2019.
Pictured left to right | First Row: Shelly Glenn, Chief Marketing and Sales Officer; Mayor Kent Guinn; Jeffrey Rubin, VP of Practice Operations; Vipul Patel, MD; Sachin Kamath, MD; Craig Reynolds, MD; Shilpa Oberoi, MD; Patrick Acevedo, MD; Mohammad Kamal, MD; Brad Prechtl, CEOSecond Row: April Watkins, Regional Lab Monitor; Andy Boggini, Optimal Outcomes; Unknown to me; Lauren Lucas, ARNP; Kim Fiscus, ARNP-C, AOCNP; Jordan Griffis, ARNP; Whitney Griffith, ARNP; DeeDee Stewart PSS Team Lead; Theresa Jones, Office Manage; Rashana Wilson, Charge Nurse; Trina Emerson, Clinic Financial Manager; Kathy Bruce, MA Team Lead; Diana Marcano, Assistant Office ManagerThird Row: Jennifer McKathan, American Cancer Society; Chris Nibe, Palm Gardens Home Care; Matt Jurusik, Scott Johnson, Jim Graham; Frank Nunziato, Director of Construction Development; Levester Jones, Director of Radiology; Brett Hipsley, Physician Liaison; Tishia Moeller from WOCA; Kevin Kinsella, Caris Life Sciences; Anna Marie Zambito, Radiology Services Supervisor; Renee Genther, ANP-B, AOCNP; Christina White, RN, OCN, Nurse Specialist; Jeff Esham, VP of Radiation Oncology and Radiology.
✚ New Port Richey | Spring FlingOn May 4, the New Port Richey staff and physicians welcomed more than 300 patients and family members
for a Spring Fling Patient Appreciation event.
Pictured left to right | Samuel McIntyre, Cheryl Leichssenring, Courtney Pryor, Elise Bingham, Tracy Adams, Sabrina Martin, Tim McDaniels, Steve Longenecker, Denise Anderson, Joann Dresch, Lisa Spiller, Melissa Gonzalez, Claudia Salazar, Charkay Suiters, Patty Ortiz, Sophia Fang, Kim Fox, VP Practice Opeations Jeff Rubin, Michelle Brown, Brianna Brown, Laura Broshears, Linda Wilson, Jackie Reilly, Sunita Subedi, Amanda Roeding, Mary Mobley, Asti Rego, Physician Liaison Manager Maria Ramos-Person, Mara Carideo, Amanda Ernst, Veronica Filardo, Joshua Ducas, Letitia Alvarez, Crystal Clark, Julie Briggs, Shannon Chaffin, Michelle Bonetti, Savanna McCabe, Chief Marketing & Sales Officer Shelly Glenn, Sharon Barello and Dagmar Schobert.
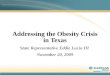
✚ Day of Champions | Daytona BeachOn June 5, FCS and Florida Hospital hosted the National Cancer Survivors Day at Jackie Robinson
Ballpark. Guests enjoyed BBQ and the Daytona Tortugas game vs. the Clearwater Threshers. Celgene sponsored the fireworks.
Pictured left to right | Physician Liaison Kay Simpkins, Financial Counselor Kim Heller, Jaylise Maldonad Daughter of Sabrina, Patient Service Specialist Sabrina Maldonad, Care Management Manager Beth Wittmer RN, Associate Director, Care Management Don Champlain RN, MHA, FCS Volunteer Program Manager (North) Rebecca Davis and FCS Foundation Executive Director Lynn Rasys.
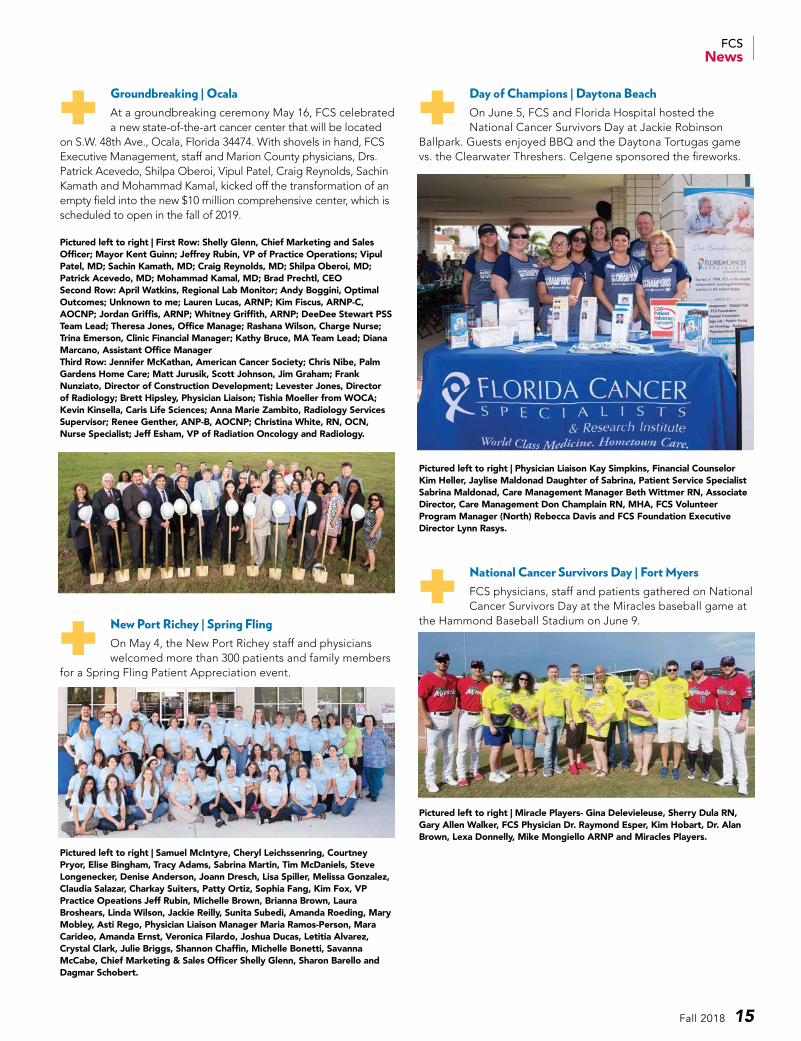
✚ National Cancer Survivors Day | Fort MyersFCS physicians, staff and patients gathered on National Cancer Survivors Day at the Miracles baseball game at
the Hammond Baseball Stadium on June 9.
Pictured left to right | Miracle Players- Gina Delevieleuse, Sherry Dula RN, Gary Allen Walker, FCS Physician Dr. Raymond Esper, Kim Hobart, Dr. Alan Brown, Lexa Donnelly, Mike Mongiello ARNP and Miracles Players.

16 FCS The Magazine
✚ Subaru Blanket Donation | TampaThank you to Reeves Subaru and The Leukemia & Lymphoma Society-Suncoast Chapter for delivering
blankets to patients at the Tampa Cancer Center in honor of the #SubaruLovestoCare program!
Pictured left to right | Pisandro Moncion, Subaru Sales Manager; Miranda Zoloty, LLS Campaign Manager; Rose Bullock, Receptionist; Jennifer Kober, Event & Marketing Assistant; Hans Lindau, Finance Manager; Breanna Castle, Receptionist; Dr. Magda Melchert, FCS Physician; Dr. Michael Scott, FCS Physician; Sam Watkins, Regional Director; Monica Tyler, Senior Physician Liaison; Brandy Kovarsky, LLS Campaign Manager; Austin Simon, LLS Senior Campaign Manager.
✚ Subaru Blanket Donation | BradentonThank you to Reeves Subaru and The Leukemia & Lymphoma Society-Suncoast Chapter for delivering
blankets to patients at our Bradenton location in honor of the #SubaruLovestoCare program!
Pictured left to right | Physician Liaison Mary Ellen Woska, Assistant Office Manager Paula Bauer, Associate Regional Director of Operations Jodi Lohnes, Conley Subaru President Jeff Conley, Susan Conley, Dr. Robert Whorf, Dr. Ana Van Der Wall, Dr. Brian Berry, Celeste Montoya ARNP, Leukemia & Lymphoma Society Campaign Manager Brandy Kovarsky, Conley Subaru Sales Manager Robert Mulroy and Conley Subaru Fixed Operations Manager Alan Conley
✚ Patient Adocacy Network EventOn June 20, 2018, FCS Gainesville Cancer Center Physician, Dr. Lucio Gordan, was the guest speaker for the Community
Oncology Alliance - Patient Advocacy Network (CPAN) event.
Pictured left to right | Brett Hipsley, Physician Liaison, Don Champlain, Director of Care Management, Lisa Clark, RN, FCS Physician, Dr. Lucio Gordan, Charise Holcombe, PA-C Genentech
✚ First CPAN Chapter Meeting in Fort Myers Held at the Fort Myers Cancer Center
Pictured left to right | Emile Pearl, Renee Pearl, Hannah Shraiar, Wendy Shraiar and Lora McCann.
✚ Tampa Cancer Center | Bucs Movie DayThe Tampa Bay Buccaneers hosted Tampa Cancer Center’s patients’ children for the annual movie day!
FCS CMSO Shelly H. Glenn was a guest speaker at the Light the Night kick-off event for 2018!
✚ Nutrition Event | HighlandsOn June 28, FCS held the second quarterly Nutrition/Survivorship event at the Highland office. FCS Nutritionist
April Rozzo presented to more than 64 in attendance about cancer fighting diets and which one can be right for you. Dr. Jooma and Dr. Alemar were on hand to help answer patient questions.
Pictured left to right | Dr. Nuruddin Jooma, Dr. Jose Alemar, FCS Nutritionist April Rozzo MS, RD, CSO, LDN, and Director of Care Management Don Champlain, RN, MHA.
FCSNews

Fall 2018 17
✚ NASCAR Xfinity Driver Matt Tifft | Daytona BeachOn July 6, FCS hosted NASCAR Xfinity driver Matt Tifft at the Florida Hospital Cancer Institute in Daytona
Beach for a patient meet and greet. Matt shared his time and journey with all of those in attendance.
Pictured left to right | Director of Radiation Oncology Eastside Michelle Rosato, FCS Physician Dr. Mudussara Khan, NASCAR Driver Matt Tifft, FCS Physician Dr. Eric Harris, and Regional Administrator of the Oncology Service Line Florida Hospital Central Division, North Region Imee Unto, RN, MSN, OCN.
✚ West Palm Beach | Blanket Warmer DonationOn July 24, Dave and Bobbi Norris of the Make a Difference Foundation passed along the gift of warmth
to our patients by donating a new blanket warmer to our West Palm Beach location. Thank you to Bespoke for their generous support on this donation!
Pictured left to right | Senior Office Manager Diana Cabrera, Senior Physician Liaison Rebecca Appelbaum, Head Nurse Naomi Poston, Dr. Marilyn Raymond, Dave & Bobbi Norris, Dr. Dan Spitz, Regional Director of Operations Lois Brown, and FCS CMSO Shelly Glenn.
✚ LWR Cancer Center GroundbreakingFlorida Cancer Specialists is building a new cancer center for Lakewood Ranch near the corner of Lakewood Ranch
Boulevard and State Road 70 to serve the fast-growing population of Manatee County. The $16 million facility, which will house the cancer center, will be completed in the Summer of 2019.
Pictured left to right | The Lunz Group Jim Graham, FCS VP of Radiation & Radiology Jeff Esham, FCS CMSO Shelly Glenn, Joe Hwang COO LWR Medical Center, Andy Boggini Principal of Optimal Outcomes, FCS Associate Regional Director Jodi Lohnes, Heather Kasten President/CEO of Lakewood Ranch Business Alliance, FCS CEO Brad Prechtl, MBA, FCS Physician Dr. Fadi Kayali, FCS Physician Dr. Miguel Pelayo, FCS Physician Dr. Janice Eakle, FCS Physician Dr. Amir Hirandi and FCS Physician Liaison Mary Ellen Woska.
✚ Grace Girls Home | Sri LankaFCS Physician in Largo, Florida, Dr. Nuruddin Jooma, MD, MPH, donates his time and efforts to Grace Girls
Home, an orphanage located in Sri Lanka. This past summer, Dr. Jooma and his family purchased clothing for the girls and donated iPads and other tech software for education purposes. Dr. Jooma will be returning next Spring in hopes to provide more donations from FCS physicians and staff. Dr. Jooma and his work with Grace Girls Home will be featured in our next issue. For more information on Grace Girls Home visit GraceGirlsHome.org.
FCSNews

