Embed Size (px)
Citation preview

THE LONG-TERM SURVIVAL OF CARTILAGE H O M O G R A F T S I N M A N 1
By THOMAS GIBSON, F.R.C.S.E., F.R.F.P.S.G. Plastic Surgery Unit, Glasgow Royal Infirmary
W. BRIAN DAVIS, B.Sc., M.D., D.P.H. Department of Pathology, Clinical Laboratories,
The Victoria Infirmary of Glasgow
and R. C. CURRAN, M.D. Department of Pathology, University of Sheffield
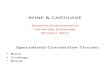
FOR many years it has been known that homograffs of cartilage will survive in animals for a very much longer time than most other tissues and may well persist indefinitely. Leopold first demonstrated this in I88I by transplanting small fragments of embryonic cartilage into the anterior chamber of rabbits' eyes ; within a few months the fragments grew to many times their original size (Fig. i). Davis (I913) found no differences between autograft and homograft rib cartilage transplanted into pedicle flaps in dogs and this was confirmed by Gorbunoff (i93o). Homografts of epiphyseal cartilage will survive for long periods in dogs, but the cells play no part in bone growth (yon Tappeiner, i913). Dupertuis (i94i) observed growth in rib cartilage homograffs taken from young rabbits and implanted subcutaneously. Bacsich and Wybum (I947) and Craigmyle (I955) have confirmed the prolonged survival of cartilage homografts in the guinea-pig and in the rabbit.
In man the difficulty in obtaining living cartilage for homografts has greatly restricted its clinical use, although maternal ear cartilage has enjoyed some popularity for aural reconstruction ; Gillies (I92O) and Gillies and Millard (I957) reported satisfactory results but Greeley (I944) found that such grafts underwent absorption. B/ickdahl et al. (I954) reviewed a series of twenty-five grafts of maternal ear cartilage and noted complete disappearance of two and partial absorption of seven after an average interval of less than two years. A homograft of rib cartilage transplanted from an infant into a 6-year-old child was examined four years later by Peer (I955). Direct measurement showed that it had decreased in size, and in one area had been absorbed and was replaced by fibrous tissue; the chondrocytes of the remainder, however, appeared as living cells.
The ultimate fate of cartilage homograffs in man is therefore still in doubt. Animal experiments suggest that they should survive indefinitely; the meagre clinical material available indicates that some are completely absorbed. However, absorption does not necessarily mean that a homograft reaction has occurred ; it may be due solely to failure of the cartilage to " take " as a free graft. We have investigated the problem by experimental implants in human volunteers.
i A preliminary report of this study was published in the Transplantation Bulletin (I957, 4, IOS) ; at that time homograft cartilage cells had been shown to be still alive fifteen months after transplantation.
3 A x77

