Embed Size (px)
Citation preview

T H E J O U R N A L O F T H E E U R O P E A N A S S O C I A T I O N F O R P A L L I A T I V E C A R E
European Journal ofPalliative Care COMMENT
265 Love your data Ros Taylor
CliNiCal MaNagEMENT
266 Managing malignant bowel obstruction with lanreotide in the community
Kate Markham, Shan Shan Vijeratnam and Pia Amsler
SpONSOrED arTiClE – CliNiCal MaNagEMENT
270 Treating cancer pain Andrew Dickman
MulTiDiSCipliNary TEaM
278 Paediatric palliative nursing: the tensionbetween closeness and professional distance
Regula Buder and Andre Fringer
pErSpECTiVE
282 The convenient death of King George V: a look back at history
Sandy Macleod and Jane Vella-Brincat
pErSpECTiVE
285 The Sydney Institute of Palliative Medicine:evolution and contribution
Ghauri Aggarwal, Jan Maree Davis, Frank Brennan and Kristen Turner
rESEarCh
290 Does current UK research address priorities in palliative and end-of-life care?
Florence Todd Fordham, Bridget Candy, Stevie McMillan and Sabine Best
hOliSTiC CarE
294 Mindfulness meditation and pain management in palliative care
Irene Campagnolo Maschio
CliNiCal MaNagEMENT
299 Antibiotic use in the last two weeks of life for home hospice patients in Singapore
Ong Eng Koon and Chong Poh Heng
rESEarCh
305 EAPC Early Researcher Award 2013 – looking back
Meera Agar, Barbara Gomes and Jeroen Hasselaar
EurOpEaN iNSighT
309 Romanian National Association for Palliative Care: quality assurance for palliative care in Romania
Malina Dumitrescu and Vladimir Poroch
November/December 2016, Volume 23 Number 6 www.ejpc.eu.com
Visitwww.ejpc.eu.comto read the current issue online or to access the EJPC archive
Book review
››A Practical Guide to End of Life CareCarmel Grealish
page281
Case 89Managing symptoms ofneuroendocrine tumours in a 62-year-old man with impaired cognitionAndrew Gill
page276
The case study masterclass
Copyright © Hayward Medical Communications 2016. All rights reserved. No unauthorised reproduction or distribution. For reprints or permissions, contact [email protected]

EUROPEAN ASSOCIATION FOR PALLIATIVE CARE
www.eapcnet.eu
SOCIEDAD ESPAÑOLA DE CUIDADOS PALIATIVOS
www.secpal.com
Congress OrganisationINTERPLAN Congress, Meeting & Event Management AGLandsberger Str. 15580687 Munich, Germany
Phone: +49 (0)89 - 54 82 34-771Fax: +49 (0)89 - 54 82 34-44
Email: [email protected]
See you in Madrid!
More information: www.eapc-2017.org
EAPC 201715th World Congress of the European Association for Palliative CareProgressing Palliative Care
18 – 20 May 2017 Madrid, Spain
Register at: www.eapc-2017.org
© M
adri
d V
isit
ors
& C
onve
nti
on B
urea
u, 2
013,
NoP
hot
o
11:50

263EUROPEAN JOURNAL OF PALLIATIVE CARE, 2016; 23(6)
www.ejpc.eu.com
For further contact details, and information regarding subscriptions, please see overleaf ››
T H E J O U R N A L O F T H E E U R O P E A N A S S O C I A T I O N F O R P A L L I A T I V E C A R E
European Journal ofPalliative Care
Publisher Sarah Strachan. Publications ManagerMartin Griffiths. Managing Editor Paul Docherty. Junior Editorial Project Manager Annabel Gammon. Advertising and Subscriptions Co-ordinator Harriet Abbs. Art Editor Richard Seymour. Designer Juliana Carey.
The data, opinions and statements appearing in the articles herein are those of the contributor(s) concerned; they are not necessarily endorsed by the Publisher, Editors or Editorial Advisory Board.Accordingly, the Publisher, Editors and Editorial Advisory Board and their respective employees, officers and agents accept no liability for the consequences of any such inaccurate or misleading data,opinion or statement. The European Journal of Palliative Care is abstracted/indexed in the Cumulative Index to Nursing and Allied Health Literature (CINAHL) and Scopus. Articles from the European Journal of Palliative Care are also indexed in Scirus. The titles the European Journal of Palliative Care and le Journal Européen de Soins Palliatifs are the property of Hayward Group Ltd and, together with the content, are bound by copyright. Copyright © 2016 Hayward Group Ltd. All rights reserved. ISSN 1352-2779 (Print). ISSN 1479-0793 (Online). Printed by The Magazine Printing Company Plc.Cover picture:Madonna with Pomegranate, Reuven Rubin (born 1893) © SuperStock/SuperStock
Editor
Professor Julia Riley, London, UK
Deputy Editors
Dr Carol Davis, Southampton, UK
Professor Philip Larkin, Dublin, Ireland
Editorial Advisory Board
Dr Carlos Centeno, Pamplona, Spain
Dr Massimo Costantini, Reggio Emilia, Italy
Dr Joanne Droney, London, UK
Dr Marilène Filbet, Lyon, France
Professor Bridget Johnston, Glasgow, UK
Dr Saskia Jünger, Bonn, Germany
Professor Stein Kaasa, Trondheim, Norway
Dr Daniela Mosoiu, Brasov, Romania
Professor David Oliver, Canterbury, UK
Professor Lukas Radbruch, Bonn, Germany
Professor Tiina Saarto, Helsinki, Finland
Professor Keri Thomas, Shrewsbury, UK
Corresponding Members of Editorial Advisory Board
Professor Eduardo Bruera, Houston, USA
Professor Cynthia Goh, Singapore, Republic of Singapore
Dr Emmanuel BK Luyirika, Kampala, Uganda
Professor Rod MacLeod, Sydney, Australia
Dr Faith Mwangi-Powell, Nairobi, Kenya
Professor Russell K Portenoy, New York, USA
Dr Luzito J de Souza, Mumbai, India
Dr Roberto Wenk, Buenos Aires, Argentina
Dr Mohammad Zafir Al-Shahri, Riyadh, Saudi Arabia
Book Reviews EditorDr Vinnie Nambisan, London, UK
Published by Hayward Medical Communications, a division of Hayward Group Ltd.Address for correspondence The Pines, Fordham Road, Newmarket CB8 7LG, UK. Tel+44 (0)1638 723560. Fax+44 (0)1638 723561.Registered office 8–10 Dryden Street, Covent Garden, London WC2E 9NA, UK. Email [email protected] Editorial enquiries email [email protected] Website www.hayward.co.uk
Copyright © Hayward Medical Communications 2016. All rights reserved. No unauthorised reproduction or distribution. For reprints or permissions, contact [email protected]

264 EUROPEAN JOURNAL OF PALLIATIVE CARE, 2016; 23(6)
The European Journal of Palliative Care is anofficial journal of the European Association for Palliative Care, Onlus (EAPC). The EAPC was established to promote palliative care inEurope and to act as a focus for all those who work, or have an interest, in the field of palliative care.
It is the goal of the EAPC to gather andrepresent all healthcare professionals andvolunteers working in palliative care acrossEurope and to include as many members aspossible in the daily life of the association.
The EAPC was created in 1988 by42 founding members from nine Europeancountries. It has grown rapidly since itsfoundation. In 2016, the EAPC has individualmembers from 48 countries across the worldand collective members from 57 nationalassociations in 32 European countries,representing a movement of many thousandsof health- and social care workers andvolunteers contributing to palliative care.
If you would like to know more and/orbecome a member of the EAPC, please visitwww.eapcnet.eu
If you have any questions aboutsubscriptions, please email:
For any editorial queries,please email:
For information on how toadvertise in the journal,please contact:
Tel: +44 (0)1638 723560email: [email protected]
ContactsSubscriptions
The European Journal of Palliative Care (EJPC) is available only on subscription. Each subscription runs for one year (six issues).
We are currently offering three levels of subscription:
Online onlyYou will be able to access the
current issue PLUS all the articles in the EJPC archive in PDF format.
n
Print onlyYou will receive six issues
per year of the printed journal.
n
Print AND onlineYou will receive six issues per year of the printed journal AND you will be able to
access the current issue PLUS all the articles in the EJPC archive in PDF format.
Type of Personal Institution*subscription EAPC member Non-member
Online only £85 £100 £300
Print only £75 £100 £275
Print AND online £130 £150 £425
Annual subscription rates: Europe
Type of Personal Institution*subscription EAPC member Non-member
Online only £85 £100 £300
Print only £125 £150 £350
Print AND online £180 £200 £475
Annual subscription rates: rest of the world
* The rates quoted for institutions are for non-teaching/non-research use in a hospital palliative care department, in ahospice at a single site or for a hospital library at a single site. Large academic institutions, multiple-site universities,multiple-site and multinational organisations, and institutions offering related training courses should apply for a quotationtailored to their requirements. Please contact us at: [email protected]
Subscribe online atwww.ejpc.eu.com
Copyright © Hayward Medical Communications 2016. All rights reserved. No unauthorised reproduction or distribution. For reprints or permissions, contact [email protected]

265EUROPEAN JOURNAL OF PALLIATIVE CARE, 2016; 23(6)
www.ejpc.eu.com Comment
The goal is to turn data into information, and information into insight.
Carly Fiorina, former CEO, Hewlett Packard
B I remember Dame Barbara Monroe, retiredCEO of St Christopher’s, saying that a drawerfull of thank-you letters wasn’t enough tounderstand the impact of your service. Ithought she was wrong at the time – but I nowknow she was right! Quality is certainly aboutpatient and family experience, and we need tosystematically collect experience data beyondletters, but it’s also about outcomes, impactand reach. The reach of a service is critical – andreach is about knowing whom you aresupporting and those whose needs are notbeing met. Those unmet needs are the leversfor change, for funds, for making a difference.So counting is one thing – but perhaps morecrucially, noticing trends, benchmarking withothers and understanding local demographicsare vital steps on the way to comprehensivepalliative care for all.
We know that many people who might benefitfrom palliative care are still not being seen – thismeans there is physical and emotional suffering,‘total pain’ on a significant scale in a country ratedtop of the world in palliative care.1 Without acomplete national data set, the story is so difficult totell. My first plea then is to all organisations, NHSand charitable, who are collecting data that you aregenerous and brave enough to share your numbers.Only then can we tell the stories that need to betold about unmet need, about whether preferencesare being met, about how people are dying.
So what do we know now? The Minimum DataSet (MDS)2 has been collected from hospices andNHS teams in England, Wales and Northern Irelandfor over 20 years. It is supported by Public HealthEngland and Hospice UK and collated by theNational Council for Palliative Care. About 70% ofthe inpatient and community data comes fromcharitable hospices and 90% of the hospital datacomes from the NHS.
Key limitations of the MDS are that it misses outon Scottish and paediatric data and it countsnumbers of people attending different aspects of aservice (day care, inpatient care, home care) – itdoesn’t tell us the total number of individualpatients getting palliative support as a proportionof all deaths. That’s a vital unanswered question.
Despite its flaws, however, the MDS is stillconfirming important trends. Topline messages arethat community teams (hospice and NHS) areseeing approximately 30% of expected deaths,with 81% of community palliative patients dyingout of hospital, compared to the national averageof 50%. This is such an important statistic. It showsthat palliative support doubles the likelihood ofdying at home – what we don’t know is the mosteffective configuration of teams to do this.
The latest MDS also highlights the fact that mosthospice care now goes far beyond the hospicebuilding. There are only 2,760 hospice bedsnationally – so there will always be a cap on thenumber of possible inpatient hospice deaths,which stand at only about 6% of all deaths. But theMDS tells us that many hospices are influencing upto 30% of those in the last year of their lives,through their community and clinic teams – that’s astatistic we need to shout about.3
This year’s data also confirms an increase in thenumber of patients admitted to hospice beds fromhospital. This is good for hospital patients who nolonger need or want the intensity of hospital – butdoes this mean it is more difficult to get a hospicebed for patients in crisis at home?
Where could we do better? The answer must liein equity and diversity. Fifty years after the birth ofhospice care, services are still dominated by cancerpatients. The good news is that rates of referral topalliative care for heart disease, lung disease anddementia are rising. There are initiatives all aroundthe UK driving earlier palliative referral for alldiagnoses, sharing resources and expertise andrecognising that the suffering of cancer patients isuniversal to all those with advancing illness.4
So counting is crucial because data underpins allinnovation.5 We will certainly need to count differentthings in the future. But If we stop counting, then wewill never know the extent of support being offered,the national story will never be told – and those in‘total pain’ will continue to rise.C
Ros Taylor,ClinicalDirector, Hospice UK
References1. The Economist Intelligence Unit. Quality of Death Index. London: EIU, 2015.www.eiuperspectives.economist.com/healthcare/2015-quality-death-index(last accessed 05/10/16)2. National Council for Palliative Care. Minimum Data Set 2014–15. London: NCPC, 2015. www.ncpc.org.uk/sites/default/files/user/documents/MergedMDSinWord.pdf(last accessed 05/10/16)3. Hospice UK. Hospice Care in the UK 2016: Scope Scale and opportunities.London: Hospice UK, 2016.www.hospiceuk.org/docs/default-source/What-We-Offer/publications-documents-and-files/hospice-care-in-the-uk-2016.pdf?sfvrsn=04. Boland J, Johnson MJ. End-of-life care for non-cancer patients. BMJ SupportPalliat Care 2013; 3: 2–3.5. Commission into the Future of Hospice Care. Future ambitions for hospicecare: our mission and our opportunity. London: CFHC, 2013. www.hospiceuk.org/what-we-offer/publications?page=2 (last accessed 05/10/16)
Love your data
Copyright © Hayward Medical Communications 2016. All rights reserved. No unauthorised reproduction or distribution. For reprints or permissions, contact [email protected]

266 EUROPEAN JOURNAL OF PALLIATIVE CARE, 2016; 23(6)
Clinical management www.ejpc.eu.com
M alignant bowel obstruction is acommon distressing complicationin patients with advanced
abdominal or pelvic carcinoma.1,2 In mostpatients with advanced disease, surgicaloptions, such as a colostomy or ventinggastrostomy, may not be feasible due toperitoneal carcinomatosis, ascites, multipleco-morbidities and poor performance status,3
posing a challenge to healthcare professionals.The medical management of bowel
obstruction is complex. There is limited datato support lanreotide, a long-actingsomatostatin analogue, in this situation.4 Inour case, lanreotide significantly improved thesymptoms and quality of life of the patientsdescribed below, who were ambulatory andhad an undetermined prognosis, despiteadvanced intra-abdominal disease. We believethat lanreotide can be an effective treatmentin the community in this group of patients.
Case report 1This 61-year-old woman with a backgroundhistory of metastatic squamous cell carcinomaof the vagina continued to have diseaseprogression, despite treatment withchemotherapy and radiotherapy. During theinitial presentation of her illness, she wastaken to theatre for excision of the tumour butwas found to have extensive pelvic disease and instead received an end-colostomy.Following radiotherapy she developed a rightutero-cutaneous fistula, necessitating a rightnephrostomy and a left-side antegrade ureteric stent.
She was admitted to hospital with a sub-acute small bowel obstruction. A CT abdomenshowed ‘dilated proximal small bowel’. She
Managing malignant bowelobstruction with lanreotide in the communityThe medical management of malignant bowel obstruction in patients with advanced carcinoma is often
complicated by the presence of co-morbidities. Kate Markham, Shan Shan Vijeratnam and pia amsler
recount two cases that support the use of lanreotide in suitable patients
&Kate MarkhamMBChB MSc DTMH
DPMSA DCCM
Specialty Doctor inPalliative Care 1
Shan ShanSusanVijeratnamBM BSc MRCP
Specialist Registrarin PalliativeMedicine 2
Pia AmslerMD MRCP Dipl Pall Med
Medical Directorand Consultant 1
1 Isabel Hospice,Welwyn Garden City,Hertfordshire
2 Royal Free Hospital,London
was subsequently given intravenous fluids and had a nasogastric (NG) tube inserted. Hersymptoms then resolved; she was dischargedhome ten days later with support from theCommunity Palliative Care Support Team.
For the following five months, she remainedwell. Subsequently she re-presented withprofuse bilious vomiting, particularly aftermeals. She had hypoactive bowel sounds onabdominal examination and a diagnosis of intermittent small bowel obstruction wasmade. Surgical options were not possible, andshe also expressed clearly that she did not wantto have further admissions to hospital. Shedeclined a venting gastrostomy, as she alreadyhad multiple indwelling catheters in situ.Medications that could be used to treat hersymptoms included high-dose omeprazole,hyoscine butylbromide, haloperidol,levomepromazine and oxycodone IR.
The patient continued to be mobile and livean active lifestyle, with a WHO performancestatus of 1; her biggest complaint was herinability to enjoy a meal with her family.Titration of hyoscine butylbromide to a
n Consider the use of somatostatin analogue for patients in thecommunity with malignant bowel obstruction if other medicaltreatments fail.
n We recommend a trial of octreotide via syringe driver for one week initially to assess responsiveness before initiating lanreotide.
n Dose titration and frequency of injections need to be based on the clinical picture.
n Wider use of such treatment may reduce the need for admission to hospice or hospitals for symptom management and should betailored to patients’ individual needs and wishes.
Keypoints
Copyright © Hayward Medical Communications 2016. All rights reserved. No unauthorised reproduction or distribution. For reprints or permissions, contact [email protected]

267EUROPEAN JOURNAL OF PALLIATIVE CARE, 2016; 23(6)
www.ejpc.eu.com Clinical management
maximal dose of 120 mg/24 hours led tosome – but not satisfying – improvement ofher nausea and post-prandial vomiting. A trialof the somatostatin analogue octreotide wasinstigated subcutaneously; titration from 300to 900 mcg/24 hours led to an effective controlof her vomiting. During this time, shecontinued on oral hyoscine butylbromide fourtimes daily. Due to convenience, districtnursing time and the patient’s undeterminedprognosis, her treatment was converted to asingle intramuscular lanreotide injection.
Dose and interval titrationGiven the expense of lanreotide, an initialdose of 30 mg was administered, but nauseaand vomiting re-occurred after 10 days. Thedose was increased to 60 mg and a secondinjection was given 14 days after the initialsyringe driver had been discontinued; this wasthen repeated every four weeks. She had nofurther episodes of vomiting but continued tofeel nauseated three weeks after the injection.Consecutively, the dose was further increasedto 90 mg and the injection interval reduced tothree weeks (see Table 1).
To date, the patient describes a markedimprovement of her nausea and vomitingsince commencement of a somatostatinanalogue. Her quality of life has improvedsignificantly – she can travel with her familyin the UK instead of being homebound. Shehas not reported any adverse side effectsrelated to lanreotide injection.
Case report 2This 58-year-old woman had a 14-year history of ovarian carcinoma with a slow and grumbling course, and metastases present in her liver, bowel, peritoneum andhip. She received multiple treatments,including debulking surgeries and severalchemotherapies, but her disease progresseddespite these. She developed a vesicovaginalfistula, which caused her considerable distress.
After ongoing abdominal pain and nausea,a CT scan confirmed intermittent small bowel obstruction. She was started on asyringe driver with hyoscine butylbromide 60 mg and midazolam 5 mg. The hyoscinebutylbromide was gradually titrated up to 120 mg over 24 hours. This led to a resolve ofher colicky pain on defecation and eased a lotof her loose bowel, but unfortunately she still suffered nausea.
The patient was then switched tooctreotide via a syringe driver, initially at600 mcg over 24 hours, then increased to900 mcg and finally to 1,200 mcg over24 hours. This treatment provided effectivecontrol of both her nausea and colickyabdominal pain, and after one week she was
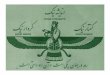
n Coloured X-ray of bariumenema. The orange/pinkcolours indicate areas wherebarium is able to pass freelythrough the bowel. The yellowarea in the centre indicates ablockage caused by a tumour.
SOvE
REIG
N/ISM
/SCIE
NCE P
HOTO
LIBR
ARY
Table 1. Symptom control
Case 1
First-line treatment: levomepromazine 12.5 mg/24 hrs via syringe driver; hyoscinebutylbromide titrated to 120 mg/24 hrs; oxycodone 60 mg/24 hrs via syringe driver
Second-line treatment: octreotide 300–900 mcg/24 hrs via syringe driver; oxycodone60 mg/24 hrs and levomepromazine 12.5 mg/24 hrs via syringe driver; oral hyoscinebutylbromide 20 mg qid
Third-line treatment: lanreotide 30–90 mg 3-weekly injection; oxycodone 60 mg/24 hrs;levomepromazine 12.5 mg/24 hrs via syringe driver; oral hyoscine butylbromide 20 mg qid
Case 2
First-line treatment: hyoscine butylbromide 60–120 mg/24 hrs; midazolam 5 mg/24 hrsvia syringe driver
Second-line treatment: octreotide 600–1,200 mcg/24 hrs; midazolam 5 mg/24 hrs viasyringe driver
Third-line treatment: lanreotide 30–60 mg 4-weekly injection; oxycodone 10 mg/24 hrs;levomepromazine 12.5 mg/24 hrs; hyoscine butylbromide 60 mg/24 hrs; midazolam5 mg/24 hrs via syringe driver
Copyright © Hayward Medical Communications 2016. All rights reserved. No unauthorised reproduction or distribution. For reprints or permissions, contact [email protected]

268 EUROPEAN JOURNAL OF PALLIATIVE CARE, 2016; 23(6)
Clinical management www.ejpc.eu.com
switched to injections of intramuscular30 mg lanreotide every four weeks.
Dose and titrationLanreotide was initially started at 30 mg everyfour weeks; two weeks later it was titrated upto 60 mg every four weeks, with the patientrequiring cyclizine in concordance.
Two months later the patient required aninpatient stay at the hospice, as she hadnausea and vomiting. A separate syringedriver containing oxycodone 10 mg,levomepromazine 12.5 mg, hyoscinebutylbromide 60 mg and midazolam 5 mgover 24 hours was commenced, whichcontrolled her symptoms well. This wascontinued instead of switchingback to oral drugs on discharge,as there was a significant degreeof malabsorption from thesmall bowel. Lanreotide wascontinued in order to avoid asecond syringe driver withoctreotide, allowing the patientmore freedom. To date, five months later, shecontinues to have this syringe driver alongsidefour-weekly 60 mg lanreotide injections togood effect (see Table 1). She has reported noadverse side effects from the lanreotide.
Discussion Malignant bowel obstruction remains achallenging condition to manage. Clinicalpractice guidelines suggest the use of anti-emetics, analgesics and antisecretory drugs,as well as proton pump inhibitors, as first-line treatment.3
Somatostatin analogues could be used whenother medications are effective, or when otherantisecretory agents, such as hyoscinebutylbromide, only partially control thesymptoms.5 Somatostatin analogues work byinhibiting the secretion of insulin, glucagon,and enteropancreatic peptides such as gastrin,vasoactive intestinal peptide and substance P.This subsequently decreases blood flow at thesplanchnic vein and portal system and reducesgastrointestinal motility and intestinalsecretion.6 Collectively, these mechanismsdecrease the rate of nutrient absorption andreduce the likelihood of vomiting.
In the single clinical trial that has beenpublished for lanreotide in patients withintestinal obstruction with peritonealcarcinomatosis, it was shown to be effective.4
In a case report comparing hyoscinebutylbromide with octreotide to hyoscinebutylbromide alone and octreotide alone in aman with gastric cancer and a high level ofobstruction, it was found that symptoms werenot controlled when either drug wasadministered alone.7
However, somatostatin analogues can beexpensive. An injection of octreotide acetate of 200 μg/ml costs £70. A depot injection oflanreotide 30 mg costs about £320; 60 mgcosts about £550 and 90 mg costs over £730.8
In order to assess whether a patient wouldrespond to a somatostatin analogue, a trial of octreotide should be given via a syringedriver for one week; once proven to be
effective, the drug can beswitched to the longer-actinglanreotide, which can then beadministered every 3–4 weeks.Depending on the octreotidedose required, a single monthlylanreotide injection cantherefore be more cost-
effective, both in terms of nursing-time toattend to the syringe driver daily and for themedication itself.
Lanreotide was a viable alternative tooctreotide for both patients described here. Itwas at least as effective at controlling thesymptoms of intermittent small bowelobstruction and led to a marked improvementin both patients’ quality of life. Althoughexpensive, the use of lanreotide should beconsidered in ambulatory patients withadvanced disease who are not expected to diewithin a few weeks.
Declaration of interestThe authors declare that there is no conflict of interest.
AcknowledgementsWe would like to thank the patients included in the study for their consentto anonymous discussion.
References1. Mercadante S. Assessment and management of mechanical bowelobstruction. In: Portenoy RK, Bruera E (eds). Topics in Palliative Care, vol 1.New York: Oxford University Press, 1997: 113–130.2. Ripamonti C. Malignant bowel obstruction. In: Advanced Cancer Patients.New York: Oxford University Press, 2002: 235–252.3. NHS Scotland. Scottish Palliative Care Guidelines – Bowel Obstruction.Edinburgh: NHS Scotland, 2014.www.palliativecareguidelines.scot.nhs.uk/guidelines/symptom-control/bowel-obstruction.aspx (last accessed 11/03/16)4. Marini P, Blumbery J, Landau Q et al. Symptomatic treatment withlanreotide microparticles in inoperable bowel obstruction due to peritonealcarcinomatosis, a randomized, double-blind, placebo controlled phase 3study. J Clin Oncol 2012; 30: 4337–4343.5. Massacesi C, Galaezzi G. Sustained release octreotide may have a role in thetreatment of malignant bowel obstruction. Palliat Med 2006; 20: 715–716.6. Laval G, Guirimand F et al. Recommendations for bowel obstruction withperitoneal carcinomatosis. J Pain Symptom Manage 2014; 48: 75–91.7. Mercadante, S. Scopolamine butylbromide plus octreotide inunresponsive bowel obstruction. J Pain Symptom Manage 1998; 16: 278–80.8. Twycross R, Wilcock A, Howard P. Palliative Care Formulary, 5th edn.Nottingham: Palliativedrugs.com Ltd, 2014.
Depending on theoctreotide doserequired, a singlemonthly lanreotideinjection can be morecost-effective
Copyright © Hayward Medical Communications 2016. All rights reserved. No unauthorised reproduction or distribution. For reprints or permissions, contact [email protected]

