Embed Size (px)
Citation preview

Revising a Medical School Curriculum: The Iowa Experience
David Asprey, PhD, PA-C, Assistant Dean Office of Student Affairs and Curriculum

Disclaimer
• What I am presenting represents the hard work of hundreds of people
• No conflict of interest to declare

Iowa Experience
• Last major curriculum revision was in 1995 • The College of Medicine had positive outcomes
(nothing was broken) • Large academic health center (1100 full time
faculty, 26 departments, etc…) • More energy devoted to patient care and
research • 150 medical students (100 resident/50 Non
resident), 25 PA students • LCME visit in September of 2009

“It is easier to move a cemetery, than to change a school curriculum”
- Woodrow Wilson

Outstanding Results
• Pass rates for USMLE examinations
excellent
• <1% academic attrition over last decade
• Excellent student satisfaction scores on
AAMC Graduation Questionnaires
• High level of satisfaction with IA graduate
performance in residency programs

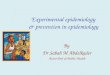
USMLE Step 1 Mean Scores
190
195
200
205
210
215
220
225
230
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011
Me
an
Sc
ore
Year
UI Mean National Mean 228


Case for Curriculum Renewal
• Exponential ↑ in knowledge
• Changing environment – Societal demographics
– Health care reform
• Technologic advances – Availability and management of information
– Methods of delivering curriculum

Case for Curriculum Renewal
• LCME Report identified:
– a need for the CCOM to review its entire curriculum (ED-35)
– a need for greater central oversight for the curriculum (ED-33)
• Dean Rothman’s charge to systematically review, revise and implement a renewed undergraduate medical education curriculum for the CCOM

Modeling Committee Charge
• Design an educational structure that will –address patient and societal needs that are
anticipated to significantly impact healthcare in the near future
– improve integration of basic, clinical, and social sciences within and across all four years
–provide earlier clinical experience and appropriate skill development
–promote learner-centered education, student well-being, engagement, and active learning

Curriculum Renewal Steering Committee
• Met weekly
• Engaged stakeholders in what skills, competencies, etc… were necessary for physicians in 2020
• Reviewed curriculum changes at other medical schools around the country
• Examined the unique opportunities at the university of Iowa
• Agreed to be the “champions” for effective the desired curricular revision.

Curriculum Renewal
• Convened Steering Committee - 11/09
• Charged 4 modeling committees to develop a proposed new curriculum - 4/10
• Held retreat to present the 4 models - 9/10 http://www.healthcare.uiowa.edu/2020/committees.htm
• Gathered feedback on curricular themes of models

Modeling Committee Members
Bridge to the 21st Century 2M: Two Metaphor Education Reciprocal Integration Clinical Centered Education with
Reinforced Foundations
Nancy Rosenthal, Chair
Pathology
George Bergus, Chair
Family Medicine
Vincent Liu, Chair
Dermatology
Marc Pizzimenti , Chair
Anatomy/Cell Biology
Manish Aggarwal, Medical Student JoAnn Benda, Pathology Jason Anderson, Medical Student Charles Clark, Orthopaedic Surgery
Brandon Alleman, Medical Student Allison Boardman, Medical Student Rick Axelson, OCRME Mara Determan, Medical Student
Jill Bowman, Medical Student Amy Dowden, Internal Medicine Donald Brown, Internal Medicine Mary grace Elson,
Obstetrics/Gynecology
Joseph Chen, Orthopaedic Surgery Randy Grout, Medical Student Paul Christine, Medical Student Jeff Emrich, OSAC
Eve Clark, Radiology Collin Kreple, Medical Student Sarah England, Physiology/Biophysics Jill Endres, Family Medicine
Kristen Gerjevic, Medical Student Linda Madson, Psychiatry Daniel Fox, Medical Student Joshua Fischer, Medical Student
Hans House, Emergency Medicine Nick Pantazis, Anatomy/Cell Biology Michael Haugsdal, Medical Student Jaci Haugsdal, Medical Student
Janna Lawrence, Hardin Library Benjamin Reinking, Pediatrics Darren Hoffmann, Anatomy/Cell
Biology
Eric Kaiser, Medical Student
Frances Meyer, Internal Medicine Penny Rembolt, OSAC Sobia Khaja, Otolaryngology Paul Leonard, Anesthesia
Jeff Pettit, OCRME Adrienne Samar, Medical Student Jeff Murray, Pediatrics Erwin Shibata, Physiology/Biophysics
Peter Rubenstein, Biochemistry Deborah Segaloff,
Physiology/Biophysics
Amal Shibli-Rahhal, Internal Medicine Jack Stapleton, Internal Medicine
Kate Thoma, Family Medicine Jane Viner, Medical Student Mark Smith, Radiation Oncology Michael Takacs, Emergency Medicine
Teri Thomsen, Neurology Linda Walton, Hardin Library Sonia Sugg, Surgery Kelly Thormodson, Hardin Library
Robert Yang, Orthopaedic Surgery Liz Takacs, Urology Jerry Weiss, Internal Medicine
Christine Ziebold, Pediatrics Gerry Wickham, OSAC
Ann Willemsen-Dunlap, Anesthesia
William Zeitler, OSAC

Potential Curriculum Models
• Discipline based (current)
• Organ based
• Complaint based
• Mechanism of disease (and health) based
• Etc…


