Embed Size (px)
Citation preview

The internatianai Journai of Periodantics S Restarative Dentistry

141
Socket Seal Surgery Combined WithImmediate Implant Placement:A Novel Approach for Single-ToothReplacement
CobiJ. Landsberg. DMD'
Guided bane regeneration procedures around immediafety piacedimpiants may resuit in weii-asseaintegrated fixtures, but because of com-piexed flap manipulatian. the functionai. phonetic, and esthetic resuit moybe unsatisfactory, especiaiiy when performed in the maxiiiary onteriorregion of the mouth. For betfer results a modified ridge preservatian tech-nique, called "socket seai surgery " which combines bane and satt tissuegrafting and is performed prior fo impianf piacement has been suggesfed.A nove/ approach is presenfed in which sacket seai surgery is performedsimuitaneausiy with impianf piacement ta achieve optimai repiooement ofan extracted maxiiiary anterior toath. (inf J Periodont Resf Denf1997,17:141-149,)
'Private Practice, Tel-Aviv, Israel.
Reprint reauests. Or Cobi J. Landsberg, 53 Gordon St, Tel-Aviv, IsraelÓ4394. E-mail: [email protected],ii
Alveolar ridge résorption foliow-ing tooth removol is a physiolog-icolly undesirabie but on un-avoidabie phenomenon.' inmost ooses the residual ridgedefecf becomes o problematicsite that is difficuif fo resfore,both functionally ond estheti-cally either by a "oonventionai"tooth-supported restorationor by an implant-anohoredrestoration. Reoentiy the devel-opment of guided fissue regen-erafion (GTR) procedures fhatmoy regenerate bone in defi-cient sites of the jows expandedfhe possibilities for impianfpiocement.^-'" These osfeopro-mofive procedures may be per-formed either prior to^'^-^'" orsimuitaneousiy with impiantpiocement.s-'iû.'.io-ia |n eithercase, a membrane barrier isused to oilow only bone-formingceils fo repopulate fhe deficientbony sife. The membrane thatmust cover the whole bonydefect should, in turn, preferabiybe compieteiy covered by sofftissue during the entire heoiingprocess, which takes ó to 9
Voiumel7, Number 2,1997
142
months for sufficient maturationof the regenerated bone to beachieved,^"'2
However, immedioteiy aftertooth extraction a soft tissuegap is created on top of theridge (as a result of the opensocket), and submerging themembrane under protectivesoft tissue may necessitate com-piex fiap manipulation.^''"^^ Thisusuaiiy involves some undesir-able side effects, such as mar-ginal gingival recession of theadjacent teeth and ioss of kera-tinized gingiva and interdentaipapiilary height." Such soft tis-sue ioss may significontly com-promise esthetics and phonet-ics, especiaily in fhe maxilioryanterior region of the mouth. Toprevent fhese undesirableresults, a modified regenerativeapproach, calied "sockef sealsurgery" (SSS), has been sug-gested in which flap elevation isnot performed while bone andsoft fissue grafts are used, thusenabling opfimai preservationof fhe ridge topography imme-diately after tooth extraction,'^However, it takes 6 to 9 monthsfor regenerated bone to be-come mature ond suitable forimpianf piaoemenf. To eiiminatethe waiting period betweentooth extraotion and implantplacement, a modified tech-nique is presented, whereby SSSis performed simultaneously withimpiant placement immedi-ateiy posfextracfion.
Clinical procedure
Exomination and assessment ofthe impiant site
As no flap elevation is per-formed prior fo impiant place-ment, the topography andquaiity of the ridge should bethoroughiy evaiuafed ciinicaiiy,radiographicaliy, and occasion-ally by computerized tomo-graphic (CT) scan, if, for exam-ple, a iarge buccopalatal bonydepression exists apical to thetooth to be removed, flap eie-vation and a convenfionaimembrone borrier shouid pre-ferabiy be used for ridge aug-mentation prior fo or simulfane-ousiy wifh implanf piacemenf.
Surgical steps
Sooket preparation. Affer gentietooth extraction without fiapelevafion, fhe fresh sockef isthoroughly debrided of granuia-fion tissue and residual peria-dontai iigament fibers. Thesocket bony walls are further de-corticated fa increase the par-ticipation of endosteai bone-forming ceils in fhe wound. Thegingival walls at the socket ori-fioe are gentiy de-epithelializedby a water-cooled high-speedcoarse diamond bur, therebyexposing fhe vascuiarized lam-ina propria responsibie for nour-ishing and revascularizing thesoft tissue graft to be piacediater at the socket orifice.
