Embed Size (px)
Citation preview

The Institute for Attachment The Institute for Attachment and Child Developmentand Child Development
Presented by: Presented by:
Forrest R. Lien, LCSW-DirectorForrest R. Lien, LCSW-DirectorEmail: [email protected]: [email protected]
P.O. Box 730 – Kittredge, CO 80457 (303) 674-1910-phone (303) 670-3983-Fax
www.InstituteForAttachment.org
“Achieving Permanency For Children Diagnosed With Reactive Attachment Disorder”
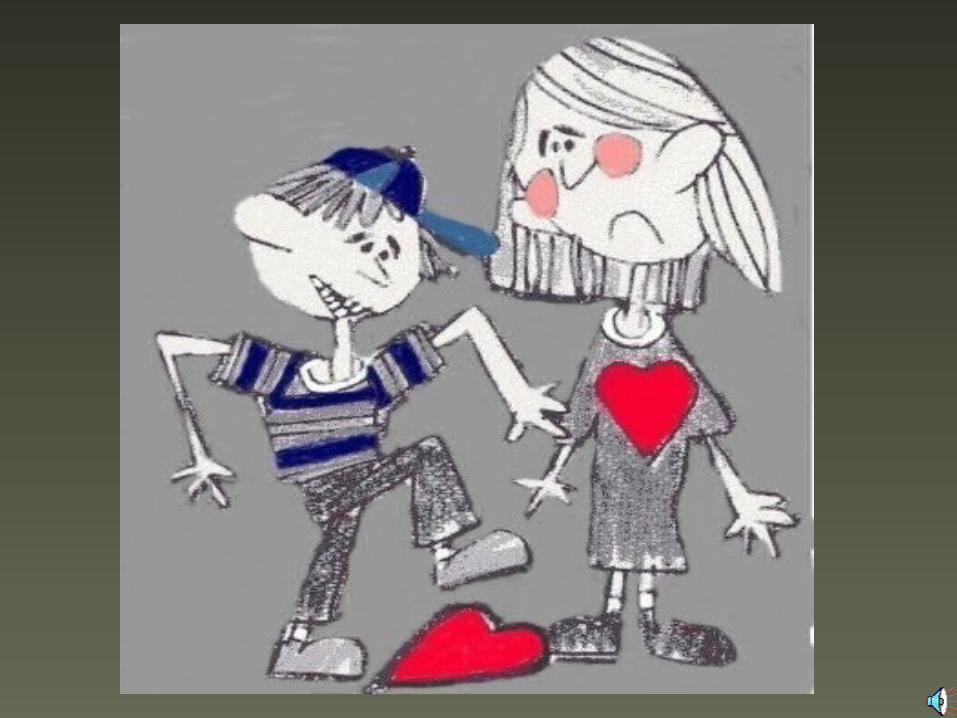
Attachment CyclesAttachment Cycles11stst Year Year
Necessary
ingredients of development of basic trust and attachment:
• Eye Contact• Food• Motion• Touch• Verbal Contact• Emotional Contact• Smiles
State of
High Arousal (rage)
Satisfaction ofNeed
(gratification)
Relaxation of Tension
(trust)
Need
Trust Of
Caretaking
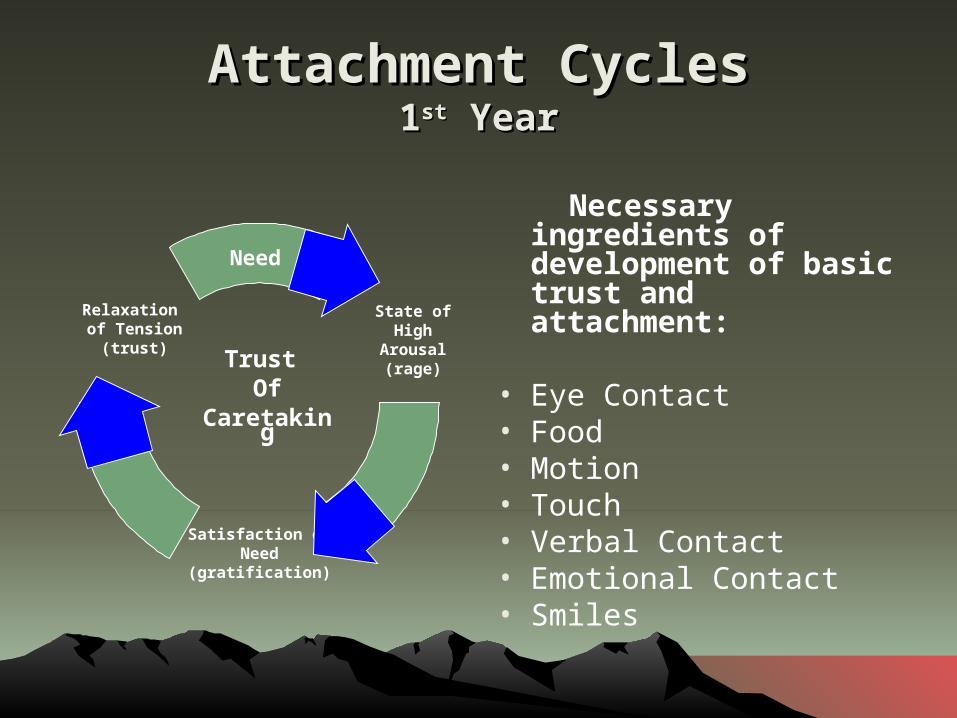
Attachment CyclesAttachment Cycles 2nd Year2nd Year
Necessary ingredients of development of autonomy, good character foundation and conscience.
