Embed Size (px)
Citation preview

522 | SEPTEMBER 2013 | VOLUME 10 www.nature.com/nrgastro
Neuroscience Research Unit, Hôpital St-Luc (CHUM), 1058 Rue St-Denis, Montreal, QC H2X 3J4, Canada. [email protected]
The liver–brain axis in liver failure: neuroinflammation and encephalopathyRoger F. Butterworth
Abstract | Systemic inflammation is common in liver failure and its acquisition is a predictor of hepatic encephalopathy severity. New studies provide convincing evidence for a role of neuroinflammation (inflammation of the brain per se) in liver failure; this evidence includes activation of microglia, together with increased synthesis in situ of the proinflammatory cytokines TNF, IL-1β and IL-6. Liver–brain signalling mechanisms in liver failure include: direct effects of systemic proinflammatory molecules, recruitment of monocytes after microglial activation, brain accumulation of ammonia, lactate and manganese, and altered permeability of the blood–brain barrier. Ammonia and cytokines might act synergistically. Existing strategies to reduce ammonia levels (including lactulose, rifaximin and probiotics) have the potential to dampen systemic inflammation, as does albumin dialysis, mild hypothermia and N-acetylcysteine, the latter two agents acting at both peripheral and central sites. Minocycline, an agent with potent central anti-inflammatory properties, reduces neuroinflammation, brain oedema and encephalopathy in liver failure, as does the anti-TNF agent etanercept.
Butterworth, R. F. Nat. Rev. Gastroenterol. Hepatol. 10, 522–528 (2013); published online 2 July 2013; doi:10.1038/nrgastro.2013.99
IntroductionHepatic encephalopathy is a severe ne uropsychiatric com-plication of both acute liver failure (ALF) and chronic liver failure (CLF) that is characterized by cognitive and motor disturbances progressing to stupor and coma. The development of hepatic encephalopathy heralds a poor prognosis with a marked effect on patient sur-vival, liver transplantation priority and outcome, as well as on health-related quality of life. Rational, effective approaches for the prevention and treatment of hepatic encephalopathy are, therefore, urgently required.
Despite several decades of investigation, the mecha n-isms responsible for hepatic encephalopathy in liver failure are still not fully understood (Figure 1, Box 1). Ammonia continues to attract a great deal of support as the major can didate toxin. However, other toxic agents such as man-ganese, mercaptans, some fatty acids and tryptophan deriv-atives have also been proposed as agents with the poten tial to cause central nervous system (CNS) disturbances in liver failure. Ammonia-lowering strategies are the mainstay of current standard-of-care in most liver centres. How ever, these approaches have, at times, been found to be only partially effective (CLF) or completely ineffective (ALF) in hepatic encephalopathy,1,2 suggesting that alternative (or additional) m echanisms have an important role.
Evidence now suggests that both systemic and central proinflammatory mechanisms are acting alone or in concert with other toxins including ammonia. This Review discusses the evidence for such mechanisms and
their role in the pathogenesis of hepatic enceph alopathy. Novel diagnostic and therapeutic opportunities p rovided by current research in this area are also presented.
Liver failureSystemic inflammationSystemic inflammation resulting from infection and/or hepatocyte cell death is common in liver failure;3,4 the aeti-ology of liver failure and, in the case of toxic liver injury, the nature of the toxin, have been shown to determine the characteristics of the inflammatory response.5 In a study of >200 patients with ALF, the acquisition of a systemic inflammatory response syndrome was found to be a major predictor of hepatic encephalopathy.6 In other studies, a marked correlation was found to exist between the severity of systemic inflammation and that of hepatic encephalo-pathy. For example, circulating levels of TNF, a potent proinflammatory cytokine, are increased as a function of the severity of hepatic encephalopathy in both patients7 and experimental animals8 with liver failure. More over, the presence of TNF gene polymorphisms is known to in fluence the clinical outcome in patients with ALF.9
Precipitating factors for hepatic encephalopathy, such as sepsis, hyponatraemia, gastrointestinal haemorrhage and renal failure, are known to increase production of TNF.7 Moreover, in a study including 100 patients with cirrhosis and systemic inflammation resulting from infection, the presence of proinflam matory mediators (including TNF) was found to exacerbate n europsychiatric symptoms.10
Neuroinflammation and encephalopathyThe first direct evidence for the existence of neuro-inflammation in liver failure—consisting of activation of
Competing interestsR. F. Butterworth declares associations with the following companies: Merz Pharmaceuticals, Otsuka Pharmaceuticals and Salix Pharmaceuticals. See the article online for full details of the relationships.
REVIEWS
© 2013 Macmillan Publishers Limited. All rights reserved

NATURE REVIEWS | GASTROENTEROLOGY & HEPATOLOGY VOLUME 10 | SEPTEMBER 2013 | 523
microglial cells (Figure 2) together with increased levels of TNF, IL-1β and IL-6 in the brain—was unequivocally demonstrated in experimental animals with ALF result-ing from hepatic devascularization.11 Microglial cells constitute the resident macrophages of the brain and have the ability to recognize a wide range of homeostatic disturbances from vascular or tissue damage to impend-ing cellular energy failure. When activated, microglia release a wide range of cytokines and chemokines with proinflammatory or anti-inflammatory properties.
