Embed Size (px)
Citation preview
The CRAJ is online! You can find us at: www.stacommunications.com/craj.html
Volume 17, Number 4 • Winter 2007
The Journal of the Canadian Rheumatology Association
FOCUS ONCommunications in Rheumatology
EDITORIALCryptic Communication
PRESIDENTIAL AND VICE-PRESIDENTIAL GREETINGS
IMPRESSION AND OPINIONDr. Duncan Gordon and The Journal of RheumatologyDr. Barry Koehler: Founding The Journal of the Canadian Rheumatology AssociationDr. Steve Edworthy: The Canadian Rheumatology Association WebsiteUpdate on the Future of the CRA WebsiteDoctor Video: A Guide to Electronic Medical Specialists
NORTHERN (HIGH)LIGHTSMilestones: Dr. Harold Fireman
JOINT COMMUNIQUÉSt. Michael’s Hospital: The ACPAC ProgramCAPA on the MenuMSK Boot CampPracticing Rheumatology in Quebec: Portrait of a Solo PracticeRegional News: Winnipeg, Manitoba, Trois-Rivières, Québec
Victoria, British Columbia
HALLWAY CONSULTDr. Peter Lee: Raynaud’s Phenomenon
JOINT COUNTAssessing Medical Publications
Mission StatementThe mission of the CRAJ is to encourage discourse among the Canadian rheumatology community for theexchange of opinions and information.
CRA EDITORIAL BOARD
Copyright©2007 STA HealthCare Communications Inc. All rights reserved. THE JOURNAL OF THE CANADIAN RHEUMATOLOGY ASSOCIATION is published by STA Communications Inc. in Pointe Claire, Quebec. None of the contents of this publication may be reproduced, stored in a retrieval system or transmitted in any form or by any means (electronic, mechanical,photocopying, recording or otherwise) without the prior written permission of the publisher. Published every three months. Publication Mail Registration No. 40063348. Postage paid atSaint-Laurent, Quebec. Date of Publication: December 2007. THE JOURNAL OF THE CANADIAN RHEUMATOLOGY ASSOCIATION selects authors who are knowledgeable in their fields.THE JOURNAL OF THE CANADIAN RHEUMATOLOGY ASSOCIATION does not guarantee the expertise of any author in a particular field, nor is it responsible for any statements by such authors. The opinions expressed herein are those of the authors and do not necessarily reflect the views of STA Communications or the Canadian Rheumatology Association. Physicians should takeinto account the patient’s individual condition and consult officially approved product monographs before making any diagnosis or treatment, or following any procedure based onsuggestions made in this document. Please address requests for subscriptions and correspondence to: THE JOURNAL OF THE CANADIAN RHEUMATOLOGY ASSOCIATION, 955 Boul. St. Jean, Suite 306, Pointe-Claire, Quebec, H9R 5K3.
The editorial board has complete independence in reviewing the articles appearing in this publication and isresponsible for their accuracy. The advertisers exert no influence on the selection or the content of materialpublished.
PUBLISHING STAFF
Paul F. BrandExecutive Editor
Russell KrackovitchEditorial Director, Custom Division
Maeve BrooksManaging Editors
Mandi WatsonAssociate Editor
Dana WittenbergerEditor-proofreader, French
Donna GrahamProduction Manager
Dan OldfieldDesign Director
Jennifer BrennanFinancial Services
Robert E. PassarettiPublisher
EDITOR-IN-CHIEFGlen Thomson, MD, FRCPCFormer President, CanadianRheumatology AssociationAssociate Professor,University of ManitobaWinnipeg, Manitoba
MEMBERS:Ken Blocka, MD, FRCPCBurrard Health BuildingVancouver, British Columbia
Michel Gagné, MD, FRCPCPolyclinique St-EustacheSt-Eustache, Quebec
James Henderson, MD, FRCPCChief, Internal Medicine,Dr. Everett Chalmers HospitalTeacher, Dalhousie UniversityFredericton, New Brunswick
Joanne Homik, MD, MSc, FRCPCAssistant Professor of Medicine,University of AlbertaEdmonton, Alberta
Sindhu Johnson, MD, FRCPCClinical Associate,Division of Rheumatology University Health Network-Toronto Western Hospital SiteInstructor,University of TorontoToronto, Ontario
Majed M. Khraishi, MD, FRCPCMedical Director,Nexus Clinical ResearchClinical Professor of Rheumatology,Memorial UniversitySt-John’s, Newfoundland
Gunnar R. Kraag, MD, FRCPCPresident, Canadian RheumatologyAssociationProfessor of Medicine,University of OttawaThe Ottawa HospitalOttawa, Ontario
Diane Lacaille, MD, FRCPCAssistant Professor of RheumatologyRheumatology DepartmentUniversity of British ColumbiaVancouver, British Columbia
Barbara A. E. Walz LeBlanc, MD, FRCPCHead, Division of Rheumatology,Credit Valley HospitalMississauga, Ontario
Janet Markland, MD, FRCPCClinical Professor, Rheumatic Diseases Unit Royal University HospitalVisiting Consultant, Saskatoon City HospitalMedical Staff, St. Paul’s HospitalClinical Professor, University of SaskatchewanSaskatoon, Saskatchewan
Eric Rich, MD, FRCPCStaff, Centre Hospitalier de l’Université de Montréal (CHUM)-HôpitalNotre-DameAssistant Professor, Université de MontréalMontreal, Quebec
John Thomson, MD, FRCPCVice-president, Canadian RheumatologyAssociationStaff, The Ottawa Hospital–Civic CampusTeacher, University of OttawaOttawa, Ontario
Lori Tucker, MDClinical Associate Professor in Pediatrics,University of British ColumbiaFaculty, Centre for Community Child Health ResearchDivision of Pediatric RheumatologyBritish Columbia's Children's HospitalVancouver, British Columbia
Michel Zummer, MD, FRCPCPast President, Canadian RheumatologyAssociationAssistant Professor,Université de MontréalChief, Division of Rheumatology,Hôpital Maisonneuve-RosemontMontreal, Quebec

CRAJ 2007 • Volume 17, Number 4 3
“Hours of waiting in a crowd of similarly
afflicted individuals. Threadbare seats with
cushioning long since crushed to angstrom
thickness by tens of thousands of prior buttocks. One tele-
vision to distract from the ordeal: no sound to accompa-
ny the surreal purple picture on the screen. Staff with no
will to serve with the antiquated equipment at their dis-
posal. Much time to ponder: money could buy a
much-better experience.”
While this cryptic communication could equally well
describe the experience in many hospital emergency
rooms (try it yourself as a civilian sometime), this was a
description written at 35,000 feet on a trip back from
Britain earlier this autumn on a national airline. Proud as
we are of all things bearing national symbols, there is
much that needs renovation in our country.
The CRA over the last number of years has been stalwart
in its resolution to improve professional arthritis care in
Canada. Many projects and persons have been funded by
the CRA to achieve these goals. The CRA over multiple
administrations have been careful stewards of the fund
which was started at less than $5,000 in the early 90s.
The Kraag administration has carried on in this tradition
of diligence. The latest quest to assist another venerable
Canadian institution—The Journal of Rheumatology—has
been considered during long meetings and with considerable
debate. The CRA hopes that it will be possible to keep
Canadian this journal which has long communicated so
many major Canadian rheumatologic ideas to the world.
Communication is the most basic medical skill. From
taking a history to describing the esoteric discoveries in
the laboratory, the ability to relay information in an
understandable and accurate manner is critical. This
issue explores communication in rheumatology from the
peer-reviewed science in Dr. Duncan Gordon’s esteemed
publication through the CRA’s distribution of informa-
tion through print and electronic media.
The Journal of the Canadian Rheumatology Association has
been most fortunate to have had the unrestricted sponsor-
ship of Pfizer to support these efforts. STA Communications
should be commended for their professionalism and
enthusiasm for this ongoing project. Our Managing
Editor, Maeve Brooks, will be on maternity leave presently
and deserves a big Christmas present for her wonderful
and creative work. Paul Brand, the Executive Editor, is the
organizational force behind this publication and will have
a Happy New Year if all our contributors get their articles
in on time! Our new Managing Editor, Mandi Watson, a
seasoned rugby player, fears no rheumatologist: the quar-
terly deadlines will be met!
As this year draws to an end, it is appropriate to thank
President Dr. Gunnar Kraag, VP Dr. John Thomson, Secretary-
Treasurer Dr. Jamie Henderson, and Executive Coordinator
Christine Charnock and all the CRA Executive who have given
great service and leadership throughout 2007.
Merry Christmas, Happy Hannukah, and joyous cele-
brations of all kinds to you and yours. May the New Year
bring some favourable tailwinds and some first-class
service for everyone!
Glen T.D. Thomson, MD, FRCPC
Editor-in-Chief
EDITORIAL
Cryptic CommunicationBy Glen Thomson, MD, FRCPC
Communications are dependent on timing. The editor in Aldershotexploring new techniques in publishing to ensure articles aresubmitted before deadlines!
Editing inappropriate content for the benefit of CRAJ readers whileon assignment at the Vatican Museum.
he holiday issue
of the CRAJ pro-
vides me with
the very pleasant opportunity of
saying hello to everyone and
wishing you all a great Holiday
Season. I hope you all take the
opportunity to make family,
friends and non-professional
activities your priority and take
the time to relax and recharge
your batteries. I might suggest
turning off your e-mail for
14 days. We should be able to
shouldn’t we?
There was sadness in 2007 as
we lost Dr. Adel Fam and Dr. Dale
McCarthy. They were loved and
respected by all who knew them
and had an enormous impact on
patients, students and colleagues.
They will be fondly remembered.
I would like to express my grat-
itude and that of the CRA Executive and Board for the
outstanding job that Christine Charnock does as the
Executive Coordinator of the CRA. She truly is the engine
of our organization. As always our members who serve on
committees, the executive and board of directors contin-
ue to work tirelessly on our behalf and remain the
strength of the organization. They do this while main-
taining their day jobs where their performance isn’t too
shabby either.
The possible purchase of The Journal of Rheumatology
remains a high priority for the CRA and we should have a
proposal to present to the membership no later than our
annual meeting at Tremblant.
