Embed Size (px)
Citation preview

The Intersection of Population Health & the Health Care Workforce – Considerations for the Future
Anthony Keck EVP System Innovation and Chief Population Health OfficerBallad Health [email protected]
June 28, 2018

About Ballad Health
• Created by the merger of Mountain States Health Alliance and WellmontHealth System eff. 02.01.2018
• 21 hospitals, including:
o Three tertiary centers
• Two Level I and one Level II trauma
o Thirteen community hospitals
o Dedicated children’s hospital
o Freestanding inpatient behavioral health
o Three critical access hospitals
• 500+ free-standing SNF beds
• Outpatient MAT clinic
• Wound care, sleep labs, home care, DME, hospice, retail pharmacies
• 800+ provider group practice
June 28, 2018Presentation Title
2

About Ballad Health
• 15,000+ team members
• 106,940 annual inpatient discharges
• 477,647 annual ER visits
• 2.8 million+ annual outpatient visits
• $2.17 billion annual revenue
June 28, 20183

About Our Region
June 28, 20184
• Mountainous terrain ofSouthern Appalachia
• Serving 29 counties in Tennessee, Virginia, Kentucky and North Carolina
• Approximately 1 million residents in the service area

June 28, 20185

About Our Region
State Health Rankings:
June 28, 20186
➢ Core “urban” counties of Washington and Sullivan rank 2 and 4 for clinical care
County Health Rankings – Health Outcomes by County
TENNESSEE VIRGINIA
Washington 19 of 95 Washington 63 of 133
Sullivan 25 of 95 Grayson 72 of 133
Greene 41 of 95 Wythe 78 of 133
Carter 47 of 95 Scott 92 of 133
Hamblen 55 of 95 Smyth 102 of 133
Unicoi 64 of 95 Russell 113 of 133
Hawkins 70 of 95 Tazewell 118 of 133
Johnson 77 of 95 Lee 119 of 133
Hancock 86 of 95 Buchanan 122 of 133
Cocke 92 of 95 Wise 124 of 133
Dickenson 125 of 133
TENNESSEE: 45th of 50 VIRGINIA: 19th of 50

Social Determinants of Health
June 28, 20187

Accountable Health Communities Grant
• $2.52M in funding over 5 years to test if navigation services to Medicare and Medicaid beneficiaries would lower the overall cost of care
• 75,000 eligible Medicare and Medicaid beneficiaries will be screened for emergency department utilization and unmet social determinants of health
o Screenings occur in emergency departments, labor & delivery, inpatient psychiatric, and primary care providers
o All beneficiaries with identified unmet needs will receive community referral summary listing local resources
o At least 2,048 beneficiaries will receive navigation services (must have reported two or more ED visits in past 12 months and at least one unmet social need)
• Partnering with Virginia Department of Medical Assistance Services (DMAS)
8

AHC Grant - Screening Tool (Self-Reported)
• ED utilization of past 12 months
• Describe current living situation (i.e., steady place to live or not, mold, pests, lack of heat, water leaks, smoke detectors, lead pipes/paint, working oven)
• Within past 12 months, ever worried about having enough food or food running out
• Any issues with reliable transportation for daily living
• Within past 12 months, have any utility companies threatened to shut off services
• How often is your safety threatened (i.e., physically, insults, threats with harm, screaming/cursing)
• Series of demographic questions (i.e., gender, ethnicity, race, education level, size of household, annual household income)
9

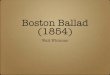
AHC Grant - Pilot Experience - Screening
10
2,547
1,602
1,165
598
256
0
500
1,000
1,500
2,000
2,500
3,000
BeneficiariesScreened
High RiskBeneficiaries
Beneficiaries withNeeds
BeneficiariesRandomized
Nu
mb
er o
f C
om
ple
ted
Screen
ing
s
Pilot-Screening Results(As of 4/17/18)
Control
Navigation
854