One study reported arterio–venous differences in the levels of TNF and interleukins in blood sampled from an artery and reverse jugular catheter in 16 patients with ALF caused by paracetamol overdose.12 These findings are consistent with the production of these cytokines in the CNS of these patients, a hypothesis further supported by a report of increased expression of genes coding for these cytokines in the brains of animals with ALF.8 The extent of microglial activation and the magnitude of the concomitant increases of cytokine mRNA levels were found to be predictive of the severity of encephalopathy and the p resence of brain oedema.8
Similar findings of microglial activation and brain accumu lation of proinflammatory cytokines were reported in a second animal model of ALF result-ing from azoxymethane-induced toxic liver injury.5,13 Evidence consistent with a role of brain-derived pro-inflammatory cytokines in the pathogenesis of hepatic encephalopathy in this model were also derived from animal studies in which deletions of the genes encod-ing Tnf or Il-1β were found to delay onset of hepatic encephalopathy and to attenuate brain oedema in ALF.14 In 2012, microglial activation and motility were dem-onstrated to occur in the frontal cortex of these mice using an in vivo two-photon imaging technique and, in this case, microglial activation occurred at fairly late stages of encephal opathy.15 Another research group confirmed these findings using the same mouse model and also found altered expression of certain chemo-kines (including C–C motif chemokine 2, Ccl2) in the brain.16 Microglial activation was also reported in autop-sied brain tissue from a patient with ALF resulting from viral hepatitis.17
Although microglial activation and brain cytokine accumulation have been consistently described in ALF, findings in CLF are less consistent, which is related, in part, to differences in the aetiology of liver failure and/or cirrhosis. For example, microglial activation was reported in experimental cirrhosis resulting from bile-duct resection and ligation in mice18 and rats.19 By con-trast, end-to-side surgical portacaval a nastomosis in rats has minimal effects on brain cytokines20 and portal vein ligation in the same species does not result in micro-glial activation, although it does result in increased Il‑6 expression;21 the exact nature of the neural cell expressing these changes was not determined in this study. On the other hand, microglial activation was observed in autopsied cerebral cortical tissue from eight patients with cirrhosis of varying aetiology who died in hepatic coma.22
Key points
■ Both acute and chronic liver failure result in neuroinflammation—an inflammatory response in the central nervous system (CNS) characterized by microglial activation and brain accumulation of proinflammatory cytokines
■ Evidence suggests that neuroinflammation contributes to the pathogenesis of the CNS manifestations of acute and chronic liver failure, including hepatic encephalopathy as well as brain oedema and its complications
■ Liver-to-brain proinflammatory signalling in liver failure involves humoral and neural routes; new evidence indicates that monocyte recruitment, changes in levels of ammonia, lactate, manganese and alterations in blood–brain barrier permeability might also have a key role
■ Many currently available therapies used in the treatment of encephalopathy and brain oedema in liver failure (including lactulose, albumin dialysis and mild hypothermia) have the requisite properties to limit systemic and/or neuroinflammation
■ Early investigations found that anti-inflammatory agents (such as ibuprofen, anti-TNF agents and minocycline) are effective in the treatment of the CNS complications of experimental liver failure
Liver–brain proinflammatory signallingMultiple mechanisms underlying liver–brain proinflam-matory signalling have been suggested. Box 2 provides a summary of the proposed mechanisms, which are d iscussed in detail below.
Monocyte recruitment In systemic inflammatory disorders including liver failure, communication between the periphery and the brain occurs by one or more of three routes: the traditional humoral and neural routes, and also via the active recruit-ment of monocytes into the brain.18 This latter process is a result of initial microglial activation; peripheral TNF sig-nalling is a key component in this process. Neurological complications occurring in an animal model of biliary cirrhosis—the bile-duct resected mouse—were shown to
Blood–brainbarrier
Encephalopathy
Increased levels of proinammatory cytokinesand neuroinammation
Increased ammonialevels in the brain
Liver failure
Hyperammonaemia
Microglial activation
Systemicinammation
Lactate accumulationin the brain
Figure 1 | Underlying mechanisms of hepatic encepthalopathy. Both acute and chronic liver failure result in systemic inflammation and hyperammonaemia. Increased levels of ammonia in the brain lead to lactate accumulation. Both systemic inflammation and brain lactate accumulation cause activation of microglia and increased production of proinflammatory cytokines (neuroinflammation). Prevention of neuroinflammation delays the progression of encephalopathy in liver failure.
REVIEWS
© 2013 Macmillan Publishers Limited. All rights reserved

524 | SEPTEMBER 2013 | VOLUME 10 www.nature.com/nrgastro
be the consequence of monocyte recuitment in response to TNF signalling and occurred via microglial activation. Specifically, peripheral TNF signalling stimulates microglia to produce CCL2, which subsequently mediates monocyte recruitment into the brain.18 These findings were suggested to constitute a novel immune-to-brain communication pathway with the potential to result in altered neuronal excitability and neurological complications in cholestatic liver disease. Whether or not similar mechanisms occur in liver failure of viral or toxic aetiology has not been definitively established but, in line with the latter possi-bility, McMillin et al.16 reported increased Ccl2 expression in the frontal cortex of mice with azoxymethane-induced ALF that was correlated with the degree of microglial acti-vation. Increased Ccl2 immunoreactivity was found to be predominantly neuronal in this study. Moreover, inhibition of Ccl2 activation led to a marked slowing of encephalo-pathy progression in this animal model, again suggesting a role for microglial recruitment through Ccl2.16
AmmoniaGiven the widely accepted view that ammonia has a key role in the pathogenesis of hepatic encephalopathy and fol-lowing up on the reports of microglial activation and increased synthesis of proinflammatory cytokines in both autopsy samples and in tissue from experimental animal models of hepatic encephalopathy, a series of studies (both in vitro and in vivo) have been undertaken to evaluate the role of ammonia in the pathogenesis of these neuro-inflammatory responses. A study in cultured microglial cells revealed that this cell preparation is less susceptible to substantial morphological or functional modifications than astroglial cells when exposed to toxic concentrations of ammonia.23 Moreover, although a subsequent study pro-vided evidence for activation of microglial cultures after exposure to ammonia,22 in neither study did exposure to ammonia have any marked effect on the release of pro-inflammatory cytokines by these cells. In an ex vivo study, feeding of ammonium salts to healthy rodents resulted in microglial activation together with increased brain levels of Il-1β.19 However, a subsequent ex vivo study found no such changes,15 even though both studies identified disturbances of cognitive and motor function. Possible explanations for these discrepancies might relate to the choice of brain
region under investigation; in the ex vivo study,19 changes were only evident in subcortical structures, particularly the cerebellum, whereas studies using an in vivo technique15 are, by necessity, limited to cerebral cortex.