Improvement of our website remains a top priority and you
will be hearing of some exciting changes in the near future
from Dr. Andy Thompson. We already have a new server and
will have a much more sophisticated site with enormous
potential such as the ability to provide high-quality video
and web casting. A lot more to come on this so stay posted.
Our Scientific Program remains our jewel and this year
Dr. Alf Cividino has taken over from Dr. Janet Pope as Chair
of the Scientific Committee. The
program looks outstanding so I
look forward to seeing you all at
Mont Tremblant.
In this year’s summer issue of
the CRAJ, Dr. Metro Ogryzlo was
featured; the history of the
Metro A. Ogryzlo International
Fellowship was reviewed and sev-
eral recipients of the Ogryzlo
Fellowship were interviewed. The
award was created by the CRA
with the intention that funds be
raised from members. Such
funding has decreased in recent
years so that less than a third of
the award was supported by the
CRA and the rest by the Arthritis
Society in the last year. TAS will
no longer provide funding so the
award’s future is threatened. I do
not think that this should be
allowed to happen.
It is my objective over the next few months to convince you
that it is important for the CRA to recognize pioneers such as
Metro Ogryzlo and to continue to support this award that
our organization committed to so many years ago.
It will soon be time for another needs assessment and
there is lots of discussion about our meeting sites.
Another Mexican/Canadian meeting looks set for 2011.
We are going to try Kananaskis for our western meeting in
2009 and there is discussion of looking at some
non-skiing venues.
Enough about work! I’d like to get back to the priority
of this greeting. I wish to thank all of you who make the
CRA the success that it is, and as president I order you all
to have a great holiday season.
Till Tremblant!
…………………………………..so it goes
Gunnar Kraag, MD, FRCPC
President, CRA
4 CRAJ 2007 • Volume 17, Number 4
PRESIDENTIAL GREETINGS
Greetings from the CRA President
President Kraag asking not what you can do for the CRAbut what the CRA can do for you!

VICE-PRESIDENTIAL GREETINGS
s I write
this mes-
sage, I am
sitting in my hotel room in
Boston. It is a gray and rainy
afternoon and I am waiting for
the 2007 American College of
Rheumatology (ACR) meeting
to start in earnest. Thousands
of rheumatologists are gather-
ing from all over the world,
coming together to listen, to
talk, to learn, to teach and to
connect. As I reflect on the
past year, since last year's ACR
meeting, I feel continuing sat-
isfaction and continuing
excitement as our specialty
becomes increasingly confi-
dent in its ability to control
inflammatory rheumatic diseases. We are feeling more
and more comfortable with our "new" treatments and talk
of cure and drug-free remission is now commonplace.
This week, we will hear of more novel and exciting treat-
ments. As far as we have come, especially in the past 10
years, I wonder if it is really still only the beginning. What
will things look like 10 years hence?
I'm looking forward to meeting up with Canadian
rheumatologists here in Boston. There is always a good
contingent at the ACR meeting and along with the learn-
ing and teaching and the talking and listening, there will
be laughter and warmth as the Canadian “family” of
rheumatologists connects.
The CRA remains busy on numerous fronts. Under Dr.
Gunnar Kraag’s strong leadership the CRA has continued
to do its usual work and more. Dr. Alf Cividino, our new
Scientific Chair, along with his Scientific Committee has
put together what looks to be another outstanding pro-
gram for the CRA meeting at Mont Tremblant in March of
next year. Dr. Proton Rahman has taken over this year as
Abstract Committee Chair from Dr. Sindhu Johnson and
we are expecting record numbers of abstracts. Dr.
Heather MacDonald-Blumer continues her important
work as Chair of the Education Committee.
Dr. Andy Thompson as
Website Chair has been busy
with major educational initia-
tives about to come to fruition.
Dr. Jamie Henderson, our rock
solid Secretary/Treasurer con-
tinues to watch over the books
with a careful Scottish eye and
offers sage advice on all the
important CRA issues. Our
past president, Dr. Michel
Zummer, continues his impor-
tant work as Access-to-Care
Committee Chair and has
been making certain to con-
tinue to maintain contact and
interaction with our Mexican
colleagues (he has been offi-
cially designated as Minister of
Mexican-Canadian Affairs). Dr.
Vivian Bykerk our Therapeutics Chair has been kept busy
working on updating guidelines and dealing with the
press in such issues as the withdrawal of lumiracoxib. Dr.
Janet Markland and her Human Resources Committee are
busy getting the word out to residents and medical stu-
dents that Rheumatology is “the place to be.” Special
thanks are due to Dr. Arthur Bookman and his “Journal of
Rheumatology” Committee who have been dealing with
the exciting but very demanding issue of the possible
purchase of The Journal of Rheumatology. Of course none of
this work could happen without the person that makes it
all happen, our Executive Coordinator, Christine
Charnock.
As the days shorten, the last of the autumn leaves flutter
to the ground and the north winds grow colder, I would
like to take this opportunity to wish you and your loved
ones a peaceful, restful and rejuvenating Holiday Season.
I look forward to seeing many of you at the CRA meeting
at Mont Tremblant in March 2008.
Sincerely,
John Thomson,
Vice-President, CRA
5CRAJ 2007 • Volume 17, Number 4
Holiday Greetings!
Vice-President John Thomson formally briefing CRA ExecutiveCoordinator Christine Charnock on behaviour at the Harvard Club

The Journal of Rheumatology was founded by Dr. Metro Ogryzlo but you were there from theinception. What were the challenges at the beginningof The Journal and later with the untimely passing of Dr. Ogryzlo?In the early 1970s, Dr. Ogryzlo knew that otolaryngolo-
gists, under the Editor Peter Alberti, founded their own
medical journal that had been quite successful. He was
acquainted with Dr. Alberti which gave him insight into
the world of publishing and hope that this could be done
for rheumatology. Dr. Ogryzlo’s idea was that a journal
could stimulate interest in rheumatology and the study of
arthritis in Canada. This idea of the journal was quite
controversial as, at the time, there were two other major
journals: Arthritis & Rheumatism and Annals of the Rheumatic
Diseases. When these other journals discovered that
Dr. Ogryzlo wanted to found his own journal, they tried to
persuade him otherwise. They promised to be more
accommodating and appoint some Canadian editorial
board members. But this was not Dr. Ogryzlo’s intention.
He wanted to have a journal that would stimulate interest
and work in Canada.
Looking at the hard facts, there were only 200 rheuma-
tologists in Canada at that time. Therefore this couldn’t
only be a purely Canadian journal, the market would not
have supported it. This had to be a Canadian-based inter-
national publication. This would be the only way.
Fifty contributors were invited for the first issue, which
was launched during the 1974 PANLAR Congress. The con-
tributors were international and the editorial board com-
prised worldwide leaders in the field of rheumatology. That
mix continues today: Most Canadian rheumatologists
receive The Journal, while the majority of our subscribers
are from elsewhere: The USA, Europe, Australia, Latin
America, and as far as Japan, Korea and China.
As for the CRA, back in those early days, they did not
understand why The Journal was needed seeing as two
other journals were on the market. The idea was that the
journal in Canada was not necessary but desirable because
it would have a stimulating effect on Canadian rheumatol-
ogy even though few of the articles were written by
Canadian authors. In this fashion, The Journal would have
an international, national and local impact. Dr. Ogryzlo
wanted The Journal to be the official journal of the CRA and
they turned it down, saying it wasn’t the right time.
The challenges at the beginning included establishing
The Journal, fostering interest in potential contributors,
receiving accreditation and recognition from the US
National Library of Medicine so that articles would be regis-
tered. This accreditation was not automatic. In order to
accomplish this, you had to demonstrate that you were wor-
thy of this recognition.
Also, The Journal was financed by 30 rheumatologists
across Canada who made a small investment to get The
Journal off the ground. In this way, we had financial backing,
advertisers, authors and reviewers. In fact, what happened
was our authors became our reviewers, and subscribers
became our authors and reviewers. So you end up with a
loop of quality participants involved in the work of The
Journal. So it is not a one-man band, it’s a group interest-
ed in the academic advancement of rheumatology.
Therefore the challenges were to get readers in rheuma-
tology to buy into this concept and for us to come up with
a good product.
Would you tell us about the stages of publication overa typical month and how much time you spend withyour multiple briefcases in preparing your monthlyedition of The Journal of Rheumatology?We’ve got an office team, we have a Managing Editor and
a whole team of editors. After Dr. Ogryzlo’s untimely pass-
ing, we formed an Editorial Committee that still functions
today, not with the same people but following the same
idea and process.
Dr. Duncan Gordon and The Journal ofRheumatology
Dr. Duncan Gordon is Editor of The Journal of Rheumatology since 1979. He is also a rheumatology consultant atthe University Health Network-Toronto Western Hospital Site and Professor of Medicine at the University of Toronto.
CRAJ 2007 • Volume 17, Number 46
IMPRESSION AND OPINION
CRAJ 2007 • Volume 17, Number 4 7
We meet every two weeks and look at articles, decide
which are worth sending out for review and which review-
ers will review specific articles and which articles will be
published and when. We call this the “hanging commit-
tee,” like the Tate Gallery in London, because we decide,
in effect, which “pictures to hang.”
We typically publish half of the articles submitted, not
necessarily because some articles aren’t good but
because some are merely not appropriate for our journal.
The articles chosen are of course always strengthened by
our reviewers comments, and our editorial board also
comprises rheumatologists with years of experience. So
we survived Dr. Ogryzlo’s passing by benefiting from the
two years he worked hard to establish The Journal and set
this system in place.
The Journal of Rheumatology is one of the best-recognized peer-reviewed publications in the fieldof arthritis. What aspects of The Journal has kept it inthe forefront over the last number of decades? When we started, we were the new kids on the block!
There were three or four peer-reviewed journals and now
there are twenty something. We were unique in that we
were the only rheumatology journal in the world owned
by rheumatologists, which is interesting.
Some of the things we’ve done since we started, of course,
have been copied which is always the case with good ideas.
We’ve always tried to bring controversy to our editorial
pages, I think being provocative is important. We want to get
people thinking and to say what they mean and mean what
they say. We often run cross editorials where we showcase
different view points. We also had our letter section which
often included reader complaints or opinions, so we often
get a crossfire going there as well. At the time we launched,
this was new and different and gave us recognition. We’re
also very user friendly and we do our best to be fair.