Maintain parental control while allowing child to explore and begin to make good choices for themselves.
State of
High Arousal (rage)
Acceptance Of
Limits
Mutual goodFeelings
Wants
Trust Of
Control
TRUST ATTACHMENT AUTONOMY

Sub-Types of Attachment Sub-Types of Attachment DisorderDisorder
1. AVOIDANT-isolation, avoid closeness, seldom seek comfort, avoid relationships, passive-aggressive, avoid feelings, intense sadness and loneliness, believe their rejection by birth mom was justified
2. ANXIOUS-crazy liars, fake emotions, emotionally empty, “good actors”, chameleons, often fool therapists that they’re normal and parents aren’t
3. DISORGANIZED-disorganized, odd, and bizarre behaviors. Other psychiatric disorders, unpredictable moods, excessively excitable, frequent sensory or neurological problems, difficult to manage
4. AMBIVALENT-openly angry, defiant, destructive, dangerous, superficially charming, lack of empathy, delinquent acts, most prevalent subtype in mental health systems
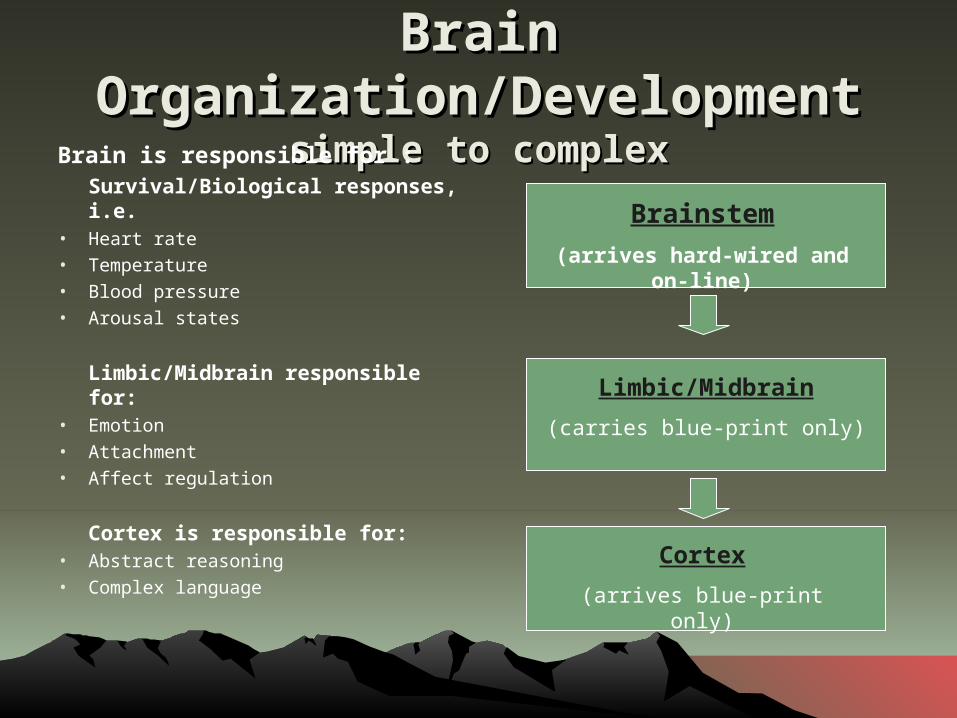
Brain Brain Organization/DevelopmentOrganization/Development
simple to complexsimple to complexBrain is responsible for :Survival/Biological responses, i.e.
