Embed Size (px)
Citation preview

The Interaction of HIV, Nutrition, and Poverty: Living with the Consequences
Moving from Research to Policy and Practice
Trinity College Dublin, 3rd November 2016

Please note that these are that these presentations contain preliminary findings from
the NOURISH Project - analysis of the data is ongoing
Contact NOURISH Project Manager Sarah Glavey [email protected] for
further information

Welcome and Overview
Time Session
9.30-9.45am “Welcome and Overview of NOURISH” Martina Hennessy, NOURISH Principal Investigator, Associate Dean of Research, TCD
Sarah Glavey, NOURISH Project Manager/Research Fellow
9.45-10.15am
“Information delivery and entrepreneurial skills sharing: evidence from two randomized field experiments on women living with HIV in Uganda”
Gaia Narciso, Professor of Economics, TCD
10.15-10.45am
“Investigating the connections between environment, agriculture and food and nutrition security in Karamoja”
Solomon Olum, NOURISH Researcher, Gulu University
10.45-11.15am
“Supplementary Feeding in Adults and Children living with HIV in and around Kampala”
Martina Hennessy, NOURISH P.I., Professor of Medical Education, TCD Derek Doherty, Professor of Immunology, TCD
11.15-11.30am
Coffee Break
11.30 – 12.45pm
“From Research to Policy and Practice” Elaine Collins, Finance Manager, Valid Nutrition
Breda Gahan, Global HIV and AIDS Programme Advisor, Concern Worldwide Edward Lahiff, Lecturer, Dept. Food Business and Development, University College Cork
Vincent Maher, HIV Policy Lead, Irish Aid, Department of Foreign Affairs and Trade Eoin Wrenn, Head of Region, Horn and East Africa, Trócaire
Chair: Connell Foley, Director of Strategy, Advocacy and Learning, Concern Worldwide
12.45- 1.00pm
“Next Steps for Research, Policy and Practice” Martina Hennessy, Principal Investigator
1.00pm Close and light lunch

4
“No one will be left behind”

Tackling Societal Challenges through Research

Irish Aid Research Strategy 2015-18: One World- One Future
2. FRAGILE STATES AND SITUATIONS
1
GLOBAL
HUNGER
3. CLIMATE CHANGE
4. TRADE AND ECONOMIC GROWTH
1. GLOBAL HUNGER
5. ESSENTIAL SERVICES
6. HUMAN RIGHTS AND ACCOUNTABILITY
7. HUMANITARIAN ASSISTANCE
Research Strategy Objectives •To build evidence, new and existing, on Irish Aid priorities for
poverty reduction.
•To strengthen communication and policy uptake of the findings
of Irish Aid funded and other research.
•To improve capacity to plan for, conduct and apply development
research within Irish Aid partner countries.
4. TRADE AND ECONOMIC GROWTH

The Role of the University
“No moral questions are ever abstract questions” Edmund Burke, 1839, TCD graduate
“If we still believe universities can actually change the world, then we must move beyond the conventional approach as our only way of finding answers to the most important issues of our time... Putting Global Research Questions on the agenda needs our explicit support if the questions are to become the focus of teams of academic researchers working smoothly across many disciplines… a new kind of global interdisciplinary collaboration needs to be promoted” Prendergast & Hennessy, 2015
How can a university respond?

Uganda and the Context for NOURISH
HIV: Sub-Saharan Africa had 25.8 million people living with HIV in 2014 and accounts for almost 70% of the global total of new HIV infections.
Food Security and Nutrition:
There is a need to understand the lived experience of people with HIV
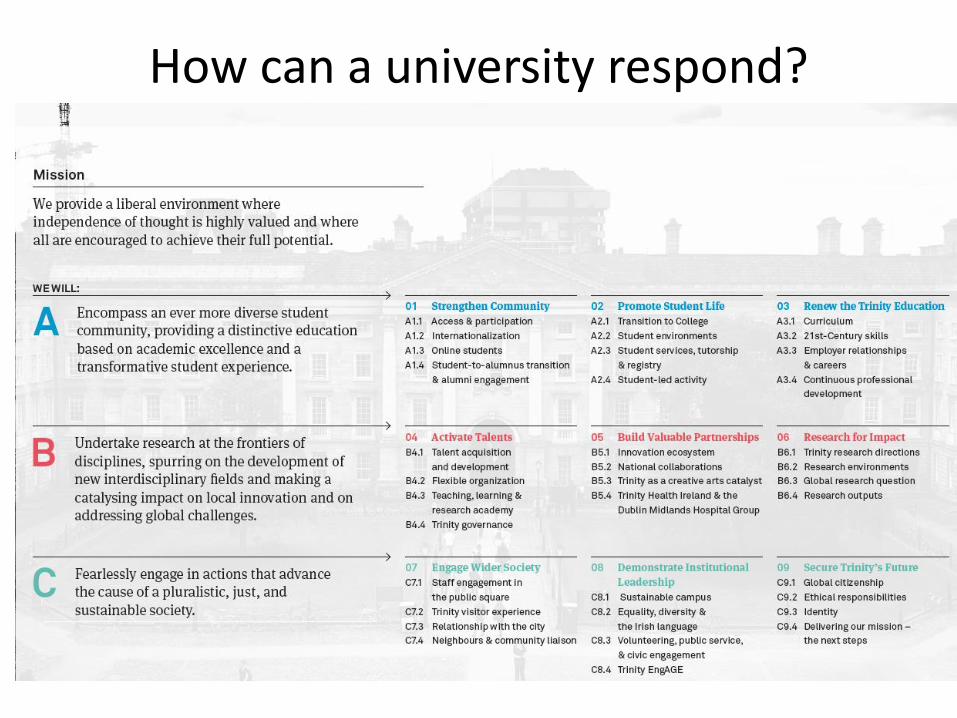
HIV- Malnutrition Interactions
Social and
economic barriers
Impaired Host
response to HIV and treatment
Food Insecurity
Increased Resilience
Increased Responsiveness
Increased Empowerment
for health
Outcomes Work Package Objectives
WP4: Build Capacity Develop frameworks to measure nutritional health in HIV
Create a database for Public health and Policy and to generate new research
Increased risk of HIV Increased morbidity at presentation
Toxicity of ART Risk of relapse Sub-optimal immune response
WP2: Examine effect of Food insecurity on adaptive capacity in Karamoja
WP1.Investigate impact of nutrition on immune and
pharmacological responses in HIV
WP3: Investigate the role of nutrition and role modelling in empowering women with HIV

Work Package 2 Household survey (N=1000) + Focus Groups (N=80) Karamoja
Work Package 1 & 4 Clinical intervention, biomarkers + Public Health platform (N=250) Kampala
Work Package 3 Randomised controlled trial across Uganda (N=4,000)

WP1 Urban
WP2 Isolated
WP3 Rural
WP4 Database
Demographics x x x x
Household survey (income, health etc.)
x x x
Physical Measures: BMI, MUAC, Waist, Wt./ Ht
x x x x
Food Freq. Q’aire or 24hr dietary recall/ diversity
x x x x
Household food insecurity access scale
x
Coping Strategy Index x
Lab data (FBC, glucose, chol), Tanita, Urinary metabolomics
x
Biomarkers; DNA, RNA, PBMCs, PK x
Policy review x x x x
Key Informant Interviews x
Overview of NOURISH Research Methods