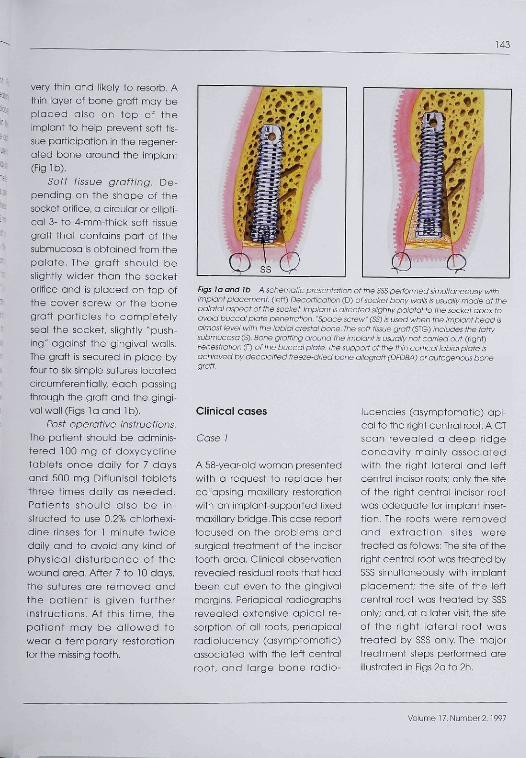
impiant piacement. Forfunctional and esthetic reasons,the impiont should be placedaxiaiiy and centraily in thesocket orifice. To achieve opti-mal implant position, the use ofa guiding surgical stent may behelpfui. A medium diamefer(usuaiiy 4 mm) impiant is pre-ferred, and the impiant heodshouid be located 1 to 2 mmapioai to the iabiai crest, oroccasionaily level with fheiabiai cresf. In this situation amodified caversorew fhaf hasno head ("space screw") isused to minimize impianf protru-sion from the socket and toailow adequate space forplaoement of the soft tissuegratt. Usually the ridge con-verges toward the nasal spine;therefore drilling should bedirected siightiy paiatai fo thesocket apex to avoid penefro-tion inta the vestibuiar mucosa(Fig la). However, there are situ-ations in which, for anatomic orprosthetic reasons, the driiismusf be directed in such a waythaf slight fenestration of thebuccGi piafe may occur. If isthen extremely important not topenetrate buf oniy lift up theperiosteum wifh the driiis andsubsequently with the impiantitself (Fig Ib).
Bone grafting. Decaicifiedfreeze-dried particuiated boneallograft (DFDBA) or powderedautogenous bone harvestedfrom the asteotomy is graftedbetween the impiant body andthe iabiai plate if the latter is
Tiie internatianai Journai af Periodontias & Restorotive Dentistry
143
very thin and likely fo resorb. A'^ thin iayer of bone groft may be^ placed also on top of fhe" implant to heip prevent soft tis-
'* sue participation in the regener-ated bone around the implant
•• CFiglb)." Saff tissue grafting. De-'I* pending on the shope of the^ socket orifice, a circular or eliipti-
oal 3- fo 4-mm-thick soft tissuegraft that contains part of fhesubmucosa is obtained trom thepalate. The graft should beslightly wider than the socketorifice and is placed on top of
•" the cover screw or the bonegroft perfides to compieteiyseal the socket, slightiy "push-ing" against the gingivai wolis.The graft is secured in place byfour to six simple sutures locatedcircumferentially each possingthrough the graff and the gingi-vai wail (Figs 1 a and 1 b).
: Posf operative insfructions.The patient should be odminis-tered 100 mg of doxycyclinetablets once daily for 7 daysand 500 mg Diflunisal tabietsthree times daiiy as needed.Patients shouid oiso be in-structed to use 0.2% chlcrhexi-dine rinses for 1 minute fwicedaily and to ovoid ony kind ofphysicol disfurbance of thewound area. After 7 fo 10 days,the sutures are removed andthe potient is given furfherinstrucfions. At this time, fhepatienf moy be ollcwed fowear a temporary restorationfor the missing tocfh.
