Embed Size (px)
DESCRIPTION
November Journal
Citation preview
THE
KentuckyPharmacist
News & Information for the Kentucky Pharmacist Association
Vol. , No. 6 6 November 2011
Congratulations to the KPhA Golf Team who finished first place in their flight at
UK College of Pharmacy Scholarship Golf Outing! Duane Parsons, Tyler Whisman,
Clay Rhodes and Jeff Mills made up the winning team.
More than 100 students from the University of Kentucky and Sullivan University Colleges
of Pharmacy attended KPhA Pharmacy Student Legislative Day 2011 on Nov. 16, 2011 at
the Kentucky Capitol.

THE
KENTUCKY PHARMACIST1
At this time, I vow to devote my professional life to the service of all humankind through the profession ofpharmacy.
I will consider the welfare of humanity and relief of human suffering my primary concerns.
I will apply my knowledge, experience, and skills to the best of my ability to assure optimal drug therapyoutcomes for the patients I serve.
I will keep abreast of developments and maintain professional competency in my profession of pharmacy.
I will embrace and advocate change in the profession of pharmacy that improves patient care.
I take these vows voluntarily with the full realization of the responsibility with which I am entrusted bythe public.
Kentucky Pharmacists AssociationThe mission of the Kentucky Pharmacists Association is to promote the profession of pharmacy, enhance thepractice standards of the profession, and demonstrate the value of pharmacist services within the health care system.
The Kentucky Pharmacy Education and Research Foundation (KPERF), established in 1980 as a non-profit subsidiary corporationof the Kentucky Pharmacists Association (KPhA), fosters educational activities and research projects in the field of pharmacyincluding career counseling, student assistance, post-graduate education, continuing and professional development and public healtheducation and assistance.
It is the goal of KPERF to ensure that pharmacy in Kentucky and throughout the nation may sustain the continuing need forsufficient and adequately trained pharmacists. KPERF will provide a minimum of 15 continuing pharmacy education hours. In addition, KPERF will provide at least three educational interventions through other mediums such as webinars to continuously improve healthcare for all. Programming will be determined by assessing the gaps between actual practice and ideal practice, with activities designed to narrow those gaps using interaction, learning assessment, and evaluation. Additionally, feedback from learners will beused to improve the overall programming designed by KPERF.
Copyright 2011 to the Kentucky Pharmacists Association. The Kentucky Pharmacist is the official journal of the KentuckyPharmacists Association published by-monthly. The Kentucky Pharmacist is distributed to KPhA members, paid through allocationsof membership dues. All views expressed in articles are those of the writer, and not necessarily the official position of the KentuckyPharmacists Association. Editorial, advertising and executive offices at 1228 US 127 South Frankfort, KY 40601.Phone 502.227.2303 Fax 502.227.2258 email [email protected] website http://www.kphanet.org
Editorial Office:
Oath of a Pharmacist
President’s Perspective
INCAPPS
Continuing Education - Reviewing Diabetes
November Tech/Pharmacists Quiz
Pharmacy Time Capsules
Grass Roots
Continuing Education - Where Does The Needle Go
November Tech/ Pharmacists Quiz
Pharmacy Law Brief
Pain Relief Act
Table of Contents....Oath....Mission Statement Education Beyond the classroom
Pharmacists Mutual
Continuing Education - Effective Communications
December Tech/Pharmacists Quiz
Pharmacy Policy Brief
Proclamation
CAPP
Save the date/ASPC
Frequently Called & Contacted
Board of Directors
1
2
5
7
13
14
15
18
25
26
28
29
30
31
42
43
45
47
48
49
50
Table of Contents . . . Oath....Mission Statement..... November 2011

THE
KENTUCKY PHARMACIST2
November 2011President’s Perspective.
THE
KENTUCKY PHARMACIST3
President’s Perspective. November 2011

THE
KENTUCKY PHARMACIST4
President’s Perspective. November 2011
facing independent pharmacy. From this
meeting, a new Academy for independents
has been established. The Board has
approved the Academy, and we are
currently working with leaders of the
Academy, Rosemary Smith, Luther Smith,
Jason Wallace, Jonathan Van Lahr, Leon
Claywell, Clay Rhodes, and others to
develop the organizational structure. These
individuals, along with many others, have
been very influential in leading efforts
addressing all the issues related to the
introduction of three new MCOs into our
KY Medicaid population. Their passion for
pharmacy and the efforts they are putting
forward, I believe, benefit all areas of
pharmacy. I’m excited to have them as a
new Academy in KPhA, and I hope their
enthusiasm encourages others with like
interest to consider forming an Academy
within KPhA. Please contact the office if
you have questions about how to form an
Academy.
Our Academy for Long Term Care Pharmacy
has been active with several issues related
to the nursing home industry both on a
state and national level. These include
developing new LTC pharmacy regulations
to present to the Board of Pharmacy,
addressing a proposed rule by CMS to
separate consultant pharmacists practice
from the dispensing pharmacy, and
addressing a pain relief bill to assure LTC
residents can receive timely pain
medications. Bob Bunting, Leah Tolliver
and Peggy Canler are providing strong
leadership in this area. Please contact them
for additional information or interest in
joining this Academy.
It’s obvious to see that there is a lot of
activity going on within our Association, and
from my first few months in the office, I can
tell you that this is only the beginning.
Because of the environment we are in
today, the need for your involvement in our
Association is more critical than ever. Many
exciting opportunities to be involved and
shape our profession will be developing
over the next few months. We have just
hired a new Director of Communication and
CE, Scott Sisco, and are excited to have him
on board and increase our efforts in
these areas. Please watch for
announcements through eNews, Facebook,
Twitter, email, fax blasts, etc. More than
that, don’t just watch for them, RESPOND
to them and be an active, engaged
contributor in shaping your Association and
profession!
Connect with
KPhA online!
Facebook Fan Page
www.facebook.com/KyPharmAssoc
www.twitter.com/KyPharmAssoc
Website
www.kphanet.com

THE
KENTUCKY PHARMACIST5
November 2011
Sullivan University College of Pharmacy: Experiences and Initiatives of the InterNational Center for Advanced Pharmacy Services (INCAPS)
BC Childress, PharmD; Assistant Professor and Director of the InterNational Center for Advanced Pharmacy
Services (INCAPS) at Sullivan University College of Pharmacy
Dean Hieu T Tran, PharmD; Founding Dean and Professor of the Sullivan University College of Pharmacy
The practice of pharmacy is evolutionary. Often in our recent history, the scope of practice and the clinical reach of pharmacists have adapted with the times. Pharmacy pushes forward, and is now more than dispensing medication and educating patients—a pharmacist is an integrated member of the healthcare team. From the adoption of the Doctor of Pharmacy degree (PharmD) to the surge in pharmacy residencies, it is clear that pharmacists are rising to meet the demands of a changing healthcare system.1 Even many practicing pharmacists voluntarily seek to further hone their skills through Board Certification Specialties, Master’s Degrees, or specialty certifications—such as Certified Geriatric Pharmacist (CGP) or Certification in Medication Therapy Management.2,3 As clinical practice follows this evolutionary course, pharmacists must be taught and trained to fit these roles early in their education. At the Sullivan University College of Pharmacy, innovative and new clinical services have been developed, and a revolutionary new Advanced Pharmacy Practice Experience has been created specifically to meet that crucial need.
It is not easy to establish educational programs that teach students all the components of Medication Therapy Management (MTM). Often, only classroom learning and self-study can be provided, but training students to competently provide these services requires much more detailed consultation training. In order to better educate pharmacy students in the provision of MTM services, Sullivan
University College of Pharmacy (SUCOP) has built a collaboration with one of the nation’s leading Pharmacy Benefit Managers—HUMANA. HUMANA and SUCOP have joined forces for a mission that is two-fold:
1. Provide students on Advanced Pharmacy Practice Experience (APPE) rotations with hands-on MTM experience consulting with real patients. These experiences encourage continued pharmacist participation in MTM following graduation.
2. Utilize student pharmacists in aiding HUMANA’s mission to provide perfect service to its patients that are eligible for MTM benefits.
This partnership between an academic institution and a pharmacy benefit manager is the first of its kind. Benefits of this collaboration include training and education for the students and a certificate program developed for participants. As APPE students perform MTM services during their rotation necessary for graduation, they will be eligible to receive an official certification in the Delivery of Medication Therapy Management.
This new training ground for APPE students is a vital part to the mission of the InterNational Center for Advanced Pharmacy Services (INCAPS). For almost 3 years now, since its establishment in March 2009, INCAPS has been at the cutting edge of pharmacy practice—integrating collaborative practice with physicians, medication therapy management
INCAPPS
THE
KENTUCKY PHARMACIST6
November 2011
services, and immunization delivery into a specialized ambulatory care clinic housed at SUCOP. Prior to this latest collaboration with HUMANA, INCAPS has been a source of interprofessional experiential education for pharmacy students, and has provided vast amounts of hands-on training in various areas of MTM services.
Since 2009, INCAPS has worked in collaboration with the Louisville Metro Department of Public Health to offer vaccinations across Jefferson County. These sites ranged from Louisville Metro fire and police departments, to the Jefferson County public high schools. Since this time, faculty and students on rotation at INCAPS have administered thousands of vaccines. Also in 2009 INCAPS began collaboration with the locally run MD2U: Physicians who make house calls. As part of this team effort, the clinical pharmacists and APPE students of INCAPS have made house calls to patient referrals in order to provide immunizations, patient education, and MTM services. In addition to these, INCAPS has been a major supporter of the RxTherapy Management program of the Kentucky Pharmacists Association, and as of 2011 provides MTM services to over 500 eligible patients in the Commonwealth of Kentucky alone. With this program, students are trained to help educate patients and work with their primary care providers to improve both their quality of life as well as medication therapy. Since its inception in 2009, INCAPS faculty and students have been part of over 2000 MTM consults, multiple health and wellness fairs, and various educational classes and programs in the community. All of the services provided utilized APPE students in the design and delivery.
As the practice of pharmacy continues to evolve, it is the type of innovation modeled by INCAPS at Sullivan University College of Pharmacy that will continue to pave the way for future pharmacists to be a vital part of the healthcare team. As healthcare reform creates waves for change and the value of pharmacy-
driven MTM grows, other Pharmacy Academies throughout the country may seek to emulate this type of practice model in order to better train students to perform MTM services.
INCAPS is always open to further collaborate and support other groups or institutions in the continued development and implementation of these services. For more information, please contact the Sullivan University College of Pharmacy at 502-413-8640. Questions can also be directed to Dr. BC Childress, the Director of INCAPS at Sullivan University College of Pharmacy.
Sullivan University College of Pharmacy, Office of the Dean (502) 413-8640 BC Childress, PharmD Director of the InterNational Center for Advanced Pharmacy Services (INCAPS) (502) 413-8991 [email protected] References:
1. Murphy JE, Nappi JM, Bosso JA, et al. American College of Clinical Pharmacy’s vision of the future: postgraduate pharmacy residency training as a prerequisite for direct patient care practice. Pharmacotherapy 2006;26:722–33.
2. Delivering Medication Therapy
Management Services in the
Community. !merican Pharmacist’s
Association 2011. Available at:
http://www.pharmacist.com/AM/Temp
late.cfm?Section=Delivering_Medicatio
n_Therapy_Management_in_the_Com
munity. Accessed on: July 22, 2011.
3. MS in Pharmacy Medication Therapy
Management Online. University of
Florida 2011. Available at:
http://pharmd.distancelearning.ufl.edu
/mtm-program/. Accessed on: July 22,
2011.
INCAPPS