International Advisory Group
Prof. Kjetil Bjorvatn, Dr Alex Bambona, Dr Elizabeth Kiboneka, Prof. Jakob Svensson, Prof Robert Gilligan, Prof. Fiona Mulcahy
Partners: Dr. Anne Mullen, National Dairy Council
UK Dr. Helen Roche, University College Dublin
WP4 Advisory Group:
Prof. Christopher Orach, MUSPH, Dr. Jesca Nsungwa, MoH, Mr. Alex
Bambona, MAAIF, Dr. Fred Makumbi, MUSPH,
Dr. Simon Kasasa, MUSPH
jj WP4
Prof. Nazarius Tumwesigye, Dr. Pamela
Nasirumbi, Geraldine Agiraembabazi,MU
Prof. Joe Barry, Sarah Glavey, TCD
The NOURISH Consortium
WP1 Dr. Andrew Kambugu, Dr. Mohammed Lamorde, IDI, Prof. Martina Hennessy, Dr. Derek Doherty, Prof. Fiona Lithander, Dr. Paul Spiers, Dr. PJ Collins, TCD Ben Kikaire, Judy Tatwangire, TCD/IDI
WP2 Prof. Pen-Mogi, Prof. Okello-Umo, Dr. Basil Mugonola, Gulu Uni Prof. David Taylor, NUS, Gaston Tumuhimbise, Archileo Kaaya, MU Christopher Muggaga, Solomon Olum, GU
WP3 Prof. Carol Newman, Prof. Gaia Narciso TCD, Prof. Archileo Kaaya, Dr. Gaston Ampe,MU, Dr. Christine Karungi, Dr. Fiona Kalinda, JCRC, Frances Nakakawa, Patrick Lubega, MU

Panel 1: NOURISH Research
• Dr. Gaia Narciso, Assistant Professor of Economics, Trinity College Dublin
• Solomon Olum, NOURISH Researcher, Gulu University
• Dr. Martina Hennessy, Associate Professor of Medical Education
• Chair: Sarah Glavey, NOURISH Project Manger/Research Fellow
Information delivery and entrepreneurial skills sharing: evidence from two randomized field experiments on women living with HIV in Uganda
Patrick Lubegaa, Frances Nakakawaa, Gaia Narcisob and Carol Newmanb
aMakerere University, Uganda bTIME, Trinity College Dublin, Ireland
Trinity College Dublin, The University of Dublin
Information delivery, Nutrition and HIV Treatment: Evidence from a randomized field experiment on women living with HIV in Uganda
Patrick Lubegaa, Frances Nakakawaa, Gaia Narcisob and Carol Newmanb
aMakerere University, Uganda bTIME, Trinity College Dublin, Ireland

Background
• Little is known about how to trigger behavioral change in relation to nutrition, particularly among vulnerable groups
• In this paper, we test the effectiveness of a nutritional information campaign on improving the health and welfare outcomes of women living with HIV in Uganda using a large-scale RCT
• We explore whether the means of communication matters and uncover some of the underlying mechanisms at work

Motivation • In many settings, people are not well informed about the benefits
associated with certain types of behavior
• The use of mass information campaigns to improve the delivery of services has recently been advocated as an important mechanism for solving information failures (Mansuri and Rao, 2013)
• However, the extent to which such information reaches the most excluded groups has been questioned (Mansuri and Rao, 2013)
• Very little research has explored how information delivered through mass campaigns matters for outcomes

What we do…
• We examine alternative means of providing nutritional information to HIV positive women
• We design and test the impact of a nutrition information campaign and explore two different means of information delivery:
1) a standard nutritional information campaign involving the distribution of posters and flyers;
2) interactive and entertaining cookery demonstrations on how to produce a locally sourced home-made nutritious food.

Experimental design We randomly selected 4 sub-regions of Uganda;
We randomly selected 24 clinics, 6 in each of the four sub-regions;
At baseline each clinic was visited for two days during the HIV clinic to recruit participants;
On average 135 women recruited in each clinic (over 3,000 respondents at baseline);
Baseline survey instrument gathers information on: Personal characteristics of woman Personal characteristics of family members Food frequency questionnaire Income Agricultural production Enterprise activity Employment Housing Access to credit and savings behavior
Experimental Design
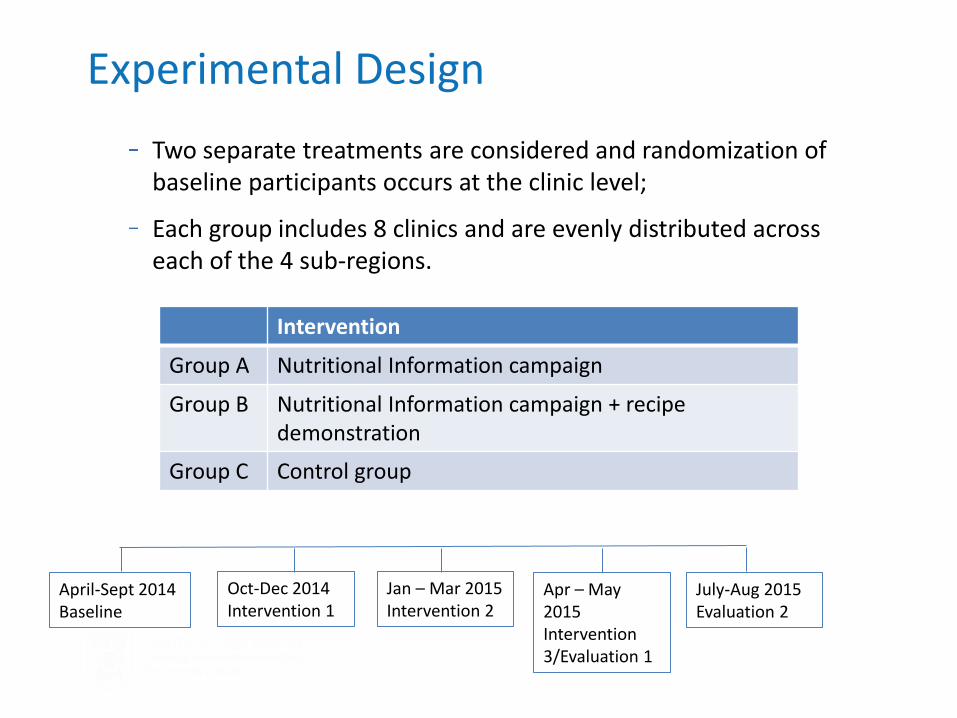
Two separate treatments are considered and randomization of baseline participants occurs at the clinic level;
Each group includes 8 clinics and are evenly distributed across each of the 4 sub-regions.
Intervention
Group A Nutritional Information campaign
Group B Nutritional Information campaign + recipe demonstration
Group C Control group
Oct-Dec 2014 Intervention 1
Jan – Mar 2015 Intervention 2
Apr – May 2015 Intervention 3/Evaluation 1
July-Aug 2015 Evaluation 2
April-Sept 2014 Baseline

Details on Interventions
Nutritional Information Campaign
Delivered by clinic staff at each visit
Content of campaign:
» Information leaflets and posters
» Hands off approach
» Allow clinics to do as they please in attempt to mimic typical campaigns by Ministry of Health