NINLARO is indicated in combination with lenalidomide and dexamethasone for the treatment of patients with multiple myeloma who have received at least one prior therapy.treatment of patients with multiple myeloma who have received at least one prior therapy.TOURMALINE-MM1: a global, phase 3, randomized (1:1), double-blind, placebo-controlled study that evaluated the safety and e� cacy
of NINLARO (an oral PI) vs placebo, both in combination with lenalidomide and dexamethasone, until disease progression or unacceptable toxicity in 722 patients with relapsed and/or refractory multiple myeloma who received 1-3 prior therapies.1
TREATING MYELOMA CAN SEEM LIKE A MARATHON
Prescribe the all-oral NINLARO regimen for long-term‡ proteasome inhibition.
Continuous treatment with a proteasome inhibitor (PI)–based regimen is associated with clinical benefi ts.1 However, most patients who have had
1 prior therapy only receive PIs for 4 to 7 months.2-4
The NINLARO® (ixazomib) regimen extended PFS by ~6 months (median: 20.6 vs 14.7 months) vs the placebo regimen in patients with multiple
myeloma who have received at least 1 prior therapy.1*†
WOULD YOU TAKE OFF YOUR SHOE WHEN RUNNING A MARATHON?
Warnings and Precautions• Thrombocytopenia has been reported with NINLARO.
During treatment, monitor platelet counts at least monthly, and consider more frequent monitoring during the fi rst three cycles. Manage thrombocytopenia with dose modifi cations and platelet transfusions as per standard medical guidelines. Adjust dosing as needed. Platelet nadirs occurred between Days 14-21 of each 28-day cycle and typically recovered to baseline by the start of the next cycle.
• Gastrointestinal Toxicities, including diarrhea, constipation, nausea and vomiting, were reported with NINLARO and may occasionally require the use of antidiarrheal and antiemetic medications, and supportive care. Diarrhea resulted in the discontinuation of one or more of the three drugs in 1% of patients in the NINLARO regimen and < 1% of patients in the placebo regimen. Adjust dosing for severe symptoms.
• Peripheral Neuropathy (predominantly sensory) was reported with NINLARO. The most commonly reported reaction was peripheral sensory neuropathy (19% and 14% in the NINLARO and placebo regimens, respectively). Peripheral motor neuropathy was not commonly reported in either regimen (< 1%). Peripheral neuropathy resulted in discontinuation of one or more of the three drugs in 1% of patients in both regimens. Monitor patients for symptoms of peripheral neuropathy and adjust dosing as needed.
• Peripheral Edema was reported with NINLARO. Monitor for fl uid retention. Investigate for underlying causes when appropriate and provide supportive care as necessary. Adjust dosing of dexamethasone per its prescribing information or NINLARO for Grade 3 or 4 symptoms.
• Cutaneous Reactions: Rash, most commonly maculo-papular and macular rash, was reported with NINLARO. Rash resulted in discontinuation of one or more of the three drugs in < 1% of patients in both regimens. Manage rash with supportive care or with dose modifi cation.
• Hepatotoxicity has been reported with NINLARO. Drug-induced liver injury, hepatocellular injury, hepatic steatosis, hepatitis cholestatic and hepatotoxicity have each been reported in < 1% of patients treated with NINLARO. Events of liver impairment have been reported (6% in the NINLARO regimen and 5% in the placebo regimen). Monitor hepatic enzymes regularly during treatment and adjust dosing as needed.
• Embryo-fetal Toxicity: NINLARO can cause fetal harm. Women should be advised of the potential risk to a fetus, to avoid becoming pregnant, and to use contraception during treatment and for an additional 90 days after the fi nal dose of NINLARO. Women using hormonal contraceptives should also use a barrier method of contraception.
Adverse ReactionsThe most common adverse reactions (≥ 20%) in the NINLARO regimen and greater than the placebo regimen, respectively, were diarrhea (42%, 36%), constipation (34%, 25%), thrombocytopenia (78%, 54%; pooled from adverse events and laboratory data), peripheral neuropathy (28%, 21%), nausea (26%, 21%), peripheral edema (25%, 18%), vomiting (22%, 11%), and back pain (21%, 16%). Serious adverse reactions reported in ≥ 2% of patients included thrombocytopenia (2%) and diarrhea (2%).
Special Populations• Hepatic Impairment: Reduce the NINLARO starting
dose to 3 mg in patients with moderate or severe hepatic impairment.
• Renal Impairment: Reduce the NINLARO starting dose to 3 mg in patients with severe renal impairment or end-stage renal disease requiring dialysis. NINLARO is not dialyzable.
• Lactation: Advise nursing women not to breastfeed during treatment with NINLARO and for 90 days after the last dose.
Drug Interactions: Avoid concomitant administration of NINLARO with strong CYP3A inducers.
All trademarks are the property of their respective owners.
©2018 Millennium Pharmaceuticals, Inc., a wholly owned subsidiary of Takeda Pharmaceutical Company Limited.All rights reserved. Printed in USA 8/18 MAT-US-IXA-18-00331
*The NINLARO regimen included NINLARO+lenalidomide+dexamethasone. The placebo regimen included placebo+lenalidomide+dexamethasone. †95% CI, 17.0-NE and 95% CI, 12.9-17.6, respectively; HR=0.74 (95% CI, 0.587-0.939); P=0.012. ‡Defi ned as treatment to progression or unacceptable toxicity. NE=not evaluable; PFS=progression-free survival.
REFERENCES: 1. Moreau P, Masszi T, Grzasko N, et al; for TOURMALINE-MM1 Study Group. Oral ixazomib, lenalidomide, and dexamethasone for multiple myeloma. N Engl J Med. 2016;374(17):1621-1634. 2. Yong K, Delforge M, Driessen C, et al. Multiple myeloma: patient outcomes in real-world practice. Br J Haematol. 2016;175(2):252-264. 3. Jagannath S, Roy A, Kish J, et al. Real-world treatment patterns and associated progression-free survival in relapsed/refractory multiple myeloma among US community oncology practices. Expert Rev Hematol. 2016;9(7):707-717. 4. Romanus D, Raju A, Yong C, et al. Duration of therapy in U.S. patients treated for relapsed/refractory multiple myeloma (RRMM) in the real world. Poster presented at: European Hematology Association 21st Congress; June 9-12, 2016; Copenhagen, Denmark.
Important Safety Information
Please see accompanying Brief Summary.
S:14.5”
S:1
0”
T:16.75”
T:10
.87
5”
B:17.25”
B:1
1.1
25
”
IXAZ17CDNY2641_FALL FCS_2018_King_r5.indd 1 8/23/18 12:30 PM

NINLARO is indicated in combination with lenalidomide and dexamethasone for the treatment of patients with multiple myeloma who have received at least one prior therapy.treatment of patients with multiple myeloma who have received at least one prior therapy.TOURMALINE-MM1: a global, phase 3, randomized (1:1), double-blind, placebo-controlled study that evaluated the safety and e� cacy
of NINLARO (an oral PI) vs placebo, both in combination with lenalidomide and dexamethasone, until disease progression or unacceptable toxicity in 722 patients with relapsed and/or refractory multiple myeloma who received 1-3 prior therapies.1
TREATING MYELOMA CAN SEEM LIKE A MARATHON
Prescribe the all-oral NINLARO regimen for long-term‡ proteasome inhibition.
Continuous treatment with a proteasome inhibitor (PI)–based regimen is associated with clinical benefi ts.1 However, most patients who have had
1 prior therapy only receive PIs for 4 to 7 months.2-4
The NINLARO® (ixazomib) regimen extended PFS by ~6 months (median: 20.6 vs 14.7 months) vs the placebo regimen in patients with multiple
myeloma who have received at least 1 prior therapy.1*†
WOULD YOU TAKE OFF YOUR SHOE WHEN RUNNING A MARATHON?
Warnings and Precautions• Thrombocytopenia has been reported with NINLARO.
During treatment, monitor platelet counts at least monthly, and consider more frequent monitoring during the fi rst three cycles. Manage thrombocytopenia with dose modifi cations and platelet transfusions as per standard medical guidelines. Adjust dosing as needed. Platelet nadirs occurred between Days 14-21 of each 28-day cycle and typically recovered to baseline by the start of the next cycle.
• Gastrointestinal Toxicities, including diarrhea, constipation, nausea and vomiting, were reported with NINLARO and may occasionally require the use of antidiarrheal and antiemetic medications, and supportive care. Diarrhea resulted in the discontinuation of one or more of the three drugs in 1% of patients in the NINLARO regimen and < 1% of patients in the placebo regimen. Adjust dosing for severe symptoms.
• Peripheral Neuropathy (predominantly sensory) was reported with NINLARO. The most commonly reported reaction was peripheral sensory neuropathy (19% and 14% in the NINLARO and placebo regimens, respectively). Peripheral motor neuropathy was not commonly reported in either regimen (< 1%). Peripheral neuropathy resulted in discontinuation of one or more of the three drugs in 1% of patients in both regimens. Monitor patients for symptoms of peripheral neuropathy and adjust dosing as needed.
• Peripheral Edema was reported with NINLARO. Monitor for fl uid retention. Investigate for underlying causes when appropriate and provide supportive care as necessary. Adjust dosing of dexamethasone per its prescribing information or NINLARO for Grade 3 or 4 symptoms.
• Cutaneous Reactions: Rash, most commonly maculo-papular and macular rash, was reported with NINLARO. Rash resulted in discontinuation of one or more of the three drugs in < 1% of patients in both regimens. Manage rash with supportive care or with dose modifi cation.
• Hepatotoxicity has been reported with NINLARO. Drug-induced liver injury, hepatocellular injury, hepatic steatosis, hepatitis cholestatic and hepatotoxicity have each been reported in < 1% of patients treated with NINLARO. Events of liver impairment have been reported (6% in the NINLARO regimen and 5% in the placebo regimen). Monitor hepatic enzymes regularly during treatment and adjust dosing as needed.
• Embryo-fetal Toxicity: NINLARO can cause fetal harm. Women should be advised of the potential risk to a fetus, to avoid becoming pregnant, and to use contraception during treatment and for an additional 90 days after the fi nal dose of NINLARO. Women using hormonal contraceptives should also use a barrier method of contraception.
Adverse ReactionsThe most common adverse reactions (≥ 20%) in the NINLARO regimen and greater than the placebo regimen, respectively, were diarrhea (42%, 36%), constipation (34%, 25%), thrombocytopenia (78%, 54%; pooled from adverse events and laboratory data), peripheral neuropathy (28%, 21%), nausea (26%, 21%), peripheral edema (25%, 18%), vomiting (22%, 11%), and back pain (21%, 16%). Serious adverse reactions reported in ≥ 2% of patients included thrombocytopenia (2%) and diarrhea (2%).
Special Populations• Hepatic Impairment: Reduce the NINLARO starting
dose to 3 mg in patients with moderate or severe hepatic impairment.
• Renal Impairment: Reduce the NINLARO starting dose to 3 mg in patients with severe renal impairment or end-stage renal disease requiring dialysis. NINLARO is not dialyzable.
• Lactation: Advise nursing women not to breastfeed during treatment with NINLARO and for 90 days after the last dose.
Drug Interactions: Avoid concomitant administration of NINLARO with strong CYP3A inducers.
All trademarks are the property of their respective owners.
©2018 Millennium Pharmaceuticals, Inc., a wholly owned subsidiary of Takeda Pharmaceutical Company Limited.All rights reserved. Printed in USA 8/18 MAT-US-IXA-18-00331
*The NINLARO regimen included NINLARO+lenalidomide+dexamethasone. The placebo regimen included placebo+lenalidomide+dexamethasone. †95% CI, 17.0-NE and 95% CI, 12.9-17.6, respectively; HR=0.74 (95% CI, 0.587-0.939); P=0.012. ‡Defi ned as treatment to progression or unacceptable toxicity. NE=not evaluable; PFS=progression-free survival.
REFERENCES: 1. Moreau P, Masszi T, Grzasko N, et al; for TOURMALINE-MM1 Study Group. Oral ixazomib, lenalidomide, and dexamethasone for multiple myeloma. N Engl J Med. 2016;374(17):1621-1634. 2. Yong K, Delforge M, Driessen C, et al. Multiple myeloma: patient outcomes in real-world practice. Br J Haematol. 2016;175(2):252-264. 3. Jagannath S, Roy A, Kish J, et al. Real-world treatment patterns and associated progression-free survival in relapsed/refractory multiple myeloma among US community oncology practices. Expert Rev Hematol. 2016;9(7):707-717. 4. Romanus D, Raju A, Yong C, et al. Duration of therapy in U.S. patients treated for relapsed/refractory multiple myeloma (RRMM) in the real world. Poster presented at: European Hematology Association 21st Congress; June 9-12, 2016; Copenhagen, Denmark.
Important Safety Information
Please see accompanying Brief Summary.
S:14.5”
S:1
0”
T:16.75”
T:10
.87
5”
B:17.25”
B:1
1.1
25
”
IXAZ17CDNY2641_FALL FCS_2018_King_r5.indd 1 8/23/18 12:30 PM

