Embed Size (px)
DESCRIPTION
journal
Citation preview

Copyr
Eur J Anaesthesiol 2015; 32:666–671
ig
FroMe
CoE-
02
ORIGINAL ARTICLE
The kalaemic and neuromus
cular effects ofsuccinylcholine in centronuclear myopathyA pilot investigation in a canine model
Manuel Martin-Flores, Monique D. Pare, Luis Campoy, Marta Romano, Emily A. Tomak and
Robin D. Gleed
BACKGROUND Myopathies are generally considered toincrease the risk for succinylcholine-induced hyperkalaemiaand may affect the duration of action of neuromuscular block-ers. Centronuclear (myotubular) myopathy (CNM) is conge-nital and produces various degrees of muscular weakness andassociated complications such as respiratory failure. Theeffects of succinylcholine and the potentially lethal con-sequences of hyperkalaemia on patients with CNM areunknown due to its rarity. One source of information is thedog, as CNM occurs naturally in dogs. Because of its remark-able similarity with the disease in man, canine CNM can serveas a model to further our knowledge of the effects of succi-nylcholine.
OBJECTIVES We examined the kalaemic and neuromuscu-lar effects of succinylcholine in dogs with and without auto-somal-recessive CNM.
DESIGN A prospective, experimental study.
SETTING Anaesthesiology laboratory, College of VeterinaryMedicine, Cornell University, New York, USA.
PATIENTS Six dogs with autosomal-recessive CNM and sixcontrol dogs.
INTERVENTIONS Dogs received succinylcholine 0.3 mgkg�1 during isoflurane anaesthesia.
ht © European Society of Anaesthesiology. Un
m the Department of Clinical Sciences, College of Veterinary Medicine (MM-F, MDdicine, Cornell University, Ithaca, New York, USA (MR, EAT)
rrespondence to Manuel Martin-Flores, DVM, DACVAA, College of Veterinary Medmail: [email protected]
65-0215 Copyright � 2015 European Society of Anaesthesiology. All rights reser
MAIN OUTCOME MEASURES Whole blood potassiumconcentration was measured 5 min before and after succi-nylcholine administration. Neuromuscular function wasmeasured with acceleromyography and single twitch stimu-lation.
RESULTS All dogs recovered uneventfully from anaesthesia.The increase in potassium concentration [mean (SD)] follow-ing succinylcholine was similar between groups: CNM 0.5(0.4) mmol l�1 and control 0.7 (0.4) mmol l�1 (P¼0.47).Recovery of the single twitch to 25, 75 and 90% was longerin the CNM group (all P<0.001); 90% recovery took 35.5(1.18) min for the CNM group and 23.3 (1.68) min for thecontrol group.
CONCLUSION CNM did not exacerbate the increase inblood potassium that is ordinarily seen with succinylcholine.Recovery from succinylcholine was nearly 50% longer indogs with CNM. Although our sample size is too small toevaluate the incidence of succinylcholine-induced hyperka-laemia, extrapolation of these findings suggests thatincreased duration of action should be expected if succi-nylcholine is given to a patient with autosomal-recessiveCNM.
Published online 21 January 2015
Introduction
Centronuclear myopathy (CNM), also called myotubularmyopathy, is a congenital disease characterised by
centrally placed nuclei and generalised muscle weak-
ness.1 CNM exists in X-linked recessive, autosomal-
recessive and autosomal-dominant forms. The severity
of muscular weakness and associated complications such
as respiratory failure is greatest for the X-linked form and
mildest for the autosomal-dominant form.1 From obser-
vations in France, the incidence of confirmed X-linked
CNM is reported to be approximately 2/100 000 male
authorized reproduction of this article is prohibited.
