Embed Size (px)
Citation preview

The Inhibitory Effect of Kell Blood Group Antibodies on Erythroid Progenitor Cell Growth
By
Eva Seto
A thesis submitted in conformity with the requirements for the degree of Master of Science
Department of Laboratory Medicine & Pathobiology University of Toronto
© Copyright by Eva Seto 2008

ii
The Inhibitory Effect of Kell Blood Group Antibodies on Erythroid
Progenitor Cell Growth
Eva Seto
Master of Science
Department of Laboratory Medicine & Pathobiology
University of Toronto
2008
Abstract
The clinical manifestations of hemolytic disease of the fetus and newborn mediated by anti-K, an
antibody of the Kell blood group system, have features that are distinguishable from the classical
form of the disease. Affected fetuses may have low numbers of circulating reticulocytes. As
well, antibody titers and amniotic fluid bilirubin levels are not reliable predictors of anemia.
These observations suggest that antibodies to Kell glycoprotein lead to anemia through
suppression of erythropoiesis. This study established a liquid in vitro erythroid progenitor cell
culture model in which to perform biochemical analyses on the mechanism of the suppressive
growth effect of anti-Kell glycoprotein. Using this culture model, this study demonstrated the
requirement for co-ligation of Kell glycoprotein by a bivalent antibody for growth suppression.
The absence of markers of apoptosis in cell cultures treated with anti-Kell glycoprotein suggests
that the mechanism of growth suppression is distinct from programmed cell death and necrosis.
Furthermore, this growth suppression cannot be rescued by direct addition of erythropoietin.

iii
Acknowledgements
I would like to thank my supervisor, Dr. Greg Denomme, for his mentorship and continued
support. His efforts to ensure my graduate training was a fulfilling and rewarding experience are
greatly appreciated.
I would also like to thank my committee members, Dr. B. Fernandes, Dr. G. Seaward, Dr. F.
Tsui, and Dr. C. Wang, for their guidance and valuable input throughout this project.
To all members of the Denomme lab, thank you for your friendships, great conversation and
many wonderful lunches. I would particularly like to thank Dr. D. Wang for his technical
expertise and support.
I would like to extend my sincerest gratitude to my parents, Jim and Bernice, and Gary. They
have always believed in me and provided me with unwavering support.
Finally, I would like to acknowledge funding support during my Master’s program, awarded
through the Ontario Graduate Scholarship.

iv
Table of Contents Abstract ii
Acknowledgements iii
Table of Contents iv
List of Tables vii
List of Figures viii
List of Appendices ix
Abbreviations x
1.0 Introduction 1
1.1 History of hemolytic disease of the fetus and newborn (HDFN) 2
1.2 Blood group antigens that can cause HDFN 4
1.3 Laboratory and clinical management of HDFN 5
1.4 Clinical features of anti-K HDFN 6
1.5 The Kell blood group system 7
1.6 The KEL and XK genes 8
1.7 Kell glycoprotein polymorphisms 8
1.8 Structure of Kell glycoprotein 9
1.9 Kell glycoprotein as an enzyme 11
1.10 Structure of XK 11
1.11 Function of XK 12
1.12 The Kell-Kx complex 13
1.13 Kell glycoprotein and XK are connected to the cell cytoskeleton 14
1.14 Kell and erythropoiesis 16
1.15 In vitro studies of antibodies to the Kell blood group system 18
1.16 Objectives and Hypothesis 20
2.0 Retrospective Review 21
2.1 Predictive fetal blood group genotyping 22
2.1.1 Laboratory review of fetal blood group genotyping tests 22
2.2 Clinical management of HDFN 23
2.2.1 Retrospective review of health care resource utilization 24

v
3.0 Materials and Methods 28
3.1 In vitro suppression of erythroid progenitor cells 29
3.1.1 Preparation of CD34+ cells 29
3.1.2 Preparation of antibodies 29
3.1.3 Liquid cell culture system 30
3.1.4 Immunophenotype analysis 30
3.2 Effect of anti-Kell glycoprotein Fab on erythroid progenitor proliferation 31
3.2.1 Preparation of anti-Kell glycoprotein Fab and anti-GYPC Fab 31
3.2.2 Characterization of anti-Kell glycoprotein Fab and anti-GYPC Fab product
32
3.2.3 Effect of anti-Kell glycoprotein Fab on erythroid progenitor liquid cultures
32
3.3 Role of apoptosis in the growth inhibitory effect of anti-Kell glycoprotein 33
3.3.1 Phosphatidylserine asymmetry in anti-Kell glycoprotein induced erythroid cells
33
3.3.2 Effect of a general caspase inhibitor on the growth inhibitory effect of anti-Kell glycoprotein
33
3.3.3 Caspase activation in anti-Kell glycoprotein induced erythroid cell cultures
34
3.3.4 Mitochondrial membrane potential in anti-Kell glycoprotein treated cells 34
3.4 The ability of erythropoietin to rescue the growth inhibitory effect of anti-Kell glycoprotein
34
3.5 Statistical analysis 35
4.0 Results 36
4.1 Erythroid progenitor proliferation in liquid culture system 37
4.2 Immunophenotype of erythroid progenitors in liquid culture 38
4.3 Effect of antibodies to Kell glycoprotein and blood group specific antibodies on erythroid progenitor cells in liquid culture
39
4.4 Characterization of anti-Kell glycoprotein Fab product 40
4.5 Effect of anti-Kell glycoprotein Fab on erythroid progenitor proliferation 41
4.6 Phosphatidylserine asymmetry in anti-Kell glycoprotein induced erythroid progenitors
43
4.7 Effect of a general caspase inhibitor on the growth inhibitory effect of anti-Kell glycoprotein
44

vi
4.8 Caspase activation in anti-Kell glycoprotein induced erythroid cell cultures 47
4.9 Mitochondrial membrane potential of anti-Kell glycoprotein treated cells 49
4.10 Ability of serial additions of erythropoietin to rescue growth suppression caused by anti-Kell glycoprotein
51
5.0 Discussion 53
5.1 Clinical and laboratory impact of HDFN 54
5.1.1 Laboratory review of fetal blood group genotyping tests 54
5.1.2 Retrospective review of health care resource utilization 55
5.2 In vitro suppression of erythroid progenitor cells 57
5.2.1 Progression through erythropoiesis in liquid cell culture 57
5.2.2 Suppression by antibodies to Kell glycoprotein and blood group specific antibodies
58
5.3 Requirement for antigen co-ligation for growth inhibitory effect 59
5.3.1 Characterization of Fab products 59
5.3.2 Effect of Fab products on erythroid progenitor proliferation 60
5.4 Role of apoptosis in the growth inhibitory effect of anti-Kell glycoprotein 61
5.4.1 Phosphatidylserine asymmetry in anti-Kell glycoprotein induced erythroid progenitors
61
5.4.2 Effect of a general caspase inhibitor on the growth inhibitory effect of anti-Kell glycoprotein
62
5.4.3 Caspase activation in anti-Kell glycoprotein induced erythroid cell cultures
62
5.4.4 Mitochondrial membrane potential of anti-Kell glycoprotein treated cells 63
5.5 Ability of serial additions of erythropoietin to rescue growth suppression caused by anti-Kell glycoprotein
63
5.6 Summary 64
5.7 Future Directions 65
6.0 References 68
7.0 Appendices 80

vii
List of Tables Table 1. Order of expression of cell-surface markers on differentiating erythroid cells. 18
Table 2. Summary of cost analysis for fetal blood group genotyping. 27
Table 3. Immunophenotype of CD34+ cells seeded in liquid culture. 38
Table 4. Percent of events with loss of JC-1 red fluorescence.
50

viii
List of Figures Figure 1. Diagram of the Kell-XK complex.
10
Figure 2. Schematic representation of Kell glycoprotein and XK within the 4.1R multiprotein complex in the red cell membrane.
15
Figure 3. Distribution of antigens for which fetal blood group was tested.
23
Figure 4. Comparison of the mean number of clinic visits or procedures per woman with Kell-positive, antigen-positive, or antigen-negative fetus.
26
Figure 5. Representative cell proliferation in two-stage culture protocol in the absence of suppressive antibody.
37
Figure 6. Percent growth suppression of treated erythroid progenitors.
39
Figure 7. Suppression of progenitor proliferation by anti-Kell glycoprotein Fab and anti-(heavy and light chain).
42
Figure 8. Annexin V-FITC and PI labeling of erythroid progenitors treated with anti-Kell glycoprotein.
43
Figure 9. Suppression of progenitor proliferation by anti-Kell glycoprotein in the presence of Z-VAD-FMK.
45
Figure 10. Suppression of progenitor proliferation by etoposide and partial rescue by Z-VAD.
46
Figure 11. Mean fluorescence intensity of ApoStat of erythroid progenitors treated with anti-Kell glycoprotein.
48
Figure 12. JC-1 assay of anti-Kell glycoprotein treated erythroid progenitors.
49
Figure 13. Proliferation of erythroid progenitors in the presence of serially added excess erythropoietin and anti-Kell glycoprotein.
52

ix
List of Appendices Appendix A. Agglutination grading of indirect agglutination test. 81
Appendix B. Cell surface marker expression of CD34+ cells seeded in liquid culture. 82
Appendix C. Non-reducing SDS-PAGE analysis of Kell glycoprotein Fab product. 83
Appendix D. Characterization of anti-GYPC Fab product. 84
Appendix E. Non-reducing SDS-PAGE analysis of anti-GYPC Fab product. 85
Appendix F. Effect of anti-GYPC Fab on erythroid progenitor proliferation. 86
Appendix G. Caspase activation of erythroid progenitors treated with anti-Kell glycoprotein
87

x
Abbreviations ~(H+L) anti-(heavy and light chain) 4.1R protein 4.1 BCA bicinchoninic acid BFU-E burst-forming unit-erythroid BrdU 5-bromo-2-deoxyuridine CCCP carbonyl cyanide 3-chlorophenylhydrazone cdk cyclin-dependent kinase CFU-E colony-forming unit-erythroid CFU-GEMM colony-forming unit-granulocyte, erythroid, macrophage, megakaryocyte DIM detergent-insoluble material DMSO dimethyl sulfoxide Epo erythropoietin ET-3 endothelin-3 FACS fluorescence activated cell sorting FITC fluorescein isothiocyanate Ge Gerbich GM-CSF granulocyte-macrophage colony stimulating factor GP glycoprotein GYPA glycophorin A GYPC glycophorin C HDFN hemolytic disease of the fetus and newborn IgG immunoglobulin G IL interleukin IMDM Iscove’s Modified Dulbecco’s Medium IVIG intravenous immune globulin JAK2 Janus kinase 2 JC-1 5,5’,6,6’-tetrachloro-1,1’,3,3’-tetraethylbenzimidazol-carbocyanine iodide K Kell, KEL1 K0 Kell-null k Cellano, KEL2 MAP mitogen-activated protein MFI mean fluorescence intensity MWCO molecular weight cut off OHIP Ontario Health Insurance Plan PBS phosphate buffered saline PI propidium iodide pRb retinoblastoma protein PS phosphatidylserine RBC red blood cell Rh Rhesus RhAG Rh-associated glycoprotein SCF stem cell factor SDS-PAGE sodium dodecyl sulfate – polyacrylamide gel electrophoresis

xi
SEM standard error of the mean Stat signal transducer and activator of transcription Z-VAD-FMK Z-Val-Ala-Asp-CH2F-fluoromethyl ketone