THE
KENTUCKY PHARMACIST7
November 2011Reviewing Diabetes
Reviewing Diabetes Guidelines
Compiled by Danny Jaek, Pharm.D. Candidate
Judy Thompson, PharmD, BCPS, CDE, Preceptor
There are no financial relationships to disclose.
Universal Activity # 0143-9999-11-061-H01-P
1.0 Credit Hours (0.1 CEUs)
Reprinted with permission of the authors and the Alaska Pharmacists Association where this article
originally appeared.
Objectives:
At the conclusion of this knowledge-based lesson, successful participants should be able to:
• Describe the treatment algorithms for type 2 diabetes from the American Diabetes Association and
from the American Association of Clinical Endocrinologists.
• Identify the goals of therapy for diabetes treatment.
• Discuss the role of new agents to treat diabetes.
There are nearly 24 million Americans with
diabetes in the United States, and every year
1.3 million people are diagnosed with type 2
diabetes. That translates to nearly 3,500
persons a day! In order to manage this growing
epidemic, we must incorporate several different
treatment modalities to best manage care for
our patients with diabetes: lifestyle changes,
preventative health screenings, nutrition
counseling, medications, and support groups.
Even among the diabetes medications, there
are over twenty different choices on the market
today. How do we provide the best care
possible when there are so many options
available?
The Guidelines
There are several groups that have published
their own set of guidelines for the treatment of
type 2 diabetes in non-pregnant adult patients.
Both the American Diabetes
Association/European Association for the Study
of Diabetes (ADA/EASD) and the American
Association of Clinical
Endocrinologists/American College of
Endocrinology (AACE/ACE) are leading
organizations that have produced guidelines
outlining a treatment roadmap for optimal care
of patients with diabetes. While these
documents advocate many similar practice
principles, it is important to consider the
differences between the two. The provider
must ultimately tailor diabetes treatment to the
individual patient in accordance with published
guidelines and clinical experience.
Monitoring Diabetes
When monitoring patients with diabetes,
both organizations advocate the use of
regular hemoglobin A1C testing. Regular

THE
KENTUCKY PHARMACIST8
November 2011Reviewing Diabetes
testing, at least two times per year in
patients meeting treatment targets and
quarterly in patients who are not meeting
goals or whose therapy has changed. This
blood test provides an approximate 3 -
month snapshot of an individual’s glycemic
control. The ADA recommends an A1C goal
of ≤7% while the AACE/ACE goal is ≤6.5%.
Each publication provides justification for
its respective recommendation. For most
patients the ADA prefers a less -intensive
goal to prevent hypoglycemic events. The
ADA advocates for providers to consider
lower A1C goals for individual patients, if
this can be achieved without significant
hypoglycemia. These patients generally
have a shorter duration of diabetes, long
life expectancy and no significant CVD. In
contrast, the AACE/ACE advocates for an
!1C goal of ≤6.5% for all patients.
Therapeutic Options
Both organizations have published their
own algorithms for treating individuals with
type 2 diabetes. The AACE/ACE guidelines
determine a patient’s treatment by
stratifying individuals according to their
current A1C level. The AACE/ACE algorithm
cites six goal priorities for medication
selections-
1. minimize risk and severity of
hypoglycemia
2. minimize risk of weight gain
3. include major classes of FDA
approved medications
4. selection of therapy based on A1C
stratification and documented
ability of medication to lower A1C
5. consideration of both fasting and
post prandial glucose as targets
6. consideration of total cost of
therapy including medication,
supplies, hypoglycemia, adverse
events and diabetes associated
complications.
For patients with A1C levels of 7.5% or
lower AACE/ACE concludes a goal of 6.5%
can be achieved with monotherapy.
Metformin is the preferred agent and is
usually the most appropriate initial choice
unless there is a contraindication, such as
renal disease. If A1C goals are not being
reached, the guidelines recommend
additional oral medications first, then
insulin if A1C levels are still high. If insulin is
to be started in a patient, there are four
general approaches that can be taken:
. basal insulin, using a long-acting
insulin (glargine or detemir),
generally given once daily; . premixed insulins, using a rapid-
acting analogue and protamine
(NovoLog or Humalog Mix), usually
given twice daily with breakfast and
dinner but occasionally used only
with the largest meal; . basal-bolus insulin or multiple daily
injections, using rapid-acting insulin
analogues at mealtime—aspart,
lispro, or glulisine along with one of
the long-acting insulin analogues,
glargine or detemir; . a meal-time insulin regimen,
involving use of the rapid-acting

THE
KENTUCKY PHARMACIST9
November 2011Reviewing Diabetes
insulin analogues, but without a
basal or long-acting insulin
component is an additional option.
This may be possible if the patient is
being treated with an insulin
sensitizer (metformin) that provides
adequate control of fasting plasma
glucose.
The AACE/ACE guidelines recommend
against the use of intermediate-acting
insulins such as insulin N or insulin R
because their duration of action does not
adequately mimic the body’s normal
physiology. As a result, these agents are
often associated with an increased risk of
hypoglycemia.
Figure 1 details the AACE/ACE stratification
by A1C and recommended combinations
based on the patients A1C. For example,
according to the AACE/ACE guidelines a
patients whose A1C is 8%, would have the
provider consider four different medication
combinations
1. Metfomrin plus a GLP-1
2. Metformin plus a DPP-4 inhibitor
3. Metformin plus a TZD
4. Metformin plus a sulfonylurea or
glinide
ADA/EASD Guidelines
The ADA guidelines selected specific therapies
on their effectiveness in lowering glucose,
extraglycemic effects that may reduce long
term complications, the medications safety
profile, tolerability, ease of use, and cost. The
algorithm takes into account the characteristics
of the individual interventions and advocates
Figure 1

THE
KENTUCKY PHARMACIST10
November 2011Reviewing Diabetes
for aggressive lowering of glycemia as close to
the time of diagnosis as possible. Similarly to
AACE/ACE, metformin is the preferred initial
agent along with lifestyle changes (diet,
exercise, and weight loss). If lifestyle
intervention and the maximal tolerated dose of
metformin fail to achieve glycemic targets,
another medication should be added within 2-3
months. If A1C is less than 8.5%, a sulfonylurea
(other than glyburide or chlorpropamide) or
basal insulin should be added. Higher A1C’s
should be treated with
metformin and insulin.
The algorithm also
includes second-line “less
well-validated” therapies
(i.e. less clinical trial data,
less outcome data, and
less clinical experience
than other therapies) for
use in selected clinical
settings such as a
reduced risk of hypoglycemia. These options
suggest using pioglitazone or a GLP-1 agonist
(exenatide or liraglutide) in addition to
metformin and lifestyle changes. Although
addition of a third agent can be considered, this
approach is usually not preferred since the
same level of glycemic control can be achieved
with insulin.
The ADA algorithm provides specific
instructions for initiating and maintaining a
patient on insulin. They recommend starting
with bedtime intermediate-acting insulin or
bedtime or morning long-acting insulin at a
dose of 10 units or 0.2 units per kilogram.
Regular monitoring of fasting blood glucose
levels in the morning should be performed so
the insulin dose can be
titrated, typically by 2
units every few days, to
achieve fasting glucose
levels of 70-130 mg/dL. If
A1C levels are above
target after 2-3 months,
blood glucose testing
should be performed
before lunch, dinner, and
bedtime to determine if additional meal-time
injections are needed. While on insulin, both
sets of guidelines recommend discontinuing
diabetes drugs that either increase the risk of
hypoglycemia or are not approved for use with
Figure 2

THE
KENTUCKY PHARMACIST11
November 2011Reviewing Diabetes
insulin (sulfonylureas and exenatide).
Metformin should continue to be administered
with insulin unless the patient develops a
contraindication.
Newer Agents
Both sets of guidelines address the role of
newer classes of diabetes medications that are
helping patients manage their disease.
Glucagon-like peptide-1 (GLP-1) agonists such
as exenatide and liraglutide are two injectable
drugs that stimulate the pancreas to release
insulin at mealtimes, decrease glucagon release,
and increase satiety. Dipeptidyl peptidase 4
(DPP-4) inhibitors such as sitagliptin, saxagliptin,
and the recently approved linagliptin are oral
agents that enhance the effect of GLP-1 by
preventing its breakdown. These agents reduce
a patient’s A1C by approximately 0.5 to 1% with
relatively little risk of hypoglycemia. and are
weight neutral or support weight loss.
In light of these observations, the AACE/ACE
guidelines favor the use of these agents over
sulfonylureas or thiazolidinediones when
adding on to metformin therapy. On the other
hand, the ADA guidelines consider these agents
to be “less well-validated” therapies.
Self-Monitored Blood Glucose
Self-monitoring of blood glucose (SMBG) is an
important element in adjusting or adding new
drug therapies and, in particular, titrating
insulin doses. The need for and number of
required SMBG measurements are not clear
and are dependent on the medications used.
Oral agents that are not likely to cause
hypoglycemia do not usually require SMBG.
The AACE/ACE guidelines recommend daily
SMBG checks for patients on bedtime basal
insulin or dinnertime premixed insulin. For
each additional injection of insulin per day,
SMBG should be increased in frequency to
ensure successful titration of each dose. The
ADA guidelines suggest targeting daily fasting
and preprandial glucose levels when SMBG is
employed. ADA guidelines target a fasting
plasma glucose of 90-130 mg/dL and a
postprandial plasma glucose of <180 mg/dL.
AACE/ACE guidelines target a fasting plasma
glucose of <110 mg/dL and a postprandial
plasma glucose of <140 mg/dL.
The implications of uncontrolled diabetes can
lead to long-term consequences that increase
human suffering and reduced quality of life.
Much of the complications that occur can be
substantially reduced by interventions that
achieve glucose levels close to the nondiabetic
range. When we use guidelines provided by the
leading organizations in diabetes, the American
Diabetes Association, the European Association
for the Study of Diabetes, the American
Association of Clinical Endocrinologists/
American College of Endocrinology we provide
an evidence-based level of diabetes care to our
patients.
References:
? Rodbard, H W, Jellinger, P S, Davidson, J A, et
al. (2009). Statement by an American
association of clinical
endocrinologists/American college of
endocrinology consensus panel on type 2
diabetes mellitus: An algorithm for glycemic
control. Endocrine practice, 15(6), 540-59.
? Nathan, D M, Buse, J B, Davidson, M B, et al.
(2009). Medical management of hyperglycemia
in type 2 diabetes: A consensus algorithm for
the initiation and adjustment of therapy: A
consensus statement of the American diabetes
association and the European association for