• Heart rate• Temperature• Blood pressure• Arousal states
Limbic/Midbrain responsible for:
• Emotion• Attachment• Affect regulation
Cortex is responsible for:• Abstract reasoning• Complex language
Brainstem
(arrives hard-wired and on-line)
Limbic/Midbrain
(carries blue-print only)
Cortex
(arrives blue-print only)
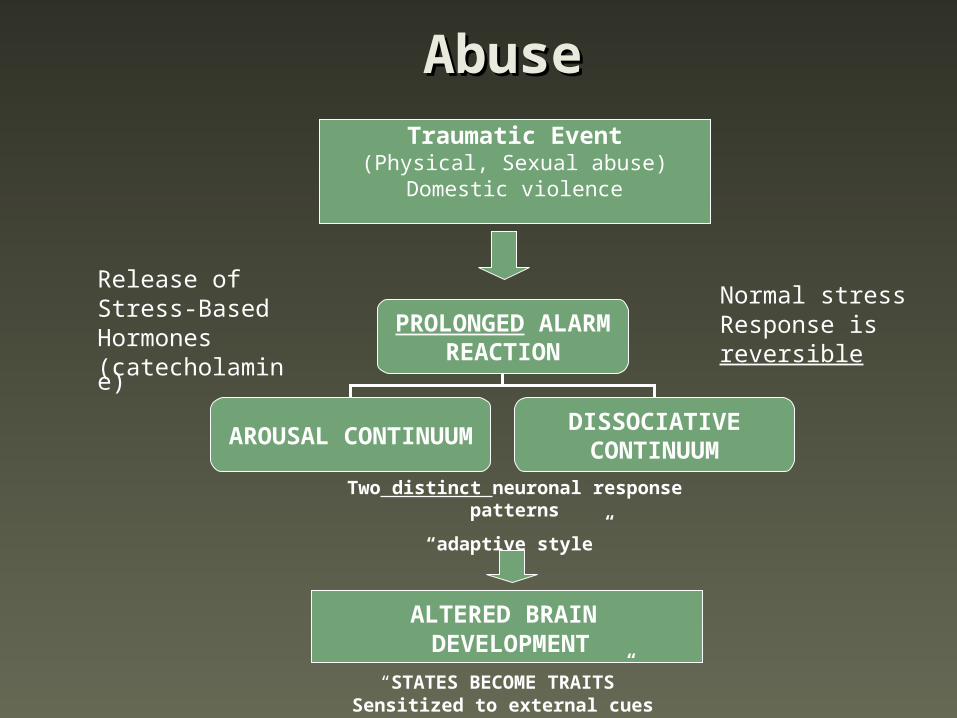
AbuseAbuseTraumatic Event
(Physical, Sexual abuse)Domestic violence
Release ofStress-BasedHormones(catecholamine)
Normal stressResponse is reversible
PROLONGED ALARMREACTION
AROUSAL CONTINUUMDISSOCIATIVECONTINUUM
Two distinct neuronal response patterns
“adaptive style”
ALTERED BRAIN DEVELOPMENT
“STATES BECOME TRAITS”Sensitized to external cues

CausesCausesAny of the following conditions put
a child at high risk of developing an attachment disorder. The
critical period is from conception to about twenty-six months of
age.