1
Chapter 1
Introduction

2
1.1 History of hemolytic disease of the fetus and newborn (HDFN)
The first description of hemolytic disease of the fetus and newborn (HDFN) is thought to be in
1609 by Louise Bourgeois, a French midwife who delivered twins—one of whom had hydrops
fetalis and died soon after birth, the other baby was icteric and died several days later. For the
next 300 years, the literature is replete with reports of neonates with apparently unrelated and
unexplained syndromes characterized by varying degrees of severe jaundice (“icterus gravis
neonatorum”), generalized edema (“universal edema of the fetus”), or severe anemia
(“congenital anemia of the newborn”). It was not until Dr. Louis K. Diamond’s groundbreaking
study in 1932 (Diamond et al. 1932) that these syndromes were recognized to be manifestations
of the same disease process. The term “erythroblastosis fetalis” coined by Rautmann in 1912
(Rautmann 1912) to describe the blood findings in cases of universal edema was such a
prominent feature that it was used widely to describe these syndromes until it was replaced by
‘hemolytic disease of the newborn’. However, it was recognized that ‘hemolytic disease of the
newborn’ did not fully describe the continuum of the disorder: the hemolytic disease did not
evolve at birth but was present in fetuses. Thus, in more recent years, the term ‘hemolytic
disease of the fetus and newborn’ has been favoured.
In 1938, Darrow postulated that the hemolysis is due to transplacental passage of maternal
antibodies to the fetal circulation (Darrow 1938). One year later, an unusual case of intra-group
agglutination was reported: an immediate reaction in a blood group O woman who had received
her husband’s group O blood shortly after delivery of a stillborn fetus with erythroblastosis
(Levine et al. 1939). Levine’s suggestion that the infant had inherited a ‘blood factor’ (red blood
cell antigen) from the father that was immunologically foreign to the mother led to the discovery
of the Rhesus (Rh) system, the first non-ABO blood group system, by Landsteiner and Weiner in
1940 (Landsteiner et al. 1940). This discovery laid the groundwork for Levine (Levine et al.
1941) to implicate feto-maternal Rh incompatibility as the cause of hemolysis in neonates with
erythroblastosis fetalis. Levine et al. observed that women with hemolytic transfusion reactions
occurring in the absence of ABO incompatibility were negative for the newly discovered Rh type
and the atypical agglutinin in their serum had Rh specificity. The final link came from the
observation that the infants of these women were frequently stillborn or died soon after birth
with erythroblastosis fetalis. In 1954, Chown’s report of mothers becoming sensitized as a result

3
of transplacental hemorrhage made the association between fetal red blood cells (RBC) and the
stimulation of maternal antibody production (Chown 1954).
HDFN is a classic example of type II immune hypersensitivity (Hughes-Jones et al. 1982). It is
caused by erythroid specific antibodies in alloimmunized women that cross the placenta into the
fetus where they initiate immune destruction of fetal erythroid cells. Most clinically significant
antibodies to red cell surface antigens are produced in response to antigen-positive red cells:
either donor red cells following transfusion, or cells of fetal origin that carry an antigen inherited
from the father, following fetomaternal hemorrhage during pregnancy or at parturition.
Antibodies that cause HDFN are restricted to Immunoglobulin G (IgG) (mostly IgG1 and IgG3),
as antibodies of other classes are not transported across the placental barrier. These antibodies
are often produced with high affinity and in high titer. When they are transferred to the fetus,
IgG-coated fetal and neonatal red cells are lysed by splenic macrophages (Archer 1965).
Once immunization occurs, several factors determine the severity of the resulting hemolytic
disease. They include the antigen specificity, the titer and affinity of the antibody, and the
immunoglobulin subclass. HDFN at its most severe may cause fetal death as early as the 17th
week of pregnancy (Daniels et al. 2006). However, many antigen-positive infants with
detectable maternal blood group-specific antibodies in their serum are unaffected or only mildly
affected and require no treatment; about 20 percent are severely affected in utero (Eder et al.
2004; Moise 2005). About one-half of those severely affected fetuses have significant hemolysis
before 34 weeks’ gestation and require intrauterine transfusion. The hemolysis caused by red
blood cell sensitization and removal from the circulation by the mononuclear phagocytic system
results in anemia and the formation of the breakdown products of hemoglobin. HDFN can
demonstrate a broad spectrum of symptoms ranging from mild anemia and hyperbilirubinemia in
an infant to life-threatening complications before birth. Fetal anemia can lead to congestive
heart failure, intrauterine growth retardation, and hydrops as a consequence of hepatic
dysfunction. If the infant is born alive, hydrops developed in utero may be evident and the
disease can result in the accumulation of unconjugated bilirubin in the infant (jaundice) because
the infant’s liver cannot conjugate bilirubin at a rate necessary to clear the bilirubin from the
massive RBC destruction. Unconjugated hyperbilirubinemia can develop into kernicterus and

4
cause permanent cerebral damage leading to infant death. At its mildest, neonatal jaundice, often
treated with phototherapy, is the only clinical sign of HDFN.
1.2 Blood group antigens that can cause HDFN
Human red cells express numerous polymorphic surface proteins that are antigenic and
consequently have blood group specificity. Antibodies to these structures are important in
HDFN and transfusion medicine and have led to a very detailed understanding of the nature of
the red cell surface. There are at least 29 blood group systems on mature erythrocytes, which
express as many as 302 known antigens (Daniels et al. 2007). Distinguishing between
potentially clinically significant and non-clinically significant antibodies is important in
alloimunized women to predict the severity of HDFN. Anti-D is the most common antibody
specificity that causes HDFN. The advent of the routine administration of antenatal and
postpartum Rh immune globulin for preventing D-negative women from producing anti-D after
or during a D-positive pregnancy, has significantly reduced the incidence of this type of
alloimmunization. Since the introduction of routine postpartum prophylaxis in the 1960s, the
incidence of Rh alloimmunization in the U.S. and Canada has fallen from 10.0 cases to 6.7 cases
for every 1000 live-born infants (Bowman et al. 1977; Martin et al. 2002). However, HDFN
continues to be a challenge in the management of fetal morbidity and mortality and attention has
increasingly been focused on other clinically significant blood group antibodies for which
immune prophylaxis is unavailable. More than 50 different red-cell antigens have been reported
to be associated with HDFN (Moise 2008), but most cases of severe fetal anemia that require
treatment in utero are caused by anti-D, anti-c, or anti-K (Kell). Severe hemolytic disease
requiring intrauterine transfusion were caused by anti-D, -c, or –K in 85 percent, 3.5 percent, and
10 percent of hemolytic anemia cases, respectively (van Kamp et al. 2005).

5
1.3 Laboratory and clinical management of HDFN
Over the course of the last decade, the molecular bases for almost all of the clinically significant
blood group polymorphisms have been elucidated. Consequently, it is now possible to determine
blood group phenotypes from DNA with a high degree of accuracy. This technology is being
applied to determining blood groups when suitable red cells are not available, such as fetal
testing. Predictive prenatal genotyping has played an important role in the detection of fetuses at
risk for HDFN.
The clinical management of potential HDFN relies first on the measurement of antibody levels in
the maternal circulation. If antibody levels are high, amniocentesis may be performed to assess
the extent of fetal hemolysis more accurately and to collect amniotic fluid samples to be used in
molecular blood group genotyping. However, these invasive procedures have associated risks
including pregnancy loss or transplacental hemorrhage leading to stimulation of maternal
antibody levels and a worsening of fetal anemia (Eisenberg et al. 2002; Alfirevic et al. 2007).
The initial blood group and antibody screen that is performed for all pregnant women not only
identifies D-negative women who are candidates for Rh immunoglobulin prophylaxis, but also
identifies women who are already alloimmunized who require further monitoring for HDFN.
When a clinically significant maternal antibody is present, the blood group zygosity of the
biological father should be determined by blood group antigen typing. The results from paternal
antigen phenotyping is used to assess whether there is a 50:50 chance the fetus can inherit the
autosomal gene. Serologic phenotyping using red cells is appropriate for all antigens with the
exception of RhD because there is no antithetic allele. If the father is heterozygous for the blood
group antigen, fetal genetic testing should be considered in the context of clinical indicators.
Thus, the predictive test is valuable in that fetuses found to be at risk for HDFN can be closely
monitored for possible intervention whereas fetuses found to be antigen-negative require no
further surveillance and can return to routine care.