Figs la and lb A schematic presentation of the SSS performed s¡mu¡taneous¡y withimplant placement, (left) Decorflcafion (D) of socket bony walls is usuoliy made at thepalatal aspect of the socket implant is directed sUghtiy paiatai to the socket apex toavoid buccai p¡ate penetration. 'Spaoe screw'(SS) is used when the impiant head ¡salmost Ievei with the ¡obial crestai bone. The soft tissue graff (STG) includes the taffysubmucosa (S) Bone grafting around the implant is usually not carried out. (right)Fenestration (F) of the buocai p¡ate. The support of the thin corticoi labial plate isachieved by decaicitied freeze-dried bone aiiogroft (DFDBA) or autogenous bonegraff.
Clinical cases
Cose /
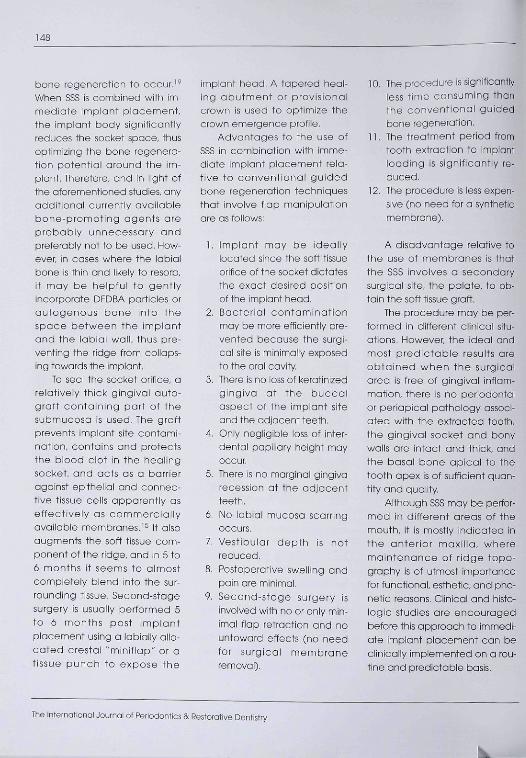
A 58-year-old woman presentedwifh o request to repiace hercciiapsing maxiliary restorationwith an implant-supported fixedmaxiiiary bridge. This case reportfocused on fhe probiems andsurgicoi treatment of the incisortooth area, Ciinical observationrevealed residuai roots that hadbeen cut even to the gingivoimargins, Periapicai radiographsreveaied extensive apical ré-sorption cf ali roots, periapicairadiolucency (asymptomotic)ossociated with the left centrairoot, ond large bone radio-
iucencies (asymptomatic) api-cal to the right central root, A OTscan revealed o deep ridgeconcavity mainly ossociafedwifh the right lateral ond leftcentral incisor roots; only the siteof fhe right centrai incisor rootwas adequate for impianf inser-fion. The roots were removedond extracfion sifes weretreated os foiiows: The site of theright cenfrai root was treated bySSS simuitaneousiy with impiontpiacement; the site of the leftcentral root was treoted by SSSoniy: and, at a later visit, the siteof fhe right loterai root wastreated by SSS oniy. The majortreatment steps performed areillusfrated in Figs 2o to 2h.
Volume 17, Number 2,1997

144
Fig 2a (above) Clinicql view of maxii-iary incisar toath area.
Fig 2b (right) Radiographie periapicolview ot the raot of the ieft centralincisor ond the rodiolucency apical tathe apex of the roat of the right lateralincisar
Fig 2c Brónemark fixture piacedimmediateiy pasfexfrqctlon of the rightcentral raot. Note the intact soft tissueorifice of the sockets.
Fig 2d (top) Gingival groft placed ontop of the cover screw and sutured.Freeze-dried bone particles are graftedqniy in the neighboring socket.
Fig 2e (bottom) Another gingivalautograft is placed to seai the sacketof the ieft centrai raat.
Figs 2f. 2g. and 2h Five mcnths posf-SSS in the extraction sites af the central rootsand 4 months post-SSS m the extraction site of the right lateral roat. (top left) Thewidth of the residual ridge has been maintained, (bottom left) The implaht is circum-ferentiqlly surraunded by bone and the ridge topography in the incisor teeth areqhas been mqintained. (right) Radiqgraphic periapicai view. The tixture appears wellasseointegrated and pqsses aiose to the bone radiqiucehcy thqt was Initialiy pre-sent.