While I think we have a high-quality and innovative
publication, we always knew we would never have the
same impact as Arthritis & Rheumatism or the Annals of the
Rheumatic Diseases. These journals publish criteria for var-
ious diseases, articles which get much cited. Our ambi-
tion was to become an Avis not a Hertz!
With the arrival of the Internet era, there have beentremendous changes in all areas of publication. Howhas the Internet affected peer-reviewed scientificpublications? How has this affected The Journal ofRheumatology?
There’s a ying and yang effect with electronic communi-
cation. The good thing is that it provides instant gratifi-
cation. In the early days, we would send our reviewers a
package by the mail, which included a letter inviting them
to review this article. And so when you receive this in the
mail you typically take some time to think about it. You
don’t just put it in the trashcan. With web-based review
systems, you can quickly respond that you are not inter-
ested and put it out of your mind. So the result is that our
submissions have gone up 30% in the last five years as
everything seems to get done faster with the Internet but
by the same token our reviewers are inclined to decline
reviewing material as everyone is busy. So in that sense
instant gratification means instant rejection!
No doubt the Internet has led to our growth and our
creative growth but it is also much less personalized. But
the Internet is not going away, it is here to stay so we have
to work within it.
Changes have occurred in some scientific grants withnew requirements to publish publicly in a timelyfashion. How will this affect The Journal ofRheumatology and other publications?Yes, what you are referring to is the concept of open
access (OA). There is pressure from some parts of the
planet to have all medical articles “open.” For example,
the United States Congress argues that it pays for
research at the National Institutes of Health (NIH) and
asks why one should pay to have access to this informa-
tion. When Harold Varmus, the Noble Laureate, was head
of NIH, he promoted the idea of open access. He pre-
sented the idea that instead of The Journal being support-
ed by subscribers and advertisers in the conventional way,
it should be supported by authors and research funders.
The author would have to pay to have his article pub-
lished which would be borne by the researcher. Certain
We’ve always tried to bring controversy
to our editorial pages, I think being
provocative is important. We want to get
people thinking and to say what they
mean and mean what they say.

CRAJ 2007 • Volume 17, Number 48
research bodies, such as The Wellcome Trust, stated that
they would not allow the researcher to publish a paper in
a journal unless it was instantly and openly available. The
Journal of Rheumatology remains a subscriber-based
publication, but our editorials and correspondence are
freely available to all website visitors. An author-pays
option is being contemplated. Now I’m noticing with
rheumatic diseases that some pharmaceutical companies
are paying big bucks to have open-access articles pub-
lished. It is definitely controversial. When the Editor of
the Annals of the Rheumatic Diseases, which is the best-
known journal in Internal Medicine, canvassed sub-
scribers and asked if they would still subscribe to the
journal if it was open access, the response was a resound-
ing “no.”
The other role player is the advertiser. The advertiser is
invested in the print version as they don’t know how to
measure the impact of online advertising yet. Some journals
give away their content for free and have suffered financial-
ly due to it. The Journal of the American Medical Association was
doing this for a long time and lost a ton of money and have
since stopped. The Canadian Medical Association Journal, an
open and free-access publication, is heavily subsidized by
advertising. If you look at a copy of that journal, a large pro-
portion of pages are advertisements. The leading medical
journals like The Lancet don’t buy into this idea, but I do
believe The New England Journal of Medicine will be making
their articles accessible within six months of publication.
So how this will affect The Journal of Rheumatology is a
work in progress. We don’t know the answer quite yet.
Will there be a change in the role of peer-reviewedscientific publications in the next decade?As research advances, the need for better understanding
will require a wider scope. There are all kinds of areas of
study and so I think the role will not change but increase.
It will be more of the same I think. I think The Journal of
Rheumatology, and other medical journals like it, have an
important role to play in what we call the medical discov-
ery cycle. Scientific publications have a responsibility to
ensure that what is published serves our patients and
society. Because our society is becoming more reliant on
techonology, we need to be especially transparent in the
conduct, sponsorship and publication of scientific
advances. The trust we establish with our readership must
be earned and maintained through such actions.
The idea of the peer-review process affects every level of
scientific publishing: the decision to fund a grant, main-
taining accountability, having submitted materials reviewed
and receiving and publishing Letters to the Editor.
These are not the only challenges we face. Reviewers
sometimes try to protect their “turf” by delaying the pub-
lication of an article and will sit on the information.
There is also misconduct by authors who can fake data or
have duplicate publications.
Taking all this into consideration, peer-reviewed scien-
tific publications have to maintain a steadfast role in the
face of these challenges.
Will there be a change in the way that scientificjournals are published? Do you foresee a day when alljournals are electronic and that the “hard copy”edition is a thing of the past?Advertisers have a big role to play in equation as they are
currently unwilling to support the electronic medium.
Recently Elsevier has been trying to garner favor by guar-
anteeing open access to certain researchers but that is
very experimental. People like to read on paper, they like
print. I don’t know what will come of this…journal ipods?
I don’t see this happening in the near future and I don’t
see leading journals giving up their ownership. For exam-
ple, the Massachussetts Medical Society owns The New
England Journal of Medicine and it has been a great money
maker for them. A lot of the journals are owned by med-
ical societies so in that sense the profits role back to the
organization to do good work.
Unless advertisers can measure the impact of online
advertising vs. their print version, this will not happen.
Scientific publications have a
responsibility to ensure that what is
published serves our patients and society.
IMPRESSION AND OPINION
The CRA membership wish to express our sympathy and condolences to our colleague and friend
Duncan Gordon on the recent tragic loss of his son.

Dr. Barry Koehler: FoundingThe Journal of the CanadianRheumatology AssociationDr. Barry Koehler, the founding Editor of The Journal of the Canadian RheumatologyAssociation (CRAJ), is a staff rheumatologist at The Richmond Hospital and Clinical ProfessorEmeritus of Medicine at the University of British Columbia.
You were the founding Editor of the CRAJ in 1992. Whydid the Canadian Rheumatology Association (CRA) feelthat a publication was necessary at that time? Were thereany obstacles to starting the journal?I don’t think there were a lot of obstacles. The concept arose
from the fertile mind of Dr. Paul Davis, President of the CRA
at the time. Given that we were in the process of separating
our annual meeting from that of the Royal College, it
seemed timely to raise the profile of the organization. We
had a lot of support and published the journal through
STA HealthCare Communications Inc. with the help of
Paul Brand. I think it actually developed quite smoothly.
Was there a time when the CRAJ nearly ceased itsoperation? What were the challenges in the early days ofthe publication?Again, the development of the journal occurred in an easy
fashion, probably easier than we deserved! Everything devel-
oped quite effortlessly; people were happy to contribute
material and there was a lot of enthusiasm from the CRA
board. From my recollection this was a smooth event.
Fortunately, there were no big problems during my tenure.
The CRA separated from the Royal College in 1994 with thefirst Annual Meeting at Mont Tremblant in February 1995.Did the establishment of an in-house publication have insome small way a role in the spirit of independence that ledto the development of the “new CRA?”I don’t think many rheumatologists related strongly to the
CRA as a professional association. While most
rheumatologists belonged to the CRA and attended
meetings, it was not regarded as a very important
organization. I think, in fact, that most rheumatologists saw
The Arthritis Society as serving their needs and taking on
the role of an advocate for rheumatology. For a number of
reasons I think this shifted and, compared to the 1960s, 70s
and even early 80s, rheumatologists didn’t feel as well
represented by The Arthritis Society. Add to that the fact
that we were now breaking away to form an independent
new scientific journal, I think the journal played an
important role within the membership and in the creation
of a new version of the CRA.
The CRAJ continues to publish quarterly in a hardcopyformat. It is available through the CRA website in anelectronic version. Will there continue to be a role for aprinted version of the CRAJ? Do you see the time whenthe publication is strictly electronic?I think it is going to follow the path of most other journals.
My suspicion is that it may well become a solely electronic
medium just because of cost and efficiency. It hasn’t hap-
pened yet but maybe in 10 years it will. I think younger read-
ers will be very comfortable using an electronic medium.
When they get to my age they’ll probably be expecting that
because it’s convenient. You start to wonder why we are using
all this paper, it’s expensive and so on. For the most part, I
think people are going to be ready to use electronic versions.
It also makes sense in terms of storage. If you want to refer to
an article written two years ago, the likelihood is that you
won’t have that journal lying around. You look it up online! I
think accessing this publication online makes sense.
Do you have any thoughts on the future direction of theCRAJ?I think Dr. Glen Thomson has really moved this publication
along very nicely. He has organized it very well with some
political content, some history and some science. I think the
CRA is focused on the science more now with their work on
guidelines and research. I think the journal content
includes a nice balance. I doubt that anyone would want to
see the journal become a purely political vehicle so balanc-
ing this is good. It’s a successful format. I continue to pick it
up and read it. I suspect most members feel this way; it’s not
regarded as a throw-away journal.
CRAJ 2007 • Volume 17, Number 4 9
CRAJ 2007 • Volume 17, Number 410
Dr. Edworthy is a staff rheumatologistat Foothills Medical Centre andAssociate Professor of Medicine at theUniversity of Calgary.
There are few organizations today thatdo not have a presence on the Internet,yet when you launched the firstCanadian Rheumatology Association(CRA) website this was very novel. Wouldyou tell us what led the CRA to launchthe website when it did? What obstaclesdid you face?You are correct in noting that when the
CRA was developing its website in the mid-1990s, there
weren’t many examples to follow of not-for-profit medical
organizations developing their own website. Our biggest
challenge was raising the website concept to a priority
level in the face of many other competing ideas.
Fortunately, the executive recognized the need to establish
a good electronic environment from which to publish
CRA information to members.
We were restricted by the types of software and hard-
ware we could use, which meant a greater technical
expertise was required to manage our site at that time.
Another obstacle was that the CRA leadership had ques-
tions about the value this would have for its members. For
example, would members want to go to the Internet when
they could get their information via mail? Also, there were
some fears that the information might be in some way
misconstrued or cause unforeseen repercussions within
the medical community as it became available outside our
group. There were also some uncertainties about using a
new technology. Once we had decided to go ahead with it,
we were very fortunate to have Elisia Teixeira take on the
role of “webmistress,” which she continues to perform
today.