.
/ ~ , ,\
\
~ s /
! /
/ @
J
G.
x78

LONG-TERM SURVIVAL OF CARTILAGE HOMOGRAFTS IN MAN I79
MATERIAL AND METHODS
T w e n t y - o n e e x p e r i m e n t a l i m p l a n t s w e r e m a d e s u b c u t a n e o u s l y . S o m e o f t h e v o l u n t e e r s w e r e h a v i n g m u l t i p l e - s t a g e o p e r a t i o n s a n d so t h e ca r t i l age c o u l d be r e m o v e d read i ly at a l a t e r date . I n t w o pa t i en t s t h e s t u m p o f an a c r o m i o t h o r a c i c t u b e p e d i c l e r e m a i n e d a f t e r a fac ia l r e c o n s t r u c t i o n a n d a ser ies o f six a n d o f e igh t i m p l a n t s r e s p e c t i v e l y was m a d e .
T h e h o m o g r a f t s w e r e t r a n s p l a n t e d w i t h i n t w o h o u r s o f t h e i r r e m o v a l f r o m t h e d o n o r . Al l b u t t w o w e r e o f r ib ca r t i l age ; one s p e c i m e n o f ea r a n d one o f
Speci- i Host I Donor Site of Duration in '~'S Uptake men ! (Sex and ] (Sex and Source. No. Age). ! Age). Insertion. Tissues. Test.
I M., 43 2 M., 32 3 M., 74
4 M., 74
5 M., 48
6 M., 48
7 M., 37 8 M., 48
9 M., 48
IO M., 48
I I M . , 48
12 M., 48
13 i . , 48
14 M., 48
15 M., 48
16 M., I4
I7 M., 14
18 M., 14
19 M., I4
2o M., 14
21 M., 14
M . ~ M., F.,
F.,
g., 22
F., 22
M., I4 M., T 9
M., I9
M., I9
M., I9
M., I9
M., I9
M., I9
M , I9
M., 19
M., I9
M., 19
M., I9
M., 19
M., 19
33 Rib 28 Nasal septum 24 Rib tip with peri-
chondrium 24 Rib without peri-
chondrium Rib tip with peri-
chondrium Rib without peri-
chondrium Ear Rib
Rib
Rib
Rib
Rib
Rib
Rib
Rib
Rib
Rib
Rib
Rib
Rib
Rib
Abdominal wall Abdominal pedicle Acromio-thoracic
pedicle Acromio-thoracic
pedicle Acromio-thoracic
pedicle Acromio-thoracic
pedicle Neck Acromio-thoracic
pedicle Acromio-thoracic
pedicle Acromio-thoracic
pedicle Acromio-thoracic
pedicle Acromio-thoracic
pedicle Acromio-thoracic
pedicle Acromio-thoracic
pedicle Acromio-thoracic
pedicle Acromio-thoracic
pedicle Acromio-thoracic
pedicle Acromio-thoracic
pedicle Acromio-thoracic
pedicle Acromio-thoracic
pedicle Acromio-thoracic
pedicle
2 weeks z months 2 months
2 months
3 months
3 months
7 months 2 1 months
5 months
7½ months
12 months
14.1, months +
I8 months
2I months
24 months
2½ months
5 months
7½ months
12 months
14 months
24 months ~-
_L
FtG. x (see facing page) One page of Leopold's ( I 8 8 I ) beautiful coloured lithographs. The diagrams (3, 4 and 6) indicate the original size of the fragments of embryonic rabbit cartilage transplanted into the anterior chamber of rabbits' eyes. All grew to many times their original size. The intervals after transplantation were: 3a, 28 days; 3b and 3c, i26 days; 4a, 28 days; 4b, 126 days; 6a, 5 ° days; 6b, I I 3 days. The specimen in 4 apparently outgrew its blood supply and did not develop further after 4 weeks. In the others, note the blood vessels coursing over the grafts ; these transplants were not freely floating but in intimate
contact with the host.

18o BRITISH JOURNAL OF PLASTIC SURGERY
nasal scptal cartilage were also inserted. Two implants were made in each of two patients; one was a rib tip almost completely covered by perichondrium, while from the other the entire perichondrium was removed. Parallel work with
autogcnous cartilage (Curran and Gibson, 1956) showed that the presence or absence of peri- chondrium does not influence the survival of a graft and for all subsequent implants trans- verse slices of rib cartilage 2 to 3 mm. thick were used. Thus bare cartilage formed the greater part of the exposed surface, but perichondrium was retained at the periphery so that its behaviour also could be studied.
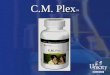
The implants were excised at intervals which varied from two weeks to two years. The surrounding tissue was retained intact whenever possible and the specimen was divided into two portions ; one was fixed and studied histologically whilst the other was tested for its ability to metabolise sulphate in vitro. It has been shown previously (Curran and Gibson, 1956) that sulphate containing 35S is taken up only when the
F:to. 2. cells are alive. The clinical An autoradiograph showing a positive z~S uptake test. details of the implants and There are bursts of radiation, each centred on a chondro- the results of the zsS uptake cyte. Dead cartilage shows only scattered background
activity. × x2o. test are given in the table. In addition to our own
material, we have been privileged to examine four specimens of maternal ear cartilage grafts provided by Sir Harold Gillies; these had been excised at intervals of ten months to twenty-two years after insertion.
RESULTS
zsS Uptake Test.--All but two of the specimens examined showed active metabolism of sulphate by the chondrocytes ; a typical autoradiograph is shown in Fig. 2. The two exceptions, one from each of the series, showed no uptake and presumably had died soon after transplantation. One was found to be lying free in the host tissues ; the other was enclosed by loose areolar tissue.
His to logy . - -The behaviour of the fibrous perichondrium proved to be of particular interest. Up to two months after insertion it appeared to be quite