• Genetic predisposition• Maternal ambivalence toward pregnancy• Traumatic prenatal experience, in-utero exposure to alcohol/drugs • Birth trauma • Sudden separation from primary caretaker ( i.e. illness or death of mother or
sudden illness or hospitalization of child.)• Undiagnosed and/or painful illness, such as colic or ear infections• Inconsistent or inadequate day care • Unprepared mothers with poor parenting skills• Abuse ( physical, emotional, sexual)• Neglect• Frequent moves and/or placements ( foster care, failed adoptions)
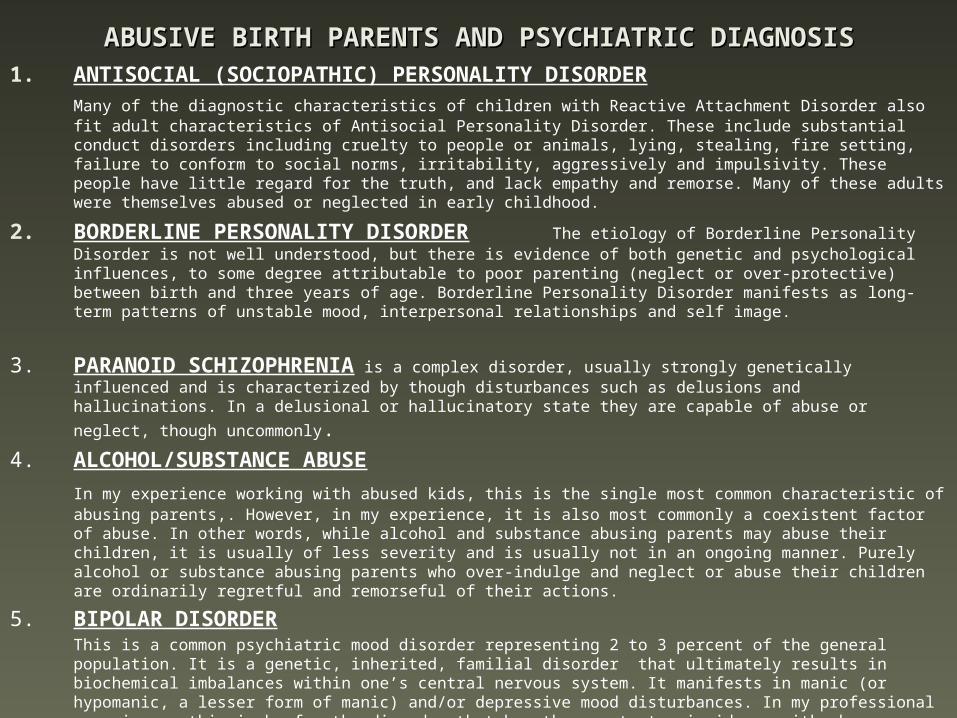
ABUSIVE BIRTH PARENTS AND PSYCHIATRIC DIAGNOSISABUSIVE BIRTH PARENTS AND PSYCHIATRIC DIAGNOSIS1. ANTISOCIAL (SOCIOPATHIC) PERSONALITY DISORDER
Many of the diagnostic characteristics of children with Reactive Attachment Disorder also fit adult characteristics of Antisocial Personality Disorder. These include substantial conduct disorders including cruelty to people or animals, lying, stealing, fire setting, failure to conform to social norms, irritability, aggressively and impulsivity. These people have little regard for the truth, and lack empathy and remorse. Many of these adults were themselves abused or neglected in early childhood.
2. BORDERLINE PERSONALITY DISORDER The etiology of Borderline Personality Disorder is not well understood, but there is evidence of both genetic and psychological influences, to some degree attributable to poor parenting (neglect or over-protective) between birth and three years of age. Borderline Personality Disorder manifests as long-term patterns of unstable mood, interpersonal relationships and self image.
3. PARANOID SCHIZOPHRENIA is a complex disorder, usually strongly genetically influenced and is characterized by though disturbances such as delusions and hallucinations. In a delusional or hallucinatory
state they are capable of abuse or neglect, though uncommonly.4. ALCOHOL/SUBSTANCE ABUSE
In my experience working with abused kids, this is the single most common characteristic of abusing parents,. However, in my experience, it is also most commonly a coexistent factor of abuse. In other words, while alcohol and substance abusing parents may abuse their children, it is usually of less severity and is usually not in an ongoing manner. Purely alcohol or substance abusing parents who over-indulge and neglect or abuse their children are ordinarily regretful and remorseful of their actions.
5. BIPOLAR DISORDERThis is a common psychiatric mood disorder representing 2 to 3 percent of the general population. It is a genetic, inherited, familial disorder that ultimately results in biochemical imbalances within one’s central nervous system. It manifests in manic (or hypomanic, a lesser form of manic) and/or depressive mood disturbances. In my professional experience, this is by far the disorder that has the greatest coincidence with abuse or neglect of children and as such is the genetic disorder that these children with coexistent Reactive Attachment Disorder also inherit. The degree of self-centeredness, irritability and intensity of rage reactions while in a manic state is frequently sufficient to create severe abusive conditions. Correspondingly, the degree of profound depression is likewise severe and prolonged enough to create long standing neglectful circumstances.