The sheer novelty of websites and theInternet has faded somewhat. How mustwebsites evolve to be better sources ofeducational material and information? The Internet is now “business as usual!”
Through the CRA website, we’ve got a great
opportunity for users to share their prac-
tice knowledge through audits of practices,
treatment of patients and presentation of
challenging cases. Those types of interac-
tive activities can now be managed very
effectively with online tools such as
Elluminate®. We are now in a position to
present the type of content that is required
on the web to attract attention: solid medical information
for patients, primary-care practices and rheumatology
colleagues. The work involved in providing this informa-
tion is substantial, particularly having to be presented in
an electronic format rather than print.
Another step is ensuring that there is a more
direct-to-the-consumer approach…the consumer being
the individual rheumatologists, others interested in
rheumatology, patients and even other associations which
are engaged with the CRA.
A major challenge for all websites is being known on the
worldwide web. One has to keep on top of being visible on
search engines like Google™ or you just don’t get found.
Another challenging new Internet direction for physi-
cians is the use of personal health records online. This is
a concern for physicians because they feel it is outside
their realm of practice. But this is definitely a consumer-
driven trend that will be hard for established medicine to
avoid. I’m anticipating that websites such as the CRA will
become interlinked and perhaps become a part of the
personal health record. That’s the direction some of us in
the informatics arena are exploring, with various tech-
nology firms.
Dr. Steve Edworthy: The Canadian RheumatologyAssociation Website
IMPRESSION AND OPINION
CRAJ 2007 • Volume 17, Number 4 11
In your view, how should established journals embracethe new electronic technology? Do established scientificjournals ignore the Internet as their peril?Any journal that cannot provide an electronic source to
their readership is definitely in peril. At this point, all the
students that I work with at the University level rely totally
on the electronic form of articles and I doubt they ever
use paper sources. When they can’t get access to a journal
online, they merely ignore that one.
There are many problems with competing in the elec-
tronic journal world. It’s not a trivial task: there’s a lot of
time and money that needs to be invested, a change in
style and likely a different business model for the produc-
tion of the electronic journal. However, if you take an
established journal with a good track record and do a
good job of moving it into the electronic format, they
have a much better chance of competing in the market.
Organizations like the CRA have limited resources andare increasingly dependent upon advertising to enableand promote education and information. This appearsto be the long-standing trend on the Internet ingeneral. Is this the way that communication inrheumatology and medicine in general should evolve?Are there any alternatives to their “business model?”It’s true that the CRA has limited resources and that
advertising is a mechanism to obtain necessary funds.
That model works but its downside is that it is annoying
to the reader to have that kind of information in their
face. It may be somewhat dangerous also in the sense that
advertising may serve as a conflict of interest with the
educational content being presented, which may discuss
a product or certain classes of drugs.
Many people are looking for an alternative to that busi-
ness model. I can’t say what would work better for the
CRA. Some websites operate on a subscription basis and
charge for membership. There can also be a limit to the
amount of advertising exposure for corporations which
have other values.
There may be a chance for collaboration with other
organizations willing to fund the website or participate in
other activities that do not show on the website but are of
value to the website and the CRA. There are ways to utilize
the Internet that do not draw on advertising dollars. For
example, we are beginning to see clinical trials operating
via the Internet. Performing these trials can be of tremen-
dous value to companies and to society. A well-established
website, with a good track record, could conceivably offer
a service that wouldn’t require advertising but could facili-
tate a more efficient clinical-trial methodology.
There is also potential for an interesting collaboration
with the Canadian Medical Association (CMA). The CMA
has tremendous expertise in a variety of internet-based
services including the provision of patient information,
an “online store” with electronic products that doctors
can purchase. They demonstrate a real interest in helping
doctors’ practices become more efficient. The possibility
of a partnership with such an association for the CRA
would be a tremendous business opportunity. To link
forces with the CMA, which has a much bigger market and
some drivers the CRA doesn’t have, is the best business
opportunity I see for the CRA’s future.
In what direction would you like to take the CRAwebsite in the next five to ten years?In addition to the great work it is involved with today,
under the leadership of Dr. Andy Thompson, I would like
the CRA to become more integrated with our medical
practices. I would like the CRA website to facilitate the
secure exchange of communication and medical informa-
tion between caregivers.
Any journal that cannot provide an
electronic source to their readership is
definitely in peril.
The Internet is now “business as usual!”
Through the CRA website, we’ve got a
great opportunity for users to share their
practice knowledge through audits of
practices, treatment of patients and
presentation of challenging cases.
The CRA website continues to function effectively with
more than 40 visitors a day and more than 15 of our
members logging in each day. We hope to further
improve these statistics with some upcoming changes and
developments.
A new look: We will introduce a slightly-revised page
layout. We are doing this in reaction to the needs of our
members and to allow for more flexible sponsorship
opportunities.
Easier-to-find important content: Our members stat-
ed that they were having some difficulty finding important
information such as meeting dates and new highlights and
programs. To accommodate this we will have a content sec-
tion on the main landing page and get rid of the “ticker
tape” running across the top of the page.
More prominent links: Our other committees wanted
more prominent access to their programs. As such, we will
have areas on the home page with direct links to other
important CRA resources such as The Journal of
Rheumatology!
Changing sponsorship model: Our sponsorship model
is changing for the better. We are now allowing our
sponsors to post their continuing medical education (CME)
programs on our
server. You’ll notice
a clearly identified
“sponsorship sec-
tion” on the right
hand side of the website. By “clicking” on this section our
members will be able to view CME programs provided by our
sponsors. Realizing that some of these programs may con-
tain an inherent bias, all programs in the sponsorship sec-
tion will be clearly identified. The CRA executive feels that
this transparent sponsorship model will be mutually benefi-
cial for the CRA, our membership, and our sponsors.
This is an exciting time for the CRA website as we move
into our next phase of development with the commitment
of promoting the pursuit of excellence in arthritis care,
education and research.
Dr. Andy Thompson & Elisia Teixeira
Dr. Andy Thompson is Chair of the CRA’s Website
Committee and Elisia Teixeira is the CRA’s Website
Webmistress.
12 CRAJ 2007 • Volume 17, Number 4
IMPRESSION AND OPINION
Update on the Futureof the CRA WebsiteBy Andy Thompson, MD, FRCPC, and Elisia Teixeira
The 2007 ACR Meeting in Boston
CRAJ 2007 • Volume 17, Number 4 13
1. Dr. Mario
Game/System: Dr. Mario (Nintendo Entertainment
System)
Skill: Treats only those afflicted with blue, red and yel-
low viruses
Real-world specialty: Infectious Disease specialist who
must be tenured in a University Hospital to have such a
narrow scope of practice and still make a living.
2. The Professor
Game/System: The Legend of Zelda: Ocarina of Time
(Nintendo 64)
Skill: Uses only potions and herbal remedies
Real-world specialty: Practicing medicine without a
license as part of the “alternative medicine” movement
3. Dr. Stiles
Game/System: Trauma Centre: Under the Knife
(Nintendo DS)
Skill: Slows down time to perform surgery
Real-world specialty: Canadian surgeon, the slowing
down time may be the reason we have such long waiting
lists for operations
4. Dr. Robotnik:
Game/System: Sonic the Hedgehog (Sega Genesis)
Skill: obsesses about a talking hedgehog and plans end-
less failed revenges on his foes.
Real-world specialty: Medical administrator on another
delusional quest
Doctor Video: A Guide to Electronic Medical Specialists By Ian T. D. Thomson
What do our children learn about medicine from their omnipresent video games? It is necessary for parentsand physicians to communicate with these young minds so that they understand these video characters in thecontext of what doctors do in the real world.
This quick search for video doctors failed to reveal any practicing rheumatology. When will this obvious omission be
corrected?

Afew years ago, I had
reported in the CRAJ
that Dr. Harold
Fireman had retired. Harold
read the piece while in his
office after his secretary had
brought it to him asking
what they were doing work-
ing if he was retired. He
called and assured me he
was hard at work with no
immediate plans for retire-
ment.
I called him when I
recently heard that he had
retired and he immediately
confirmed that “yes, Gunnar, this time it is true.” I asked
him if he would do an interview and he said he would be
delighted. He asked me how old I thought he was, and
when I hesitated he informed me that he was 88 years old.
At this point he asked to be excused and continue the
conversation another time as he was just leaving for a
scheduled tennis match. I snapped the attached photos
the day after our interview.
I met Harold for the interview and had a number of
questions ready to go, but Harold was well prepared and
started right in. Questions were not required.
He didn’t start on himself, but rather began by talking
about Wally Graham. He recalled that the entire curricu-
lum in Rheumatology was covered by a single lecture
given in less than an hour by Dr. Wally Graham who cov-
ered osteoarthritis, rheumatoid arthritis, ankylosing
spondylitis, gout, and collagen diseases. It was 1940 when
Harold heard that lecture, and he still remembers it as
one of the best he has ever heard. He recalls Wally as
very good looking, slim, and very energetic and restless.
He played the piano, held the Canadian record for the
440-yard dash, and was a supreme motivator. He felt it
tragic that he died suddenly
at the age of 56 years and
was sure that he would have
continued to make major
contributions to rheuma-
tology. He was a strong influ-
ence on Harold in guiding
him to choose rheumatology
as a career.
He also recalled Dr. Almond
Fletcher as one of the leaders
in arthritis, and described
him as a slight, almost
cachectic man who always
looked unwell, but was very
bright. He felt his influence
paled in comparison to Wally Graham. He actually left the
field of arthritis to work with Dr. Walter Campbell who spe-
cialized in diabetes and on making this switch Harold
recalls him saying “don’t hold it against me!” This was at the
time that the first dose of insulin was actually given to a
patient at the Toronto General Hospital.
Harold graduated in 1942 and had a job waiting for him
at the Barnes Hospital in St. Louis, but was stopped from
going because he was needed in the armed forces and
served in the Air Force from 1942 to 1946. He recalls
another physician who was also in the Air Force,
Dr. Metro Ogryzlo and still remembers having dinner with
Metro in Moncton. The food they were used to was most-
ly powdered and he recalls how excited Metro was when
they were served sour pickles—a relative delicacy com-
pared to everything else. He also recounts a story told to
him by Dr. Phil Rosen, who recalled an encounter with a
young physician whom he did not know coming from
another ward and literally grabbing him with excitement
over a case that he had just seen and dragging him over to
show him. The young physician was Metro and that meeting
and relationship led to Phil’s career in rheumatology.