the study of diabetes. Diabetes care, 32(1), 193-
203.
? Ray, K, Seshasai, S R, Wijesuriya , S, et al.
(2009). Effect of intensive control of glucose on
cardiovascular outcomes and death in patients
with diabetes mellitus: A meta-analysis of
November 2011 — Reviewing Diabetes Guidelines
1) Which of the following organizations have published
guidelines for the treatment of Type 2 diabetes?
A. American Diabetes Association
B. American Association of Encocrinologists
C. American Academy of Pediatrics
D. A and B are correct
2) True or False: a patient with type 2 diabetes with a n A1C
level of 7.5% is considered at goal according to the ADA
guidelines.
A. True
B. False
3) LS is a 67-year old male with good renal function who has
just been diagnosed with diabetes. His A1C level is 7%.
Which of the following medications would be the most
appropriate first-line therapy?
A. Glyburide
B. Metformin
C. Rosiglitazone
D. Pioglitazone
4) All of the following are medications that increase the risk
of hypoglycemia except
A. Glyburide
B. Glipizide
C. Exenatide
D. Insulin aspart
5) Which of the following fasting blood glucose levels would
be in target for a patient with type 2 diabetes according to
the ADA guidelines?
A. 65 mg/dL
B. 109 mg/dL
C. 133 mg/dL
D. 140 mg/dL
6) Which of the following medications is not included in the
ADA algorithm’s two tiers of preferred agents?
A. Metformin
B. Pioglitazone
C. Basal insulin
D. Sitagliptin
7) JT is a 50 year old male currently being treated for type 2
diabetes with metforminH glipizideH and glargine. His
diabetes team has decided to add on bolus insulin to help
better control his blood glucose. Which of these
medications should be discontinued with the addition of
aspart?
A. Metformin.
B. Glipizide
C. Glargine
D. B and C are correct
8) GLP-1 agonist reduce a patient’s A1C by about
A. 0.2-0.5%
B. 0.5-1%
C. 1-2%
9) Which of the following basal-bolus insulin regimens are
correctly paired?
A. Detemir-glargine
B. Glulisine-aspart
C. Glargine-lispro
D. NPH-detemir
10) True or False: When initiating basal insulin, bedtime
long-acting insulin is an appropriate choice.
A. True
B. False
randomized controlled trials. Lancet,
373(9677), 1765-72.
? American Diabetes Association.
Standards of Medical Care in Diabetes -
2011. Diabetes Care. 2011;34 (Suppl 1):S11-
S61.
THE
KENTUCKY PHARMACIST12
November 2011Reviewing Diabetes

13
THE
KENTUCKY PHARMACIST
November Tech/Pharmacists Quiz November 2011

THE
KENTUCKY PHARMACIST14
Time Capsule November 2011

THE
KENTUCKY PHARMACIST15
Grass Roots November 2011
Students Take the Lead By Danielle Waymeyer and David Roy
Danielle Waymeyer is a third professional year student from Florence, Ky., who completed her pre-
professional course work at Thomas More College. David Roy is a first professional year student from Fort Thomas, Ky., who completed his pre-professional course work at Northern Kentucky University.
Both are students at the University of Kentucky College of Pharmacy in Lexington.
Participants in the visit to Ruwe Family Pharmacy included: Danielle Waymeyer, David Roy, Matt Stevens, Kelley Ratermann, Troy Stinson, Don Ruwe and Zach Thompson.
reimbursement models for pharmacists from
Medicare and Medicaid.
This initiative was kick-started by students Zach
Thompson, PharmD candidate 2014, and Kelley
Ratermann, PharmD candidate 2013, following
Kelley's stint as a student intern at the
American Pharmacists Association over the
summer. Efforts began in early September with
students identifying potential pharmacies
interested in collaborating to host pharmacy
visits with congressional representatives or
members of their staff. Persistence and
perseverance prevailed, and the students were
.
Focusing on the future, University of Kentucky
College of Pharmacy students recently began to
reach out to members of Kentucky's
Congressional delegation to highlight the value
of pharmacists' services. The first installment in
a statewide initiative was held on Oct. 25, 2011,
in Florence, Ky. (Congressional District 4). Matt
S t e v e n s , G r a n t D i r e c t o r a n d F i e l d
Representative for Congressman Geoff Davis'
office, visited Ruwe Family Pharmacy and
received the ideal therapeutic dose of
knowledge about the vital needs in the
c o m m u n i t y f o r m e d i c a t i o n t h e r a p y
m a n a g e m e nt a n d t h e n e e d fo r fa i r

THE
KENTUCKY PHARMACIST16
November 2011
KPhA Remembers KPhA desires to honor members who are no longer with us. Please keep KPhA
informed by sending this information to [email protected].
Deceased members for 2011 will be honored permanently at the KPhA office with a White Coat.
current care models and therapy management strategies. It was clearly shown that MTM services reduce medication errors, money spent for hospitalization as a result of those errors, in addition to improving quality of life and care to the aging population of patients in our society. Another tool that was used to present the necessity of these services was a patient session that included a quick demonstration about how MTM and interventions by pharmacists are successful methods in reducing cost, morbidity and hospitalizations. The encounter ended with a photograph session as well as an official "ask" session concerning the specific points of the meeting and Congressman Davis' stance on issues such as H.R. 891.
This first grassroots effort in Kentucky, designed to highlight the critical role of pharmacists and MTM in ensuring the safe and effective use of medications, was a success. This collaboration of student pharmacist and pharmacist constituents to host pharmacy visits is an effective model that should be explored and utilized for other grassroots efforts. Should you be contacted in the future about hosting such an event to showcase the capabilities of pharmacists, we hope you will join in.
= = = The authors acknowledge assistance from: Dr. Joseph Fink, Dr. Trish Freeman, Ms. Kelley R a t e r m a n n a n d M r. Z a c h T h o m p s o n
(Editor’s Note: A second visit to Commons Community Pharmacy is detailed on the followingpage)
.
.
. .
acknowledged for their efforts when a visit with Matt Stevens to Ruwe Family Pharmacy in District 4 was scheduled. The visit provided an opportunity for students to demonstrate their passion for pharmacy and request support for H.R. 891-Medication Therapy Management Benefits Act of 2011. This bill amends part D of Title XVIII of the Social Security Act to promote medication therapy management under the Medicare Part D prescription drug program. The official summary includes creation of a personal medication record and a recommended medication action plan in consultation with the individual and the prescriber; it also includes specific guidelines with regard to requiring prescription drug plan sponsors to reimburse pharmacists and other entities furnishing MTM services based on resources and time required to provide such services. The students were not a lone in these endeavors and were accompanied by UK faculty member and KPhA Board member, Trish Freeman, and student constituents of the 4th district - David Roy, Danielle Waymeyer and Troy Stinson (future 4th district constituent). Don Ruwe, pharmacist and owner/partner at Ruwe Family Pharmacy, hosted the visit and highlighted Ruwe Family Pharmacy's program, Aging in Place, and the model of care that he uses to support his patients in Florence and the surrounding counties.
During the visit, pharmacists and studentsvoiced their concerns regarding vital needs within the community that could be met with
.
Grass Roots

THE
KENTUCKY PHARMACIST17
November 2011KPhA Grass Roots Legislative Eforts
KPhA Grassroots Legislative Efforts
KPhA partnered with the UK
College of Pharmacy to bring
Congressman John Yarmouth to
Commons Community
Pharmacy in Louisville where he met with UK
students and staff of the pharmacy.
KPhA Pharmacy Student Legislative Day 2011
Yarmouth visits Commons Community Pharmacy Congressman John
Yarmouth discusses pharmacy industry issues
on his visit to Commons Community Pharmacy.
Congressman John Yarmouth talks with Dr. Chris Harlow.
Above: Jan Gould, Kentucky Retail Federaton Senior Vice President discusses how government and the profession of pharmacy are related; Right: More than 100 students from UK and Sullivan attended.
Senator Julie Denton, the featured speaker, explains how the legislature studies issues before making informed decisions.
THE
KENTUCKY PHARMACIST18
November 2011Where does the needle go?

THE
KENTUCKY PHARMACIST19
November 2011Where does the needle go?

THE
KENTUCKY PHARMACIST17
THE
KENTUCKY PHARMACIST20
November 2011Where does the needle go?

THE
KENTUCKY PHARMACIST21
November 2011
Although recommendations by the EPA provide guidance 22, state regulations do not consistently mirror them. For instance, Virginia regulations state that sharps should be placed in opaque, puncture-resistant containers. Once full, the lid should be securely taped onto the container and placed in a trashcan. These regulations do not specifically address any of the other options recommended by the EPA. 23 Since each locality can specify how sharps should be handled, it is important to find out what special procedures are required and what is available in each area. More information can be obtained through state laws and regulations or by contacting the local waste management authority.
Table 1. Advantages and Disadvantages Feature Drop Boxes/
Supervised Collection Sites
Mail-Back Programs
Syringe/ Needle Exchange Programs
At-Home Needle Destruction Devices
Special Waste Pick-up
Prevents sharps being introduced into the solid waste disposal system
Yes Yes Yes No Yes
Convenience of sites to all consumers
No Yes No Yes Yes
Availability to most consumers No Yes No Yes No
Costs supported by local government or community organizations
No No Yes No In some areas
Cost of the program to the consumer
Low High Moderate Low (clipping devices) Moderate-High (destruction devices)
Moderate
Privacy for the consumer No Yes No Yes Yes
Conclusion Each year, millions of patients in the United States administer medications via injections at home. The majority of these needles are discarded into the public solid waste system or improperly discarded. This poses a risk of injury. Needlestick injuries in the community are underreported thus the implications to public health underestimated. Monitoring mechanisms are not thorough and reporting compliance is low. Collaboration is needed between the government, community, hospitals and the research community to address and monitor the problem more effectively. The Coalition of Safe Community Needle Disposal is working with the EPA to increase awareness efforts. Current recommendations by the EPA for disposal include drop boxes/supervised collection sites, mail-back programs, syringe/needle exchange programs, at -home needle destruction devices, and resident special waste pick-up.
Where does the needle go?