BRIEF SUMMARY OF PRESCRIBING INFORMATIONNINLARO (ixazomib) capsules, for oral use
1 INDICATIONNINLARO (ixazomib) is indicated in combination with lenalidomide and dexamethasone for the treatment of patients with multiple myeloma who have received at least one prior therapy.
5 WARNINGS AND PRECAUTIONS5.1 Thrombocytopenia: Thrombocytopenia has been reported with NINLARO with platelet nadirs typically occurring between Days 14-21 of each 28-day cycle and recovery to baseline by the start of the next cycle. Three percent of patients in the NINLARO regimen and 1% of patients in the placebo regimen had a platelet count ≤ 10,000/mm3 during treatment. Less than 1% of patients in both regimens had a platelet count ≤ 5000/mm3 during treatment. Discontinuations due to thrombocytopenia were similar in both regimens (< 1% of patients in the NINLARO regimen and 2% of patients in the placebo regimen discontinued one or more of the three drugs).The rate of platelet transfusions was 6% in the NINLARO regimen and 5% in the placebo regimen. Monitor platelet counts at least monthly during treatment with NINLARO. Consider more frequent monitoring during the first three cycles. Manage thrombocytopenia with dose modifications and platelet transfusions as per standard medical guidelines.5.2 Gastrointestinal Toxicities: Diarrhea, constipation, nausea, and vomiting, have been reported with NINLARO, occasionally requiring use of antidiarrheal and antiemetic medications, and supportive care. Diarrhea was reported in 42% of patients in the NINLARO regimen and 36% in the placebo regimen, constipation in 34% and 25%, respectively, nausea in 26% and 21%, respectively, and vomiting in 22% and 11%, respectively. Diarrhea resulted in discontinuation of one or more of the three drugs in 1% of patients in the NINLARO regimen and < 1% of patients in the placebo regimen. Adjust dosing for Grade 3 or 4 symptoms.5.3 Peripheral Neuropathy: The majority of peripheral neuropathy adverse reactions were Grade 1 (18% in the NINLARO regimen and 14% in the placebo regimen) and Grade 2 (8% in the NINLARO regimen and 5% in the placebo regimen). Grade 3 adverse reactions of peripheral neuropathy were reported at 2% in both regimens; there were no Grade 4 or serious adverse reactions. The most commonly reported reaction was peripheral sensory neuropathy (19% and 14% in the NINLARO and placebo regimen, respectively). Peripheral motor neuropathy was not commonly reported in either regimen (< 1%). Peripheral neuropathy resulted in discontinuation of one or more of the three drugs in 1% of patients in both regimens. Patients should be monitored for symptoms of neuropathy. Patients experiencing new or worsening peripheral neuropathy may require dose modification.5.4 Peripheral Edema: Peripheral edema was reported in 25% and 18% of patients in the NINLARO and placebo regimens, respectively. The majority of peripheral edema adverse reactions were Grade 1 (16% in the NINLARO regimen and 13% in the placebo regimen) and Grade 2 (7% in the NINLARO regimen and 4% in the placebo regimen).Grade 3 peripheral edema was reported in 2% and 1% of patients in the NINLARO and placebo regimens, respectively. There was no Grade 4 peripheral edema reported. There were no discontinuations reported due to peripheral edema. Evaluate for underlying causes and provide supportive care, as necessary. Adjust dosing of dexamethasone per its prescribing information or NINLARO for Grade 3 or 4 symptoms.5.5 Cutaneous Reactions: Rash was reported in 19% of patients in the NINLARO regimen and 11% of patients in the placebo regimen. The majority of the rash adverse reactions were Grade 1 (10% in the NINLARO regimen and 7% in the placebo regimen) or Grade 2 (6% in the NINLARO regimen and 3% in the placebo regimen). Grade 3 rash was reported in 3% of patients in the NINLARO regimen and 1% of patients in the placebo regimen. There were no Grade 4 or serious adverse reactions of rash reported. The most common type of rash reported in both regimens included maculo-papular and macular rash. Rash resulted in discontinuation of one or more of the three drugs in < 1% of patients in both regimens. Manage rash with supportive care or with dose modification if Grade 2 or higher.5.6 Hepatotoxicity: Drug-induced liver injury, hepatocellular injury, hepatic steatosis, hepatitis cholestatic and hepatotoxicity have each been reported in < 1% of patients treated with NINLARO. Events of liver impairment have been reported (6% in the NINLARO regimen and 5% in the placebo regimen). Monitor hepatic enzymes regularly and adjust dosing for Grade 3 or 4 symptoms.5.7 Embryo-Fetal Toxicity: NINLARO can cause fetal harm when administered to a pregnant woman based on the mechanism of action and findings in animals. There are no adequate and well-controlled studies in pregnant women using NINLARO. Ixazomib caused embryo-fetal toxicity in pregnant rats and rabbits at doses resulting in exposures that were slightly higher than those observed in patients receiving the recommended dose.
Females of reproductive potential should be advised to avoid becoming pregnant while being treated with NINLARO. If NINLARO is used during pregnancy or if the patient becomes pregnant while taking NINLARO, the patient should be apprised of the potential hazard to the fetus. Advise females of reproductive potential that they must use effective contraception during treatment with NINLARO and for 90 days following the final dose. Women using hormonal contraceptives should also use a barrier method of contraception.
6 ADVERSE REACTIONSThe following adverse reactions are described in detail in other sections of the prescribing information:• Thrombocytopenia [see Warnings and Precautions (5.1)]• Gastrointestinal Toxicities [see Warnings and Precautions (5.2)]• Peripheral Neuropathy [see Warnings and Precautions (5.3)]• Peripheral Edema [see Warnings and Precautions (5.4)]• Cutaneous Reactions [see Warnings and Precautions (5.5)]• Hepatotoxicity [see Warnings and Precautions (5.6)]
6.1 CLINICAL TRIALS EXPERIENCEBecause clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.The safety population from the randomized, double-blind, placebo-controlled clinical study included 720 patients with relapsed and/or refractory multiple myeloma, who received NINLARO in combination with lenalidomide and dexamethasone (NINLARO regimen; N=360) or placebo in combination with lenalidomide and dexamethasone (placebo regimen; N=360). The most frequently reported adverse reactions (≥ 20%) in the NINLARO regimen and greater than the placebo regimen were diarrhea, constipation, thrombocytopenia, peripheral neuropathy, nausea, peripheral edema, vomiting, and back pain. Serious adverse reactions reported in ≥ 2% of patients included thrombocytopenia (2%) and diarrhea (2%). For each adverse reaction, one or more of the three drugs was discontinued in ≤ 1% of patients in the NINLARO regimen.Table 4: Non-Hematologic Adverse Reactions Occurring in ≥ 5% of Patients with a ≥ 5% Difference Between the NINLARO Regimen and the Placebo Regimen (All Grades, Grade 3 and Grade 4)
NINLARO + Lenalidomide and Dexamethasone
N=360
Placebo + Lenalidomide and Dexamethasone
N=360
System Organ Class / Preferred Term N (%) N (%)
All Grade 3
Grade 4 All Grade
3Grade
4
Infections and infestationsUpper respiratory tract infection 69 (19) 1 (< 1) 0 52 (14) 2 (< 1) 0
Nervous system disordersPeripheral neuropathies* 100 (28) 7 (2) 0 77 (21) 7 (2) 0
Gastrointestinal disordersDiarrheaConstipationNauseaVomiting
151 (42)122 (34)92 (26)79 (22)
22 (6)1 (< 1)6 (2)4 (1)
0000
130 (36)90 (25)74 (21)38 (11)
8 (2)1 (< 1)
02 (< 1)
0000
Skin and subcutaneous tissue disorders
Rash* 68 (19) 9 (3) 0 38 (11) 5 (1) 0
Musculoskeletal and connective tissue disorders
Back pain 74 (21) 2 (< 1) 0 57 (16) 9 (3) 0
General disorders and administration site conditions
Edema peripheral 91 (25) 8 (2) 0 66 (18) 4 (1) 0
Note: Adverse reactions included as preferred terms are based on MedDRA version 16.0. *Represents a pooling of preferred terms
(Continued on next page)
T:7”
T:10”
IXAZ18CDNY6401_Brief_Summary_A_Size_r3.indd 1 8/13/18 6:55 PM
IXAZ17CDNY2641_FALL FCS_2018_King_BS_r5.indd 1 8/23/18 12:31 PM
Brief Summary (cont’d)
Table 5: Thrombocytopenia and Neutropenia (pooled adverse event and laboratory data)
NINLARO + Lenalidomide and Dexamethasone
N=360
Placebo + Lenalidomide and Dexamethasone
N=360
N (%) N (%)
Any Grade Grade 3-4 Any Grade Grade 3-4
Thrombocytopenia 281 (78) 93 (26) 196 (54) 39 (11)
Neutropenia 240 (67) 93 (26) 239 (66) 107 (30)
Herpes ZosterHerpes zoster was reported in 4% of patients in the NINLARO regimen and 2% of patients in the placebo regimen. Antiviral prophylaxis was allowed at the physician’s discretion. Patients treated in the NINLARO regimen who received antiviral prophylaxis had a lower incidence (< 1%) of herpes zoster infection compared to patients who did not receive prophylaxis (6%).Eye DisordersEye disorders were reported with many different preferred terms but in aggregate, the frequency was 26% in patients in the NINLARO regimen and 16% of patients in the placebo regimen. The most common adverse reactions were blurred vision (6% in the NINLARO regimen and 3% in the placebo regimen), dry eye (5% in the NINLARO regimen and 1% in the placebo regimen), and conjunctivitis (6% in the NINLARO regimen and 1% in the placebo regimen). Grade 3 adverse reactions were reported in 2% of patients in the NINLARO regimen and 1% in the placebo regimen.The following serious adverse reactions have each been reported at a frequency of < 1%: acute febrile neutrophilic dermatosis (Sweet’s syndrome), Stevens-Johnson syndrome, transverse myelitis, posterior reversible encephalopathy syndrome, tumor lysis syndrome, and thrombotic thrombocytopenic purpura. 7 DRUG INTERACTIONS7.1 Strong CYP3A Inducers: Avoid concomitant administration of NINLARO with strong CYP3A inducers (such as rifampin, phenytoin, carbamazepine, and St. John’s Wort).8 USE IN SPECIFIC POPULATIONS8.1 Pregnancy: Risk Summary: Based on its mechanism of action and data from animal reproduction studies, NINLARO can cause fetal harm when administered to a pregnant woman. There are no human data available regarding the potential effect of NINLARO on pregnancy or development of the embryo or fetus. Ixazomib caused embryo-fetal toxicity in pregnant rats and rabbits at doses resulting in exposures that were slightly higher then those observed in patients receiving the recommended dose. Advise women of the potential risk to a fetus and to avoid becoming pregnant while being treated with NINLARO. In the U.S. general population, the estimated background risk of major birth defects and miscarriage in clinically recognized pregnancies is 2-4% and 15-20%, respectively. Animal Data: In an embryo-fetal development study in pregnant rabbits there were increases in fetal skeletal variations/abnormalities (caudal vertebrae, number of lumbar vertebrae, and full supernumerary ribs) at doses that were also maternally toxic (≥ 0.3 mg/kg). Exposures in the rabbit at 0.3 mg/kg were 1.9 times the clinical time averaged exposures at the recommended dose of 4 mg. In a rat dose range-finding embryo-fetal development study, at doses that were maternally toxic, there were decreases in fetal weights, a trend towards decreased fetal viability, and increased post-implantation losses at 0.6 mg/kg. Exposures in rats at the dose of 0.6 mg/kg was 2.5 times the clinical time averaged exposures at the recommended dose of 4 mg.8.2 Lactation: No data are available regarding the presence of NINLARO or its metabolites in human milk, the effects of the drug on the breast fed infant, or the effects of the drug on milk production. Because the potential for serious adverse reactions from NINLARO in breastfed infants is unknown, advise nursing women not to breastfeed during treatment with NINLARO and for 90 days after the last dose.8.3 Females and Males of Reproductive Potential: Contraception - Male and female patients of childbearing potential must use effective contraceptive measures during and for 90 days following treatment. Dexamethasone is known to be a weak to moderate inducer of CYP3A4 as well as other enzymes and transporters. Because NINLARO is administered with dexamethasone, the risk for reduced efficacy of contraceptives needs to be considered. Advise women using hormonal contraceptives to also use a barrier method of contraception. 8.4 Pediatric Use: Safety and effectiveness have not been established in pediatric patients.8.5 Geriatric Use: Of the total number of subjects in clinical studies of NINLARO, 55% were 65 and over, while 17% were 75 and over. No overall differences in safety or effectiveness were observed between these subjects and younger subjects, and other reported clinical experience has not identified
differences in responses between the elderly and younger patients, but greater sensitivity of some older individuals cannot be ruled out.8.6 Hepatic Impairment: In patients with moderate or severe hepatic impairment, the mean AUC increased by 20% when compared to patients with normal hepatic function. Reduce the starting dose of NINLARO in patients with moderate or severe hepatic impairment.8.7 Renal Impairment: In patients with severe renal impairment or ESRD requiring dialysis, the mean AUC increased by 39% when compared to patients with normal renal function. Reduce the starting dose of NINLARO in patients with severe renal impairment or ESRD requiring dialysis. NINLARO is not dialyzable and therefore can be administered without regard to the timing of dialysis10 OVERDOSAGE: There is no known specific antidote for NINLARO overdose. In the event of an overdose, monitor the patient for adverse reactions and provide appropriate supportive care.17 PATIENT COUNSELING INFORMATIONAdvise the patient to read the FDA-approved patient labeling (Patient Information).Dosing Instructions• Instruct patients to take NINLARO exactly as prescribed. • Advise patients to take NINLARO once a week on the same day and at
approximately the same time for the first three weeks of a four week cycle. • Advise patients to take NINLARO at least one hour before or at least two
hours after food. • Advise patients that NINLARO and dexamethasone should not be taken at the
same time, because dexamethasone should be taken with food and NINLARO should not be taken with food.
• Advise patients to swallow the capsule whole with water. The capsule should not be crushed, chewed or opened.
• Advise patients that direct contact with the capsule contents should be avoided. In case of capsule breakage, avoid direct contact of capsule contents with the skin or eyes. If contact occurs with the skin, wash thoroughly with soap and water. If contact occurs with the eyes, flush thoroughly with water.
• If a patient misses a dose, advise them to take the missed dose as long as the next scheduled dose is ≥ 72 hours away. Advise patients not to take a missed dose if it is within 72 hours of their next scheduled dose.
• If a patient vomits after taking a dose, advise them not to repeat the dose but resume dosing at the time of the next scheduled dose.
• Advise patients to store capsules in original packaging, and not to remove the capsule from the packaging until just prior to taking NINLARO.
Thrombocytopenia: Advise patients that they may experience low platelet counts (thrombocytopenia). Signs of thrombocytopenia may include bleeding and easy bruising.Gastrointestinal Toxicities: Advise patients they may experience diarrhea, constipation, nausea and vomiting and to contact their physician if these adverse reactions persist.Peripheral Neuropathy: Advise patients to contact their physicians if they experience new or worsening symptoms of peripheral neuropathy such as tingling, numbness, pain, a burning feeling in the feet or hands, or weakness in the arms or legs.Peripheral Edema: Advise patients to contact their physicians if they experience unusual swelling of their extremities or weight gain due to swelling.Cutaneous Reactions: Advise patients to contact their physicians if they experience new or worsening rashHepatotoxicity: Advise patients to contact their physicians if they experience jaundice or right upper quadrant abdominal painOther Adverse Reactions: Advise patients to contact their physicians if they experience signs and symptoms of acute febrile neutrophilic dermatosis (Sweet’s syndrome), Stevens-Johnson syndrome, transverse myelitis, posterior reversible encephalopathy syndrome, tumor lysis syndrome, and thrombotic thrombocytopenic purpura Pregnancy: Advise women of the potential risk to a fetus and to avoid becoming pregnant while being treated with NINLARO and for 90 days following the final dose. Advise women using hormonal contraceptives to also use a barrier method of contraception. Advise patients to contact their physicians immediately if they or their female partner become pregnant during treatment or within 90 days of the final dose.Concomitant Medications: Advise patients to speak with their physicians about any other medication they are currently taking and before starting any new medications.
Please see full Prescribing Information for NINLARO at NINLARO-hcp.com.
All trademarks are the property of their respective owners. ©2017 Millennium Pharmaceuticals, Inc., a wholly owned subsidiary of Takeda Pharmaceutical Company Limited. All rights reserved.
AUG 2018 MAT-US-IXA-18-00350
T:7”
T:10”
IXAZ18CDNY6401_Brief_Summary_A_Size_r3.indd 2 8/13/18 6:55 PM
IXAZ17CDNY2641_FALL FCS_2018_King_BS_r5.indd 2 8/23/18 12:31 PM

