Embed Size (px)
Citation preview
J. clin. Path. (1962), 15, 414
The kidney in rheumatic heart diseaseDOROTHY S. RUSSELL
From the Bernhard Baron Institute ofPathology, The London Hospital
SYNOPSIS Histological evidence of glomerulonephritis is reported in 95 (3866%) of a series of
246 necropsies with concomitant rheumatic carditis. The details of these findings are given and
their significance is discussed.
Although renal, and in particular glomerular,changes have long been recognized in the collagendiseases as a group, surprisingly little has beenrecorded of the kidney in rheumatic carditis. In 1932Bell reported glomerulitis in 21 % of a series of104 cases with active rheumatic endocarditis, chronicchanges being absent in 53. He described theglomerular lesion as diffuse, consisting of anincreased number of endothelial cells, with occa-sional thickening of the basement membranes. Insome examples the capillaries contained an excess ofleucocytes. In three cases he found focal lesions ofthe tuft, described as being of embolic type; these,however, were unaccompanied by any terminalinfection. On the other hand Baehr and Schifrin(1932) found only three examples of glomerulo-nephritis amongst 235 cases in which death was dueto rheumatic heart disease. Active carditis was pre-sent in 118. They excluded patients over 31 years ofage to avoid confusion with atherosclerotic valvulardeformities. Not surprisingly, they concluded thatglomerulonephritis was not associated with rheu-matic carditis. This view seems to have been tacitlyaccepted thereafter, and Allen (1951) dismisses thesubject with a brief but somewhat equivocal state-ment.A few chance observations suggested that the
matter merited further investigation. To this end aseries of 246 cases was selected for examinationfrom material available from 1911 to 1959. Caseswere rejected where intercurrent infection, especiallybacterial endocarditis, extensive infarction of thekidneys, gross post-mortem change, or other factorswere prejudicial to the analysis. Chronic heartfailure was the cause of death in most instancesbut some patients died from a variety of intercurrentdiseases. Elderly subjects with slight degrees ofmitral-cusp thickening were excluded on the groundsthat the rheumatic basis of this condition is question-
Received for publication 24 January 1962.
able. Cases over 40 years of age with solitary diseaseof the aortic valve were also excluded unless thecondition was clearly rheumatic. The series in factcontained only four examples of solitary aorticvalvulitis; two of these patients were 43 and 57 yearsold respectively.
Otherwise material was accepted from all decadeswhether the valvular changes were acute, chronic, orcombined.
TECHNICAL NOTES
Paraffin-embedded sections stained with haematoxylinand eosin were principally used. Frozen sections stainedwith Sudan III and haematoxylin were frequently avail-able after 1928. When more precise observation wasrequired the blocks were re-cut, with special care topreserve a constant thickness, and stained with periodic-acid-Schiff (P.A.S.) and with azan. Since the assessment ofslight degrees of proliferative glomerulitis (numericalincrease of endothelial cells with or without thickeningof the basement membranes of the tuft) proved a majordifficulty in analysis, photomicrographs at constantmagnification were made from a graded series of selectedglomeruli in P.A.S. preparations, including controls.These, mounted on a card, were useful for reference.
RESULTS
Of the 246 cases examined, 95 (38-6%) were judgedto show some form of glomerulonephritis.
1 In 16 there was an advanced nephritis re-
sembling that of Bright's disease. (a) In five thekidneys were contracted, the microscopical picturesuggesting type 2 nephritis (Ellis) in three instancesand type 1 in two. Death was due to uraemia in twocases of the former, and to chronic heart failure inthe rest. (b) In the remaining 11 cases of this groupthe kidneys were of normal size or enlarged. Lipoidflecks were visible in the cortex in two instances;otherwise there was nothing to suggest more thanback-pressure congestion. Two subjects, however,
414
copyright. on 2 June 2019 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.15.5.414 on 1 Septem
ber 1962. Dow
nloaded from
The kidney in rheumatic heart disease
FIG. I FIJ. 2
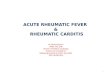
FIG. 1. Proliferative glomerulitis and capsulitis with increase of adjacent interstitial tissue. From male aged 49 wit/severe mitral stenosis and rheumatic vegetations. P.A.S. x 290.