Ammonia–cytokine synergismOf note, ammonia has the potential to act in concert with proinflammatory cytokines in a synergistic manner leading to hepatic encephalopathy in liver failure. In fact, an impressive correlation has been reported between cir-culating ammonia and TNF levels in patients with hepatic encephalopathy as a result of CLF.7 Evidence in support of ammonia–cytokine synergism has been provided by clini-cal studies in patients with cirrhosis with superimposed infection and hyperammonaemia. These patients display a considerable deterioration of cognitive and motor function that is reversed after resolution of the inflammatory state.10 At the cellular level, human cerebrovascular endothelial cells exposed to TNF in vitro manifest increased ammonia uptake.24 Moreover, cultured astrocytes exposed to com-binations of ammonia and recombinant cytokines display additive increases in expression of both heme oxygenase 1 and inducible nitric oxide synthase, consistent with the presence of oxidative and/or n itrosative stress caused by these agents in a synergistic manner.25
Lactate The concentration of lactate in the brain is increased in patients and in experimental animal models of ALF or CLF. The severity of clinical symptoms,26–30 EEG changes31 and degree of microglial activation8 are well-correlated with increased brain lactate. Brain lactate concentrations of 10–12 mM have been reported at coma stages of encephalo-pathy in liver failure;27–29 concentrations of this magni-tude resulted in substantially increased TNF and IL-6 release from cultures of microglial cells.23 Accumulation of lactate in the brain has been attributed to an inhibitory effect of ammonia on the tricarboxylic acid cycle enzyme α-ketoglutarate dehydrogenase32 and/or activation of the glycolytic enzyme p hosphofructokinase 1.33
Manganese Manganese deposits in basal ganglia structures of the brain are consistently found in patients with cirrhosis34,36 but not in those with ALF.35 Such deposits result from impaired hepatobiliary elimination of the metal together with the presence of portal–systemic shunting. The presence of manganese deposits has been linked with the presence of bilateral T1-weighted signal hyperintensities on MRI,34–36 and to dopaminergic cell death in these structures,37,38 a finding that offers a cogent explanation for the high prevalence of parkinsonism in cirrhosis.38 Considerable evidence supports the notion that neuroinflammatory mechanisms are implicated in these n eurotoxic effects of manganese. For example, manganese has been suggested to control inflammatory cytokine output from micro-glia,39 as well as stimulate microglia to release hydrogen peroxide40 and nitric oxide.41 Manganese-stimulated gen-eration of reactive oxygen species by microglia might also be a key mediator of dopaminergic neuronal cell loss.40
Box 1 | Neuroinflammatory mechanisms in HE
Current evidence for neuroinflammatory mechanisms in hepatic encephalopathy ■ Correlation of encephalopathy grade with microglial
activation ■ Graded increase in production of proinflammatory
cytokines in the brain ■ Slowing of encephalopathy progression by anti-
inflammatory strategies (namely, proinflammatory cytokine gene deletion, etanercept, infliximab, minocycline)
■ Anti-inflammatory properties of current therapies (lactulose, rifaximin, probiotics, mild hypothermia, N-acetylcysteine, albumin dialysis)
Abbreviation: HE, hepatic encephalopathy.
REVIEWS
© 2013 Macmillan Publishers Limited. All rights reserved

NATURE REVIEWS | GASTROENTEROLOGY & HEPATOLOGY VOLUME 10 | SEPTEMBER 2013 | 525
Increased brain manganese uptake in CLF is therefore likely to provide an additional signalling system with the potential to result in neuroinflammation and oxidative and/or nitrosative stress, both of which could explain the phenomenon of selective dopaminergic neuronal cell loss and parkinsonism in cirrhosis.
Blood–brain barrier permeability Results of both in vitro and in vivo studies have demon-strated that exposure to proinflammatory cytokines (such as TNF and IL-1β) leads to increased blood–brain barrier (BBB) permeability.42–44 These findings suggest that a pro-inflammatory state, characteristic of liver failure, results in alterations of BBB permeability and in this way pro-vides yet another potential liver–brain signalling pathway. The issue of BBB permeability in liver failure has been studied in both acute and chronic experi mental liver failure leading to a divergence of opinion on the subject. Earlier studies in animals with ALF resulting from hepatectomy or galactosamine-induced toxic liver injury provided evidence for rupture of the BBB.45,46 However, subsequent electron microscopic studies in material from both experimental animals47 or patients48 with ALF did not confirm these findings and went on to demonstrate that brain oedema, which is characteristic of ALF, is pre-dominantly cytotoxic (derived from cell s welling) rather than vasogenic (derived from BBB rupture).
The subject of permeability of the BBB in ALF was re assessed in the azoxymethane hepatotoxicity model but, again, findings are equivocal. Whereas there is excellent general agreement that the BBB remains grossly intact in this animal model,49–52 some investigators have reported subtle changes in expression of BBB tight junction pro-teins.53,54 These alterations in expression are caused by activation of epidermal growth factor receptor resulting in increased permeability to Evans blue dye, which could indicate increased permeability of the BBB to small mol-ecules such as ammonia and water.55 It should be noted, however, that these findings were not confirmed by others.51,52 Certainly, accumulation of ammonia and water does occur in ALF, but whether this is the consequence of increased BBB permeability awaits further studies.