THE
KENTUCKY PHARMACIST22
November 2011
As a pharmacist, it is important to learn more about what your state or locality offers and talk with your patients about the options available for safe disposal. It is important to talk with patients about their options and find the one that fits them the best Table 2. Resources
Resources Website
Organizations
United States Environmental Protection Agency (EPA)
http://www.epa.gov/osw/nonhaz/industrial/medical/disposal.htm
Center for Disease Control and Prevention (CDC)
http://www.cdc.gov/needledisposal/index.htm
Coalition of Safe Community Needle Disposal
http://www.safeneedledisposal.org/
International Sharps Injury Prevention Society
http://www.isips.org/
Syringe mail-back programs
Waste Management http://www.wm.com/products -and-services/residential-other-waste-solutions/syringe-collection.jsp
Sharps Compliance Corporation http://www.sharpsinc.com/disposal_mail_product_page.htm
Stericycle http://www.stericycle.com/consumer -needle-disposal.html
Medasend http://www.medasend.com/
Syringe destruction devices
Disentegrator® http://www.disintegratorplus.com/
NeedleZap® http://www.needlezap.com/in dex.html
BD Safe-Clip™ Device http://www.bd.com/us/diabetes/page.aspx?cat=7002&id=7416
References
1. Coalition of Safe Community Needle Disposal. http://www.safeneedledisposal.org/genprob.html. Accessed June 10, 2009.
2. United States Environmental Protect ion Agency (EPA). Community Options for Safe Needle Disposal. Oct. 2004. http://www.epa.gov/osw/nonhaz/industrial/medical/med -govt.pdf. Accessed June 10, 2009.
3. Mallin AR, Sinclair D. Needlestick injuries and potential body fluid in the emergency department. CJEM 2003; 5: 36-37.
4. Workbook for Designing, Implementing, and Evaluating a Sharps Injury Prevention Program. Division of Healthcare Quality and Promotion. Atlanta, GA: Centers for Disease Control and Prevention (CDC): 2008. [Available online at http://www.cdc.gov/sharpssafety/pdf/sharpsworkbook_2008.pdf.] Accessed June 10, 2009.
5. Occupational Safety and Health Administration (OSHA). Occupational exposure to bloodborne pathogens:needlesticks and other sharps injuries; final rule. Federal Register 2001; 66: 5317.
6. Center for Disease Control and Prevention. Syringe Disposal December 2005. Accessed on January 18, 2010. http://www.cdc.gov/idu/facts/aed_idu_dis.pdf.
7. Sandra C. Thompson. Blood-borne viruses and their survival in the environment: is public concern about community exposures justified? Aust and N Z J Public Health 2003; 27: 602-607.
8. Haber PS, Young MM, Dorrington L, Jones A, Kaldor J, Kanzow S, Rawlinson WD. Transmission of hepatitis C virus by needlestick injury in community settings. J Gastroenterol Hepatol 2007; 22: 1882-1885.
Where does the needle go?
THE
KENTUCKY PHARMACIST23
November 2011
9. Jagger J, Bentley MB. Disposal-related sharp-object injuries. Advances in Exposure Prevention 1995;1:1-6.
10. Panlilio AL, Orelien JG, Srivastava PU, Jagger J, Cohn RD, Cardo DM. Estimate of the annual number of percutaneous injuries among hospital-based healthcare workers in the United States, 1997-1998. Infect Control Hosp Epidemiol 2004;25:556-562.
11. O’Leary FM and Green TC. Community acquired needlestick injuries in non-health care workers presenting to an urban emergency department. Emerg Med 2003; 15: 434-440.
12. Handle with care: how to throw out used insulin syringes and lancets at home. EPA530 -K-99-008. Washington, DC: US Environmental Protection Agency, 1999.
13. Coalition of Safe Need Disposal. http://www.safeneedled isposal.org/gentypes.html. Accessed June 10, 2009.
14. Specifics of Local Jurisdictions Sharp Collection Programs. Accessed June 15, 2009. http://www.ciwmb.ca.gov/HHW/Sharps/LocalProgram.pdf .
15. New York State Directory of Community Sharps Collection Sites. A ccessed June 15, 2009. http://www.nyhealth.gov/diseases/aids/harm_reduction/needles_syringes/sharps/docs/nassau.pdf.
16. Michigan Department of Environmental Quality, Waste and Hazardous Materials Division. Sharps Collection Programs for Michigan Residents. Accessed June 15, 2009. http://www.michigan.gov/documents/deq/whm -stsw-sharps-collection-list_196524_7.pdf.
17. Wisconsin Department of Natural Resources. Sharps Disposal. Accessed June 15, 2009. http://dnr.wi.gov/org/aw/wm/medinf/sharps.htm .
18. SF Recycling & Disposal Inc. San Francisco Needle/Syringe Disposal Program. Accessed January 20, 2010. [Available online at: http://www.sfrecycling.com/needles/index.php?t=d]
19. Center for Disease Control and Prevention. Prevention !mong Injection Drug Users. “!ppe ndix A: Key Strategies for Preventing Blood -Borne Pathogen Infection Among Injection Drug Users. Accessed January 20, 2010. [Available online at: http://www.cdc.gov/idu/pubs/ca/appendixA.htm .]
20. Woolfrey, Paul and Kirby, R. Lee. “Hypodermic needles in t he neuropathic foot of patient with diabetes”. Canadian Medical !ssociation Journal. 1998, Edition 158, vol 6.
21. Solid Waste Disposal & Transfer Station. Salem, Virginia. http://www.salemva.gov/depts/swd/sharppup.html. Accessed June 10, 2009.
22. United States Environmental Protection Agency (EPA). Protect Yourself, Protect Others. Safe Options for Home Needle Disposal. [Available online at: http://www.epa.gov/osw/nonhaz/industrial/medical/med -home.pdf] Accessed June 10, 2009.
23. Regulation 16VAC25-90-1910.1030(d)(4)(iii)(A) & 9VAC20-120-220. Practice GreenHealth. Virginia Regulations. Accessed June 10, 2009. http://cms.h2e-online.org/ee/rmw/rmw-regulations/state-rmw-regulations/virginia/
FDA launches website on safe disposal of used needles and other “sharps”
Improperly disposed sharps pose public health risks
The U.S. Food and Drug Administration launched a new website (http://www.fda.gov/MedicalDevices/ProductsandMedicalProcedures/HomeHealthandConsumer/ConsumerProducts/Sharps/ucm20025647.htm) for patients and caregivers on the safe disposal of needles and other so -called “sharps” that are used at home, at work and while traveling.
The website will help people understand the public health risks created by improperly disposing of used sharps and how users should safely dispose of them. “Safe disposal of used needles and other sharps is a public health priority,” said Jeffrey Shuren, M.D., director of the FD!’s Center for Devices and Radiological Health. “This website provides information about how to keep used sharps from ending up in places where they could harm people.”
Where does the needle go?

THE
KENTUCKY PHARMACIST24
November 2011
December 2011 — Where does this used needle go?
1.) Approximately how many injections are administered each year by users of self-injectable medications?
A. 9 million B. 900 million C. 1 billion D. 3 billion
2. ) Which of the following is a concern when needles are not disposed of properly?
A. Needlestick injuries B. Transmission of bloodborne pathogens C. Potential physical and emotionial pain associated with a needlestick D. All of the above
3.) Which of the following statements regarding needlestick injuries (NSIs) is true?
A. NSIs are only a concern for individuals working in health care facilities B. The EP! has produced recommendations for used sharps disposal C. Appropriate disposal of used sharps eliminates the risk of NSIs D. All of the above
4.) Which of these groups may have the greatest risk of exposure afer used needles that were inappropriately disposed enter the public solid waste management system?
A. Recycling facility workers B. Health care workers C. Law enforcement personnel D. None of the above
5.) Which of the following disposal options would be the most expensive for the patent but better -suited for patents who live in rural areas?
A. Mail-back programs B. Syringe/needle exchange programs (SEPs) C. Special waste pick-up D. All of the above
6.) Which of the following waste disposal options may not prevent introduction of contaminated sharps into the solid waste system?
A. Drop boxes/supervised collection sites B. Needle clipping devices C. Mail-back programs D. Syringe/needle exchange programs (SEPs)
7.) Which of the following options is the most widely available for consumers across the country?
A. Drop boxes/supervised collection sites B. Mail-back programs C. Syringe/needle exchange programs (SEPs) D. Special waste pick-up
8.) Which of the following disposal option descriptions or examples are correct?
A. The NeedleZap® is a syringe mail-back program B. The BD Safe- TMClip device is a needle destruc-ton device C. The special waste pick-up service in Salem, Vir-ginia is a type of syringe exchange program D. None of the above are correct.
9.) Where can you find information regarding sharps disposal?
A. Center for Disease Control and Prevention Website B. Safe Needle Coalition Website C. Environmental Protection Agency Website D. All of the above
10.) What are important factors when recommending a disposal option to a patent?
A. Availability in your locality B. Convenience for the patent C. Cost to the patent D. All of the above
Where Does The Needle Go?
THE
KENTUCKY PHARMACIST25
November 2011
December 2011– Where Does This Used Needle Go?
Universal Activity # 0143-9999-11-060-H05-P PHARMACISTS ANSWER SHEET
Name ________________________________________________ KY Lic. # __________________________________
Address ________________________________________________________________________________________
PLEASE CIRCLE THE APPROPRIATE ANSWERS:
1.
A B C D
3. A B C D
5. A B C D
7. A B C D
9. A B C D
2.
A B C D
4. A B C D
6. A B C D
8. A B C D
10.A B C D
Information presented in the activity:
Met my educational needs ___Yes ___No Figures and tables were useful ___Yes ___No
Achieve the stated objectives ___Yes ___No Posttest was appropriate ___Yes __ _No
Was well written ___Yes ___No Commercial bias was present ___Yes
___No
Is relevant to my practice ___Yes ___No
Unmet Objectives:______________________________________________________________________________
I hereby certify that I completed this self-study program independently and without assistance from any other party.
Signature _________________________________________________ Date _________________________________
This activity is a FREE service to members of the Kentucky Pharmacists Association. The fee for non-members is $30. The fee for duplicate certificates is $5. Please send a self addressed, stamped envelope to KPERF, 1228 US 127 South, Frankfort, KY 40601.
The Kentucky Pharmacy Education & Research Foundation is accredited by The Accreditation Council for
Pharmacy Education as a provider of continuing Pharmacy education.
Expiration Date: December 1, 2014 Successful Completion: Score of 80% will result in 1.0 contact hour or 0.10 CEUs.
Participants who score less than 80% will be notified and permitted one re-examination.
December 2011– Where Does This Used Needle Go? TECHNICIANS ANSWER SHEET. Not ACPE approved for Technicians. Name _______________________________________________KY Cert. # __________________________________ Address ________________________________________________________________________________________
PLEASE CIRCLE THE APPROPRIATE ANSWERS:
1.
A B C D
3. A B C D
5. A B C D
7. A B C D
9. A B C D
2.
A B C D
4. A B
C D
6. A B C D
8. A B C D
10.A B C D
Met my educational needs ___Yes ___No Figures and tables were useful ___Yes ___No
Achieve the stated objectives ___Yes ___No Posttest was appropriate ___Yes __ _No Was well written ___Yes ___No Commercial bias was present ___Yes
___No
Is relevant to my practice ___Yes ___No I hereby certify that I completed this self-study program independently and without assistance from any other party.
Signature _________________________________________________ Date _________________________________
December Tech/Pharmacists Quiz