FIG. 2. Proliferative glomerulitis with increase of interstitial tissute. Details in text. P.A.S. x 290.
were uraemic at the time of death. Microscopically adiffuse nephritis, suggestive of type 1, was found inthree cases (Fig. 1), associated with polyarteritisnodosa in one; in two cases the picture resembledthat of type 2 nephritis, but the remaining six casescould not be assigned to either category (Fig. 2).The kidneys represented by Fig. 2 were of normal
size and finely flecked with lipoid. The principalglomerular change was an uneven proliferativeglomerulitis. In a few glomeruli the capsularepithelium was heaped up, and occasionally fusionof the tuft to the capsule had led to disorganizationthrough invasion by fibroblasts. The interstitialtissue was diffusely increased, sparsely cellular andoedematous. The lumina of the tubules containedmany red corpuscles. The patient, aged 50 at death,was known to have rheumatic endocarditis at 45, hisurine then being reported as normal. Ten weeksbefore death the urine became dark and three weekslater he was admitted to hospital with heart failure,albuminuria, and haematuria. Following this he hada phase of uraemia, but his blood urea returned tonormal and death was ultimately due to heartfailure.
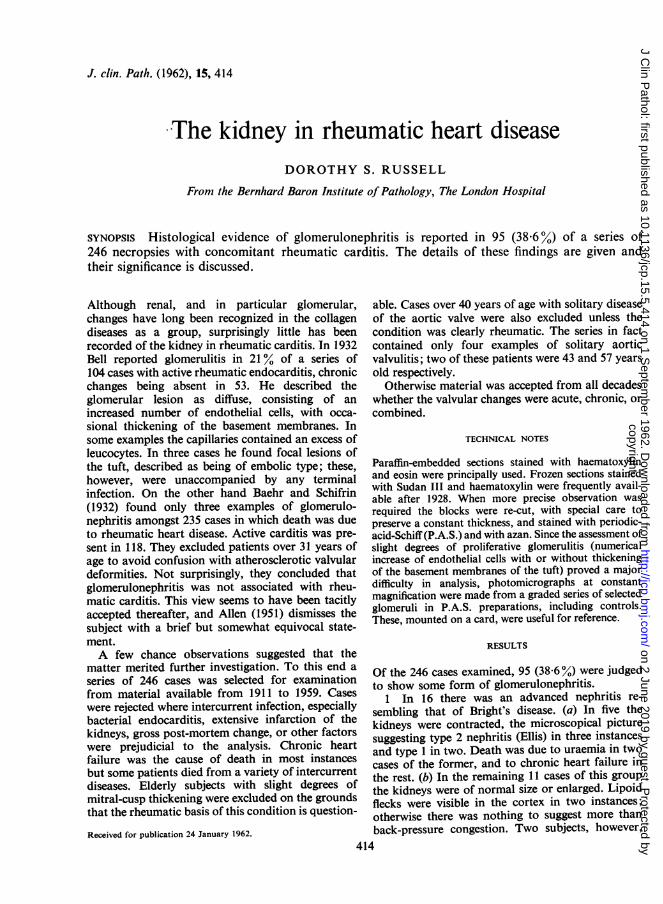
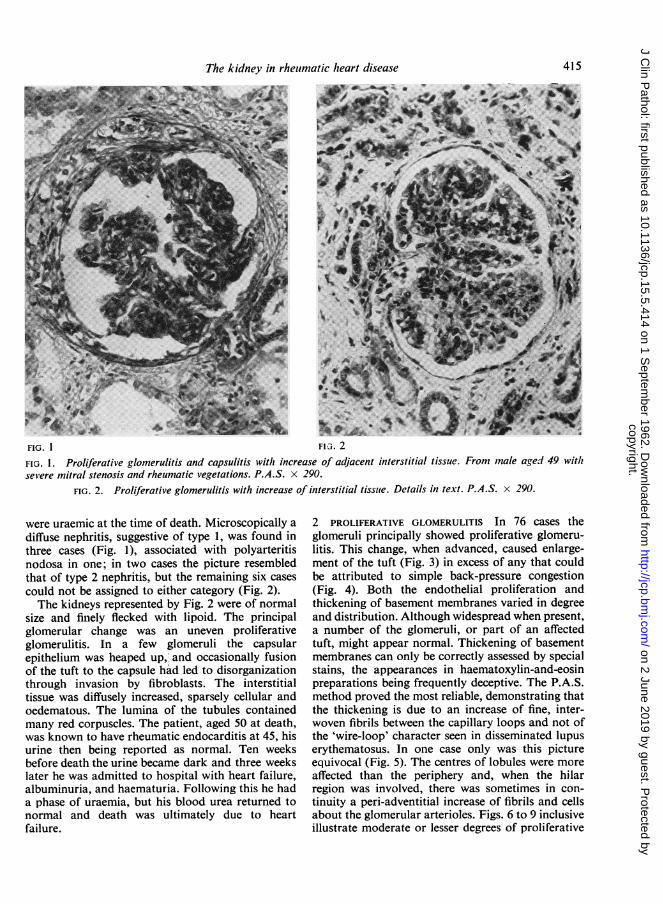
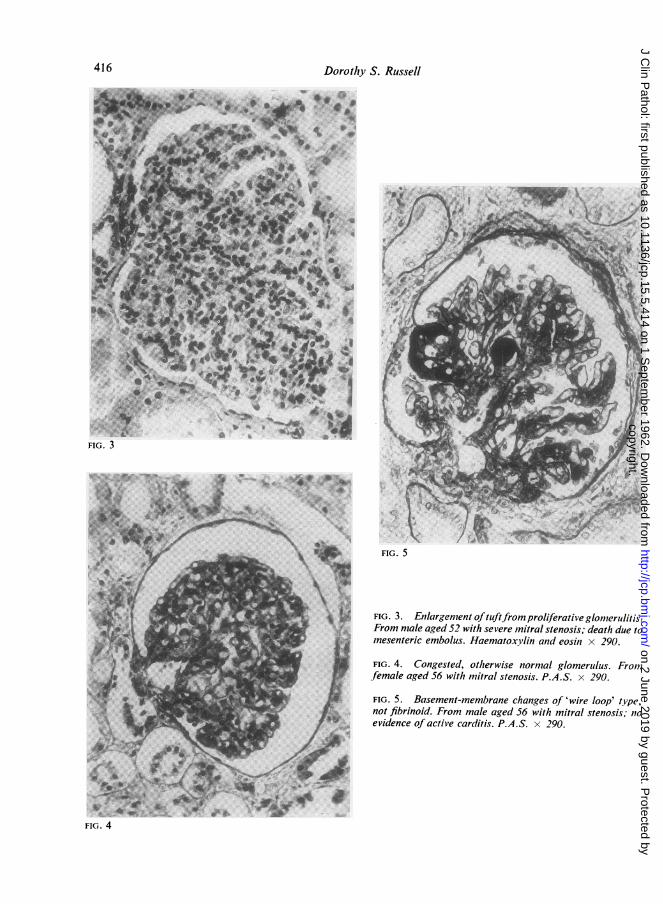