Hayward Medical Communications
’Tis the season of giving and Haywardcan’t wait to get into the festive spirit.
With a new deal or discount every week in therun-up to Christmas and offers on journal advertising,subscriptions, the What is …? series and Hayward’sbooks, there’s something for everyone this season.
Don’t miss out – check out the latest offers atwww.hayward.co.uk/offers2016
Hayward’sChristmas countdown
Insight Experience Flexibility Partnership Integrity |www.hayward.co.uk |t |v|ą |Copyright © Hayward Medical Communications 2016. All rights reserved. No unauthorised reproduction or distribution. For reprints or permissions, contact [email protected]

270 EUROPEAN JOURNAL OF PALLIATIVE CARE, 2016; 23(6)
Sponsored article – Clinical management www.ejpc.eu.com
I t has been suggested that the firstsymptom for which patients with cancerconsult a physician is pain from bone
metastasis.1 In fact, in a recent pan-Europeansurvey of cancer patients, the most commonreason for the initial consultation that led tothe cancer diagnosis was pain.2 Pain isbelieved to be experienced in 56–75% ofpatients with advanced disease.3–5 The impactof pain on quality of life can be devastating;cancer patients with pain report significantlylower levels of performance status and higher levels of total mood disturbance than those who are pain-free, as well assignificantly more anger, fatigue, depression,confusion and lethargy.6
What is pain?Pain, as defined by the InternationalAssociation for the Study of Pain, is ‘anunpleasant sensory and emotional experienceassociated with actual or potential tissuedamage, or described in terms of suchdamage.’ 7 Pain may be either acute or chronic,depending on its onset and duration. Inaddition to acute and chronic categories, paincan be further divided into three types, basedon aetiology and clinical features: nociceptive,neuropathic and mixed.8,9
Nociceptive painNociceptive, or inflammatory, pain is caused bystimulation of nociceptors in the peripheralnervous system and is produced by thermal,chemical or mechanical damage. There are twotypes of nociceptive pain: somatic and visceral.Somatic pain is produced by the activation ofperipheral nociceptors found in skin, bone,joints and muscles. Typically described asaching or throbbing, the pain is generallylocalised and constant and can be precipitatedby movement. Visceral pain is produced by thestimulation of nociceptors within internalorgans. It is often poorly localised and can bereferred to non-visceral areas. Visceral pain canbe described as constant and sharp.
Treating cancer painandrew Dickman explains some of the complexities of the generation and
perception of pain, and considers established and emerging methods of dealing
with complex, chronic cancer pain
&AndrewDickmanMSc DPharm FFRPS
MRPharmS
ConsultantPharmacist,1Project Lead,2HonoraryLecturer 3
1 Blackpool TeachingHospitals NHSFoundation Trust,Blackpool,Lancashire, UK
2 Marie Curie PalliativeCare Institute,University ofLiverpool
3 Graduate School ofPharmaceuticalSciences, OsakaUniversity, Japan
Neuropathic painNeuropathic pain is caused by damage to orchanges in the central or peripheral nervoussystem and can occur spontaneously in theabsence of a stimulus. In essence, it is caused by a dysfunctional plasticity that altersnociceptive pain transmission, leading toenhanced responses to both noxious andinnocuous stimuli. Depending on the nerveaffected, the pain may be shooting, stabbing,lancinating, electric, burning, cold or itching.
Mixed painMixed pain involves both nociceptive andneuropathic pain mechanisms and is thecategory into which cancer pain falls. Tumourgrowth can induce tissue damage and therelease of inflammatory mediators, as well ascausing direct nerve damage throughcompression or infiltration. Cancer patientsmay also experience neuropathic pain due tochemotherapy; co-morbidities such asdiabetes mellitus may also contribute to thedevelopment of neuropathic pain.10
Neuromatrix of painThere have been substantial developments inthe understanding of pain at molecular andcellular levels since Melzack and Wall’spioneering gate theory in 1965.11 It is nowrecognised that pain perception is not a simple
n About a third of cancer patients continue to experience strongpain when treated using the WHO pain ladder.2,14,15
n Cancer pain is mixed, involving both nociceptive and neuropathicpain mechanisms. It is complex, with multifactorial causes, and itsmanagement must consider psychological, social and spiritual needs.
n If used as a framework rather than a strict protocol, the WHO painladder allows for a more individualised model of pain management.
n A multimodal, mechanism-based approach incorporates optionssuch as adjuvant analgesics alongside opioids, methadone as asecond-line opioid and tapentadol, which represents a new classof analgesics with a unique dual action.
IRE/G16 0025 Date of Preparation: October 2016
Keypoints
Copyright © Hayward Medical Communications 2016. All rights reserved. No unauthorised reproduction or distribution. For reprints or permissions, contact [email protected]

271EUROPEAN JOURNAL OF PALLIATIVE CARE, 2016; 23(6)
www.ejpc.eu.com Sponsored article – Clinical management
linear experience resulting from injury,inflammation and other tissue damage. Pain isa subjective experience that can be influencedby many factors, including emotional state,past experiences, attention and distraction,which can serve to either augment or attenuatethe pain experience. Indeed, Dame CicelySaunders introduced the concept of ‘total pain’to describe the interaction between physical,emotional, psychological and social sufferingexperienced by cancer patients.12 Melzack’slater neuromatrix theory proposes that weexperience pain as a result of a complexinterplay of cognition, emotion and sensationmediated through a matrix of several diversebrain regions. The pain experience occurswhen activity from all areas is integrated in thefrontal cortex, rather than directly by a sensoryinput caused by injury orinflammation.13 For example,chronic pain syndromes exist inwhich no obvious tissuedamage is apparent. Patientsexperiencing pain from thesesyndromes can display signs ofpsychological or physical stress,suggesting that genetic influences and theneural–hormonal mechanisms of stress are asimportant as the neural mechanisms ofsensory transmission to the pain experience.
Pain mechanismsPeripheral tissue damage generates pain signalsthat are usually transmitted via small,myelinated Aδ fibres (fast) and unmyelinatedC-fibres (slow) to the dorsal horn of the spinalcord. Various inflammatory mediators, such asbradykinins, prostaglandins and nerve growthfactor, can sensitise the nociceptor, making itmore prone to activate at lower stimulationthresholds. Aδ fibres transmit rapid, sharp painand are responsible for the initial reflexresponse to acute pain. C fibres respond tochemical, mechanical and thermal stimuli,often resulting in burning pain. Aδ and C fibressynapse with secondary afferent neurones inthe dorsal horn. The nociceptive signal ispropagated through relay synapses in thespinal cord, medulla, hindbrain and thalamusand terminates at multiple cortical sites.
Negative reinforcement of chronic painComplex interactions occur in the dorsal hornbetween afferent neurones, interneurones anddescending modulatory pathways. Noxious
stimuli received by dorsal horn neuronesproject to various regions of the brain,including the thalamus, cortex and limbicsystem, via the spinothalamic tract. Sensoryaspects of pain are established by activity incortical areas through relays in the thalamus,whereas emotional aspects of pain are probablyestablished by spinal neurones projecting tolimbic areas of the brain, such as the amygdala.Persistent inputs into the limbic areas are likelyto be the cause of the co-morbidities thatpatients with cancer pain often report, such asanxiety, depression and insomnia. Neuronesfrom higher centres of the brain, such as theamygdala, periaqueductal gray (PAG) regionand the rostral ventromedial medulla (RVM),project to the spinal cord, forming descendingmodulatory pathways. These higher centres of
the brain exert influences onthe perception of pain by eitherinhibiting or facilitating thetransmission of nociceptivesignals within the dorsal horn.In chronic pain states, such ascancer-induced bone pain,increased spinal sensitivity is
believed to be caused by abnormal descendingcontrols; these may in turn be partly driven bychanges in limbic areas of the brainprecipitated by persistent inputs that causecommon co-morbidities, such as anxiety anddepression. Thus, these co-morbidities canimpact on the pain experience, leading to asituation of negative reinforcement.9
The PAG and the RVM are key areas of thebrain involved in endogenous pain controlthrough descending inhibitory modulation.These monoaminergic pathways utilise theneurotransmitters noradrenaline andserotonin (see Figure 1). The descendingnoradrenergic pathway has onlyantinociceptive effects; the serotonergicpathway, in contrast, has been shown to exertboth antinociceptive and nociceptive effects.14
Pain assessmentCancer pain is complex, chronic and often hasmultiple causes. Besides the pain of cancer itself,patients may also experience pain due totreatments such as chemotherapy, radiotherapyor drugs; opioids, for example, often lead topainful constipation. There may also be otherissues, such as underlying anxiety, depression,insomnia, fear or anger. Such factors will have adirect effect on a patient’s pain experience, and
persistent inputs intothe limbic areas arelikely to be the cause ofthe co-morbidities thatpatients with cancerpain often report
Copyright © Hayward Medical Communications 2016. All rights reserved. No unauthorised reproduction or distribution. For reprints or permissions, contact [email protected]

272 EUROPEAN JOURNAL OF PALLIATIVE CARE, 2016; 23(6)
Sponsored article – Clinical management www.ejpc.eu.com
addressing a patient’s concerns or fears, inaddition to administering analgesia, can help toreduce suffering. A multidisciplinary approachto pain management must take into accountpsychological, social and spiritual needs. In fact,drug therapy alone is unlikely to be adequatetreatment for chronic pain of any cause. Thesuccessful pharmacological treatment of cancerpain relies on an accurate pain assessment, withan appreciation of the underlyingpathophysiology. Analgesia should be regularlyreassessed in order to determine:� the efficacy of the treatment� the tolerability of the treatment� any change in response (increasing doses of
opioids do not always indicate tolerance;there could be disease progression ordevelopment of opioid-induced hyperalgesia)
� whether the treatment is ineffective or inappropriate.
Pharmacotherapy of painNon-pharmacological measures undoubtedlyhave an important role in the comprehensivemanagement of cancer pain, but medication-driven pain management arguably forms thecritical aspect of care.
The WHO analgesic ladderAcceptable pain relief in up to 70% of cancerpatients is thought possible using the WHOthree-step analgesic ladder.2,14,15 Of course, thismeans that at least 30% of patients do notachieve acceptable pain relief. The WHOprotocol is nearly 30 years old and has itslimitations, although it is clearly of benefit forthe majority. It is, however, accepted todaythat this approach should be considered aframework rather than a rigid protocol, andthe severity or type of pain should determinethe analgesic to be used. We have gained abetter understanding of pain mechanisms andanalgesic pharmacology in recent years; it hasbeen suggested that a more individualisedmodel of managing cancer pain is needed, onethat adopts a mechanism-based andmultimodal approach.16
Step 1 of the WHO ladder involves usingnon-opioid drugs, such as paracetamol or non-steroidal anti-inflammatory drugs (NSAIDs),with or without an adjuvant analgesic (a drugwith analgesic properties but a primaryindication other than alleviating pain). If painremains uncontrolled, Step 2 is used: a ‘weak’opioid, such as codeine or tramadol, for mild-
n Figure 1. Pain transmissionand modulation.Disruption of the pain-modulatingdescendingpathways is thoughtto be involved in thedevelopment ofchronic pain, such as cancer pain. Suchdisruption may becaused, in part, bypersistent inputs tothe limbic areas thatlead to anxiety anddepression. Thusthese co-morbiditiescan reinforce thepain experience,leading to a vicious circle.
Descending modulatory pathwayPathways from higher centres of braininfluence perception of pain by inhibitingor facilitating transmission of pain signalsfrom dorsal horn to brain
Peripheral nerve This type of nervetransmits pain signalsto dorsal horn
Dorsal horn
Thalamus Relays in thalamusconnect to cortex
Cortex Sensory aspects of painestablished here
AmygdalaEmotional aspects of pain established hereand in other parts of the limbic system
Ascending pain pathwayAscending pathways transmit pain signals to various parts of the brain,including thalamus, cortex and limbic system. Persistent inputs into limbicareas lead to co-morbidities such as depression, anxiety and insomnia
Descending inhibitorypathway
NoradrenalineNoradrenaline released by descending pathway binds topresynaptic membrane, inhibitingneurotransmitter release and thereforeattenuating pain transmission
Post-synapticterminal
Pre-synaptic membrane
Pre-synapticterminal
Periaqueductalgray (PAG) region
Copyright © Hayward Medical Communications 2016. All rights reserved. No unauthorised reproduction or distribution. For reprints or permissions, contact [email protected]

273EUROPEAN JOURNAL OF PALLIATIVE CARE, 2016; 23(6)
www.ejpc.eu.com Sponsored article – Clinical management
to-moderate pain, is added to Step 1 treatment.If pain persists, Step 3 is introduced: a ‘strong’opioid, such as morphine, replaces the weakopioid and is titrated according to pain relief.
Paracetamol has analgesic and antipyreticactivities similar to those of aspirin, but noanti-inflammatory action. NSAIDs are aheterogeneous group of analgesics and themost common class of drugs prescribedworldwide. They are analgesic, antipyretic andanti-inflammatory. Although effective inmild-to-moderate cancer pain, bothparacetamol and NSAIDs have limited value insevere pain due to adverse effects as the doseescalates. NSAIDs are often used in patientswith cancer pain because it is assumed there isan opioid-sparing effect. However, evidence tosupport the use of non-opioids as co-analgesics in cancer pain is weak.17,18
Opioids are the mainstay of cancer painmanagement and the only analgesics withproven benefit when the pain is severe.19 It hasbeen suggested that on Step 2, more potentopioids at lower doses should take the place ofless potent opioids. For patients with mild-to-moderate pain, Step 2 of the WHO analgesicladder still applies. Patients with severe pain,however, should be offered a stronger opioidusing a clear dose titration schedule accordingto pain levels.20 However, dose escalation of anopioid used as a sole analgesic is often limitedby adverse effects, such as sedation orconstipation. This issue can be addressed inseveral ways, including proactive managementof adverse effects and using alternative routesof administration, adjuvant analgesics or adifferent opioid.16,21 Oral morphine iscommonly seen as the first-choice opioid, butthe available evidence suggests no importantdifferences between morphine, oxycodoneand hydromorphone. Any one of these drugscan therefore be used as the first-choice opioidfor moderate-to-severe pain.22
Multimodal approachesGiven the complex molecular mechanismspresent in the pain pathway, it is unsurprisingthat opioids alone often fail to control paincompletely.23 Opioids may be less effective inthe treatment of neuropathic pain, or indeednociceptive pain with an element ofinflammation.24,25 In such circumstances, itmay be necessary to adopt a multimodalapproach to analgesia and use drugs withmultiple mechanisms.
Adjuvant analgesicsOne approach is to use an adjuvant analgesic(see Table 1) alongside the opioid treatmentregimen. Whether the adjuvant should be usedwith the opioid initially, or whether the opioidshould be titrated to its maximum tolerateddose before adding in the adjuvant, is unclear,and the available data are contradictory.26 Thechoice of a specific adjuvant depends on anumber of factors, including type of pain(nociceptive or neuropathic), co-existingmorbidity and current medication; selection isas much an art as a science. In some cases, thetype of pain may suggest a particular adjuvant,while in others, existing co-morbidities orconcurrent medication may determine it.
MethadoneAnother approach is to use methadone, which is recommended as a second-line opioid in cases of refractory or neuropathicpain.22 Methadone is a unique opioid in that itexhibits additional pharmacodynamic effects,such as inhibition of noradrenaline andserotonin reuptake, thereby enhancing theinhibitory effects of the descending pathway.27
Given the wide interpatient variability in thepharmacokinetics of methadone, it should beused only under the guidance of a specialist.28
Table 1. adjuvant analgesics and suggested indications
Suggestedindication adjuvant
Neuropathic pain
AmitriptylineCarbamazepineDexamethasone
DuloxetineGabapentinPregabalinKetamine*
Musculoskeletal pain
DexamethasoneDiazepam
NSAIDsBisphosphonate
(e.g., pamidronate, zoledronic acid)
Smooth muscle spasm e.g., bowel colic
GlycopyrroniumHyoscine butylbromideHyoscine hydrobromide
*To be used only under the guidance of a specialist
Copyright © Hayward Medical Communications 2016. All rights reserved. No unauthorised reproduction or distribution. For reprints or permissions, contact [email protected]

274 EUROPEAN JOURNAL OF PALLIATIVE CARE, 2016; 23(6)
Sponsored article – Clinical management www.ejpc.eu.com
TapentadolA recent development in analgesia is theintroduction of tapentadol. This represents anovel class of centrally acting analgesic: it is aμ-opioid receptor agonist–noradrenalinereuptake inhibitor (MOR-NRI) and thusfacilitates monoaminergic transmission indescending pain inhibitory pathways. Thesepharmacodynamic properties suggest that itcould be a suitable agent for the solemanagement of moderate to severe cancerpain. Several studies have concluded thattapentadol is effective and generally well-tolerated in the management of cancer pain inpatients who were previously receiving strongopioids or were opioid naive.29–36 It has beenshown to provide comparable efficacy tomorphine and oxycodone in the managementof cancer pain, with improved gastrointestinaltolerability.35,36 It is clear that tapentadolrepresents an efficacious alternative to strongopioids, and with increasing clinicalexperience its place in cancer painmanagement will become evident.
Concluding remarksCancer pain is a complex sensory andemotional experience and is always subjective.Co-morbidities, such as anxiety anddepression, can have a direct effect on apatient’s pain experience. The treatment ofcancer pain will invariably be multimodal,incorporating analgesics with complementarymodes of action, as well as non-pharmacological measures that deliveremotional, psychological and spiritual support.Patients should be advised that they may neverbe completely free of pain and they may haveto change their lifestyles to ensure that paindoes not become an overwhelming problem.
The currently accepted practices in cancerpain management are set to changedramatically with a shift towards a mechanism-based, multimodal approach to drug selection.The future promises to revolutionise painmanagement through the development ofhighly specific drugs and, potentially,genetically determined, individualised therapy.The management of cancer pain willundoubtedly become more complicated, butwith the tantalising prospect of optimalanalgesia with minimal adverse effects.
Declaration of interestDr Andrew Dickman has received an honorarium from Grünenthal Pharma for thecontent development of this article. Editorial control remained with the author.
References1. Mercadante S. Malignant bone pain: pathophysiology and treatment. Pain 1997; 69: 1–18.2. Breivik H, Cherny N, Collett B et al. Cancer-related pain: a pan-European surveyof prevalence, treatment, and patient attitudes. Ann Oncol 2009; 20: 1420–1433.3. van den Beuken-van Everdingen MH, de Rijke JM, Kessels AG et al. Highprevalence of pain in patients with cancer in a large population-based studyin the Netherlands. Pain 2007; 132: 312–320.4. Solano JP, Gomes B, Higginson IJ. A comparison of symptom prevalence infar advanced cancer, AIDS, heart disease, chronic obstructive pulmonarydisease and renal disease. J Pain Symptom Manage 2006; 31: 58–69.5. Teunissen SC, Wesker W, Kruitwagen C et al. Symptom prevalence inpatients with incurable cancer: A systematic review. J Pain Symptom Manage2007; 34: 94–104.6. Lin C-C, Lai Y-L, Ward SE. Effect of cancer pain on performance status,mood states, and level of hope among Taiwanese cancer patients. J PainSymptom Manage 2003; 25: 29–37.7. International Association for the Study of Pain. IASP Taxonomy. www.iasp-pain.org/Taxonomy#Pain (last accessed 14/10/16)8. Woolf CJ. What is this thing called pain? J Clin Invest 2010; 120: 3742–3744.9. Falk S, Dickenson AH. Pain and nociception: mechanisms of cancer-induced bone pain. J Clin Oncol 2014; 32: 1647–1654. 10. Fallon MT. Neuropathic pain in cancer. Br J Anaesth 2013; 111: 105–111.11. Melzack R, Wall PD. Pain mechanisms: a new theory. Science 1965; 150:971–979.12. Clark D. ‘Total pain’, disciplinary power and the body in the work of CicelySaunders, 1958–1967. Soc Sci Med 1999; 49: 727–736.13. Melzack R. Pain and the neuromatrix in the brain. J Dent Educ 2001; 65:1378–1382.14. Kwon M, Altin M, Duenas H et al. The role of descending inhibitorypathways on chronic pain modulation and clinical implications. Pain Pract2014; 14: 656–667.15. Valeberg BT, Rustoen T, Bjordal K et al. Self-reported prevalence, etiology,and characteristics of pain in oncology outpatients. Eur J Pain 2008; 12: 582–590.16. Raphael J, Ahmedzai S, Hester J et al. Cancer pain: part 1:Pathophysiology; oncological, pharmacological, and psychologicaltreatments: a perspective from the British Pain Society endorsed by the UKAssociation of Palliative Medicine and the Royal College of GeneralPractitioners. Pain Med 2010; 11: 742–764.17. Nabal M, Librada S, Redondo MJ et al. The role of paracetamol andnonsteroidal anti-inflammatory drugs in addition to WHO Step III opioids inthe control of pain in advanced cancer—a systematic review of theliterature. Palliat Med 2012; 26: 305–312.18. Franceschi F, Iacomini P, Marsiliani D et al. Safety and efficacy of thecombination acetaminophen-codeine in the treatment of pain of differentorigin. Eur Rev Med Pharmacol Sci 2013; 17: 2129–2135.19. Wiffen PJ, Wee B, Moore RA. Oral morphine for cancer pain. CochraneDatabase Syst Rev 2013; 7: CD003868.20. Mercadante S. Management of cancer pain. Intern Emerg Med 2010;5(Suppl 1): S31–S35.21. McNicol E. Opioid side effects and their treatment in patients with chroniccancer and noncancer pain. J Pain Palliat Care Pharmacother 2008; 22: 270–281.22. Caraceni A, Hanks G, Kaasa S et al. Use of opioid analgesics in thetreatment of cancer pain: evidence-based recommendations from the EAPC.Lancet Oncol 2012; 13: e58–68.23. Mercadante S. Managing difficult pain conditions in the cancer patient.Curr Pain Headache Rep 2014; 18: 395.24. Tzschentke TM, Christoph T, Kögel B et al. (-)-(1R,2R)-3-(3-dimethylamino-1-ethyl-2-methyl-propyl)-phenol hydrochloride (tapentadol HCl): a novelmu-opioid receptor agonist/norepinephrine reuptake inhibitor with broad-spectrum analgesic properties. J Pharmacol Exp Ther 2007; 323: 265–276.25. McNicol ED, Midbari A, Eisenberg E. Opioids for neuropathic pain.Cochrane Database Syst Rev 2013; 8: CD006146.26. Raptis E, Vadalouca A, Stavropoulou E et al. Pregabalin vs. opioids for thetreatment of neuropathic cancer pain: a prospective, head-to-head,randomized, open-label study. Pain Pract 2014; 14: 32–42.27. Codd EE, Schank RP, Schupsky JJ et al. Serotonin and norepinephrine uptakeinhibiting activity of centrally acting analgesics: structural determinants androle in antinociception. J Pharmacol Exp Ther 1995; 274: 1263–1270.28. Fredheim OM, Moksnes K, Borchgrevink PC et al. Clinical pharmacology ofmethadone for pain. Acta Anaesthesiol Scand 2008; 52: 879–889.29. Mercadante S, Porzio G, Ferrera P et al. Tapentadol in cancer pain management:a prospective open-label study. Curr Med Res Opin2012; 28: 1775–1779.30. Imanaka K, Tominaga Y, Etropolski M et al. Ready conversion of patientswith well-controlled, moderate to severe, chronic malignant tumour-relatedpain on other opioids to tapentadol extended release. Clin Drug Investig2014; 34: 501–511.31. Mercadante S, Porzio G, Aielli F et al. Opioid switching from and totapentadol extended release in cancer patients: conversion ratio with otheropioids. Curr Med Res Opin 2013; 29: 661–666.32. Mercadante S, Porzio G, Adile C et al. Tapentadol at medium to highdoses in patients previously receiving strong opioids for the management ofcancer pain. Curr Med Res Opin 2014; 30: 2063–2068.33. Schikowski A, Krings D, Schwenke K. Tapentadol prolonged release forsevere chronic cancer-related pain: effectiveness, tolerability, and influenceon quality of life of the patients. J Pain Res 2014; 8: 1–8.34. Schwenke K, Agbalaka A, Litzenburger B. Tapentadol Prolonged Releaseas Used in Clinical Practice in Patients with Severe Chronic Tumor Pain. J Palliat Care Med 2015; 5: 211.35. Kress HG, Koch ED, Kosturski H et al. Tapentadol prolonged release formanaging moderate to severe, chronic malignant tumor-related pain. PainPhysician 2014; 17: 329–343.36. Imanaka K, Tominaga Y, Etropolski M et al. Efficacy and safety of tapentadolextended release in Japanese and Korean patients with moderate to severe,chronic malignant tumor-related pain. Curr Med Res Opin 2013; 29: 1399–1409.
Copyright © Hayward Medical Communications 2016. All rights reserved. No unauthorised reproduction or distribution. For reprints or permissions, contact [email protected]