THE
KENTUCKY PHARMACIST26
Pharmacy Law Brief November 2011
Pharmacy Law Brief: Activities and Supervision of Pharmacist Interns
Author: Joseph L. Fink III, B.S.Pharm., J.D., Professor of Pharmacy Law and
Policy, Department of Pharmacy Practice and Science, UK College of Pharmacy
Question: At various times of the year we have a great array of individuals in the prescription department serving our patients – pharmacists, student pharmacists who are on an academic rotation or employed to accumulate internship hours, and registered technicians, some of whom are certified and others who are in the process of becoming certified. Would you please review the contemporary expectations regarding supervision of pharmacist interns? It’s been awhile since I was an intern myself and I suspect things may have changed some. Response: The clearest way to approach this question is to begin with you, the pharmacist. Pharmacists have what could be viewed as plenary authority – all encompassing, full and absolute authority over what occurs in the pharmacy. With this comes ultimate responsibility for tasks assigned to or performed by others under the supervision of the professional on duty. For this reason the pharmacist should select well and supervise appropriately the activities of others assisting with the prescription prepa ration and information dissemination process known as the practice of pharmacy. Student pharmacists who are registered with the Board of Pharmacy as pharmacist interns are for purposes of this discussion considered the same as student pharmacists on an academic rotation. The overarching rule is that the pharmacist intern is limited to doing things that the supervising pharmacist authorizes. By law the pharmacist intern may perform technical tasks under supervision of a pharmacist starting with the first day on the job. The phrase, “technical tasks” includes things such as retrieving the medication stock container from the shelf, counting the tablets or capsules and measuring liquids, pouring medications into the prescription bottle and affixing the label to the container. If authorized by the supervising pharmacist the pharmacist intern may also take part in
professional tasks. This wording, “professional tasks”, is more broad and includes anything a pharmacist can do except [1] the final check of a pr escription before it leaves the pharmacy, and [2] assisting with the transfer of a controlled substance prescription from your pharmacy to another. The pharmacist who oversees the pharmacist intern is expected under the law to provide “supervision” of the acts and activities of the aspiring pharmacist. The rules in this area are as

THE
KENTUCKY PHARMACIST27
November 2011Pharmacy Law Brief
follows, keyed to the level of progression of the pharmacist -intern through the professional curriculum:
During the student’s first year of pharmacy school professional tasks may be performed under “immediate supervision” by a pharmacist whereas after the first year of pharmacy school (as a PY2, PY3 or PY4 student) the pharmacist intern may perform professional tasks under “general supervision” by a pharmacist.
The phrase immediate supervision requires that the pharmacists directly oversee and hear what the intern is doing. Alternatively, general supervision means that a pharmacist must be present and available to answer questions as needed by the intern.
To review, the pharmacist preceptor needs to keep two dimensions of the preceptor -intern relationship in mind – what types of tasks or duties may be assigned to the student as well as what level or intensity of supervision is required. The bottom line is that the supervising pharmacist has ultimate authority and responsibility for professional activities performed in the service of patients Please note that additional information on the issues discussed here is available in a publication prepared by Casey Combs, a PY3 student at the UKCoP to provide pre-pharmacy students with information and guidance. This document is available for viewing on the College website at http://pharmacy.mc.uky.edu/programs/prepharm/files/Positioning_Yourself_to_Succeed_in_Pharmacy.pdf
Disclaimer: The information in this column is intended for educational use and to stimulate professional discussion among colleagues. It should not be construed as legal advice. There is no way such a brief discussion of an issue or topic for educational or discussion purposes can adequately and fully address the multifaceted and often complex issues that arise in the course of professional practice. It is always the best advice for a pharmacist to seek counsel from an attorney who can become thoroughly familiar with the intricacies of a specific situation, and render advice in accordance with the full information.
Submit Questions: [email protected]
Questions about the Medicaid MCOs? Check out the KPhA website (www.kphanet.org) and click on
KY Medicaid Updates.
Still have a question or concern? Send it to Executive Director Robert McFalls at [email protected]
or call 502-227-2303.
THE
KENTUCKY PHARMACIST28
Pain Relief Act November 2011

THE
KENTUCKY PHARMACIST29
Education Beyond The Classroom November 2011
An Education Beyond the Classroom
By Molly Trent, PharmD Candidate 2014
Taking on a new position is always exciting although it does not come without a degree of uncertainty and fear. These were my initial feelings as President-elect of the APhA-ASP Chapter at the University of Kentucky College of Pharmacy. In preparation for the upcoming year, UK sends the APhA-ASP President-elect to the Summer Leadership Institute (SLI). SLI is a three day conference in Washington D.C that is designed to alleviate concerns and prepare student pharmacist leaders within APhA-ASP for the challenges and excitement ahead.
The weekend began with visits to Capital Hill to meet with Kentucky legislators to discuss the Loan Repayment Eligibility Act and Medication Therapy Management Empowerment Act, which are currently being considered in Congress. As a student pharmacist, it is never too early begin advocating for the profession. This reality was made clearer to me after seeing the impact that students had on getting these two bills to Congress. The aforementioned were a result of proposals passed at the previous years APhA Annual Meeting.
The following day was devoted to a leadership-training workshop. This was designed to help participants determine leadership styles as well as personal strengths and weaknesses. From this activity, I learned the importance of modifying my leadership style to match the situation and people I am working to motivate.
The workshop also taught student leaders how to run meaningful meetings and how to best make professional contacts. The remainder of the weekend was spent networking with the more than 170 fellow student pharmacist leaders. We shared chapter achievements from prior years and discussed new events planned for the upcoming year. This networking opportunity allowed me to share the accomplishments of our chapter and bring back new ideas. Throughout the weekend, I also collected multiple business cards from other student leaders and APhA staff that I could contact for help and support throughout my year as APhA-ASP Chapter President.
Aldous Huxley once said, “Experience is not what happens to a man. It is what a man does with what happens to him.” SLI was a wonderful experience because it pushed me outside my comfort zone and taught me to think more like a leader. However, these three days will just remain an experience if I do not continue to apply the knowledge and skills I gained from SLI throughout my term as APhA-ASP Chapter President. It is my hope that over the next two years my leadership abilities will continue to grow and that I will allow my experiences to constantly mold me into a better and more effective leader. Thank you to the Kentucky Pharmacists Association for this opportunity!
THE
KENTUCKY PHARMACIST30
Pharmacists Mutual November 2011

THE
KENTUCKY PHARMACIST31
Effective Communications November 2011
Effective Communication Strategies for Sharing Key Pharmacy Messages
By Leah Godzina, MPA Director of Communications Universal Activity # 0143-9999-11-062-H04-P 1.0 Credit Hours (0.1 CEUs)
Learning Objectives At the conclusion of this session, successful participants will be able to:
1. Develop talking points on concepts important to the profession and utilize resources available through MPA .
2. Identify ways to reach out to the community and share significant pharmacy messages.
3. Identify ways to effectively communicate with the media on key pharmacy issues. 4. Define strategies for different types of media interviews, including in -person, over
the phone and on-camera. 5. Establish and maintain effective media relationships.
Reprinted with permission of the authors and Michigan Pharmacists Association where this article originally appeared.
The media and the public are important audiences that require consistent and valuable communication/ Whether it’s through a newspaper, on the radio or on television, news media in your community can be a highly effective strategy to convey important pharmacy messages. Pharmacists must make their priorities connect with the general public, legislators and the media.
With the profession constantly changing, it’s important for pharmacists to educate key individuals on the value they provide. The question is sometimes asked, “How
do
we make these priority messages resonate with the public, legislators and media?” Pharmacists can’t always be on the defense, or they will never score enough points to be recognized on the board.
Reporters, columnists, editorial writers and other media professionals are gatekeepers of information with the means to share that information on a state, national and even international level. They are important people
to have on your side, or at least to
educate so they can fairly and accurately
convey pharmacy’s message and provide fair coverage.
Defining Your Pharmacy Priorities
The profession of pharmacy covers a wide range of health care issues. Because pharmacists’ interests are wide and can span multiple areas, it’s important for you to define your priorities before you shape your message(s).
In September 2010, Michigan Pharmacists Association (MPA) sent out a survey to all pharmacists in Michigan asking what pharmacy practice issue was most important to them. The top three were outsourcing of prescriptions (mail-order pharmacy), medication errors (nonpunitive reporting environment) and pharmacy benefit manager (PBM) transparency, with 33 percent, 12.5 percent and 10.7 percent of the votes respectively.
In addition to these important issues, it’s vital
to look at the big picture and answer
the question, “What do you wish people knew and believed about pharmacists?”