2 PROLIFERATIVE GLOMERULITIS In 76 cases theglomeruli principally showed proliferative glomeru-litis. This change, when advanced, caused enlarge-ment of the tuft (Fig. 3) in excess of any that couldbe attributed to simple back-pressure congestion(Fig. 4). Both the endothelial proliferation andthickening of basement membranes varied in degreeand distribution. Although widespread when present,a number of the glomeruli, or part of an affectedtuft, might appear normal. Thickening of basementmembranes can only be correctly assessed by specialstains, the appearances in haematoxylin-and-eosinpreparations being frequently deceptive. The P.A.S.method proved the most reliable, demonstrating thatthe thickening is due to an increase of fine, inter-woven fibrils between the capillary loops and not ofthe 'wire-loop' character seen in disseminated lupuserythematosus. In one case only was this pictureequivocal (Fig. 5). The centres of lobules were moreaffected than the periphery and, when the hilarregion was involved, there was sometimes in con-tinuity a peri-adventitial increase of fibrils and cellsabout the glomerular arterioles. Figs. 6 to 9 inclusiveillustrate moderate or lesser degrees of proliferative
415
copyright. on 2 June 2019 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.15.5.414 on 1 Septem
ber 1962. Dow
nloaded from
Dorothy S. Russell
FIG. 3
*V. .;..:- zwk
FIG. 5
FIG. 3. Enlargement /ftuftfrom proliferative glomerulitis.From male aged 52 with severe mitral stenosis; death due tomesenteric embolus. Haematoxylin and eosin x 290.
FIG. 4. Congested, otherwise normal glomerulus. Fromfemale aged 56 with mitral stenosis. P.A.S. x 290.
FIG. 5. Basement-membrane changes of 'wire loop' type,not fibrinoid. From male aged 56 with mitral stenosis; 11oevidence of active carditis. P.A.S. x 290.