Treatment 1: Nutritional Information Campaign

Treatment 2: Recipe Demonstration
Locally sourced Home-made Nutritious Foods
Nutritionists working in each region to establish locally sourced ingredients that can be used to prepare a Home-Made Nutritious Food.
Products tested at Makerere University for nutrient content, taste and aesthetic appeal – similar to bringing product to market
Intervention takes the form of cookery demonstrations

Trinity College Dublin, The University of Dublin
Treatment 2: Recipe Demonstration

Did the campaign lead to a behavioural change in relation to nutrition?
Obs: 6,200
Information campaign
Recipe demonstration
Access to information
+ +
Meals +
Snacks
Litres of Water
Treated Water

Did the campaign lead to improved health and education outcomes?
Information campaign
Recipe demonstration
Sick -
% Child sick -
% Child absent school
- Midline
Child absent - School fees
-
Child absent - Sick

Did the campaign impact on income and livelihoods?
Obs: 6,200
Information campaign
Recipe demonstration
Personal income +
Other household income
Wage income
Crop income
Livestock income
Enterprise income +
Operates an enterprise
+

Income and livelihoods
Question: What is different about the cookery clinics?
There are two possibilities:
i. Women in cookery clinics become better nourished because they are eating the recipes. In the information only clinics they are just following the guidelines on the brochure so they are not getting the full effect.
ii. There is something about the way the information is delivered that empowers women to work harder.

Anthropometrics and Nutritional intake
Information campaign
Recipe demonstration
Anthropometrics
BMI -
Upper Arm Circumference
Waist circumference -
Nutritional intake (end-line data)
Calories +
Protein +
Fat +
Carbs
Fibre
Minerals +
Vitamins +

Empowerment
Control over.. Information campaign
Recipe demonstration
Personal income - alone
+
Personal income – husband
Personal income – joint
-
Household income - alone
Household income - husband
Household income - joint

Conclusion
• The provision of basic information changes the nutritional intake of women and their health but has limited impact on other welfare outcomes
• In contrast, participation in the cookery campaigns has significant effects on incomes and female empowerment, with knock on effects for children’s school attendance
• Our results suggest that standard information campaign have limited impact on objectively measured outcomes. The participatory cookery demonstrations, on the other hand, have further-reaching effects.
• Positive impact on personal income and the decision to start an enterprise
• Payment of school fees and reduces the proportion of days that children are absent from school
• More empowered, exercising greater control over their own personal incomes
Conclusion
Cookery demonstrations could impact differently in two ways:
1) Demonstration of the recipe is more effective than a passive information campaign
…. both campaigns increased the nutritional content of women’s diets; some evidence that the cookery campaign impacted positively on the mineral and vitamin intake of women
2) the actual activity of bringing women together creates social ties that both empowers and enables the women to engage in more economic activity.
….no evidence that the cookery campaign impacted on the formation of social ties, but positive effects on empowerment
Overall, our results suggests that the medium through which information is delivered can be an empowering tool in itself to improve well-being for vulnerable populations.

Inspiring women: Experimental evidence on sharing entrepreneurial skills in rural Uganda
Patrick Lubegaa, Frances Nakakawaa, Gaia Narcisob and Carol Newmanb
aMakerere University, Uganda bTIME, Trinity College Dublin, Ireland

Trinity College Dublin, The University of Dublin
Motivation
– Role models and bottom-up knowledge sharing;
– Do role models and bottom-up knowledge sharing have an impact in the way in which discriminated individuals think and behave?
– Is this impact permanent or does it fade away over time?

Trinity College Dublin, The University of Dublin
Literature review
– Guyon and Huillery (2014): disadvantaged individuals perform worse when they are reminded of their group;
– Hoff and Pandey (2006, 2014): making identity salient can negatively affect performance of low-caste boys;
– Bernard et al. (2014): impact of screening documentaries about people who had succeeded in agriculture or small business in Ethiopia.
This project
• focuses on a specific group of individuals, who are discriminated and carry a substantial social stigma.
• spans over a longer time horizon

Experimental design We randomly selected 4 sub-regions of Uganda;
We randomly selected 16 clinics, 4 in each of the four sub-regions;
At baseline each clinic was visited for two days during the HIV clinic to recruit participants;
On average 135 women recruited in each clinic;
Baseline survey instrument gathers information on: Personal characteristics of woman Personal characteristics of family members Food frequency questionnaire Income Agricultural production Enterprise activity Employment Housing Access to credit and savings behavior

Experimental Design
One treatment is considered and randomization of baseline participants occurs at the clinic level
Each control and treatment group includes 8 clinics and is evenly distributed across each of the 4 sub-regions
Intervention
Group T Inspiring women videos
Group C Control group
April-Sept 2014 Baseline
Oct-Dec 2014 Intervention 1
Jan – Mar 2015 Intervention 2
Apr – May 2015 Intervention 3/Mid-evaluation
July-Aug 2015 Intervention 4
Sept-Dec 2015 Endline evaluation

Trinity College Dublin, The University of Dublin
Intervention
Video screening at HIV clinics;
One video for each round of intervention;
Four 3-minutes videos;
Group discussion during and after video screening;
Posters;
Casting: 4 inspiring women with business activities;
Video structure:
Background information
How they started their businesses
Challenges
Targets for the future
“I run my own businesses. I have done this and you too can do it”

Trinity College Dublin, The University of Dublin
Inspiring women
Sarah
Alice
Jovia
Mugenyi

Outcomes
• Income and livelihoods
• Empowerment
• Health and education
• Savings and credit