THE
KENTUCKY PHARMACIST32
November 2011Effective Communications
Many pharmacists want the public to be aware that they do more than just count pills and dispense medications, so an important message to convey may be “pharmacists are uniquely qualified to understand the function of medications and ensure safe and effective patient therapy.” Your priorities may focu s on a number of other things, such as a specific piece of legislation that would affect the profession. Advocating on behalf of pharmacy and educating legislators on important health care issues also is an important aspect of communicating effectively. Audience
Knowing who your audience is and understanding how to best communicate with them is also important in sharing your message(s). To be sure we communicate clearly, we need to adjust how we say something and what information we include, and recognize
that each audience
understands messages differently. In general, most pharmacists want to
communicate their pharmacy priorities to three key audiences: patients/general public, legislators and the media.
Patients/General Public
Most patients and the general public are not skilled in health care terminology, and different generations like to communicate in different ways. Also, when patients come to a pharmacy, they usually have a need, so it’s important to put yourself in their shoes when you’re trying to explain pharmacy issues. Be sincere; no one likes to be judged or talked down to.
Legislators
Legislators have full schedules. They’re looking to do the most good
and want the outcome to help the most people, not just pharmacy. The information they’d be most interested in is the impact of
legislation or concepts in numbers or dollar amounts. Communicating information to them should be done in a professional and respective way. The Media Lastly, the media traditionally have a set timetable. When it comes to pharmacy issues, in addition to hearing from a pharmacist, they often want a local or patient perspective. Backing up what you say with statistics or examples also makes you a credible source.
A pharmacy message or priority has to be a reality, or
something you’re able to prove.
Those things you deemed as what you wish people would know or believe about pharmacists have to be evident in pharmacy practice.
No matter who you want to reach, be sure you also review the 10 Cs of Communication (Table 2)
before you start
your strategy. Crafting Messages and Talking Points
After you’ve determined your priorities and defined your audience, the most critical element of success is your main message. First, define what’s important , or your key statement. In other words, what’s the single most important statement that you’d like people to remember?
Now that you’ve determined what’s important, outline why it’s important. Reinforce and clarify your key statement by providing background information
and
a call to action. In addition, collect evidence to back it up, such as anecdotes, research and statistics.
MPA developed many talking points on key pharmacy issues that members also have the opportunity to utilize. Pharmacy priority talking points are available at MichiganPharmacists.org/advocacy/priorities, and other materials also are
available in the Patient Education Library at MichiganPharmacists.org/resources/education.
THE
KENTUCKY PHARMACIST33
November 2011Effective Communications
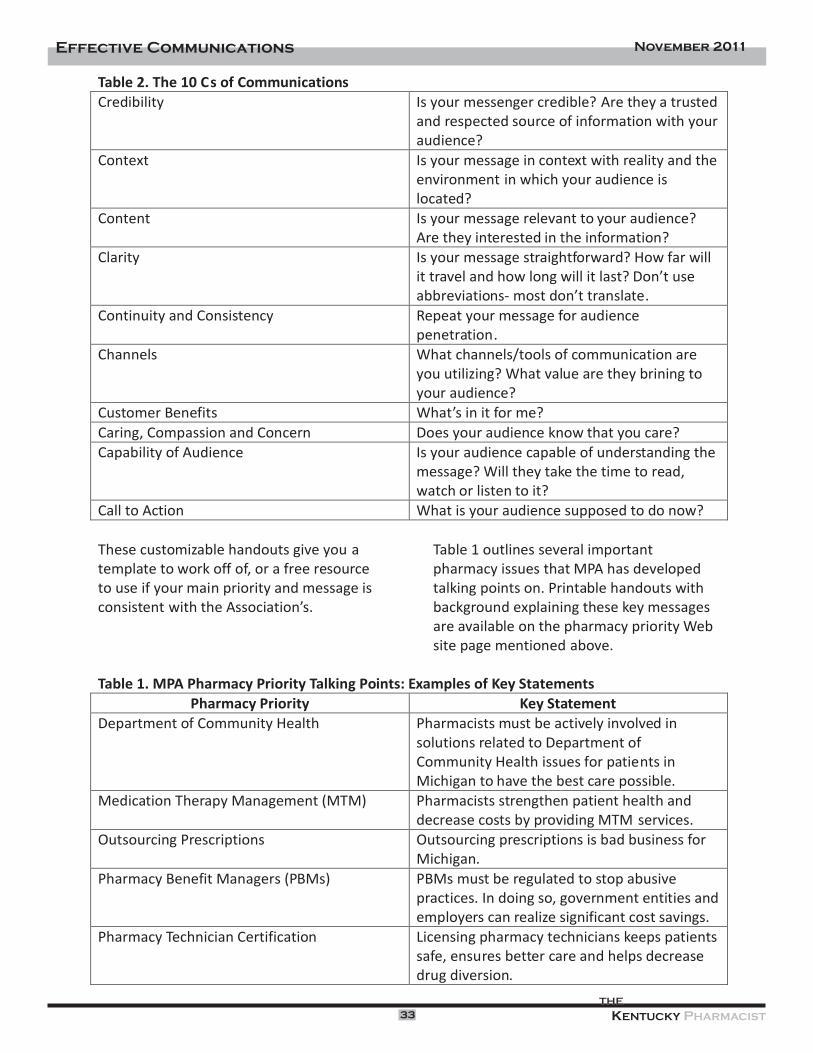
Table 2. The 10 Cs of Communications Credibility Is your messenger credible? Are they a trusted
and respected source of information with your audience?
Context Is your message in context with reality and the environment in which your audience is located?
Content Is your message relevant to your audience? Are they interested in the information?
Clarity Is your message straightforward? How far will it travel and how long will it last? Don’t use abbreviations- most don’t translate.
Continuity and Consistency Repeat your message for audience penetration.
Channels What channels/tools of communication are you utilizing? What value are they brining to your audience?
Customer Benefits What’s in it for me? Caring, Compassion and Concern Does your audience know that you care? Capability of Audience Is your audience capable of understanding the
message? Will they take the time to read, watch or listen to it?
Call to Action What is your audience supposed to do now?
These customizable handouts give you a template to work off of, or a free resource to use if your main priority and message is consistent
with the Association’s.
Table 1 outlines several important pharmacy issues that MPA has developed talking points on. Printable handouts with background explaining these key messages
are available on the pharmacy priority Web site page mentioned above.
Table 1. MPA Pharmacy Priority Talking Points: Examples of Key Statements
Pharmacy Priority
Key Statement
Department of Community Health
Pharmacists must be actively involved in solutions related to Department of Community Health issues for patients in Michigan to have the best care possible.
Medication Therapy Management (MTM)
Pharmacists strengthen patient health and
decrease costs by providing MTM services.
Outsourcing Prescriptions
Outsourcing prescriptions is bad business for Michigan.
Pharmacy Benefit Managers (PBMs)
PBMs must be regulated to stop abusive practices. In doing so, government entities and employers can realize significant cost savings.
Pharmacy Technician Certification
Licensing pharmacy technicians keeps patients safe, ensures better care and helps decrease drug diversion.

THE
KENTUCKY PHARMACIST34
November 2011
Effective Communications
Sharing Your Message So, your message has been developed; now what do you do? There are severa l ways that you can share your priorities with the community.
Write a Letter to the Editor or Opinion Editorial Writing a letter to the editor is one route you could go. Letters to the editor reach a very large audience and almost every newspaper or magazine publishes them. They also give you a chance to rebut information that was not accurately conveyed in a
news article. These
letters also are frequently used by community leaders or legislators to gauge public sentiment about current issues in the news.
In addition to letters to the editor, people often submit opinion editorials for publication. These types of pieces often
are
clipped out
of newspapers or bookmarked on the newspaper’s Web site for individuals to share with colleagues, legislators, friends, etc. These types of submissions can be sent to a newspaper’s opinion editor, but be aware that constrained word counts often exist, so you may want to check the publication guidelines in advance to be sure your message can be conveyed within their limits.
Become a Trusted Resource
Another option for sharing your message is to become a resource for a reporter. Identify reporters who cover health care in your local newspaper or television station and establish yourself as a reliable source of information. Reaching out and inviting them to your practice site could help educate them on what pharmacists do and why it’s important, and then remain in regular contact. Reporters who find
an expert who’s easy to understand and work with tend to go back to that source frequently. You also can sign up for Help a Reporter Out (HARO) at www.helpareporterout.com , and when you have a story to share on a topic, offer the information to a reporter. HARO is one good way to spread information and get high-quality, free publicity for your business. Host a Legislator Pharmacy Visit
Becoming a trusted source for legislators can be useful as well. Inviting them to your pharmacy for a visit will help educate them on important pharmacy services and give them a chance to interact with patients and ask questions about your practice. Feedback from your visits also allows MPA to plan future advocacy efforts and identify potential allies in promoting a pharmacy-friendly legislative agenda. A legislative visit report is available at MichiganPharmacists.org/advocacy/grassroots.
MPA is also willing to
send out a media advisory, or provide you with a template to create your own, to get the word out about a legislative pharmacy visit.
Talk Back
Talk radio and other talk -back opportunities also provide
a good means
for you to share your message. You can get involved in talk radio by being interviewed as a guest
or calling into talk radio programs. The opportunity exists for you to create your own Internet radio talk show, such as through www.blogtalkradio.com, and share topics that concern you or

THE
KENTUCKY PHARMACIST35
November 2011
Effective Communications
information about your priorities to the public. Utilize Social Media Social media has become a powerful tool for getting the word out. Web sites like Facebook, LinkedIn and Twitter provide so many new web-based and mobile technologies to communicate through/ It’s important to understand that you cannot completely control your message through social media, but rather, you can begin participating
in
the conversation and significantly influence it.
A simple social media post often is not enough to convey the full importance of a topic, but including links to expand on key ideas and utilizing multimedia, such as videos, photos and blog posts, can create value for your followers and showcase your knowledge.
Many people are using social media
for successful public relations efforts, and social media resources offer unique features that may be used to advance the role of pharmacy in health care initiatives. Because social media is so far-reaching, you also can
be connected to or network with those you wouldn’t otherwise. Use the messages you craft to speak to these people.
Sharing content with your audience or potential customers also is
a great way to generate more interest in your field, a particular service, your professional priorities and more.
Perfect Your Media Skills
When sharing your message, it’s also important for you to acquire media skills. In many ways, the media acts as a gatekeeper to the community and is a powerful force in shaping opinions and creating perceptions.
Because of this, it’s important for you to learn how to establish and maintain good media skills and develop long-lasting relationships with your local media. Organization is key to speaking powerfully on behalf of the profession. Many organizations have internal public relations staff to gather certain information when a media representative calls. Whether someone else does it, or you do it yourself, it is essential that you know who called, what they called about, when they called, where they called from, their deadline and any other facts your company deems important.
It’s okay to take the request and call back within their deadline with organized answers. Developing guidelines for
media
calls is critical to getting and staying organized in
your public relations efforts.
Once you’ve planned and organized, there are many things to keep in mind when implementing media communication, including what to do after you’ve agreed to talk with a reporter, how to handle bad questions, positive and negative
words to
use, on/off the record, body language and tips for looking good on television.
After agreeing to speak with a reporter, you’ll need to do the following.
?
Be a source before you are a subject
?
Respond quickly; reporters are almost always working under a strict deadline
?
Anticipate any and all questions
?
Prepare your responses
?
Know your key messages; go over your talking points in advance, or have them in front of you during phone conversations.
?
Know your facts and stick to them
?
Do not speculate or editorialize- if you don’t know, then don’t pretend

THE
KENTUCKY PHARMACIST36
November 2011Effective Communications
you do. If you need to look into a question, let them know and get back to them within their deadline.
? Avoid sarcasm ? Be brief; get your key
messages out early in the conversation
? Know when to stop talking ? Tell the truth ? Don’t take anything
personally ? Keep your cool- act, don’t
react ? Be human
? Think and talk visually ? Speak simply; avoid technical
jargon ? Repeat your key messages
before you conclude; a reporter will almost always ask “Is there anything else?”
To go along with anticipating any and all questions, reporters sometimes may ask you what are considered “bad” questions. Table 3 lists different types of bad questions and how to handle them appropriately.
Table 3. Handling “Bad” Questions from Repor ters
Type of Question
How to Handle It
Loaded question:
Begins with false or
misleading statements and asks for a response
Restate the question correcting any inaccuracies, and then answer it
Unacceptable alternatives:
Offers choice
between two extremes of false situations
Don’t repeat the question, restate the reality- explain the real situation
Hypothetical question: Requests comment on a “what if” situation- reporter is usually fishing for information
Respond to a real situation only- don’t guess, speculate or offer opinions, and don’t answer questions that are beyond your area of expertise
Commentary: Requests comment on a
statement made by someone else
Don’t comment on hearsay or a study you haven’t reviewed- unless you’ve personally heard the statement and are qualified to respond, don’t. Instead, suggest the reporter contact the source directly
Rapid-fire questions: One question fired after
another, without an opportunity to respond
First, only answer the questions you want to. Stop if you are continually interrupted and don’t go on until the reporter stops, then respond to each individual question
In addition to bad questions, there also are bad or negative words that should be avoided. When it comes to the profession of pharmacy, positive
words are those such as patient, pharmacy, pharmacists, medication, therapy and education, whereas words to avoid, or negative
words, would include those like druggist, drugs, pills and abuse.
When speaking to a reporter, it’s never recommended to go “off the
record,” meaning the material you provide them
may not be published or broadcasted. There are certain phrases, listed below, that reporters may use to make it sound like you’re speaking off the record.
?
Not for attribution:
Information may be published, but the source of the information may not be identified. If you ever agree to this, make sure you know whether or not this applies to your name only, your