416
od,
copyright. on 2 June 2019 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.15.5.414 on 1 Septem
ber 1962. Dow
nloaded from
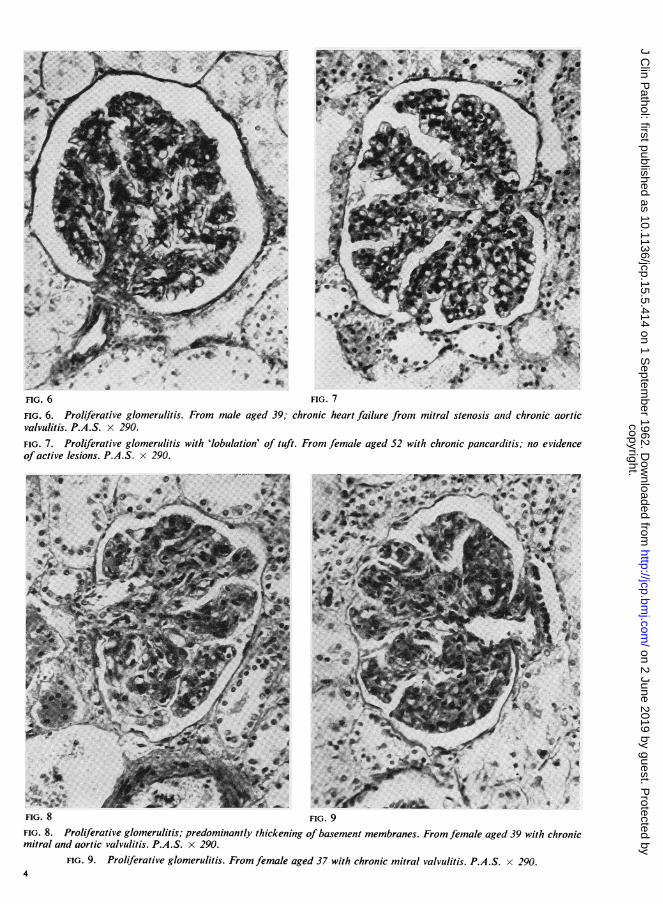
FIG. 6 FIG. 7
HIG. 6. Proliferative glomerulitis. From male aged 39; chronic heart failure fromn mitral stenosis anid chronic aorticvalvulitis. P.A.S. x 290.FIG. 7. Proliferative glomerulitis with 'lobulation' of tuft. From female aged 52 with chronic pancarditis; no evidenceof active lesions. P.A.S. x 290.
sswr o'- t j +fA j W
*44
.:A A.A.2W
HIG. 8 FIG. 9
HIG. 8. Proliferative glomerulitis; preominanly thd3;hickigo baement memburaes.ro Frmita ftemalesaged39wtchronicarimtaanaotcvalvulitis. P.A.S. x 290.
FIG. 9.Prolifnerative glomerulitiswt lblto'ouf.From fema leaged37 with chronicmitrl vlvu itis.PnoSx vi290.
Ft> t ; il r5~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~4S,;f
FIG. 8 FIG. 9FIG. 8. Proliferative glomerulitis; predominantly thickening of basement membranes. From female aged 39 with chronicmitral and aortic valvulitis. P.A.S. x 290.
FIG. 9. Proliferative glomerulitis. From female aged 37 with chronic mitral valvulitis. P.A.S. x 290.