The issue of BBB integrity in relation to proinflammatory mechanisms in ALF was taken to a new level of complexity fol lowing a report in 2012. Mice with azoxymethane-induced
ALF were treated using lipo polysaccharide (LPS)—an agent known to cause micro glial activation and increased production of TNF and IL-1β.56,57 LPS, given at a dose that was insufficient to cause changes in healthy animals, led to precipitation of hepatic encephalopathy and unequivocal physical rupture of the BBB in mice with ALF.58 Although BBB perme ability in patients with cirrhosis has not been systematically studied, it is well established that uptake of ammonia into the brain is increased in cirrhosis. One possible mechanism for this increased uptake is increased BBB permeability to ammonia, which was gleaned from PET studies in patients.59 Permeability of the barrier to the increased circulating concentrations of proinflammatory cytokines in liver failure has yet to be assessed.
Diagnostic implicationsActivated microglia express transcripts for translocator protein (previously known as peripheral-type benzo-diazepine protein), a mitochondrial membrane protein expressed by neuroglia (both astrocytes and microglia).60 Increased translocator protein expression in the brain has been observed in animal models of both ALF61 and CLF,62–64 as well as in brain tissue from patients with cirrhosis who died in hepatic coma.65 Activated microglia indicative of a neuroinflammatory response have been reported in dis-orders such as multiple sclerosis using the PET ligand 11C-PK11195.66 Activated microglia have also been reported in patients with cirrhosis with hepatic encephalopathy,67 in whom particularly intense signals were apparent in the anterior cingulate cortex, a brain structure that is associ-ated with the control of attention (Figure 3). These find-ings suggest a role for neuro imaging techniques for the assessment of regional metabolic alterations in relation to cognitive dysfunction in patients with cirrhosis.
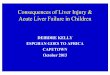
Sham ALF-6 h ALF-coma
Figure 2 | Microglial activation in the brains of rats with ALF. Representative micrographs showing the effect of hepatic devascularization on microglial activation in cerebral cortex of sham-operated rats (Sham), ALF at pre-coma, pre-oedema (ALF-6 h) and ALF at coma and oedema (ALF-coma) stages of encephalopathy. Rats at the coma and oedema stage had markedly greater levels of microglial activation than rats at the pre-coma, pre-oedema stage. Abbreviation: ALF, acute liver failure. Permission obtained from Nature Publishing Group © Jiang, W. J. Cereb. Blood Flow Metab. 29, 944–952 (2009).
Box 2 | Liver–brain proinflammatory signalling in liver failure
Possible mechanisms: ■ Induction of established humoral–neural
proinflammatory cytokine transfer ■ Monocyte recruitment into brain via microglial activation ■ Increased blood–brain ammonia transfer ■ Ammonia and proinflammatory cytokine synergism ■ Brain lactate accumulation ■ Increased blood–brain manganese transfer ■ Increased blood–brain barrier permeability
REVIEWS
© 2013 Macmillan Publishers Limited. All rights reserved

526 | SEPTEMBER 2013 | VOLUME 10 www.nature.com/nrgastro
Novel therapeutic opportunitiesExisting ammonia-lowering therapies Ammonia-lowering agents such as lactulose,68 rifaxi-min69 and L-ornithine L-aspartate70 remain the therapy of choice for hepatic encephalopathy, particularly in cirrho-sis, whereas these agents are much less effective in ALF.2 However, it should be noted that some of these agents might also act upon proinflammatory mechanisms. For example, lactulose treatment in patients with cirrhosis results in decreased severity of hepatic encephalopathy and a parallel reduction in circulating TNF levels,71 an action that has been attributed to the ability of lactulose to decrease both intestinal bacterial overgrowth and absorp-tion of endotoxin.7 Similar mechanisms of action have been proposed to explain the beneficial effects of various anti-biotics used in the treatment of hepatic encephalo pathy, including aminoglycosides and rifaximin.7 The experi-mental drug ornithine phenylacetate has been shown to cause concomitant reductions of both ammonia and Tnf levels in rats.72 The past decade has witnessed an upsurge of interest in the use of probiotics for the treatment of hepatic e ncephalopathy in cirrhosis73 and, again, the beneficial effect of these agents has been attributed, at least in part, to effects on the production and activity of TNF.7
Anti-inflammatory agents The common anti-inflammatory drug ibuprofen has been shown to restore locomotor activity74 and learning ability20 in animals with mild hepatic encephalopathy resulting from surgical end-to-side portacaval shunts. Mechanisms seem to involve the reduction of oxidative and/or nitro-sative stress, but with no marked actions on levels of proinflammato ry cytokines.
A study in 2012 using mice with azoxymethane-induced ALF demonstrated that inflammatory cascades driven by Tnf have a role in the progression of ALF and the accom-panying severity of hepatic encephalopathy.75 In this study, treatment with the TNF-neutralizing agent etanercept was
found to attenuate both systemic and central inflamma-tion leading to delayed progression of liver failure and hepa tic encephalopathy. Further evidence for a key role of pro inflammatory mechanisms in general, and for TNF in par ticular, in the pathogenesis of hepatic e ncephalo-pathy in ALF was provided by studies using gene-depleted animals. Bemeur et al.14 showed that knockdown of the gene coding for the Tnf receptor resulted in a delay in the onset of hepatic encephalopathy and prevention of brain oedema in mice with az oxymethane-induced acute liver injury. In this study, deletion of the gene Il‑1 had similar beneficial effects. Treatment with infliximab, a mono clonal antibody against TNF, has also been shown to delay the progression of en cephalopathy in bile-duct ligated rats given LPS.72
Albumin dialysis Other currently available therapies for the treatment of ALF or acute-on-chronic liver failure and their neuro-logical complications also have the potential to inhibit proinflammatory mechanisms. For example, the albumin dialysis system MARS (molecular adsorbent recirculatin g system), which is known to be effective in these con-ditions, effectively removes TNF leading to improved clinic al outcome.76
Mild hypothermia Mild hypothermia is increasingly being used as a bridge to liver transplantation in ALF.77 This approach has been shown, in experimental animal models, to act by limiting both systemic proinflammatory78 and neuro inflammator y79 responses.