Income and livelihoods
Obs: 3,600
Videos
Operates an enterprise +
Works for a wage
Personal income +
Household income
Wage income
Crop income
Livestock income +
Enterprise income +
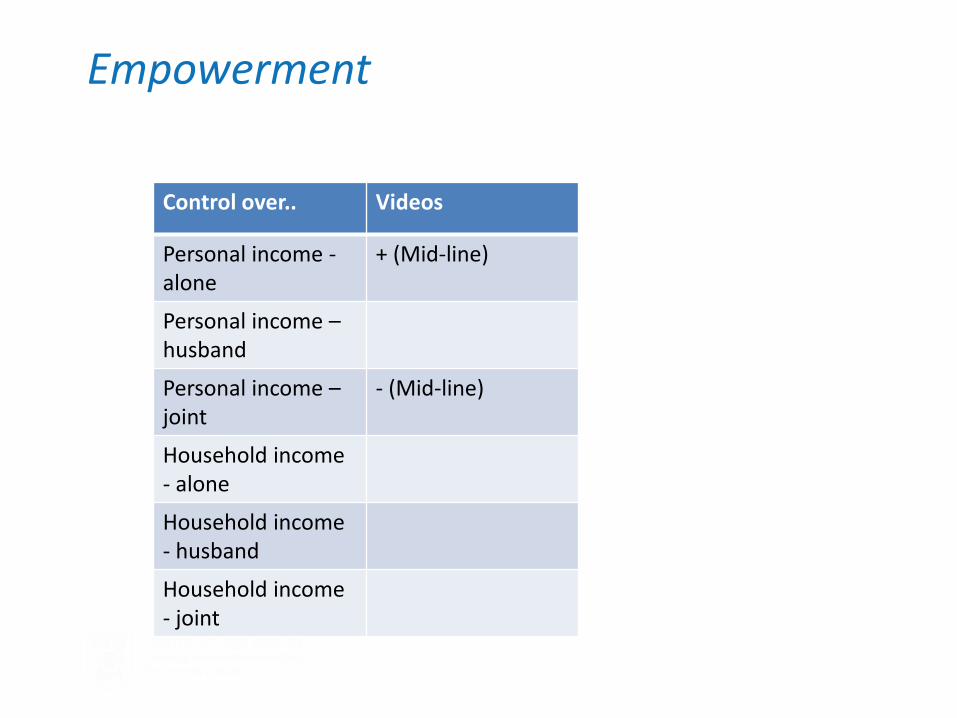
Empowerment
Control over.. Videos
Personal income - alone
+ (Mid-line)
Personal income – husband
Personal income – joint
- (Mid-line)
Household income - alone
Household income - husband
Household income - joint
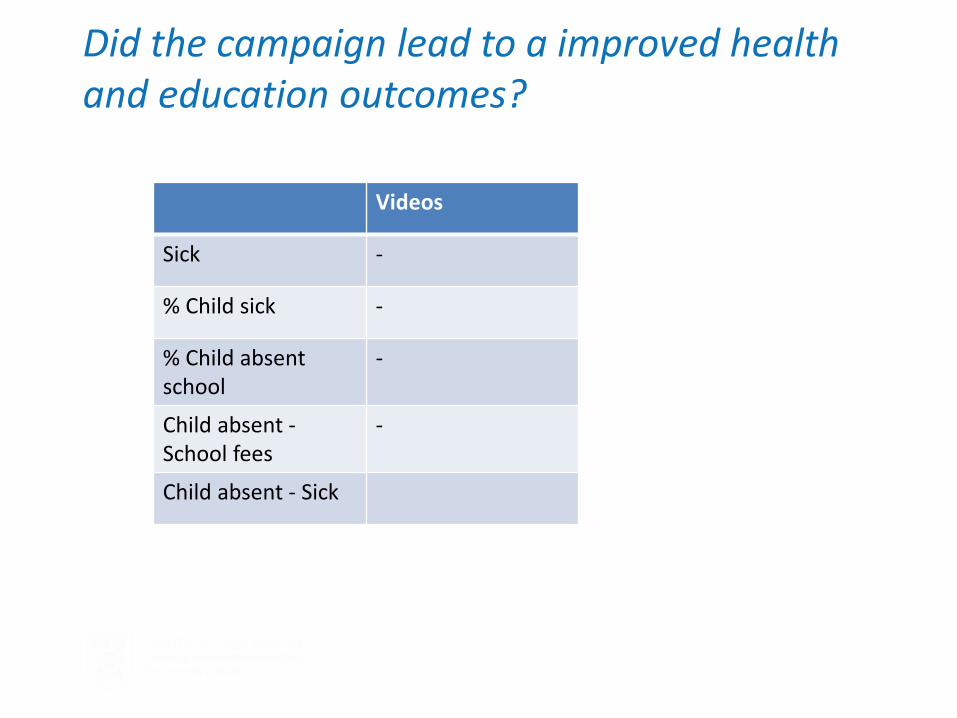
Did the campaign lead to a improved health and education outcomes?
Videos
Sick -
% Child sick -
% Child absent school
-
Child absent - School fees
-
Child absent - Sick

Other outcomes
Videos lead to more informal savings
There may be much longer term effects associated with the video intervention

Conclusions
Roles models have a positive effect on probability of starting a business, personal income and income from enterprises and livestock.
The fact that other household income and income from other activities is not affected suggests that this is due to the message contained in the videos.

Conclusions
Some evidence of increase in control over personal resources in video clinics.
Decline in joint control of personal finances;
Videos lead to
» better health among women and their children
» lower proportion of children absent from school
» In particular they reduce the probability that children are absent from school because of school fees.
Videos lead to more informal savings
There may be much longer term effects associated with the video intervention

Thank You!

Acknowledgements • Collaborating partners:
• Joint Clinical Research Centre (JCRC) • Makerere University • Trinity College Dublin
• We are grateful to a number of people for their valuable comments and insights. These include:
• We are also grateful to the large team of research assistants who took part in the fieldwork component of this project for their dedication and commitment
• We also thank our scientific advisory team for their input and advice
• Prof Martina Hennessy, TCD
• Prof Nazarius Mbona, Makerere
• Dr Cissy Kityo, JCRC
• Prof Archileo Kaaya, , Makerere
• Dr Gaston Ampe, Makerere
• Ms Max Walusimbi, Makerere
• Dr Fiona Kalinda, JCRC
• Ms Christine Karungi, JCRC
• Prof Fiona Lithander, Bristol
• Prof Joe Barry, TCD
• Prof Ceppi Merry, TCD
• Sarah Glavey and Sarah O’Reilly, TCD
Investigating the connections between environment, agriculture and food and nutrition
security in Karamoja, Uganda
Solomon Olum, MSc, NOURISH Researcher, Gulu
University

NOURISH Project: Work Package 2 • Host partner: Gulu University, Uganda • Supervisors and project team
Prof. Taylor David (National University of Singapore, formerly TCD)
Prof. Duncan Ongeng (Gulu University) Prof. Okello-Uma (Gulu University) Dr. Basil Mugnola (Gulu University) Prof. Kaaya Anchileo, (Makerere University) Dr. Gaston A. Tumuhimbise, (Makerere University) Prof. J.H. Nyeko Pen-Mogi-PI, (Gulu University)
• 2 students
PhD: Christopher Mugagga MSc: Solomon Olum *Absorbed by Gulu University as lecturers *Gulu University is a community-oriented institution, with moto “for community transformation”

Background • Karamoja with highest food and nutrition insecurity
(UDHS, 2011)
• Lowest human development indicators
20% of the households food insecure and a further 38%
moderately food insecure (Gerlad & Jing, 2012).
45% U5 are stunted ; 70% U5 and 43% of WCBA are anemic (UBOS/IFC, 2012).
High childhood disease prevalence; Malaria (43.3%) (UNICEF/ACF, 2009), fever (40.9%) and diarrhea (20.3%) (UBOS/IFC,
2012).
• Ecologically; one planting season, highly sporadic rains
• Pastoral lifestyle
• Ethnically diverse with unique cultural features

Map of Karamoja: (5/7 districts studied)

Objectives of Work Package 2
Investigate:
The principal causes of nutritional stress and poor
health
Forms of food production and livelihoods that are
most vulnerable to chronic and transitory external
pressures.
Factors (including cultural determinants)
contributing to food and nutrition insecurity

Methodology • Households surveys
Food security—HFIAS
Dietary survey; FFQ, HDDS, 24-recall