copyright. on 2 June 2019 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.15.5.414 on 1 Septem
ber 1962. Dow
nloaded from
Dorothy S. Russell
W
FIG. 10
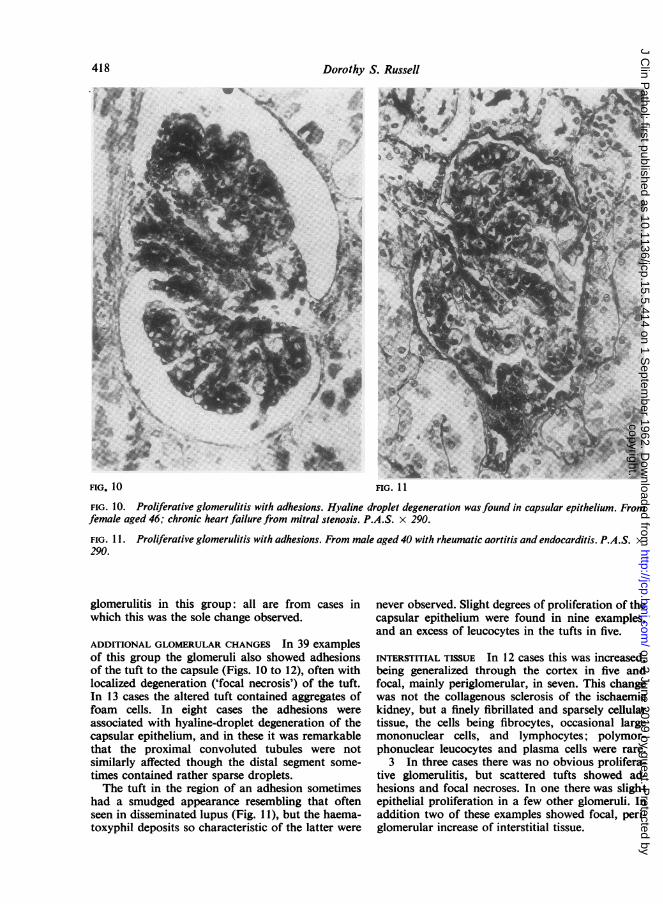
FIG. 10. Proliferative glomerulitis with adhesions. Hyaline droplet degeneration was found in capsular epithelium. Fromfemale aged 46; chronic heart failure from mitral stenosis. P.A.S. x 290.
FIG. I 1. Proliferative glomerulitis with adhesions. From male aged 40 with rheumatic aortitis and endocarditis. P.A.S. x290.
glomerulitis in this group: all are from cases inwhich this was the sole change observed.
ADDITIONAL GLOMERULAR CHANGES In 39 examplesof this group the glomeruli also showed adhesionsof the tuft to the capsule (Figs. 10 to 12), often withlocalized degeneration ('focal necrosis') of the tuft.In 13 cases the altered tuft contained aggregates offoam cells. In eight cases the adhesions wereassociated with hyaline-droplet degeneration of thecapsular epithelium, and in these it was remarkablethat the proximal convoluted tubules were notsimilarly affected though the distal segment some-times contained rather sparse droplets.The tuft in the region of an adhesion sometimes
had a smudged appearance resembling that oftenseen in disseminated lupus (Fig. 11), but the haema-toxyphil deposits so characteristic of the latter were
never observed. Slight degrees of proliferation of thecapsular epithelium were found in nine examples,and an excess of leucocytes in the tufts in five.
INTERSTITIAL TISSUE In 12 cases this was increased,being generalized through the cortex in five andfocal, mainly periglomerular, in seven. This changewas not the collagenous sclerosis of the ischaemickidney, but a finely fibrillated and sparsely cellulartissue, the cells being fibrocytes, occasional largemononuclear cells, and lymphocytes; polymor-phonuclear leucocytes and plasma cells were rare.
3 In three cases there was no obvious prolifera-tive glomerulitis, but scattered tufts showed ad-hesions and focal necroses. In one there was slightepithelial proliferation in a few other glomeruli. Inaddition two of these examples showed focal, peri-glomerular increase of interstitial tissue.
418l.""
r
copyright. on 2 June 2019 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.15.5.414 on 1 Septem
ber 1962. Dow
nloaded from
The kidney in rheumatic heart disease
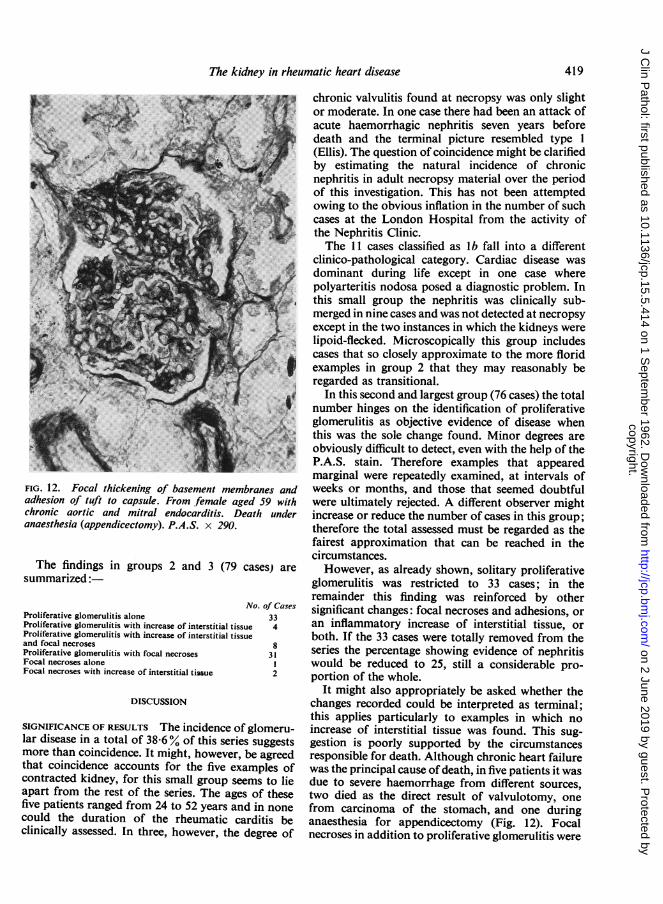
FIG. 12. Focal thickening of basement membranes andadhesion of tuft to capsule. From.female aged 59 withchronic aortic and mitral endocarditis. Death underanaesthesia (appendicectomy). P.A.S. x 290.