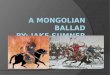
AHC Grant - Pilot Experience - Screening
11
32%(815)
21%(525)
4%(110)
19%(478)
14%
(358)
0
100
200
300
400
500
600
700
800
900
Food Housing Safety Transportation Utility
Percen
t o
f C
om
ple
ted
Screen
ing
s
Pilot-Screening Results(As of 4/17/18)

A new model is needed
• Unlock some portion of the 30%+ of waste in the health system by reducing the wasteful duplication of resources created by two competitors simply shifting market share back and forth a few percentage points each year.
• Redirect these savings into better access and quality and invest in community based resources to improve the social determinant profile of our region.
• Build responsive services and systems by listening better to our patients and community rather that “medsplaining”.
June 28, 201812

June 28, 201813
Certificate of Public Advantage & Cooperative Agreement

COPA Terms of Certification / Virginia Order Authorizing Cooperative Agreement
• Tennessee TOC: 116 Pages• Virginia Order: 151 Pages
• TOC 7 Sections
o Definitions
o Statutory Requirements and Factual Findings
o Monetary Obligations and Commitments
o Non-Monetary Obligations and Commitments
o Managed Care Contracts and Pricing Limitations
o Active Supervision
o Miscellaneous Provisions
14

Ballad Health’s investments in our region
$85 million toward behavioral health to create capacity for residential addiction recovery services and develop community-based mental health resources, like mobile health crisis management teams and intensive outpatient treatment options.
$85 million in academics and research to educate and train healthcare providers that are in short supply, and build the research capacity of local universities and colleges to spur outside research investment.
June 28, 201815

Ballad Health’s investments in our region
$75 million to address key population health needs, focusing on some of our most serious health challenges like diabetes, heart disease and infant mortality.
$28 million toward rural health services, including better access to same-day primary care, support for maternal and prenatal health, and more.
June 28, 201816

Ballad Health’s investments in our region
$27 million toward children’s services to create pediatric emergency rooms in Kingsport and Bristol and expand pediatric telemedicine, mobile health and specialty clinics in rural areas.
$8 million to enable health information exchange to allow healthcare providers both inside and outside of Ballad Health to easily share health information that improves patient care.
June 28, 201817

Indices and Measures
• Population Health Index – 26 measures
• Access to Care Index – 28 measures
• Quality Index – 16 measures
18

Indices and Measures – Population Health
Category COPA MeasureSmoking Smoking (% of adults self-reported as smokers)
Smoking Mothers who smoke during pregnancy
Smoking Youth tobacco use
Obesity Physically active adults
Obesity Physically active students
Obesity Obesity- Counseling & Education
Obesity Overweight and obesity prevalence among TN Public School Students
Breast Feeding Average mPINC score
Breast Feeding Breastfeeding initiation
Breast Feeding Infants breastfed at six (6) months
Substance Abuse NAS Births
Substance Abuse Drug deaths
Substance Abuse Adults - Prescription drugs
Vaccinations Children - On-time vaccinations
Vaccinations Vaccinations - HPV Females
Vaccinations Vaccinations - HPV Males
Vaccinations Vaccinations - Flu Vaccine, older adults
Child Health Teen pregnancy rate
Child Health 3rd grade reading level
Child Health Dental sealants (children 6-9)
Child Health Dental sealants (adolescents 13-15)
Child Health Infant mortality
Child Health Low birthweight
Mental Health Frequent mental distress
Diabetes # of people with pre-diabetes identified and referred to a prevention program
Mortality Ratio of premature deaths (higher density / lower density counties)
19