JOINT COMMUNIQUE
Milestones: Dr. Harold Fireman By Gunnar Kraag, MD, FRCPC
14 CRAJ 2007 • Volume 17, Number 4
NORTHERN HIGHLIGHTS

He recalls Phil Rosen telling him that he collected
wooden clocks largely because he felt he should match
his colleague, Dr. Hugh Smythe, who was collecting
Japanese pillows. These pillows were also made of wood.
He interned at the Ottawa Civic Hospital because he
could not go to the United States, as mentioned, and this
is how he subsequently also came to settle in Ottawa. He
did some training in Kingston and recounted many sto-
ries about the infamous Dr. Malcolm Brown, Dr. Russell
Cecil whose text was the best at the time, Dr. Eric
Bywaters, and others. Harold would be a superb after-din-
ner speaker as he is a natural storyteller and his experi-
ences are fascinating.
Interns, in those days, did not get paid except for a
bonus at the end of the year which was about $50. They
were provided with room and board as well as a laundry
service. Harold recalls that a way to make some money was
to donate blood for which you got about $15. Of course
in those days the blood was taken immediately to the
patient and not stored.
Prices were such that he could go to the Fairmont
Château Laurier with a date for dinner and dancing at the
cost of $1.50...so $15 was a lot of money. As a result, he
thinks that he and his fellow trainees were likely quite
anemic.
He received his fellowship in 1961 and, along with
Dr. Henry Sims, started an arthritis clinic at the Ottawa
Civic Hospital. He also built up his practice with patients
who had arthritis since nobody wanted to care for them
as the general feeling was that nothing could be done.
There was no Ontario Health Insurance Plan (OHIP) in
those days and all the hospital work they did was pro bono.
Harold feels that the last 20 years were his best and
most enjoyable. He never minded going to work because
he loved it and never considered it a chore.
As to the secret of his longevity, he attributes it partly to
genetics, but primarily to staying active so his advice to
me was “stay active!” Harold continues to play tennis regu-
larly, he also plays bridge, travels, reads and participates in a
medical history club where he recently made a presentation.
Voltaire didn’t produce his greatest work until he was
67 years old and Harold said his best and most enjoyable
years were from the age of 68 years to 88 years. He loved
what he did and kept active and engaged. The next time I
feel like a nap, I’ll ask myself: “What would Harold do?”
Harold has the knack of holding you a bit spellbound
because he tells a story so well. I wish we had the space to
tell them all.
Congratulations to Harold on a great career!
Dr. Gunnar Kraag, MD, FRCPC
President, CRA
Harold about to unleash his scorching backhand for another win!
As to the secret of his longevity, he
attributes it partly to genetics, but
primarily to staying active so his advice
to me was “stay active!”
15CRAJ 2007 • Volume 17, Number 4
The Advanced Clinician Practitioner in Arthritis
Care (ACPAC) Program is a University of Toronto,
faculty of medicine-based continuing education
certificate program in advanced musculoskeletal
(MSK)/arthritis care for experienced MSK physiothera-
pists and occupational therapists.1 This program was
developed at St. Michael’s Hospital (SMH) in collabora-
tion with The Hospital for Sick Children (HSC) and The
University Health Network, Toronto, and is run with the
help of over 60 faculty members, consisting of both aca-
demic and community healthcare professionals. Preceded
by the practitioner program at HSC,2 this interdisciplinary
health professional program is currently housed at SMH.
This innovative program was developed in response to a
documented need for an interdisciplinary approach in
diagnosing and managing patients with osteoarthritis
(OA) and rheumatoid arthritis (RA).3
The decrease in the number of rheumatologists due to
decline in program enrollment and aging population of
existing rheumatologists has been well-documented.4
There is increasing interest by the Ontario Ministry of
Health to change the current model of care for chronic
diseases and it is mandatory that all members of the
arthritis care team in such a model be appropriately
trained.
The ACPAC program is delivered in an episodic format,
consisting of 10 intensive units (academic and clinical),
offered one week per month. The program is based on
expected competencies and is rigorously evaluated.
The curriculum is based on the integration of material
from five core modules including Basic Science Theory
Underlying MSK Practice (n = 1), Foundations of Clinical
Practice (n = 1), Therapeutic Management (n = 1), and
the Art and Science of Clinical Practice (n = 2).
To date, since 2005, 13 trainees have graduated from
this program; 10 trainees have been accepted to the
2007-2008 academic year. All trainees are accepted
using strict criteria, come from institutions with full support
and a plan to return as practitioners working under med-
ical directives in a team environment. The trainees come
from rural (under-serviced), community non-academic
and academic health centers across Ontario. Evaluation
of the effectiveness of curricular design as well as the
development of new models of care/reintegration process
is ongoing.
The ACPAC program is being offered at a critical time in
the context of rapidly changing healthcare delivery in the
Province of Ontario. As arthritis care givers, we need to
position ourselves at the forefront of developing new and
effective models of chronic disease management.
The ACPAC program was originally developed with the
financial assistance of Amgen/Wyeth (unrestricted edu-
cational grant), Arthritis Society (Ontario branch), St.
Michael’s Hospital and its Foundation. Currently it is also
supported by a three-year grant from the Ontario
Ministry of Health and an unrestricted educational grant
from Abbott.
References:1. The ACPAC Program website. Available at:
http://www.stmichaelshospital.com/programs/mobility/acpac.php. Accessed September 10th, 2007.2. Campos A, Graveline C, Ferguson JM, et al. The Physical Therapy Practitioner: An Expanded Role for
Physical Therapy in Pediatric Rheumatology. Physiother Can 2001 Fall; 53(4):282-7.3. MacKay C, Devitt R, Soever L, et al. An Exploration of Comprehensive Interdisciplinary Models for Arthritis.
Arthritis Community Research & Evaluation Unit (ACREU). University Health Network; April 2005. 4. Hanly, JG. Manpower in Canadian academic rheumatology units: current status and future trends.
Canadian Council of Academic Rheumatologists. J Rheumatol 2001; 28(9):1944-51.
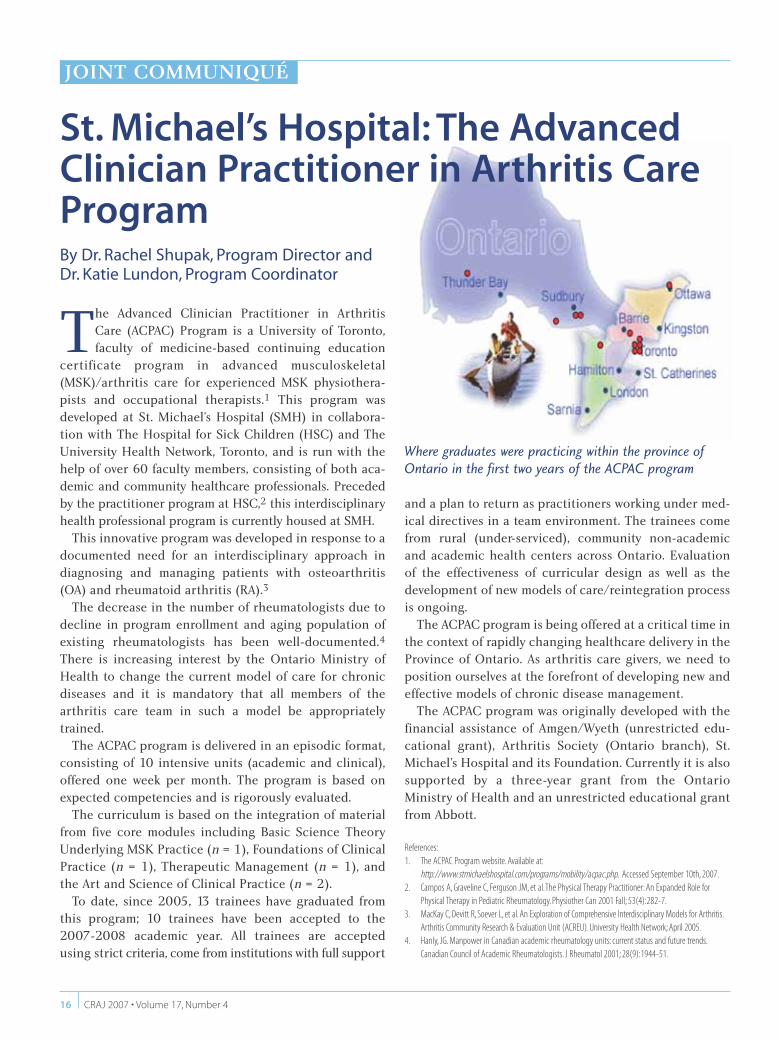
Where graduates were practicing within the province ofOntario in the first two years of the ACPAC program
St. Michael’s Hospital: The AdvancedClinician Practitioner in Arthritis CareProgramBy Dr. Rachel Shupak, Program Director and Dr. Katie Lundon, Program Coordinator
16 CRAJ 2007 • Volume 17, Number 4
JOINT COMMUNIQUÉ

CAPA on the MenuBy Ken Blocka, MD, FRCPC
Ihad the pleasure of being seated next to Ms. Anne Dooley,
President of the Canadian Arthritis Patient’s Alliance
(CAPA) at the windup banquet of this year’s annual meet-
ing of the CRA at Lake Louise. Like many rheumatologists, I
was just vaguely aware of CAPA but had no clear understand-
ing of the organization’s goals and objectives. Any uncertain-
ty I had was quickly dispelled by the enlightening conversa-
tion that transpired between bitefuls of buttery beef.
Anne is a passionate and articulate spokesperson for
CAPA, a patient-driven national advocacy organization
with members and supporters across Canada. CAPA cre-
ates links between Canadians with arthritis and assists
them to become more effective advocates with the ulti-
mate goal of improving the quality of life for all patients
affected by the disease.
Established in 2001, CAPA communicates the latest in
knowledge, research and health policy issues and works
collaboratively with a range of partner organizations
throughout Canada.
CAPA’s strategic priorities include:
• Raising awareness about arthritis to ensure timely and
uniform access to appropriate medications, health
professionals and services.