Methodology • Focus groups
• Key Informants interview

Methodology
• Anthropometry
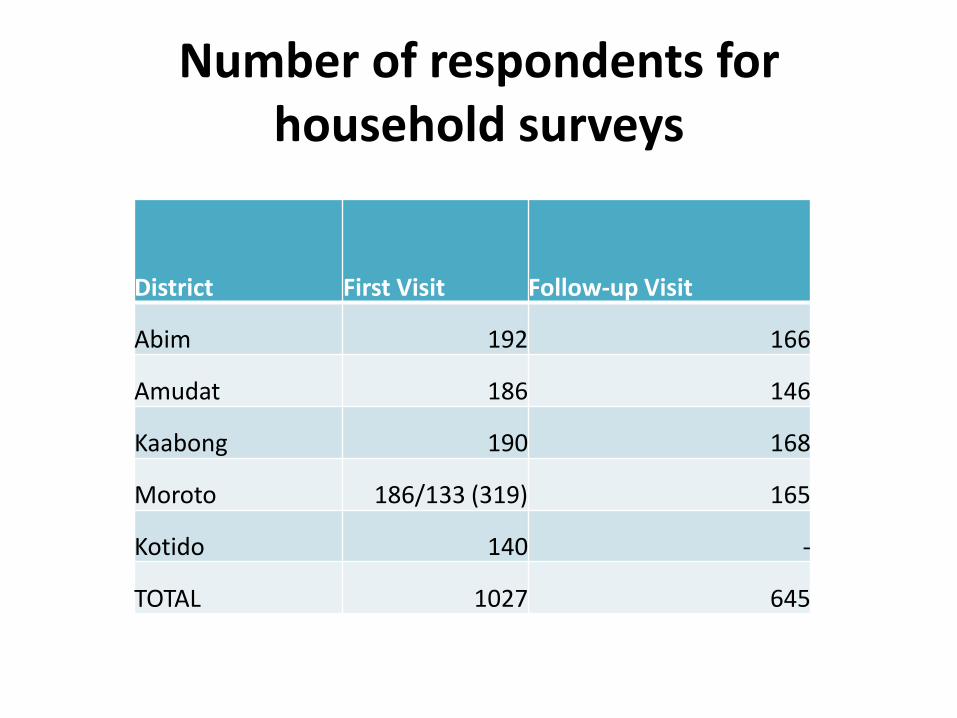
Number of respondents for household surveys
District First Visit Follow-up Visit
Abim 192 166
Amudat 186 146
Kaabong 190 168
Moroto 186/133 (319) 165
Kotido 140 -
TOTAL 1027 645

Key findings
• High household food insecurity
Household food insecurity score and coping strategy index
Sub-county
Mean±SD of food
insecurity score P value
Mean±SD of Coping
strategy index (CSI) P value
Nadunget 15.65±5.21 0.271 119.286±47.40a < 0.00
Tapac 15.11±3.07 122.264±30.94a
Nakapelimor
u 14.24±4.56 94.057±46.06b
Kacher 14.79±3.80 98.100±42.36b
Total 14.94±4.21 108.148±43.65

Key findings • Poor dietary practices Low number of meals
Low and infrequent consumption of animal foods
Low dietary diversity
Number of meals taken by households
Percent of households that took different
number of meals in 24 hours
Ethnic group No meal at all 1-2 meals
3 or more
meals
Jie 1.6 74.8 23.6
Labwor 0 50.0 50.0
Matheniko 0 93.9 6.1
Tepeth 3.0 68.2 28.8
Others (Acholi, Turkana) 0 62.5 37.5
Total 1.5% 77.3% 21.2%

Poor nutritional indices (WAZ,HAZ,WHZ)
Weight for Height-Kaabong

Causes of food and nutrition insecurity and poor health
• Low calorie and nutrient intake
• Cultural aversion to nutritious foods (e.g. ASFs)
• Poor food insecurity coping strategies
• Poor housing predisposes to poor health
• Big family sizes (majority >10 members)
• Low educational attainment

Proportion of households with adequate intake of calorie and nutrients
Percentage of households that took at least the minimum RDA
Age
group
19-30 years 31-50 years 51-70 Years Above 70 years
District Kotido Moroto Kotido Moroto Kotido Moroto Kotido Moroto RDA
Calorie 20.8 7.1 25.9 3.9 12.5 0 0 0 2000-
2200Kcal
Water 27.1 21.4 10.3 39.2 9.4 32.6 N/A 38.5 2.7 litre
Proteins 58.3 14.3 63.8 21.6 53.1 14 N/A 23.1 46g
Carbohyd 81.2 64.3 75.9 60.8 75.0 41.9 N/A 46.2 130g
Fiber 45.8 39.3 46.6 35.3 62.5 37.2 N/A 38.5 21-25g
Calcium 12.5 0 8.6 0 0 2.3 0 0 1000mg
Iron 41.7 10.7 43.1 13.7 84.4 51.2 N/A 46.2 8-18g
Zinc 43.8 10.7 43.1 5.9 40.6 7.0 0 0 8g
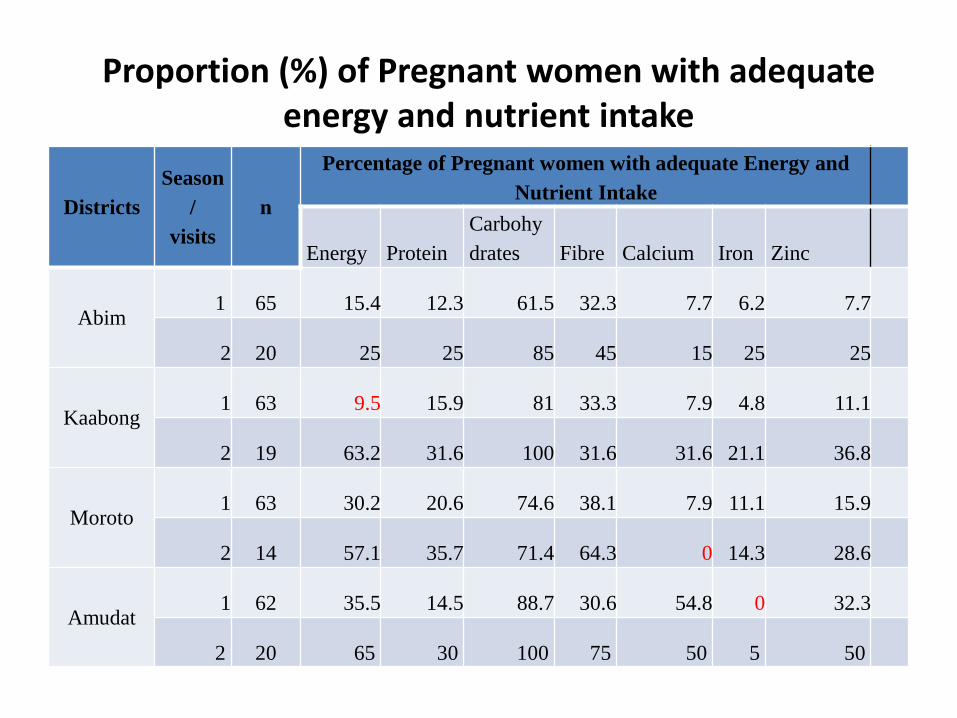
Proportion (%) of Pregnant women with adequate energy and nutrient intake
Districts
Season
/
visits
n
Percentage of Pregnant women with adequate Energy and
Nutrient Intake
Energy Protein
Carbohy
drates Fibre Calcium Iron Zinc
Abim 1 65 15.4 12.3 61.5 32.3 7.7 6.2 7.7
2 20 25 25 85 45 15 25 25
Kaabong 1 63 9.5 15.9 81 33.3 7.9 4.8 11.1
2 19 63.2 31.6 100 31.6 31.6 21.1 36.8
Moroto 1 63 30.2 20.6 74.6 38.1 7.9 11.1 15.9
2 14 57.1 35.7 71.4 64.3 0 14.3 28.6
Amudat 1 62 35.5 14.5 88.7 30.6 54.8 0 32.3
2 20 65 30 100 75 50 5 50