LONG-TERM SURVIVAL OF CARTILAGE HOMOGRAFTS IN MAN 18I
FIG. 3 A homograft excised after two months (specimen 3) ; the appearances of the perichonclrium are quite normal.
(Masson-Goldner trichrome.) × i2o.
FIG. 4 In this homograft excised after two and a half months (specimen 16) the perichondrium has been largely replaced by young collagenous tissue infiltrated by lymphocytes and plasma cells. We believe this to be an example of a homograft rejection phenomenon to the fibrous tissue of
the transplant. (Masson-Goldner trichrome.) × 12o.

182 BRITISH JOURNAL OF PLASTIC SURGERY
normal (Fig. 3). In the two specimens which were removed at two and a half months, however, the perichondrium was infiltrated extensively with lymphocytes, plasma cells, and young fibroblasts (Fig. 4).
In all the subsequent specimens perichondrium was absent and it was replaced by a layer of loose areolar tissue (Fig. 5). The intense infiltration that was noted at two and a half months is interpreted as a homograft reaction in the perichondrium which ultimately progressed to complete absorption. Throughout
FIG. 5 Ait~r five months in the tissues (specimen 16) the peri- chondrium has disappeared and has been replaced by a layer of fibrous tissue derived presumably from the host. This layer is continuous with that covering the cut surface, which shows some erosion. Some round-ceU infiltration persists, but this was absent from later specimens.
(Masson-Goldner trichrome.) × IOO.
the experimental series there is a striking absence of any inflammatory infiltration around the cartilage itself, and this helps to confirm the immunity of cartilage to the homograft rejection phenomenon.
Apart from the behaviour of the perichondrium, the histological appearances were similar to those previously reported with autografts (Davis and Gibson, I956). A moderate degree of surface erosion and absorption had occurred on all bare surfaces, while the surface which had an intact perichondrial layer at the time of transplantation was unaffected. It was noteworthy that even when the fibrous perichondrium had been destroyed, no absorption of the underlying cartilage had occurred (Fig. 6).
Maternal Ear Cart i lage.--The four specimens supplied by Sir Harold Gillies had been excised from different patients after intervals of ten months, ten months, three and a half years, and twenty-two years. They were received in

LONG-TERM SURVIVAL OF CARTILAGE HOMOGRAFTS IN MAN I8 3
a fixing solution and so an uptake test could not be performed. One of, the ten- month specimens had been excised because of chronic sinus formation, and although much of the cartilage appeared to be normal there had been some destruction from sepsis and the inflammatory reaction precluded a confident
FIG. 6
A homograft excised after two years (specimen I5). Although the perichondtium has been replaced by host fibrous tissue there has been no absorption of the underlying cartilage which is easily recognised by the peripheral layer of
flattened cells. (Masson-Goldner trichrome.) × IOO.
histological assessment. The other specimens were removed at secondary operations and had the following microscopical appearances.
Ten Months.--There was no soft tissue around this specimen, but the chondrocytes appeared normal. A portion of the cartilage had been sectioned at the time of transplantation, and using this as a control no changes could be found after the ten months' sojourn in the host tissues.
Three and a half Years.--The greater part of the cartilage was of normal appearance and there was no cellular infiltration around the graft. One area had been partly absorbed and the absorptive process appeared to be continuing; this, however, affected but a very small part of the specimen.

18 4 BRITISH JOURNAL OF PLASTIC SURGERY
Twenty-two Years.--This again showed normal ear cartilage with chondrocytes which appeared to have been alive at the time of fixation (Fig. 7). The specimen had been removed because of a " cys t" developing on the ear. The " cys t"
FIG. 7
A portion of maternal ear cartilage graft excised after twenty-two years (Sir Harold O~llies' specimen). The cells appear to be normal and to have been alive up to the time of fixation. (Masson-Goldner trichrome.) × IOO.
appeared to be a haematoma with deposition of calcium, but no calcification was evident in the cartilage itself.
DISCUSSION
So far as is known the two years' survival of cartilage cells which we have demonstrated is by far the longest proved survival of any human cell in another individual, with the possible exception of corneal grafts and of instances in identical twins ; further, it suggests that survival could be indefinite. Sir Harold Gillies' specimen of maternal ear cartilage transplanted to a child twenty-two years before confirms this ; although a test for viability of the cells could not be made, their normal appearance indicates that they had certainly been alive to within a brief time prior to fixation.