N-acetylcysteine N-acetylcysteine, an agent with well-established hepato-protective and neuroprotective80 properties, prevents hepatic damage caused by azoxymethane exposure with concomitant normalization of brain levels of gluta thione. It also prevents hepatic encephalopathy and brain oedema in animals with ALF caused by azoxymethane.13
Minocycline New therapeutic dimensions aimed at the prevention and treatment of hepatic encephalopathy in ALF selectively target the brain. Minocycline is a semi-synthetic tetra-cycline that has been shown to limit microglial activa-tion in a wide range of neurodegenerative con ditions.81 Interestingly, the anti-inflammatory properties of the agent are independent of its antimicrobial properties. Studies in the hepatic devascularized rat model of ALF demonstrated that minocycline not only prevents microglial activation but also attenuates the increase in synthesis of TNF and interleukins8 in the brain leading to lowering of oxida-tive and/or nitrosative stress.82 A subsequent reduction in the progression of hepatic encepha lopathy as well as the pr evention of brain oedema was observed in these animals.
Chemokine receptor antagonists A preliminary report describes a beneficial effect of CCR2 and CCR4 chemokine receptor antagonists in slowing the
Anteriorcingulatecortex
1
0
Figure 3 | Microglial activation in a patient with cirrhosis and mild hepatic encephalopathy imaged using PET and the translocator protein ligand 11C-PK11195. Note the increased signal intensities in frontal cortex, particularly in anterior cingulate cortex—a brain structure known to be implicated in the control of attention. Binding of 11C-PK11195 to translocator protein is currently considered to be indicative of microglial activation in a wide range of neurological disorders. Image kindly provided by Dr Simon Taylor-Robinson, Imperial College, London, UK.
REVIEWS
© 2013 Macmillan Publishers Limited. All rights reserved

NATURE REVIEWS | GASTROENTEROLOGY & HEPATOLOGY VOLUME 10 | SEPTEMBER 2013 | 527
progression of hepatic encephalopathy in experimental ALF resulting from azoxymethane hepatotoxicity.16
ConclusionsNeuroinflammation, characterized by microglial activation and mobilization of proinflammatory cytokines, occurs in both acute and chronic liver failure and its occurrence heralds the onset of CNS complications such as encepha-lopathy and brain oedema. Mechanisms responsible for these neuroinflammatory responses include direct effects of systemic inflammation, recruitment of monocytes, the effects of ammonia, manganese and lactate, as well as increased permeability of the BBB and oxidative and/or nitrosative stress resulting from microglial activation. In relation to microglial activation, synergistic effects of ammonia and proinflammatory cytokines have been shown to occur. Diagnostic and therapeutic oppor-tunities provided by these discoveries include a novel PET imaging technique for the assessment of brain function in liver failure using the microglial activation
PET ligand 11C-PK11195 as well as the anti-inflammatory agents etanercept and minocycline.
Review criteria
The central themes of the Review as agreed by the author and editors were neuroinflammation as it relates to the pathogenesis of encephalopathy in liver failure, and notions of liver–brain signalling in this regard. Articles were selected using PubMed with the search terms “neuroinflammation AND liver failure/disease”, “microglial activation”, “liver–brain signalling AND liver disease” alone and in combination, all in the English language and published 1995–present. Published abstracts from the American Association for the Study of Liver Diseases 2012 and European Association for the Study of the Liver 2012 were also searched to capture the most recent retrievable citations published in abstract form. Reference lists from key review articles were also included in the searches with no predetermined timeline to include a historical perspective when deemed appropriate. Multiple citations to the same experimental finding were kept to a minimum.
1. Als-Nielsen, B., Gluud, L. L. & Gluud, C. Nonabsorbable disaccharides for hepatic encephalopathy: systematic review of randomised trials. BMJ 328, 1046 (2004).
2. Acharya, S. K., Bhatia, V., Sreenivas, V., Khanal, S. & Panda, S. K. Efficacy of L-ornithine L-aspartate in acute liver failure: a double-blind, randomized, placebo-controlled study. Gastroenterology 136, 2159–2168 (2009).
3. Rolando, N. et al. The systemic inflammatory response syndrome in acute liver failure. Hepatology 32, 734–739 (2000).
4. Shawcross, D. L., Davies, N. A., Williams, R. & Jalan, R. Systemic inflammatory response exacerbates the neuropsychological effects of induced hyperammonemia in cirrhosis. J. Hepatol. 40, 247–254 (2004).
5. Bémeur, C. & Butterworth, R. F. Liver–brain proinflammatory signalling in acute liver failure: role in the pathogenesis of hepatic encephalopathy and brain edema. Metab. Brain Dis. http://dx.doi.org/10.1007/s11011-012-9361–3.
6. Vaquero, J. et al. Infection and the progression of hepatic encephalopathy in acute liver failure. Gastroenterology 125, 755–764 (2003).
7. Odeh, M. Pathogenesis of hepatic encephalopathy: the tumour necrosis factor-α theory. Eur. J. Clin. Invest. 37, 291–304 (2007).