Indices and Measures – Access to Care
20
Category COPA MeasureED Pediatric Readiness of ED
ED Excessive ED Wait Times
Patient Access Specialist Recruitment and Retention
Patient Access Personal Care Provider
Utilization Preventable Hospitalizations - Medicare
Utilization Preventable Hospitalizations - Adults
Screenings Screening - Breast Cancer
Screenings Screening - Cervical Cancer
Screenings Screening - Colorectal Cancer
Screenings Screening - Diabetes
Screenings Screening - Hypertension
ED Asthma ED Visits - Age 0-4
ED Asthma ED Visits - Age 5-14
Perinatal Prenatal care in the first trimester
Mental Health Follow-Up after Hospitalization for Mental Illness (Children 6-17)
Mental Health Follow-Up after Hospitalization for Mental Illness (Adults 18+)
Mental Health Antidepressant Medication Management - Effective Acute Phase Treatment
Mental Health Antidepressant Medication Management - Effective Continuation Phase Treatment
Substance Abuse Engagement of Alcohol or Drug Treatment
Substance Abuse SBIRT administration - hospital admissions
Substance Abuse Rate of SBIRT administration - ED visits
Patient Experience Patient Satisfaction and Access Surveys
Patient Experience Patient Satisfaction and Access Surveys - Response Report

June 28, 201821
Our Approach

Expanded Chronic Care Model

ECCM Model: Ballad Population Health Focus and Strategies
1. Develop population health infrastructure within the health system and the community• Ballad Department of Population Health• Accountable Care Community
2. Redesign Ballad as a community health improvement organization• Delivery system improvement and redesign• Information systems and decision support and information
exchange• Improved self-management and personal skill development
3. Enable community resources and sound health policy• Strengthen community action• Advocate for sound health policy• Create supportive environments
June 28, 201823

Behavioral Health
Children’sServices
Rural Services
Population Health
Strategic Themes Across All Plans
• Early Intervention/Strong Starts
Theme #1
• Alternative Points of Access
Theme #2
• Team-Based Care & Navigation
Theme #3
• Integrated Behavioral Health
Theme #4

Workforce demands
Community based health workers
• Peers
• Parish nurses
• Promotoras/CHWs
• Navigators
• Community engagement specialists
Behavioral health specialists
• Psychiatrists
• Psychologists
• LCSW
Mid-level providers
• APNs
• PAs
June 28, 201825
Technologists
• Data scientists
• Programmers
• Operational excellence
Primary care capacity and productivity
Competencies
• Team based care
• Patient engagement/active listening/motivational interviewing
• Community collaboration
• eHealth
• Implementation science

June 28, 201826
Workforce Considerations for Population Health

What is population health?
1: Policies, systems and services designed to help each individual reach their fullest potential.
2: Whatever the payor says it is
June 28, 201827

Workforce considerations
Relationship with a personal care provider is a strong predictor of better health. We are wasting considerable existing primary care capacity.
• Ineffective and burdensome data entry and charting
• Patients we don’t need to see physically or at all which clog up the system for those who need it most
• Activities better done by others
• Poor scheduling practices
• Lack of assistive technologies
• Too much low value care/too little high value care
• Too much “futile” care i.e care rendered useless because of unacknowleged social/environmental limitations
June 28, 201828

Workforce Considerations
We need to get serious about behavioral health
• BH is a/the leading cause of disease burden in the world yet the private health care sector is generally content to let the government worry about it.
• Mental Health Parity has not been achieved
• Behavioral health training needs to be improved in primary care in residency and through continuing education
• We are not training a sufficient number of behavioral health providers
• We should expand capacity to provide telepsychiatry and to provide teleconsulting support to primary care – especially pediatrics
June 28, 201829

Workforce Considerations
We need to change the way we train health care and public health professionals
• Interprofessional education and training (capstones, simulation, table top exercises)
• Poverty simulations and anti-racist training
• Public health and health systems cross-training
• Implementation science
• Culture of safety/failure analysis
• Communication – especially listening
We need to think about who we recruit. We need more providers who look like the community and have shared life experiences
June 28, 201830

Workforce Considerations
FFS based payment systems inhibit population health
• FFS based payments systems tend to favor licensed professionals performing specifically defined health care services
• Global payments allow providers to determine what activities performed by what level of resource bring the most value to the patient
• Consolidation in hospitals and health systems combined with growing physician employment – especially primary care - may be inhibiting acceptance of more risk based contracts
We need to be comfortable with non-licensed professionals: peer counselors and mentors, community health workers, etc. We need to understand what they bring to the table and not try to “professionalize” them.
June 28, 201831

June 28, 2018Presentation Title
32