PALEXIA SR®, PALEXIA® Film-coated Tablets and PALEXIA Oral Solution®
Prescribing InformationRefer to the Summary of Product Characteristics (SmPC) before prescribing.Presentation: Palexia SR: 50 mg (white), 100 mg (pale yellow), 150 mg (pale pink), 200mg (pale orange) and 250 mg (brownish red) prolonged-release tablets contain 50 mg,100 mg, 150 mg, 200 mg and 250 mg of tapentadol (as hydrochloride) respectively.Palexia Film-coated Tablets: 50 mg (white), 75 mg (pale yellow) and 100 mg (pale pink)film-coated tablets contain 50 mg, 75 mg and 100 mg of tapentadol (as hydrochloride)respectively. Palexia Oral Solution: 20 mg/ml oral solution containing 20 mg tapentadol(as hydrochloride) in 1 ml solution. Indication: Palexia SR is indicated for the managementof severe chronic pain in adults, which can be adequately managed only with opioidanalgesics. Palexia Film-coated Tablets and Palexia Oral Solution are indicated for therelief of moderate to severe acute pain in adults, which can be adequately managed onlywith opioid analgesics. Dosage and method of administration: Individualise accordingto severity of pain, the previous treatment experience and the ability to monitor the patient.Can be taken with or without food. Palexia SR and Palexia Film-coated Tablets: Swallowedwhole with sufficient liquid. Palexia SR should not be divided or chewed. Palexia OralSolution: Can be taken undiluted or diluted in water or non-alcoholic drinks. Palexia SRdosage: Initial dose 50 mg twice a day. Switching from other opioids may require higherinitial doses. Titrate in increments of 50 mg twice a day every 3 days for adequate paincontrol. Total daily doses greater than 500 mg not recommended. Palexia Film-coatedTablets and Oral Solution dosage: Initial dose 50 mg every 4 to 6 hours. On the first dayof dosing, an additional dose may be taken 1 hour after the initial dose, if no pain control.The first day’s dose should not exceed 700 mg. Maximum maintenance daily dose of upto 600 mg. Duration of treatment: Palexia Film-coated Tablets and Oral Solution: Thepossibility of switching to Palexia SR should be considered if longer term treatment isrequired, and pain relief is achieved with Palexia Film-coated Tablets or Oral Solution inthe absence of intolerable adverse events. Discontinuation of treatment: Taper dosegradually to prevent withdrawal symptoms. Renal/hepatic impairment: Not recommendedin patients with severe cases. Caution and dose adjustments with moderate hepaticimpairment. Elderly: May need dose adjustments. Children below 18 years: Notrecommended. Contraindications: Hypersensitivity to ingredients, suspected or havingparalytic ileus, acute intoxication with alcohol, hypnotics, centrally acting analgesics orpsychotropics. Not for use when mu-opioid receptor agonists are contraindicated (e.g.significant respiratory depression, acute or severe bronchial asthma or hypercapnia).Special warnings and precautions: At risk patients may require monitoring due tomisuse, abuse, addiction or diversion. At high doses or in mu-opioid receptor agonistsensitive patients, dose-related respiratory depression may occur. Caution and monitoringrequired with impaired respiratory function. Should not use in patients susceptible tointracranial effects of carbon dioxide retention (e.g. increased intracranial pressure,impaired consciousness or coma). Use with caution with head injury, brain tumours,moderate hepatic impairment, biliary tract disease including acute pancreatitis. Notrecommended if history of or at risk of seizures or with severe renal or hepatic impairment.Care should be taken when combining with mixed mu-opioid agonists/antagonists (e.g.pentazocine, nalbuphine) or partial mu-opioid agonists (e.g. buprenorphine). Should notuse with hereditary problems of galactose intolerance, Lapp lactase deficiency or glucose-galactose malabsorption. Interactions: Use with benzodiazepines, barbiturates and opioidanalgesics, antitussive drugs and substitutive treatments may enhance the risk ofrespiratory depression. Central nervous system (CNS) depressants (e.g. benzodiazepines,antipsychotics, H1-antihistamines, opioids, alcohol) can enhance the sedative effect andimpair vigilance. Consider dose reduction with respiratory or CNS depressant agents. Inisolated cases, there have been reports of serotonin syndrome in a temporal connectionwith the therapeutic use of tapentadol in combination with serotoninergic medicinalproducts (e.g. serotonin re-uptake inhibitors). Use with strong inhibitors of uridinediphosphate transferase isoenzymes (involved in glucuronidation) may increase systemicexposure of Palexia/Palexia SR. Caution if concomitant administration of strong enzymeinducing drugs (e.g. rifampicin, phenobarbital, St John’s Wort) starts or stops as this maylead to decreased efficacy or risk for adverse events, respectively. Avoid use in patientswho have taken monoamine oxidase inhibitors (MAOIs) within the last 14 days, due tocardiovascular events. Pregnancy and lactation: Use in pregnancy only if the potentialbenefit justifies the potential risk to the foetus. Not recommended during and immediatelybefore labour and delivery. Do not use during breast feeding. Driving and usingmachines: May have major effect on ability to drive and use machines, especially at thebeginning or change in treatment, in connection with alcohol or tranquilisers. Undesirableeffects: Very common (≥1/10): dizziness, somnolence, headache, nausea. Palexia SRonly: constipation. Palexia Film-coated Tablets and Oral Solution only: vomiting. Common(≥1/100, <1/10): decreased appetite, anxiety, sleep disorder, tremor, flushing, diarrhoea,dyspepsia, pruritus, hyperhidrosis, rash, asthenia, fatigue, feeling of body temperaturechange. Palexia SR only: depressed mood, nervousness, restlessness, disturbance inattention, involuntary muscle contractions, dyspnoea, vomiting, mucosal dryness, oedema.Palexia Film-coated Tablets and Oral Solution only: confusional state, hallucinations, drymouth, muscle spasms, constipation, abnormal dreams. Other important undesirableeffects: palpitations, heart rate increased (uncommon ≥1/1000, <1/100), convulsion(rare ≥1/10,000, <1/1000). Palexia SR only: drug hypersensitivity including angioedema,anaphylaxis and anaphylactic shock (uncommon ≥1/1000, <1/100), heart rate decreased(uncommon ≥1/1000, <1/100), respiratory depression (rare ≥1/10,000, <1/1000).Palexia Film-coated Tablets and Oral Solution only: respiratory depression (uncommon≥1/1000, <1/100), hypersensitivity including angioedema, anaphylaxis and anaphylacticshock (rare ≥1/10,000, <1/1000), heart rate decreased (rare ≥1/10,000, <1/1000). Noevidence of increased risk of suicidal ideation or suicide with Palexia/Palexia SR. Additionalinformation is available on request. Overdose: Seek specialist treatment (see SmPC).Legal classification: POM, CD (Schedule II). Marketing Authorisation numbers andpack sizes: Palexia SR: 50 mg: PA 1189/7/4, 28 and 56 packs; 100 mg: PA 1189/7/5,56 pack; 150 mg: PA 1189/7/6, 56 pack; 200 mg: PA 1189/7/7, 56 pack and 250 mg:PA 1189/7/8, 56 pack. Palexia Film-coated Tablets: 50 mg: PA 1189/7/1, 28 and 56packs; 75 mg: PA 1189/7/2, 28 and 56 packs; 100 mg: PA 1189/7/3, 28 packs. PalexiaOral Solution: 20 mg/mL: PA 1189/7/11, 200 ml bottle. Marketing AuthorisationHolder: Grünenthal Ltd, Regus Lakeside House, 1 Furzeground Way, Stockley Park East,Uxbridge, Middlesex, UB11 1BD, UK. IRE/P14 0003. Date of Preparation: March 2014.
Each year, NICE publishes dozens
of new guidelines – are you left
with unanswered questions about
guideline implementation?
Do you want to understand how
systematic reviews work? Are you
interested in finding out more
about the use of different kinds
of statistics in healthcare?
Our What is ...? titles
could be the answer.
N The What is ...? series aims to demystify
some of the terminology, techniques and
practices used to assess and act upon clinical
and economic evidence in healthcare.
N What is ...? titles include the following:
• Implementing NICE guidance
• What is evidence-based medicine?
• What is quality of life?
… and many more!
Ħ Please visit
webstore.haywardpublishing.co.uk
to browse the full range.
É For institutional access, please contact
[email protected] for a quote.
E V I D E N C E - B A S E D H E A L T H C A R E
theory • knowledge • practiceThe What is ...? series is published by Hayward Medical Communications
10%DISCOUNTFOR EJPCSUBSCRIBERS
Copyright © Hayward Medical Communications 2016. All rights reserved. No unauthorised reproduction or distribution. For reprints or permissions, contact [email protected]

Brian originally presents to his GP witha persistent pyrexia following a visit tothe Middle East. He is investigated for atropical disease, but when it becomesapparent that the symptoms ofdiarrhoea and flushing predate his trip,subsequent investigation shows anelevated urine 5-hydroxyindolaceticacid (5-HIAA), and a CT scan suggests adisseminated carcinoma. A positronemission tomography scan andsomatostatin receptor scintigraphyconfirm multiple liver lesions but donot reveal the existence of a primary.Brian is diagnosed with a well-differentiated metastaticgastroenteropancreaticneuroendocrine tumour (NET).
Brian is subsequently treated with lanreotide to try and managesymptoms associated with NEThormonal hypersecretion. Later thesame year, he is treated with lutetiumtherapy and chemoembolisation, butthis is of little help: although imagingsuggests a reduction in the size of hisliver metastases, Brian continues todeteriorate symptomatically.
Carcinoid heart diseaseJust prior to Brian’s admission to thehospice, an echocardiogram showsthat he has severe right heart failureand that, from a cardiology point ofview, he needs a tricuspid valvereplacement. The prognosis related to
his primary cancer remains unclear, buthis right heart failure is at a very latestage in the disease trajectory.
Brian is admitted to the hospice with low mood, fatigue, severeperipheral oedema, diarrhoea,breathlessness on exertion and a hard,scaly, erythematous, pruritic rashextending over both legs and hands.His abbreviated mental test score(AMTS) is 6/10. He is also strugglingwith the uncertainty of his prognosis. In the hospice, he becomes frustratedduring discussions with healthcareprofessionals because he often feelsthat people are talking too quickly forhim to be able to keep up. However,Brian has good insight into hiscognition and is able to followconversations and make decisions with the support of his wife.
Following discussions with both thecardiologists and the oncologists, Brianis advised that he could be transferredto hospital to receive acute treatmentfor his heart failure or he could receivesimilar treatment at the hospicecombined with the best supportivecare. Long discussions take place withBrian and his wife, both together andon their own. Emphasis is placed onthe fact that there is a risk that if Brian
deteriorates secondary to treatment,the hospice would not necessarily havethe backup to address the medicalproblems. The main challenge is toensure that Brian makes an informeddecision. Discussions over several dayswith the support of his wife mean thatwe feel confident that Brianunderstands the various options andcan retain the information, weigh upthe risks and benefits andcommunicate his wishes to us. Hechooses to stay in the palliative caresetting, where he has high-dosefurosemide and daily monitoring of hisrenal function, weight and fluidbalance. His peripheral oedema doesimprove, as do his exercise toleranceand mobility, although his overallcondition continues to deteriorate.
PellagraBrian’s skin condition is his mainconcern. The itching prevents himsleeping and he feels that thehardening of his skin affects hismobility. He has previously beentreated with potent topical steroids fordermatitis, but to little avail. Reflectingon his disease and the history of therash starting as an erythematous,blistering rash and subsequentlybecoming thickened, rough and darklypigmented, we feel that this most likelyrepresents pellagra. He is started on ahigh-dose vitamin B complex three
* All names have been changed to protect patient confidentiality
EUROPEAN JOURNAL OF PALLIATIVE CARE, 2016; 23(6)276
The case studymasterclass www.ejpc.eu.com
Case 89. Managing symptoms ofneuroendocrine tumours in a 62-year-oldman with impaired cognitionn Brian* is a 62-year-old man who lives in a small terraced house with his wife. Following a head injury 20 years
ago, his memory deteriorated and his speech became impaired, but he manages to continue with the activities
of daily living with full independence. Brian does need assistance from his wife in understanding any complex
discussions and to help him with decision-making.
Each case study masterclass comprises a detailed case history followed by a series of questions designed to test your knowledgeand give you food for thought. The suggested answers can be found on page 308 of this issue.
Andrew Gill BSc MBChB MRCGP DipPallMed Specialty Doctor inPalliative Medicine, Sue Ryder Care, Manorlands Hospice,Oxenhope, West Yorkshire, UK
Copyright © Hayward Medical Communications 2016. All rights reserved. No unauthorised reproduction or distribution. For reprints or permissions, contact [email protected]

277EUROPEAN JOURNAL OF PALLIATIVE CARE, 2016; 23(6)
times a day, along with cetirizine 20 mgdaily and ranitidine 150 mg twice dailyfor the itch, and regular emollients anda potent topical steroid. There wassome objective improvement in therash and a marked reduction in pruritis,although the skin remains thickened.This improvement is sustained.
Cognition and moodThroughout his stay in the hospiceBrian’s mood, cognitive ability andcapacity fluctuate. His AMTS varies, asdoes his fatiguability, which influenceshis ability to engage in communication.The team find discussions with Brian onhis own challenging, and it is clear thatBrian finds it difficult to followconversations, which subsequentlyputs significant pressure on his wife.Brian’s frustration is apparent, as is theeffect it has on his already fragilemood. He expresses feelings ofworthlessness and often thinks hissituation is hopeless. An anti-depressant is considered, but afterdiscussion regarding the risk ofpotentiating some carcinoidsymptoms, Brian decides to continuewithout any pharmacologicalmanagement for his depression.
Despite the communicationdifficulties, the team feels that Briancan make capacitous decisions throughappropriately timed supporteddiscussions. Although these causesignificant stress for Brian, he is givensupport by the hospice psychologist,who also offers therapeutic support toBrian’s wife. She is put in touch with acarer support group, offeredcomplementary therapy and advisedto see her own GP should she feel herown mood deteriorating. Thefacilitated discussions allow Brian toexpress his preferences for care andparticularly that his preferred place ofdeath is his own home. Furtherdiscussions around advanced careplanning are attempted with Brian, buthe is resistant to these because of thelevel of fatigue that follows.Nonetheless, both the team and hisfamily feel that should Brian lose the
capacity to make decisions, they have agood understanding of his wishes andare now better placed to makedecisions in Brian’s best interest shouldthe need arise.
The outcomeOverall, Brian feels better than onadmission to the hospice. His skin feelsbetter, he is less breathless and hisbowel movements have improved.However, he is generally very frail andmobile over only short distances. Hisliver function has deteriorated and hisalbumin has dropped, despite a gooddiet and the improvement of hissymptoms. Brian reflects on the
uncertainty of his prognosis andtreatments. Rather than being able toprovide answers to reduce hisuncertainty, the medical teamacknowledge it and explain that theyshare it. The limitations of medicaltreatment are discussed and Briancomes to the conclusion that theremay be a point where he is ‘as well ashe is going to be’.
Brian’s discharge home is carefullyplanned with support from districtnurses, hospice at home and privatecarers, along with close specialistpalliative care follow-up. The events ofhis admission and the expectations forthe future are shared with Brian’s GP viaa telephone discussion and dischargeletter. The hospice psychologistcontinues to support both Brian andhis wife after discharge.
Brian manages at home for longerthan we expect. He continues to enjoytime with his family, although he doesnot manage to make it out to hisbeloved narrowboat again. He diescomfortably at his preferred place ofdeath five months after leaving thehospice. His wife will continue to besupported by the team n
Declaration of interestThe author declares that there is no conflict of interest.
www.ejpc.eu.com The case studymasterclass
1 How do NETs present?
2 What is the cause of pellagra,and what are the treatmentoptions?
3 What is the pathophysiology ofcarcinoid heart disease?
4 What is the Mental Capacity Act,and what help can be providedto aid decision-making?
Questions
nBefore he was admitted tothe hospice, Brian spent muchof his time sailing hisnarrowboat on canal tripswith his family.DAvID MUSCROFT/SHUTTERSTOCK.COM
Copyright © Hayward Medical Communications 2016. All rights reserved. No unauthorised reproduction or distribution. For reprints or permissions, contact [email protected]

278 EUROPEAN JOURNAL OF PALLIATIVE CARE, 2016; 23(6)
Multidisciplinar y team www.ejpc.eu.com
T he closeness between nurses andchildren is a major characteristic ofpaediatric palliative care, and nurses
dedicate themselves to its pursuit so that theycan bring to life the very essence of theirprofession. Closeness encompasses the fourdimensions of palliative care: physical,mental, social and spiritual. At the same time,nurses are aware, through their education andpractice, of the need for professional distancein certain situations. So how do nurses inpaediatric palliative care cope with thetension between these two aspects of theirwork, both of which are fundamental to it?
To investigate possible answers to thisquestion, we surveyed the available literatureusing an integrative review design,1 whichincorporates different types of publishedmaterial, including both qualitative andquantitative articles and grey literature such asresearch reports and discussion papers,
without the need for a formal qualityassessment.2 The literature was systematicallysearched with predefined inclusion andexclusion criteria in the databases PubMedand PsycINDEX. A total of 110 suitable articleswere identified for an initial investigation,which produced 12 publications that weredeemed suitable for a more detailed, in-depthanalysis. The relevant themes that weredistilled from the literature are summarised below.
Understanding nursing’s central rolePaediatric palliative care involves expertisefrom several professional disciplines, andparticular significance is attached to nursing.Nurses become immediately and intimatelyinvolved with those whom they care forthrough physical touch, spatial closeness andthe time spent with affected children – theirrole is central. In trying to understand thenurse’s role, certain key questions arise. Whatkind of response is evoked in nurses by thedying and death of children? And how donurses cope while carrying out this work,which is never routine? These questions arenot addressed in established definitions ofpaediatric palliative care, making it all themore important to understand how nursesperceive their own role in this discipline.3
Paediatric palliative care has become a partof vocational training and further education,but caring for dying children requiresextensive, in-depth practical experience onthe part of nurses. Lack of preparation anddirect experience can lead to uncertaintyabout the correct approach to the end of life,and these factors may have an increasinglyburdensome effect on nurses’ professional
Paediatric palliative nursing: the tension between closenessand professional distanceCaring for children who are dying puts special demands on the medical staff who care for them,
and no one knows this better than palliative care nurses. regula Buder and andré Fringer look at
the difficulties of the job and consider how nurses deal with them
n Nurses who gain enough experience to understand their ownvulnerabilities and resources, and who address the tensionbetween them from a professional perspective, can increase therange of their abilities and set clear boundaries betweenthemselves and the child.
n Inexperienced nurses may find it difficult to maintain aprofessional relationship and draw boundaries.
n It is essential for nurses to be able to acknowledge andcommunicate the end-of-life scenario. Relationships with dyingchildren and their families are a key factor in nursing quality.
n Nurses need a way to express their emotional distress and thusovercome their potential isolation; they can do this by recountingtheir traumatic experiences to others, which reassures them thatthe child is not forgotten.
Keypoints
&Regula BuderMAS FHO Palliative Care
Nurse1
André FringerMScN (RN) Professorof NursingScience, ProjectManager andHead of Course,(Master ofAdvanced Studiesin Palliative Care)2
1 KinderspitexNordwestschweiz,Nenzlingen,Switzerland
2 FHS St.Gallen,University ofApplied Sciences,Switzerland
Copyright © Hayward Medical Communications 2016. All rights reserved. No unauthorised reproduction or distribution. For reprints or permissions, contact [email protected]

279EUROPEAN JOURNAL OF PALLIATIVE CARE, 2016; 23(6)
www.ejpc.eu.com Multidisciplinar y team
practice.4 Experienced nurses can recogniseand articulate the requirements of theirprofessional role with clarity. With increasingproficiency, they can learn to distancethemselves from burdensome emotions andsituations and set a clear boundary betweenthemselves and the child. Less experiencednurses, however, may find it difficult tomaintain a professional relationship and draw boundaries.5
Recognising vulnerabilityProfessional nursing requires consistentpatient-centricity and ethical responsibility, asPatricia Benner explains.6 She states thatpatients’ inner experiences are always the startof a journey for the nurse. Thus nursinginvolves much more than simply technicaland standardised activities based on medicalor scientific knowledge. Benner emphasisesthat nurses are constantly improving theirunderstanding of people’s physical andmental vulnerabilities, which they protect byacting ethically and addressing patients’individual needs.6 This requires nurses in turnto actively confront their own vulnerabilitiesand resilience. Paediatric palliative care nurseswho successfully recognise the tensionbetween their vulnerabilities and resources,and who address this tension from aprofessional perspective, can increase therange of their abilities, making themselvesmore open to vital encounters with dying children.
Acknowledging the end of life Why is it still not standard to offer paediatricpalliative care at the appropriate time tochildren who would benefitfrom it? A research group led bySharon Docherty investigatedthis issue, and it became clearthat healthcare professionalswere often unwilling to give upthe hope that their patientsmight recover, and that advances in treatinglife-limiting diseases will continue in generalto extend life and, sometimes, offer thepossibility of curative therapy. Such advancesdo bring risks of increased suffering ifsustaining life remains the primary focus andthe understanding of palliative care isrestricted to care very close to the end of life.7
Another obstacle to implementingpaediatric palliative care at the most
appropriate time is uncertainty in theprognosis and course of disease in children.Starting palliative care earlier whilecontinuing curative therapy when there isuncertainty about the prognosis can increasehelpful communication and improve thequality of life of affected children.8
For these reasons it is essential for nurses tobe able to acknowledge and unambiguouslycommunicate to the professional caregiversand the family that the child could or will die.If they do not, occupational stresses are notdefined and emotional labour cannot beadequately explained. This is the prerequisitefor implementing paediatric palliative care asa holistic encounter and providing needs-based care. However, professionals should beaware that the concept of hope remains partof palliative care until the end, particularly inchildren. The hope is not necessarily that thechild might recover; it could be the parents’hope that the end of life will make some sense
of the situation, or thechild’s hope that thebirthday money they aresaving will one day pay forthe trip around the worldthey have been dreaming of.Such hope can make it easier
to deal with the reality of the situation, and itacts like a bridge for a nurse’s communicationwith the family.
Establishing relationshipsThe term ‘palliative care’ implies arelationship between the person receiving care and the person giving it. Nurses mustconsciously shape this relationship, and theirhonesty and authenticity are prerequisites for
Experienced nurses canrecognise and articulatethe requirements oftheir professional rolewith clarity
n Relationships with dyingchildren and the maintenanceof hope are key factors in theprovision of end-of-life care.
THAN
ONGS
UK H
ARAK
UNNO
/SHU
TTER
STOC
K.CO
M
Copyright © Hayward Medical Communications 2016. All rights reserved. No unauthorised reproduction or distribution. For reprints or permissions, contact [email protected]