8. Jiang, W., Desjardins, P. & Butterworth, R. F. Cerebral inflammation contributes to encephalopathy and brain edema in acute liver failure: protective effect of minocycline. J. Neurochem. 109, 485–493 (2009).
9. Bernal, W., Donaldson, P., Underhill, J., Wendon, J. & Williams, R. Tumor necrosis factor genomic polymorphism and outcome of acetaminophen (paracetamol)-induced acute liver failure. J. Hepatol. 29, 53–59 (1998).
10. Shawcross, D. L. et al. Infection and systemic inflammation, not ammonia, are associated with Grade 3/4 hepatic encephalopathy, but not mortality in cirrhosis. J. Hepatol. 54, 640–649 (2011).
11. Jiang, W. et al. Unequivocal evidence for cytokine accumulation in brain in experimental acute liver failure. Hepatology 44 (Suppl. 1), 366A (2006).
12. Wright, G., Shawcross, D., Olde Damink, S. W. & Jalan, R. Brain cytokine flux in acute liver failure
and its relationship with intracranial hypertension. Metab. Brain Dis. 22, 375–388 (2007).
13. Bémeur, C., Vaquero, J., Desjardins, P. & Butterworth, R. F. N-acetylcysteine attenuates cerebral complications of non-acetaminophen-induced acute liver failure in mice: antioxidant and anti-inflammatory mechanisms. Metab. Brain Dis. 25, 241–249 (2010).
14. Bémeur, C., Qu, H., Desjardins, P. & Butterworth, R. F. IL-1 or TNF receptor gene deletion delays onset of encephalopathy and attenuates brain edema in experimental acute liver failure. Neurochem. Int. 56, 213–215 (2010).
15. Thrane, V. R. et al. Real-time analysis of microglial activation and motility in hepatic and hyperammonemic encephalopathy. Neuroscience 220, 247–255 (2012).
16. McMillin, M. et al. Increased neuronal chemokine CCL2/MCP-1 expression is associated with hepatic encephalopathy and contributes to neurological decline. Hepatology 56 (Suppl. 1), 958A (2012).
17. Butterworth, R. F. Hepatic encephalopathy: a central neuroinflammatory disorder? Hepatology 53, 1372–1376 (2011).
18. D’Mello, C., Le, T. & Swain, M. G. Cerebral microglia recruit monocytes into the brain in response to tumor necrosis factor α signaling during peripheral organ inflammation. J. Neurosci. 29, 2089–2102 (2009).
19. Rodrigo, R. et al. Hyperammonemia induces neuroinflammation that contributes to cognitive impairment in rats with hepatic encephalopathy. Gastroenterology 139, 675–684 (2010).
20. Cauli, O., Rodrigo, R., Piedrafita, B., Boix, J. & Felipo, V. Inflammation and hepatic encephalopathy: ibuprofen restores learning ability in rats with portacaval shunts. Hepatology 46, 514–519 (2007).
21. Brück, J. et al. Locomotor impairment and cerebrocortical oxidative stress in portal vein ligated rats in vivo. J. Hepatol. 54, 251–257 (2011).
22. Zemtsova, I. et al. Microglia activation in hepatic encephalopathy in rats and humans. Hepatology 54, 204–215 (2011).
23. Andersson, A. K. et al. Lactate contributes to ammonia-mediated astroglial dysfunction during hyperammonemia. Neurochem. Res. 34, 556–565 (2009).
24. Duchini, A., Govindarajan, S., Santucci, M., Zampi, G. & Hofman, F. M. Effects of tumor necrosis factor-α and interleukin-6 on fluid-phase permeability and ammonia diffusion in CNS-derived endothelial cells. J. Invest. Med. 44, 474–482 (1996).
25. Chastre, A., Jiang, W., Desjardins, P. & Butterworth, R. F. Ammonia and proinflammatory cytokines modify expression of genes coding for astrocytic proteins implicated in brain edema in acute liver failure. Metab. Brain Dis. 25, 17–21 (2010).
26. Tofteng, F. et al. Cerebral microdialysis in patients with fulminant hepatic failure. Hepatology 36, 1333–1340 (2002).
27. Mans, A. M., DeJoseph, M. R. & Hawkins, R. A. Metabolic abnormalities and grade of encephalopathy in acute hepatic failure. J. Neurochem. 63, 1829–1838 (1994).
28. Zwingmann, C., Chatauret, N., Leibfritz, D. & Butterworth, R. F. Selective increase of brain lactate synthesis in experimental acute liver failure: results of a [1H-13C] nuclear magnetic resonance study. Hepatology 37, 420–428 (2003).
29. Chatauret, N., Zwingmann, C., Rose, C., Leibfritz, D. & Butterworth, R. F. Effects of hypothermia on brain glucose metabolism in acute liver failure: a H/C-nuclear magnetic resonance study. Gastroenterology 125, 815–824 (2003).
30. Rose, C. et al. Association of reduced extracellular brain ammonia, lactate, and intracranial pressure in pigs with acute liver failure. Hepatology 46, 1883–1892 (2007).
31. Deutz, N. E., Chamuleau R. A., de Graaf, A. A., Bovée W. M. & de Beer, R. In vivo 31P NMR spectroscopy of the rat cerebral cortex during acute hepatic encephalopathy. NMR Biomed. 1, 101–106 (1988).
32. Lai, J. C. & Cooper, A. J. Brain α-ketoglutarate dehydrogenase complex: kinetic properties, regional distribution, and effects of inhibitors. J. Neurochem. 47, 1376–1386 (1986).
33. Ratnakumari, L. & Murthy, C. R. Response of rat cerebral glycolytic enzymes to hyperammonemic states. Neurosci. Lett. 161, 37–40 (1993).