The International Journal of Periodontics & Restorative Dentistry

145
Case 2
A ó7-year-old man presentedwifh pain associafed wifh themaxillary righf central inciser.Clinical examination revealeda mobile pcrceioin crown withminimai refenfion fo fhe root.The neighboring teeth werecompieteiy intoct except forthe righf laferai incisor, whichhad a Class 111 discolored oom-posife resforafion. The crownaftached fo ifs posf was eosilyremoved, revealing a sfoblebuf moderafely fractured roof.No potholcgy v os defectedradiographicGily, and a CTscan of fhe orea reveoled oslight ridge concavity apicoi tofhe roof apex,
Atter a defaiied expiano-tion of fhe treatment options tothe pofient, the patient choseto repiace the toofh with a sin-gle implant-supported resfo-rofion, Sockef seal surgery,combined with immedioteimpianf piacemenf as previ-ously desoribed, was fhe surgi-coi treatment selected. Themajor steps pertormed are iiius-frated in Figs 3a fo 3j,
Fig 3a (above) Preoperative moxiiioryonterior teeth of Cose 2. Note theasymmetry of the incisor teeth anoto-my. The orown of the right centrai incisorwas mobile.
Fig 3b (right) Radiographie view of theorea of the oentrai incisors. Note fheinddeduate crown-root connection.
Fig 3c Bränemark fixture with coverscrew is impianted into the socket.Note the minimoi tissue injury.
Fig 3d Freeze-dried bone particlesore pioced on top of the cover screw.
Fig 3e Gingival aufogroft sutured togingivqi wails of the socket. Note initiaiqnohorqge of graft by two needles.
Fig 3t Gingivoi autogrort is securedinto place by six simple sutures.
Voiume 17, Number 2,1997

146
Fig 3g Gingival autogroft at 1 manth.Note the complete seal of the sockefand the adequate ridge topography.
Fig 3h Five months posf impiantplacement. Note fhe adequate widthof the ridge and the impianf in optimaiposition
Fig 3i Labioi view cf the restoredceramic crown. Note the natural crownappearance and adequate surround-ing gingivai tissue. (Prosthodontist: Dr I.Landsberg, Tel-Aviv. Israei: DentaiLobaratcry: Nobiiceram. Tei-Aviv. israei.)
Fig 3¡ i?adiographic periapical view afthe resfored tooth. Note that the fixtureappears to be weii osseointegrated.
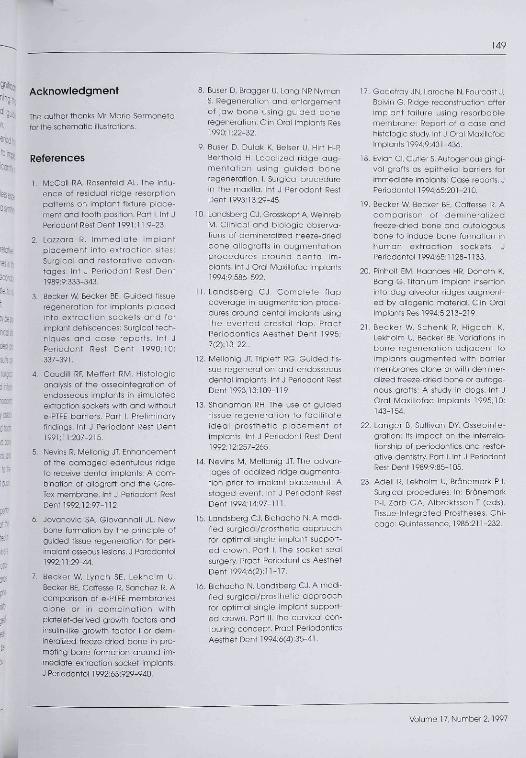
Figs 4a to 4d (Top ieft) Steri-Oss impiant is inserted info the sacket. DFDBA is piocedbetween the impiant and a thin iabiai plate, aop rigtit) Six months foiiowing implantinsertion there is adequate ridge topography and o biending ot the san tissue graftwith the surrounding mucoso. (Bottom ieft) implant is exposed with a smaii diametertissue punch. Note the adequate quantity and quaiity of the soft tissue. (Bottomright) Tapered heaiing abutmenf is cannected to the impiont to recontaur the peri-abutment mucasa. Not minimqi bianching of fhe compressed soft tissue.