280 EUROPEAN JOURNAL OF PALLIATIVE CARE, 2016; 23(6)
Multidisciplinar y team www.ejpc.eu.com
a trusting relationship. In an atmosphere oftrust, the patient feels more able to feel secureand confident in asking the questions andaddressing the issues that are important tothem.9 Since the late 1990s, the Greekpsychologist Danai Papadatou has advocatedrethinking the way we build relationships. She assumes that in paediatric palliative care, a clear distinction between the professionalperson and the dying child and their family is impossible, and she therefore recommends a relationship-based approach.10 An encounter with a dying child is a formativeexperience for nurses; it helps them to mature and develop an in-depthunderstanding of humanity and suffering.11
Thus, relationships with dying children and their families are a key factor in nursing quality.
Balancing closeness and distance:the nurse as human beingConducting care in a deliberate fashion allows nurses to be more aware of theiremotions, which helps to reduce the impact in their private lives of the emotional issues produced by their professional role.12
However, setting professional boundaries is not easy, particularly in thecontext of paediatric palliativecare. Indeed, some nursesassociate the term ‘professionaldistance’ with a lack of caring –although they will havelearned the theoreticalimportance of setting
professional boundaries during theireducation, in their daily practice they findthat the theory often cannot be applied.
Caring for dying children and supportingtheir families involves an extremely intimateencounter with pain, grief and loss that evokesdeep empathy in the nurse. Nurses continueto be concerned about the balance betweencloseness and distance even after a child hasdied; once the patient’s nursing care iscomplete, it is important to shape the ongoingrelationship with the family. Following achild’s sudden death or a long period ofcaring, nurses will benefit from debriefing andprofessional support to help them deal withthe process of mourning; palliative care nursesshow a high demand for such support.13
Despite the fact that palliative care has beenestablished as a specialist discipline in some
countries, nurses in paediatric palliative caremay find themselves deeply isolated.14
Nurses need a way to express theiremotional distress and thus overcome theirisolation, but they also want to avoidconfronting others with their experiences, astalking about children dying is considered adifficult subject.15 By talking with people whoare similarly affected and narrating their ownexperiences to them, nurses can impartmeaning to the death of a child, which can bean important part of coping with grief.16
Judy Rashotte encourages paediatricpalliative care nurses to dwell on the storiesthat haunt them, encouraging them tonarrate and re-narrate these experiences toeach other. This allows the nurses not only tofeel emotional relief but also to make theirpersonal experience accessible to others,which helps by reassuring them that the childis not forgotten.17
The Latin root of the word ‘palliative’ ispalliare, which means to cloak or shield. It isimportant to remember that from time totime, even nurses require a protective shell.However, this shell must be permeable, so thatwe remain open to dying and death – andthereby open to life.
Declaration of interestThe authors declare that there is no conflict of interest
References1. Whittemore R, Knafl K. The integrative review: updated methodology. J Adv Nurs 2005; 52: 546–553.2. Grant JM, Booth A. A typology of reviews: an analysis of 14 review typesand associated methodologies. Health Info Libr J 2009; 26: 91–108.3. Clarke J, Quin S. Professional carers' experiences of providing a pediatricpalliative care service in Ireland. Qual Health Res 2007; 17: 1219–31. 4. Pearson HN. “You’ve only got one chance to get it right”: children’s cancernurses’ experiences of providing palliative care in the acute hospital setting.Issues Compr Pediatr Nurs 2013; 36: 188–211.5. Cook KA, Mott S, Lawrence P, Jablonski J, Grady MR, Norton D et al. Copingwhile caring for the dying child: nurses’ experiences in an acute care setting.J Pediatr Nurs 2012; 27(4): e11–21. 6. Benner P. Stufen zur Pflegekompetenz. From Novice to Expert. Bern: Huber, 2012.7. Docherty SL, Miles MS, Brandon D. Searching for “the dying point:”providers’ experiences with palliative care in pediatric acute care. Pediatr Nurs2007; 33: 335–41.8. Davies B, Sehring SA, Partridge JC, Cooper BA, Hughes A, Philp JC et al.Barriers to palliative care for children: perceptions of pediatric health careproviders. Pediatrics 2008; 121: 282–8. 9. Erichsen E, Danielsson EH, Friedrichsen M. A phenomenological study ofnurses’ understanding of honesty in palliative care. Nurs Ethics 2010; 17: 39–50.10. Papadatou D (ed.). In the face of death: Professionals who care for the dyingand the bereaved. New York: Springer Publishing; 2009.11. Berterö C. District nurses' perceptions of palliative care in the home. Am J Hosp Palliat Care 2002; 19: 387–91.12. Keene EA, Hutton N, Hall B, Rushton C. Bereavement Debriefing Sessions:An Intervention to Support Health Care Professionals in Managing TheirGrief After the Death of a Patient. Pediatr Nurs 2010; 36: 185–90.13. Conte TM. Pediatric oncology nurse and grief education: a telephonesurvey. J Pediatr Oncol Nurs 2011; 28: 93–9. 14. MacConnell G, Aston M, Randel P, Zwaagstra N. Nurses' experiencesproviding bereavement follow-up: an exploratory study using feministpoststructuralism. J Clin Nurs 2013; 22: 1094–102.15. McCloskey S, Taggart L. How much compassion have I left?: Anexploration of occupational stress among children’s palliative care nurses. Int J Palliat Nurs 2010; 16: 233–41.16. Macpherson CF. Peer-supported storytelling for grieving pediatriconcology nurses. J Pediatr Oncol Nurs 2008; 25: 148–63.17. Rashotte J. Dwelling with stories that haunt us: building a meaningfulnursing practice. Nurs Inq 2005; 12: 34–42.
Once the patient’snursing care iscomplete, it isimportant to shape theongoing relationshipwith the family
Copyright © Hayward Medical Communications 2016. All rights reserved. No unauthorised reproduction or distribution. For reprints or permissions, contact [email protected]

This sensible yet sensitive guide to all thingsend of life is thoughtfully written with a holisticapproach. The reader finds instant empathywith the case studies of Maria, Albert andJenny as the book takes us on their personalend-of-life journeys, with clear explanations ofsymptoms and issues along the way.
The narrative addresses the feelings and fearsof all those involved, offering guidance on howto deal with the physical issues of dying anddeath, and providing answers to all the commonquestions encountered in palliative care settings.Panels in each chapter encourage the reader toreflect and research. The denial, fear andinexperience often seen at the end of life can begently alleviated with some basic knowledgeand wise counsel, and this book provides both.
How often I have wished for a simple guidelike this to support communication with agrieving family who can barely hear and absorbwords through their sorrow. I would love themto have access to this book, not instead of thehuman touch, but so that they could turn to it in quieter moments.
So much of the content resonated with me. I recognised the difficulties experienced by manyfamilies during my years on the ward, along withtheir questions and fears and the differingattitudes and cultural beliefs that influence howwe approach the end of life. I particularly smiledat the scenario chosen to illustrate the conflict ofopinion regarding the involvement of children: adeceased relative with the family spread aroundthe room, while children play on the floor. Thebook describes two caregivers; the first believesthis scene to be beautiful and fitting, the secondfeels it is wholly inappropriate to have children inthe same room as a deceased relative. Of course,there is no right or wrong answer, each view issupported and the reader is inspired to exploretheir own thoughts and feelings.
I would have appreciated the opportunity to study such an honest and comprehensiveguide when I began working in palliative care. I believe that in addition to helping familiesunderstand the situation in which they findthemselves, this guide could be an effectiveresource in the training of future caregivers �
I would haveappreciated theopportunity tostudy such anhonest andcomprehensiveguide when Ibegan workingin palliative care
A Practical Guide to End of Life CareSadler C (ed); London: Open University Press, 2015; 216 pages; PB (RRP: £20.99; ISBN: 9780335263561), eBook (RRP: £20.99; ISBN: 9780335263578)
Book review
� Carmel Grealish,Senior HealthcareAssistant, St Joseph’sHospice, London, UK
Hayward publishesmedical journalsWith a suite of titles covering much of
modern medicine, Hayward’s journals
are at the forefront of developments in
healthcare. Containing a broad blend
of review articles, policy updates and
practical information alongside regular
columns, editorials and patient
information, Hayward’s journals
are the perfect vehicle to promote
your products and services to
a specialist audience.
g
For more information please contactHarriet Abbs, Advertising and SubscriptionsCoordinator [email protected]
IMAGE: ELLICA/SHUTTERSTOCK.COMCopyright © Hayward Medical Communications 2016. All rights reserved. No unauthorised reproduction or distribution. For reprints or permissions, contact [email protected]

282 EUROPEAN JOURNAL OF PALLIATIVE CARE, 2016; 23(6)
Perspective www.ejpc.eu.com
On the evening of 20th January 1936,King George V of Great Britain andIreland, Emperor of India, was perhaps
assisted in his dying by his physician, LordDawson of Penn. This remained a well-keptsecret until the doctor’s private diary wasopened 50 years after the king’s death. Dr Dawson was to describe his management ofthe king’s final illness as ‘a facet of euthanasiaor so called mercy killing’.1 The predominantincentive for the actions of the attendingdoctor appear to have included chronologicalconvenience. This is a neglected influence inthe literature about physician-hastened death.
The patientGeorge V ascended the throne in 1910. He wasdevoted to his country and empire and was ahard-working monarch. He was a heavysmoker, and in 1928 he suffered pleurisycomplicated by a lung abscess. His physician,Dr Dawson, located and drained this abscess,undoubtedly saving the king’s life and makingDawson a national celebrity.1 A long, 13-weekrecuperation followed. A London Hospitalnurse, Sister Catherine Black, was chosen toattend him full-time, and she did so until hisdeath. She reported his recurrent daytimesleepiness and nocturnal restlessness, notingthat he preferred a prone position. Sometimesshe would administer oxygen to him in theearly hours of the morning.
Despite his failing health, further years ofadoration and personal popularity touchedand amazed the king,2 and his dedication toroyal duties did not diminish until late 1935.In November of that year the 71-year-old kingwas noted by Dawson to have an ‘obviousdiminishment of energy and interest’. In earlyJanuary 1936, Sister Black informed Dawsonthat the king was experiencing phases ofsleepiness and breathlessness; indeed shedescribed the king as feeling ‘cheap’.3
The convenient death of KingGeorge V: a look back at historyWhen the role of King George V’s doctor in assisting his death in 1936 came to light 50 years later,
general opprobrium was heaped upon the doctor. Sandy Macleod and Jane Vella-Brincat use the
case to highlight the potential role of chronological convenience in end-of-life decision-making
&Sandy MacleodFRANZCP FRACP
AssociateProfessor1 andPsychiatrist andPalliative MedicineSpecialist2
Jane Vella-BrincatBScPharm (Hons)
Pharmacist3
1 University ofCanterbury,Christchurch, New Zealand
2 Burwood Hospital,Christchurch, New Zealand
3 ChristchurchHospital,Christchurch, New Zealand
The king was reported in late January to betired and often unable to concentrate, buthaving some ‘lucid moments’.
Dr Dawson was more than the king’sphysician. He was a Privy Councillor, withlong experience in this role.3 There should be no interval in which the throne is notoccupied, but there was no indication that the king himself had participated in any form of advance directive regarding hisimminent demise. The formation of a Council of State was required in order torecognise his successor, but obtaining theking’s written assent was practically difficultbecause of his poor health. At a hastilyconvened Council meeting the king was ableto verbally approve the proceedings. Heapologised for his inability to concentrate.With apparently great adroitness, Dawson putthe pen in his hand and guided it, saying,‘Make a mark, Sir, and you may signafterwards.’ Two marks, XX, were made.3 Afterthe meeting the king went to bed andremained asleep during an examination byDawson, who prognosticated that he wouldbe unlikely to live through the night. The kingwas ‘sinking’; Dawson took up a menu-cardand, writing on his knee, composed the
n King George V’s death was in all probability hastened by his physician, Dr Dawson.
n In the lead-up to his death, the king was delirious, a situation that precipitated unique constitutional issues.
n His attending nurse, Sister Catherine Black, refused to administerthe fatal injection planned by Dr Dawson.
n Palliative sedation was apparently not Dr Dawson’s intent.
n Chronological convenience and/or inconvenience may impact on end-of-life decision-making in those jurisdictions in whichmedically assisted dying is permissible.
Keypoints
Copyright © Hayward Medical Communications 2016. All rights reserved. No unauthorised reproduction or distribution. For reprints or permissions, contact [email protected]

283EUROPEAN JOURNAL OF PALLIATIVE CARE, 2016; 23(6)
www.ejpc.eu.com Perspective
famous press and radio release: ‘The King’s lifeis moving peacefully towards its close.’
That evening the king was reported as being‘cyanotic, recumbent flat in bed, slowlyprogressive myocardial failure, no obviouslung congestion but cerebral thrombosis andalmost venous stasis’.3 The family, includingthe heir, told Dawson that they had no wishfor the king’s life to be prolonged if the illnesswas judged to be mortal. Dawson was incomplete agreement and promised to directthe treatment accordingly.2 Morphine wasadministered by injection mid-evening by his nurse as there was ‘a little evidence ofstruggle’, after which he roused and wasreputed to utter to his nurse, ‘God damn you,’or maybe ‘Bugger Bognor!’ The king thenlapsed into a stupor and coma.
Dawson wrote, ‘At about 11 pm it was evidentthat the last stage might endure for manyhours. Hours of waiting just for the mechanicalend when all that is really life has departed onlyexhausts onlookers and keeps them so strainedthat they cannot avail themselves of the solaceof thought, communion or prayer. I thereforedecided to determine the end.’2 Dr Dawsoninjected 50 mg of morphine and 65 mg ofcocaine into the comatose king’s distendedjugular vein. Sister Black was disturbed by thesemedical events, Dawson noted, and hadrefused to give the injection herself.1 Within15 minutes the king’s breathing quietened, hebecame placid and the physical struggle ceased.Cheyne-Stokes breathing commenced, and at11.55 pm he died. As revealed by Dawson’sdiary, one of his reasons for his medical actionsthat evening was ‘to ensure the announcementshould appear in the morning edition of TheTimes and not some lesser publication later inthe day’.1 Dawson was able to return promptlyto his busy private practice in London thefollowing morning.1
The doctorBertrand Edward, Viscount Dawson of Penn,(1864–1945), was the physician and trustedfriend to four kings.4 A physician at theLondon Hospital, he was the most admiredand respected doctor of his generation. He wasan influential medical politician and an earlyarchitect of the NHS. He had the reputation of ‘a very good, caring doctor’, who possessed‘superb humanity’ and ‘kindly wisdom’.4
Dawson was subsequently to support thedefeat of the 1936 Voluntary Euthanasia
(Legalisation) Bill, arguing that it was a matterbest left to the conscience of the individualdoctor rather than official regulators.5
Dawson’s actions, when revealed, did notreceive praise. Sir Douglas Black, a pastpresident of the Royal College of Physicians,said Lord Dawson appeared to have committedan ‘evil’ act for the sake of a ‘marginal good’.6
DiscussionThe description of the sick king over his lastdays emphasises the acute distress that hiscondition was causing both to himself andthose around him.3 In his terminal phase theking was dysgraphic (experiencing difficultyin writing), indeed agraphic (unable to write),and experiencing a delirium. A notuncommon sign of delirium, dysgraphiawould have significantly compromised theking’s regal duties.7 An incompetent kingraised major constitutional difficulties.Reducing the cognitive and environmentalload on the king’s brain was clearly instituted,but pharmacological interventions fordelirium were then not available. The medicalirreversibility of the king’s health was
nA portrait of KingGeorge v and QueenMary, c.1914.CIRCA IMAGES/GLASSHOUSE IMAGES/SUPERSTOCK
Copyright © Hayward Medical Communications 2016. All rights reserved. No unauthorised reproduction or distribution. For reprints or permissions, contact [email protected]

284 EUROPEAN JOURNAL OF PALLIATIVE CARE, 2016; 23(6)
Perspective www.ejpc.eu.com
undeniable. Dyspnoea is uncomfortable anddistressing and is a potential indication forpalliative sedation in modern practice.Intractable delirium may be a firmerindication for such sedation.
Thus a reasonable question is whether ornot Dawson practised palliative sedation. We can say that the choice of ‘sedating agents’would seem to have been pharmacologicallyunusual. Dawson’s morphine dose selectionwas likely to have been significant in a frailpatient with respiratory failure (though thereis no record of the dose provided for relief ofthe dyspnoea earlier in the evening). Thiswould suggest that his intent was not merelyto sedate. The use in combination withcocaine was intriguing. Similarpharmaceutical agents, such as
methylphenidate, may be used to addressfatigue and depression in the dying, but theytend not to be effective in the imminentlyterminal phase.7 Perhaps Dawson wasattempting to induce a fatal arrhythmia?
There is the possibility that the king died anatural, and not a hastened, death.Undoubtedly his death was imminent andmisattribution of the cause of death in suchsituations – attributing the cause to the lastmedication administered – is not uncommon.Dawson obviously had discussed his proposedcourse of action with family. The principle ofdouble effect – acting with the intention ofbringing about a good effect (for example,relieving pain) with the unintendedconsequence of a bad effect (death) – is notsuggested by the available evidence.
The timing of the death was a criticalconsideration for Dawson. The patient wasunique and the circumstances extraordinary.Lord Dawson seemingly acted to protect theconstitution of the kingdom and to relieve theappalling distress of his terminally ill patient.His medical intention appears to have beeneuthanasia. His timing was clearly convenientto himself, the press and presumably thenation. Chronological convenience may be a relevant influence in the consideration ofeuthanasia, but it has rarely been consideredor acknowledged in the literature aboutmedically hastening dying. It has beenestimated that doctor-assisted dying inEuropean countries shortens life by less than amonth in most cases.8 In addition, it has beenshown that palliative sedation does not hastendeath – it actually prolongs dying by perhaps afew days.9 These findings would suggest thatchronological convenience and/orinconvenience might impact upon end-of-lifedecisions in those modern jurisdictions inwhich medically assisted dying is allowed.
Declaration of interestThe authors declare that there is no conflict of interest.
References1. Ramsey JHR. A king, a doctor, and a convenient death. BMJ 1994; 308: 1445.2. Watson F. The Death of George V. History Today 1986; 3: 21–30.3. Watson F. Dawson of Penn: A Biography. London: Chatto and Windus, 1950: 275–279.4. Munks Roll (Royal College of Physicians), Vol. IV (1826–1925): 446.5. Watson F. Dawson of Penn: A Biography. London: Chatto and Windus, 1950: 238–239.6. Lelyveld J. The New York Times, November 28, 1986.7. Macleod AD, Whitehead LE. Dysgraphia and terminal delirium. Palliat Med1997; 11: 127–32.8. van der Heide A, Deliens L, Faisst K et al. End-of-life decision-making in sixEuropean countries: descriptive study. Lancet 2003; 362: 345–50.9. Maltoni M, Pittureri C, Scarpi E et al. Palliative sedation therapy does nothasten death: results from a prospective multicenter study. Ann Oncol 2009;20: 1163–1169.
Are you interested in reviewing new books for the European Journal
of Palliative Care?
Have you read a recently published book that you think our readers would be
interested in hearing about?
We are looking for book reviewers from any profession or country. Anyone
with an interest in palliative care can potentially contribute. Both the books reviewed and the reviews themselves have to be in English.
If this sounds interesting, please get in touch with us
via email at [email protected]
Call for book reviewers
Copyright © Hayward Medical Communications 2016. All rights reserved. No unauthorised reproduction or distribution. For reprints or permissions, contact [email protected]

285EUROPEAN JOURNAL OF PALLIATIVE CARE, 2016; 23(6)
www.ejpc.eu.com Perspective
T he Sydney Institute of PalliativeMedicine (SIPM) originated at the RoyalPrince Alfred Hospital (RPAH), Sydney,
in the mid-1980s, since when it has played asignificant role in shaping the development ofpalliative medicine as a clinical science and as aspeciality in New South Wales (NSW), Australiaand internationally. Before the RoyalAustralasian College of Physicians becameinvolved in training doctors in palliative careand the Australasian Chapter of PalliativeMedicine came into being, the instituteprovided a focus for palliative medicinetraining for doctors. In time it produced leadersin this field who were instrumental in thedevelopment of many palliative care services,not only in NSW but also nationally andinternationally. SIPM continues to facilitatethe ongoing development of palliativemedicine with continued involvement in anumber of activities, including registrartraining, annual symposia and theinternational and humanities programmes. Itnow is a virtual institute that is not based at anyone facility but continues to be governed by anexecutive committee.
Context and backgroundThe care of patients with progressive life-limiting illness has always been a centralactivity in medical practice. In the 19thcentury, institutions were created with thecare of such patients as their principal role –examples were to be found in Dublin andLondon.1 In the 1960s, a hospice movementevolved in the UK, principally through thework of Cicely Saunders. Her work inspiredclinicians around the world including BalfourMount in Canada, Michael Kearney in Ireland
The Sydney Institute of Palliative Medicine: evolution and contributionghauri aggarwal, Jan Maree Davis, Frank Brennan and Kristen Turner look at how the
Sydney Institute of Palliative Medicine came into being and played a pioneering role in
the transformation of palliative care provision in Australia and elsewhere in the world
&GhauriAggarwalFRACP FAChPM
FFPMANZCA Chair 1
and Head ofDepartment 2
Jan MareeDavisFRACP FAChPM
Education Lead,1Area Director 3 andMedical Director 4
Frank BrennanFRACP FAChPM
Palliative CarePhysician 4,5
Kristen TurnerFAChPM SpecialistPalliative MedicinePhysician6
1 Sydney Institute ofPalliative Medicine,Sydney, Australia
2 Concord Centre forPalliative Care,Sydney, Australia
3 Palliative CareService, South-Eastern SydneyLocal Health District,Sydney, Australia
4 Palliative CareService, St GeorgeHospital, Sydney,Australia
5 Calvary Hospital,Sydney, Australia
6 CampbelltownHospital, Sydney,Australia
and, in Australia, Brian Dwyer, Brian Pollard,Jocelyn Kramer, Ian Maddocks, Norelle Lickissand others.
The foundations for a hospital-basedpalliative care service in Sydney were laiddown as a direct result of a visit from BalfourMount to the RPAH in 1982, where hechallenged senior clinicians regarding the careof dying patients. By 1985, a decision wasmade to expand and restructure the hospital’sprovision of palliative care and to appoint afull-time consultant physician to improve thecare of patients within the hospital.2 By theend of that year, the Palliative Care Service(PCS) at RPAH was one of three existing inteaching hospitals in Sydney, but the first thatwould be led by a consultant physician withfull admitting rights and responsibilities,which also included the community setting.
The inspiration-led beginnings of palliativemedicine elsewhere in the world were
matched by a growingrecognition locally inSydney of: the needs of
n Palliative medicine began to evolve internationally in the late 1980s.
n The Sydney Institute of Palliative Medicine (SIPM) was established in1989 to oversee palliative medicine training for doctors. It played alarge role in shaping the development of palliative medicine as aclinical science and a speciality in NSW, Australia, and internationally.
n During the 1990s, SIPM became the largest unified group ofregistrar training positions – both in Australia and internationally.
n SIPM continues to facilitate the development of palliative medicineand to oversee registrar training across NSW, Australia, and attractsdoctors from many countries, who, once trained, return home toestablish or develop their own palliative care service.
Keypoints
Copyright © Hayward Medical Communications 2016. All rights reserved. No unauthorised reproduction or distribution. For reprints or permissions, contact [email protected]