P, LC, RDG), and Cornell University Hospital for Animals, College of Veterinary
icine, Cornell University, Ithaca, NY, 14853 USA
ved. DOI:10.1097/EJA.0000000000000222

Cop
Succinylcholine and centronuclear myopathy 667
births per year; however, the overall incidences of other
forms of CNM are unknown.1
Hyperkalaemia and even fatal rhabdomyolysis have
been associated with the use of neuromuscular blocking
agents such as succinylcholine (SCh) in patients with
other myopathies and some diseases that affect muscle
development, such as Duchenne muscular dystrophy.2–8
Little is known about CNM because its rarity means that
there is very little objective information available
regarding the use of neuromuscular blocking agents
in these individuals. From the available reports, it is
apparent that neuromuscular blocking agents are
usually avoided.9–11 Some anaesthesiologists have even
opted to remove SCh from the operating room when
anaesthetising patients with X-linked CNM, presum-
ably to avoid accidental use.12 Administration of SCh to
patients with unrecognised myopathies has been
reported, in some cases with fatal results.6,13 To our
knowledge, there are no reports on the effects of SCh in
patients with CNM.
Autosomal-recessive CNM has been described in Lab-
rador retriever dogs.14 Clinical signs and histological
characteristics of CNM in these animals are identical
to those encountered in man.15 To our knowledge, the
canine model is the only naturally occurring model avail-
able and it reflects very closely the changes that occur
with autosomal-recessive CNM in humans.15 The rarity
of CNM and the potentially lethal consequences of
hyperkalaemia exclude prospective investigations into
the use of SCh in patients, and accordingly, we have
chosen to use canine CNM as a model for a prospective
investigation into the effects of agents used during gen-
eral anaesthesia in man.
In this pilot investigation, we compared the kalaemic and
neuromuscular effects of SCh in dogs with CNM against
those in control animals. We hypothesised that the
increase in blood potassium (Kþ) after SCh adminis-
tration would be greater in CNM dogs than in normal
control animals and that the duration of neuromuscular
block would be longer in the affected animals.
Materials and methodsAnimalsSix purpose-bred adult Labrador retriever dogs with
diagnosed autosomal-recessive CNM, weighing 20.4 to
33.3 kg, and a group of six healthy adult purpose bred
beagles, weighing 7.1 to 11.3 kg were used. Sample size
was limited by the availability of animals with CNM.
Autosomal-recessive canine CNM was diagnosed
through DNA testing by an independent laboratory
(DDC Veterinary, Fairfield, Ohio, USA). None of the
dogs were receiving any type of medication before this
study. All procedures were approved by the Cornell
Institutional Animal Care and Use Committee (Protocol
number 2012-0088; 19 July 2012).
yright © European Society of Anaesthesiology. U
General anaesthesia and neuromuscular monitoringFood but not water was withheld overnight prior to
anaesthesia. A catheter was placed in a cephalic vein
and dexmedetomidine (Dexdomitor; Orion Corporation,
Espoo, Finland) 2 mg kg�1 was administered intra-
venously (i.v.). General anaesthesia was induced with
i.v. propofol (Propoflo; Abbott Laboratories, North Chi-
cago, Illinois, USA) 2 mg kg�1. The trachea was intubated
and the lungs were ventilated to normocapnia with iso-
flurane (Isothesia; Butle Schein Animal Health, Dublin,
Ohio, USA) (end-tidal concentration 1.3 to 1.5%) in
oxygen. Dexmedetomidine 2 mg kg�1 h�1 and lactated
Ringer’s solution (5 ml kg�1 h�1) were infused through-
out the procedure. The electrocardiogram, SpO2, capno-
graphy, end-tidal isoflurane concentration, systemic
arterial blood pressure waveform and oesophageal
temperature were monitored continuously. Oesophageal
temperature was maintained between 378C and 388C by
the use of a forced warm air device.
Neuromuscular function was assessed on a thoracic limb
with acceleromyography (AMG; TOF Watch SX, Orga-
non, Ireland) as described previously.16 Briefly, with the
dog in left lateral recumbency, the dependent limb was
held extended and slightly elevated so that the carpus
and manus (paw) could flex freely during nerve stimu-
lation. A 150 g elastic preload was applied to the paw to
facilitate return of the carpus to an extended position
during neuromuscular monitoring. Stimulating needles
were placed subcutaneously over the ulnar nerve and the
acceleration transducer was taped to the palmar aspect of
the paw. After at least 30 min of general anaesthesia and
15 min of single twitch stimulation (0.1 Hz, pulse
duration 0.2 ms, 50 mA), the AMG monitor was calibrated
(CAL 2). Single twitch stimulation was then resumed.