Cases
An 18-year old woman pre-sented with pain associatedwith a traumatized maxillary
right central incisor Ciinicai andradiographie examination re-vealed a verticaiiy fracturedroot with a poor prognosis.Affer patient consultation, the
decision was made to repiacethe root with an immediateiyinserted impiont using SSS. Themajor steps performed are illus-troted in Figs 4a to 4d.
The Internatipnai Journal of Periodontics & Restorative Dentistry

147
Discussion
Socket seal surgery is a modifiedregenerative procedure per-formed immediateiy postextrac-tion and is used mainly in themaxillary anterior region. If oanbe used prior to impiant place-ment'^ and, when foliowed byfhe cervicai contouring con-cept"' at the prosthetic phase,may aohieve an optimal func-fional, phonetic, and estheticresult. The SSS may also be usedwith very satisfactory resultsfor ridge preservation prior toconvenfionai toofh-supporfedrestorative cases. However, inimplant cases, a 6 to 9 monthpostsurgery waiting period isrequired for the regeneratedbone to mature and becomesuifoble for implanf place-ment.'^ To minimize the treat-ment period, if is advantageousto place impiants directiy intofresh extraction sites. It has beenwidely demonstrated that imme-diate impiant placement maybe predictably successtui when"conventionai" GTR fechniquesare used simuifaneously withimplanf piacement.^'''^•'•'^"'^Different membrane barriers,such as e-PTFE, "'' coliagen,'''ond others, have been usedin this regard. Recently a modi-fied approach was describedin which autologous gingivalgraffs were used as "epithelialbarriers" for guided bane regen-eration in defects associatedwith immediateiy placed im-plants, ^ it was suggesfed that
exoiusion of fiap epitheiium fromthe wound area may be suffi-cient for bone promotionaround fhe implant. In eithercase, reiativeiy complex flapmanagement is involved withsubsequent loss of kerafinizedtissue and interdental papiiiaryheight the restoration of whichmay require a challenging sec-ondary plastic soft tissue surgery.In contrast, the SSS does nofinvolve Hap eievation, thus mini-mizing traumatic injury to thesoft and hard tissue compo-nents of the sockef and optimiz-ing the preservation of ridgetopography.
As desoribed previousiy, amedium diameter impiant ispreferred as it may be iocaiizedlevel with the labial crestalbone, thereby minimizing thesuioular depth around the abut-ment and crown and optimizingthe emergence profiie of thecrown. A smaiier diameter im-plant is inferior in strength andmay have fo be iocaiized toofar subcresfaiiy fo allow the de-sired emergence profiie of thecrown, thereby increasing suicu-iar depth and compromisinghygiene maintenance. A iargerdiameter (4.5 to 5.5 mm)impiant may be superior, but themaxiiiary anterior ridge is usuallytoo thin to contain it.
As shown, there are situa-tions in whioh the impiant mayhave tenesfrafed the bucoaibone to a iimifed extent. If theperiosteum at the fenestrationsite is oniy siightiy lifted up by
the implant with no signifioantinjury, it may be assumed thatthere wiii be no significant nega-tive impact on the osseointegra-tion process and the final stabiiityond long-term function of the im-pianf. This ossumption is sup-ported by ciinicai documenta-fion that demonstrates thepossibility of iiffing up the perio-steum^^ or fhe Schneiderianmembrane of the maxillarysinus,^^ foiiowing intentionaipenetration of the cortioaibone by the implant apex with-out an untoward effecf.
Autogenous bone graft orDFDBA, when pioced oroundand on top ot the implant maybe used to induoe or oonducebone formafion around theimplant maintain spoce underthe gingival graft to maximizecoronal bone regenerafion,prevent ooilapse of fhe ridgewhen bony wails are thin andcan resorb, or as a substrate torlocal delivery of growth factors.
The use of DFDBA in boneregenerative prooedures hasbecome controversiai. Someolinioal and histoiogic sfudiesand case reports demonstratethe beneficioi use of DFDBAprior fo or simultaneous withimplant piacement, especialiyin noturally nonspace-makingbony defecfs,^'''^-^'' In contrastofher studies"-^^ claim no con-tributory or inhibitory effect ofDFDBA on the regenerationprooess, especiaily in extraotionsockets that are consideredideal defeots for spontaneous
yolumel7,Number2,1997
148
bone regeneration to occur.'''When SSS is combined with im-mediate impiant placement,the impiont body signiticantiyreduces the socket space, thusoptimizing the bone regenera-tion potentiai oround the im-piant. Therefore, and In iight otttie atorementioned studies, anyadditional currentiy avaiiabiebone-promoting agents areprobabiy unnecessary andpreferably not to be used. iHow-ever, in cases where the labialbone is thin and lii<eiy to resorb,it may be helpful to gentlyincorporate DFDBA particles orautogenous bone into thespace between the implantand the labiai wall, thus pre-venting the ridge from coiiaps-ing towards the impiant.