286 EUROPEAN JOURNAL OF PALLIATIVE CARE, 2016; 23(6)
Perspective www.ejpc.eu.com
patients and their families; the significantdearth of understanding of the mechanismsand management of the symptomatology andpsychosocial needs of patients and theirfamilies; the very small numbers of doctorsinvolved; and the need for greater training inthis evolving area of medicine.
Origins of SIPMSIPM’s founding director, Norelle Lickiss,identified that a crucial component for the growth of palliative care services and,indeed, of palliative medicine generally, was the nurturing and training of competentand skilled doctors.3 Kristen Turner shared this vision and became the first registrar ofRPAH’s PCS in 1986. At this time palliativemedicine was not a speciality; there was no local training programme and local doctors interested in training needed to travel overseas.
Other training positions were soonestablished in the RPAH consultative service,the palliative care inpatient unit at EversleighHospital and the community home visitsservice.4,5 As there was still no accepted
pathway to a speciality, theInstitute of Palliative Medicinewas created to integrate,co-ordinate and accredit thetraining in these various services.It was formalised and enhanced
in 1989 and later renamed SIPM. By 1990,John Dwyer, the clinical and academic head ofPrince of Wales Hospital – another teachinghospital in Sydney, affiliated with theUniversity of New South Wales – expressedthat institution’s desire to enhance its existingpalliative care service. A particular focusdeveloped in the associated gynaecologicalcancer unit at the Royal Hospital for Womenheaded by Neville Hacker, as had occurred atthe RPAH. Over the next decade, withexpansion in all the major teaching hospitalsin Sydney, SIPM became the largest unifiedgroup of registrar training positions – both inAustralia and internationally – encompassingthree settings: teaching hospital, palliativecare inpatient unit and community services.
Early visionNorelle Lickiss’ vision included inculcating intrainees the highest standards of internalmedicine. She also emphasised theimportance of understanding the depth of the
psychosocial and spiritual dimensions ofserious illness, utilising perspectives drawnfrom the humanities, sharing her knowledgeand insights in the time-honoured way ofmedical apprenticeship. It was clear that acomprehensive registrar training programmewas required in order to ensure that certainstandards implied in the College of Physicianstraining programmes, would be rigorouslyapplied to palliative medicine, so that thisspeciality could compete with others on alevel playing field and be seen as a ‘proper’medical speciality in its own right. Palliativemedicine was evolving worldwide – it wasrecognised as a medical speciality in the UK in1987 and in Australia in 1988, with the firstChair of Palliative Care established in FlindersUniversity, South Australia.6
For SIPM, two important philosophicalunderpinnings of palliative medicine clinicaltraining were the concept of the patient asteacher and the use of the palliative medicineconsultation as an educational tool in itself:7
each consultation gave a rich opportunity toteach and demonstrate the learning goals inpalliative care, with the patient providing theunique context of their individual problems,needs and insights.
Comprehensive clinical training Trainees were drawn from a variety ofbackgrounds and training programmes,including general practice, internal medicine and radiation oncology, for either career training in palliative medicine orskills enhancement relevant to other careerpaths.8 Career trainees from backgroundsother than the Royal Australasian College ofPhysicians (RACP) training programme wererequired to formally complete an SIPMCertificate. This involved a core period of 18months, and preferably two years, spent in apalliative care service associated with ateaching hospital, at least six months in aspecialised inpatient palliative care unit plus experience in consultative palliativemedicine in both a general hospital and acommunity setting. A strong apprenticeshipethos was employed.9 Formal teachingsessions, weekly clinical meetings and aweekly ‘journal club’ supplemented theclinical work. Kristen Turner (the first SIPMregistrar) was the Co-ordinator of RegistrarTraining from 1994 to 2003 and cruciallyinvolved in the preparation of educational
Cicely Saunders’ …work inspiredclinicians aroundthe world
Copyright © Hayward Medical Communications 2016. All rights reserved. No unauthorised reproduction or distribution. For reprints or permissions, contact [email protected]

287EUROPEAN JOURNAL OF PALLIATIVE CARE, 2016; 23(6)
material and mentoring of registrars. TheSIPM Certificate programme was closelysupervised with evaluations by an internaland external examiner. Throughout thatperiod the latter role was filled by GeoffreyHanks from the UK, who visited Australiaevery two years in the 1990s. Hanks’s adviceand encouragement to SIPM was pivotal andgreatly appreciated. The UKrecognised the quality of SIPMtraining and accredited oneyear of higher training,leading to senior registrarsfrom the UK joining theprogramme in 1994–1996.The certificate programme paralleled thepathway of training in palliative medicine established by the RACP andforeshadowed the eventual establishment of the Chapter of Palliative Medicine withinthe college in 1999.10
EducationIn addition to bedside teaching and clinicalexposure, a strong focus of SIPM was formalteaching. From its inception there was a keenrecognition by both Norelle Lickiss andKristen Turner of the significant advances thatwere occurring in all aspects of palliativemedicine and the importance of
incorporating that knowledge into thetraining of registrars.
In the institute’s early days there was noformal registrar education programme. Muchof the education occurred in the setting of thePCS journal club held every Tuesdayafternoon. This was attended by all registrars,consultants and senior staff, including clinical
nurse consultants and thebereavement servicecounsellor. Following journalclub, registrars convened inthe local hotel to shareexperiences and to providesupport to each other. This
informal networking was an invaluable part ofthe training. In addition, a core of giftednurses, including Ralph Waldsax, JoanHartley, Cheryl Dunn and Joan Ryan,nurtured this enterprise from its embryonicbeginnings and encouraged all those involved.
As the number of trainees and training sitesgrew, the need to formalise and standardiseaspects of the educational programme was recognised.
In the 1990s, the RACP formally establisheda palliative medicine curriculum. A decadelater the Chapter of Palliative Medicine wasestablished; it now oversees trainee educationand supervises registrars in their requirements
The patient provided theunique context of theirindividual problems,needs and insights
www.ejpc.eu.com Perspective
n The Royal Prince AlbertHospital, Sydney, home ofthe Sydney Institute ofPalliative Medicine.JANEEN FOFFANI
Copyright © Hayward Medical Communications 2016. All rights reserved. No unauthorised reproduction or distribution. For reprints or permissions, contact [email protected]

288 EUROPEAN JOURNAL OF PALLIATIVE CARE, 2016; 23(6)
Perspective www.ejpc.eu.com
of Project and Case Study. The Chapter has alsoestablished a Diploma in Palliative Medicine.
This has meant evolution of SIPM’s role inprovision of and contribution to registrartraining, with an Educational Subcommitteeestablished in 2007. This subcommittee hasestablished bimonthly seminars that are heldand attended by all the SIPM registrars –Advanced Trainees, Diploma trainees andothers – in Sydney and the entire NSW statecohort. Topics are selected in order to addressknowledge ‘gaps’ identified by the EducationCommittee and/or according to topicsdeemed to be of general interest andrelevance. Seminars cover topics such asClinical Ethics, Pain, Pathophysiology andPharmacology, and Grief and Bereavement, as well as topics addressing the humanities.This programme is complementary to theRACP programme, which has developedonline learning modules in recent years.
Annual symposiumFrom its early days, SIPM has hosted an annualsymposium. The SIPM Symposium wasestablished to educate, disseminate ideas andto maintain dialogue between clinicians. Over the years, presentations by local andinternational speakers – including GeoffreyHanks and Ilora Finlay from the UK, NicolasChristakis and Jack Coulehanfrom the USA, MichaelKearney from Ireland and NeilMacDonald from Canada –have inspired doctors in theirpractice. Today, the SIPMSymposium continues toattract prominent speakers to a two- to three-day programme, including a researchafternoon at which final-year AdvancedTrainees are encouraged to present projects. A unique feature of these symposia has beenthe creation of a doctors-only session entitled‘Cautionary Tales’, at which clinicians coulddiscuss difficult, humbling and challengingcases in a safe environment.
NSW Palliative Care Registrar NetworkIn the late 1990s attempts were made todevelop a board that would oversee SIPM’sactivities and outline the institute’s vision andgoals; the resultant body has now evolved intothe current SIPM Executive, which is overseenby an administrative officer.
For an extended period, SIPM was thelargest stakeholder in registrar training inpalliative medicine in NSW. Recruitment wasinitially on an ad hoc basis, and interviewsfocused on the interest of the candidate inpalliative care and their communication skills.
Over time, the number of registrar trainingsites increased and there needed to be astandardised recruitment and selectionprocess. Initial discussion about how tostreamline the recruitment process took placewithin the SIPM Executive, Medical Oncologyand Radiation Oncology specialities and theDepartment of Health. In 2013, SIPM tookleadership in forming an NSW Palliative CareRegistrar Network. A rotating convenor drawnfrom directors of palliative care from thedifferent local health districts formed part ofthe governance. This process was seen as fairand maintained an even distribution oftrainees across the state. By 2016 there were 41 registrar positions.
International activitiesFrom the outset, Norelle Lickiss wasdetermined to seek out the best new ideas andthinking from around the world relevant topalliative medicine and incorporate them intoSIPM’s activities. There was recognition ofopportunities to assist colleagues in less
affluent environments,notably with issues in cancerpain relief and the care ofincurable and dyingpatients. The first few SIPMtrainees spent a year or moreon fellowships with some of
the key international leaders in these areas.The international dimensions of SIPM have
grown organically. Norelle Lickiss didconsiderable international teaching in theearly to mid-1990s. SIPM colleagues continueto participate in teaching in the Asia-Pacificarea in collaboration with local leaders andexperts. This philosophy of internationalteaching is valued by all involved.
From initiation, the training programmeattracted international registrars and fellows,who then returned to their home nations toestablish or develop services in Asia, Oceania,the Middle East and Europe.
The international programme continues tobe vibrant and is expanding. Partnershipshave been formed with other organisationssuch as Hospis Malaysia, Asia Pacific Hospice
international registrars… returned to their homenations to establish ordevelop services there
Copyright © Hayward Medical Communications 2016. All rights reserved. No unauthorised reproduction or distribution. For reprints or permissions, contact [email protected]

289EUROPEAN JOURNAL OF PALLIATIVE CARE, 2016; 23(6)
www.ejpc.eu.com Perspective
Network and the Lien Collaborative inSingapore. Future plans are underway topartner with these organisations in an attemptto develop a distance-learning programme fora diploma or masters of palliative medicine.
Humanities programmeHumanities were always recognised withinSIPM as a vital component in broadening theway in which patients are understood, and inbridging the experiential gap between abiomedical education and the need fordoctors to be deeply cognisant of a sharedhuman condition with their patients. Thisaspect of patient-centred care is now muchbetter-recognised, and the humanities areseen as ‘integral in the training of all thoselooking after human beings in the final part oftheir life journey.’11
The SIPM humanities programme wasmultifaceted, incorporating literature, art,drama and music into various educationalevents, including poetry reading evenings co-organised by SIPM and the University ofSydney.12 Humanities sessions continue to beincorporated into the format of the annualsymposium, giving the audience a diversity oflearning and experiential opportunities.
Research The necessary focus in the early years was intraining adequate numbers of skilledclinicians to provide expert hands-on care, butin-house audits and several unpublishedstudies were subsequently undertaken. Casereports illustrating novel approaches tosymptom relief were published.13–15 Furtherresearch considerations more graduallyevolved, particularly after the return to RPAHof Paul Glare as Head of Palliative Care. In themid-1990s a Sydney clinical trials groupincluded members of SIPM who participatedin pain and opioid trials. Researchers withinSIPM provided important early groundworkaround dignity,16 opioid purchasing patternsin Australian settings,17 suffering andprognostication.18 SIPM-trained clinicianshave also completed PhD programmes inmatters relevant to palliative care and exerciseacademic and research leadership.
ConclusionSIPM continues to be as relevant today as at itsinception in the 1980s. It pioneered the largestAustralian training programme for palliative
medicine registrars before the creation of theAustralasian Chapter of Palliative Medicine,RACP, and continues to provide leadership inthe current networked recruitment process.
As influenced by its founder Norelle Lickiss,the institute continues to emphasise thepatient as teacher, the practice of secularpalliative care and the strength to be gainedfrom solid internal medicine skills combinedwith an ability to reflect on and understandthe essence of suffering. These values continueto underpin the institute’s many activities.
The solid foundation provided by SIPM formany doctors has enabled us to go forth anddevelop services and educational programmesand to become leaders in palliative care.‘Patient as person’ continues to be the focus ofour care and enables the patient to becomeour educational resource.
Declaration of interestThe authors declare that there is no conflict of interest.
AcknowledgmentsThe authors recognise the assistance of several colleagues in preparing thisarticle, notably Norelle Lickiss AO, Clinical Professor (Hon), University ofSydney and Consultant Emeritus at Royal Prince Alfred Hospital and RoyalHospital for Women, Sydney – Founder of SIPM and continuing mentor; andJaneen Foffani, current SIPM Administrative Officer.
References1. Payne S, Lynch T. International progress in creating palliative medicine as aspecialized discipline and the development of palliative care. In: Cherny N,Fallon MT, Kaasa S et al (eds). Oxford textbook of palliative medicine, 5th edn.Oxford: Oxford University Press, 2015: 3–9.2. Lewis MJ. Medicine and care of the dying: a modern history. Oxford: OxfordUniversity Press, 2007: 142.3. Turner KS, Lickiss JN. Postgraduate training in palliative medicine: theexperience of the Sydney Institute of Palliative Medicine. Palliat Med 1997;11: 389–394.4. Lickiss N, Glare P, Turner K et al. Palliative care in central Sydney: the RoyalPrince Alfred Hospital as catalyst and integrator. J Palliat Care 1993; 9: 33–43.5. Lickiss JN, Wiltshire J, Glare PA, Chye RWM. Central Sydney Palliative CareService: potential and limitations of an integrated palliative care servicebased in a metropolitan teaching hospital. Ann Acad Med Singapore 1994; 23: 264–270.6. Lewis MJ. Medicine and care of the dying: a modern history. Oxford: OxfordUniversity Press, 2007: 146.7. Turner KS, Lickiss JN. Postgraduate training in palliative medicine: theexperience of the Sydney Institute of Palliative Medicine. Palliat Med 1997;11: 389–394.8. Turner KS and Lickiss JN. The Sydney Institute of Palliative Medicineregistrar training program. Innovations in End-of-Life Care 2002; 4: 8p9. Turner KS, Lickiss JN. Postgraduate training in palliative medicine: theexperience of the Sydney Institute of Palliative Medicine. Palliat Med 1997;11: 389–394.10. Cairns W, Yates PM. Education and training in palliative care. Med J Aust2003; 179: 26. 11. Kirklin D. The role of humanities in palliative medicine. In: Hanks G,Cherny NI, Christakis NA (eds). Oxford textbook of palliative medicine, 4th edn.Oxford: Oxford University Press, 2010: 1603.12. Goulston SMJ. Medical education in 2001: the place of the medicalhumanities. Intern Med J 2001; 31: 123–127.13. Philip J, Lickiss JN, Grant PT et al. Corticosteroids in the management ofbowel obstruction on a gynecological oncology unit. Gynecol Oncol 1999; 74: 68–73.14. Chye RWM, Lickiss JN. The use of corticosteroids in the management ofbilateral malignant ureteric obstruction. J Pain Symptom Manage 1994; 9: 537–540.15. Agar M, Broadbent A, Chye R. The management of malignant psoassyndrome: case reports and literature review. J Pain Symptom Manage 2004;28: 282–293.16. Turner K, Chye RWM, Aggarwal G et al. Dignity in dying: a preliminarystudy of patients in the last three days of life. J Palliat Care 1996; 12: 7–13.17. Turner KS, Kaye K, Philip J et al. Opioid purchasing patterns: an indicatorof cancer pain relief? 4th Australian Palliative Care Conference. Canberra,Australia, 1997.18. Glare P, Virik K. Independent prospective validation of the PaP score interminally ill patients referred to a hospital-based palliative medicineconsultation service. J Pain Symptom Manage 2001; 22: 891–898.
Copyright © Hayward Medical Communications 2016. All rights reserved. No unauthorised reproduction or distribution. For reprints or permissions, contact [email protected]

290 EUROPEAN JOURNAL OF PALLIATIVE CARE, 2016; 23(6)
Researc h www.ejpc.eu.com
The Palliative and end of life carePriority Setting Partnership (PeolcPSP)and the James Lind Alliance (JLA)
sought to identify the research priorities thatare most important to patients, carers, andhealth and social care professionals involvedat the end of life.1,2 The PeolcPSP identified 83questions that were not shown to be answeredby an up-to-date systematic review (throughCochrane or identified via the Database ofAbstracts of Reviews of Effects3). Carers,patients and clinicians highlighted a top ten list from the 83 questions at aprioritisation workshop.
Palliative and end-of-life careresearch is underfundedThis project used the UK Clinical ResearchCollaboration’s Health Research ClassificationSystem (HRCS) dataset, composed of£2 billion of funding in 2014 from 64governmental and charitable funders acrossthe UK.4 This dataset shows that end-of-liferesearch represents only 0.16% of the totalhealth-related research active in 2014. The2014 dataset is the third to be conducted butthe first to be made publicly available. Usingthese publicly available data, we set out todiscover whether there is currently ongoingresearch that already addresses any of thequestions put forward by the PeolcPSP.
The aims of this project were to:� help researchers avoid duplication by
highlighting current research� foster collaboration by showing who is
already active in addressing specific research questions
� encourage researchers to tackle questionsthat are not currently examined at all.
MethodologyKeywords for each of the 83 PeolcPSPquestions were identified, and the HRCS 2014dataset of 14,394 grant abstracts was searchedfor links. The resulting abstracts were screenedfor relevance to the individual PeolcPSPquestions and divided into:� interventional grants: projects that
proposed an intervention (see Box 1) toaddress the question
� direct grants: projects that had a direct link to the question but did not propose an intervention. For the purposes of this research, these are
referred to together as ‘strong funding’.Detailed results for all 83 questions are due tobe published in a forthcoming report.5 Table 1shows the number of strong grants and thetotal funding allocated in 2014 for the top tenPeolcPSP priorities.
All top ten research questions are already attracting some research interestOur analysis shows that the top ten researchpriorities for palliative and end-of-life care,as highlighted by patients, carers andclinicians, are all already attracting someresearch interest and funding, even thoughat very different levels (see Table 1). The table
Does current UK researchaddress priorities in palliativeand end-of-life care?The Palliative and end of life care Priority Setting Partnership uncovered 83 unanswered research questions.
Florence Todd Fordham, Bridget Candy, Stevie McMillan and Sabine Best show that, as current UK research
starts to address some of these questions, UK open grant data have the potential to encourage collaboration
&Florence ToddFordhamPhD ProjectCoordinator 1
Bridget CandyPhD Researcher 2
StevieMcMillanBA (Hons) ResearchGrants Officer 1,3
Sabine BestPhD Head ofResearch1
1 Marie Curie UK,London
2 Marie Curie PalliativeCare ResearchDepartment,University College,London
3 Pancreatic CancerUK, London
Interventions aretreatments, care and otheractions that are designed to make a difference topatients, carers and familiesand that can be tested andevaluated by research.
Box 1.What is anintervention?
Copyright © Hayward Medical Communications 2016. All rights reserved. No unauthorised reproduction or distribution. For reprints or permissions, contact [email protected]

291EUROPEAN JOURNAL OF PALLIATIVE CARE, 2016; 23(6)
www.ejpc.eu.com Researc h
Table 1. results of the grant mapping exercise in relation to the top ten peolcpSp priorities in 2014, ranked by funding amount 5
Top ten priority questions
Strong uK fundingamount (of
which proposedinterventions)
Number of strong uKgrants addressing
the question (ofwhich proposedinterventions)
Systematicreview butquestionremains
unanswered*
Top ten rankposition
What are the best ways to determine a person’spalliative care needs, then initiate and deliver this carefor patients with non-cancer diseases (such as chronicobstructive pulmonary disease [COPD], heart failure,motor neurone disease [MND], AIDS, multiple sclerosis,Crohn’s disease, Parkinson’s disease, dementia and stroke)?
£4,307,040(£758,347) 31 (6) NO 6
How can access to palliative care services be improvedfor everyone, regardless of where they are in the UK?
£1,915,340(£528,256) 16 (4) NO 2
What are the benefits, and best ways, of providingcare in the patient’s home, and how can home care be maintained as long as possible? Does good coordination of services affect this?
£1,565,916(£45,820) 11 (1) YES 6 8
How can it be ensured that staff, including health careassistants, are adequately trained to deliver palliativecare, no matter where the care is being delivered? Doesincreasing the number of staff increase the quality ofcare provided in all settings? To what extent doesfunding affect these issues?
£1,414,488(£321,796) 11 (1) NO 5
What are the benefits of Advance Care Planning andother approaches to listening to and incorporatingpatients’ preferences? Who should implement this and when?
£1,225,808(£234,801) 13 (3) YES 7 3
What are the best ways to assess and treat pain anddiscomfort in people at the end of life withcommunication and/or cognitive difficulties, perhapsdue to motor neurone disease (MND), dementia,Parkinson’s disease, brain tumour (includingglioblastoma) or head and neck cancer, for example?
£1,003,763(£399,855) 4 (2) NO 10
What are the core palliative care services that should beprovided, no matter what the patient’s diagnosis is?
£628,219(£0) 5 (0) NO 7
What are the best ways to make sure that there iscontinuity for patients at the end of life, in terms of thestaff that they have contact with, and does thisimprove quality of palliative care? Would having adesignated case-coordinator improve this process?
£528,015(£0) 5 (0) NO 9
What are the best ways of providing palliative careoutside of ‘working hours’ to avoid crises and helppatients to stay in their place of choice? This includessymptom management, counselling and advice, GP visits and 24-hour support, for patients, carers and families?
£516,924(£0) 4 (0) NO 1
What information and training do carers and familiesneed in order to provide the best care for their lovedone who is dying?
£343,410(£265,383) 9 (5) YES 8 4
* As of January 2015
Copyright © Hayward Medical Communications 2016. All rights reserved. No unauthorised reproduction or distribution. For reprints or permissions, contact [email protected]

Palliative care beyond cancer: a sizeable research communityThe £4.3 million received by the PeolcPSP mostfunded top ten priority in 2014 – palliative carefor people with non-cancer diseases – financed31 grants, including six that proposedinterventions. Research addressing this prioritycovers a range of conditions (see Figure 1).Neurological conditions take up almost three-quarters of the funding; of this, 80% relates todementia, of which 82% is government-funded. This highlights the effect of a recentpush by the UK government to increasedementia research in 2012.11
292 EUROPEAN JOURNAL OF PALLIATIVE CARE, 2016; 23(6)
Researc h www.ejpc.eu.com
shows that three of the top ten questionsreceived no funding to supportinterventions in 2014. This contrasts withthe question that received the most funding,tackling palliative care in a wide number ofnon-cancer diseases, which received fundingtotalling £4.3 million in 2014, 18% of whichproposed to test an intervention. This willhopefully help to bring much-neededchange to practice in this area in the future.
Research questions that currentlyattract little attentionThe top ten priority that received the leastresearch funding in 2014 addressed the need for further research on support andinformation for families and carers. The totaldirect funding to this question amounted toonly £343,410. Of this, £265,383 came fromfive small interventional grants and the restcame from four direct grants. Three-quartersof this funding came from Marie Curie, withmost of it funded in a one-off themed researchcall that focused on informal carers and wasco-funded by Dimbleby Cancer Care.9
The number one priority, as decided bypatients, carers and healthcare professionals,asked how best to provide out-of-hourspalliative care. This priority attracted noresearch proposing interventions and receivedonly £516,924 of direct funding, which is just0.03% of the total health research funding in2014.10 It is clear that there is much need forfurther research to propose and testinterventions to address the issue of out-of-hours palliative care, which is so important tocarers, patients and health and social careprofessionals. The same can be said for thequestions relating to continuity of care andthe core palliative care services; bothquestions attracted no research proposinginterventions and only a limited amount ofdirect funding in 2014.
Our wider analysis shows that of the 83research questions identified in the PeolcPSP,19 are not addressed by any research projectsdirectly tackling the question.5 A further 10questions were addressed by less than £50,000of strongly related funding in 2014. Thesubtheme of bereavement received nostrongly related funding in 2014, with nodirect or interventional grants addressing anyof the four questions in the theme. The detailsof this analysis are included in a forthcomingfull report.5
Respiratory8% Stroke
4%
Cardiovascular6%
Generic healthrelevance
10%
Neurological72%
n Figure 1. Health categories
represented in top tenquestions relating tonon-cancer diseases
n Published in 2015, the PeolcPSP report is being used to guidepalliative and end-of-life care research funding.
n We have reviewed an open database of 2014 UK health researchgrant data to identify if and how current research is addressing the83 PeolcPSP questions.
n The aims of this project include helping researchers avoidduplication by highlighting current research and fosteringcollaboration by showing who is already active in addressingspecific questions.
n This project highlights that research spending in palliative and end-of-life care remains low, with pockets of good news. It also highlightsthe need for more research proposals and testing interventions totackle the problems encountered in palliative and end-of-life care.
n The number one PeolcPSP priority – how to provide palliative careout of hours – is one of the questions most in need of furtherresearch investment.
n Of the 83 questions, 19 are not addressed by any directly relatedresearch funding active in 2014.
Keypoints
Copyright © Hayward Medical Communications 2016. All rights reserved. No unauthorised reproduction or distribution. For reprints or permissions, contact [email protected]