After the single twitch signal had been stable for at least
3 min, SCh 0.3 mg kg�1 was administered i.v. as a fast
bolus through a free-flowing infusion of the isotonic
crystalloid solution. This dose produces complete neu-
romuscular block in normal dogs.17,18 During recovery
from SCh, the changes in the height of the single twitch
were recorded until no further increases were observed
for at least 5 min. The average of the first six values for
single twitch amplitude after the recovery plateau was
established was used as the final single twitch amplitude.
All values for single twitch after administration of SCh
were normalised to this final single twitch value.19
Arterial blood was sampled 5 min before and 5 min after
injection of SCh for analysis of electrolytes, glucose and
acid–base status with a point-of-care device (i-STAT
system; Abbott Point of Care Inc, Princeton, New Jersey,
USA). Blood samples were obtained from the arterial
catheter and analysed immediately.
Statistical analysisThe distribution of all variables was tested for normality
(Shapiro–Wilk test, Minitab 16.2.4). Whole blood
nauthorized reproduction of this article is prohibited.Eur J Anaesthesiol 2015; 32:666–671

Copyr
668 Martin-Flores et al.
potassium concentration before and after SCh adminis-
tration were compared within groups with the paired
t-test. The increase in Kþ concentration relative to base-
line was compared between groups with the two-sample
t-test. The sensitivity (gain) of the AMG monitor and all
recovery variables [return of single twitch to 25, 75 and
90% of the final single twitch height and recovery index
(interval between ST 25 and 75%)] were compared
between groups with two-sample t-tests. Differences
were considered significant when P value was less than
0.05. All parametric data are summarised as mean (SD).
Descriptive statistics [nonparametric distribution;
median (IQR)] for electrolytes other than Kþ, acid–base
variables and glucose before and after SCh administration
are also presented.
ResultsAll dogs recovered uneventfully from general anaesthe-
sia. A transient decrease in arterial blood pressure of at
least 20% was observed in two CNM dogs following SCh.
These changes were self-limiting and required no inter-
vention.
Kalaemic, other electrolytic, acid–base and glucoseeffects of succinylcholineIn two animals from the control group, venous blood
samples were used in lieu of arterial samples because of
failure of the arterial catheter. Following SCh adminis-
tration, Kþ increased by 0.5 (0.4) mmol l�1 [16% (1.15)] in
the CNM group and by 0.7 (0.4) mmol l�1 [18% (1.2)] in
control dogs; each was a significant increase from base-
line; P¼ 0.03 and 0.01, respectively (Fig. 1). However,
the percentage increase from baseline was not different
between groups (P¼ 0.47). Other electrolyte, acid–base
and glucose values obtained before and after Sch admin-
istration are summarised in Table 1. There was a little
change after SCh was given.
ight © European Society of Anaesthesiology. Un
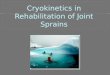
Fig. 1
5.0
4.5
4.0
3.5
3.0
2.5Pre Post
Control
K+
(m
mol
L–1
)
Blood potassium concentration before and after succinylcholine 0.3 mg kg�1
�Significant increase from baseline after succinylcholine; P<0.05. Howeve
Eur J Anaesthesiol 2015; 32:666–671
Neuromuscular effects of succinylcholineOnset time was 1.4 (0.4) min for CNM and 1.7 (0.6) min
for control dogs (P¼ 0.47). Times to 25, 75 and 90%
recovery were significantly longer (P� 0.001) for CNM
dogs than for controls (Fig. 2). The recovery index
was not significantly different between the treatment
groups [CNM 8.3 (3.5) vs. control 3.9 (2.1) min; P¼ 0.15].
Performance of acceleromyographyCalibration of the AMG required several attempts in dogs
affected with CNM, in which the evoked excursion of the
paw was minimal. After calibration, the AMG reports the
value of sensitivity (gain) required to set the control
response to 100%. The sensitivity after calibration was
significantly greater for CNM dogs [CNM 481 (30) vs.
control 308 (80); P¼ 0.003], suggesting that signal ampli-
fication by the AMG monitor was larger in those animals.