BRIEF SUMMARY OF PRESCRIBING INFORMATIONNINLARO (ixazomib) capsules, for oral use
1 INDICATIONNINLARO (ixazomib) is indicated in combination with lenalidomide and dexamethasone for the treatment of patients with multiple myeloma who have received at least one prior therapy.
5 WARNINGS AND PRECAUTIONS5.1 Thrombocytopenia: Thrombocytopenia has been reported with NINLARO with platelet nadirs typically occurring between Days 14-21 of each 28-day cycle and recovery to baseline by the start of the next cycle. Three percent of patients in the NINLARO regimen and 1% of patients in the placebo regimen had a platelet count ≤ 10,000/mm3 during treatment. Less than 1% of patients in both regimens had a platelet count ≤ 5000/mm3 during treatment. Discontinuations due to thrombocytopenia were similar in both regimens (< 1% of patients in the NINLARO regimen and 2% of patients in the placebo regimen discontinued one or more of the three drugs).The rate of platelet transfusions was 6% in the NINLARO regimen and 5% in the placebo regimen. Monitor platelet counts at least monthly during treatment with NINLARO. Consider more frequent monitoring during the first three cycles. Manage thrombocytopenia with dose modifications and platelet transfusions as per standard medical guidelines.5.2 Gastrointestinal Toxicities: Diarrhea, constipation, nausea, and vomiting, have been reported with NINLARO, occasionally requiring use of antidiarrheal and antiemetic medications, and supportive care. Diarrhea was reported in 42% of patients in the NINLARO regimen and 36% in the placebo regimen, constipation in 34% and 25%, respectively, nausea in 26% and 21%, respectively, and vomiting in 22% and 11%, respectively. Diarrhea resulted in discontinuation of one or more of the three drugs in 1% of patients in the NINLARO regimen and < 1% of patients in the placebo regimen. Adjust dosing for Grade 3 or 4 symptoms.5.3 Peripheral Neuropathy: The majority of peripheral neuropathy adverse reactions were Grade 1 (18% in the NINLARO regimen and 14% in the placebo regimen) and Grade 2 (8% in the NINLARO regimen and 5% in the placebo regimen). Grade 3 adverse reactions of peripheral neuropathy were reported at 2% in both regimens; there were no Grade 4 or serious adverse reactions. The most commonly reported reaction was peripheral sensory neuropathy (19% and 14% in the NINLARO and placebo regimen, respectively). Peripheral motor neuropathy was not commonly reported in either regimen (< 1%). Peripheral neuropathy resulted in discontinuation of one or more of the three drugs in 1% of patients in both regimens. Patients should be monitored for symptoms of neuropathy. Patients experiencing new or worsening peripheral neuropathy may require dose modification.5.4 Peripheral Edema: Peripheral edema was reported in 25% and 18% of patients in the NINLARO and placebo regimens, respectively. The majority of peripheral edema adverse reactions were Grade 1 (16% in the NINLARO regimen and 13% in the placebo regimen) and Grade 2 (7% in the NINLARO regimen and 4% in the placebo regimen).Grade 3 peripheral edema was reported in 2% and 1% of patients in the NINLARO and placebo regimens, respectively. There was no Grade 4 peripheral edema reported. There were no discontinuations reported due to peripheral edema. Evaluate for underlying causes and provide supportive care, as necessary. Adjust dosing of dexamethasone per its prescribing information or NINLARO for Grade 3 or 4 symptoms.5.5 Cutaneous Reactions: Rash was reported in 19% of patients in the NINLARO regimen and 11% of patients in the placebo regimen. The majority of the rash adverse reactions were Grade 1 (10% in the NINLARO regimen and 7% in the placebo regimen) or Grade 2 (6% in the NINLARO regimen and 3% in the placebo regimen). Grade 3 rash was reported in 3% of patients in the NINLARO regimen and 1% of patients in the placebo regimen. There were no Grade 4 or serious adverse reactions of rash reported. The most common type of rash reported in both regimens included maculo-papular and macular rash. Rash resulted in discontinuation of one or more of the three drugs in < 1% of patients in both regimens. Manage rash with supportive care or with dose modification if Grade 2 or higher.5.6 Hepatotoxicity: Drug-induced liver injury, hepatocellular injury, hepatic steatosis, hepatitis cholestatic and hepatotoxicity have each been reported in < 1% of patients treated with NINLARO. Events of liver impairment have been reported (6% in the NINLARO regimen and 5% in the placebo regimen). Monitor hepatic enzymes regularly and adjust dosing for Grade 3 or 4 symptoms.5.7 Embryo-Fetal Toxicity: NINLARO can cause fetal harm when administered to a pregnant woman based on the mechanism of action and findings in animals. There are no adequate and well-controlled studies in pregnant women using NINLARO. Ixazomib caused embryo-fetal toxicity in pregnant rats and rabbits at doses resulting in exposures that were slightly higher than those observed in patients receiving the recommended dose.
Females of reproductive potential should be advised to avoid becoming pregnant while being treated with NINLARO. If NINLARO is used during pregnancy or if the patient becomes pregnant while taking NINLARO, the patient should be apprised of the potential hazard to the fetus. Advise females of reproductive potential that they must use effective contraception during treatment with NINLARO and for 90 days following the final dose. Women using hormonal contraceptives should also use a barrier method of contraception.
6 ADVERSE REACTIONSThe following adverse reactions are described in detail in other sections of the prescribing information:• Thrombocytopenia [see Warnings and Precautions (5.1)]• Gastrointestinal Toxicities [see Warnings and Precautions (5.2)]• Peripheral Neuropathy [see Warnings and Precautions (5.3)]• Peripheral Edema [see Warnings and Precautions (5.4)]• Cutaneous Reactions [see Warnings and Precautions (5.5)]• Hepatotoxicity [see Warnings and Precautions (5.6)]
6.1 CLINICAL TRIALS EXPERIENCEBecause clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.The safety population from the randomized, double-blind, placebo-controlled clinical study included 720 patients with relapsed and/or refractory multiple myeloma, who received NINLARO in combination with lenalidomide and dexamethasone (NINLARO regimen; N=360) or placebo in combination with lenalidomide and dexamethasone (placebo regimen; N=360). The most frequently reported adverse reactions (≥ 20%) in the NINLARO regimen and greater than the placebo regimen were diarrhea, constipation, thrombocytopenia, peripheral neuropathy, nausea, peripheral edema, vomiting, and back pain. Serious adverse reactions reported in ≥ 2% of patients included thrombocytopenia (2%) and diarrhea (2%). For each adverse reaction, one or more of the three drugs was discontinued in ≤ 1% of patients in the NINLARO regimen.Table 4: Non-Hematologic Adverse Reactions Occurring in ≥ 5% of Patients with a ≥ 5% Difference Between the NINLARO Regimen and the Placebo Regimen (All Grades, Grade 3 and Grade 4)
NINLARO + Lenalidomide and Dexamethasone
N=360
Placebo + Lenalidomide and Dexamethasone
N=360
System Organ Class / Preferred Term N (%) N (%)
All Grade 3
Grade 4 All Grade
3Grade
4
Infections and infestationsUpper respiratory tract infection 69 (19) 1 (< 1) 0 52 (14) 2 (< 1) 0
Nervous system disordersPeripheral neuropathies* 100 (28) 7 (2) 0 77 (21) 7 (2) 0
Gastrointestinal disordersDiarrheaConstipationNauseaVomiting
151 (42)122 (34)92 (26)79 (22)
22 (6)1 (< 1)6 (2)4 (1)
0000
130 (36)90 (25)74 (21)38 (11)
8 (2)1 (< 1)
02 (< 1)
0000
Skin and subcutaneous tissue disorders
Rash* 68 (19) 9 (3) 0 38 (11) 5 (1) 0
Musculoskeletal and connective tissue disorders
Back pain 74 (21) 2 (< 1) 0 57 (16) 9 (3) 0
General disorders and administration site conditions
Edema peripheral 91 (25) 8 (2) 0 66 (18) 4 (1) 0
Note: Adverse reactions included as preferred terms are based on MedDRA version 16.0. *Represents a pooling of preferred terms
(Continued on next page)
T:7”
T:10”
IXAZ18CDNY6401_Brief_Summary_A_Size_r3.indd 1 8/13/18 6:55 PM
IXAZ17CDNY2641_FALL FCS_2018_King_BS_r5.indd 1 8/23/18 12:31 PM
Brief Summary (cont’d)
Table 5: Thrombocytopenia and Neutropenia (pooled adverse event and laboratory data)
NINLARO + Lenalidomide and Dexamethasone
N=360
Placebo + Lenalidomide and Dexamethasone
N=360
N (%) N (%)
Any Grade Grade 3-4 Any Grade Grade 3-4
Thrombocytopenia 281 (78) 93 (26) 196 (54) 39 (11)
Neutropenia 240 (67) 93 (26) 239 (66) 107 (30)
Herpes ZosterHerpes zoster was reported in 4% of patients in the NINLARO regimen and 2% of patients in the placebo regimen. Antiviral prophylaxis was allowed at the physician’s discretion. Patients treated in the NINLARO regimen who received antiviral prophylaxis had a lower incidence (< 1%) of herpes zoster infection compared to patients who did not receive prophylaxis (6%).Eye DisordersEye disorders were reported with many different preferred terms but in aggregate, the frequency was 26% in patients in the NINLARO regimen and 16% of patients in the placebo regimen. The most common adverse reactions were blurred vision (6% in the NINLARO regimen and 3% in the placebo regimen), dry eye (5% in the NINLARO regimen and 1% in the placebo regimen), and conjunctivitis (6% in the NINLARO regimen and 1% in the placebo regimen). Grade 3 adverse reactions were reported in 2% of patients in the NINLARO regimen and 1% in the placebo regimen.The following serious adverse reactions have each been reported at a frequency of < 1%: acute febrile neutrophilic dermatosis (Sweet’s syndrome), Stevens-Johnson syndrome, transverse myelitis, posterior reversible encephalopathy syndrome, tumor lysis syndrome, and thrombotic thrombocytopenic purpura. 7 DRUG INTERACTIONS7.1 Strong CYP3A Inducers: Avoid concomitant administration of NINLARO with strong CYP3A inducers (such as rifampin, phenytoin, carbamazepine, and St. John’s Wort).8 USE IN SPECIFIC POPULATIONS8.1 Pregnancy: Risk Summary: Based on its mechanism of action and data from animal reproduction studies, NINLARO can cause fetal harm when administered to a pregnant woman. There are no human data available regarding the potential effect of NINLARO on pregnancy or development of the embryo or fetus. Ixazomib caused embryo-fetal toxicity in pregnant rats and rabbits at doses resulting in exposures that were slightly higher then those observed in patients receiving the recommended dose. Advise women of the potential risk to a fetus and to avoid becoming pregnant while being treated with NINLARO. In the U.S. general population, the estimated background risk of major birth defects and miscarriage in clinically recognized pregnancies is 2-4% and 15-20%, respectively. Animal Data: In an embryo-fetal development study in pregnant rabbits there were increases in fetal skeletal variations/abnormalities (caudal vertebrae, number of lumbar vertebrae, and full supernumerary ribs) at doses that were also maternally toxic (≥ 0.3 mg/kg). Exposures in the rabbit at 0.3 mg/kg were 1.9 times the clinical time averaged exposures at the recommended dose of 4 mg. In a rat dose range-finding embryo-fetal development study, at doses that were maternally toxic, there were decreases in fetal weights, a trend towards decreased fetal viability, and increased post-implantation losses at 0.6 mg/kg. Exposures in rats at the dose of 0.6 mg/kg was 2.5 times the clinical time averaged exposures at the recommended dose of 4 mg.8.2 Lactation: No data are available regarding the presence of NINLARO or its metabolites in human milk, the effects of the drug on the breast fed infant, or the effects of the drug on milk production. Because the potential for serious adverse reactions from NINLARO in breastfed infants is unknown, advise nursing women not to breastfeed during treatment with NINLARO and for 90 days after the last dose.8.3 Females and Males of Reproductive Potential: Contraception - Male and female patients of childbearing potential must use effective contraceptive measures during and for 90 days following treatment. Dexamethasone is known to be a weak to moderate inducer of CYP3A4 as well as other enzymes and transporters. Because NINLARO is administered with dexamethasone, the risk for reduced efficacy of contraceptives needs to be considered. Advise women using hormonal contraceptives to also use a barrier method of contraception. 8.4 Pediatric Use: Safety and effectiveness have not been established in pediatric patients.8.5 Geriatric Use: Of the total number of subjects in clinical studies of NINLARO, 55% were 65 and over, while 17% were 75 and over. No overall differences in safety or effectiveness were observed between these subjects and younger subjects, and other reported clinical experience has not identified
differences in responses between the elderly and younger patients, but greater sensitivity of some older individuals cannot be ruled out.8.6 Hepatic Impairment: In patients with moderate or severe hepatic impairment, the mean AUC increased by 20% when compared to patients with normal hepatic function. Reduce the starting dose of NINLARO in patients with moderate or severe hepatic impairment.8.7 Renal Impairment: In patients with severe renal impairment or ESRD requiring dialysis, the mean AUC increased by 39% when compared to patients with normal renal function. Reduce the starting dose of NINLARO in patients with severe renal impairment or ESRD requiring dialysis. NINLARO is not dialyzable and therefore can be administered without regard to the timing of dialysis10 OVERDOSAGE: There is no known specific antidote for NINLARO overdose. In the event of an overdose, monitor the patient for adverse reactions and provide appropriate supportive care.17 PATIENT COUNSELING INFORMATIONAdvise the patient to read the FDA-approved patient labeling (Patient Information).Dosing Instructions• Instruct patients to take NINLARO exactly as prescribed. • Advise patients to take NINLARO once a week on the same day and at
approximately the same time for the first three weeks of a four week cycle. • Advise patients to take NINLARO at least one hour before or at least two
hours after food. • Advise patients that NINLARO and dexamethasone should not be taken at the
same time, because dexamethasone should be taken with food and NINLARO should not be taken with food.
• Advise patients to swallow the capsule whole with water. The capsule should not be crushed, chewed or opened.
• Advise patients that direct contact with the capsule contents should be avoided. In case of capsule breakage, avoid direct contact of capsule contents with the skin or eyes. If contact occurs with the skin, wash thoroughly with soap and water. If contact occurs with the eyes, flush thoroughly with water.
• If a patient misses a dose, advise them to take the missed dose as long as the next scheduled dose is ≥ 72 hours away. Advise patients not to take a missed dose if it is within 72 hours of their next scheduled dose.
• If a patient vomits after taking a dose, advise them not to repeat the dose but resume dosing at the time of the next scheduled dose.
• Advise patients to store capsules in original packaging, and not to remove the capsule from the packaging until just prior to taking NINLARO.
Thrombocytopenia: Advise patients that they may experience low platelet counts (thrombocytopenia). Signs of thrombocytopenia may include bleeding and easy bruising.Gastrointestinal Toxicities: Advise patients they may experience diarrhea, constipation, nausea and vomiting and to contact their physician if these adverse reactions persist.Peripheral Neuropathy: Advise patients to contact their physicians if they experience new or worsening symptoms of peripheral neuropathy such as tingling, numbness, pain, a burning feeling in the feet or hands, or weakness in the arms or legs.Peripheral Edema: Advise patients to contact their physicians if they experience unusual swelling of their extremities or weight gain due to swelling.Cutaneous Reactions: Advise patients to contact their physicians if they experience new or worsening rashHepatotoxicity: Advise patients to contact their physicians if they experience jaundice or right upper quadrant abdominal painOther Adverse Reactions: Advise patients to contact their physicians if they experience signs and symptoms of acute febrile neutrophilic dermatosis (Sweet’s syndrome), Stevens-Johnson syndrome, transverse myelitis, posterior reversible encephalopathy syndrome, tumor lysis syndrome, and thrombotic thrombocytopenic purpura Pregnancy: Advise women of the potential risk to a fetus and to avoid becoming pregnant while being treated with NINLARO and for 90 days following the final dose. Advise women using hormonal contraceptives to also use a barrier method of contraception. Advise patients to contact their physicians immediately if they or their female partner become pregnant during treatment or within 90 days of the final dose.Concomitant Medications: Advise patients to speak with their physicians about any other medication they are currently taking and before starting any new medications.
Please see full Prescribing Information for NINLARO at NINLARO-hcp.com.
All trademarks are the property of their respective owners. ©2017 Millennium Pharmaceuticals, Inc., a wholly owned subsidiary of Takeda Pharmaceutical Company Limited. All rights reserved.
AUG 2018 MAT-US-IXA-18-00350
T:7”
T:10”
IXAZ18CDNY6401_Brief_Summary_A_Size_r3.indd 2 8/13/18 6:55 PM
IXAZ17CDNY2641_FALL FCS_2018_King_BS_r5.indd 2 8/23/18 12:31 PM
22 FCS The Magazine
I t started with a noble goal: Make sure low-income and uninsured patients have access to quality healthcare by helping hospitals provide care and recoup some of the losses they incur.
How? By requiring drug manufacturers who participate in the Medicaid program to sell outpatient drugs at discount to qualifying hospitals and other providers.
The 340B Drug Pricing Program, established by Congress in 1992, has provided access to medicines and healthcare for people who otherwise might not be able to afford them. However, a lack of reporting requirements, clear parameters and oversight authority have created a situation in which the patients in the program its supposed to serve have fewer treatment options, and those options often come at a higher cost. At the same time, it gives qualifying hospitals an unfair advantage in the healthcare marketplace over community-based providers, particularly in cancer treatment.
“340B had good intentions, to help hospitals treating indigent patients,” said Brad Prechtl, CEO of FCS. “But it has morphed into a program in which the hospitals get the benefits with all their patients, whether they’re paying or indigent. In our opinion, it’s a very unfair system.”
According to a two-year study released in January by the U.S. House of Representatives’ Energy and Commerce Subcommittee on Oversight and Investigations: “Covered entities can purchase medicines at 340B prices for patients that have insurance, entities can also use the program to generate ‘340B revenue.’”
Simply put, some hospitals buy the medicine at the pharmaceutical discount but collect the full price from the patient’s insurance company.
“Cancer drugs are much more expensive than most other medications,” said Dr. Michael Diaz, Director of Patient Advocacy for both FCS and the Florida Society of Clinical Oncology. “Cancer patients require more intense care to manage the symptoms and the side effects of treatment.”
The growth of the 340B Program has resulted in higher costs for all cancer drugs because the pharmaceutical companies are required to pay higher rebates to the 340B facilities, he said.
The House study also noted a trend of hospitals buying private oncology clinics and increasing the cost of care for the patient through facility fees, “even though the treatment that the patient receives has not changed.” Numerous studies have shown that treatment in hospitals historically has been much
more expensive than in clinics and physicians’ offices. With fewer clinics available to treat patients, the cost of treatment is more likely to increase.
Earlier this year, a U.S. District Court upheld a decision by the Centers for Medicare and Medicaid Services to reduce the supplemental reimbursement rate to 340B hospitals and surgical centers. It’s a good start, Prechtl said. “It closes the gap.”
Prechtl is concerned about the adverse effect the uneven playing field could have on patient care, especially community-based care such as FCS’s model, in which patients are treated close to home with family and friends nearby for support. Primary care and specialist physicians employed by a 340B health system might feel pressured to refer their patients to a 340B facility; however, given that the hospital gets paid more from commercial carriers than a community-based practice does due to the reimbursement structures, this costs
the healthcare insurer. It also causes the patient greater exposure to costs through higher co-pays and out-
of-pocket costs. In addition, traveling to the closest 340B facility could place increased stress on the
patient as it may not be very close to their home.
“These 340B hospitals aren’t found on every corner like a CVS or a Walgreens,” Prechtl said. “The closest one might be two hours’ drive away.”
A recent study by the Berkeley Research Group documented the shift
in oncology care from physicians’ offices to hospitals over the past 10 years. The
study, “The Oncology Drug Marketplace: Trends in Discounting and Site of Care,”
found the percentage of Medicare Part B claims for chemotherapy drug administration in a hospital
outpatient setting increased from 23 percent in 2008 to almost 50 percent in 2016. Hospitals with 340B certification accounted for 38 percent of Medicare Part B hospital oncology drug reimbursement in 2008; by 2016, it had increased to 67 percent.
The researchers concluded that the increase in profit margins with drugs purchased at 340B discount has created “substantial financial incentives for 340B hospitals to expand oncology services, despite overall healthcare costs increasing as a result of this shift in site of care.”
Multiple bills have been introduced in both the House and the Senate calling for facilities’ detailed accounting of program use and for adequate oversight.
“The 340B program has been misused by some,” Diaz said. “We need to ensure it’s being used for the patients who need it.”
FCSFeature
Plan B for 340BChange Needed For Drug Program So It Can Help Those Who Need It MostBY AUDREY POST