There is a sizeable community of researchersnow looking at non-cancer conditions, suchas heart failure,12 non-cancer lung diseasessuch as chronic obstructive pulmonarydisease13 and interstitial lung disease,14
stroke,15 organ failure 16 and dementia.17 This isvery encouraging, though clearly the overallamount spent on this question is splitbetween many disease areas.
Next stepsThis project shows only a snapshot of UKresearch addressing the questions identified bypatients, carers and clinicians. There will beresearch not included in this dataset that mightbe active now or have finished before 2014. It isclear, however, that as none of the 83 questionshave been answered in a systematic review, theneed for more research in palliative and end-of-life care remains. In particular, it is necessary todevelop and test interventions that addresspatient and carer needs in this area.
The PeolcPSP project has shown that someareas of palliative and end-of-life care research are making progress, and funder initiativessuch as the former UK prime minister’s‘challenge on dementia’, along with smallerthemed calls by charities such as DimblebyCancer Care and Marie Curie, are clearlyhaving an impact in an area so strongly inneed of more research.
Other areas of need, such as bereavement,are not currently addressed by research at allor by only a small amount. The full report ofthis project, which will be released soon,allows researchers and funders to identifycurrently active projects and, through those,researchers and clinicians already engaged in aparticular field. We hope that it might help toidentify potential future collaborators since italso includes references to research that is onlyweakly linked to a particular question.
We hope that highlighting the questionswith little current funding will encourageresearchers and funders to endeavour to look into these further. Some questions, inparticular in the top ten, are broad researchpriorities and might require further work to identify more focused research questions. A recent local initiative from theCollaboration for Leadership in AppliedHealth Research and Care (CLAHRC) GreaterManchester has demonstrated a method ofachieving this. It used focus groups andworkshops with local carers and health care
professionals to identify more detailedresearch questions relevant to local needwithin the PeolcPSP top ten questions.18
Research funders can help by providingclearer information about funding streamsthat are open for palliative and end-of-life care research and by supporting researchers in developing applications in new topic areas.Collaborations between funders in areas of common interest will help to make betteruse of limited research funds and avoidunnecessary duplication. In the UK, a group of funders with an interest in palliativeand end-of-life care meets regularly as the UK end of life care Research Interest Group (UKeolcRIG).19
Acknowledgements The authors are grateful to Dr Sanjay Thakrar and Professor Bill Noble foradvice on the search terms used to conduct the grant mapping project.
References1. PeolcPSP. Palliative and end of life care Priority Setting Partnership (PeolcPSP) –final report. London: PeolcPSP, 2015.https://palliativecarepsp.files.wordpress.com/2015/01/peolcpsp_final_report.pdf(last accessed 22/08/16)2. Smith R, Best S, Noble B. Identifying palliative and end of life care research priorities: a UK approach to consult end users. Eur J Pall Care 2015;22: 114–7.3. DARE: www.crd.york.ac.uk/crdweb/; Cochrane: www.cochranelibrary.com/cochrane-database-of-systematic-reviews/ (last accessed 01/09/16)4. UK Clinical Research Collaboration. UK Health Research Analysis 2014.London: UK Clinical Research Collaboration, 2015. www.hrcsonline.net/pages/uk-health-research-analysis-2014 (last accessed 01/09/16)5. Todd Fordham F, Candy B, Noble B et al. How is current palliative and end oflife care research addressing the priorities of patients, families and clinicians?London: Marie Curie, 2016 (in press)6. Gomes B, Calanzani N, Curiale V et al. Effectiveness and cost-effectivenessof home palliative care services for adults with advanced illness and theircaregivers. Cochrane Database Syst Rev 2013; 6: CD007760.7. Houben CH, Spruit MA, Groenen MT et al. Efficacy of advance careplanning: a systematic review and meta‐analysis. J Am Med Dir Assoc 2014; 15: 477–489.8. Capurro D, Ganzinger M, Perez‐Lu J, Knaup P. Effectiveness of ehealthinterventions and information needs in palliative care: a systematic literaturereview. J Med Internet Res 2014; 16: e72.9. Dimbleby Marie Curie Research Fund.www.mariecurie.org.uk/research/funding-research/dimbleby-marie-curie-research-fund (last accessed 19/08/16)10. UK Clinical Research Collaboration. UK Health Research Analysis 2014.London: UK Clinical Research Collaboration, 2015.www.hrcsonline.net/sites/default/files/UKCRCHealthResearchAnalysis2014%20WEB.pdf (last accessed 23/08/16)11. Department of Health. Prime Minister's challenge on dementia 2020.www.gov.uk/government/uploads/system/uploads/attachment_data/file/414344/pm-dementia2020.pdf (last accessed 19/08/16)12. Denvir, M. Murray, S. and Boyd, K. Future care planning: a first step topalliative care for all patients with advanced heart disease. Heart 2015; 101: 1002–7.13. Javadzadeh S, Chowienczyk S, Booth S, Farquhar MC. Comparison ofrespiratory health-related quality of life in patients with intractablebreathlessness due to advanced cancer or advanced COPD. BMJ SupportPalliat Care 2016; 6: 105–8.14. Boland J, Reigada C, Yorke J et al. The adaptation, face, and contentvalidation of a needs assessment tool: progressive disease for people withinterstitial lung disease. J Palliat Med 2016; 19: 549–5.15. Burton C, Payne S, Turner M et al. The study protocol of: ‘Initiating end oflife care in stroke: clinical decision-making around prognosis’, BMC PalliatCare 2014; 13: 55.16. Kendall M, Carduff E, Lloyd A et al. Different experiences and goals indifferent advanced diseases: comparing serial interviews with patients withcancer, organ failure, or frailty and their family and professional carers. J PainSymptom Manage 2015; 50: 216–224.17. Jones L, Candy B, Davis S et al. (2016). Development of a model forintegrated care at the end of life in advanced dementia: A whole systems UK-wide approach. Palliat Med 2016; 30: 279–295.18. NHS NIHR Collaboration for Leadership in Applied Health Research andCare (CLAHRC) for Greater Manchester. Next steps for end-of-life research:Research priorities defined for Greater Manchester. Salford: Salford Royal NHSFoundation Trust, 2016.19. Marie Curie. UK end of life care Research Interest Group (UKeolcRIG).www.mariecurie.org.uk/research/end-of-life-care-research-interest-group(last accessed 01/09/16)
293EUROPEAN JOURNAL OF PALLIATIVE CARE, 2016; 23(6)
www.ejpc.eu.com Researc h
Copyright © Hayward Medical Communications 2016. All rights reserved. No unauthorised reproduction or distribution. For reprints or permissions, contact [email protected]

294 EUROPEAN JOURNAL OF PALLIATIVE CARE, 2016; 23(6)
Holistic care www.ejpc.eu.com
Pain is one of the most commonsymptoms reported in palliative careand is widely recognised as impacting
on all aspects of quality of life.1 Much researchhas been, and continues to be, carried out intothe processes underlying pain caused bycancer. Kumar, for example, describes amechanism-based classification of cancer painthat contains the following categories: centraland peripheral sensitisation; sympatheticallymaintained; nociceptive; and cognitive-affective pain.2 He addresses thepatho-physiology of cancer pain whileproviding a better understanding of patients’symptoms and response to treatments. TheBritish Pain Society states that cancer andnon-cancer pain share the same neuro-patho-physiological pathways,3 but further studiesare necessary to more fully understand thecauses of pain in non-cancer patients.4
In cancer patients, the WHO analgesicladder is the most commonly used medicalstrategy, and non-pharmacologicalinterventions can be used in conjunction withit to maximise a patient’s functionality andcontrol ‘over pain and circumstances’.2 In thiscontext of a multimodal approach to pain,
mindfulness meditation (MM) is gaininggrowing attention.
What is mindfulness? The concept of mindfulness is rooted inancient philosophical traditions such as Buddhism and Hinduism and is acomponent of vipassana (meditationpractised in Theravada Buddhism) and Zenmeditation. Kabat-Zinn, the pioneer of MM inWestern medicine, defined it in psychologicalterms as ‘paying total attention to the presentmoment with a non-judgemental awarenessof the inner and/or outer experience’,5
extrapolating it from any religious orphilosophical tradition.
During MM, the subject is asked to focuseither on their breathing or on sensory,emotional and cognitive happenings withoutinterpreting them or assigning them a positiveor negative value. The aim is to learn to livedeeply in the present experience withoutidentifying with it or overlaying it withconscious or unconscious projections, thusdeveloping acceptance.6
Pike cautions against the use of the term‘mindfulness’ alone on the basis that it doesnot contain any reference to the body andmay thus lead to misunderstanding regardingthe practice. He suggests that the term ‘body-mindfulness practice’ focuses more on theawareness of sensations arising from the bodyduring mindfulness practice. The suffix‘-fulness’ stands, in his view, for ‘awareness ofa full and unseparate body-mind complex’,which reveals the full extent of the practiceand its aim to alter physical symptomsthrough mind control.7
Mindfulness-based Cognitive Therapy(MBCT) and Mindfulness-based StressReduction (MBSR) are clinical approachesstructured to organise the original concept of
Mindfulness meditation and painmanagement in palliative careAs mindfulness meditation grows increasingly popular as a subject of study and as a practice in clinical
settings, irene Campagnolo Maschio looks into how the practice works and whether it has a valid
application in palliative care patients
&IreneCampagnoloMaschioBSc Physiotherapist,Princess AliceHospice, Esher,Surrey
n Pain is one of the main symptoms reported in palliative care andhas a huge impact on quality of life.
n Mindfulness meditation (MM) is receiving increased interest, alongwith other non-pharmacological interventions, for its potential tocontrol pain and maximise patient functionality in palliative care.
n Research shows MM is able to affect pain perception by modifyingthe activation of specific brain areas. However, more studies inpalliative settings are needed.
n MM can restore a sense of control ‘over pain and circumstances’,which is often lost in palliative care patients.
Keypoints
Copyright © Hayward Medical Communications 2016. All rights reserved. No unauthorised reproduction or distribution. For reprints or permissions, contact [email protected]

in his neuromatrix theory.9 The processing of information coming from our sensorysystem is informed by our own unique past experiences, present physical andpsychological condition and futureexpectations; the way in which a nociceptivestimulus is transformed into the subjectiveexperience of pain is one of the best examples of this process.10 Moseley statesthat it is the ‘implicit perception of threat thatdetermines the outputs, not the state of thetissues, not the actual threat to the tissues’.11
Tsang et al describe how thediagnosis of a life-limiting illnessposes a threat to the individual,resulting in a hypothalamic-pituitary-adrenal axis activation(that is linked to the fight-and-flightresponse) with a consequentialincrease in pain level.12
Edenfield and Saeed report that meditationelicits the relaxation response mediated by theparasympathetic nervous system; this reducesthe state of alarm created by the hyperarousalof the sympathetic nervous system andcounteracts the effects of stress hormones.13
Chiesa and Serretti found that the use of MMreorganises brain activity, with sustainedattention leading to a reduction in excessiveemotional reactivity and thus a cognitivecontrol of emotions.5 The ability to detach
295EUROPEAN JOURNAL OF PALLIATIVE CARE, 2016; 23(6)
mindfulness into standardised clinicalinterventions. As mindfulness is theirfundamental component, researchers tend togroup MBCT and MBSR together withvipassana and Zen practices in studies onmeditation. Specific differences exist betweenthe above approaches, however, that impacton their ability to provide a coherent andsystematic framework for mindfulness. Thereis also uncertainty about the role the differentcomponents of each approach have played inobserved clinical outcomes.5
How is it thought to work? The possibility of influencing healthand disease through the mind wascentral to the medical practices of theancient civilisations of Egypt andGreece, traditional Chinese medicineand Indian Ayurveda. Westernresearchers, after focusing on the body forcenturies, are now recognising and mappingthe interaction between mind, nervoussystem, immune system and the body usingscientific methods.8
Exactly how our perception of pain occurs isunknown, but scientists today generally agreethat pain perception is linked not only todamage incurred by a bodily structure but isalso affected by our physical, emotional andmental states, as suggested by Melzack (2001)
it is important for theclinician to tailor theintervention to the singlepatient’s pathology in orderto increase effectiveness
www.ejpc.eu.com Holistic care
n The exact mechanismsof pain remain unknown,but it is established thatpain is influenced by ouremotions, memories andstate of mind.AGSANDREW/SHUTTERSTOCK.COM
Copyright © Hayward Medical Communications 2016. All rights reserved. No unauthorised reproduction or distribution. For reprints or permissions, contact [email protected]

296 EUROPEAN JOURNAL OF PALLIATIVE CARE, 2016; 23(6)
Holistic care www.ejpc.eu.com
from negative emotions improves the mind-body interaction and can possibly explain theclinical results of MM.5
Possibilities and challenges in palliative settingsAn inverse relationship has been foundbetween meditation experience and painperception, but it is not clear if there arebaseline differences in the people recruitedthat might explain this result.6 Zeidan et alfound positive changes in pain sensitivityafter only one 20-minute meditation sessionper day for four days.10 These results comefrom non-clinical studies and require furtherinvestigation in a clinical context. They aresuggestive, however, of the possibility ofeffectively modifying pain perception in ashort period of time, enabling its applicationin a palliative setting, where time is afundamental variable.
An obvious weakness of all research in thisarea is the impossibility of conducting double-blind studies in meditation due to the natureof the intervention. Thenecessity for the patient tohave an active attitudetowards the technique maycreate a further bias linked to motivation and the abilityto participate in theintervention.14 Shennan et alpoint out how illiterate andpoorer people are generallyexcluded in the studiesreviewed, which can be a limit to a generalisedapplication of MM.15
In an interesting critique of the use of MMin clinical settings, Teasdale et al drawattention to the fact that MM should not beregarded as a mere attentional technique thatcan influence clinical problems in a quick andsimple way.16 Because MM includes variouscomponents, such as relaxation, self-management, acceptance and cognitivechanges, it is important for the clinician totailor the intervention to the single patient’spathology in order to increase effectivenessand avoid unhelpful treatments.
This raises questions about the ethicality ofapplying a potentially ineffective treatment.In a vulnerable population such as those inpalliative care, it is of paramount importanceto weigh ‘treatment burden against thepotential benefits’, and to discuss the patient’s
preferences.17 Professionals working with end-of-life patients have, however, been found tobe confident in discussing and facilitatingrationalised treatment refusal in order toincrease quality of life.18
Davidoff describes what he calls the‘responsibility paradox’, which arises from thebelief embedded in most types of alternativemedicine that mind and spirit hold deepwithin the remedy for most illnesses, innerresources that the patient needs to access inorder to heal himself.19 Talking in generalabout the use of alternative therapies, hewarns practitioners of the risk of instilling inthe patient a sense of guilt or fault if they areunable to modify their symptoms throughmind control. On the other hand, Davidoffrecognises that empowering the patient canbe a ‘crucial therapeutic tool’. Increasing thepatient’s control over body, emotions andthoughts, as offered by MM, is highlybeneficial and of particular value in peoplesuffering from life-limiting illnesses, in whommemories from past experiences, fear for the
future and detachment fromtheir own body can have ahuge impact.
Gotink et al state that ‘inchronic care both MBCT andMBSR help patients to copewith pain’, with an overallimprovement in quality of lifethanks to the acceptance-basedintervention typical of MM.14
A study by Tsang et al showshow the practice of body scanning (that is,becoming aware of the sensations arising fromthe body) can reduce overwhelming pain interminally ill cancer patients.12 Benefits werealready significant after the first week ofindividual practice and sustained andenhanced after a month of home sessions five days per week.
Bates describes her experience of leadingmindfulness groups in a hospice setting. Sheempasises the value of the group insupporting individuals in the practice of MM,even if patients with serious agitation, severedeafness, psychiatric disorders and severepost-traumatic stress are better treated inindividual sessions. She points out thatpalliative patients lack the energy to followthe strict practice of MBSR and MBCT but canbenefit from a modified practice.20 She givesno data regarding pain management.
physiotherapists arewell placed amonghealthcare professionalsto teach mindfulness inclinical settings becausethey are already trainedin facilitating body-awareness
Copyright © Hayward Medical Communications 2016. All rights reserved. No unauthorised reproduction or distribution. For reprints or permissions, contact [email protected]

297EUROPEAN JOURNAL OF PALLIATIVE CARE, 2016; 23(6)
www.ejpc.eu.com Holistic care
Ways of implementing MM There is an ongoing and open discussionamong researchers and practitioners aboutvarious methods of teaching mindfulness andtheir implications for the outcomes. Shennanet al found that among the 13 articles includedin their systematic review, no data regardingfacilitators were provided and only one authorsuggested that age and delivery style mightinfluence the patient’s perception of thepractice.15 Shennan et al also found nocorrelation between contact time andbenefits, while Gotink et al found a positivedose–response relationship between minutesof practice and stress reduction14 – meaningthat the benefits are significantly greater themore MM is practised.
In Pike’s opinion, physiotherapists are wellplaced among healthcare professionals toteach mindfulness in clinical settings becausethey are already trained in facilitating body-awareness through exercises, postures andbreathing techniques.7 Lee et al report awillingness among GPs to combineconventional and non-conventionaltreatments, along with recognition of theneed to develop better knowledge andunderstanding of complementary andalternative therapies in order to be able toadvise patients appropriately.21
Economically, MM therapy is generallyconsidered to be cost-effective by studies and reviews. Bates, however, states that MM will not be effective in reducing costs in a hospice setting due to the amount ofprofessional resources needed to plan andfollow up the intervention.20
Mindfulness practice is considered easy toimplement, with little or no risk involved onboth a physical and emotional level, if led bytrained and experienced practitioners.14,22
Conclusions To summarise, MM has been proved effectivein non-clinical settings at modulating painthrough the activation of specific brain areasresponsible for attentional mechanisms andemotional response to pain perception.Clinical studies show its effectiveness inchronic pain management, but further studiesare required to build on the evidence for theeffectiveness of MM in palliative care.Guidance is also needed on the screening ofpatients and the most appropriate setting(group versus individual treatment), contact
time (duration of single session andprogramme) and facilitator characteristics. It must be remembered, however, that good-quality randomised controlled trials aredifficult to apply in a palliative setting due to the nature of the patients.
The ability to pay sustained attention anddevelop acceptance allows the patient to workon all pain components from the physicallevel to the emotional and mental. MMrequires an active attitude and can restore asense of control over pain and circumstances,which is often lost in terminally ill patients.Because the palliative population isvulnerable, it is paramount that patients arescreened in order to identify those most likelyto benefit from the intervention and givemore scientific direction to the growingpopularity of MM therapy.
Declaration of interestThe author declares that there is no conflict of interest.
References1. Paice J, Ferrell B. The management of cancer pain. CA Cancer J Clin 2011; 61: 157–182. 2. Kumar S. Cancer Pain: A critical review of mechanism-based classificationand physical therapy management in palliative care. Indian J Palliat Care2011; 17: 116–126.3. British Pain Society. Cancer Pain Management. London: BPS, 2010.www.britishpainsociety.org/static/uploads/resources/files/book_cancer_pain.pdf (last accessed 16/08/15)4. Chan, V, Sorger B, Rosenfeld K et al. Pain and palliative medicine. J RehabilRes Dev 2007; 44: 279–294.5. Chiesa A, Serretti A. A systematic review of neurobiological and clinical features of mindfulness meditation. Psychol Med 2010; 40:1239–1252.6. Zeidan F, Grant J, Brown C, Mchaffie J, Coghill R. Mindfulness meditation-related pain relief: Evidence for unique brain mechanisms in the regulationof pain. Neurosci Lett 2012; 520: 165–173.7. Pike A. Body-mindfulness in physiotherapy for the management of long-term chronic pain. Phys Ther Rev 2008; 13: 45–568. Mayden K. Mind-body therapies: evidence and implications in advancedoncology practice. J Adv Pract Oncol 2012; 3: 357–373.9. Melzack R. From the gate to the neuromatrix. Pain 1999; Aug(S6): S121–S126.10. Zeidan F, Martucci K, Kraft R et al. Brain mechanisms supporting themodulation of pain by mindfulness meditation. J Neurosci 2011; 31:5540–554811. Moseley L. Reconceptualising pain according to modern pain science.Phys Ther Rev 2007; 12: 169–178.12. Tsang S, Mok E, Lam S, Lee J. The benefit of mindfulness-based stressreduction to patients with terminal cancer. J Clin Nurs 2012; 21: 2690–2696. 13. Edenfield T, Saeed S. An update on mindfulness meditation as a self-helptreatment for anxiety and depression. Psychol Res Behav Manag 2012; 5: 131–141.14. Gotink R, Chu P, Busschbach J et al. Standardised mindfulness-basedinterventions in healthcare: an overview of systematic reviews and meta-analyses of RCTs. PloS ONE 2015; 10: e012434415. Shennan C, Payne S, Fenlon D. What is the evidence for the use ofmindfulness-based interventions in cancer care? A review. Psychooncology2011; 20: 681–697.16. Teasdale J, Segal Z, Williams M. Mindfulness training and problemformulation. Clin Psychol Sci Pract 2003; 10: 157–160.17. Sav A, Kendall E, McMillan S et al. ‘You say treatment, I say hard work’:treatment burden among people with chronic illnesses and their carers inAustralia. Health Soc Care Community 2013; 21: 665–674.18. Demain S, Gonçalves A, Areia C et al. Living with, managing andminimising treatment burden in long term conditions: a systematic review ofqualitative research. PloS ONE 2015; 10: e0125457 19. Davidoff, F. Weighing the alternatives: lessons from the paradoxes ofalternative medicine. Ann Intern Med 1998; 129: 1068–1070.20. Bates, U. Mindfulness in a palliative-care setting. In: Fraser A (ed). Thehealing power of meditation, 1st edn. Boston: Shambhala Publications, Inc.,2013: 140–158.21. Lee R, Hlubocky F, Stafford R, Daugherty C. An international pilot study ofoncology physicians’ opinions and practices on complementary andalternative medicine (CAM). Integr Cancer Ther 2008; 7: 70–75.22. Mansky P, Wallerstedt D. Complementary Medicine in Palliative Care and Cancer Symptom Management. Cancer J 2006; 12: 425–431.
Copyright © Hayward Medical Communications 2016. All rights reserved. No unauthorised reproduction or distribution. For reprints or permissions, contact [email protected]

C A L L F O R N O M I N A T I O N S
EJPC Palliative Care Policy Development AwardIn 2013, the European Journal of Palliative Care (EJPC), in collaborationwith the European Association for Palliative Care (EAPC), launched the
EJPC Palliative Care Policy Development Award, which is aimed at individuals who have made a substantial contribution to policy development through their research,
clinical practice or as policy activists, in any country or region in the world.
n
Do you know someone who has made a major contribution to palliative care policy development?
n
Do you think they deserve to havetheir contribution recognised?
n
The first three editions of the EJPC Award have been a great success. Now we are asking you to send us your nominations so that we have
a large pool of strong candidates for the fourth edition.
Nominations will be judged by a panel of EJPC Editorial Board members chaired by EJPC Editor Professor Julia Riley.
The winner will be announced at the closing ceremony of the 15th EAPC World Congress in Madrid, Spain (18–20 May 2017).
n
Nominations for the 2017 EJPC Award are open and the deadline for submissions is 19 March 2017. The submission form is available on the EJPC Award
page of the EJPC website: www.ejpc.eu.com/ejpcaward
Copyright © Hayward Medical Communications 2016. All rights reserved. No unauthorised reproduction or distribution. For reprints or permissions, contact [email protected]

This study sought to determine the factorsassociated with antibiotic use in patientsunder the care of HCA Hospice Care (HCA),the largest home hospice service provider inSingapore. Discussion of these factors could beused to highlight deficiencies in practice andencourage improvement in the standard ofcare in antibiotic use for hospice patients atthe end of life.
MethodHCA provides home hospice care to patientswith a life-limiting disease and prognosis ofone year or less. It serves an average of800–850 patients at any one time and hassupported more than 55,500 patients since its inception in 1989.
This is a retrospective electronic case notereview with subsequent descriptive study ofdeceased patients who had been under the
299EUROPEAN JOURNAL OF PALLIATIVE CARE, 2016; 23(6)
www.ejpc.eu.com Clinical management
The prevalence of antibiotic use inpatients receiving palliative careranges from 20% to more than 50%
across different settings.1,2 However, asystematic review of antibiotic use inpalliative care found that the supportingevidence for this treatment is weak.3 First,there have never been direct comparisonsbetween patients who received antibioticsand those who did not. A definitive diagnosisof an infection can also be challenging in thehome setting, where laboratory andradiological investigative options are limited.In addition, the perception of changes insymptoms once antibiotic therapy beginsremains largely subjective; a change inclinical status may be related to othermedications that are administeredconcurrently, or simply due to varyingtrajectories of the underlying disease.
Although the use of antibiotics at the end oflife may alleviate symptoms associated with aurinary tract infection,3 some have arguedthat antibiotics may inappropriately prolonglife for hospice patients and unnecessarilyincrease the burden of treatment. Thedevelopment of antimicrobial resistance isalso a valid concern in hospice care, when fullcourses of antibiotic treatments frequentlycannot be completed as recommended.4
In a study in Singapore, Lo et al concludedthat the use of antibiotics in an inpatienthospice setting had been rational, in caseswhere there were clear indications for startingantibiotics and subsequent symptomimprovement was fairly well documented.5
However, significant patient factors –including functional status, oral intake andcommunication with patient and familyregarding antibiotic use – were not evaluated.
Antibiotic use in the last twoweeks of life for home hospicepatients in SingaporeStudies have indicated that the use of antibiotics in palliative care settings is widespread but lacks
supporting evidence. Ong Eng Koon and Chong poh heng used a retrospective review to assess the
prevalence and standards of practice involved in the use of antibiotics for home hospice patients
n There is a paucity of evidence regarding the benefits ofadministrating antibiotics to patients supported in the homesetting near the end of life. Since antibiotic use is not without itsburdens, we have elected to study decedent demographics andcircumstances of antibiotic use within a home hospice service inSingapore to improve our understanding of prescribing patterns.
n The results of this paper show that antibiotic use in this cohort wasnot common, at 6%, but there were deficiencies in clinical practicein terms of indications and monitoring of antibiotic use.
n Despite initiation of antibiotics at home, 27% of patientseventually died in an acute care hospital.
n It is clear that communication with patients and caregiversregarding antibiotic use at the end of life is important. In addition,future research should compare treatment outcomes and place ofdeath between patients who had antibiotics prescribed at homeand those who did not.
&Ong Eng KoonMBBS MMED (FM)
Registrar1
Chong PohHengMBBS MMED (FM) FAMS
Medical Director2
1 Department ofPalliative Medicine,National CancerCentre, Singapore2 HCA Hospice Care,Singapore
Keypoints
Copyright © Hayward Medical Communications 2016. All rights reserved. No unauthorised reproduction or distribution. For reprints or permissions, contact [email protected]