6
1.4 Clinical features of anti-K HDFN
Antibodies to the Kell blood group system cause life-threatening transfusion reactions and severe
alloimmune anemia, with alloantibodies to the K antigen the most common (Coombs et al. 1946;
Race et al. 1975; Salmon et al. 1984). In fact, maternal anti-K is the second most common
alloantibody after anti-D and accounts for 10-15% of all cases of antibody-mediated severe
hemolytic anemia (Vaughan et al. 1991). In one series of tests, maternal anti-K was detected in
127 pregnancies. Thirteen of 127 pregnancies with maternal anti-K resulted in a K-positive
baby, 5 (38%) of whom were severely affected with HDFN (Caine et al. 1986). The reason for
the low incidence is because the father may not be positive for the K antigen; most anti-K appear
to be induced by blood transfusion. Therefore, it is not surprising that it is becoming common
practice in some countries for girls and women of childbearing age to be transfused only with K-
negative red cells, though anti-K stimulated by transfusion seems to cause a less severe disease
than anti-K stimulated by a previous pregnancy (Poole et al. 2007). Subsequent pregnancies are
more likely to be severely affected than first pregnancies because of the anamnestic immune
response. IgG anti-K is a persistent antibody and is usually detectable in a patient’s serum for
many years after an immunization event. In addition to anti-K, antibodies of all Kell blood
group system specificities have the potential to cause HDFN. At least eight of the antigens have
been associated with HDFN although cases are usually, but not invariably, mild. HDFN
requiring at least fetal transfusion has been reported for anti-K, -Kpa (KEL3), -Kpb (KEL4), -Jsa
(KEL6), -Jsb (KEL7), -Ula, -Ku (KEL5), –K22, and -Ula (KEL10).
The clinical characteristics of anti-K HDFN are distinguishable from the classical form of the
disease caused by anti-D. The utility of antibody titers in monitoring K-antigen-sensitized
pregnancies is limited because the severity of intrauterine disease may not correlate with
maternal serum antibody titres (Bowman et al. 1992). It is also harder to predict severity of anti-
K disease from amniotic fluid bilirubin levels obtained from serial amniocentesis since anti-K
HDFN is associated with lower concentrations of amniotic fluid bilirubin than in anti-D HDFN
of equivalent severity (Leggat et al. 1991; Weiner et al. 1996). Postnatal hyperbilirubinemia is
not prominent in babies with hemolytic disease caused by anti-K. Affected fetuses have lower
numbers of circulating reticulocytes and normoblasts compared to fetuses with anti-D HDFN,
with levels that are inappropriately low for the degree of fetal anemia (Weiner et al. 1996).

7
There is also reduced reticulocytosis and erythroblastosis in the anti-K disease compared with
anti-D HDFN (Weiner et al. 1996).
These observations have led to the hypothesis that the pathogenesis of HDFN caused by anti-K
differs from that due to anti-D. There may be less hemolysis in HDFN caused by anti-K
compared with HDFN of comparable severity due to anti-D, and fetal anemia in anti-K HDFN
may result predominantly from a suppression of erythropoiesis (Weiner et al. 1996; Vaughan et
al. 1998). Recent findings suggest that anti-K results in the phagocytosis of early erythroid
progenitor cells (Daniels et al. 2003) before they become sufficiently hemoglobinised since Kell
glycoprotein is one of the first erythroid-specific antigens to appear on erythroid progenitors
during erythropoiesis, whereas the Rh proteins appear much later. Moreover, anti-K has been
shown to suppress erythropoiesis in vitro (Weiner et al. 1996; Vaughan et al. 1998).
1.5 The Kell blood group system
The Kell system was first identified in 1946 by Coombs with the help of his newly developed
antiglobulin test (Coombs et al. 1946). Rh incompatibility with the mother, Mrs. Kell, had been
ruled out as the cause of hemolytic disease in her child. Subsequently, Kell became one of the
most important blood group systems in transfusion medicine. The Kell blood group system is
distinguished by its highly polymorphic nature having more than 28 alloantigens.
The expression of the Kell blood group antigens relies on two proteins, Kell glycoprotein and
XK, which are linked by a disulfide bond and encoded by two different genes. One is the
autosomal gene, KEL, which codes for the 93 kDa glycoprotein that contains the Kell blood
group antigens (Lee et al. 1995). The other, XK, is X-linked and codes for a 50.9 kDa protein
that carries the Kx antigen (Bertelson et al. 1988).

8
1.6 The KEL and XK genes
The KEL gene spans about 21.5 kb on chromosome 7q33 with its coding sequence organized into
19 exons ranging in size from 63 to 283 bp. The 5’ untranslated region does not contain a TATA
sequence and instead has several GATA-1 and SP-1 binding sites (Lee et al. 1995). Although
Kell expression is highest in erythroid cells, recent studies also show substantial expression on
myeloid progenitor cells and testis and a lesser amount in other tissues such as the brain, heart,
and skeletal muscle (Lee et al. 2000; Wagner et al. 2002). KEL shares a consensus sequence
with a large family of M13 zinc-dependent endopeptidases (Lee et al. 1999).
The XK gene is mapped to Xp21 at a region between the Duchenne muscular dystrophy gene and
the chronic granulomatous disease gene (Bertelson et al. 1988). The 5’ untranslated region of
XK is 82 bp, and the transcript contains a large, 3713 bp, 3’ untranslated region. The gene is
composed of three exons, with exon 1 towards the telomere and exon 3 closest to the centromere
of the chromosome. The XK expression is highest in erythroid cells and skeletal muscle and is
expressed to a lesser degree in the heart, brain, and pancreas (Lee et al. 2000).
1.7 Kell glycoprotein polymorphisms
While the role of the Kell glycoprotein in red cell physiology is unknown, the Kell blood group
system is well characterized in terms of its antigenicity. The Kell blood group system is highly
polymorphic, and at present is known to express 28 different alloantigens that have been
classified into five antithetical sets of high and low prevalence antigens with the others being
independently expressed or having unknown antithetical partners. The different phenotypes are
due to single nucleotide mutations in the coding region of the KEL gene that result in an amino
acid substitution leading to the presentation of different cell surface epitopes (Lee 1997; Lee et
al. 2000). Inheritance is autosomal and codominant. The KEL1 (K)/KEL2 (k) antithetical allelic
set of antigens is of particular interest because the K antigen is the most immunogenic of all the
Kell antigens and antibodies to K comprise the vast majority of Kell HDFN cases. Antibodies to
K develop in about 5% of K-negative persons receiving a single unit of K-positive incompatible
blood (Giblett 1961). Approximately 9% of the Caucasian population and 2% of people of
African descent have the K-POSITIVE RBC phenotype with virtually all antigen positive
individuals being heterozygous. The allele, KEL1, is due to a 698C T nucleotide change in

9
KEL2 that results in a Thr193 Met substitution at an N-glycosylation consensus sequence, and
the glycoprotein is expected to have four instead of five N-linked carbohydrate moieties (Lee et
al. 1995). Lack of a carbohydrate side chain may expose different parts of the protein leading to
immunogenicity.
Point mutations can affect the number of copies of Kell glycoprotein on the red cell membrane.
One such phenotype is the Kell-null (K0) phenotype, where the Kell glycoprotein and thus the
Kell antigens are absent from the surface of the red cell membrane. The most common mutation
causing this phenotype introduces premature stop codons in exons 4, 6, and 9, downstream from
exon 3, which encodes the transmembrane domain, producing a truncated protein. These
truncated proteins are presumably degraded intracellularly and are not transported to the cell
surface (Daniels et al. 1996; Lee et al. 2001).
Kell expression may be affected by its association with the XK protein. In the McLeod
phenotype, the red cells have depressed expression of Kell and lack XK. XK gene mutations
comprised of deletions, nonsense, or slice-site mutations lead to the absence of the XK protein or
the production of a truncated XK that is devoid of the Kell glycoprotein-binding site (Ballas et
al. 1990; Jung et al. 2003).
1.8 Structure of Kell glycoprotein
The Kell protein is a 93 kDa type II red cell membrane glycoprotein which spans the plasma
membrane once (Lee et al. 1993). Kell has a short 46 amino acid intracellular N-terminal
domain, a single transmembrane domain, and a large 665 amino acid extracellular C-terminal
domain which contains a zinc-binding catalytic pentapeptide consensus sequence, HExxH (in
Kell, HELLH) (Lee 1997). The Kell glycoprotein contains five possible N-glycosylation sites
and 16 cysteine residues (Figure 1). One of the cysteine residues is linked to Kx and another is
located within the transmembrane domain. The remaining 14 are on the ectodomain, forming
seven intramolecular disulphide bonds that stabilize the extracellular structure and preserve the
endopeptidase activity of the Kell protein. A three-dimensional model of Kell protein,
constructed on the basis of the crystal structure of neutral endopeptidase 24.11, showed that Kell
has two globular extracellular domains consisting largely of α-helical structures (Lee et al.

10
2003). The domain closest to the cell membrane contains the enzyme-active site. The surface of
the other domain, away from the active site contains the amino acid residues whose substitutions
lead to the different phenotypes.
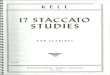
Figure 1. Diagram of the Kell-XK complex.
The transmembrane domains of Kell and XK are depicted as cylinders. Cysteine residues are
marked by “C” and the Kell Cys72 to XK Cys347 disulfide linkage is shown. The location of
the Kell blood group polymorphisms and the zinc-binding enzymatic active site, HELLH, is
shown (Lee et al. 2000) (used with permission).

11
1.9 Kell glycoprotein as an enzyme
Kell glycoprotein shows substantial homology with the neprilysin (M13) subfamily of
mammalian zinc-dependent endopeptidases; enzymes that process a variety of biologically active
peptides. Kell activates endothelins with a preference for endothelin-3 (ET-3). Recombinant
soluble Kell and human red cells expressing Kell process ET-3 by cleavage of its biologically
inactive precursor, big ET-3 (Lee et al. 1999). ET-3 is a potent biopeptide with multiple
physiological functions including control of developmental processes, ion transport, and acting
as a vasoconstrictor regulating vascular tone (Stjernquist 1998). In a recent study of catalytic
activity, it was found that K-POSITIVE red blood cells have a similar big endothelin-3-cleaving
activity compared to the common k-positive phenotype (Sha et al. 2006). This is not surprising
as the single nucleotide polymorphism that leads to the amino acid substitution in the K-
POSITIVE phenotype is present in the outer globular domain which is distinct from the enzyme
active site. Kell’s structural similarity to endopeptidases may suggest a role in protein regulation
and cell growth in erythroid cells (Vaughan et al. 1998). However, the physiological role of
Kell’s putative enzymatic activity is unclear and it is not known whether the Kell glycoprotein
processes any other biopeptides. K0 cells, which lack all Kell antigens, are clinically and
haematologically normal and exhibit no defects in erythropoiesis (Marsh et al. 1990).
1.10 Structure of XK
XK is a non-glycosylated polytopic 50.9 kDa protein that is predicted to have 10 transmembrane
domains with intracellular N- and C- termini and shows structural characteristics of prokaryotic
and eukaryotic membrane transport proteins (Ho et al. 1994). The N-terminal domain of XK
consists of only three amino acids, while the C-terminal domain is composed of 71 amino acids
(Russo et al. 1998). It shares extensive similarities with the ced-8 protein of the nematode
Caenorhabditis elegans where it controls the timing of programmed cell death (Khamlichi et al.
1995). XK is linked to the Kell glycoprotein by a single disulphide bond (XKcys347-
KellCys72) (Lee et al. 2000).