Symptoms of Attachment DisorderSymptoms of Attachment Disorder• Superficially engaging, charming (phoniness)• Lack of eye contact• Indiscriminately affectionate with strangers• Lacking ability to give and receive affection (not cuddly on parents
terms)• Extreme control problems: often manifest in covert or “sneaky”
ways• Destructive to self, others, things• Cruelty to animals • Chronic lying• No impulse controls• Learning lags and disorders• Lacking cause and effect thinking • Lack of conscience• Abnormal eating patterns • Poor peer relationship• Preoccupied nonsense questions and incessant chatter• Inappropriately demanding and clingy • Abnormal speech patterns• Parents appear unreasonably hostile and angry

Characteristics of Attention Deficit Disorder, Bipolar Characteristics of Attention Deficit Disorder, Bipolar Disorder, and Reactive Attachment DisorderDisorder, and Reactive Attachment Disorder
John F. Alston, M.D., P.C.John F. Alston, M.D., P.C.Website: www.johnalstonmd.comWebsite: www.johnalstonmd.com
Symptoms Attention Deficit Disorder
Bipolar Disorder
Reactive Attachment
Disorder
Age of Onset Infancy to toddler, Infancy to toddler,
6 years, 13 years6 years, 13 years2 to 3 years, 6 2 to 3 years, 6 years, 13 to 25 years, 13 to 25 yearsyears
Birth to 3 yearsBirth to 3 years
Family History
ADHD, academic ADHD, academic difficulties (based on difficulties (based on task incompletion), task incompletion), alcohol and substance alcohol and substance abuseabuse
Any mood disorder Any mood disorder (depression or (depression or bipolar), academic bipolar), academic difficulties (based difficulties (based on motivation on motivation problems or problems or opposition or opposition or defiance), alcohol defiance), alcohol and substance and substance abuse, adoption, abuse, adoption, ADHDADHD
Abuse and neglect, Abuse and neglect, severe emotional and severe emotional and behavior disorders, behavior disorders, alcohol, and alcohol, and substance abuse. substance abuse. Abuse neglect in Abuse neglect in parents’ own early parents’ own early lifelife
Lifelong Prevalence
3 to 6 % general 3 to 6 % general populationpopulation
3 to 5 % of general 3 to 5 % of general populationpopulation
Uncommon to Uncommon to commoncommon
Etiology
Genetic, Genetic, Neurochemical, fetal Neurochemical, fetal development, brain development, brain traumas, nutritional traumas, nutritional deficiencies, deficiencies, exacerbated by stressexacerbated by stress
Genetic, Genetic, exacerbated by exacerbated by stress and stress and hormoneshormones
Psycho physiologic Psycho physiologic secondary to neglect, secondary to neglect, abuse, mistreatment, abuse, mistreatment, abandonmentabandonment

WORKING WITH PARENTSWORKING WITH PARENTSAssess the developmental level and needs of
parents.
1. Intact at-risk family – child remains in abusive situation.a. High incidence of parents with poor attachment
histories of their own.b. All of the qualities of unattached children still
present in grown up form.c. Not available for education (cortex).
2. Foster families.a) Assess availability for work of attachment.b) Impact of personal trauma history – usually not
explored.3. Adoptive families.
a) Education re: attachment and traumab) Family of origin history will become important and
needs to be explored over time.c) Respite !!!!


Post Traumatic Stress in Post Traumatic Stress in ParentsParents
Causes
Repeated rejectionsby child – giving and
giving with little or nolasting positive return
Relentless, unendingcontrol battles – need
for incredible self-control at all times
Changes within yourself &family that seem out of yourcontrol & are not apparent
choices
Primary Symptoms
Avoidance of thoughts & feeling,, decreased interest
& participation in significant events
Psychological/Physicaldistress at exposure to
trigger events thatsymbolize the trauma
Decreased affect & displayof feelings, sense of beingdetached or estranged from
others
Secondary Symptoms & Effects
Feeling that you are unlikeOthers, damaged sense
of self-worth,feeling out of control of emotion
Selectivity in perceptions,victim identity, fatigue and depression, loss of security
Increase arousal sleep problems,Irritable, angry,
hyper vigilance, higher startleresponse
HelplessnessHopelessness
AngerRAGE

TREATMENT FOSTER CARE:TREATMENT FOSTER CARE:Developmental ModelDevelopmental Model
.
A) Creating a circle of security in a family setting-Line of site safety-developmental circle of security with environmental controls-Parents direct and redirect -Children learn life skills living in a family i.e. doing chores, learning respectful communication, cooperative play, build self-confidence-Learn to trust that adults will keep you safe-children give up control
B) Skilled attachment therapist leads the team- Empathic confrontation – therapist is coach/guide, providing balance of challenge and support
C) Creating a circle of community support-school, police, caseworkers
D)Psychiatric Care and Neurofeedback
E)Working with Attachment Figure i.e. relative, adoptive parent, foster parent-creating safety with attachment figure by helping with emotional triggers, parent training, attachment therapy