• To ensure a meaningful voice in arthritis research at all
decision-making levels.
• To create a source of information for adults and
children with arthritis and their support communities.
• And to assist adults and children in obtaining access to
care and reimbursement and other services that may be
required in managing a potentially lifelong disorder.
I was particularly struck by the CAPA premise that the first
expert in arthritis is the person who has it. A self-evident
concept? Perhaps, but one which represents a sea change in
attitude for a profession which has traditionally viewed the
physician as the acknowledged expert and the patient the
compliant supplicant. The realization among patients that
they are both entitled to and capable of providing a valuable
and necessary opinion is no less profound.
I personally have always regarded my relationship to
patients as a partnership and, where possible, have
sought to engage my patients in every aspect of the
decision-making process. I am sure that we have all rec-
ognized how this type of interaction may pay dividends as
far as adherence to care and the overall quality of the
physician-patient experience. We learn from our patients
all the time. No matter how well intentioned and learned
our recommendations may be it is our patients who must
ultimately decide what is best for them.
Whether seated across from their physician, a policy maker,
a pharmaceutical company or a grant adjudication commit-
tee, our patients bring a unique and valuable perspective.
I applaud organizations such as CAPA for promoting
and fostering this perspective and for helping to empow-
er our patients to see themselves as key stake holders in
the battle against arthritis. It is a “win-win” strategy for us
all and CAPA deserves our fullest support.
“Coffee or dessert anyone?”
For information about CAPA please contact Anne Dooley
President, Canadian Patients Alliance: [email protected] or
www.arthritis.ca/CAPA
MSK Boot Camp By Joanna Bostwick
Every December for the past four years, Dr. Alf Cividino
has coordinated a four-week “MSK Boot Camp” for sec-
ond-year medical students. As the name suggests, this
specialty elective offers a broad base of opportunity to
learn musculoskeletal (MSK) medicine. The elective is tai-
lored to each student’s personal learning objectives,
which vary depending on their respective interests in
either rheumatology, physiatry, family medicine or ortho-
pedic surgery.
A day in the MSK Boot Camp is filled with interactive tuto-
rials or group lectures, clinical skills in MSK physical exami-
nation, and special procedures such as joint injections. As
18 CRAJ 2007 • Volume 17, Number 4
JOINT COMMUNIQUÉ

CRAJ 2007 • Volume 17, Number 4 19
well, students are assigned to a variety of different clinics
each week to gain hands on experience with complex
rheumatologic cases. For one of the four weeks, students
are part of the in-patient rheumatology service, which
gives medical students exposure to management of
patients assigned to Internal Medicine. Weekly rheuma-
tology and orthopedic radiological rounds add to the
understanding of disease presentation and severity.
There is a real sense of collegiality and support
amongst the Hamilton rheumatologists. The students
meet weekly with the group at rheumatology rounds and
share their experiences, thereby gaining valuable experi-
ence presenting and interpreting case studies. On two
separate occasions, students delivered a 45-minute pres-
entation to the doctors. Although initially nerve wrecking,
the experience was monumental to help students gain
confidence in applying their knowledge base and to be
able to face challenging questions from our preceptors.
My personal experience has been very rewarding, and in
many respects, life changing. I have had a long-standing
interest in musculoskeletal medicine, an interest that devel-
oped while studying kinesiology at the undergraduate level.
While I initially enrolled in the MSK Boot Camp elective
simply out of this interest, it turns out I got more out of it
than I ever could have expected. In my first week of “boot
camp,” I met a young man who had a near death experience
with Wegener’s granulomatosis, an elderly patient crippled
by rheumatoid arthritis, and a young woman struggling
with Lupus. All three suffered from serious rheumatologic
diseases, but yet maintained a positive spirit and a sense of
humour that I found truly inspiring.
The rheumatologists working with the “boot camp” stu-
dents have been great teachers. Everyone I have met has
been friendly and incredibly passionate about his or her
field. In my personal experience, I have found the level of
support and encouragement from the physicians to be
quite inspiring. One case that particularly stands out in
my mind is that of a young father who had recently been
diagnosed with Ankylosing Spondylitis (AS). He was
eagerly waiting approval from the government for the use
of a Biologic drug, as he did not have a drug plan that
would cover the high cost of this treatment (which is very
troubling, as studies have shown that early management
in AS can significantly improve prognosis). Although it
must be quite frustrating for physicians to deal with the
fact that the high cost of medication can sometimes limit
treatment options, it has been wonderful to witness the
level of advocacy rheumatologists have shown for their
patients. The satisfaction of helping people control serious
health problems over a long period of time and the reward
of developing genuine long-term friendships with
patients in the process has been the most attractive
aspect of a career in rheumatology.
Upon reflection, rheumatology provides a wonderful
blend of basic physical examination and the rapidly
expanding science of immunology. I enjoy the challenge of
diagnosing patients and trying to understand the patho-
physiology of autoimmune and inflammatory diseases.
While at the MSK Boot Camp, I quickly realized that the
field of rheumatology offers a number of interesting career
opportunities allowing practitioners to tailor their respec-
tive practices to their personal interests and to constantly
learn new things. And considering that the root causes of
so many diseases remain unknown, rheumatology is a field
that is ripe with potential in terms of further advancement
and future research. This is what draws me to rheumatology:
the patients, the independence, and the learning.
There is a sense of excitement about the pace of scien-
tific progress in this field and the likelihood that this
progress will translate into new practical therapies for
people with rheumatic diseases. With a nationwide short-
age of trained rheumatologists and an increasing burden
of MSK diseases in our currently aging population, I
sense that a career in rheumatology would allow me to
balance my personal life with the challenges that rheuma-
tologists will be faced with in the near future.
From left to right: Dr. Cividino and McMaster University’s 2008Michael G DeGroote School of Medicine graduating students whoparticipated in the MSK Boot Camp: Nadine Gebara, JoannaBostwick and Hinal Sheth.
At first, I practiced medicine as a general practitioner for
four years in Abitibi in Rouyn-Noranda and in Laval at the
Cité de la Santé. Then, from 1984 to 1999, I practiced as a
rheumatologist and internist at the Sacré-Coeur de
Montréal Hospital. I finally set up a solo practice in Saint-
Eustache in a polyclinic where I have been practicing for the
last eight years already. In total, I have been practicing med-
icine for 34 years, including six years of residency!
Why a solo practice after years in a university setting
(hospital affiliated with the Université de Montréal)? First
of all, to be closer to home!
I also made that decision because I wanted to practice
rheumatology on a full-time basis, incorrectly thinking that
it would be less intense. In a clinic with 30 GPs and a very
vast population pool consisting of at least 250,000 people,
from Lachute to Terrebonne and from Laval (North-West
area) to Tremblant, there definitely is no shortage of work!
On the contrary, the practice has become quite diversi-
fied! After several months, requests to participate in com-
mittees, to teach or provide medical consultations and hold
conferences for physicians or the public flowed in. I recently
also received requests to teach preceptorship sessions.
Four years ago, a small clinical research practice was set
up and a nurse clinician was hired on a part-time basis.
Research is mainly focused on genetics (recruitment in
osteoporosis, osteoarthritis and rheumatoid arthritis),
phase III studies (rheumatoid arthritis, psoriatic arthritis,
etc.) and two phase II projects. I also participate in the Early
RA registry of my colleague Murray Baron from McGill.
In my opinion, running a solo practice has allowed me
to have a more flexible schedule and to combine all my
activities. In addition, my participation in the Convention
has increased in the last few years, enabling me to keep in
touch with several colleagues and update my knowledge
in our profession.
During my free time, my wife Francine and I “work” golf
courses in the summer. During the other seasons, we keep
busy by going to the cinema, reading, walking and travel-
ling. Happy grandparents to two grandchildren, we have
also replaced some leisure time with providing “babysit-
ting services”!
To summarize, running a solo rheumatology practice is
still very appealing to me and allows me to spend precious
time with my family and friends.
Practicing Rheumatology in Quebec:Portrait of a Solo PracticeBy Michel Gagné, MD, FRCPC
The most exciting recent news from Manitoba is a positive
report on the human resources front. Winnipeg has now
added four new rheumatologists to the region, bringing our
total to eleven. Dr. Shikha Mittoo joined the academic group
at Health Sciences Centre in July 2007. She trained at Johns
Hopkins University and comes to Winnipeg with a special
interest in pulmonary involvement of connective tissue dis-
eases. Drs. Ramandip Singh and Adarshdip Brar completed
their training in Winnipeg in 2006 and 2007 respectively, and
have become our first husband and wife rheumatology team.
They have established a joint practice (awful pun fully intend-
ed) in the community. Dr. Snezana Barac also completed her
training in Winnipeg in 2007 and is commencing her com-
munity practice once the fellowship exams are completed.
As winter approaches, we remember that we were blessed
with a beautiful summer this year in Manitoba allowing all
of us to pursue our various non-rheumatologic interests.
Dr. Glen Thomson coached some of Canada’s hopefuls for
World Cup 2014. Dr. Dave Robinson canoed with his fami-
ly and trained for the Joints in Motion climb in Peru. Drs.
Tim McCarthy and Christine Peschken filled their summer
days at their respective cottages with their families. Dr.
Carol Hitchon was busy with long-distance cycling. Dr.
Hani El-Gabalawy was involved in an intense cross-training
program getting ready for another hockey season.
Meanwhile, I continued to struggle with my golf game and
trained to improve my time at the Royal Victoria Marathon.
REGIONAL NEWS
20 CRAJ 2007 • Volume 17, Number 4
JOINT COMMUNIQUÉ
Update fromManitobaBy Cory Baillie, MD, FRCPC
CRAJ 2007 • Volume 17, Number 4 21
Since 1999, I have been working as a rheumatologist in the
Rheumatology/Physiatry Clinic for Central Quebec, located
at Trois-Rivières in the Mauricie Region. There are currently
four rheumatologists in our group (Drs. Louise Rouleau,
Michèle Dessureault, Frederic Morin and myself), and we will
soon be welcoming a new recruit, Dr. Clode Lessard. We are
a highly dynamic team, involved in a great number of very
interesting professional activities.