300 EUROPEAN JOURNAL OF PALLIATIVE CARE, 2016; 23(6)
Clinical management www.ejpc.eu.com
care of HCA. All of the patients who diedwithin the period of January–June 2015 andwere prescribed antibiotics within two weeksof their death were included in the study;patients who were on topical antibiotics were excluded.
All patient visits were documentedelectronically within specific time segments of clinical care. The information on differentaspects of antibiotic use was retrieved from thevarious segments corresponding to the visitwhen antibiotics were prescribed. Thefollowing factors were assessed:l Patient demographics:
– Age– Sex– Functional status in terms of
Eastern CooperativeOncology Group (ECOG)score, mobility and activitiesof daily living (ADL)
– Presence of feeding tube– Volume of oral intake– Primary diagnoses and
cognitive function.l Characteristics of antibiotic usage:
– Source of prescription– Duration of treatment– Type of antibiotic– Site of infection– Effect on symptoms– Reasons for cessation.
l Communication with patient and/orcaregiver, including any documentation of communication regarding theindication, side effects, duration andoutcomes of antibiotic use. Specifically,any request by the caregiver to initiateantibiotics was also noted.
l Place of death.All data collection was performed by the first
author and analysed using Microsoft Excel.
ResultsA total of 1,008 patients died during the studyperiod of six months, of which 63 (6%) haddocumented antibiotic use within two weeksof their death.
DemographicsThe mean age of the patients was 75 years (seeTable 1). There were slightly more men (57%)than women. Most of the patients (97%) hadan ECOG score of 3–4 and 93% required someform of assistance in their daily activities;
although most were not being tube fed, only17% of those who were still eating were takingnormal amounts of food; 84% had cancer, and75% of them were alert.
Antibiotic useAt 43%, the most common site of infectionwas the chest, based on clinical signs andsymptoms (see Table 2). However, 37% ofpatients – a significant proportion – did nothave documentation on the site of infectionas part of clinical assessment, even though allof them had at least one symptom or sign ofsepsis noted, including fever, cough, purulent
sputum or lung crepitationson auscultation.
The attending homehospice team startedantibiotics in more than half – 57% – of cases, and co-amoxiclav was the mostcommonly prescribedantibiotic (71%). The meantime before death that
antibiotics were started was six days. Themean duration of antibiotic use was five days.Antibiotic treatment continued until the timeof death in 70% of patients. Only 21% of thewhole cohort had documented improvementof presenting symptoms.
CommunicationIn 81% of cases there was no documentation ofcommunication with the patient or caregiverregarding the use of antibiotics (see Table 3).Only one (2%) caregiver had requested thatantibiotics be used for a patient.
Place of demiseOf the 63 patients, 44 (70%) died at home, 17 (27%) died in the hospital followingreadmission, despite antibiotic use at home,and two (3%) died in the nursing home wherethey had lived.
DiscussionDemographicsThe prevalence of antibiotic use in this group of patients is much lower than thatpreviously reported in other studies.1, 2 Thismay be due to practice differences betweenthe home hospice and hospital. In the latter,clinical management tends to be moreaggressive due to the availability of a widechoice of parenteral antibiotics.
Some have arguedthat antibiotics mayinappropriatelyprolong life forhospice patients and unnecessarilyincrease the burden of treatment
Copyright © Hayward Medical Communications 2016. All rights reserved. No unauthorised reproduction or distribution. For reprints or permissions, contact [email protected]

301EUROPEAN JOURNAL OF PALLIATIVE CARE, 2016; 23(6)
www.ejpc.eu.com Clinical management
Table 1. patient demographics
Number of patients (%) N=63
a. Age (years)
Range 44–99
Mean 75
Median 76
b. Gender
Male 36 (57)
Female 27 (43)
c. ECOG status
1 —
2 1 (2)
3 23 (37)
4 38 (60)
Not documented 1 (2)
d. Mobility
Independent —
Supervised 4 (6)
Assisted 10 (16)
Chairbound 7 (11)
Bedbound 41 (65)
Not documented 1 (2)
e. Activities of daily living
Independent 2 (3)
Supervised 1 (2)
Assisted 21 (33)
Dependent 38 (60)
Not documented 1 (2)
f. Oral intake
Poor 18 (29)
Moderate 24 (38)
Normal 11 (17)
Tube feeding 8 (13)
Not documented 2 (3)
g. Primary Diagnoses
Cancer 53 (84)
Non-cancer 10 (16)
h. Cognitive function
Unresponsive 2 (3)
Drowsy 9 (14)
Confused 3 (5)
Alert 47 (75)
Not documented 2 (3)
Table 2. Characteristics of antibiotic use
Number of patients (%) N=63
a. Site of infection
Chest 27 (43)
Urinary tract 7 (11)
Sacral sore 2 (3)
Soft tissue 3 (5)
Hepatobiliary tract 1 (2)
Not documented 23 (37)
b. Choice of antibiotics
Co-amoxiclav 45 (71)
Ciprofloxacin 12 (19)
Clarithromycin 2 (3)
Levofloxacin 2 (3)
Metronidazole 2 (3)
c. Prescribing source
Home hospice 36 (57)
Hospital 17 (27)
General practitioner 1 (2)
Not documented 9 (14)
d. Time of antibiotic use before death (days)
Range 1–14
Mean 6
Median 6
e. Duration of antibiotic use (days)
Range 1–14
Mean 5
Median 5
f. Reason for cessation of antibiotics
Course completion 5 (8)
Deterioratingcondition 12 (19)
Readmitted tohospital 1 (2)
Death 44 (70)
Not documented 1 (2)
g. Change in infective symptoms
Improved 13 (21)
Worsened 3 (5)
No change 1 (2)
Not documented 46 (73)
Copyright © Hayward Medical Communications 2016. All rights reserved. No unauthorised reproduction or distribution. For reprints or permissions, contact [email protected]

� In the context of the growingrecognition of the emotionaland psychological needs ofpatients and carers at the end oflife, Jenny Strachan introduces‘Psychology in palliativepractice’, a new series for 2017and beyond. The seriestranslates some of psychology’s‘big ideas’ into practical advice,and Jenny begins with a look atattachment theory, in which sheexamines both the theory andhow knowledge of it promotespsychologically informedpractice for all members of themultidisciplinary team.
� In this issue’s ‘European insight’section, Wei liu and ping guoplace palliative care in China in its global, historical,geographical and culturalcontexts. They investigate thechallenges faced by thoseseeking to implement palliativecare in China and, looking to thefuture, ask, ‘Can a good death beachieved for Chinese patientswith advanced illness?’
� Tuberculosis remains a worldwideproblem that mainly affectspeople in Africa and Asia but alsooccurs in developed nations.Fiona runacres and colleaguesin Australia assess the clinicalguidance available for providingappropriate care to patients withTB at the end of life.
� Intriguingly, a hospice inManchester has found that theyare bucking the national trendregarding the average length ofstay in a hospice, theirs beingshorter. A far higher proportionof their patients die in thehospice. Carmen Chan andMichael Tapley explain how aHospice Transfer Projectbetween the hospice and thelocal hospital enables manymore patients who will dieimminently to benefit from the care given in the hospice.
� Edith ubogagu provides anupdate on symptom control inthose patients receiving palliativecare who experience nausea andvomiting, in which she reviewsthe literature on variouspharmacological interventions.
� In a paper produced by theTaskforce on Palliative Care for People with Heart Diseasejointly set up by the EuropeanAssociation for Palliative Care and the Heart FailureAssociation of the EuropeanSociety of Cardiology, ManuelMartínez-Sélles et alexamine the complexities ofproviding palliative care topatients with advanced heartfailure and the importance oftimely intervention.
� Earlier this year, the RoyalLiverpool and BroadgreenUniversity Hospitals NHS Trustopened a state-of-the-artacademic palliative care unit. Its aims are to provide specialistcare for patients with the mostcomplex, high-dependencypalliative and end-of-life careneeds and, once these needs havebeen addressed, to dischargepatients to the most appropriateplace of care, such as home orhospice, in line with their needsand wishes. A key benefit is areduced length of stay in hospital.Ben O’Brien and colleaguesexplain the immense benefits thata custom-designed unit can bringto patients and their families – and consequently to staff as well.
All future copy may alter at the publisher’s discretion.
If you are not already a subscriber to thejournal, why not ensure that you receive your copy of the next issue by setting up your order online? See page 264 for detailsof subscription rates or go straight to ourwebsite (www.ejpc.eu.com).
In the next issue …
EUROPEAN JOURNAL OF PALLIATIVE CARE, 2016; 23(6)
www.ejpc.eu.com
Although patients in this study who werestarted on antibiotics were mostly alert, their functional status was poor. Togetherwith findings that they were also less likely to have adequate oral intake, prognosis for these patients is poor, based on severalprognostic tools.6,7
However, antibiotics can improvesymptoms related to infections, even at theend of life,3,8 and it is worth noting that themajority of these patients (75%) were also stillalert at the point of assessment. It is not sosurprising that antibiotics were initiated, eventhough the prognosis was short.
The assessment before starting antibiotics in this special group of patients with limited prognosis would need additionalpredictive factors on top of those obtained by the use of general prognostic toolscommonly used for hospice patients in order to validate the use of antibiotics. Thesefactors would help to assess the reversibility of acute episodes of infection. Such factorscould include assessment of: previousepisodes of similar infections; previousantibiotic use; and disease-specific conditions such as anatomical disruptions,compromised immunity and poor bodily reserves.
Characteristics of antibiotic useA significant proportion of patients (37%) hadno documented diagnosis regarding the site ofinfection. This is consistent with previousstudies, in which the proportion of patientswho were administered antibiotics and hadactually had a documented diagnosis ofinfection was as low as 15%.2,9
Chest infections were the most commontype of infection noted, lung malignanciesbeing one of three most frequently diagnosedcancers locally.10 Associated respiratorysymptoms from cancer, such as cough ordyspnoea, are common and could overlapwith those expected in chest infections,possibly explaining the high figures found inthis study.
Initiation of antibiotic use was noted to be as close as one day before death (mean of six days) and was commonly continued upto the patient’s death. However, there was a lack of documentation regardingimprovement in symptoms or difficulty in medication administration followingantibiotic initiation. It was not possible
Copyright © Hayward Medical Communications 2016. All rights reserved. No unauthorised reproduction or distribution. For reprints or permissions, contact [email protected]

303EUROPEAN JOURNAL OF PALLIATIVE CARE, 2016; 23(6)
www.ejpc.eu.com Clinical management
to ascertain if this was due to suboptimaldocumentation or failure to review symptomsonce antibiotics had started. Withoutdemonstrating any benefit, it would not bejustified to impose this additional burden oftreatment on both the patient (who is likelyto have developed swallowing difficulties bythis time) and their caregivers. Thus,assessment and documentation of treatmentoutcomes need to be improved.
CommunicationThe lack of communication regarding the useof antibiotics is a cause for concern. As most ofthe patients were noted to be alert, theopportunity to explore goals of care and carepreferences should not be missed.
Future studies should determine thosefactors that foster or hinder communicationbetween the physician and patients orcaregivers, as part of ethical practice.
Interestingly, only one caregiver had askedfor antibiotics to be started, suggesting thatthe decision to start antibiotics was nearlyalways medically guided.
Place of deathIt has been noted that patients generally prefer to die at home.11 However, a significantproportion of patients (27%) were readmittedto an acute care hospital despite priorinitiation of antibiotics at home. Futureresearch on treatment outcomes followinghospital readmission and the effect ofantibiotics on symptom control and mortality can provide further insight into the benefit of aggressive antibiotic treatmentand escalation of care in this group of patients. Further details, including theduration of oral antibiotic use, change in the patient’s condition and any caregiverstress that may contribute to subsequenthospital readmission, will also provide insight about whether initial treatment athome was warranted and advisable.
LimitationsThe number of patients assessed was relatively small and the factors assessed were based purely on the retrospective review of documented electronic case notes.Communication was also noted to be poor.
However, these results show the prevalenceof antibiotic use at the end of life for homehospice patients. In addition, they illustrate
the lack of documented indications ofantibiotic use and of subsequent monitoring.
Finally, a significant proportion of patientseventually sought treatment in a hospital,raising questions about whether the place ofcare would have been different without theuse of antibiotics at home.
ConclusionThis study demonstrates deficiencies in good clinical practice regarding antibiotic use at the end of life for home hospicepatients. It provides insight into prescribingpatterns and should encourage furtherresearch into the differences in outcomesbetween initiating and withholding antibioticuse in this group of patients.
Declaration of interestThe authors declare that there is no conflict of interest.
References1. Oneschuk D, Fainsinger R, Demoissac D. Antibiotic use in the last week of life in three different palliative care settings. J Palliat Care 2002; 18: 25–8.2. Albrecht JS, Mcgregor JC, Fromme EK et al. A nationwide analysis ofantibiotic use in hospice care in the final week of life. J Pain Symptom Manage 2013; 46: 483–490.3. Rosenberg JH, Albrecht JS, Fromme EK et al. Antimicrobial use forsymptom management in patients receiving hospice and palliative care: a systematic review. J Palliat Med 2013; 16: 1568–1574.4. Levin PD, Simor AE, Moses AE et al. End-of-life treatment and bacterialantibiotic resistance: a potential association. Chest 2010; 138: 588 –594.5. Lo TJ, Wu HY, Ong WY et al. An audit on antibiotic use at the end of life ininpatient hospice patients – Are we contributing to over-medicalization ofdying? Prog Palliat Care 2015; 23: 220–223.6. Glare P, Virik K. Independent validation of palliative prognostic score interminally ill patients referred to a hospital-based palliative medicineconsultation service. J Pain Symp Manage 2001; 22: 891–898.7. Maltoni M, Nanni O, Pirovano M et al. Successful validation of the palliativeprognostic score in terminally ill cancer patients. J Pain Symp Manage 1999;17: 240–247.8. Nakagawa S, Toya Y, Okamoto Y et al. Can anti-infective drugs improve theinfection-related symptoms of patients with cancer during the terminalstages of their lives? J Palliat Med 2010; 13: 535–540.9. Chun ED, Rodgers PE, Vitale CA et al. Antimicrobial use among patientsreceiving palliative care consultation. Am J Hosp Palliat Care 2010; 27:261–265.10. National Registry of Diseases Office. Singapore Cancer Registry, InterimAnnual Report, Trends in Cancer Incidence in Singapore, 2010–2014.Singapore: NRDO, 2015. www.nrdo.gov.sg/docs/librariesprovider3/default-document-library/cancer-trends-2010-2014_interim-annual-report_final-(public)-updated-23-oct.pdf?sfvrsn=0 (last accessed 11/09/16)11. Lien Foundation. Death Attitudes Survey. Singapore: Lien Foundation, 2014.www.lienfoundation.org/sites/default/files/Death%20survey%20Presser%20Final%20-%20Combined_0.pdf (last accessed 11/09/16)
Table 3. Communication with patient/caregiver regardingantibiotic use
Number of patients (%) N=63
a. Documented conversation regarding antibiotic use
Yes 12 (19)
No 51 (81)
b. Documentation of caregiver’s request for antibiotic
Yes 1 (2)
Not documented 62 (98)
Copyright © Hayward Medical Communications 2016. All rights reserved. No unauthorised reproduction or distribution. For reprints or permissions, contact [email protected]

304 EUROPEAN JOURNAL OF PALLIATIVE CARE, 2016; 23(6)
Reader sur vey www.ejpc.eu.com
SReadersurveyresults
Respondentscame from across themultidisciplinary team
38%Palliative care physicians15%Nurses6%
Oncologists6%
Psychologists
82% 53% 43% 78%
find the EJPCextremely/very useful
use it as areferenceresource
use it to aidtheir own or
others’ training
find the EJPCof great benefit; theremainder regard itas of some benefit
94% 71% 90%
agree/stronglyagree that they find the EJPCinformative
agree/stronglyagree that the EJPCinfluences theirpatient care
agree/stronglyagree that they trustthe information theyread in the EJPC
T H E J O U R N A L O F T H E E U R O P E A N A S S O C I A T I O N F O R P A L L I A T I V E C A R E
European Journal of
Palliative Care COMMENT
265 Love your data
Ros Taylor
CLINICAL MANAGEMENT
266 Managing malignant bowel obstruction
with lanreotide in the community
Kate Markham, Shan Shan Vijeratnam and Pia Amsler
SPONSORED ARTICLE CLINICAL MANAGEMENT
270 Treating cancer pain
Andrew Dickman
MULTIDISCIPLINARY TEAM
278 Paediatric palliative nursing: the tension
between closeness and professional distance
Regula Buder and Andre Fringer
PERSPECTIVE
282 The convenient death of King George V:
a look back at history
Sandy Macleod and Jane Vella-Brincat
PERSPECTIVE
285 The Sydney Institute of Palliative Medicine:
evolution and contribution
Ghauri Aggarwal, Jan Maree Davis, Frank Brennan
and Kristen Turner
RESEARCH
290 Does current UK research address priorities
in palliative and end-of-life care?
Florence Todd Fordham, Bridget Candy, Stevie McMillan
and Sabine Best
HOLISTIC CARE
294 Mindfulness meditation and pain
management in palliative care
Irene Campagnolo Maschio
CLINICAL MANAGEMENT
299 Antibiotic use in the last two weeks of life
for home hospice patients in Singapore
Ong Eng Koon and Chong Poh Heng
RESEARCH
305 EAPC Early Researcher Award 2013 –
looking back
Meera Agar, Barbara Gomes and Jeroen Hasselaar
EUROPEAN INSIGHT
309 Romanian National Association for
Palliative Care: quality assurance for
palliative care in Romania
Malina Dumitrescu and Vladimir Poroch
November/December 2016, Volume 23 Number 6www.ejpc.eu.com
Visitwww.ejpc.eu.comto read the current issue online or to access the EJPC archive
Book review
��A Practical Guide to End of Life CareCarmel Grealish
page281
Case 89 Managing symptoms of
neuroendocrine tumours in a 62-year-
old man with impaired cognition
Andrew Gill
page276
The case study masterclass
Copyright © Hayward Medical Communications 2016. All rights reserved. No unauthorised reproduction or distribution. For reprints or permissions, contact [email protected]

�Meera Agar:‘The EAPC award hasgiven me a deeperappreciation of how tobetter foster in others theenthusiasm and driveneeded to undertakegroundbreaking research’
305EUROPEAN JOURNAL OF PALLIATIVE CARE, 2016; 23(6)
Receiving the Early Researcher Award in2013 was a huge honour and privilege that
marked 10 years as a clinician scientist trying toimprove care for people with delirium at the endof life. The plenary presentation in Pragueremains a defining moment in my career andhighlighted that expert EAPC researcherssupport the fundamental importance ofevidence-based delirium care. This spirit ofacknowledgement comes with a recognition thatthe research community walks alongside us tosupport our success.
Three years on, I am the Professor of PalliativeMedicine, University of Technology Sydney, anexciting new position in an interdisciplinary centrethat aims to improve quality of life for people withchronic illness requiring palliative care, with astrong focus on equity, diversity and social justice.My research focus is on supportive care needs
www.ejpc.eu.com Researc h
EAPC Early Researcher Award2013 – looking backSince 2009, through its Early Researcher Award, the European Association for Palliative Care (EAPC) has
recognised and supported the work of scientists and clinicians who make an outstanding contribution
to palliative care research. Here, Meera Agar, Barbara Gomes and Jeroen Hasselaar reflect on the path their
careers have taken since they won the award in 2013
First prizeCollaboration and mentorshipMeera Agar, Professor of Palliative Medicine, Centre for Cardiovascular and Chronic Care, Faculty of Health,University of Technology Sydney, Sydney, Australia
R
relating to the impacts of advanced illness on thebrain, an area in which I have now completedthree clinical trials.
I particularly enjoy my roles with various nationaltrials groups, including Improving Palliative Carethrough Clinical Trials (ImPaCCT) – the New SouthWales (NSW) palliative care clinical trials group –the Palliative Care Clinical Studies Collaborative(PaCCSC), the Cooperative Trials Group for Neuro-Oncology (COGNO), the Psycho-oncologyCo-operative Research Group (PoCoG) and theCognitive Decline Partnership Centre (CDPC). In theareas of advocacy and policy I am also involvedwith National Palliative Care Standards, theAustralasian Delirium Association (ADA), theEuropean Delirium Association (EDA) and ChoosingWisely Australia. I have fostered collaborations tosupport our colleagues in Asia Pacific – for examplethe Lien Collaborative for Palliative Care inMyanmar – as they drive the agenda to improvepalliative care access and services.
Moving to an academic position has alsoallowed me to have a more substantial role inmentoring and capacity building, and the nextgeneration of researchers in palliative care havemuch to offer. Most importantly, I have been ableto support higher degree research students in atruly interdisciplinary academic environment thatneeds to be the norm for the future. The EAPCaward has given me a deeper appreciation of howto better foster in others the enthusiasm and driveneeded to undertake groundbreaking researchthat will help ensure people who have faradvanced illness receive the best care possible, sothat they can focus on living their lives to the full.The best evidence is needed to guide themanagement of their symptoms or theconfiguration of their healthcare, as for mostpatients we have just one chance to get it right. Iam also passionate about ensuring women inacademic roles have the flexibility and support toachieve to their full potential. This is an area I have
Copyright © Hayward Medical Communications 2016. All rights reserved. No unauthorised reproduction or distribution. For reprints or permissions, contact [email protected]

fter 10 years of research and training inpalliative care in the UK, I was honoured to
be one of the Early Research Award winners in2013. This ended up being a major life turningpoint, leading to my homeland return and theaward in 2016 of the first professorship inpalliative care in Portugal, hosted at the Facultyof Medicine of the University of Coimbra.
New and exciting times lie ahead, building onseeds that grew at the Cicely Saunders Institute,
306 EUROPEAN JOURNAL OF PALLIATIVE CARE, 2016; 23(6)
been able to foster more active discussion about, in the palliative care research community inparticular, as the last three years also included aperiod of maternity leave. I am also pleased that my son’s first words weren’t ‘randomised controlled trial’ !
As I reflect on my career since 2013, success isstill defined by my mentors and collaborators fromall walks of life and by being truly interdisciplinaryin spirit and intent, all of which offer support andboost the drive and resilience you need to be thebest you can be, regardless of the challenges. It wasthe questions, ‘What would be the best carepossible for this person?’ and ‘Is there a way we cando this better?’ that became the driver of myclinical care and research questions and led to thework that culminated in the Early ResearcherAward in 2013, and they continue to drive myapproach to this day �
Researc h www.ejpc.eu.com
A
under Professor Irene Higginson’s ‘gardener’s eye’.For the last few years, I have been leading aresearch project (the DINAMO Project) that hashelped energise advanced training and optimisehome palliative care in Portugal, and in that timethe project has come a long way. We trained a teamof eight promising medical doctors andresearchers, who became masters in palliative careat King’s College, London, and are now making adifference to the integration of palliative care intothe daily practice of family medicine, internalmedicine, oncology and paediatrics. Together, weundertook studies that showed the level of needand the impact of palliative care in the homecontext and at an important clinical service in theinterface of hospital and community – theemergency department. Results from other studieswill be forthcoming soon.
One great achievement was to inform the policyU-turn towards prioritising the development ofhome palliative care – this is at the heart of a newPortuguese national palliative care strategy,published in November 2016. The strategy aims toat least triple the number of home palliative careteams by 2018, which means that a lot morepeople will have access to an alternative toinstitutional care and will be able to die at home,if that is their wish, benefiting from specialist homesupport. We look forward to the next two years,during which changes will be implemented, andhope that these help reverse the country’s upwardhospital death trend.
I spent the last year conducting interviews with patients and family caregivers in Portugal for a new study to determine which attributes ofhome palliative care are most valued by serviceusers. This gave me invaluable insight on howservices operate in urban and rural regions andhow patients and families view them. We areapplying an original technique from healtheconomics called the discrete choice experiment,which is helping us quantify the value that peoplegive to different attributes related to home visits,family support, information and planning, andteam availability. Preliminary findings werepresented at the 9th World Research Congress ofthe EAPC in Dublin, 2016.
In September 2016, I was awarded aProfessorship in Palliative Care at the Faculty ofMedicine of the university of Coimbra. Coimbra isone of the oldest niversities in Europe and is in the500 top universities of the world. It is a front runnerin health science and education and integratespalliative care into the curriculum for the 280medical students who enroll each year. There is also
�Barbara Gomes:‘We trained eightpromising doctors andresearchers, who arenow making adifference to the dailypractice of familymedicine, internalmedicine, oncologyand paediatrics’
Joint second prizeOne of life’s turning pointsBarbara Gomes, Invited Assistant Professor at University of Coimbra, Faculty of Medicine; Research Fellow at CicelySaunders Institute, King’s College London, UK
Copyright © Hayward Medical Communications 2016. All rights reserved. No unauthorised reproduction or distribution. For reprints or permissions, contact [email protected]