Your best choice for quality cancer care. We are Florida Cancer Specialists. As the largest independent community oncology and hematology practice in the U.S., we provide more care to
more patients in more communities across Florida than any other cancer treatment organization. Our patients trust
us and would recommend us to friends and family — awarding us a world-class Net Promoter Score exceeding
87%, putting us among the top customer-centric companies worldwide. We’ve been selected as a participating
vendor in the value-based programs for Oncology Care Model, United Healthcare and Cigna, as well as a Blue
Distinction Center for Cancer Care, recognized for our higher-quality care and improved patient outcomes.
These distinctions, along with cutting-edge technologies and innovative clinical trials, allow us to do what we
do best every day: provide world-class, compassionate care to our patients.
See how we’ve been leading the fi ght against cancer for over 30 years at FLCancer.com
100LOCATIONS
NEARLY
Scores above 75% are exceptional
110+NATIONAL
CLINICAL TRIALSPHASE 1, 2 & 3
ACCESS TO
72,000NEW PATIENTS
TREATED THIS YEAR
87%PATIENT SATISFACTION:
EARNED NET PROMOTER SCORE OF
1THE ONLY COMMUNITY ONCOLOGY PRACTICE RECOGNIZED AS A BLUE DISTINCTION CENTER FOR CANCER CARE IN FLORIDA
World-Class Medicine. Hometown Care. Where Hope is
Powered by ScienceTM