THE
KENTUCKY PHARMACIST37
November 2011Effective Communications
organization or anything else about you.
? Background: This typically means the reporter is simply doing some research on a subject before doing a story and will not use your name for publication, but make sure you clear this with the reporter.
? Just between us: Never use this phrase or agree to it with a reporter
? Check it with me before you use it: This allows the reporter to go over information or quotes with you before publication
?
Read it to me before you use it:
Never use this with a reporter; they will rarely read the story to you before it’s published. All you can do is make sure your facts and quotes are accurate.
!s a general rule, if you’re not prepared to be quoted, don’t say something. Reporters aren’t obligated to check with you before they use a quote, or read or provide a story to you for review before it’s published.
When doing on-camera interviews, or in-person reporter interviews, body language and fashion come into play as well. Body language can often answer a reporter’s question faster than you can. Watch for these revealing signs:
Signs of Confidence
?
Uncross your legs ?
Move toward the edge of your chair
?
Lean toward the reporter
?
Loosen your tie or unbutton your coat (print or radio only)
?
Nod your head
?
Gesture (moderately)
?
Initiate and maintain eye contact
?
Use a loud, clear voice
?
Vary your vocal tones
?
Vary your positions
Signs of Nervousness
? Cover your mouth ? Scratch your nose, ears or head ? Tug at your clothes, play with
your jewelry, pen, paper, etc. – if you’re a hand fidgeter, fold your hands
? Slump ? Look down and avoid eye
contact ? Make unpleasant or
inappropriate facial expressions ? Look away ? Keep your body rigid ? Hunch your shoulders ?
Verbal pauses (um, ah, uh, etc.)
If you are nervous, it’s okay to bring notes and refer to them. Even during on-camera interviews, there’s often a break between spots and questions.
There are other good tips to utilize for on-camera interviews. Fashion is important to ensure that you look your best on television and represent yourself and your organization in a professional manner. It is suggested that men wear medium and dark toned sport coats (not black), such as
charcoal, with an off-white, gray or pastel colored shirt. For ties, stick with medium and dark colors with plain and moderate (unbusy)
patterns. In addition, it’s
recommended that men shave stubble prior to an on-camera interview.
For women, suits and dresses should be simple and tailored in wool, cotton or linen,
avoiding reflective and shiny fabrics . Blouses can be off-white, gray or pastel and jewelry should be minimal.
In addition, some general on-camera interview tips include:
?
Remove nametags, hats, pens, wallets and notepads, and other nonessential things that could distract viewers.

? Silk ties and blouses could cause static interference with microphones clipped to clothing.
? Avoid comb-overs, “big hair” or anything that draws attention away from the Important matter you’ll be discussing.
? Red, black and white are okay to wear, but black and white will create a monochromatic picture instead of taking advantage of television’s living color. Wearing these colors if you have very light or very dark skin also could
compromise the picture’s overall exposure.
?
Wear tailored, form-fitting clothing. Television tends to “add weight” to the on-camera person.
Put Your Media Skills Into Practice
A good way to develop media and interview skills is to learn from others. Media
communication takes practice, and the only way to learn is to watch other pharmacy professionals in action and to evaluate your own practice. Determine what worked and what didn’t and decide what you learned that could help the next time around. If you’re asked the same questions in a future interview or want to reiterate different points the next time around, make note of it, and if you’re ever called again to speak on the same or similar subject you’ll be better prepared.
Table 4 provides several tips for establishing and sustaining good media relationships. Once you’ve served as a reliable source and expert on pharmacy topics, these are important things to keep in mind to maintain that relationship.
Even when there
isn’t breaking news or something crucial to
pharmacy in the news, it’s important to stay in contact with key members of the media.
Table 4. Tips for Establishing and Maintaining Media Relationships
Tips
Additional Information
Find out who key health care reporters in your state are
Develop an accurate contact list and keep it up-to-date
Hold one-on-one meetings with key reporters
?
Go to their office
?
Get to know them
?
Present your key issues and leave behind materials
?
Offer your assistance as a resource
?
Discover what kind of stories peak
their interest and how to best correspond with them
Understand the reporter’s deadline
?
Follow guidelines of how they best like to be contacted
?
Meet their deadlines through this form of communication
Try not to sent out blanket press releases
?
Customize press releases to each reporter (particularly key health care reporters)
?
Send to them personally rather than through a distribution list
Avoid images and attachments
?
Don’t include attachments along with e-mail press releases

THE
KENTUCKY PHARMACIST39
November 2011Effective Communications
? E-mails could go to their spam folder or be deleted altogether
Follow up with reporters ? Show your appreciation for attention to an issue
? Take that opportunity to educate them further
Follow key reporters ? Send them an e-mail if you thought a story they wrote was good/informative/insightful
?
Reporters like genuine praise
Use e-mail correspondence
?
Reporters prefer e-mail correspondence
?
Never fax, unless they specifically say to
?
No time to retype a statement, especially under deadline
Record your interactions with reporters
?
Keep track of each time you interact with a reporter or the media
?
Follow up and be familiar with how they like to be contacted or what issues they’ve already been educated on
Find local connections
?
Establish local connections for state and national stories
?
Reporters often want a local perspective on national issues
?
Supply them with the names of media-trained members who are familiar with your organization’s positions and talking points
Create a triage system in your organization
?
Reporter calls should never go to voicemail
?
They are on deadline and often need to speak with someone right away
?
Develop a system that addresses the reporter’s request, even if you need to take a message and return the call after preparing information
Pharmacists are the medication experts on the health care team. As a pharmacist, you are uniquely qualified to help consumers take charge of their health care by making wise choices regarding medications. As a resource, pharmacists can be powerful tools, educating the media, legislators and the public on important priorities.
When communicating your key pharmacy messages to the community, it’s important to
stay organized by establishing a strategy, developing talking points and keeping your media skills in check. Effectively sharing your priorities could take pharmacy to a new level, by educating the public, legislators and media, and getting the word

THE
KENTUCKY PHARMACIST40
November 2011Effective Communications
out there about key initiatives that impact the profession. Several concepts in this article were shared from a public relations campaign developed
in collaboration with The Rossman Group in Lansing. MPA would like to thank Rossman, as well as Jill Cobb, B.A., for their contributions to the development of this continuing education home study.
KPhA hires new director of communications and continuing education
The Kentucky Pharmacists Association named Scott Sisco as its new director for communications and continuing education. “This position plays a pivotal role in providing the highest level of service to our members,” said Robert McFalls, Executive Director. “We are thrilled to have someone of Mr. Sisco’s talent to join our team.” Sisco’s background includes several newsroom positions at daily newspapers around Kentucky and alumni relations support positions at Western Kentucky Universi ty and Kentucky State University. He holds two degrees from WKU: a Bachelor’s degree in Print Journalism and a Master’s in Communication. “I look forward to informing the pharmacists of Kentucky about issues relating directly to them, and managing the continuing education process efficiently,” Sisco said. “One of my goals is to connect with the younger pharmacists, and engage them in the activities of the Association. I also want to continue to provide excellent service to all Kentucky pharmacists.” The mission of the Kentucky Pharmacists Association is to promote the profession of pharmacy, enhance the practice standards of the profession, and demonstrate the value of pharmacist services within the health care system. For more information, contact Scott Sisco at 502-227-2303 or [email protected].

THE
KENTUCKY PHARMACIST41
November 2011Effective Communications
December 2011-2 — Effective Communication Strategies for Sharing Key Pharmacy Messages
1) In a recent survey published in the September 2010 issue of Michigan Pharmacist, what was the top pharmacy practice issue?
A. E-prescribing B. Mail order C. PBM transparency D. Audits
2) What is the preferred method of communication for most reporters?
A. E-mail B. Fax C. Leter D. Phone
3) What is the most critical element of success in efectvely communicatng key pharmacy messages? A. Crafing your main message B. Determining your audience C. Handling “bad” questons appropriately D. Dressing properly 4) True or False: It is never recommended to go off the record with a reporter.
A. True B. False
5) What is one of the 10 Cs of Communication? A. Comprehensiveness B. Challenge C. Contract D. Channels
6) What is one of the pharmacy priorities MP! has developed talking points on?
A. Health care reform B. Medication therapy management (MTM) C. Electronic health records (EHRs) D. Patent -centered medical home (PCMH)
7) True or False: It is okay to take down a message from a reporter and call back within their deadline with organized answers.
A. True B. False
8) One way for a pharmacy professional to share their key message with a legislator is to:
A. Storm into their office B. Start a protest at the Capitol C. Schedule a legislator pharmacy visit D. Send them a letter E. Both c and d
9) During an on-camera interview, a common sign of nervousness mentoned is:
A. Avoiding eye contact B. Smiling excessively C. Biting your lip D. Leaning toward the reporter
10) How is it recommended that you handle a hypothetcial question?
A. Restate the queston, correctng any inaccuracies, and then answer it B. Respond to a real situaton only C. Answer only questions that you want to D. Don’t repeat the question, restate the reality

THE
KENTUCKY PHARMACIST42
November 2011
December 2011-2–
Effective Communication Strategies for Sharing Key Pharmacy Messages
Universal Activity # 0143-9999-11-062-H04-P
PHARMACISTS ANSWER SHEET
Name ________________________________________________ KY Lic. # __________________________________
Address ________________________________________________________________________________________
PLEASE CIRCLE THE APPROPRIATE ANSWERS:
1.
A B C D
3. A B C D
5. A B C D
7. A B
9. A B C D
2.
A B C D
4. A B
6. A B C D
8. A B C D E
10.A B C D
Information presented in the activity:
Met my educational needs ___Yes ___No Figures and tables were useful ___Yes ___No
Achieve the stated objectives ___Yes ___No Posttest was appropriate ___Yes __ _No
Was well written ___Yes ___No Commercial bias was present ___Yes
___No
Is relevant to my practice ___Yes ___No
Unmet Objectives:______________________________________________________________________________
I hereby certify that I completed this self-study program independently and without assistance from any other party.
Signature _________________________________________________ Date _________________________________
This activity is a FREE service to members of the Kentucky Pharmacists Association. The fee for non-members is $30. The fee for duplicate certificates is $5. Please send a self addressed, stamped envelope to KPERF, 1228 US 127 South, Frankfort, KY 40601.
The Kentucky Pharmacy Education & Research Foundation is accredited by The Accreditation Council for
Pharmacy Education as a provider of continuing Pharmacy education.
Expiration Date: December 1, 2014 Successful Completion: Score of 80% will result in 1.0 contact hour or 0.10 CEUs.
Participants who score less than 80% will be notified and permitted one re-examination.
December 2011-2– Effective Communication Strategies for Sharing Key Pharmacy Messages
TECHNICIANS ANSWER SHEET. Not ACPE approved for Technicians.
Name _______________________________________________KY Cert. # __________________________________
Address ________________________________________________________________________________________
PLEASE CIRCLE THE APPROPRIATE ANSWERS:
1.
A B C D
3. A B C D
5. A B C D
7. A B
9. A B C D 2.
A B C D
4. A B
6. A B C D
8. A B C D E
10.A B C D
Met my educational needs ___Yes ___No Figures and tables were useful ___Yes ___No
Achieve the stated objectives ___Yes ___No Posttest was appropriate ___Yes __ _No Was well written ___Yes ___No Commercial bias was present ___Yes
___No
Is relevant to my practice ___Yes ___No
I hereby certify that I completed this self-study program independently and without assistance from any other party.
Signature _________________________________________________ Date _________________________________
December Tech/Pharmacists Quiz