We are affiliated with the Centre Hospitalier Régional de Trois-
Rivières (CHRTR). The trend in rheumatology these days is to
send patients for outside-hospital care, but our group con-
siders it essential to maintain an in-hospital department in
order to treat patients with complex pathologies, such as
severe vasculitis or collagenosis. We are recognized as inflam-
matory disease specialists and are therefore frequently asked
to consult with regard to complex multisystem disorders.
We are all deeply involved in the training of medical
students and residents. Around ten residents rotate
through our clinic each year. We use this opportunity to
fully explain our specialty, and with some success, since a
number of them have subsequently chosen rheumatology
as their subspecialty. In actual fact, I think I was the first
resident to apply for a rotation at Trois-Rivières in 1994. I
am sure they had absolutely no idea that that young
unknown resident would ultimately become a colleague!
In 2005, the CHRTR became a designated medical train-
ing facility affiliated with the Université de Montréal. This
means that students can now take their full medical train-
ing in Trois-Rivières, from pre-med, core medical courses
and clerkship, to residencies in family medicine. All our
department members have lent a hand in the training of
these future physicians in various areas. I would like to
mention Dr. Dessureault’s outstanding input in particular:
she has worked tirelessly on the introduction and supervi-
sion of the first year students’ mentoring program. We are
also happy to welcome rheumatology residents who express
an interest in doing their rotation with us.
As far as clinical research is concerned, we are partici-
pating in several study protocols related to arthrosis,
osteoporosis and, obviously, rheumatoid arthritis. We also
supervise an infusion centre in our clinic. This service has
become necessary because of the growing number of
intravenous treatments now available.
In short, things are really moving in the Mauricie area
and you can rely on our team to maintain the standard
that rheumatology is a dynamic specialty, with close ties
to its community.
News from Trois-RivièresJean-Luc Tremblay, MD
British Columbian rheumatologists have had something to
celebrate this year, as long-standing efforts within the
Specialist society, have finally led to attention to disparity
issues for rheumatology and other disadvantaged groups,
using the MANDI formula, that compares net daytime
income from Monday to Friday between specialities. This
has been the culmination of a long hard fight.
Rheumatology has already had a 17% increase in fees, and
should receive at least another 6%, over the next three years.
This latter amount may increase, depending on the total
amount available for distribution. A fee dispute between the
Specialists and General Practice is still under appeal in the
courts, leading to a delay in the final settlement. Disparity
correction is always controversial among specialists, and
there is no guarantee of future progress on this front,
although we are hoping and working, to ensure that this will
be an on-going process.
On the Pharmacare front, BC is on the verge of finally
accepting coverage for biologics for ankylosing spondylitis. At
present, only etanercept is covered by BC for psoriatic arthri-
tis. An appeal through the BCMA, has led to an agreement
with Pharmacare to also reduce the amount of paperwork
required for annual approvals for biologics, although bureau-
cratic processes have delayed institution of these reforms as
yet. We expect approval for at least one of the biologics for the
ankylosing spondylitis indication in the near future.
In Victoria, we are still in the process of getting used to liv-
ing with the new medical school. Rheumatology has been
involved in a very limited way so far, but we hope to have more
influence in teaching, and perhaps influencing students
towards a career in rheumatology in the near future. We have
two rheumatologists who are working part-time and one on
the verge of retirement, out of a complement of five. We have
an active CME program, with meetings of the Vancouver
Island rheumatogists bi-annually. We have been fortunate in
attracting several speakers of international stature, such as
Dan Furst and Vibeke Strand, to these meetings. Although
leisure is supposed to be part of the life-style of Victoria, the
local rheumatologists haven’t see much of it.
Notes from VictoriaBy Milton Baker, MD, FRCPC

Raynaud’s PhenomenonBy Peter Lee, MD, FRCPC
Not all clinically significant questions have been definitively answered by randomized double-blind placebo-controlled trials. The Hallway Consult by-line in the Journal of the Canadian Rheumatology Associationwill seek a consensus answer from rheumatologic experts for your difficult questions. Please forward questions for future issues to: [email protected].
Management of Raynaud’s Phenomenon:Raynaud's phenomenon occurs in more than 90% of patients
with scleroderma and tends to be more severe in patients with
the limited form of disease and when compared to primary
and secondary Raynaud's phenomenon of other causes.
Scleroderma patients also have Raynaud's phenomenon that
is less responsive to vasodilator therapy because of the under-
lying vasculopathy involving the digital arteries with intimal
hyperplasia, vessel wall thickening and luminal narrowing.
The first step in the management of Raynaud's phenome-
non is to educate the patient on self-management with dress-
ing warmly in cold-temperature environments and avoiding
known precipitating factors such as handling cold objects and
emotional stress. Cessation of smoking is imperative but often
difficult to achieve.
Medical treatment of Raynaud's phenomenon is not always
necessary but indicated if despite the above measures, the
symptoms (pain, numbness or both) are severe enough to
result in impaired hand function. Treatment is obviously
required if the patient has developed ischemic lesions with
digital gangrene or ulceration. Initial treatment is usually with
an oral vasodilator. A long-acting formulation of nifedipine is
most frequently prescribed. However, use of this medication is
often limited by the occurrence of dizziness and headaches
even with lower doses. An appropriate starting dose would be
30 mg OD. Amlodipine and felodipine tend to be associated
with fewer hypotensive-type side effects. Losartan, an
angiotensin II receptor antagonist, has been shown to be more
effective than placebo and as effective as nifedipine, in a dose
of 50 mg OD and may be a useful alternative.
Topical nitroglycerin is sometimes useful in the treatment of
Raynaud's phenomenon. I have usually added this to the treat-
ment regimen when an oral vasodilator alone has not been
sufficiently effective. Hypotension is again the limiting factor
but can be minimized by administering the topical and oral
therapies 12 hours apart rather than together. In the case of a
digital ulcer, it is not necessary to apply the nitroglycerin
directly to the involved finger which tends to be messy and
can result in local skin irritation. Using a nitroglycerin patch
(anywhere on the body) is more convenient.
While widely prescribed in the treatment of more severe
Raynaud's phenomenon, the efficacy of oral vasodilators in
practice is quite limited and often inadequate especially if
ulceration or gangrenous changes have developed. In this
situation, more aggressive therapy is indicated but unfortu-
nately the choice of treatment with efficacy that has been
proven by randomized clinical trials is limited.
With severe Raynaud's phenomenon, complicated by
ischemic lesions, the use of prostaglandin analogues have
been shown to be effective, resulting in a reduction in fre-
quency and severity of attacks as well as improvement of dig-
ital ischemic lesions. Both alprostadil and iloprost appear to
have similar efficacy but the latter (which can be administered
through a peripheral rather than central venous line) is not
Case History: A 37-year-old male presents with a 10-year history of systemic sclerosis with limitedskin involvement and is seeking advice regarding management of his Raynaud's phenomenon. HisRaynaud's phenomenon is classic with tricolor changes of his fingers following cold exposure oremotional stress. On examination he has skin thickening that is limited to his fingers and back of hishands. Nailfold microscopy revealed the presence of capillary dilatation and ischemic areas withvessel drop-out. He was not able to tolerate previous treatment with nifedipine and amlodipinebecause of headaches. Marked improvement of his Raynaud's phenomenon occurred after anotherphysician treated him with a phosphodiesterase Type-5 inhibitor because of erectile dysfunction. Heis now able to wash dishes in cold water without colour change or discomfort of his hands.
22 CRAJ 2007 • Volume 17, Number 4
HALLWAY CONSULT

23
available in North America. Alprostadil is usually administered by
continuous intravenous (IV) infusion for a 72-hour period and in
the absence of cardiac manifestations is well tolerated.
Treatment is more effective if administered early before irre-
versible gangrene has developed or the ischemic ulcer has
become large (more than 5 mm in diameter).
The use of prostaglandin analogues is limited by the need
for continuous or repeated IV infusion and with alprostadil a
central venous line is necessary. Oral forms of prostaglandin
analogues have not been found to be effective. However, two
placebo-controlled clinical trials have shown bosentan (an
endothelin-1 receptor antagonist) to be effective in reducing
the frequency of recurring ischemic digital ulcers in patients
with scleroderma. However, the treatment did not increase the
rate of healing of the existing ulcers. The cost of bosentan is
extremely high and severely restricts its application in the
treatment of severe Raynaud's phenomenon.
An alternative treatment for severe Raynaud's phenomenon
is with phosphodiesterase Type-5 inhibitors. Efficacy has been
indicated in a number of case reports and in a small study
sildenafil 50 mg bid was found to be more effective than place-
bo in reducing the frequency and duration of attacks as well as
improving capillary flow and digital ulcers. As with bosentan,
there are no studies to indicate long-term efficacy and safety
with this treatment. Again expense is a limiting factor.
Obtaining either bosentan or sildenafil through provincial
health benefit plans is difficult if not impossible, primarily
because of the expense and the fact that Raynaud's phenome-
non is (not yet) an approved indication for these treatments.
In cases of severe scleroderma-related Raynaud's phenome-
non that have not responded to conventional therapy, alterna-
tive treatments to consider include oral anticoagulation with
warfarin and digital sympathectomy. I have personally
observed patients who have experienced a marked reduction
in the frequency of ischemic ulcers following oral anticoagula-
tion. Surgical cervical or lumbar sympathectomy is not an
effective long-term treatment and has long been abandoned
in the management of severe Raynaud's phenomenon.
However, chemical sympathectomy (cervical or lumbar) with
injections of local anesthetic may be effective in reversing local
vasospasm. Surgical digital sympathectomy has more recently
been advocated and claimed to be effective in anecdotal
reports. These treatments are unproven and their efficacy need
to be confirmed by randomized clinical trials but such studies
are seldom feasible because of the relative rarity of the disease.
Severe Raynaud’s phenomenon in patients with scleroderma
can be due to proximal macro-vascular occlusion and vascular
reconstruction in this situation may be helpful.
While there have been new and more effective therapies
available for the treatment of severe Raynaud's phenomenon
associated with scleroderma, the overall management of this
problem remains limited and frustrating.
PAGE HEADER
23CRAJ 2007 • Volume 17, Number 4
Sponsored by an unrestricted educational grant from Pfizer Canada.
Dr. Peter Lee is Director of the Scleroderma Clinic at the Rebecca MacDonald Centre for Arthritis and Autoimmune Disease, a
consultant rheumatologist at Mt. Sinai Hospital and Professor of Medicine at the University of Toronto, in Toronto, Ontario.