The findings in groups 2 and 3 (79 cases) are
summarized:
No. of CasesProliferative glomerulitis alone 33Proliferative glomerulitis with increase of interstitial tissue 4Proliferative glomerulitis with increase of interstitial tissueand focal necroses 8Proliferative glomerulitis with focal necroses 31Focal necroses alone IFocal necroses with increase of interstitial tissue 2
DISCUSSION
SIGNIFICANCE OF RESULTS The incidence of glomeru-lar disease in a total of 38-6% of this series suggestsmore than coincidence. It might, however, be agreedthat coincidence accounts for the five examples ofcontracted kidney, for this small group seems to lieapart from the rest of the series. The ages of thesefive patients ranged from 24 to 52 years and in nonecould the duration of the rheumatic carditis beclinically assessed. In three, however, the degree of
chronic valvulitis found at necropsy was only slightor moderate. In one case there had been an attack ofacute haemorrhagic nephritis seven years beforedeath and the terminal picture resembled type 1(Ellis). The question of coincidence might be clarifiedby estimating the natural incidence of chronicnephritis in adult necropsy material over the periodof this investigation. This has not been attemptedowing to the obvious inflation in the number of suchcases at the London Hospital from the activity ofthe Nephritis Clinic.The 11 cases classified as lb fall into a different
clinico-pathological category. Cardiac disease wasdominant during life except in one case wherepolyarteritis nodosa posed a diagnostic problem. Inthis small group the nephritis was clinically sub-merged in nine cases and was not detected at necropsyexcept in the two instances in which the kidneys werelipoid-flecked. Microscopically this group includescases that so closely approximate to the more floridexamples in group 2 that they may reasonably beregarded as transitional.
In this second and largest group (76 cases) the totalnumber hinges on the identification of proliferativeglomerulitis as objective evidence of disease whenthis was the sole change found. Minor degrees areobviously difficult to detect, even with the help of theP.A.S. stain. Therefore examples that appearedmarginal were repeatedly examined, at intervals ofweeks or months, and those that seemed doubtfulwere ultimately rejected. A different observer mightincrease or reduce the number of cases in this group;therefore the total assessed must be regarded as thefairest approximation that can be reached in thecircumstances.However, as already shown, solitary proliferative
glomerulitis was restricted to 33 cases; in theremainder this finding was reinforced by othersignificant changes: focal necroses and adhesions, oran inflammatory increase of interstitial tissue, orboth. If the 33 cases were totally removed from theseries the percentage showing evidence of nephritiswould be reduced to 25, still a considerable pro-portion of the whole.
It might also appropriately be asked whether thechanges recorded could be interpreted as terminal;this applies particularly to examples in which noincrease of interstitial tissue was found. This sug-gestion is poorly supported by the circumstancesresponsible for death. Although chronic heart failurewas the principal cause of death, in five patients it wasdue to severe haemorrhage from different sources,two died as the direct result of valvulotomy, onefrom carcinoma of the stomach, and one duringanaesthesia for appendicectomy (Fig. 12). Focalnecroses in addition to proliferative glomerulitis were
419
copyright. on 2 June 2019 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.15.5.414 on 1 Septem
ber 1962. Dow
nloaded from
Dorothy S. Russeli
found in three of these cases, and in two there wasan increase of interstitial tissue.