THE
KENTUCKY PHARMACIST43
November 2011Pharmacy Policy Brief
Pharmacy Policy Brief: What Is Policy? Robert Zachary Thompson, Pharm.D. Candidate 2014
An Introductory Note: This is the first installment in a new series, Pharmacy Policy Brief, to appear in The Kentucky Pharmacist. The information in this column is intended to address timely and practical policy issues of interest to pharmacists, pharmacist interns and pharmacy technicians with the goal being to encourage thought, reflection and exchange among practitioners. It is not the goal of this series to fully a nd completely discuss the various facets of the policy issues presented; rather, it is to introduce the topics and issues to facilitate and encourage interchange and discourse. This first installment addresses some basic information about policy. Author: Robert Zachary Thompson is a second professional year Pharm.D. student
at the UK College of Pharmacy. Zach completed his pre-professional education at the University of Kentucky and is a native of Cadiz, Ky .
Issue: Pharmacists deal with a wide variety of policies in their professional and
personal lives. But what exactly is encompassed in the word “policy”? Discussion: Pharmacists, pharmacist interns, and pharmacy technicians are faced with policy everyday in their actions taken within the pharmacy . Policies are implemented by the state and federal government, by third -party entities, and multiple other entities dealing with procedures that are carried out within the pharmacy itself. Many pharmacists, pharmacist interns, and pharmacy employees do not understand the exact definition of policy and are confused about how it applies to them. Policy has many different definitions and applies to different aspects of everyday life. Policies are plans of action that guide decision-making and work to achieve favorable outcomes or aim to avoid negative ones. The word policy does not directly indicate what is done but instead states what should be done in certain situations. Policies can also be created by a particular organization to state their stance on a given issue dealing with their profession. Policies are often brought about by statutes and regulations created through governing bodies. The types of policy that relate to pharmacy include pharmaceutical policy, pharmacy policy, drug policy, and medi cation use policy[1]. Policies can apply in different geographical areas, and may be split up by the areas in which they are followed. Geographical aspects of policy can range from international to personal with many stops along the way as shown in Figure 1. Figure 1. Flow of Geographical Aspects of Policy

THE
KENTUCKY PHARMACIST44
November 2011Pharmacy Policy Brief
An example of policy implemented by a national governing body is the Omnibus Budget Reconciliation Act of 1990 (OBRA ‘90). This policy mandated that all pharmacists dispensing a prescription for a Medicaid beneficiary must offer counseling to the patients. This policy put the pharmacist directly in charge of proper medication use by patients and greatly transformed pharmacy practice when it was implemented. Examples of policy created outside the pprofession of pharmacy and outside of governing bodies are those made by corporate entities to dictate what is done concerning specific situations. These policies can be made to deal with situations concerning disciplinary actions that may need to be taken. They may state what the punishment for a given offense may be or the investigational processes that must be followed. A pharmacist may also have personal policies to dictate whether they dispense a medication. A current issue that deals with a pharmacist personal policy is the dispensing of medications used for lethal injections. A pharmacist may have personal or religious objections to dispensing these medications. They also may feel pressure from the individuals outside the profession to dispense and in turn may set up personal policies to deal with this pressure. Having a general knowledge of policy can help the profession of pharmacy grow exponentially in the future. As more policies are made each day being acclimated with the different types can help grow an individual. Applying this knowledge to situations can help expand patient care as well as prepare ones self to deal with unforeseen events.
1. Fink III JL, Talbert J, Blumenschein K. Policy-Related Degree Options for Pharmacists Interested In Careers in the Health Care Field. Hosp Pharm, 2010; 45(2):135-141.
Have an Idea?
Suggestions regarding topics for consideration are welcome. Please send them to [email protected].
www.twitter.com/KyPharmAssoc
www.facebook.com/KyPharmAssoc
Get updates as they happen. Connect with KPhA on Twitter and Facebook

Gov. Beshear proclaims October 2011 as Pharmacist Month
THE
KENTUCKY PHARMACIST45
Sullivan University College of Pharmacy
November 2011
Colmon Eldridge, III, executive assistant to Kentucky Gov. Steve Beshear, presents a proclamation to the KPhA Board of
celebrates accreditation
Sullivan University’s College of Pharmacy celebrated its accreditation with games,
addresses students, faculty
ice cream and fun. Right:
Pharmacy President and
Joey Matingly, Jefferson
County Academy of
Directors proclaiming October 2011 as Pharmacist Month in Kentucky.
KPhA Director,
and staff.
misinformation about the cost of prescription drugs. Dr. Jason Wallace, Grant County Drugs,
National Group formed to campaign against
In the summer of 2011, a group of pharmacy owners banded together to form a coalition designed to take on PBM abuse, mandatory mail order and other threats to pharmacists.
—
Transparency (PUTT); The organization now
earlier this year, including segments on CBS,
For more information on
Their efforts led to an incorporated entity
consists of 100 pharmacists and pharmacy
awareness, the group launched a national
significant media attention since its launch
Pharmacists United for Truth
campaign focused on PBM practices and
serves as Vice Chair; PUTT has generated
owners from 30 states and is growing. Through media outreach and public
and the
Pharmacists United for Truth and
PUTT, see http://www.truthrx.org
and Transparency
New York Times
Proclamation
Washington Post .
PBM abuse
CNBC, the

THE
KENTUCKY PHARMACIST46
November 2011Proclamation

THE
KENTUCKY PHARMACIST47
CAPP November 2011
CAPP Seeks Nominations for Advisory Board
The University of Kentucky College of Pharmacy's new Center for the Advancement of Pharmacy Practice (CAPP) is seeking nominations of its Advisory Board. CAPP was recently created by the College to engage pharmacists in advancing the practice of pharmacy across the state, the nation and the world.
"The Advisory Board will play a crucial role in helping to chart the course for CAPP," said Trish Freeman, Director of CAPP. "Our goal is to engage pharmacy practitioners and stakeholders to help lead the conversation about how to transform the practice of pharmacy."
Freeman said she hopes the CAPP Advisory Board will be inclusive and representative of the many aspects of the pharmacy practice. She said that CAPP's chief mission is to engage pharmacy stakeholders including both practitioners and pharmacy-related organizations to create, develop and implement novel care delivery models within pharmacy practice that improve medication use and health outcomes.
"Advancing the practice of pharmacy is something that is near and dear to all of us," Freeman said. "My hope is that CAPP and its Advisory Board will help us leverage the College's education, engagement, and research strengths to improve the practice of pharmacy across the state, the nation and the world."
For instance, CAPP is working to establish a practice-based research network, which will allow community-based practitioners to collaborate with their patients and academic researchers to improve delivery and outcomes of pharmacist-provided care.
"If we really care about assuring the future of pharmacy, we have to utilize our academic and research strengths to make real changes to the practice of pharmacy," said Tim Tracy. Dean of the UK College of Pharmacy. "We have to make our research real to the profession and practitioners and use our brightest minds to develop best practices in pharmacy."
Nomination forms, which can be found on the KPhA Website by clicking on the Communications Link, should be submitted to Dr. Trish Freeman at the UK College of Pharmacy. Please email submissions to . Self-nominations are welcome. [email protected]

48
THE
KENTUCKY PHARMACIST
November 2011
Kentucky Pharmacists Association 1228 US 127 South Frankfort, KY 40601 (502) 227-2303 www.kphanet.org Kentucky Board of Pharmacy State Office Building Annex, Ste. 300 125 Holmes Street Frankfort, KY 40601 (502) 564-7910 www.pharmacy.ky.gov Pharmacy Techn ician Certification Board 2215 Constitution Avenue Washington, DC 20037-2985 (800) 363-8012 www.ptcb.org Kentucky Society of Health Systems Pharmacists 1501 Twilight Trail Frankfort, KY 40601 (502) 223-5322 www.kshp.org Kentucky Regional Poison Center (800) 222-1222 American Pharmacists Association (APhA) 2215 Constitution Avenue NW Washington, DC 20037-2985 (800) 237-2742 www.aphanet.org National Community Pharmacists Association (NCPA) 100 Daingerfield Road Alexandria, VA 22314 (703) 683-8200 [email protected] Drug Information Center Sullivan University College of Pharmacy 2100 Gardiner Lane Louisville, KY 40205 (502) 413-8638 www.sullivan.edu
Frequently Called & Contacted

49
THE
KENTUCKY PHARMACIST
November 2011Board Of Directors
BOARD OF DIRECTORS
Clay Rhodes, Louisville Chairman
[email protected] 502.476.1796
Lewis Wilkerson, Frankfort President [email protected] 502.695.6920
Frankie Hammons, Barbourville Secretary [email protected] 606.627.7575
Duane Parson, Richmond Treasurer [email protected]
502.553.0312
Kimberly Croley, Corbin
President-Elect
606.304.1029
Leon Claywell
Past President
Kelley Ratermann
Student Representative
Amanda Jett
Student Representative [email protected]
Amanda Burton, Lexington
Trish Freeman, Lexington [email protected]
Joey Mattingly, Prospect
Matt Martin, Louisville
Jeff Mills, Louisville
Glenn Stark, Frankfort
Sam Willett, Mayfield
Leah Tolliver, Lexington
Richard Sloan, Hindman
HOUSE OF DELEGATES
Tyler Whisman, Florence Speaker of the House
Matt Martin, Louisville Vice Speaker of the House [email protected]
KPERF ADVISORY COUNCIL
Ann Amerson, Lexington [email protected]
Kim Croley, Corbin
KPhA/KPERF HEADQUARTERS
1228 US 127 South, Frankfort, KY 40601
502.227.2303 (Phone) 502.227.2258 (Fax)
www.kphanet.org
www.facebook.com/KyPharmAssoc www.twitter.com/KyPharmAssoc
Robert McFalls, Executive Director [email protected]
Matt Worthy, PharmD
Director of Professional & Clinical Services [email protected]
Scott Sisco
Director of Communications and Continuing Education
Kelli Sheets, Office Manager
Christine Richardson, Clinical Pharmacist
Darcie Nixon, Administrative Assistant
Save the Date for our 2012 Annual Meeting: June 13-16, 2012
The 134th Annual Meeting of the Kentucky Pharmacists Association has been set for June 13-16, 2012 at the Marriott Griffin Gate in Lexington. Save the date and check KPhA's web site for periodic updates
). See YOU at the 134th Annual Meeting !(www.kphanet.org
THE
KENTUCKY PHARMACIST50
November 2011Save The Date/APSC

TheKentucky1228 US 127 SouthFrankfort, KY 40601
PharmacistPRSRT STD
U.S. POSTAGEPAID
Lexington, KYPermit No. 1478