Foods prohibited by culture to be eaten by women and children
Name of the food item (local name) Reason (s) for prohibiting
Offals/animal intestine (Ngamolteng) - First women who ate spoilt it.
- Pregnant women will get miscarriage
Liver (Emany) - Expecting woman will fail to deliver or her baby
dies
Pancreas (Ecid) - Woman continues bleeding/over bleed after
delivery
Animal ribs (Ngamarang) - When a woman delivers, the placenta will fail to
come out
Testis of animal (Nyito) - Young women will not produce if they eat
Spinal cord/Vertebrae bone - If a child eats, his/her uncle will die
Chicken which lack feather on the
neck (Congolese chicken): Lokulas
- The child will not have good luck in most things
Sharing water from same source - Girls of the same family who are married in one
area do not share water from the same source
unless a ritual is performed or they die

Food insecurity coping strategies for Karamoja
Coping strategy Weight assigned
Rely on less preferred and less expensive foods 3
Borrow food or money to buy food 3
Rely on help from friends/relatives 2
Limit portions at meal time 3
Limit intake to ensure children get enough 3
Reduce number of meals eaten in a day 4
Skip whole days without eating 3
Gather unusual amounts of wild foods 4
Harvest immature crops 2
Rely on casual labour for food 4
Send household members to eat elsewhere 2
Sell assest e.g. animals 2
Eat unconventional foods e.g. local brew residue,
wild foods 4

Poor housing predisposes to poor health

Educational attainment of household caregivers
District No formal education
Primary level Secondary level
Tertiary
Abim 26 56 18 1
Kaabong 63 37 1 0
Moroto 92 8 0 0
Amudat 95 4 0 0
Kotido 92.9 5.7 1.4 0

Forms of food production and livelihoods that make occupants vulnerable
• Food production generally low to support food and nutrition security
• Pastoral life style*
• Charcoal burning and cutting down trees for fuel wood
• Poor occupation (casual laboring and gardening)
• Brewing of cereals for alcohol

Household 12 month crop production value (in US dollars) segregated by sub-county (mean)

Key Recommendations
• Nutrition education to: Demystify cultural aversion to nutritious foods Raise knowledge and awareness of nutritious foods Increase calorie and nutrient intake (link food intake and
levels of activity) Minimize nutrient loss during food preparation Behaviour change communication to address cultural
food restriction and high alcohol consumption
• Natural resource management
Emphasis on conservation of wild plants to sustainably reap benefits (Vegetable, fruits, roots, medicine, fuel wood).
Increase access of local people to areas with wild plants

Key recommendations • Improvement on agricultural production
Diversification of production for both crops and animals Provision of early maturing and drought resistant varieties Encourage small animal (goats and poultry) production to cushion
against transitory food insecurity
• Improvement on WASH Increase on latrine coverage and lower open defecation Increase coverage of safe water sources
• Empowerment of households Economic empowering (IGAs) of households to cushion in hunger
periods Combat high illiteracy levels—government & development agencies Health education on family planning and benefits of small size
households

Acknowledgements
• Irish Aid/HEA-for funding the research • TCD Team- overall coordination • Makerere University- supervision, MSc study, country
coordination • Gulu University – PhD study, supervision, coordination • Professor David Taylor (NUS)- WP2 Supervision and
Sponsorship of visit to NUS (PhD and MSc Students) • All the collaborators in NOURISH project • Karamoja district local government (RDCs, CAOs, sub-
county officials, LCs) • Locally sourced RAs

Thank you for listening
Solomon Olum, MSc, NOURISH Researcher, Gulu
University

Supplementary Feeding in Adults and Children in and around Kampala
Dr. Martina Hennessy, TCD

Aims
• To investigate the role of nutrition as a determinant of treatment outcome for HIV infected adults and children in Uganda, by examining clinical, pharmacological and immunological responses to food supplementation in patients with and without malnutrition
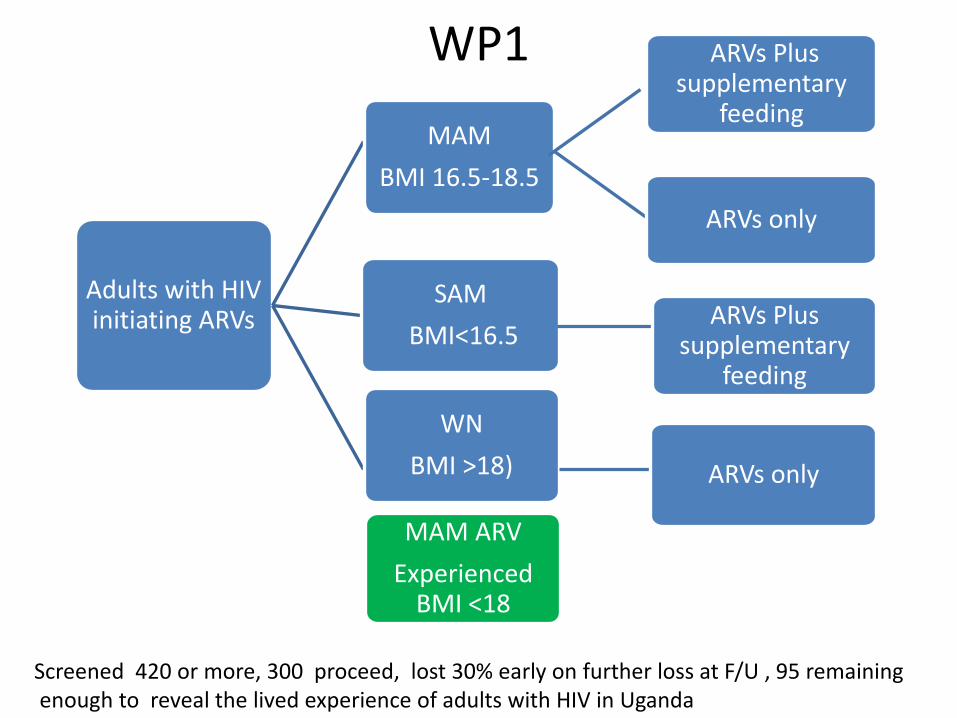
WP1
Screened 420 or more, 300 proceed, lost 30% early on further loss at F/U , 95 remaining enough to reveal the lived experience of adults with HIV in Uganda
Adults with HIV initiating ARVs
MAM
BMI 16.5-18.5
ARVs Plus supplementary
feeding
ARVs only
SAM
BMI<16.5 ARVs Plus
supplementary feeding
WN
BMI >18) ARVs only
MAM ARV
Experienced BMI <18

Nourish participants underwent a comprehensive nutrition assessment
• Food and Nutrition Related History
• Anthropometry
• Biochemical Data and Medical tests
• Nutrition Focused Physical Findings
• Client History
78