12
1.11 Function of XK
The Kx blood group system is composed of a single antigen, Kx, which is carried on the XK
protein. The Kx epitope is not defined and the function of the XK protein is unclear. However,
the absence of XK due to mutations in the XK gene, results in McLeod syndrome, an X-linked
multisystem disorder that is assigned to the neuroacanthocytosis syndromes. It is characterized
by the absence of the Kx antigen, weak expression of Kell antigens, acanthocytosis and
compensated hemolysis (Allen et al. 1961). Late onset neuromuscular manifestations include
myopathy, sensory-motor axonal neuropathy, and cardiomyopathy. Central nervous system
manifestations are similar to that of Huntington’s disease and consist of a choreatic movement
disorder, ‘subcortical’ neurobehavioural deficits, psychiatric abnormalities and generalized
seizures (Walker et al. 2007). The precise mechanism of acanthocytosis in McLeod red cells is
unknown. A number of factors, including lipid depletion or enrichment, phosphorylation of
lipids, and cytoskeletal or ionic abnormalities, can influence the lipid bilayer and thus can change
the shape of RBCs (Steck 1989). In McLeod red cells, there are no obvious factors other than
the absence of the XK protein that could contribute to the aberrant red cell morphology. Thus,
the membrane protein appears to be essential for the cellular integrity of RBCs, and defects in
transport, interactions, or both with neighbouring proteins could result in abnormal cell shape
(Ho et al. 1994).
Although the exact function of the human XK protein is not yet known, XK bears some
resemblance to an Na+-dependent glutamate transporter due to its 10 transmembrane domains
and large extracellular second loop. But, there is very little primary sequence homology between
the two varieties and the substrate of XK is not known. Six of XK’s transmembrane regions
contains charged amino acid residues (Ho et al. 1994). Depending on their arrangement, these
hydrophilic groups can form salt-bridges within the membrane, stabilizing the structure and
perhaps forming a hydrophilic pore in the membrane (Lee et al. 2000). Furthermore, XK has
numerous consensus phosphorylation sites and is a substrate for casein kinase II and protein
kinase C (Carbonnet et al. 1998). Whether XK plays a part in maintaining the proper lipid
bilayer balance is not known, but it is possible that XK has a role in stabilizing the red cell
membrane and cytoskeletal structure (Marsh et al. 1990).

13
1.12 The Kell-Kx complex
The covalent biochemical relationship of the complex formed by the Kell glycoprotein and XK
explains early serologic observations, which indicated that the expression of Kell and Kx
antigens are inter-related. Ho and associates (1994) postulated that XK may interact and
stabilize the expression of Kell and absence of XK would then result in an unstable Kell
glycoprotein, leading to decreased amounts of expression. This notion is supported by studies of
RBCs with the McLeod phenotype that showed a very weak expression of all Kell antigens.
However, RBCs with the K0 phenotype, which lacks all Kell antigens, have enhanced Kx antigen
expression (Lee et al. 2000). Western blot analyses showed that McLeod RBCs have reduced
amounts of Kell glycoprotein but, paradoxically, that K0 RBCs have a diminished, and not an
increased, amount of XK protein (Carbonnet et al. 1997). Based on the structures of the Kell-
XK complex, it is speculated that, in wild-type RBCs, the Kell glycoprotein ectodomain partially
covers the Kx epitope and when Kell is absent, as in Ko RBCs, the Kx epitope is fully exposed
(Lee 2007). K0 red cells, which appear to lack the membrane protein entirely, have normal
morphology and in vivo survival.
In erythrocytes, Kell and XK form a disulfide-linked complex, which is dependent on the
expression of XK protein (Ho et al. 1994; Calenda et al. 2006). However, Kell and XK may not
form a complex in non-erythroid tissues (Russo et al. 2000). XK is expressed independently of
Kell in the central nervous system (Claperon et al. 2007) and it is likely that the absence of XK
from the brain is responsible for the neurological symptoms associated with McLeod syndrome.

14
1.13 Kell glycoprotein and XK are connected to the cell cytoskeleton
When Kell is isolated by immunoprecipitation and sodium dodecyl sulfate – polyacrylamide gel
electrophoresis (SDS-PAGE) from red cells under non-reducing conditions, one obtains a series
of protein complexes with molecular sizes from 93 kDa up to more than 200 kDa (Redman et al.
1984; Redman et al. 1986). Each complex contains Kell non-covalently associated with other
proteins. Western blot analysis of the other proteins which co-immunoprecipitate with Kell
glycoprotein shows protein 4.1 (4.1R), spectrin, and a protein with electrophoretic mobility
similar to actin (Marsh et al. 1987). Thus, three of the major components of the red cell
cytoskeletal system are present in the immunoprecipitate. These data suggest that Kell
glycoprotein is associated with the underlying cytoskeleton. Furthermore, flow cytometry
studies of the membrane skeleton, which is experimentally defined as the detergent-insoluble
material (DIM) of the RBC after Triton-X extraction, have investigated the association of blood
group proteins and the cytoskeleton. The percentage of association of cell surface markers to the
DIM was calculated from the ratio of specific mean fluorescence intensity before and after Triton
X-100 extraction. Analysis of late erythroid precursors and human erythroleukemia K562 cells
have determined that both K and k Kell glycoprotein phenotypes have a percentage of
association with the underlying cytoskeleton of 27-96% (Gane et al. 2001). These findings
indicate that the inner portion of Kell is complexed with the cell cytoskeleton.
A recent study of 4.1R-deficient mouse red cells has provided evidence that XK, but not Kell
glycoprotein, is directly connected to the 30-kDa membrane-binding domain of 4.1R (Salomao et
al. 2008). Western blot analysis of 4.1R-/- cells showed that XK, but not Kell glycoprotein, was
significantly reduced. However, there was a significant reduction in Kell glycoprotein detected
by flow cytometry of 4.1R-/- cells with antibodies against the extracellular epitopes of Kell
glycoprotein. A streptavidin pull-down assay to examine direct binding of membrane proteins to
4.1R showed that XK, but not Kell glycoprotein, binds specifically to 4.1R. The finding of
normal levels of Kell glycoprotein by Western blot analysis but reduced levels by flow
cytometric analysis suggests possible conformational change of Kell epitopes in intact
membranes of 4.1R-deficient cells due to reduction of XK. A schematic representation of XK
and Kell glycoprotein’s position within the 4.1R complex is presented in Figure 2.

15
Figure 2. Schematic representation of Kell glycoprotein and XK within the 4.1R
multiprotein complex in the red cell membrane.
The protein complex lies at membrane skeletal junctions containing the ternary complex of
spectrin, F-actin, and 4.1R, as well as the actin-binding proteins tropomyosin, tropomodulin,
adducin, and dematin. 4.1R enters into an additional ternary interaction with glycophorin C and
p55 and also binds to band 3 (Salomao et al. 2008) (Copyright 2008 National Academy of
Sciences, U.S.A.).

16
1.14 Kell and erythropoiesis
Erythropoiesis defines the highly regulated process of differentiation and proliferation from
hematopoietic stem cells to mature erythrocytes. The primary sites of blood cell production
changes throughout the development of most vertebrates (Zon 1995). The yolk sac is the first
site of blood cell production during human ontogeny. Thickenings in the yolk sac inner
mesodermal layer develop into blood islands, endothelial sacs containing hematopoietic
cytoblasts, and differentiated embryonic erythrocytes. As the embryo develops, early circulation
is maintained by definitive hematopoietic stem cells localized to the para-aortic splanchnopleure
tissue in the ventral aspect of the embryo, which forms the region of aorta, gonad, and
mesonephros (Cormier et al. 1986; Huyhn et al. 1995). By mid-gestation, the liver is the main
organ responsible for erythrocyte production. At approximately 36 weeks’ gestation, RBC
production is limited to the bone marrow. Initially, many bones are involved in erythrocyte
production, including the femur, tibia, rib, sternum, and vertebra. After 20 years of age, most
RBC production is limited to the vertebra, sternum, ribs, and ilia, in decreasing order of
importance (Bieber 2001; Palis et al. 2001).
Erythropoiesis proceeds through the tightly regulated and stepwise differentiation from
pluripotent hematopoietic stem cells to mature erythrocytes. In response to SCF, IL-1, IL-3, IL-
6 and IL-11, hematopoietic progenitors generate mixed colonies in vitro (colony-forming unit-
granulocyte, erythroid, macrophage, megakaryocyte, CFU-GEMM), after which GM-CSF, SCF,
and IL-3 will further differentiate the colonies into committed erythroid progenitors (burst-
forming unit – erythroid, BFU-E) characterized in vitro as large erythroid-like colonies.
Additional stimulation by GM-CSF, IL-3, SCF, and Epo induces the BFU-E to differentiate into
late erythroid progenitors (colony-forming unit – erythroid, CFU-E) characterized as small
erythroid colonies. BFU-E progenitors take about 14 days to differentiate in vitro to form large
colonies; CFU-E progenitors take about 7 days to form colonies in vitro. CFU-E progenitors
undergo 3-5 mitotic divisions to differentiate into terminal erythroid cells through a series of
maturation steps in which they undergo a progressive decrease in their size, an increase in
hemoglobin concentration and an increase in chromatin density. The cells also become
progressively sensitive to erythropoietin (Epo) due to the appearance of the Epo receptor on
these cells. In the presence of Epo, CFU-E cells differentiate into morphologically recognizable