24 FCS The Magazine
COVER STORY
FCS patient, Roger Vergin, and wife Rosemary continue to overcome any hurdle.

Fall 2018 25
Cool RunningFCS Helps Roger Vergin Get His Life Back on TrackBY ROB RUSHIN
When he reached retirement age, Roger Vergin reflected on his full and varied life to date. He served on faculty at some of the nation’s finest universities, including University of California-
Berkeley, the University of Washington and Penn State. He was a successful financial planner and trusted advisor to numerous clients, including a stint as Marlon Brando’s advisor. Roger’s wife, Rosemary, could look back with similar satisfaction, earning her Ph.D. in history and establishing herself as an expert in family history research.
Retirement age came and went, but the two of them did not slow down. At age 70, Roger took up masters track and field competitions, and he excelled in every event. It quickly became apparent to his rivals that whenever Roger showed up, everyone else had to battle for second place. Nothing could stop him, and then came the chest pain.
Emergency room physicians decided his gallbladder needed to be removed, but his wife, Rosemary sensed something more was wrong, so she scoured the Internet trying to pinpoint Roger’s symptoms. She reached out to a doctor friend who told her point blank: Get Roger out of there and go see Dr. William (Bill) Harwin at Florida Cancer Specialists (FCS).
“Rosemary checked me out of the hospital in the morning,” Roger said. “They practically tried to shanghai me into surgery.”
President Emeritus & Founder, Dr. Bill Harwin suspected a rare hematologic condition called essential thrombocythemia that causes overproduction of blood platelets in the bone marrow. These cells can cluster in vital organs and create blood clots. During the initial visit, Dr. Harwin reached out to an old friend and colleague from University of Florida, Dr. Craig Kitchens, a former P/T doctor with FCS. The Head of Hematology at Shands, Kitchens is the man who literally wrote the book on bleeding and clotting disorders, and he helped Dr. Harwin’s team confirm the diagnosis and initiate an ongoing treatment that had Roger back on the track in a little over a month. To this day, he maintains a daily regimen to keep the clots at bay.
Roger’s ailment was not a blood cancer; however through FCS’s hematology connections, the team was uniquely suited to
recognize his symptoms and get him back on track. Dr. Harwin’s ability to consult with top physicians such as Dr. Kitchens made Vergin’s decision to go to FCS the best possible choice.
“He said, ‘It’s a good thing you didn’t have that surgery, because with the clots in your two organs already, there’s a good chance you wouldn’t have survived the procedure.’ I would not have lived,” he said. “So, you can see what I think of the treatment I got from Dr. Bill Harwin and FCS. They literally saved my life.”
A few years later, Rosemary had her turn under Dr. Harwin’s care. After noticing a hard breast lump one evening, she and Roger again turned to FCS for care. Dr. Harwin diagnosed an aggressive form of cancer. Again, the FCS team took an innovative approach that placed chemotherapy before surgery. Rosemary was unsure.
“The first thing a woman thinks when she finds out she has breast cancer is get it out, get it out,” she said. “But he convinced me to wait and do the chemo first.”
And?“I ended up with no cancer anywhere. Dr. Harwin ran
down the hallway shouting, ‘Rosemary, you have a complete pathologic response,’ which is the best response you could have. That’s a thrilling moment that will live in my memory forever,” Rosemary said. “He really saved my life.”
Today, both Vergins are doing great. Roger’s medications control his blood platelets, and Rosemary has been cancer-free for three years. She still works 10 hours per day for her genealogy clients. “I love it! I’m having a lot of fun,” she says.
As for Roger, he has continued his domination of the masters track and field world.
Before this interview, the couple had just returned from the Colorado Association and Mid-America Region Masters and Open Indoor Track and Field Championship. I asked him about competing at that elevation.
“Oh, that was a bit different,” he says. “Not quite so much oxygen there, but I did five events and won all five. I set records in all five of them for the mid-America region. So it was a pretty good accomplishment to break all those records.”
By the way, Roger turned 81 in August of 2018. That’s more than “pretty good.”

26 FCS The Magazine
FCSFeature
Daniel F. Hayes, MD, FACP, FASCO
Pearls of Wisdom’ for Leadership and Success in Academic Medicine Gathered Over a 35-Year CareerBY DANIEL F. HAYES, MD, FACP, FASCO REPRINTED WITH PERMISSION BY THE ASCO POST
As I complete my three-year term as ASCO President, I am stimulated to relay thoughts on “pearls of wisdom” I have picked up over the years about leadership and success, particularly
in academic medicine. Those of you who follow the commentaries of Joseph V. Simone, MD, will immediately ascertain that this sort of navel-gazing is not original. Indeed, Simone’s Maxims, first published in 1999 and now updated and expanded, has been one of the most read, and inspiring, tomes in my library for nearly two decades.
I have been educated, trained, or worked as a faculty member in five different institutions over the past 35 years.
I have witnessed visionary leadership and incredibly successful individuals in science, education, and clinical care. However, I have also had the opposite experience. The pearls of wisdom listed here are mostly my observations of those who have trained or mentored me over the years and the impact their influence has had on my career.
I have tried to cite the specific author for each “pearl” but may at times have it incorrect or the author may be unknown to me. Regardless, I hope these 35 statements about leadership are helpful to those considering a career in academia or to those who have themselves become leaders in the field of oncology.

Fall 2018 27
FCSFeature
Leadership
1. Leaders lead. Credit Allen S. Lichter, MD, FASCO, former ASCO Chief Executive Officer. What does he mean by that? Know what you want, have vision, listen to others, and seek advice, but ultimately—especially in a tense situation—take the reins and lead.
2. Make the call. Credit unknown, but the point is analogous to a call from a baseball umpire: Look at the situation in question, assess it, seek advice from others, sum it up in your mind, be confident of what you saw and what you think should be done, and then “make the call.” Indecision can paralyze a program or institution and lead to divisiveness and chaos. Sometimes you will make the wrong call, but don’t reverse your decision unless you are sure it was a mistake.
3. Plan for a Rolls Royce, but build what you can afford. Credit me, through a massive amount of advice from many of my former mentors. This pearl includes several elements, including: • Vision. What do you want your program, division,
department, cancer center, or society to look like in 5 years? Too often, leaders let their program grow by diffusion or paths of least resistance. That’s not always bad—some of my best recruits came to me by accident—but, generally, it’s better to have an idea of what you want and then go out and get it.
• A strategic plan. Dream big. Put your idea on paper. You do not have to show it to anyone, but have it where you can access it when you are ready to implement your plan.
• Prioritization. Know what you can and cannot do, and understand the available resources at your disposal. Once you have prioritized your ideas and built the blueprint to implement them, you can add to it as more resources become available.
• Development of tactics. Set up each of your priorities with a timeline, and write it down. But be sure to constantly review and assess your progress.
• Generation of metrics. Let’s face it: Most academic leaders are scientists, and scientists like data. Once you have developed a business plan based on your vision, strategic plan, priorities, and tactics, as in a clinical protocol, be prepared to measure what you have accomplished, including whether you have met your objectives, endpoints, and assumptions for success or failure.
“Know what you want, have vision, listen to others, and seek advice, but ultimately—especially in a tense situation—take the reins and lead.
-Daniel F. Hayes, MD, FACP, FASCO
4. When you are recruited for a new position, or when you recruit someone to a new position, there are three critical elements to keep in mind for success. I’m not sure who said this, but I’ve found these elements helpful: • Responsibility. Know what the job entails. Don’t let anyone
tell you “titles are not important.” They are, in fact, essential to success. Good will from your boss, although
helpful and good to have, won’t make you or your recruits successful. Knowing what your boss expects of you, or what you expect from the staff you are recruiting, will help you avoid serious problems in the future.
• Authority. Ask yourself, “What authority do I or my recruit have to ensure that our vision is executed successfully?” If you lack the authority behind the title you were given, you will get nothing done.
• Resources. Will you get, or give, the resources to accomplish your vision once you have been given the responsibility and authority to do so? If not, run, don’t walk, away from the deal.
5. Growth happens continuously; administrators think incrementally. Credit me. If you lead or direct a program that requires resources, you’ll outgrow whatever you were given, so ask for more than you need upfront, and outfox your administrative boss.
6. Do not give young people enough rope to hang themselves. Credit me. I cannot tell you how often I’ve seen bright, young, ambitious fellows or faculty members see “greener pastures” in a new job offer only to learn later that way too much is expected of them, and they soon burn out. The best advice I ever received when I was starting my career came from my faculty leaders at Dana-Farber Cancer Institute, George P. Canellos, MD, and Robert J. Mayer, MD, who said, “If you think you’re getting impressive offers now, wait 5 years and you won’t believe what you’ll be offered after you’ve actually accomplished something!”
7. The hardest part about being a resident is not being an intern. Credit me. Don’t micromanage your staff. Learn to delegate responsibilities to trusted individuals, and then let them fulfill those responsibilities.
“Don’t micromanage your staff. Learn to delegate responsibilities to trusted individuals, and then let them fulfill those responsibilities.”
— Daniel F. Hayes, MD, FACP, FASCO
Science
8. Challenge dogma. Credit me. Craig Henderson, MD, Adjunct Professor in the Department of Medicine at the University of California, San Francisco, my clinical and research mentor when I was a fellow and who continues to mentor me today. I will never forget Dr. Henderson asking, “Why are academics so dogmatic? The whole point of being an academic is to challenge what we think we know.” As a breast cancer oncologist, I constantly sing the praises of the surgeons from the 1960s, including Bernard Fisher, MD, and Umberto Veronesi, MD, among others, who challenged the Halstedian dogma of aggressive breast surgery passed down through the decades. Beyond courageous, they changed many paradigms in how we treat breast cancer and improved care for patients. We should all strive to be like them.