LONG-TERM SURVIVAL OF CARTILAGE HOMOGRAFTS IN MAN 18 5
Why should cartilage survive when virtually all other homograft cells are killed within a few weeks ? There would seem to be two reasons : (I) chondro- cytes are prevented from coming into cellular contact with the host because of the surrounding matrix, and (2) the matrix itself appears to be non-antigenic at least between individuals of the same species.
The homograft reaction can be prevented or at least greatly delayed if the tissue is protected from cellular contact with the host. Thus skin homografts transplanted into the anterior chamber of the rabbit's eye are destroyed only if they are penetrated by blood-vessels (Medawar, I948). Similarly, the homograft reaction may be prevented by enclosing the graft in a diffusion chamber which allows tissue fluids to reach and nourish the graft but prevents the ingrowth of connective tissue with its blood-vessels (Algire et al., I954 ; Weaver et al., I955). Vascularisation of other tissues always precedes the homograft rejection phenomenon and the absence of vascular ingrowth and the protective matrix are probably the most important factors in the survival of cartilage cells.
Bacsich and Wyburn (r947) have discussed the protective action of the mucopolysaccharides on homografts of cornea and cartilage. There is no doubt that the matrix of the cartilage did not excite an immune response either in our own series or in those of other workers using animals. It may be accepted, therefore, that the matrix is non-antigenic within individuals of the same species. In the case of heterografts it has been shown previously (Gibson and Davis, I953) that preserved bovine cartilage appears to produce an immune response in man ; this cartilage had, however, been denatured by boiling.
In view of our finding that all but two of our experimental homografts survived and showed no more absorption than would have been apparent in autografts, what is the explanation of the absorption which has been noted with clinical homografts, particularly of maternal ear cartilage ?
We believe that this is because a part or all of the graft has failed to " take " as a free graft. This would seem particularly liable to happen to a piece of corrugated ear cartilage placed in a loose skin pocket against the rigid skull. Blood clot would inevitably form around parts of it and we have shown in animals that cartilage embedded in blood clot will not survive. Those parts of the graft which were in close apposition to the soft tissue would live and persist, while those surrounded by blood clot would die and be absorbed. The death of our two specimens is probably to be explained by the formation of blood clot around them immediately after transplantation.
In skin grafting everyone appreciates the need for intimate contact between graft and bed, and recognises the lethal effect of collections of blood or serum under the graft. It must be stressed that the same requirements exist for cartilage grafts, whether autogenous or homogenous. In a graft to the nasal bridge the skin is in intimate contact on three sides and absorption of such grafts is very rare (Davis and Gibson, I956). In other situations such as the malar region or ill ear reconstruction, only a small area of the superficial part of the graft may be in contact with vascular tissue, whilst the remainder bridges a dead space filled with blood clot ; it is in such sites that absorption has been noted.
T h e Future o f Carti lage Homograf t s . - -The fact that in man cartilage homografts seem to behave precisely as autografts suggests wide applications of homogenous cartilage in reconstructive surgery. Cartilage cells survive somatic
3 B