Editor’s Note: Compounded preparations of sildenifil or nifedipine have had some anecdotal success in treating mild Raynaud’s.
These topical preparations have not been subject to any reported clinical trails but should be further investigated.
The 2007 ACR Meeting in Boston
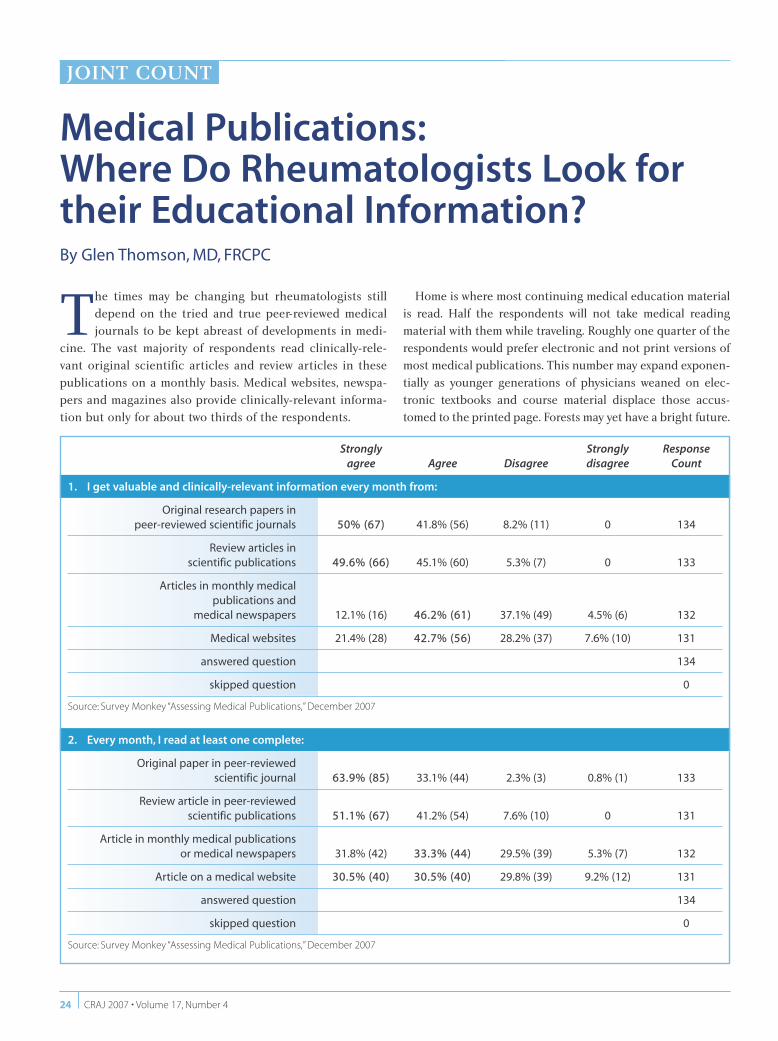
CRAJ 2007 • Volume 17, Number 424
Medical Publications: Where Do Rheumatologists Look fortheir Educational Information? By Glen Thomson, MD, FRCPC
24
JOINT COUNT
Strongly Strongly Responseagree Agree Disagree disagree Count
1. I get valuable and clinically-relevant information every month from:
Original research papers in peer-reviewed scientific journals 50% (67) 41.8% (56) 8.2% (11) 0 134
Review articles inscientific publications 49.6% (66) 45.1% (60) 5.3% (7) 0 133
Articles in monthly medicalpublications and
medical newspapers 12.1% (16) 46.2% (61) 37.1% (49) 4.5% (6) 132
Medical websites 21.4% (28) 42.7% (56) 28.2% (37) 7.6% (10) 131
answered question 134
skipped question 0
Source: Survey Monkey “Assessing Medical Publications,” December 2007
2. Every month, I read at least one complete:
Original paper in peer-reviewedscientific journal 63.9% (85) 33.1% (44) 2.3% (3) 0.8% (1) 133
Review article in peer-reviewed scientific publications 51.1% (67) 41.2% (54) 7.6% (10) 0 131
Article in monthly medical publicationsor medical newspapers 31.8% (42) 33.3% (44) 29.5% (39) 5.3% (7) 132
Article on a medical website 30.5% (40) 30.5% (40) 29.8% (39) 9.2% (12) 131
answered question 134
skipped question 0
Source: Survey Monkey “Assessing Medical Publications,” December 2007
The times may be changing but rheumatologists still
depend on the tried and true peer-reviewed medical
journals to be kept abreast of developments in medi-
cine. The vast majority of respondents read clinically-rele-
vant original scientific articles and review articles in these
publications on a monthly basis. Medical websites, newspa-
pers and magazines also provide clinically-relevant informa-
tion but only for about two thirds of the respondents.
Home is where most continuing medical education material
is read. Half the respondents will not take medical reading
material with them while traveling. Roughly one quarter of the
respondents would prefer electronic and not print versions of
most medical publications. This number may expand exponen-
tially as younger generations of physicians weaned on elec-
tronic textbooks and course material displace those accus-
tomed to the printed page. Forests may yet have a bright future.
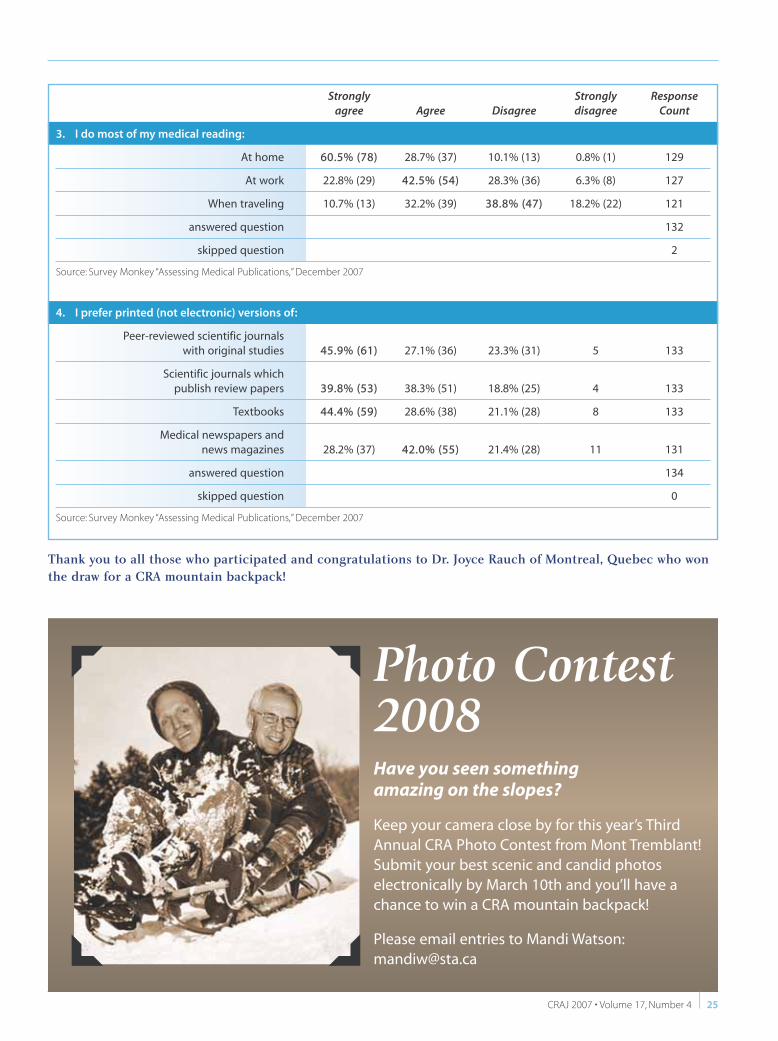
CRAJ 2007 • Volume 17, Number 4 25
Strongly Strongly Responseagree Agree Disagree disagree Count
3. I do most of my medical reading:
At home 60.5% (78) 28.7% (37) 10.1% (13) 0.8% (1) 129
At work 22.8% (29) 42.5% (54) 28.3% (36) 6.3% (8) 127
When traveling 10.7% (13) 32.2% (39) 38.8% (47) 18.2% (22) 121
answered question 132
skipped question 2
Source: Survey Monkey “Assessing Medical Publications,” December 2007
4. I prefer printed (not electronic) versions of:
Peer-reviewed scientific journalswith original studies 45.9% (61) 27.1% (36) 23.3% (31) 5 133
Scientific journals whichpublish review papers 39.8% (53) 38.3% (51) 18.8% (25) 4 133
Textbooks 44.4% (59) 28.6% (38) 21.1% (28) 8 133
Medical newspapers andnews magazines 28.2% (37) 42.0% (55) 21.4% (28) 11 131
answered question 134
skipped question 0
Source: Survey Monkey “Assessing Medical Publications,” December 2007
Thank you to all those who participated and congratulations to Dr. Joyce Rauch of Montreal, Quebec who wonthe draw for a CRA mountain backpack!
Have you seen something amazing on the slopes?
Keep your camera close by for this year’s ThirdAnnual CRA Photo Contest from Mont Tremblant!Submit your best scenic and candid photos electronically by March 10th and you’ll have achance to win a CRA mountain backpack!
Please email entries to Mandi Watson:[email protected]
Photo Contest2008
Publication of The Journal of the Canadian Rheumatology Association is madepossible through an unrestricted educational grant from Pfizer Canada.
The 2007 ACR Meeting in Boston
Zoom Zoom trying to make an extra buckselling the CRAJ at the hockey game.
The Divas of Canadian Rheumatology!
How come guys from “The Rock” always have two girls?
How come girls from Toronto always have three guys?
Hurry up and take the picture Glen so we can go back to partying!



![Jq e`epu]j` o eaj a - University of Cambridge · Published by Maney Publishing (c) IOM Communications Ltd Craj lnkbaooekj]hdeopkne]jokbo_eaj_ad]ra okia+ peiao hkopoecdpkb pda e`a]h](https://img.pdfslide.us/doc/110x75/5c77d5d009d3f23a068c2ca1/jq-eepuj-o-eaj-a-university-of-published-by-maney-publishing-c-iom-communications.jpg)