17
erythroid precursors: proerythroblasts and then basophilic erythroblasts, which are the first cells
in the pathway to synthesize hemoglobin. At the polychromatophilic erythroblast stage the first
microscopic sign of hemoglobin can be detected. Orthochromatic erythroblasts then undergo
major morphological changes, as they expulse their nucleus as well as their organelles to become
disc-shaped, hemoglobin-containing terminally differentiated erythrocytes. Enucleation is reliant
on the formation of a contractile actin ring on the plasma membrane of enucleating erythroblasts,
which is dependent on Rac GTPases and their effector mDia2 (Ji et al. 2008). Enucleating
erythroblasts cluster around a macrophage to form erythroblastic islands (Sadahira et al. 1999)
and the extruded nuclei are then engulfed by the macrophage and the erythroblasts mature into
reticulocytes, young erythrocytes. The reticulocytes remain in the bone marrow for
approximately two days before they are released into the circulation where they lose their
cytoplasmic organelles and begin to behave metabolically like mature erythrocytes (Daniels et al.
2000; Bieber 2001).
The Kell antigen is known to be expressed early in fetal life at about the tenth week of gestation
(Bony et al. 1999). Flow cytometric analysis of CD34+ cells from cord blood using Kell
antibodies indicate that Kell antigens are present at an early stage of erythroid maturation (Bony
et al. 1999). A time course analysis of the expression of blood group antigens during
erythropoiesis confirm that Kell glycoprotein appears after glycophorin C (GYPC) and before
the Rh-associated glycoprotein (RhAG) (Table 1) (Bony et al. 1999; Southcott et al. 1999;
Daniels et al. 2000). Interestingly, maternal antibodies to the Gerbich (Ge) blood group system
carried on GYPC have been shown to lead to late onset anemia requiring transfusion in infants
(Arndt et al. 2005). HDFN cases due to anti-Ge are rare but reports describe similar clinical
features as HDFN due to anti-K. Moreover, in vitro studies have shown suppression of erythroid
progenitor cell growth by anti-Ge3 (Denomme et al. 2006).

18
Days of culture Cell surface antigen 0 Glycophorin C (GYPC) ⋅ Kell glycoprotein 4 Rh-associated glycoprotein 5 Glycophorin A (GYPA) 6 Band 3, Wrb ⋅ Emm ⋅ Xga
7 RhD, RhCcEe ⋅ Glycophorin B (GYPB) ⋅ Duffy glycoprotein ⋅ Lutheran glycoprotein
Table 1. Order of expression of cell-surface markers on differentiating erythroid cells.
Time in culture for 50% of seeded CD34+ cells to become antigen-positive using a one-stage,
serum culture technique (Daniels et al. 2000).
1.15 In vitro studies of antibodies to the Kell blood group system
The body of in vitro and in vivo evidence suggests that fetal anemia in cases of Kell sensitization
is due to two mechanisms: red cell destruction and suppression of erythropoiesis. The exact
contribution of these two mechanisms has not been studied. If the latter mechanism is
predominant, this would offer an explanation in part for the decreased predictability of amniotic
fluid bilirubin levels in anti-K HDFN.
In 1998, Vaughan et al. conducted an in vitro analysis of erythroid progenitors to assess the
impact of anti-K antibodies on erythropoiesis as compared to anti-D antibodies (Vaughan et al.
1998). Serum from women sensitized to the K antigen suppressed the growth of K-positive
erythroid BFU-E and CFU-E. Monoclonal anti-K also caused a dose-dependent suppression of
growth in erythroid cells from umbilical cord blood. Monoclonal anti-D exhibited no
suppression. These observations implied that suppression of erythroid progenitor cell
proliferation was responsible for the unique pathological features of HDFN due to anti-K.
In a report by Daniels and coworkers (2003), it was suggested that anti-K may cause fetal anemia
by inducing monocyte phagocytosis of early erythroid progenitor cells. They observed in vitro
monocyte phagocytosis of anti-K sensitized immature erythroid cells. This observation also

19
provides an explanation for the lower bilirubin levels in amniotic fluid compared to the classical
form of the disease caused by anti-D since the destruction of progenitor cells is at a stage when
no hemoglobin is present in the cell.
Previous studies performed in our lab have confirmed the in vitro suppression of erythropoiesis
and suggest that, in addition to phagocytosis of IgG sensitized early erythroid cells, this
suppression may be a factor leading to the observed clinical manifestations in anti-K HDFN.
The generation of BFU and CFU-E colonies from mononuclear cells isolated from cord blood
was evaluated with a semi-solid methylcellulose assay in the presence of maternal anti-K,
commercially available monoclonal IgM anti-K, polyclonal IgG anti-K and anti-k, and a murine
anti-Kell glycoprotein. The independence of antibody class and specificity confirmed that the in
vitro observations of suppression of erythroid colonies by antibodies to the Kell glycoprotein is
not due to Fcγ receptor-mediated phagocytosis (Shahcheraghi 2005). Studies using isolated
CD34+ cells showed the suppression of erythropoiesis in the absence of other cord blood
nucleated immune cells and suggest that the suppression of erythroid progenitor cell proliferation
is a direct effect of the binding of the antibodies to the Kell glycoprotein (Shahcheraghi 2005).

20
1.16 Objectives and Hypothesis
The potential to benefit from studies on the pathobiology of HDFN due to anti-K was evaluated
by investigating the prevalence of anti-K HDFN through a retrospective review of laboratory
fetal blood group genotyping tests over a 10-year period. The clinical impact of HDFN and the
potential to benefit from research into new therapies was investigated through a retrospective
review of the health care resources and clinical procedures necessary to monitor fetuses at risk
for HDFN.
Presently, it is unclear how antibodies directed to the Kell blood group antigen suppress the
proliferation of erythroid progenitor cells. The principle objective of this study was to develop
an in vitro liquid cell culture model using commercially available anti-Kell blood group
antibodies and CD34+ umbilical cord blood-derived stem cells to explore the cellular and
intracellular mechanisms of erythroid progenitor cell suppression.
The hypothesis is that anti-Kell blood group antibodies directly alter crucial intracellular
signaling cascades in erythropoiesis. This study also explored whether co-ligation of Kell
glycoprotein caused by a bivalent anti-Kell antibody was necessary for growth suppression. As
well, this study evaluated whether apoptosis events were involved in the growth suppression of
erythroid progenitor cells caused by anti-Kell antibodies. Furthering our understanding of the
underlying mechanism of anti-K HDFN will contribute to the development of new therapies.

21
Chapter 2
Retrospective Review

22
2.1 Predictive fetal blood group genotyping
To evaluate the significance of HDFN due to anti-K in the clinical setting, a retrospective review
was performed of the laboratory fetal blood group genotyping tests over a 10-year period. The
goal of this analysis was to determine the prevalence of anti-K HDFN and evaluate any patterns
in fetal blood group genotyping results.
A retrospective review was performed of the laboratory information system for all fetal blood
group genetic tests performed from January 1997 to December 2006 at Mount Sinai Hospital,
Toronto, Canada. The laboratory information system review was performed in accordance with
Mount Sinai Hospital ethics review board approval. Information on antigen(s) tested and antigen
result was collated for each pregnancy.
2.1.1 Laboratory review of fetal blood group genotyping tests
Between January 1997 and December 2006, a total of 220 women (243 pregnancies) submitted
samples for fetal blood group genotyping and comprised the study group. Requests for fetal
blood group genotyping were submitted for a total of 13 different antigens. RHD, KEL1, and
RHE comprised the bulk of the requests (43.3, 21.8, and 12.7%, respectively) (Figure 3). There
were 16 antigen-positive results and 44 antigen-negative results for KEL1, which significantly
differs from a random distribution (Chi-square test, p = 0.0001).

23
Figure 3. Distribution of antigens for which fetal blood group was tested.
Alleles of blood group antigens were detected through predictive blood group genotyping:
RHCE∗C/ RHCE∗c allele (Rh C/c antigen), RHD (Rh D antigen), MNS1/MNS2 (M/N),
MNS3/MNS4 (S/s), RHCE∗E/RHCE∗e (Rh E/e), KEL1/KEL2 (K/k), KEL3/KEL4 (Kpa/b),
FYA/FYB (Fya/b), and JKA/JKB (Jka/b).
2.2 Clinical management of HDFN
To evaluate the clinical impact of HDFN on health care resources, the overall health care
resource costs to monitor fetuses at risk for HDFN was determined from a retrospective review
of the mean number of procedures and visits of mothers with antigen-positive versus antigen-
negative tested fetuses in two prenatal care facilities in Canada. In addition, we compare these
costs to an estimate of the costs to continually monitor alloimmunized women in the absence of
fetal blood group genotyping.