To seai the socket orifice, areiativeiy thick gingivai auto-graft containing part of thesubmucosa is used. The graftprevents implant site contami-nation, contains and protectsthe biood clot in the healingsocket, and acts as a barrieragainst epitheiial and connec-tive tissue ceils apparently aseffectively as commerciailyavaiiabie membranesJ^ it alsoaugments the soft tissue com-ponent of the ridge, and in 5 toó months it seems to almostcompietely biend into the sur-rounding tissue. Second-stagesurgery is usually performed 5to ó months post implantpiacement using a labially allo-cated crestal "minifiap" cr atissue punch to expose the
implant head. A tapered heal-ing abutment or provisionalcrown is used to optimize thecrown emergence profiie,
Advantages to the use ofSSS in combination with imme-diate implant placement rela-tive tc conventional guidedbone regeneration techniquesthat involve fiap manipuiationare as follows:
1. Impiant may be ideallylocated since the soft tissueorifice of the socket dictatesthe exact desired positionof the implant head.
2. Bacteriai contaminationmay be mere efficiently pre-vented because the surgi-cal site is minimaliy exposedto the orai cavity.
3. There is no loss of keratinizedgingiva at the buccalaspect of the impiant siteand the adjacent teeth,
4. Oniy negligibie loss of inter-dental papiiiary height mayoccur.
5. There is no marginal gingivarecession at the adjacentteeth.
6. No iabial mucosa scarringoccurs,
7. Vestibular depth is notreduced.
8. Postoperotive sweiiing andpain are minimal.
9. Second-stage surgery isinvoived with no or ohiy min-imal flap retraction and nountoward effects (no needfor surgicoi membraneremoval).
10. The procedure is significantlyless time consuming thonthe conventiohdl guidedbone regeneration.
11. The treatment period fromtooth extraction to impiontloading is significantiy re-duced.
12. The procedure is less expen-sive (no need for a syntheticmembrane).
A disadvantage reiative tofhe use of membranes is thatthe SSS invoives a secondarysurgical site, the palate, to ob-tain the soft tissue graft.
The procedure may be per-formed in different ciinical situ-ations. However, the ideai andmost predictabie resuits areobtoined when the surgicaiarea is free of gingival inflom-mation, there is no periodontaior periapical pathology associ-ated with the e>ctracted tooth,the gingival socket and bonywalls are intact and thick, andthe basal bone apicai to thetooth apex is of sufficient quan-tity and quaiity,
Aithough SSS may be perfor-med in different areas of themouth, it is mostiy indicated inthe anterior maxilia, wheremaintenance of ridge topo-graphy is of utmost importancefor functional, esthetic, and pho-netic reasons. Clinical and histo-iogic studies are encouragedbefore this approach to immedi-ate impiant piacement can beclinically implemented an a rou-tine and predictabie basis.
The International Journol oí Petiodontics & Restorative Dentistry
149
Acknowledgment
The author thanks Mr Mano Sermonetafor the schematic iiiustrations.
References
1. tvicCail RA, Rosenfeld AL. The infiu-ence of residuai ridge résorptionpatterns on impiant fixture piace-ment and tooth position. Part i, int JPeriodont Rest Dent 1991,11.9-23.
2. Lazzora R. Immediate implantpiacement into extraction sites:Surgicoi and restorative advan-tages, int J Periodont Rest Dent1989:9:333-343.
3. Becker W, Becker BE Guided tissueregeneration for impiants p iacedinto extract ion sockets and forimpiont dehiscences: Surgicai tech-niques and case reports, Int JPeriodont Rest Dent 1990:10:337-391,
A. Caudill RF, Meffert RM. Histoiogicanalysis of the osseointegratian ofendosseous impionts in simulatedextraction sockets with ond withoute-PTFE borriers. Port I, Preiiminaryfindings. Int J Penodont Rest Dent1991:11:207-215.