Adult Baseline Characteristics
CHARACTERISTIC
GROUP
Well nourished
N=23
Severely
Malnourished
N=17
Moderately
Malnourished
N=32
Malnourished
On ART
N=26
Mean Age in years (sd) 32.42 (8.39) 32.36 (6.53) 34.69 (11.77) 46.00 (8.31)
WHO STAGE at
ART initiation
I 4 0 1 0
II 15 1 6 3
III 3 2 15 18
IV 1 14 10 5
Mean Weight in Kg (Sd)
Time to ARV (mths)
58.4 (8.6)
2
44.2 (5.1)
13.8
49.5 (4.7)
8.7
45.1 (3.5)
3yrs on ARVs
Mean BMI (sd) 22.3 (1.8) 15.88 (0.7) 17.86 (0.5) 17.3 (1.1)
Mean CD4 cells/ul (sd) 299.61
(183.64)
125.8
(161.08)
205.65
(135.78)
492.69
(247.1)
Median Viral Load
(Copies/ml), (range)
0.6^105
(489- 28.5^105)
1.3^105
(1250-12.4^105)
1.8^105
(0-86^105 )
0
(0-35.6^105)

Baseline Daily Work activities lost through
illness all groups
*

Understanding The Adult Diet

HIV Positive, Moderately Acutely Malnourished (MAM) Naïve Patients. Randomised to Plumpy Nut or not x12 weeks
Group A Treated vs Untreated patients (PN) showed a significant increase in 3month BMI compared with patients own baseline BMI, but no difference between groups
Gain of approx. 5kg weight and +1 unit of BMI

Weight Change (Kg) and BMI change (Kg/M2 ) in Adult ARV experienced HIV malnourished Patients
Patients with BMI < 18.5Kg/ M2 were randomised to receive Plumpy Nut ( 2 sachets/ day) or not for 12 weeks

The effect of PN on ARV drug levels

Body Composition Analysis Moderately malnourished Severely
malnourished Well nourished
Baseline combined
Follow up with
Plumpy nut
Follow up No
Plumpynut
Baseline Follow up with
Plumpy nut
Baseline Follow up no Plumpy
nut
Age, y 35 33 38 33 33 33 33
Weight, kg
49.5
54 55 44 49 57 59
Height, cm 166
166 167 166 166 161 161
BMI, kg/m2
17.9
19 19 16 18 22 23
% fat 9.7 15.79 12 7 12 21 21
Fat mass, kg
5.9
8.9 6.3 3.1 6 11 12.6
TBW, kg 33 33.5 34.9 30 31 33 34
How do we usefully measure total body protein ?

Only 2% fall in Cholesterol
(meta-analysis of community studies (Ramsay. BMJ;1991:303:953)
Dietician = Leaflet = GP advice
(BMJ:1995:310:569)
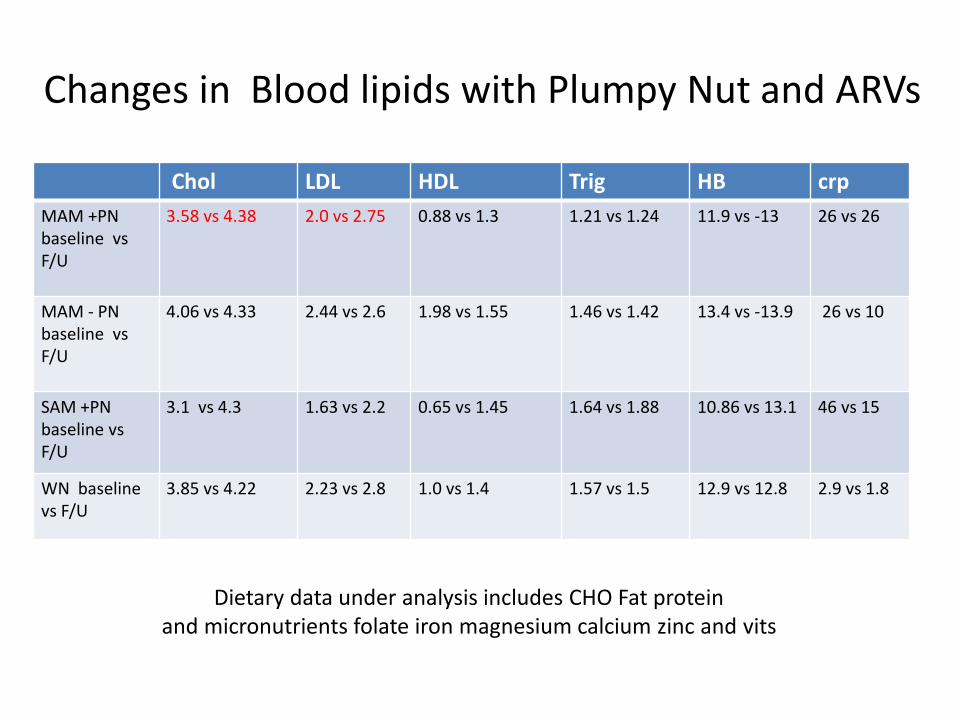
Changes in Blood lipids with Plumpy Nut and ARVs
Chol LDL HDL Trig HB crp
MAM +PN baseline vs F/U
3.58 vs 4.38 2.0 vs 2.75 0.88 vs 1.3 1.21 vs 1.24 11.9 vs -13 26 vs 26
MAM - PN baseline vs F/U
4.06 vs 4.33 2.44 vs 2.6 1.98 vs 1.55 1.46 vs 1.42 13.4 vs -13.9 26 vs 10
SAM +PN baseline vs F/U
3.1 vs 4.3 1.63 vs 2.2
0.65 vs 1.45 1.64 vs 1.88 10.86 vs 13.1 46 vs 15
WN baseline vs F/U
3.85 vs 4.22 2.23 vs 2.8 1.0 vs 1.4 1.57 vs 1.5 12.9 vs 12.8 2.9 vs 1.8
Dietary data under analysis includes CHO Fat protein and micronutrients folate iron magnesium calcium zinc and vits
Work Package 1- Main findings The presence of MAM or SAM status at initiation of ART is associated with worse presentation, micronutrient deficiency, more days lost due to illness and delay in starting ART. Generally food intake and dietary diversity if poor even when food is plentiful There is a significant cohort of adults ( 25%) and children (44%) already engaged in care that continue to be malnourished despite ART. This group responds well to RUTF For MAM patients starting treatment, there was no difference in change in BMI /weight for those given ART +RUTF compared with ART alone. Perhaps resources best used elsewhere? Preliminary results suggest that innate immune response (gamma delta expansion) to HIV treatment is affected by malnutrition

Additional Findings and Further Analysis
• Patients were compliant with ARV and PN where it was given • Degree of food insecurity and serious lack of dietary diversity ( as in
WP2) • All gained weight and some of that is attributable to the ARV
treatment PN • The effects of PN on BFC were remarkable does it have LT
significance • A sig no of patients on ARV are MN while engaged in care - a
forgotten group what can we learn from this group how should we treat them (? Not with PN)
• What about protein and metabolomics? The 24 hr dietary recall analysis will add information
• How will it affect drug handling

The Children's Study
Transdisciplinary research for global challenges is about making a different future for mankind
because the future will
be different

Naïve children n=66 (%) Exp children n=89 (%)
Male 31(47) 43 (48)
Female 35(53) 46 (52)
Nutrition status
malnourished 41(62) 44(49)
Well nourished 25(38) 45(51)
Next of Kin as mother 48(73) 65(73)
Mother on ART 34(69) 70(93)
Mother alive 53(88) 79(88)
Mother aware of HIV sero-status of father
22 (58) 56(67)
Immunization status 43(73) 74(83)
Socio-demographic characteristics of children
70% of malnourished children were between 5-12yrs, remainder between 1-5yrs, none were infants - “ The forgotten child”

Common reasons for exclusion Reasons for not being recruited Numbers Percentages
1. Suspected or confirmed malignancy 2 1.83
2. Vomiting 5 4.62
3. Congenital disorders 3 2.75
4. Cerebral palsy 2 1.83
5. ART naïve critically ill children 6 5.50
6. Odematous malnutrition 2 1.83
7. Recent RUTF use in the last 3 months 1 0.92
8. Stunted 9 8.26
9. Controversial HIV tests 2 1.83
10. Mild malnutrition 35 32.11
11. Minor with minor 3 2.75
13. HIV exposed 31 28.44
14. Doctor busy 6 5.50
15. Age range 2 1.83
Total 109 100

What are children Eating?