In one dog with CNM, the gain had to be increased
manually to its maximum (512) because calibration failed
after several attempts. We did not encounter any pro-
blems during AMG calibration in control animals.
In three out of six dogs with CNM, the AMG monitor
reported single twitch values between 10 and 20% at a
time when neuromuscular block was expected to be
maximal and when evoked motor response could neither
be seen nor palpated (Fig. 3). Such erroneous measure-
ments were not observed in the control dogs (Fig. 3).
DiscussionOur results show that the increase in Kþ after SCh was
similar for the two groups of dogs. No electrocardio-
graphic signs consistent with hyperkalaemia, such as tall
T waves, absence of P waves or wide QRS complexes,
were observed at any time.20 In two CNM dogs, we
observed a transient decrease in arterial blood pressure
after SCh, which resolved spontaneously. This might
have been due to histamine release, but no other signs
authorized reproduction of this article is prohibited.
5.0
4.5
4.0
3.5
3.0
2.5Pre Post
CNM
in dogs with autosomal-recessive centronuclear myopathy and controls.r, the increase was similar between groups.

Cop
Succinylcholine and centronuclear myopathy 669
Table 1 Median (interquartile range) concentration of electrolytes, acid–base status and glucose concentration measured 5 min before (Pre)and 5 min after (Post) succinylcholine was given to centronuclear myopathy and control dogs
CNM Control
NormalPre Post Pre Post
pH 7.39 (0.03) 7.39 (0.04) 7.3 (0.04) 7.3 (0.02) 7.35 to 7.45SBE (mmol l�1) �1 (1.5) 0 (3.25) �2.5 (2) �3 (2) �5 to 0Naþ (mmol l�1) 142.5 (1.75) 142.5 (4.75) 143.5 (3.5) 141.5 (5.25) 139 to 150iCa2þ (mmol l�1) 1.29 (0.11) 1.3 (0.09) 1.38 (0.07) 1.36 (0.03) 1.12 to 1.4Glucose (mg dl�1) 122 (26) 118.5 (36) 96 (18.5) 106.5 (11.5) 60–115
iCa2þ, ionized calcium; CNM, centronuclear myopathy; SBE, standard base excess.
such as flushing of the mucous membranes, urticaria or
signs of bronchospasm were observed. As the highest Kþ
concentrations recorded did not exceed the normal limit
for dogs (5.5 mmol l�1), it appears unlikely that an
increase in Kþ was responsible for these haemodynamic
changes.20 Moreover, the increment in Kþ observed in
both groups after SCh is in agreement with previous
reports in man (0.5 to 1 mmol l�1).21 In our study, Kþ
was measured 5 min after SCh administration; we chose
5 min because in humans, the increase in Kþ induced by
SCh peaks at 3 to 4 min.2,22,23
Succinylcholine-induced hyperkalaemia has been
reported in a variety of pathological states including
muscle trauma (inflammatory or thermal), upper and
lower motor neurone defects and severe infection,2–5
when SCh may be contraindicated. In patients with
disease of this nature, upregulation of extrajunctional
(fetal or immature) acetylcholine receptors and also an
isoform of the acetylcholine receptor, known as a7AChR,
is observed. Upon interaction with SCh, depolarisation of
extrajunctional and a7AChR occurs resulting in an exag-
gerated efflux of Kþ.23 As we did not observe hyperka-
laemia in dogs with CNM, it is unlikely that significant
upregulation of these receptors occurred. Recent obser-
vations of endplates of an individual affected with CNM
found a reduced number of acetylcholine receptors per
yright © European Society of Anaesthesiology. U
Fig. 2
100
80
60
40
20
00 10 20 30 40 50
ST
(%
)
Time (minutes)
*
*
*
CNM
Control
Spontaneous recovery of the single twitch (ST) to 25, 75 and 90%(normalised to final single twitch value) after succinylcholine0.3 mg kg�1 in dogs with autosomal-recessive centronuclear myopathy(CNM) and controls. �Significant difference between groups; P<0.05.
endplate and a reduction in the acetylcholine receptor
index. The authors also observed formation of immature
endplate regions that could potentially express immature
acetylcholine receptors.24
Succinylcholine is usually avoided in patients with malig-
nant hyperthermia, as it is known to trigger the condition.