34. Pomier-Layrargues, G., Spahr, L. & Butterworth, R. F. Increased manganese concentrations in pallidum of cirrhotic patients. Lancet 345, 735 (1995).
REVIEWS
© 2013 Macmillan Publishers Limited. All rights reserved

528 | SEPTEMBER 2013 | VOLUME 10 www.nature.com/nrgastro
35. Rose, C. et al. Manganese deposition in basal ganglia structures results from both portalsystemic shunting and liver dysfunction. Gastroenterology 117, 640–644 (1999).
36. Spahr, L. et al. Magnetic resonance imaging and proton spectroscopic alterations correlate with parkinsonian signs in patients with cirrhosis. Gastroenterology 119, 774–781 (2000).
37. Burkhard, P. R., Delavelle, J., Du Pasquier, R. & Spahr, L. Chronic parkinsonism associated with cirrhosis: a distinct subset of acquired hepatocerebral degeneration. Arch. Neurol. 60, 521–528 (2003).
38. Butterworth R. F. Parkinsonism in cirrhosis: pathogenesis and current therapeutic options. Metab. Brain Dis. http://dx.doi.org/10.1007/s11011-012-9341–7.
39. Dodd, C. A. & Filipov, N. M. Manganese potentiates LPS-induced heme-oxygenase 1 in microglia but not dopaminergic cells: role in controlling microglial hydrogen peroxide and inflammatory cytokine output. Neurotoxicology 32, 683–692 (2011).
40. Zhang, P., Lokuta, K. M., Turner, D. E. & Liu, B. Synergistic dopaminergic neurotoxicity of manganese and lipopolysaccharide: differential involvement of microglia and astroglia. J. Neurochem. 112, 434–443 (2007).
41. Filipov, N. M., Seegal, R. F. & Lawrence, D. A. Manganese potentiates in vitro production of proinflammatory cytokines and nitric oxide by microglia through a nuclear factor κB-dependent mechanism. Toxicol. Sci. 84, 139–148 (2005).
42. de Vries, H. E. et al. The influence of cytokines on the integrity of the blood–brain barrier in vitro. J. Neuroimmunol. 64, 37–43 (1996).
43. Didier, N. et al. Secretion of interleukin-1β by astrocytes mediates endothelin-1 and tumour necrosis factor-α effects on human brain microvascular endothelial cell permeability. J. Neurochem. 86, 246–254 (2003).
44. Blamire, A. M. et al. Interleukin-1β -induced changes in blood–brain barrier permeability, apparent diffusion coefficient, and cerebral blood volume in the rat brain: a magnetic resonance study. J. Neurosci. 20, 8153–8159 (2000).
45. Dixit, V. & Chang, T. M. Brain edema and the blood brain barrier in galactosamine-induced fulminant hepatic failure rats. An animal model for evaluation of liver support systems. ASAIO Trans. 36, 21–27 (1990).
46. Potvin, M., Finlayson, M. H., Hinchey, E. J., Lough, J. O. & Goresky, C. A. Cerebral abnormalities in hepatectomized rats with acute hepatic coma. Lab. Invest. 50, 560–564 (1984).
47. Traber, P. G., Dal Canto, M., Ganger, D. R. & Blei, A. T. Electron microscopic evaluation of brain edema in rabbits with galactosamine-induced fulminant hepatic failure: ultrastructure and integrity of the blood–brain barrier. Hepatology 7, 1272–1277 (1987).
48. Kato, M., Hughes, R. D., Keays, R. T. & Williams, R. Electron microscopic study of brain capillaries in cerebral edema from fulminant hepatic failure. Hepatology 15, 1060–1066 (1992).
49. Bélanger, M., Côté, J. & Butterworth, R. F. Neurobiological characterization of an azoxymethane mouse model of acute liver failure. Neurochem. Int. 48, 434–440 (2006).
50. Sawara, K. et al. Alterations in expression of genes coding for proteins of the neurovascular unit in ischemic liver failure. Neurochem. Int. 55, 119–123 (2009).
51. Palenzuela, L., Mas, A., Montaner, J. & Cordoba, J. Matrix metalloproteinase-9
in fulminant hepatic failure. Hepatology 51, 1475–1476 (2010).
52. Bémeur, C., Chastre, A., Desjardins, P. & Butterworth, R. F. No changes in expression of tight junction proteins or blood–brain barrier permeability in azoxymethane-induced experimental acute liver failure. Neurochem. Int. 56, 205–207 (2010).
53. Chen, F. et al. Occludin is regulated by epidermal growth factor receptor activation in brain endothelial cells and brains of mice with acute liver failure. Hepatology 53, 1294–1305 (2011).
54. Shimojima, N. et al. Altered expression of zonula occludens-2 precedes increased blood–brain barrier permeability in a murine model of fulminant hepatic failure. J. Invest. Surg. 21, 101–108 (2008).
55. Nguyen, J. H. Subtle BBB alterations in brain edema associated with acute liver failure. Neurochem. Int. 56, 203–204 (2010).
56. Henry, C. J., Huang, Y., Wynne, A. M. & Godbout, J. P. Peripheral lipopolysaccharide (LPS) challenge promotes microglial hyperactivity in aged mice that is associated with exaggerated induction of both pro-inflammatory IL-1β and anti-inflammatory IL-10 cytokines. Brain Behav. Immun. 23, 309–317 (2009).
57. Tanaka, S. et al. Lipopolysaccharide-induced microglial activation induces learning and memory deficits without neuronal cell death in rats. J. Neurosci. Res. 83, 557–566 (2006).
58. Chastre, A., Bélanger, M. & Butterworth, R. F. Modest systemic inflammation precipitates encephalopathy and ruptures the blood–brain barrier in acute liver failure. Hepatology 56 (Suppl. 1), 956A (2012).