Change in viral load in ARV experienced children after receiving Plumpy nut
MAM SAM
BL 3 Mo BL 3 Mo
<20 22.5 37.9 6.67 18.2
20-1000 30.6 41.4 13.3 27.3
>1000 46.9 20.7 80 54.6

Pharmacology: ART Regimen Profile
Type of ART regimen Percentage
ABC+3TC+EFV
30.77
ABC+3TC+NVP
23.08
ABC +3TC+ AZT
23.08
ABC +3TC+ LPV/r
15.38
AZT +3TC+ NVP 7.69

Nevirapine paired samples from ARV experienced MAM and SAM children at baseline and 3months post PN
NVP levels are high relative to normal values at baseline
But return to normal values with PN

Flow cytometric analysis of circulating lymphocytes
To determine the frequencies of the following cell types in PBMC • CD4+ T cells - depleted in HIV infection • CD8+ T cells • CD4-CD8- T cells • B cells • Natural killer (NK) cells • Natural T (NT) cells • Invariant natural killer T (iNKT) cells • Vδ1+ γδ T cells – expanded in HIV infection • Vδ2+ γδ T cells – depleted in HIV infection • Vδ3+ γδ T cells

Immunophenotype (Vδ3) of HIV infected children categorised by nutritional & ART status

WP1 Team - Acknowledgments Ben Kikaire, Judy OrikiriizaTatwangire, IDI/TCD Andrew Kambugu, Mohammed Lamorde, IDI
Nazarius Tumwesigye, MUSPH Martina Hennessy, Derek Doherty, Fiona Lithander, Paul Spiers, PJ Collins, Ceppie Merry, Fiona Mulcahy, Carol Newman, Gaia Narciso, Sarah Glavey, Joe Barry, TCD
Aifric O’ Sullivan, Helen Roche, UCD Anne Mullen, Kings College London/National Dairy Council UK
Pietro Pala, Jane Achan, Grace Ndeezi, Paula Munderi, MRC
The Interaction of HIV, Nutrition, and Poverty: Living with the Consequences
Moving from Research to Policy and Practice
Trinity College Dublin, 3rd November 2016

Panel Q&A
• Audience Q&A (15 mins)
Summary
• Themes Arising: – Partnership among different development
stakeholders
– Research coherence: challenges and opportunities of doing multi-disciplinary research
– Research Impact
• After the break we will move from researcher to policy and practice, gaining responses and perspectives from our panel of discussants

Panel 2: From Research To Policy and Practice
Time Session
9.30-9.45am “Welcome and Overview of NOURISH” Martina Hennessy, NOURISH Principal Investigator, Associate Dean of Research, TCD
Sarah Glavey, NOURISH Project Manager/Research Fellow
9.45-10.15am
“Information delivery and entrepreneurial skills sharing: evidence from two randomized field experiments on women living with HIV in Uganda”
Gaia Narciso, Professor of Economics, TCD
10.15-10.45am
“Investigating the connections between environment, agriculture and food and nutrition security in Karamoja”
Solomon Olum, NOURISH Researcher, Gulu University
10.45-11.15am
“Supplementary Feeding in Adults and Children living with HIV in and around Kampala”
Martina Hennessy, NOURISH P.I., Professor of Medical Education, TCD Derek Doherty, Professor of Immunology, TCD
11.15-11.30am
Coffee Break
11.30 – 12.45pm
“From Research to Policy and Practice” Elaine Collins, Finance Manager, Valid Nutrition
Breda Gahan, Global HIV and AIDS Programme Advisor, Concern Worldwide Edward Lahiff, Lecturer, Dept. Food Business and Development, University College Cork
Vincent Maher, HIV Policy Lead, Irish Aid, Department of Foreign Affairs and Trade Eoin Wrenn, Head of Region, Horn and East Africa, Trócaire
Chair: Connell Foley, Director of Strategy, Advocacy and Learning, Concern Worldwide
12.45- 1.00pm
“Next Steps for Research, Policy and Practice” Martina Hennessy, Principal Investigator
1.00pm Close and light lunch

Panel 2: From Research to Policy and
Practice • Elaine Collins, Finance Manager, Valid Nutrition
• Breda Gahan, Global HIV and AIDS Programme Advisor, Concern Worldwide
• Edward Lahiff, Lecturer, Dept. Food Business and Development, University College Cork
• Vincent Maher, HIV Policy Lead, Irish Aid, Department of Foreign Affairs and Trade
• Eoin Wrenn, Head of Region, Horn and East Africa, Trócaire
• Chair: Connell Foley, Director of Strategy, Advocacy and Learning
Breda Gahan, Global HIV and AIDS Programme
Advisor, Concern Worldwide
Trinity College Dublin, 3rd November 2016

Burden of HIV in Uganda (2015)

107
Impacts of HIV and AIDS on Food and Nutrition Security
Household member
ill with HIV and AIDS
Healthcare costs
Need for care
Productivity
Household Nutrition
Security
Savings, purchasing power
Partner becomes ill
Child care Hygiene
Food processing/
preparation Food Security
-Availability
Stability
Access to food

HIV and Malnutrition

Ref. In-Country Guidelines
Text
20080200880
2009
*Be Country, Culture, Context conscious in terms of national guidelines & implementation

Panel 2: From Research to Policy and Practice
• Short report to follow

Wrap-Up - What Next?
• Key themes emerging from the discussions today
• Next steps for NOURISH and partnerships – Work package 4 - Policy review and report
– Disseminate research findings as they are developed
– Consult widely to expand partnerships
– Make large dataset accessible
• Updates will be posted to https://www.tcd.ie/tidi/nourish/
• Check out Trinity Development Research Week by TIDI!
https://www.tcd.ie/tidi/news-events/tidi/#drw

112
“No one will be left behind”

Platform
Language Partnership
Defining
Challenge Approach
Outcome
Identification of Scale &
partnership
Research Design and performance
metrics for impact
Implementation
&
Timing
Impact
dissemination
Evidence into use
Transdisciplinary Ecosystem to address Global Challenges
Compromise Collegiality
Consistency Creativity

Academic Social Responsibility

The Interaction of HIV, Nutrition, and Poverty: Living with the Consequences
Moving from Research to Policy and Practice
All feedback and questions welcome to NOURISH Project Manager/Research Fellow, Sarah Glavey [email protected]