28 FCS The Magazine
9. Luck is not a good strategy in golf or science. Credit me. It’s important to recognize good luck when it happens, but one cannot count on being lucky in life. For success in research, plan your laboratory or clinical experiments carefully, and don’t just hope you’ll get lucky. This pearl of wisdom is particularly relevant to tumor biomarker studies, in which so many investigators pull specimens out of a freezer, run an assay, put the results together with clinical outcomes, see some interesting data, and then ask themselves, “What was the question?”
10. Appreciate good luck when you get it, and be flexible. Credit numerous people. We wouldn’t have penicillin if Scottish physician-scientist Alexander Fleming, FRS, FRSE, FRCS, had thrown away his bacterial plates because the ongoing experiments were ruined by mold dripping on them. It’s important to stay focused, but be prepared to change course if necessary.
11. Plant lots of seeds, and see which ones grow. Credit the many farmers surrounding Shelbyville, Indiana, where I grew up. Although in academia one needs to stay modestly focused, clear-cutting a forest and planting all the same tree species is a game plan for disaster. This pearl has served me well in science. I have tried to stay focused in my work, but not so much on one issue that if it fails, I have nothing else to do.
“I will never forget Dr. Henderson asking, ‘Why are academics so dogmatic? The whole point of being an academic is to challenge what we think we know.’”
— Daniel F. Hayes, MD, FACP, FASCO
12. Challenge your own study results (part 1), or don’t trust anyone who never publishes negative results. Credit me. I’m proud of having published several papers in which the reported study was a good idea, but the results didn’t bear out the hypothesis. When a fabulous hypothesis that I have developed is not supported by the data, I think of a phrase so often used in NASCAR racing: “That’s racing” or, in our world, “That’s science.”
13. Challenge your own study results (part 2), or maintain a sense of humility about your research findings. Credit Baruj Benacerraf, MD, a Nobel Laureate and President of the Dana-Farber Cancer Institute during the 1980s and 1990s. Dr. Benacerraf said, and I’m paraphrasing, “If it [your study results] is really good, someone else will tell you.”
14. Think like a physician/think like a scientist. Credit me, from lessons I’ve learned from my many mentors. At the end of every clinic day, there should be an important question to address scientifically, and at the end of every research day, there should be a clinical application to your study findings. This exercise is the epitome of translational research. Don’t write a research paper just to get promoted. Ask yourself, “So what? What do these results mean?” and think about how the results, positive or negative, might be applied to your patients’ care.
15. The hallmarks of a good clinical trial are the questions it has raised. Credit Dr. Fisher, Former Chair of the National Surgical Adjuvant Breast and Bowel Project. Don’t just walk away from your last laboratory or clinical experiment; use the result to design the next one.
16. A bad tumor marker is as bad as a bad drug. Credit me. As a second-year fellow, my mentor, Donald W. Kufe, MD, of Dana-Farber Cancer Institute, handed me a suite of monoclonal hybridomas and challenged me to find a circulating marker for breast cancer. I did find it, and it turned out to be CA15-3, which is now used worldwide to monitor patients with metastatic breast cancer. However, at the time, I assumed that, as with new drug development, there must be rules for the development and introduction of a tumor biomarker into the clinic. I was mistaken. I got lucky with CA15-3, but I’ve made many mistakes in the field. Ultimately, I’ve learned that we need to be as rigorous with the diagnostics we use to guide our treatment strategies as we are with the treatments themselves.
17. When it comes to medicine, there is no distinction between “scientist” and “clinician.”Credit Dr. Henderson. There are basic scientists, translational scientists, and clinical scientists. Each one rigorously uses the scientific method to play an important role in understanding the biology of disease and translating research to improve clinical care. Don’t let anyone speak of “the scientists” and “the clinicians” as separate entities at your institution. Defend this turf!
Patient Care
18. Never talk a surgeon into performing surgery, a radiation oncologist into giving radiotherapy, or an airplane pilot into flying. Credit me. These folks love to do what they do, so listen very carefully when they offer cautionary recommendations.
19. No patient wants to be a great case (because that means you don’t know how to treat the patient) and no patient is a great case (he or she is a person whose case happens to be interesting to you). Credit Donald W. Seldin, MD, who died recently, but who, for decades, had been the Chairman of the Department of Medicine at what is now The University of Texas Southwestern Medical Center, including while I was a resident. During our morning reports, Dr. Seldin would admonish us for being enthusiastic about a “great case” and explain that patients with serious illnesses are scared and trust that we will do our best to care for them with compassion. It was okay to learn from these patients, but not to think of them as “cases.” To this day, I think of my patients as “patients,” not “cases,” and that keeps me grounded.
20. Don’t go home until you’ve returned phone messages from patients, their family members, or their physicians. Credit Dr. Canellos. Patients are anxious to learn what their test results show or their next plan for care. Don’t keep them waiting.
21. Think of every patient as your relative and treat him or her with the same care and respect you would accord a family member. Credit Gloria Smith, a nurse practitioner with whom I worked during my mid-career, who taught me more about patient care than my mentors.
Fall 2018 29
“Patients and their family members can become emotional, irrational, and even confrontational. If you respond in kind, it only escalates the situation.”
— Daniel F. Hayes, MD, FACP, FASCO
22. You should deal rationally with irrational people, including patients and their family members. Credit me. Patients and their families are often scared and may be uninformed or poorly informed about their cancer and its treatment; they can become emotional, irrational, and even confrontational. If you respond in kind, it escalates the situation. Engaging in rational, logical, and respectful discussions can usually resolve a negative situation.
23. The patient has cancer, you don’t. Credit my father, Robert E. Hayes, a businessman, and my personal experience. This pearl echoes Dad’s motto that “the customer is always right.” As stated earlier, justifiably, patients and their family members can become emotional, irrational, and even confrontational. If you respond in kind, it only escalates the situation. Rational, logical, and respectful discussions usually—but not always—resolve such situations. They also help the staff act accordingly. I’ve tried to instill in our staff that they are the face of our institution and that first impressions are usually the lasting ones. We all need to make patients feel confident they have chosen the right cancer center. It is our job to always be friendly, compassionate, and helpful.
Administration
24. If there’s no blood involved, most crises take care of themselves. Credit Dr. Henderson. What this means is, unless it really is a crisis, some delay in addressing it won’t hurt. Rather, stay focused on what you’re doing, and get the job done.
25. Make it easy to do right and hard to do wrong. Credit Elizabeth Hammond, MD, a pathologist at Intermountain Health Care in Salt Lake City and my long-time compatriot in improving tumor biomarker tests. Careful planning is required to deal with the propensity for human error in any task, and it is amazing to see how often this pearl is broken by hospital administrators. The clumsy integration
of electronic health records in medical institutions over the past decade is a classic example of what not to do.
26. Challenge the statement “This will only take a minute” at any meeting you attend. Credit Dr. Henderson. Dr. Henderson always made the point that almost every committee is formed to settle some grievous sentinel event. However, most committees continue to meet even after the problem is solved and are compelled to take action to solve other problems, often with the proviso that “this will only take a minute.” But over time, those minutes add up. Fight the urge to get drawn into these encounters.
“Don’t overreach and think you can do something you’re not trained to do or, worse, not capable of doing or don’t have the time to complete.”
— Daniel F. Hayes, MD, FACP, FASCO
General Behavior
27. If your desk is cleared when you go home at night, you’re not doing enough. Credit Dr. Henderson. I’ve always loved this one. My perpetually messy desk would please Dr. Henderson, since it suggests I’ve managed to keep busy over the past 35 years!
28. If you’re just showing up at work and are not passionate about what you are doing, think of something else to do. Credit (I think) Emil Frei III, MD, one of the fathers of our field and a trailblazer in the use of combination chemotherapy. I don’t know if he ever slept, but we never saw him idle or not thinking about the next potential cure for cancer.

30 FCS The Magazine
29. Even when you’re on the right track, if you don’t keep moving, you’ll get run over. Credit American humorist Will Rogers.
30. Give yourself 24 hours to mope over a rejected paper or grant, and then get back to work.Credit Dr. Kufe. I’ve always loved this pearl. It’s gotten me through several crushing defeats.
31. Know yourself. Credit all of us, but in particular, Laurence J. Peter, who formulated the Peter Principle, an observation that in a hierarchy, people tend to rise to “their level of incompetence.” Don’t overreach and think you can do something you’re not trained to do or, worse, not capable of doing or don’t have the time to complete.
32. Do the unpleasant things in your day first, then do what you like to do. Credit Robert E. Hayes. My father’s point is that putting off unpleasant or disagreeable tasks doesn’t make them less unpleasant or less disagreeable, so get them done early.
33. Don’t be selfish. Credit Dr. Canellos. Your students’, fellows’, lab technicians’, postdoctoral fellows’, mentees’, or colleagues’ success is your success. During his ASCO Presidential Address, Dr. Canellos said, “My greatest clinical trial results are the fellows I have trained.” What he meant is that mentoring was as meaningful to the advancement of medicine as his own research contributions. I hope my trainees recognize that I feel the same way.
34. Talk with someone you respect who is not in medicine or science. Credit Jane Hayes, my wife, best friend, and confidante. She has a way of seeing how ridiculous we
can be, and she lets me know what is really important in any decision.
35. Behave with integrity, honesty, and respect for others. Credit my mother and father, Betsy R. and Robert E. Hayes. They were both lost to cancer over a decade ago, and I hope I’ve made them proud.
Acknowledgments: I would like to thank all of the mentors and colleagues I have quoted in this piece for both their wisdom and generosity. I would like to especially acknowledge Dr. Joseph Simone, who was very gracious with his time and comments in preparation of this piece. Finally, I want to acknowledge Dr. Donald W. Seldin, who died at the age of 97 on April 25, 2018. He will be sorely missed by the generations of medical students and internal medicine residents he trained and inspired.
Disclosure:Dr. Hayes owns stock in Oncimmune LLC, and Inbiomotion, is a consultant/advisor for Cepheid without compensation, is principal or co-investigor of sponsored clinical research for Merrimack Pharmaceuticals, Inc (Parexel International), Eli Lilly and Company, Menarini/Silicon Biosystems Veridex (Johnson & Johnson), Puma Biotechnology, Inc (subcontract Washington University, St. Louis, to University of Michigan), Pfizer, and AstraZeneca, and has received royalties from licensed technology from Janssen R&D (Johnson & Johnson).
Don’t be selfish.

Fall 2018 31FLCancer.com
Florida Cancer Specialists Pharmacy Operations department would like to give a BIG thank you to our valued sponsors of the 2018 Annual Pharmacy Trainers Conference that was held
for the Regional Pharmacy Trainers at the Hilton Hotel in West Palm Beach, Florida
World-Class Medicine. Hometown Care.
Thank YouTO THE SPONSORS OF THE
2018 Annual Pharmacy Trainers Conference

32 FCS The Magazine
Dr. David Wenk, son Kolbe, Chrissy Wenk (David’s wife), and daughters Abby and Lily.

Fall 2018 33
E ven as a high school student in New Jersey, Dr. David Wenk wanted to be a physician, but it was a Category 4 hurricane that led him to oncology.
In mid-August of 2004, Wenk was in the second month of his residency at the Moffitt Cancer Center located in Tampa, Florida. Hurricane Charley had just made landfall, devastating Port Charlotte and Punta Gorda.
“A lot of patients were displaced, many were stuck at Moffitt because they couldn’t get home,” Wenk says. “I really got to know quite a few patients, not just medically but from their personal stories.”
As he treated patients who were dealing with the dual tragedies of a cancer diagnosis and losing a home to the storm, Wenk, who had never been drawn to surgeries or procedural medicine, began to see more value in the doctor-patient relationship.
“I started realizing oncology also enabled a physician to really know your patients, understand their struggles, and form those special bonds that, unfortunately, you don’t see much anymore,” he says. “It’s absolutely the best job in the world.”
Wenk went on to complete a Fellowship in Oncology and Hematology at Moffitt and serve as a clinical faculty member in the Department of Medicine and Department of Blood and Marrow Transplantation. Today, he is part of the oncology team at Florida Cancer Specialists (FCS) in New Port Richey, holding American Board of Internal Medicine certifications in Medical Oncology, Hematology and Internal Medicine. He treats all hematologic and oncologic malignancies, as well as benign hematologic disorders.
At FCS, Wenk, whose team includes two Nurse Practitioners, is able to provide his patients with the personal attention that is so vital in cancer treatment.
“The patients know there is a team, so if I’m not available that day, they have multiple expert clinicians involved in their care,” he says. “The entire team, including the nurses, knows everyone by name.”
“With our patients, we are not just treating them, we are part of their family, and they actually see you more than a lot of their family members,” says Wenk, “I’ve been invited to several weddings!”
“When I tell a patient, ‘Look, I don’t need to see you for a couple of months,’ it’s almost like they’re sad,” he says. “I didn’t get it at first, but now I do. It becomes a family, which ultimately helps them get through the disease.”
DOCTOR SPOTLIGHT
“To give good care, you have to be up to date,” he says. “I go from prostate cancer, to breast cancer, to leukemia, to multiple myeloma, to pancreatic cancer, so you have to be up on everything.”
But the rapid changes are what make oncology such a satisfying field, added Wenk, who also recently joined FCS’ Executive Board.
“It’s got all the innovations,” he says, noting that many of the medications his patients rely on today didn’t exist 10 years ago. “Oncology is really the only field that’s changing. From a science standpoint, it’s unbelievably fascinating.”
The field’s demanding pace can be exhausting for physicians such as Wenk, who often find it difficult to step away from their work.
“The job, as much as you love it, it does, emotionally, beat you up,” he says. “I had a patient come in with stage-four lung cancer, I know the reality of the disease, but it still hurts at the end. What I’ve found is I need to periodically just get away.”
To recharge, the self-described “crazy, die-hard” Tampa Bay Buccaneers fan supports his team at home and also enjoys boating with his wife, Chrissy, and their three children: 4-year-old Lily, 3-year-old Abby and 5-month-old Kolbe.
Working so closely with patients who are fighting to stay alive has made Wenk far more mindful of the time he’s been given.
“It’s made me realize we have got to just live every day,” he says. “None of us are promised another day.”
Dr. Wenk’s Tampa Bay Buccaneers themed exam room at the New Port Richey location
Dr. David WenkFinding Joy and Hope in the Fight to Break Cancer’s GripBY KARI C. BARLOW