ig6 BRITISH jOURNAL OF PLASTIC SURGERY
death for up to seventy-two hours and a supply of living cartilage may be obtained from cadavers. The cartilage may then be stored in a viable state for periods up to six weeks at 4 ° C. (Gibson and Curran, I957). A central "bank " of living cartilage may therefore be established in any large hospital. The cadavers should be young to avoid cartilage that is calcified, and dead from conditions other than infections or malignancy. The cartilage should be removed with aseptic and antiseptic precautions and stored in a suitable solution, perhaps containing antibiotics. It is hoped to report more precisely on this at a later date. Experiments on the storage of cartilage for long periods at low temperatures ( - 7 °° to - 80 ° C.) are in progress (Gibson, I957), but to date it has been found that the cells invariably succumb at temperatures below freezing point.
Whilst most of our work applies to rib cartilage there seems no reason why homografts of ear, nose, or joint cartilage should not be used in the same way.
SUMMARY
I. Nineteen fresh homografts of rib cartilage, one of ear cartilage, and one of nasal septal cartilage have been studied in human volunteers.
2. The ability to metabolise radioactive sulphur (35S) in vitro was used as a test for viability. Nineteen of the twenty-one implants were found to be alive after intervals varying from two weeks to two years. The two specimens which failed to survive were of rib cartilage from different donors and in different hosts ; other specimens in these hosts were alive up to two years, at which time the experiments were concluded.
3. Histological examination failed to reveal any differences in the behaviour of homograft and autograft cartilage.
4. Four specimens of maternal ear cartilage provided by Sir Harold Gillies were also examined histologically. After ten months, ten months, three and a half years, and twenty-two years in the host tissues they appeared to have survived as living grafts.
5. Cartilage itself did not elicit a homograft reaction but in two specimens excised after two and a half months the perichondrium did. At two months the perichondrium was normal and from 'three months onward no perichondrium could be found.
6. It is concluded that cartilage homografts in man remain alive for at least two years and probably do so indefinitely.
7. The possibility of developing a " b a n k " of living cartilage is discussed briefly.
We continue to be indebted to Sir Harold Gillies, whose cartilage specimens and critical encouragement have been of the greatest value in our work.
Mr A. Archibald has again undertaken the technical work and Mr Hugh Gray the photography.
Fig. I is reproduced by permission of the publishers of " Virchows Archives," Springer Verlag, Berlin.

LONG-TERM SURVIVAL OF CARTILAGE HOMOGRAFTS IN MAN 187
REFERENCES
ALGIRE, G. H., WEAVER, J. M., and PREHN, R. T. (I954). J. Nat. Cancer Inst., I5, 493. B~CKDAHL, M., CONSIGLIO, V., and FALCONER, B. (1954). Brit. J. plast. Surg., 4, 263. BACSICH, P., and WYBURN, G. M. (I947). Proc. roy. Soc. Edinb., 62, 32I. CRAIGMYLE, M. B. L. (I955). Brit. J. plast. Surg., 8, 93. CURRAN, R. C., and GIBSON, T. (1956). Proc. roy. Soc., B, I44 , 572. DAVIS, J. S. (I913). Johns Hopk. Hosp. Bull., 24, II6. DAVIS, W. B., and GIBSON, T. (I956). Brit. J. plast. Surg.~ 9, 177. DUPERTUIS, S. M. (194I). Arch. Surg., 43, 32. GIBSON, T. (I957). Proc. roy. Soe, B, x47 , 528. GIBSON, T., and CURRAN, R. C. (I957). " Transactions of the International Society of
Plastic Surgeons, Stockholm, i955." Baltimore : Williams & Wilkins. GIBSON, T., and DAVIS, W. B. (I953). Brit. J. plast. Surg., 6, 4. GILLIES, H. D. (I92O). " Plastic Surgery of the Face." London : Oxford University Press. GILLIES, H., and MILLARD, R. D., Jun. (I957). " The Principles and Art of Plastic
Surgery." London: Butterworth & Co. GORBUNOFF, W. P. (1930). Arch. k!in. Chir., I 6 I , 651. GREELEY, P. (1944). Quoted by Peer (1955). LEOPOLD, G. (1881). Virchows Arch., 85,283. MEDAWAR, P. B. (1948). Brit..7. exp. Path., 29, 58. PEER, L. (1955). " Transplantation of Tissue." Baltimore : Williams & Wilkins. VON TAPPEINER, F. H. (1913). Z. ges. exp. Med., I , 491. WEAVER, J. M., ALGIRE, G. H., and PREHN, R. T. (1955). J. nat. Cancer Inst., I5, 1737.
3 B~






![Review Open Access - Microsoft · Roy Calne used 6-MP on canine kidney homografts and noted that it significantly prolonged survival[20]. His findings however were not replicated](https://img.pdfslide.us/doc/110x75/603658354cb43208c74e170c/review-open-access-microsoft-roy-calne-used-6-mp-on-canine-kidney-homografts-and.jpg)