ACTIVITY OF THE RHEUMATIC CARDITIS Evidence ofactivity was provided by the macroscopic descriptionof the characteristic vegetations and, when available,the examination of histological preparations. Thelatter were not always satisfactory and, indeed, anexhaustive examination of the heart would benecessary if evidence of rheumatic activity were tobe positively excluded. But such an examination hasnot been feasible in an enquiry of this kind. Subjectto these limitations it can only be stated that 30%of the group with glomerular changes had positiveevidence of active inflammation in the heart, whereasactivity was found in 19% in the group with norenal inflammation.
AGE INCIDENCE All decades, from the first to theeighth, are represented in both the nephritic andnon-nephritic groups. On analysis there appears tobe little difference between them: the second andthird decades are better represented in the formerthan in the latter, but in both the greatest number ofcases falls in the fourth to sixth decades. The actualfigures for consecutive decades are: (a) nephritic,1, 12, 15, 21, 16, 22, 6, 1, 1; (b) non-nephritic, 5, 8,9, 22, 41, 39, 21, 6.
EVIDENCE OF NEPHRITIS The renal implications ofrheumatic carditis were not detected clinically, withthe exception of those patients, already mentioned,who died in uraemia. Cardiac failure dominated thepicture; albuminuria and oedema were naturallyattributed to this and haematuria, if present, couldbe explained by infarction. Blood-urea estimationswere available in only 14 cases, seven of these beingin group 1. In the seven of group 2 the figures rangedfrom normal to 78 mg. % except in one case where300 mg. was recorded two months before death.
This man, aged 45, was admitted with chronicmitral and aortic endocarditis. The urine contained9/10 albumin and a deposit of leucocytes, redcorpuscles, granular and hyaline casts. He wasdischarged, one month before death, with grossanasarca and pleural effusions. At necropsy deathwas attributed to serofibrinous pericarditis. Therewas chronic endocarditis of the aortic and mitralvalves, with slight stenosis of the latter and micro-scopic evidence of active inflammation. In thekidneys a uniform diffuse fibrosis pervaded the
cortex and extended into the upper medulla. Thistissue appeared oedematous and contained scantyfibroblasts mixed with an uneven, rather sparseinfiltration of lymphocytes, plasma cells, occasionallarge mononuclear cells and neutrophil leucocytes.Proliferative glomerulitis was slight and focal.Hyaline-droplet degeneration of the capsularepithelium was associated with slight focal cellularproliferation, adhesions, and focal necroses. Iso-tropic fatty droplets occupied the epithelium of theconvoluted tubules and hyaline droplets were foundin the ascending loops of Henle. Bulky eosinophilhyaline casts were numerous.These details illustrate the kind of case in which
nephritis might well be suspected clinically. In thisinstance a nephrotic syndrome (though informationabout the plasma proteins is lacking) was associatedwith raising of the blood urea and renal changes thathave points in common with Bright's disease but donot lend themselves to any existing classification.The case also demonstrates the artificiality ofseparating the small group of 11 cases (lb) fromgroup 2: it is clearly transitional.
In conclusion, the findings in the present investi-gation support those of Bell (1932), and suggest thedesirability of further investigation of this problemboth clinically and in the laboratory. The surprisingnegative results reported by Baehr and Schifrin (1932)may be partly accounted for by their exclusion ofcases over 31 years old for, in the present series, mostof the glomerular changes were found in older sub-jects. This in itself suggests that successive attacks ofcarditis may generate an immunological state inwhich the kidneys become vulnerable, by analogywith disseminated lupus. On the other hand, theincidence of glomerulonephritis in any seriesinvestigated might depend in its turn upon theincidence of infection with nephritogenic strains ofgroup A streptococci (Rammelkamp and Weaver,1953). Further speculation is unprofitable until thebackground of combined renal and cardiac diseasein rheumatism is more fully investigated.
REFERENCES
Allen, A. C. (1951). The Kidney, p. 110. Grune and Stratton, NewYork.
Baehr, G., and Schifrin, A. (1932). In Libman Anniversary Volumes,Vol. 1, p. 125. International Press, New York.
Bell, E. T. (1932). Amer. J. Path., 8, 639.Rammelkamp, C. H., Jr., and Weaver, R. S. (1953). J. clin. Invest.,
32, 345.
420
copyright. on 2 June 2019 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.15.5.414 on 1 Septem
ber 1962. Dow
nloaded from