24
A retrospective review was performed at three tertiary care institutions of the clinical and
laboratory records of pregnant women at risk for HDFN with a fetal blood group genotype
performed on amniotic fluid-derived DNA at any time during the pregnancy. Only those
pregnancies with complete obstetrical histories and birth outcome were included in the analysis.
The review was performed in accordance with ethics review board approval at all medical sites.
Laboratory information was collated for each pregnancy and included: blood bank tests including
blood group and antibody screens or investigations, antibody titre, the fetal blood group
genotype, and amniotic fluid bilirubin analysis. The number of clinic visits, ultrasounds
including anemia Dopplers, and amniocenteses were collected for each pregnancy.
The cost to perform laboratory analysis (ABO/Rh and antibody screen, antibody identification
and titre, and ∆OD450 on amniotic fluid) and clinic visits (physical assessment, ultrasound,
Doppler, and amniocentesis) was calculated based on an estimate of labour, equipment, and test
costs. Provincial sources were consulted: Ontario Health Insurance (OHIP) Schedule for
Physician Services, OHIP Schedule for Laboratory Services, and Medical Services Insurance,
Nova Scotia. Costs are expressed in Canadian currency in 2008. The cost of the molecular
blood group genotyping was obtained from Mount Sinai Hospital, Toronto, Ontario, Canada,
where a fetal blood group genotyping program has been in place for ten years. To obtain an
estimate of the total costs by women whose fetuses were tested to be antigen-positive or
negative, the mean number of visits and procedures acquired from the retrospective review was
multiplied by the estimated costs of the resource and totaled to give an overall cost per
pregnancy. An estimate of the resources required to monitor alloimmunized women with a fetus
of unknown antigen status was acquired from clinical experience and published sources.
2.2.1 Retrospective review of health care resource utilization
Information on the clinical management of 54 women was collected and analyzed. Fetal blood
group genotyping was performed early in the pregnancy to identify antigen-positive and antigen-
negative fetuses. A total of eight different blood group antigens were tested for (RHD, RHCE*C,
RHCE*c, RHCE*E, KEL1, JKA/JKB, FYA/FYB), with RHD and KEL1 accounting for 65% of
the tests. There were 32 positive results and 22 negative results. The number of clinic visits and
the procedures performed during visits were compared between mothers with antigen-positive

25
and antigen-negative fetuses (Figure 4). Antigen-positive cases had a significantly greater
number of clinic visits, ultrasounds, amniocenteses, and anemia Dopplers than antigen-negative
cases (unpaired Student’s t-test, all p < 0.0001 except Doppler, p = 0.002). There were three
KEL1-positive cases that had a trend of requiring more resources than other antigen-positive
fetuses based on the number of clinic visits, ultrasounds, and amniocenteses. Due to the low
number of KEL1-positive cases in our study, statistical significance was not evaluated as the
analysis would be unreliable.
A clinic visit would usually include a physical assessment and the collection of maternal blood
followed by laboratory tests to screen for antibodies and determine the titre. An amniocentesis is
ultrasound guided and is performed by the obstetrician with the aid of a nurse and frequently an
ultrasound technician. Chromosome analysis (karyotyping) would be performed usually at the
time of the first procedure. The sample would then be analysed for the amniotic fluid bilirubin
level. Simultaneously, amniotic fluid could be sent for molecular blood group genotyping.
Published sources on best clinical practice (Moise 2005; Moise 2008) and clinical experience
suggest that in a first affected pregnancy where a significant red cell antigen is detected, maternal
titers are repeated every month until approximately 24 weeks, where titers are repeated every 2
weeks thereafter. Non-invasive monitoring methods such as ultrasounds and Doppler
ultrasounds can be performed during these clinic visits to detect signs of fetal anemia. An
amniocentesis would be performed if a risk of anemia is suspected. Thus, to monitor a woman
whose fetus’ antigen status is unknown and who is at risk for HDFN without performing fetal
blood group genotyping would require over the course of the pregnancy approximately 9 clinic
visits, 9 ultrasounds, and 5 Doppler ultrasounds. The proportion of pregnancies that would
require an amniocentesis was estimated from the ratio of antigen-positive fetuses with moderate
or severe disease to all pregnancies (0.30). Thus, about 30% of pregnancies would be
characterized as moderate to high risk and would require a similar number of amniocenteses as
confirmed antigen-positive pregnancies (4.7). Therefore, the estimated health care costs of
monitoring a pregnancy of unknown fetal antigen status is $1644.54 (Table 2).

26
For our cohort, the average cost incurred for a woman with an antigen-positive fetus ($2666.42)
is more than 2.5 fold greater than a woman with an antigen-negative fetus ($987.91) (Table 2).
The estimated overall clinic/laboratory cost savings is $1678.51, representing a 63% cost
reduction per antigen-negative fetus. A fetus whose antigen status is known to be negative also
results in a cost reduction when compared to a fetus whose antigen status is unknown, who
would be continually monitored (40% cost reduction).
Figure 4. Comparison of the mean number of clinic visits or procedures per woman with
K-positive, antigen-positive, or antigen-negative fetus.
Women with antigen-negative fetuses had significantly fewer clinic visits, ultrasounds including
anemia Dopplers, amniocenteses, and blood bank tests than those with antigen-positive fetuses.

27
Mean number (per patient)
Mean total cost (per patient)
Cost
(2008 CAD) Ag (+) Ag (-) Ag (+) Ag (-) Ag status unknown
Doppler ultrasonography
$44.201 5.0 0.2 $221.00 $8.84 $221.00
Complete ultrasound
$81.602 9.1 2.5 $742.56 $204.00 $734.00
Clinic visit $60.23 14.3 4.8 $861.29 $289.10 $542.07
Includes: Prenatal assessment $29.202
Maternal blood sample antibody identification
$23.273
Maternal blood sample antibody titre*
$7.763
Amniocentesis $104.59 4.7 1.3 $491.57 $135.97 $147.47
Includes: Amniocentesis
$102.002
Amniotic fluid bilirubin
$2.593
Molecular genotyping by laboratory (per blood group)
$3504 1 1 $350 $350 $0
TOTAL $2666.42 $987.91 $1644.54
Table 2. Summary of cost analysis for fetal blood group genotyping.
* Performed if antibody identification yields a positive result. 1
Medical Services Insurance, Nova Scotia (2007). 2 OHIP Schedule of Benefits for Physician Services. April 1, 2007. 3 OHIP Schedule for Laboratory Services. April 1, 1999. 1 LMS unit = $0.517. 4
Mount Sinai Hospital, Toronto, Ontario, Canada.

28
Chapter 3
Materials and Methods

29
3.1 In vitro suppression of erythroid progenitor cells
To study the pathophysiology of HDFN due to anti-Kell glycoprotein antibodies, an in vitro
liquid cell culture system was established using umbilical cord blood-derived CD34+ stem cells
as a source of erythroid progenitor cells and commercially available Kell glycoprotein
antibodies. The developed liquid cell culture model would be used to investigate the
intracellular mechanism of erythroid progenitor suppression due to anti-Kell glycoprotein.
3.1.1 Preparation of CD34+ cells
Cryopreserved human umbilical cord blood-derived CD34+ cells obtained from normal
deliveries were purchased from StemCell Technologies (Vancouver, British Columbia). Cells
were thawed in a 37°C water bath. The thawed cell suspension was aseptically transferred to a
50 ml conical tube (Becton Dickinson Labware, Franklin Lake, NJ) containing 250 µl of 1.0
mg/ml Deoxyribonuclease I (StemCell Technologies, Vancouver, British Columbia) to prevent
cell clumping. The tube was filled to 30 ml with room temperature serum-free Iscove’s
Modified Dulbecco’s Medium (IMDM). The cell suspension was centrifuged at 300 x g at room
temperature for 10 minutes. The supernatant was carefully removed and the cell pellet gently
resuspended and transferred to two 1.5 ml microtubes (AdvanTech Research Products). Cells
were washed two more times in 1 ml of serum-free IMDM before addition to culture media.
3.1.2 Preparation of antibodies
Commercially available antibodies and antisera contained sodium azide and were dialyzed to
remove the toxic effect of this agent on progenitor cell growth. Mouse monoclonal anti-Kell
glycoprotein (BRIC 203, Abcam, Cambridge, MA) was diluted in 6% bovine serum albumin
(Immunocor, Norcross, GA) to a final antibody concentration of 25 µg/ml. The dialysis was
performed using a 6000 – 8000 MWCO dialysis membrane (Spectrum Laboratories Inc., Rancho
Dominguez, CA). The dialysis was carried out at 4°C overnight in phosphate buffered saline
(PBS). The dialysate volume was 100X the sample volume and was changed 3 times. Upon
dialysis, the antibody solution was filtered through a 0.2 µm, 25 mm syringe filter (Fisherbrand)
for sterilization.

30
3.1.3 Liquid cell culture system
CD34+ cell cultures were set up in 24-well culture plates (Nunc, Roskilde, Denmark) at a density
of 1.0 x 105 cells/ml in serum-free IMDM supplemented with BIT 9500 serum substitute (1%
bovine serum albumin, 10 µg/ml recombinant human insulin, and 200 µg/ml human transferrin)
(StemCell Technologies, Vancouver, British Columbia), 50 µM 2-mercaptoethanol (Sigma,
Missouri, U.S.A.), 2 mM L-glutamine (Sigma, Missouri, U.S.A.), and 100 U/ml penicillin and
100 µg/ml streptomycin (StemCell Technologies, Vancouver, British Columbia). Cultures were
initially stimulated with erythropoietin (Epo, 2 U/ml) (Cell Sciences, Massachusetts, U.S.A.),
stem cell factor (SCF, 50 ng/ml) (PeproTech, New Jersey, U.S.A.), and interleukin (IL)-3 (100
ng/ml) (PeproTech, New Jersey, U.S.A.). The cells were incubated in a humidified chamber at
37°C containing 5% CO2. The CD34+ cells that were cultured in the presence of the
abovementioned cytokines using this protocol are referred to as erythroid progenitors. On day 3
after initial culture (termed “day 0”), cells were washed twice by centrifuging at 300 x g for 10
minutes with serum-free IMDM to remove the cytokines. Dialyzed and sterilized BRIC 203,
anti-Kpb (polyclonal antisera, Dominion Biologicals Limited, Nova Scotia), an isotype or anti-D
negative control and Epo (2 U/ml) were added to the cultures at a cell density of 1.0 x 105
cells/ml. Cell count and viability, as a measure of growth, was determined on days 1, 2, 3, 4, and
5 after antibody addition. The viable cell count was determined manually with a Neubauer
hemacytometer (Hausser Scientific, Horsham, PA) and an inverted microscope (Nikon TMS).
Using cell suspensions diluted 1:1 in trypan blue (Gibco, U.S.A.) to exclude non-viable cells.
The cells in each 1 mm2 corner of the chamber were counted and the total cell count per mm2
was calculated as an average.
3.1.4 Immunophenotype analysis
The antigen profile of cells cultured for 3-6 days was analyzed by flow cytometry. Cells were
resuspended in stain buffer (Becton Dickinson, Franklin Lake, NJ) and incubated with FITC-
conjugated anti-CD34 (Caltag Laboratories, California), anti-Kell glycoprotein, anti-glycophorin
C, anti-glycophorin A (Abcam, Cambridge, MA), or mouse IgG1 negative control (AbD Serotec,
U.S.A.). FITC-conjugated goat anti-mouse IgG (Jackson Laboratories, U.S.A.) was used to label
non-fluorescein-conjugated antibodies. Non-viable cells were excluded by propidium iodide (PI)
staining (Becton Dickinson, Franklin Lake, NJ). Samples were analyzed on a FACSCalibur flow