34 FCS The Magazine
OFFICE SPOTLIGHT
Dr. J. Wynn Sullivan

Fall 2018 35
F or too many living in Palatka, Florida, prior to 1994, cancer was a death sentence.
People in this little town with a population hovering around 10,000, situated about an hour from
Jacksonville, Florida, to the north and Gainesville, Florida, to the west, were often just living with cancer after being diagnosed, instead of seeking treatment.”
“They would just get diagnosed, and rather than going out of town for treatment, they would remain untreated,” explained Dr. J. Wynn Sullivan, Medical Oncologist at Florida Cancer Specialists’ (FCS) Palatka location.
Whether those with cancer didn’t have the resources to travel for treatment or just didn’t know where to go, Palatka was an underserved community.
On paper, Palatka appeared to be too small to support a cancer center, but Dr. Sullivan set up his practice there 25 years ago and is proud of the level of service he and his staff have provided, with the tremendous support from the community.
“I am most proud that we have brought cancer care to an area that didn’t have it,” Dr. Sullivan said. “I am proud of what we set up here and turned that around.
“We don’t just offer treatment to an area where nothing was available. We offer first-rate, full-on, can’t-do-better-anywhere-else type of cancer care.”
His practice offers medical oncology, hematology, infusion therapy, non-oncology infusions, imaging and an on-site lab. As a part of FCS, patients at the practice also have access to pathology, specialty pharmacy and more.
“I think our cancer center is out of proportion to the community. I think our equipment and our capability is beyond what most people would expect if they came to visit,” he said.
He credits his eight-person staff, who help serve about 100 patients per week and roughly 300 per month, for the success of this cancer center, which joined FCS in February 2018.
He explained that the patients come in with their families, not by themselves. They need to know they and the staff are all part of the same team. He said his staff is not afraid to bond with the patients and get to know them.
“When you get a cancer diagnosis, it’s kind of immersive.
As a provider of cancer treatment, you must do something to make that palatable, something to make it so they don’t dread coming here,” he said.
The staff is light-hearted, upbeat and genuinely interested in the lives and outside interests of patients.
“Part of the joy of this type of practice is getting to know people and being a part of the journey with them,” Dr. Sullivan said. “The staff spends a lot of time catching up with patients when they come in and they are very involved on a personal level. I think it makes a difference, and I think people appreciate it.”
“We don’t worry about separating the personal from the professional. I don’t think any of us worry about that.”
He said the environment created is part of why he became an Oncologist.
“We see the patients all the way through the treatment program and the follow-up,” Dr. Sullivan said. “We see patients a lot, not just once every few years or when they need a check-up, and we get to keep up with them. That is the biggest heal.”
Dr. Sullivan received his undergraduate degree in Microbiology at the University of Florida in Gainesville and received his Doctorate of Osteopathic Medicine at Nova Southeastern University. He finished his Residency and Fellowship at Jacksonville’s University of Florida Health Science Center, with training in Medical Oncology and Hematology.
“The patients found me,” he said. “Cancer patients are scrappy and they want to do something to get rid of their disease. During the normal course of training, I just fell in love with the oncology patients and the oncology clinic. I didn’t expect that. I was geared more towards other specialties and internal medicine.”
Dr. Sullivan received additional training from the U.S. Oncology Research in Good Clinical Practice (GCP). He is actively involved in the American Cancer Society, having served two terms as President, and he has over 30 years of clinical experience, including industry and network trials.
“The impact of learning about and treating cancer is one thing,” Sullivan says. “That’s not what got me into it. It was the patients themselves and that environment that got me hooked.”
Palatka OfficeBrings Cancer Care to the Formerly UnderservedBY KAREN MURPHY

36 FCS The Magazine
Dear Dr. Eric Harris,
It has been nearly two months since my sweet husband died. You treated him for over three
years for MDS, Hemolytic Anemia and Hemochromatosis.
Please excuse me for not knowing all of the staff’s names that came in contact with my husband,
but rest assured he knew every name. I want to thank you all, each person, from the receptionist
to the Phlebotomists to the Nursing Assistants, RNs, LPNs and lab.
When we first started this journey, I was an emotional wreck. I loved my husband so much, and
the thought of one of these diseases taking his life was too much and now we had to reconcile
three separate disease processes. Being a nurse, I instantly started thinking, what are we going
to do? I can’t live without him, and I cannot let him suffer.
He sat with me and reassured me that he was going to live a long time. In fact, he said, “I asked
God to give me three years.” He died three years and one month after diagnosis.
I cannot begin to tell you how much you all mean to me. My husband’s wish was to live a
“quality life” and not so much quantity. Thanks to everything you did, he did just that; he lived
a quality life. The last trip to the hospital, he had been working on his coins and then took a
nap. He ate a Wendy’s double cheeseburger, which he loved but had been avoiding so that
he could eat healthy, he walked into the hospital, confused but he did it. He was able to tell
the physicians what was going on. He was able to tell me what he wanted and did not want.
He had time to talk to his children to “get things together.” We had precious time to go on a
cruise, which was on our “bucket list.” He finished up everything he wanted to do. Everything!!
While in the ER, he had a heart attack and he was septic; after three years, he was just too
weak to fight.
I wish I could put into words how much it means to me to have had such a wonderful group
of people to help make his dreams and goals come true. Because of you, he had a wonderful
three years. Because of you, he did not suffer. Because of you, he continued to touch other
friends that had been diagnosed with cancer too. Because of you, I had my husband for three
years beyond what anyone expected. Because of you!!
Please do not ever feel that what you are doing is useless, because the end result is often
death. Every medical person with a degree can apply what they have learned to help people
“live,” even if that life is miserable. It is a special person who can apply what they have
learned to help people “truly live” a productive, happy life, positively affecting others and
realizing their dreams, even knowing that they are actively dying.
From our entire family, thank you!!
Patient’s wife in Edgewater
FCSPatient Letters
Fall 2018 37
It is always gratifying to receive
letters from appreciative patients.
Their kind words remind us why we
chose our careers in medicine and
inspire us to do our best work. If you
have a letter from a patient that you
would like to see published, please
submit via email to FCS Marketing
at [email protected]. Please
provide the location and date with
each letter you send.
Dear Dr. Harwin,
This is a long overdue note of gratitude to you for 25 happy, busy years. I was a patient of yours around 1993 and was diagnosed by my GP after an MRI with stage four cancer. She told me I needed to get my affairs in order. She also made me an appointment with you.
You told me that I had non-Hodgkins lymphoma, and if I had to get cancer, this was a good kind as it was beatable. You took my hand in yours and said we can beat this, and we did with a little help from upstairs and some very aggressive chemo. Up until a recent bout with viral pneumonia, I had a very busy life. I am now 94 years old and played 18 holes of golf three times a week, worked 20 hours a week in the pro shop at Kelly Greens and took care of my condo. I realize how fragile life is and wanted to say a very belated “thank you” to you for these 25 happy busy years.
I can only say again how very grateful I am, and thank you for those happy busy years.
Patient in Fort Myers
FCSPatient Letters

38 FCS The Magazine
Jeff Esham with wife, Katie, and children Jacob (left) and Emilio (center).
Fall 2018 39
When it comes to helping patients feel comfortable and reassured, FCS Vice President of Radiation Oncology and Radiology Jeff Esham has proven more than once that he’s
willing to do whatever it takes.This attitude started while he was still in school earning his
certification in Radiation Therapy at the University of Miami Jackson Memorial Hospital. A lot of his clinical hours were spent treating pediatric patients. Esham recognized that the equipment and technology used to treat cancer can be scary, especially for kids.
Esham recalls singing to one young girl named Annabelle. For a young boy named Marc, he painted his custom body cast black and decorated it to look like Mr. T of “The A-Team.” He even attached brush bristles for the spiky hair so Marc could don his hero costume for his treatments.
“I got very close to some of my patients and their families. Maybe I was young and naive, but I don’t regret it,” he said. “I’m never going to be the suit standing on the outside looking in.”
As the Kentucky native moved into management, earning an MBA along the way, that same philosophy continued to guide him.
“The patient is more than a solo person,” he said. “The patient is a family and community of support. And when a loved one is sitting in the waiting room, worried and not sure what’s being done, I’m the one who takes the loved one into the room to see.”
Esham oversees operations and strategic planning for radiation and radiology services throughout the network. He’s also responsible for developing new sites for radiology and radiation and promoting the latest technology updates.
Based in New Port Richey, Esham joined the team in 2012, shortly after FCS acquired four radiation centers in Pasco and Hernando counties. He brought a wealth of experience in building, redeveloping or upgrading oncology centers at nonprofit hospitals, including St. Mary’s Hospital, Jupiter Medical Center and Good Samaritan Hospital, all in Palm Beach County. From 2004-2010, he was the Administrative Director of Memorial Cancer Institute at Memorial Healthcare System in Hollywood, Florida, the third largest public healthcare system in the country.
CEO Brad Prechtl said FCS was fortunate to hire Esham, who has helped the network grow its radiation oncology footprint and enhance its physics capabilities through enhanced technology.
SENIOR MANAGEMENT SPOTLIGHT
“During Jeff’s tenure, we have dramatically expanded the number of PET and CT scanners we have throughout the state, both fixed and mobile units, along with bringing professional reading radiology services in-house,” Prechtl said.
FCS is preparing to seek accreditation from the American College of Radiation, a nod to the work Esham has overseen.
“All of these improvements have had a tremendous impact on FCS’s ability to offer state-of-the-art high quality care to our patients, no matter where they live,” Prechtl said. “Jeff has helped us fulfill our mission of offering world-class medicine close to home.”
FCS now has 15 fixed PET/CT scanners and three mobile units going to eight locations, with five of those being CT-only locations. FCS also offers radiation therapy, with 12 linear accelerators servicing nine locations.
Over the years, diagnostic scanners across the network were replaced, one by one, and both the patients and the doctors have loved the improvements, he said. It reflects what he calls a “patient-centric” approach.
“We have cutting edge, state-of-the-art cancer care, and our imaging should be, too,” he said. “Every decision is based on ‘Is it good for the patient?’ If so, we should do it. If not, we should rethink it.”
Just as Esham is willing to do whatever it takes to reassure patients, he’s also willing to do what it takes to help the people on his team do the best job possible. He believes if you give people the tools they need, they will excel. He sees everyone as his colleagues, not just his employees.
“I want people to have the freedom to do what’s right,” he said. “If you see something wrong, stop the line and get it corrected.”
When he’s not expanding FCS’ radiology and radiation reach, Esham enjoys spending time with his family. He and wife Katie have been married almost 30 years and have two boys, 20-year-old Emílio and 15-year-old Jacob. Katie also works in healthcare as a Perinatal Ultrasonographer.
A self-described “emotional leader,” Esham knows he made the right decision when he left X-ray technology to pursue training and a career in radiation therapy.
“I have been very blessed to be able to work with families and patients during this trying time in their lives.”
Putting the Patient FirstJeff Esham Impacts Radiation Oncology and Radiology Capabilities for FCS PatientsBY AUDREY POST

• Shop on AmazonSmile.com or iGive.com and designate the FCS Foundation as your preferred charity
Thank You for Your Continued Support of the FCS Foundation!The FCS Foundation fulfills a unique purpose for cancer patients who are struggling to pay their
everyday living expenses. Imagine cancer patients who can’t make car payments leaving them
without transportation to their physician’s office; or patients who can’t pay mortgage or rent and
are facing eviction while they are fighting for their lives. The Foundation pays for non-medical
expenses such as mortgage, rent, utilities and car payments, so that patients can concentrate
on recovering from cancer.
What Separates the FCS Foundation from Other Charities?Florida Cancer Specialists pays the overhead, which means that 100% of all donations go directly to help cancer patients in need! The FCS Foundation provides help for the entire
family, as well, by relieving some of the stress cancer patients and their family members face
on a daily basis.
Ways YOU Can Help• Volunteer and make a difference in someone’s life
• Make a special gift in memory or in honor of someone you love
• Name the FCS Foundation in your will or trust
• Donate a boat, RV or vehicle
• Support the many Foundation fundraising events throughout the state
Applications are available at Foundation.FLCancer.com/Volunteer or send email inquiries to: [email protected]
5204 Paylor Lane, Sarasota, FL 34240
For more info or to donate, call (941) 677.7181 or visit Foundation.FLCancer.com











![RetroRetrospective [Lucio Fontana, 1899-1968]spective [Lucio Fontana, 1899-1968] [1977]](https://img.pdfslide.us/doc/110x75/577cc0e41a28aba71191807d/retroretrospective-lucio-fontana-1899-1968spective-lucio-fontana-1899-1968.jpg)