Themes from Curricular Models
• Greater integration of basic/clinical/social sciences across 4 years
– Sub-cellular/molecular focus of scientific inquiry makes collaboration between basic science and clinical faculty even more important
• Organizing themes or principles
– Conceptual organization of knowledge leads to better learning
• Earlier clinical exposure
– Models suggest ambulatory experience, which more accurately reflects delivery of care
• Individualized educational programming
– Current curriculum is more structured than most

The 3 I’s
• Integration
• Innovation
• Individualization

Integration: What and why?
• Goal of curriculum is to promote student learning through knowledge discovery to greater extent than receipt
• Integration a means for improved learning not just a reorganization
• Integration of basic and clinical should emphasize the cognitive activity that occurs within the learner
• Session level integration most important
– Cause and effect: creates a framework (narrative)
– Contextualization demonstrates basic concept in a clinical situation
– Concept is not an abstraction but demonstrably applicable

Integration: Multi-layered
• Guiding principle: create deliberate structure and links to guide student learning and organization of new material as it is acquired and revisited
Curriculum design
Course development
Session level (day to day) Importance of narratives
Macro
Micro
Faculty/Staff • Basic Science • Clinical Departments • Educators • Course/clerkship

Individualization
• Clinical pathways with tailored educational experiences during final 3-5 semesters – Generalist/undifferentiated
– Medical
– Interventional
• Distinction tracks: begin in M1 year * – Research
– Service
– Medical education
– Global health
– Arts and humanities
* Exploring MA options

Innovation
Implemented 2013
Implementation 2014
• Triple helix (spiral & exemplars) – Three strands throughout all 4
years • Medicine and Society (MAS)
• Clinical and Professional Skills (CAPS)
• Mechanisms of Health
and Disease (MOHD)

Innovation (cont)
• Pre-clinical preparation completed by end of 3rd semester (integrating exemplars)
• Core clinical clerkships completed by end of 5th semester – basic science foundation of clinical practice
• Integrating exemplars and modules
• Final 3 semesters flexible – Required courses, selectives and electives
– basic science foundation of clinical practice • basic science foundation of clinical practice

Individualized Learning
• Increased elective time by 4 weeks during clinical years
• Greater variety of clerkship electives – New 2-week clerkships
• Increased flexibility in required clerkships – Selectives (Uro/Rad/Derm/Ophtho/LabMed-EKG)
• Increased elective distinction tracks – Research, Service, Teaching, Humanities, Global
– Developing Rural Medicine Program
• Expanded Distinction Tracks

Innovative Learning
• Lecture recording and podcasting – Decreased lecture and increased
discussion
• 3-D cyber anatomy • Utilizing EHR to deliver cases while
learning to utilize EHR • Exploration of new teaching strategies
(TBL, flipped classroom, Khan Academy, etc…)


CCOM Curriculum Update

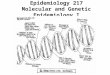
CCOM Revised Curriculum

Clinical and Professional Skills (CAPS) The goal of CAPS is to provide students with the knowledge, skills and attitudes required for professional development and clinical excellence including the sense of inquiry and lifelong habits of skill acquisition, self-assessment and reflective practice. CAPS offers sequentially more challenging clinical experiences across the four years, repeated practice opportunities, observation and feedback, simulations and self-directed learning and reflection.

Medicine and Society (MAS) consists of three consecutive, integrated courses in which students learn about disease prevention, health promotion services, public health, epidemiology, health services organizations and delivery, and community dimensions of medical practice.

In Medical Gross Anatomy students learn to identify the various components comprising the human body and how their structures and locations relate to their functions. This includes complete dissection of the human body. The course provides students with much of the new language they will need to communicate accurately and specifically with patients and other clinicians.

Foundations incorporates genetics, embryology, molecular biology, biochemistry, cell biology and histology. Students will learn the molecular events required for cellular life and describe how cells grow and interact to form the basic tissues of the human body. This course provides the necessary framework to begin to explore the six Mechanisms of Health and Disease.

The Mechanisms of Health and Disease (MOHD) curricular strand is comprised of six multi-system mechanisms. MOHD 1 and 3 cover the mechanisms of Oxygenation, Metabolism, and Genetics/Development. MOHD 2 and 4 cover the mechanisms of Immunology/Inflammation, Locomotion/Integument, and Neuropsychiatry.

In the Core Clerkships students will complete preceptorship in Family Medicine, Outpatient Internal Medicine, Community Based Primary Care, Inpatient Internal Medicine, Neurology, Obstetrics & Gynecology, Pediatrics, Psychiatry and Surgery. As a continuation of the integration design, basic science content is also being taught during the clerkship phase to ensure students are founded in the basic sciences of clinical medicine.

The individualized PATHWAYS component of the curriculum will include a menu of recommended selectives and electives for students choosing a specific pathway. These will be based on the student’s chosen future career in order to help individualize medical education and tailor it to fit the student’s needs during the next phase of their training and throughout their career. Three broad pathways are envisioned Generalist, Interventionalist, and Undifferentiated.

Lessons Learned
• Begin with the end in mind…what knowledge skills and abilities will your graduates need?
• Embrace the unique features of your University and Medical School (don’t simply copy another school’s curriculum)
• Involve key stake holders early and often
• Include students in the process

Lessons Learned
• Look for efficiencies that are win-wins (MD/PA)
• Inertia vs momentum
• Resist thinking exclusively about what will this do to me/my job
• Role of faculty development
• Involve experts in evaluation/assessment from the beginning
• Curriculum revision will be a lot of hard work but is also immensely rewarding