31
cytometer (Becton Dickinson, Franklin Lake, NJ). Ten thousand events were acquired for each
analysis and data was analyzed using CellQuest Pro software after gating on viable cells.
3.2 Effect of anti-Kell glycoprotein Fab on erythroid progenitor proliferation
To compare the effects of whole IgG anti-Kell glycoprotein and anti-Kell glycoprotein Fab on
erythroid progenitor proliferation, anti-Kell glycoprotein Fab was prepared from commercially
available whole IgG anti-Kell glycoprotein by papain digestion. Because of the suppressive
effect of anti-glycophorin C (GYPC) on BFU-E and CFU-E (Denomme et al. 2006), anti-GYPC
Fab was similarly prepared from whole IgG anti-GYPC for preliminary tests to develop the
protocol. A goat antibody to the heavy and light chain of murine IgG (~(H+L)) was also tested
for its effect on cell proliferation. The ~(H+L) was added to anti-Kell glycoprotein Fab and anti-
GYPC Fab in cell culture to reconstitute the bivalency of the Fab fragments.
3.2.1 Preparation of anti-Kell glycoprotein Fab and anti-GYPC Fab
Anti-Kell glycoprotein Fab was prepared from whole IgG anti-Kell glycoprotein (BRIC 203,
Abcam, Cambridge, MA) and anti-GYPC was prepared from whole IgG anti-GYPC (Ret40f,
Abcam, Cambridge, MA) with the ImmunoPure Fab Preparation Kit (Pierce Biotechnology,
Rockford, IL). IgG anti-Kell glycoprotein (300 µg) was added to 9,700 µg of pooled purified
IgG in the form of intravenous immune globulin (IVIG) (Gamunex, Research Triangle Park, NC)
and was incubated with papain immobilized on an agarose support overnight in a shaking
incubator at 37°C. IgG anti-GYPC (625 µl) was added to 19,375 µg of IVIG and incubated
similarly. IVIG alone (10,000 µg) was also digested and used as a negative control in cell
culture. The digest was separated from the immobilized papain using a resin separator. Protein
A columns, which bind the Fc fragments and undigested IgG, were used to purify the digest.
The flow-through, which contains the Fab fragments, was collected and dialyzed to remove
residual chemicals from the papain digestion. The dialysis was performed using a 10,000
MWCO dialysis cassette (Pierce Biotechnology, Rockford, IL). The dialysis was carried out
overnight in PBS at 4°C, which was changed 3 times during that period. Upon dialysis, the Fab
product was filtered through a 0.2 µm, 25 mm syringe filter (Fisherbrand) for sterilization.

32
3.2.2 Characterization of anti-Kell glycoprotein Fab and anti-GYPC Fab product
The dialyzed anti-Kell glycoprotein Fab and anti-GYPC Fab were analyzed by non-reducing
SDS-PAGE for purity. The concentration of the samples were estimated with a Bicinchoninic
acid (BCA) Protein Assay Kit (Pierce Biotechnology, Rockford, IL) and spectrophotometry at
562 nm absorbance. The anti-Kell glycoprotein samples were concentrated to 29 µg/ml of anti-
Kell glycoprotein Fab using a sterilized 10,000 MWCO Nanosep centrifugal device (Pall Life
Sciences, Ann Arbor, MI). The anti-GYPC Fab samples were similarly concentrated 48X. An
indirect agglutination test was used to evaluate the ability of Fab to agglutinate RBCs and the
ability of ~(H+L) added to Fab fragments to reconstitute bivalency. A 5% solution of RBCs was
mixed with 200 µl of Fab product. The mixture was spun at 700 – 800 x g and the degree of
agglutination was scored on a scale of 0 – 4, where 4 represented complete agglutination
(Appendix A) (Petz et al. 1983). The RBCs were washed four times in PBS and goat anti-mouse
~(H+L) or goat anti-mouse IgG to the Fcγ portion of immunoglobulins, (~ Fcγ) (Jackson
Laboratories, U.S.A.), was added to the RBCs and antibody solution and the degree of
agglutination was scored after centrifugation. The degree of agglutination of the Fab product
was compared to the results of the indirect agglutination test with whole IgG anti-Kell
glycoprotein, anti-GYPC, and an isotype control. Goat anti-mouse IgG with Fcγ specificity
(Jackson Laboratories, U.S.A.) was used for whole antibody indirect agglutination tests.
3.2.3 Effect of anti-Kell glycoprotein Fab on erythroid progenitor liquid cultures
Anti-Kell glycoprotein Fab was added to 1 ml erythroid progenitor cultures to a final anti-Kell
glycoprotein Fab concentration of 7.3 µg/ml. Anti-GYPC Fab was added to 1 ml erythroid
progenitor cultures at a dilution of 1:4. Goat anti-mouse IgG ~(H+L) (Jackson Laboratories,
U.S.A.) was added to cell cultures to a final concentration of 7.5 µg/ml. Fab fragments were
added to the cell suspension first and ~(H+L) was added next. IgG isotype control Fab alone and
IgG Fab plus ~(H+L) were used as negative controls.

33
3.3 Role of apoptosis in the growth inhibitory effect of anti-Kell glycoprotein
To determine whether apoptosis is involved in the mechanism of erythroid progenitor growth
suppression of anti-Kell glycoprotein, markers of apoptosis such as loss of phosphatidylserine
asymmetry and mitochondrial membrane depolarization was evaluated in erythroid cell culture.
To investigate the role of caspases, a general caspase inhibitor was added to anti-Kell
glycoprotein induced cell cultures. As well, a caspase activation assay was performed.
3.3.1 Phosphatidylserine asymmetry in anti-Kell glycoprotein induced erythroid cells
To investigate whether the growth suppression caused by anti-Kell glycoprotein is associated
with phosphatidylserine (PS) externalization on the plasma membrane, Annexin V-FITC and the
vital dye, propidium iodide (PI) (BD Biosciences, Mississauga, Ontario), were used to examine
cultured cells by flow cytometry. Cells on day 3 after antibody inducement were washed twice
with cold PBS and then resuspended in 100 µl of Annexin V binding buffer (BD Biosciences,
Mississauga, Ontario). Then, cells were incubated with 5 µl of Annexin V-FITC and 5 µl of PI
for 15 minutes at room temperature in the dark. Additional binding buffer was added to each
tube and cells were analyzed with a BD FACSCalibur flow cytometer and CellQuest Pro
software.
3.3.2 Effect of a general caspase inhibitor on the growth inhibitory effect of anti-Kell
glycoprotein
A general caspase inhibitor, Z-Val-Ala-Asp-CH2F-fluoromethyl ketone (Z-VAD-FMK) (R&D
systems, U.S.A.) (Zaks et al. 1999), was reconstituted in 10% dimethyl sulfoxide (DMSO) and
added to cell cultures to a final concentration of 100 µM Z-VAD-FMK/0.05% DMSO. A
solution of 10% DMSO was added to cell cultures to a final concentration of 0.05% as a solvent
control. Z-VAD-FMK or solvent control was added to cell cultures concurrently with anti-Kell
glycoprotein on day 3 of cell culture. Etoposide (Sigma, Missouri, U.S.A.), an antitumor agent
that blocks cell cycle progression (Sinkule 1984), was added at a final concentration of 200 µM
to induce apoptosis and served as a positive control to ensure Z-VAD-FMK was able to rescue
classical apoptosis by inhibiting caspase activation.

34
3.3.3 Caspase activation in anti-Kell glycoprotein induced erythroid cell cultures
ApoStat (fluorescein-conjugated V-D-FMK, R&D Systems), a cell-permeable, FITC-
conjugated, pan-caspase inhibitor that binds to activated caspases, was used to detect
intracellular caspase activation in cultured cells. Cells were collected on day 3 after antibody
inducement and washed once with PBS. Healthy cells and cells treated with etoposide were used
as negative and positive staining controls, respectively. Cells were resuspended in 1 ml of PBS
and 10 µl of 50 µg/ml ApoStat was added to each condition. Cells were incubated with ApoStat
in the dark for 30 minutes at 37°C. Cells were washed once in PBS to remove unbound reagent
and then resuspended in PBS. Flow cytometry was performed using a BD FACSCalibur flow
cytometer and CellQuest Pro analysis software.
3.3.4 Mitochondrial membrane potential in anti-Kell glycoprotein treated cells
To investigate whether the growth suppression induced by anti-Kell glycoprotein causes
membrane depolarization involved in apoptosis, JC-1 (5,5’, 6,6’-tetrachloro-1, 1’, 3, 3’-
tetraethylbenzimidazol-carbocyanine iodide) (Molecular Probes, Eugene, OR) labeling was
performed (Mancini et al. 1997). JC-1 was added to cell suspensions to a final concentration of
2 µM. The mitochondrial membrane potential disrupter, carbonyl cyanide 3-
chlorophenylhydrazone (CCCP), was added simultaneously with JC-1 to a final concentration of
50 µM as a positive control. Cells were analyzed on a BD FACSCalibur flow cytometer with
488 nm excitation using emission filters appropriate for Alexa Fluor 488 dye and R-
phycoerythrin.
3.4 The ability of erythropoietin to rescue the growth inhibitory effect of anti-Kell
glycoprotein
Serial additions of increased amounts of Epo were added to cultures induced with anti-Kell
glycoprotein to examine Epo’s ability to rescue the growth suppression. Five times the amount
of Epo (10 U/ml) that was used routinely in our culture system was added on days 0, 1, and 2 of
the antibody inducement period. Viable cell count was determined by trypan blue exclusion as
described in 3.1.3 on days 2, 3, and 4 after antibody addition.