The skeletal muscle ryanodine receptor (RYR1) gene has
been implicated in the development of MH and recent
evidence has shown that RYR1 mutations can also be
involved in the development of some forms of myopa-
thies with central nuclei or in patients presenting with
mixed diseases that include both core and central
nuclei.25,26 In at least one instance, malignant hyperther-
mia has developed in an anaesthetised patient with
CNM.27 Although many cases of CNM remain geneti-
cally unresolved,28 it has been suggested that RYR1
mutations might be common in individuals with CNM
and that they should be considered at risk for developing
malignant hyperthermia.26 Our experience with dogs
with autosomal-recessive CNM provided no evidence
of any signs of malignant hyperthermia being triggered
by SCh or isoflurane. Of note, this group of dogs has been
anaesthetised at least four times with isoflurane or
sevoflurane for different unrelated investigations; no
complications indicative of malignant hyperthermia were
observed.
Although there were no differences between groups in
onset time, our results show moderately longer duration
of neuromuscular blockade in dogs with CNM; the
recovery of the single twitch to 90% was delayed in
the CNM dogs by nearly 10 min. The difference in the
recovery index between groups did not quite reach
significance, but it is possible that our sample size is
too small to detect such a difference. We chose a dose of
SCh of 0.3 mg kg�1 in our investigation. Although this
dose might appear lower than that typically used in
humans, in dogs, it is commonly used to produce com-
plete block;17,18 the return of the first twitch of the TOF
to 80% of baseline after 0.3 mg kg�1 SCh takes 20 to
30 min.17,18 It is possible that the longer duration of
neuromuscular block observed in the CNM dogs could
be attributed to breed differences (Labrador retriever vs.
beagle), but no breed-specific alterations in the time-
course of neuromuscular blockers have been reported for
dogs. Furthermore, when duration of SCh was compared
nauthorized reproduction of this article is prohibited.Eur J Anaesthesiol 2015; 32:666–671

Copyr
670 Martin-Flores et al.
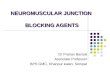
Fig. 3
100
50
00 10 20 30 40
Time (minutes)
ST
(%
)
100
50
00 10 20 30 40
Time (minutes)
ST
(%
)
Control CNM
No visible twitch
Examples of the single twitch (ST) height after succinylcholine 0.3 mg kg�1 (time zero) in a control dog and one with centronuclear myopathy (CNM).In the CNM dog, twitch heights of �20% continued to be displayed by the monitor despite the absence of any observable evoked twitch.
between greyhounds and mixed breed dogs, no differ-
ences were observed.29 It appears that the differences in
recovery times that we observed between control and
CNM dogs are relatively benign, especially if the extent
of neuromuscular blockade is being measured objec-
tively.
Acceleromyographic monitoring in dogs with CNM
proved challenging. Several attempts were required
before calibration could be performed. This was not
the case in the control animals, nor has it been our
experience when using similar protocols in earlier work.
In one dog, calibration was not possible and the gain was
manually increased to its maximum. During calibration of
the AMG, the signal (gain) is amplified so that the
response can be set to 100%. It follows that small evoked
responses might require higher signal amplification.
When signal amplification is high, the potential for erro-
neous measurements arising from background noise, such
as movement from surgical table, increases. In dogs with
CNM, the sensitivity used by the AMG was significantly
higher than in the control group, indicating higher signal
amplification. In these dogs, erroneous results were
observed at the time of complete block; the AMG dis-
played twitch heights of up to 20% when no visible or
palpable twitch could be detected (Fig. 3). This obser-
vation suggests that AMG monitoring might be prone to
erroneous measurements whenever the evoked response is
very small (and signal amplification high), as is the case in
many patients with neuromuscular disease. Similar diffi-
culties have been reported when calibrating an AMG
monitor on neonates and small infants and whether the
sensitivity of the AMG monitor is adequate for patients
producing small responses is in question.30 Presumably,
our experience of myopathic dogs represented an exag-
geration of that observation.
ight © European Society of Anaesthesiology. UnEur J Anaesthesiol 2015; 32:666–671
Our study has limitations. The sample size is small
reflecting the availability of animals with CNM and
because this is an animal model with small numbers,
our findings cannot be extrapolated directly to humans.