5. Nevins R, Mellonig JT, Enhancementof the dqmqged edentulous ridgeto receive dentai implants: A com-bination of aiiograft and the Gore-Tex membrane, int J Periodont RestDent 1992;!2:97-112.
Ó, Jovanovic SA, Giovonnqii JL. Newbone formation by the principle ofguided tissue regeneration for peri-implant osseous iesions,J Parodontol1992; 11:29-44.
7. Becker W, Lynch SE, Lekhoim U,Becker BE, Coffesse R, Sonchez R. Acomparison of e-RTFE membranesoione or in combina t ion withplatelef-derived growth factors andinsuiin-iike growth faotor I or dem-inerqiized freeze-dried bone in pro-moting bone formation around im-mediate extraction socket implants.J Periodonfol 1992:63:929-940,
8, Buser D, Bragger U, Lang NR NymanS. Regeneration and enlargementof jaw bone using guided boneregeneration, Ciin Orai Implants Res1990:1:22-32.
9. Buser D, Dulak K, Belsei U, Hirt H-RBerthoid H. Localized ridge aug-menta t ion using gu ided boneregeneration. 1, Surgicoi procedurein the maxiiia, Int J Reriodont RestDent 1993; 13:29-45.
10 Lanasberg CJ, Grosskopf A, WeinrebM. Clinical and biologic observa-tions of demineraiized freeze-driedbone allografts in augmentationprocedures around denta l im-piqnts. int J Orai Maxillofoc impionts1994:9:586-592.
11. Landsberg CJ, Comple te f lapcoverage in augmentation proce-dures around dental impiants usingthe ever ted crestai f iap. PractPeriodontics Aesthet Dent 1995;7(2): 13-22.,
12. Meiionig JT, Tripiett RG, Guided tis-sue regeneration and endosseousdental impionts, Int J Periodont RestDent 1993;13:109-119.
13. Shanamon RH. The use of guidedtissue regenerat ion to faci i i tateideai prosthet ic p iacement ofimpiants. Int J Reriodont Rest Dent1992:I2;257-2Ó5.
14. Nevins M, Meiionig JT. The advan-tages of iocaiized ridge augmenta-tion prior to implant piqcement: Astaged event, int J Periodont RestDent 1994:14:97-111.
15 Londsberg OJ, Bichacho N. A modi-tied surgicai/prosthetic approachfor optimal singie implant support-ed crown. Rarf I, The sockef sealsurgery, Rract Periodontics AesthetDent 1994:6(2):ll-17.
16, Bichacho N, Landsberg CJ. A modi-fied surgicai/prosthetic approachfor optimal single implant support-ed crown. Part II. The cervicai con-touring concept, Rract PericdonticsAesthet Dent 1994,ó(4):35-41.
17, Godefray JN, Laroche N, Fourcast J,Boivin G, Ridge reconstruction afterimpiant failure using resorbabiemembrone: Report of a case andhistoiogic study Int J Oral MaxillotocImplants 1994:9:431-436.
18, Evian CI, Cutier S, Autogenous gingi-val graffs OS epitheliai barriers forimmediate implants: Case reports. JPeriodontoi 1994:65:201-210.
19, Becker W, Becker BE, Caffesse R, Acomparison of deminerai izedfreeze-dried bone and autologousbone to induce bone formation inhuman extract ion sockets. JPeriodontol 199465:1128-1133.
20, Pinhoit EM, Haanaes HR, Donoth K,Bang G. Titanium implant insertioninto dog aiveoiar ridges augment-ed by aiiogenic material. Ciin OralImplants Res 1994:5:213-219.
21, Becker W, Schenk R, Higachi K,Lekhoim U, Becker BE, Voriations inbone regeneration od jacent toimplants augmented with barriermembranes olone or with deminer-aiized freeze-dried bone or autoge-nous grafts: A study in dogs, int JOrai Maxiiiofac impiants 1995;10:143-154,
22, Langer B, Sullivan DV. Osseointe-grqtion: its impqct on the interrela-tionship of periodontics and restor-ative dentistry Rort I. Int J PeriodontRest Dent 1989:9:85-105.
23, Adeli R, Lekholm U, Bränemark P-l,Surgicai procedures. In. BränemarkP-l, Zarb GA, Albrektsson T (eds).Tissue-Integrated Prostheses, Chi-cago: Quintessence, 1985:211-232,
Volume 17, Number 2,1997





