59. Lockwood, A. H., Yap, E. W. & Wong, W. H. Cerebral ammonia metabolism in patients with severe liver disease and minimal hepatic encephalopathy. J. Cereb. Blood Flow Metab. 11, 337–341 (1991).
60. Ruprecht, R. et al. Translocator protein (18 kDa) (TSPO) as a therapeutic target for neurological and psychiatric conditions. Nat. Rev. Drug Disc. 9, 971–988 (2010).
61. Itzhak, Y., Roig-Cantisano, A., Dombro, R. S. & Norenberg, M. D. Acute liver failure and hyperammonemia increase peripheral-type benzodiazepine receptor binding and pregnenolone synthesis in mouse brain. Brain Res. 705, 345–348 (1995).
62. Bélanger, M., Ahboucha, S., Desjardins, P. & Butterworth, R. F. Upregulation of peripheral-type (mitochondrial) benzodiazepine receptors in hyperammonemic syndromes: consequences for neuronal excitability. Adv. Mol. Cell Biol. 31, 983–997 (2004).
63. Giguère, J. F., Hamel, E. & Butterworth, R. F. Increased densities of binding sites for the ‘peripheral-type’ benzodiazepine receptor ligand [3H]PK 11195 in rat brain following portacaval anastomosis. Brain Res. 585, 295–298 (1992).
64. Desjardins, P., Bandeira, P., Rao, V. L. & Butterworth, R. F. Portacaval anastomosis causes selective alterations of peripheral-type benzodiazepine receptor expression in rat brain and peripheral tissues. Neurochem. Int. 35, 293–299 (1999).
65. Lavoie, J., Layrargues, G. P. & Butterworth, R. F. Increased densities of peripheral-type benzodiazepine receptors in brain autopsy samples from cirrhotic patients with hepatic encephalopathy. Hepatology 11, 874–878 (1990).
66. Oh, U. et al. Translocator protein PET imaging for glial activation in multiple sclerosis. J. Neuroimmune Pharmacol. 6, 354–361 (2011).
67. Cagnin, A., Taylor-Robinson, S. D., Forton, D. M. & Banati R. B. In vivo imaging of cerebral “peripheral benzodiazepine binding sites” in patients with hepatic encephalopathy. Gut 55, 547–553 (2006).
68. Prasad, S. et al. Lactulose improves cognitive functions and health-related quality of life in patients with cirrhosis who have minimal hepatic encephalopathy. Hepatology 45, 549–559 (2007).
69. Bass, N. M. et al. Rifaximin treatment in hepatic encephalopathy. N. Engl. J. Med. 362, 1071–1081 (2010).
70. Kircheis, G. et al. Therapeutic efficacy of L-ornithine-L-aspartate infusions in patients with cirrhosis and hepatic encephalopathy: results of a placebo-controlled, double-blind study. Hepatology 25, 1351–1360 (1997).
71. Odeh, M., Sabo, E., Srugo, I. & Oliven, A. Serum levels of tumor necrosis factor-α correlate with severity of hepatic encephalopathy due to chronic liver failure. Liver Int. 24, 110–116 (2004).
72. Wright, G. et al. Reduction in hyperammonemia by ornithine phenylacetate prevents lipopolysaccharide-induced brain edema and coma in cirrhotic rats. Liver Int. 32, 410–419 (2012).
73. Agrawal, A., Sharma, B. C., Sharma, P. & Sarin, S. K. Secondary prophylaxis of hepatic encephalopathy in cirrhosis: an open-label, randomized controlled trial of lactulose, probiotics, and no therapy. Am. J. Gastroenterol. 107, 1043–1050 (2012).
74. Cauli, O. et al. Neuroinflammation contributes to hypokinesia in rats with hepatic encephalopathy: ibuprofen restores its motor activity. J. Neurosci. Res. 87, 1369–1374 (2009).
75. Chastre, A. et al. Inflammatory cascades driven by tumor necrosis factor-α play a major role in the progression of acute liver failure and its neurological complications. PLoS ONE 7, e49670 (2012).
76. Guo, L. M. et al. Application of Molecular Adsorbents Recirculating System to remove NO and cytokines in severe liver failure patients with multiple organ dysfunction syndrome. Liver Int. 23 (Suppl. 3), 16–20 (2003).
77. Jalan, R., Olde Daminck, S. W., Deutz, M. E., Lee, A. & Hayes, P. C. Moderate hypothermia for uncontrolled intracranial hypertension in acute liver failure. Lancet 354, 1164–1168 (1999).
78. Vaquero, J. et al. Mild hypothermia attenuates liver injury and improves survival in mice with acetaminophen toxicity. Gastroenterology 132, 372–383 (2007).
79. Jiang, W., Desjardins, P. & Butterworth, R. F. Direct evidence for central proinflammatory mechanisms in rats with experimental acute liver failure: protective effect of hypothermia. J. Cereb. Blood Flow Metab. 29, 944–952 (2009).
80. Chen, G., Shi, J., Hu, Z. & Hang, C. Inhibitory effect on cerebral inflammatory response following traumatic brain injury in rats: a potential neuroprotective mechanism of N-acetylcysteine. Mediators Inflamm. 2008, 716458 (2008).
81. Stirling, D. P., Koochesfahani, K. M., Steeves, J. D. & Tetzlaff, W. Minocycline as a neuroprotective agent. Neuroscientist 11, 308–322 (2005).
82. Jiang, W., Desjardins, P. & Butterworth, R. F. Minocycline attenuates oxidative/nitrosative stress and cerebral complications of acute liver failure in rats. Neurochem. Int. 55, 601–605 (2009).
REVIEWS
© 2013 Macmillan Publishers Limited. All rights reserved