Nevertheless, this study adds information that might be
relevant to anaesthesiologists presented with patients
with this rare condition. The dogs in this study were
autosomal-recessive; we cannot exclude the possibility
that autosomal-dominant individuals might behave
differently. Weakness in individuals with CNM can
worsen mildly with time.1 We cannot speculate on how
progression of the disease might affect the duration and
effects of SCh. We compared groups of dogs of different
breeds and different size and weight; the control group
was composed of beagles, which were smaller than the
Labradors with CNM. Beagles are commonly used for
research purposes, and to our knowledge, no breed-
related differences in the response to neuromuscular
blockers have been reported in dogs. We did not measure
cholinesterase activity in either group, and hence, we
cannot comment on whether that could have influenced
the duration of action of SCh. However, it is noteworthy
that duration of SCh in the beagles is in accord with
previous reports.16,17 Whole blood Kþ concentrations
were only measured at baseline and 5 min after SCh
administration and it is possible that higher values of
Kþ could have gone unnoticed. However, no electrocar-
diographic changes indicative of hyperkalaemia were
observed at any point in any of the dogs. Rhabdomyolisis
has been reported after SCh was given to patients with
other myopathies.6 Although specific biomarkers for
muscle injury were not measured in these experi-
ments, all of the animals returned quickly to their pre-
experimental condition and none had signs of muscle
pain, suggesting that any muscle injury was minimal in
these animals.
authorized reproduction of this article is prohibited.

Cop
Succinylcholine and centronuclear myopathy 671
In summary, SCh 0.3 mg kg�1 resulted in similar onset
but longer duration of action in dogs with autosomal-
recessive CNM than in control ones. Autosomal-recessive
CNM did not exacerbate the increase in Kþ ordinarily
seen after succinylcholine in these animals. Although our
sample size is too limited to evaluate the incidence of
succinylcholine-induced hyperkalaemia, extrapolation of
these findings suggests that increased duration of action
should be expected if succinylcholine is given to a patient
with autosomal-recessive CNM.
Acknowledgements relating to this articleAssistance with the study: none.
Financial support and sponsorship: this work was supported by
the Section of Anesthesiology, College of Veterinary Medicine,
Cornell University.
Conflicts of interest: none.
Presentation: none.
References1 Jungbluth H, Wallgren-Pettersson. Laporte J. Centronuclear (myotubular)
myopathy. Orphanet J Rare Dis 2008; 3:26.2 Mazze RI, Escue HM, Houston JB. Hyperkalemia and cardiovascular
collapse following administration of succinylcholine to the traumatizedpatient. Anesthesiology 1969; 31:540–547.
3 Tolmie JD, Joyce TH, Mitchell GD. Succinylcholine danger in the burnedpatient. Anesthesiology 1967; 28:467–470.
4 Cooperman LH. Succinylcholine-induced hyperkalemia in neuromusculardisease. JAMA 1970; 213:1867–1871.
5 Kohlschutter B, Baur H, Roth F. Suxamethonium-induced hyperkalaemia inpatients with severe intra-abdominal infections. Br J Anaesth 1976;48:557–561.
6 Gurnaney H, Brown A, Litman RS. Malignant hyperthermia and musculardystrophies. Anesth Analg 2009; 109:1043–1048.
7 Schmidt J, Muenster T, Wick S, et al. Onset and duration of mivacurium-induced neuromuscular block in patients with Duchenne musculardystrophy. Br J Anaesth 2005; 96:769–772.
8 Wick S, Muenster T, Schmidt J, et al. Onset and duration ofrocuronium-induced neuromuscular blockade in patients withDuchenne muscular dystrophy. Anesthesiology 2005; 102:915–919.
9 Breslin D, Reid J, Hayes A, Mirakhur RK. Anaesthesia in myotubular(centrouclear) myopathy. Anaesthesia 2000; 55:471–474.