� Jeroen Hasselaar:‘For a long time, theEAPC was quite anunknown world for me, but this changedafter I received the Early Researcher Award, and also after workingwith so manyinternational colleaguesover the years’
t EAPC Prague 2013, I received the EarlyResearcher Award (second prize). I have
good memories of that moment – being almosttwo metres tall and gently bowing to receive theprize from the hands of Professor Sheila Payne.
The Prague congress was also a turning pointfrom another perspective. After a period of hardwork seeking support for a national programme forpalliative care in the Netherlands, I was worriedthat we would lose momentum. In Prague Iorganised a meeting with some influential Dutch
307EUROPEAN JOURNAL OF PALLIATIVE CARE, 2016; 23(6)
a successful masters course in Continuing andPalliative Care, co-ordinated by Professor MaríliaDourado since 2013. I am honoured to hold theprofessorship and to have the means to furthergrow palliative care training at Coimbra and leadthe development of a new European researchcentre of excellence in the field.
These achievements would not have beenpossible without the contributions of the patientsand families who took part in our studies, thesupport of the Calouste Gulbenkian Foundation,which funds the DINAMO Project and theprofessorship, the mentorship of Professor IreneHigginson, the contributions of my clinical andacademic colleagues, and the encouragement ofmy family and friends �
www.ejpc.eu.com Researc h
A
palliative care colleagues and we decided to makeone more push. We were soon invited into theupper echelons of the Dutch Health Ministry andthe Netherlands organisation for health researchand development (ZonMw), and I was asked topropose a national programme for palliative care. The proposal resulted in the Dutch Parliamentapproving funding of 51 million euros for a nationalprogramme, which is underway and beingimplemented until 2020. It is so good to seepalliative care growing as a field in the Netherlands,because much work remains to be done.
Late in 2012, we received a grant from the EU foran international project on best practices inintegrated palliative care (www.insup-c.eu), ofwhich I am co-ordinator. Imagine sitting at yourcomputer and receiving an email from the EUstating in a few sentences that your proposal isawarded – I could hardly believe it! In January 2013we had the startup meeting in Amsterdam, with acollaboration of 11 partners, including the WHOand EAPC. This year, the project will come to an endwith a congress in Brussels and a freedownloadable book on integrated palliative care.Co-ordinating such a big project is not always easy,but we have a wonderful and skilled group ofpeople. Last year, I was invited to the ESMOcongress in Vienna to talk about our project. I wasalso appointed as an external collaborator at theUniversity of Navarra, Spain. And with Sheila Payne,I was invited to co-edit a special edition of PalliativeMedicine on integrated care.
Just before InsupC started up, I travelled toNigeria with one of my PhD students for atelemedicine and palliative care project. It was agreat experience, assimilating a different culture,working with Professor Soyannwo’s team andco-writing a publication. More PhDs are coming up,on subjects such as ehealth and palliative care,integrated palliative care and palliative sedation –the latter was the subject of my own PhD thesis in2010, and I have an ongoing interest in its clinicaland ethical aspects.
Looking back, I attended my first EAPC congressin 2005. For a long time, the EAPC was quite anunknown world for me, but this changed after Ireceived the Early Researcher Award, and also afterworking with so many international colleaguesover the years. I work in a great team led byProfessor Kris Vissers at the Radboud ExpertiseCenter of Pain and Palliative Medicine, RadboudUniversity Medical School, and I look forward toexploring the world further. I hope that the EAPCwill continue to encourage young researchers and clinicians �
Joint second prizeBuilding programmes …Jeroen Hasselaar, Assistant Professor in Palliative Care, Radboud University Medical Center, Nijmegen, The Netherlands
Copyright © Hayward Medical Communications 2016. All rights reserved. No unauthorised reproduction or distribution. For reprints or permissions, contact [email protected]

How do NETs present?NETs are rare in oncology practice, soexposure to symptom management inpalliative care is limited. The symptomsthat need to be controlled tend to be thesame as at disease presentation. Non-functioning NETs usually present withlocal tumour effects, such as pain, nauseaand vomiting or anaemia or symptomsassociated with metastasis.1 Ramage et al1
summarised the symptoms of functioningNETs according to which peptidehormone is released (see Table 1). Thesymptoms are secondary to vasoactivecompounds generally secreted by livermetastases, such as adrenocorticotropichormone, kallikrein, gastrin, histamine,serotonin (5-hydroxytryptamine),prostaglandins and calcitonin.1
What is the cause of pellagra, andwhat are the treatment options?Pellagra is caused by a lack of vitamin B3(niacin) or its precursor tryptophan.Deficiency of vitamin B3 affects thecellular functions in multiple organs andtissue and can cause diarrhoea, dermatitis
and mental disturbance. While pellagramay be a primary disease due to poordietary intake of vitamin B3, it may also besecondary to conditions that affect niacinintake, absorption or metabolism.2 Incarcinoid syndrome, it is the result ofexcess consumption of dietary tryptophanby the serotonin-producing tumour.2 Themainstay of pellagra treatment isimproved overall nutrition with a high-protein diet and vitamin B complexsupplementation.2
What is the pathophysiology of carcinoid heart disease?The pathophysiology of carcinoid heartdisease is unclear. Vasoactive substanceswith fibroblast proliferative propertiesare released by the tumour at a greaterquantity than the liver can excrete.3
These lead to the formation ofendocardial plaques, mainly on the rightside of the heart on the downstream sideof the tricuspid and pulmonary valves,causing a mixture of valvular stenosisand regurgitation. Serotonin is thoughtto be the substance that plays a majorrole in fibrogenesis in the heart, andpatients with carcinoid heart diseasetend to have higher levels of urine5-HIAA, the serotonin metabolite.3
What is the Mental Capacity Act, and what help can beprovided to aid decision-making?The Mental Capacity Act (MCA) 2005 4
was designed to protect and restorepower to vulnerable people aged 16 andover who lack capacity and live inEngland and Wales. It also supports thosewho do have capacity and choose to planfor their future. Five statutory principlesunderpin all acts carried out, anddecisions taken, in relation to the act: 4
l a presumption that everyone hascapacity unless proved otherwise
l a person must be given all practicablehelp before anyone treats them as not
being able to make their own decisionsl people have the right to make decisions
that others may judge as unwisel anything done on behalf of a person
who lacks capacity must be in theirbest interest
l any decision made must interfere theleast with a person’s rights andfreedoms of action.
A two-stage test determines anindividual’s decision-making capacity: 4
l Is there an impairment of ordisturbance in the functioning of aperson’s mind or brain?
l If so, is the impairment or disturbancesufficient that the person lacks thecapacity to make a particular decision?
The MCA says that you are unable tomake your own decision if you cannot doone or more of the following four things:l understand information given to youl retain that information long enough to
be able to make the decisionl weigh up the information available to
make the decisionl communicate your decision.In Brian’s case, there were times when helacked capacity, but with the support ofhis wife, the use of time and simplificationof verbal communication, he did havecapacity at crucial times, and as such wasable to make decisions regarding his owntreatment. When supporting a person inmaking a decision, it is prudent to thinkabout language, form of communication,location of discussion, who may be ofhelp, such as a carer or advocate, and thetiming of any decision �
Declaration of interestThe author declares that there is no conflict of interest.
References1. Ramage JK, Ahmed A, Ardill J et al. Guidelines for themanagement of gastroenteropancreatic neuroendocrine(including carcinoid) tumours (NETs). Gut. 2012; 61: 6–32.2. Shah GM, Shah RG, Veilette H et al. Biochemical assessment ofniacin deficiency among carcinoid cancer patients. Am JGastroenterol. 2005; 100: 2307–2314.3. Grozinsky-Glasberg S, Grossman AB, Gross DJ. Carcinoid heartdisease: From pathophysiology to treatment - ‘Something in theway it moves’. Neuroendocrinology. 2015; 101: 263–273.4. Social Care Institute for Excellence. Mental Capacity Act (MCA)Resource. Available from:www.scie.org.uk/publications/ataglance/ataglance05.asp (lastaccessed 05/09/16)
Case 89 answers Managing symptomsof neuroendocrine tumours in a 62-year-old man with impaired cognition
The case studymasterclass www.ejpc.eu.com
EUROPEAN JOURNAL OF PALLIATIVE CARE, 2016; 23(6)308
››Read …this patient’s full case history in the ‘masterclass’ section onpages 276–277 of this issue.
Table 1. Symptoms offunctioning NETs1
Tumour Symptoms
InsulinomaConfusion, sweating, dizziness,weakness, unconsciousness,relief with eating
GastrinomaZollinger-Ellison syndrome of severe peptic ulceration,diarrhoea
GlucagonomaWeight loss, diabetes mellitus,stomatitis, diarrhoea, necrolyticmigratory erythema
vIPomaverner-Morrison syndrome orprofuse watery diarrhoea withmarked hypokalaemia
SomatostatinomaWeight loss, diarrhoea,steatorrhoea, diabetes mellitus, cholelithiasis
Copyright © Hayward Medical Communications 2016. All rights reserved. No unauthorised reproduction or distribution. For reprints or permissions, contact [email protected]

MălinaDumitrescuandVladimirPorochRomanianNationalAssociationfor PalliativeCare
309EUROPEAN JOURNAL OF PALLIATIVE CARE, 2016; 23(6)
Romanian National Associationfor Palliative Care: qualityassurance for palliative care in Romania
In this section, European and international palliative care organisations areinvited to explain their goals, express their hopes and voice their concerns
The Romanian National Association for Palliative Care has proposed a new methodology for the
accreditation of palliative care services in the country
EUROPEAN insight
W ith a geographical area of almost240 million sq km, Romania ranks as the
ninth largest country in the EU and is the seventhlargest by population, with just under 20 millioninhabitants. With a negative birth rate, highmortality and an increasingly migratory workforce,Romania’s population decreased by 7.2% between2002 and 2011, while the proportion of peopleaged over 75 increased from 4.9% to 7.2% duringthe same period.1
In Romania, causes of death roughly follow thetypical pattern prevalent in the EU, and diseases ofthe circulatory system and cancer are by far theleading causes of mortality. Cardiovasculardiseases currently account for 1,293 deaths per100,000 inhabitants, while cancer is the secondmajor cause of death, averaging 270 deaths per100,000 inhabitants.2 The ageing trend of thepopulation gradually shifts the disease patterntowards chronic progressive diseases, with peoplerequiring long-term and palliative careinterventions integrated into the generalhealthcare system.
The palliative care seedPalliative care started in Romania as early as 1992,when the Hospice Casa Sperantei Foundation wasset up in the city of Brasov as a non-governmentalcharity, a UK-Romanian hospice partnershipinitiated by Graham Perolls from the UK. Theorganisation assumed the mission to introduce
and develop palliative care in Romania. Thebeginnings were focused on providing home-based palliative care for adult cancer patientsfollowing their discharge from the oncologyhospital. In 1996, the Brasov hospice team wasextended, reaching out to children with cancerand life-limiting conditions and providingpalliative care in children’s homes, in closeco-operation with the Brasov Paediatric Hospital.
A decade later, Hospice Casa Sperantei – the firstRomanian centre for palliative care services andeducation – was built in Brasov. The hospice hosts a13-bed adult inpatient unit for cancer patients and apaediatric inpatient unit with six beds for childrenwith a range of life-limiting diseases. It is now one ofthe largest non-governmental organisations inRomania, with over 260 employees and 350volunteers, and provides services for 2,500 newpatients each year in Bucharest and the county ofBrasov. It has been actively involved in developingservices and national and international educationprogrammes in the palliative care field, and in theadvancement and integration of palliative care intothe Romanian healthcare system. In 2003, HospiceCasa Sperantei was nominated by the Open SocietyFoundations (OSF), formerly the Open SocietyInstitute, as one of five beacons of excellence in SE Europe (along with hospices in Budapest, Poznan,St Petersburg and Warsaw) in an exhaustive study ofend-of-life care, carried out among 475 services in28 countries in Eastern Europe and Central Asia.3
Copyright © Hayward Medical Communications 2016. All rights reserved. No unauthorised reproduction or distribution. For reprints or permissions, contact [email protected]

310 EUROPEAN JOURNAL OF PALLIATIVE CARE, 2016; 23(6)
The National Association of Palliative CareIn 1997, a group of enthusiastic professionals led byDr Daniela Mosoiu founded the National Associationof Palliative Care (ANIP). The association is open toany professionals working in palliative care servicesor interested in this field.
Several regulations specific to palliative care were advanced by ANIP and boosted thedevelopment of new services over the last decade: a new law for pain control medication(2005); 4 financing mechanisms 5 for inpatient unitsby fee per admission day (since 2007) and for home-based palliative care by fee per visit (since 2010),through the national health insurance system; andthe establishment of minimum staffing ratios forpalliative care inpatient units (2010). ANIP alsopublishes a palliative care services directory everysecond year.
ANIP members have been actively involved inseveral pilot projects (see Box 1) concerned withservices development and national educationprogrammes for palliative care professionals, as wellas in legal initiatives in support of the new field.
Standards for palliative care servicesAlong with support for the quantitative extension ofservices throughout the country and the appropriateeducation of palliative care professionals at pre- andpost-graduate level, ANIP had a significant input inelaborating national standards for palliative careservices in various settings.
In 2002, ANIP initiated a consultation process with groups of various specialists in palliative care,including physicians, nurses, social workers,psychologists and services administrators, in anattempt to develop minimum standards forpalliative care services in Romania. These first
standards were developed with the support of theNational Hospice and Palliative Care Organization(NHPCO) in the USA. The standards were conceivedas a set of criteria to be met by any potentialpalliative care service, and also to help health andfunding authorities evaluate existing and emergingservices. The standards were reviewed andupgraded for inpatient units, outpatient clinics andhome-based services in a similar process in 2010.
20 years of palliative careservices developmentSince 1992, new palliative care services have been setup in both the public and private healthcare systems.The current legal framework and the fundingmechanisms have been gradually encouraging theemergence of new palliative care services, particularlyas inpatient units. Home-based palliative care servicesare still isolated private initiatives, and their fundingthrough the health insurances system is low, despitethe fact that 70% of people die at home in Romaniaand most of them wish to be looked after in theirhome environment at the end of life.
The map of specialised palliative care services, as illustrated in the last service directory publishedin 2014 12 by ANIP, shows 79 services delivered by47 providers – 20 in the public healthcare system,23 non-governmental charitable organisations and4 for-profit services. It has been estimated thatmore than 150,000 people annually need palliativecare in Romania, using an international estimationmethodology 13 based on epidemiological criteria.Comparing the esimated needs for palliative careservices for oncological and non-oncologicalpatients to the actual services available, Romaniahad 7.9% needs coverage in 2015. The distributionof services was rather inconsistent, with 19counties out of 41 still having no palliative careproviders. The slow and random development ofservices is due to the fact that palliative care hasonly recently been included in the nationalhealthcare strategy,14 with an ambitious strategicobjective of reaching 60% coverage of the overallneeds for palliative care by 2020.
A national strategy for palliative care In support of the 60% coverage objective, ANIPdeveloped, in partnership with the Ministry ofHealth, a proposal for a national palliative carestrategy, in a joint consultation process with palliativecare services professionals and internationalhealthcare consultants. The proposed strategy wasbased on the existing resources available and on agradual and consistent development of services in all
EUROPEAN insight… www.ejpc.eu.com
Box 1. National Association of Palliative Care pilot projects
� Integration of palliative care in the medical treatment of advancedmalignancies for the benefit of patients and for increasing quality ofmedical care in various healthcare institutions.6
� Overcoming disparities in access to quality basic palliative care in thecommunity: partnerships to identify and improve clinical, educational,legal and economical barriers.7
� Creating a national evaluation system for palliative care servicestargeting vulnerable populations.8
� Developing a new pathway for management of palliative carepatients with advanced cancer in Iaşi county.9
� Physicians’ education for pain in NE Romania – PEPNER.10
� Open online courses with videos for the palliative clinical field andintercultural and multilingual medical communication – MedLang.11
Copyright © Hayward Medical Communications 2016. All rights reserved. No unauthorised reproduction or distribution. For reprints or permissions, contact [email protected]

311EUROPEAN JOURNAL OF PALLIATIVE CARE, 2016; 23(6)
the 41 counties of Romania, and encompassed threedistinct types of service: l patients’ self-care educationl basic palliative care provided by family doctors
in the community for patients with cancer andother progressive illnesses who have non-complex conditions
l specialist pallative care services for patients with complex, chronic progressive diseases and co-morbidities. The principle of the strategy is to ensure patients’
access to services at geographical levels: for relativelyuncomplicated cases – basic palliative care services atlocal level, as close as possible to their home location;for cases with complex needs – specialised palliativecare services at regional/county level. The nationallevel is devoted to education of staff, research andraising awareness of palliative care. The principles of the national strategy were included in the recentHealth Sector Reform supported by a World Bankloan15 between 2014 and 2020. The project willsupport an equitable development of palliative careservices throughout all counties, with 29 inpatientunits in areas without coverage, 90 home care teamsand 90 outpatient clinics.
Quantity and quality inpalliative care services deliveryToday, ANIP envisages a new stage in thedevelopment of palliative care in Romania.Following the slow and steady quantitativedevelopment of services over the past two decades,and with the current support of the World Bankhealth reform project, the organisation has beenconcerned for the quality of existing and emergingservices. To this end, ANIP proposed a novelmethodology for the accreditation of all services ininpatient units and home-based services, public orprivate. The two-year pilot project receivedEuropean Economic Area (EEA) Grants funding andwas a good opportunity for co-operation betweenpublic and private sector representatives; it aimed toinclude specific palliative care standards in thenational accreditation process of hospitals andhome-care. The project taskforce consisted of a widerange of stakeholders with interests in theadvancement of palliative care. These included:professionals from various disciplines, such asphysicians, nurses, psychologists, social workers, inpublic and private service providers; andrepresentatives of public hospitals, such as theRegional Oncology Centre in Iaşi and the MunicipalHospital Campia Turzii, charitable hospiceorganisations, healthcare decision-makers andfunding authorities (health insurance houses).
The group developed two specificmethodologies for the accreditation of palliativecare services in inpatient units and home-basedservices and defined the accreditation process. The methodology was detailed and published inthe ‘Accreditation Guidelines for Palliative CareProviders’. 16 The providers are awarded four levelsof accreditation:l Level A – excellence in palliative care provisionl Level B – high level of palliative care provisionl Level C – basic level of palliative care provisionl Level D – accredited with compliance plan.
The newly proposed methodology was adopted by the National Agency for theManagement of Healthcare Quality and will beused in the next accreditation cycle to assess allpalliative care providers in Romania in inpatientunits and home-based services.
As a professional organisation, ANIP and its members are committed in the years to come to playing an increasing role in the national development of palliative care in Romania at academic, educational, professional and scientific levels, as well as working towardsquality services development, advocacy and awareness �
References1. Vasile V, Dobre A, Overview of demographic evolution in Romania, RRS,2015; 4: 27–45.2. Eurostat. Causes of death statistics. Luxembourg: European Communities,2013. ec.europa.eu/eurostat/statistics-explained/index.php/Causes_of_death_statistics (last accessed 04/09/16)3. Clark D, Wright M. Transitions in end of life care: hospice and relateddevelopments in Eastern Europe and Central Asia. Buckingham: Open UniversityPress, 2003: 176–194.4. The Parliament. Law No 339: concerning the legal regime of plants, narcoticdrugs and psychotropic substances, and narcotic and psychotropicpreparations. Official Gazette of Romania, 2005; 1095. www.ier.ro/sites/default/files/traduceri/L-339_2005.pdf (last accessed 04/09/16)5. Mosoiu D, Dumitrescu M, Connor S, Developing a Costing Framework forPalliative Care Services. J Pain Symptom Manage, 2014; 4: 719–729.6. Oncology Institute Prof. Dr. Ion Chiricuţă, Cluj Napoca. IZERZO project.www.iocn.ro/en/Research/The-projects-web-pages/IZERZO.html (lastaccessed 04/09/16)7. Kantonsspital St. Gallen. Overcoming disparities on access to quality basicpalliative care in the community. //research.kssg.ch/Projekte/einfache-Suche/57716 (last accessed 04/09/16)8. Casa Sperantei. Creating a national evaluation system for palliative careservices targeting vulnerable populations.www.studiipaliative.ro/proiecte/evaluarea-serviciilor-de-ingrijiri-paliative-coerent/ (last accessed 04/09/16)9. European Palliative Care Academy. Developing a New Pathway forManagement of Palliative Care Patients with Advanced Cancer in Iaşi County.www.eupca.eu/vladimir-poroch/ (last accessed 04/09/16)10. International Association for the Study of Pain. Physicians’ education forpain in NE Romania (PEPNER). www.iasp-pain.org/Education/Content.aspx?ItemNumber=5458 (last accessed 04/09/16)11. MedLang. Project homepage. www.medlang.eu/ (last accessed 04/09/16)12. National Association for Palliative Care. Directory of palliative care servicesin Romania, 2014. www.anip.ro/resurse/catalogul-serviciilor-de-ingrijire-paliativa-din-romania/ (last accessed 22/08/16)13. Higginson I. The palliative care of Londoners: needs, experience, outcomesand future strategy. London: London Regional Strategy Group for PalliativeCare, 2001.14. Romanian National Healthcare Strategy 2014–2020. //ms.gov.ro/upload/Anexa%201%20-%20Strategia%20Nationala%20de%20Sanatate%202014-2020.pdf (last accessed 01/09/16)15. World Bank, Health Sector Reform, Improving Health System Quality AndEfficiency Project.) documents.worldbank.org/curated/en/333121468095642862/Romania-Health-Sector-Reform-Improving-Health-System-Quality-and-Efficiency-Project (last accessed 01/09/16)16. Hospice Casa Sperantei. Palliative care providers’ guide for accreditation,2016. www.studiipaliative.ro/projects/national_evaluation_system_palliative_care/
www.ejpc.eu.com EUROPEAN insight…
Copyright © Hayward Medical Communications 2016. All rights reserved. No unauthorised reproduction or distribution. For reprints or permissions, contact [email protected]

Launching in 2017 | FREE resourceAre you a healthcare
professional working in eye care?•
Are you keen to continuously improve theway you manage and treat your patients?
•Do you want to keep up to date with the latest
opinions, guidance and practical advice in this field?•
Then Ophthalmology in practiceis the journal for you!
•For more information and to register for your FREE print copy, visit www.ophthalmologyinpractice.co.uk
•Follow us:
t | @ophthinpractice |v| @ophthalmologyinpractice |ą | Ophthalmology in practice
Brought to you by Hayward Medical Communications | www.hayward.co.uk | +44 (0)1638 723560IMAGE: JUERGEN FAELCHLE/SHUTTERSTOCK.COMCopyright © Hayward Medical Communications 2016. All rights reserved. No unauthorised reproduction or distribution. For reprints or permissions, contact [email protected]



![Avas evam Shahri - uptownplanning.gov.inuptownplanning.gov.in › Go › From_Jan2007_Dec2007 › Main_Text.pdf · 1 l[a ;k & 154@vkB&3&07&3214lh@96 iz’skd] Jh “kda j vxokyJh](https://img.pdfslide.us/doc/110x75/5f12f2c966b1147e18719de2/avas-evam-shahri-a-go-a-fromjan2007dec2007-a-maintextpdf-1-la-k.jpg)