10 Gottschalk A, Heiman-Patterson T, deQuevedo R 2nd, Quinn PD. Generalanesthesia for a patient with centronuclear (myotubular) myopathy.Anesthesiology 1998; 89:1018–1020.
yright © European Society of Anaesthesiology. U
11 Tokarz A, Gaszynski T, Gazsynski W, Arkuszewski P. General anesthesiawith remifentanil and propofol for a patient with centronuclear (myotubular)myopathy. Eur J Anaesthesiol 2002; 19:842–844.
12 Costi D, Van der Walt J. General anesthesia in an infant with X-linkedmyotubular myopathy. Pediatr Anesth 2004; 14:964–968.
13 Segura LG, Lorenz JD, Weingarten TN, et al. Anesthesia and Duchenne orBecker muscular dystrophy: review of 117 anesthetic exposures. PediatrAnesth 2013; 23:855–864.
14 Kramer JW, Hegreberg GA, Bryan GM, et al. A muscle disorder of Labradorretrievers characterized by deficiency of type II muscle fibers. J Am Vet MedAssoc 1976; 169:817–820.
15 Pele M, Tiret L, Kessler J-L, et al. SINE exonic insertion in the PTPLA geneleads to multiple splicing defects and segregates with the autosomalrecessive centronuclear myopathy in dogs. Hum Mol Genet 2005;14:1417–1427.
16 Martin-Flores M, Gleed RD, Basher KL, et al. TOF-Watch monitor: failure tocalculate the train-of-four ratio in the absence of baseline calibration inanaesthetized dogs. Br J Anaesth 2012; 108:240–244.
17 Jones RS, Heckmann R, Wuersch W. Observations on the duration of actinof suxamethonium in the dog. Br Vet J 1978; 134:521–523.
18 Cullen LK, Jones RS. The nature of suxamethonium neuromuscular block inthe dog assessed by train-of-four stimulation. Res Vet Sci 1980; 29:281–288.
19 Fuchs-Buder T, Claudius C, Skovgaard LT, et al. Good clinical researchpractice in pharmacodynamics studies of neuromuscular blocking agentsII: the Stockholm revision. Acta Anaesthsiol Scand 2007; 51:789–808.
20 Schaer M. Therapeutic approach to electrolyte emergencies. Vet ClinNorth Am Small Anim Pract 2008; 38:513–533.
21 Yentis SM. Suxamethonium and hyperkalaemia. Anaesth Intensive Care1990; 18:92–101.
22 Collier CB. Suxamethonium pains and early electrolyte changes.Anaesthesia 1978; 33:454–461.
23 Martyn JA, Richtsfeld M. Succinylcholine-induced hyperkalemia in acquiredpathologic states. Etiologic factors and molecular mechanisms.Anesthesiology 2006; 104:158–169.
24 Liewluck T, Shen XM, Milone M, Engel AG. Endplate structure and para-meters of neuromuscular transmission in sporadic centronuclear myopathyassociated with myasthenia. Neuromuscul Disord 2011; 21:387–395.
25 Jungbluth H, Zhou H, Sewry CA, et al. Centronuclear myopathy due to a denovo dominant mutation in the skeletal muscle ryanodine receptor (RYR1)gene. Neuromuscul Disord 2007; 17:338–345.
26 Wilmshurst JM, Lillis S, Zhou H, et al. RYR1 mutations are a common causeof congenital myopathies with central nuclei. Ann Neurol 2010; 68:717–726.
27 Quinn RD, Pae WE, McGary SA, Wickey GS. Development of malignanthyperthermia during mitral valve replacement. Ann Thorac Surg 1992;53:1114–1116.
28 Jeannet PY, Bassez G, Eymard B, et al. Clinical and histological findings inautosomal centronuclear myopathy. Neurology 2004; 35:1484–1490.
29 Curtis MB, Eicker SE. Pharmacodynamic properties of succinylcholine ingreyhounds. Am J Vet Res 1991; 52:898–902.
30 Driessen JJ, Robertson EN, Booij LH. Acceleromyography in neonates andsmall infants: baseline calibration and recovery of the responses afterneuromuscular blockade with rocuronium. Eur J Anaesthesiol 2005;22:11–15.
nauthorized reproduction of this article is prohibited.Eur J Anaesthesiol 2015; 32:666–671