35
3.5 Statistical analysis
For the retrospective review of fetal blood group genotyping tests, chi-square tests using
Microsoft Excel software were performed to determine whether the distribution of positive and
negative results were significantly different. For the review of health care resource utilization,
unpaired Student’s t-tests using Microsoft Excel software were performed to determine whether
the difference in the number of clinic visits and procedures by women whose fetuses were tested
to be antigen-positive or negative was significant. P values less than 0.05 were considered to
indicate statistical significance.
In each experiment, the data for the test sample was paired with the negative control. For cell
proliferation studies, percent growth suppression was calculated by subtracting the viable cell
count of the test sample from the control group and dividing that value by the cell count of the
control group. To determine if the percent growth suppression of two test samples were
statistically different, the p value was determined by a two-sided Student’s t-test for unpaired
data using Microsoft Excel software. For flow cytometry data, the quadrant marker or the
positive staining area was determined by the negative and positive controls. The percent of
events in the quadrant of interest was tabulated for the test sample and the control sample. To
determine if the percent of events were statistically different between two test samples, the p
value was determined by a two-sided Student’s t-test for paired data using Microsoft Excel
software. P values less than 0.05 were considered to indicate statistical significance.

36
Chapter 4
Results

37
4.1 Erythroid progenitor proliferation in liquid culture system
An in vitro culture system was developed in which to evaluate the effect of antibodies on
erythroid progenitor proliferation. When a one-stage protocol was used, where cells were
cultured in the presence of IL-3, SCF, and Epo throughout, antibody-induced cell growth
suppression was not observed (data not shown). Thus, CD34+ cells were cultured in two stages:
in stage 1, cryopreserved CD34+ cells were cultured in the presence of IL-3, SCF, and Epo for
three days in which minimal proliferation was observed (Figure 5). By the third day, cells
approached an exponential proliferation stage (upper data point on Day 0 in Figure 5) and the
cells were washed, reconstituted in Epo, adjusted to 1 x 105 cells/ml, and then induced with
antibodies in stage 2 of culture. Generally, by day 4 of stage 2 of culture, the cells reached a
growth plateau and cell viability rapidly declined (viability data not shown).
Figure 5. Representative cell proliferation in two-stage culture protocol in the absence of
suppressive antibody.
To evaluate the suppressive effect of antibodies on cell proliferation, antibody addition occurs on
day 3 of initial culture (termed “Day 0” throughout this study) and cells are evaluated up to day
4.

38
4.2 Immunophenotype of erythroid progenitors in liquid culture
CD34+ cells seeded in liquid culture were analyzed for expression of cell surface markers to
determine progression through erythropoiesis. Manufacturer’s purity analysis of cryopreserved
cells by flow cytometry guaranteed above 90% expression of CD34. The cell surface marker
expression profile reveals that within 3 days of initial culture (i.e. day 0, the day on which
antibody is added), 67.5% of erythroid cells still express CD34 and only 1.4% express
glycophorin A, the accepted marker for late erythroid progenitors (Gahmberg et al. 1978;
Robinson et al. 1981) (Table 3). After 6 days of initial culture (day 3 after antibody addition),
the majority of the cells (87.1%) express glycophorin A and only 2.8% of analyzed cells express
CD34. After 3 days of initial culture, the majority of the cells express glycophorin C (83.4%).
Kell glycoprotein expression occurs after glycophorin C and by day 3, is expressed on 82.5% of
cells. Incubating CD34+ cells with anti-Kell glycoprotein on day 0 of initial culture did not alter
the immunophenotype of the cells compared to untreated cells (data not shown).
Day*
CD34
Glycophorin A
Glycophorin C
Kell glycoprotein
Day 0 67.5% 1.4% 83.4% 3.7%
Day 1
41.3%
15.6%
85.1%
44.2%
Day 3
2.8%
87.1%
98.4%
82.5%
Table 3. Immunophenotype of CD34+ cells seeded in liquid culture.
Percent of cells positive for cell surface marker after initial seeding from cryopreserved CD34+
cells as analyzed by flow cytometry (see Appendix B for flow cytometry data). * refers to the
day of culture when antibody would be added. Thus, on day 0, cell expansion in the presence of
cytokines had accumulated enough cells for flow cytometric analysis.

39
4.3 Effect of antibodies to Kell glycoprotein and blood group specific antibodies on
erythroid progenitor cells in liquid culture
The growth inhibitory effect of anti-Kell glycoprotein and anti-Kpb in liquid culture was
determined by viable cell count and trypan blue exclusion test (Figure 6). Growth suppression of
anti-Kell glycoprotein and anti-Kpb treated cells were compared to cells treated with an
isotype/negative control. Anti-Kell glycoprotein caused 29-49% growth suppression 1-4 days
after addition of antibodies to the erythroid progenitor cultures. Anti-Kpb caused 27-68% growth
suppression 2-4 days after addition to cultures. There was no significant difference between the
viability of the cell cultures. Isotype control cultures had cell viabilities between 88-100%.
Anti-Kell glycoprotein-induced cultures had cell viabilities between 84-92%. Anti-Kpb-treated
cultures had cell viabilities between 71-93%.
Figure 6. Percent growth suppression of treated erythroid progenitors.
Percent growth suppression normalized to the isotype control (not shown). Viable cell count
determined by trypan blue exclusion test. Results expressed as mean percent suppression ±
standard error of the mean (SEM) (Anti-Kell glycoprotein, n = 4; Anti-Kpb, n = 2).

40
4.4 Characterization of anti-Kell glycoprotein Fab product
The anti-Kell glycoprotein Fab product after papain digestion and Protein A column purification
was analyzed by non-reducing SDS-PAGE for purity. SDS-PAGE analysis of Fab fragments
showed one main band at 50 kDa (Appendix C). A faint band can be detected at 30 kDa, but the
absence of a band at 150 kDa indicated the absence of intact IgG. The BCA protein assay
determined the concentration of the Fab sample to be 325 µg/ml. Since anti-Kell glycoprotein
consisted of 3% of the initial IgG concentration, the estimated concentration of anti-Kell
glycoprotein Fab was 9.8 µg/ml. The volume of the Fab product was reduced by 3X with a
centrifugal device to concentrate the sample to 29 µg/ml. The indirect agglutination test showed
that the Fab product alone did not agglutinate RBCs (degree of agglutination = 0). When the
cells were washed and ~(H+L) was added to the RBC/Fab solution, agglutination was observed
(degree of agglutination = 2). There was no agglutination observed when an antibody to the Fcγ
portion of immunoglobulins was used for the indirect agglutination test. Whole IgG anti-Kell
glycoprotein at a concentration of 25 µg/ml agglutinated RBCs when an antibody to the Fcγ
portion of immunoglobulins was added (degree of agglutination = 4). There was no
agglutination when an isotype control was added to RBCs, nor when ~(H+L) or ~ Fcγ was
added. Anti-GYPC Fab product was similarly characterized (Appendix D, E).

41
4.5 Effect of anti-Kell glycoprotein Fab on erythroid progenitor proliferation
The proliferation of erythroid progenitors was examined in the presence of anti-Kell glycoprotein
Fab fragments and ~(H+L). Anti-Kell glycoprotein Fab did not significantly inhibit progenitor
proliferation. Anti-Kell glycoprotein Fab with anti-(H+L) inhibited the proliferation of erythroid
progenitors by 20-23% relative to the negative control Fab alone on days 2, 3 and 4 after
antibody inducement (Figure 7). Anti-(H+L) with negative control Fab did not cause
suppression. The degree of suppression caused by anti-Kell glycoprotein Fab with anti-(H+L)
was significant (p < 0.05). Whole IgG anti-Kell glycoprotein inhibited proliferation by 28-45%.
Anti-GYPC Fab also did not significantly inhibit progenitor proliferation, but erythroid
progenitor growth suppression was reconstituted when ~(H+L) was added (Appendix F).

42
Figure 7. Suppression of progenitor proliferation by anti-Kell glycoprotein Fab and anti-
(heavy and light chain).
Percent growth suppression was normalized to negative control Fab alone (not shown). Anti-
Kell glycoprotein Fab fragments did not cause significant suppression of erythroid progenitor
proliferation. * Anti-Kell glycoprotein Fab and anti-(H+L) caused significant suppression
relative to anti-Kell glycoprotein Fab alone (p < 0.05). Anti-(H+L) with negative control Fab did
not cause suppression. Results are expressed as mean percent suppression (±SEM) with three
vials of CD34+ cells (n = 3).

43
4.6 Phosphatidylserine asymmetry in anti-Kell glycoprotein induced erythroid progenitors
To investigate whether the growth suppression caused by anti-Kell glycoprotein is through an
apoptotic mechanism, phosphatidylserine externalization on the plasma membrane was
evaluated. The high affinity acidic phospholipid binding protein, Annexin V-FITC, and the vital
dye propidium iodide (PI) were used to examine erythroid progenitors by flow cytometry on day
+3 after antibody addition. Anti-Kell glycoprotein treated samples do not have increased binding
of Annexin V-FITC compared to the negative control (p > 0.05) (Figure 8). In addition, anti-
Kell glycoprotein did not have increased PI staining compared to the negative control (upper left
and upper right quadrants).
A. Isotype control B. Anti-Kell glycoprotein
Figure 8. Annexin V-FITC and PI labeling of erythroid progenitors treated with anti-Kell
glycoprotein.
Representative flow cytometry analysis of cells cultured for 3 days after antibody addition and
labeled with Annexin V-FITC and PI. A. Cells treated with isotype control. B. Cells treated
with anti-Kell glycoprotein. There was no significant difference (n = 6, p = 0.31) between the
samples in the number of events that were Annexin V-FITC positive (upper right and lower right
quadrants) or PI positive (upper left and upper right quadrants).
13.1%
22.5% 18.9%
11.1%

44
4.7 Effect of a general caspase inhibitor on the growth inhibitory effect of anti-Kell
glycoprotein
The proliferation of erythroid progenitors in the presence of anti-Kell glycoprotein and the
general caspase inhibitor, Z-VAD-FMK, was examined. Anti-Kell glycoprotein alone inhibited
proliferation by 32-41% compared to cells cultured with an isotype control. Anti-Kell
glycoprotein with Z-VAD inhibited the growth of erythroid progenitors to a similar degree (22-
57%) relative to the negative control on days 2, 3 and 4 after antibody inducement (Figure 9).
Therefore, Z-VAD did not significantly rescue the growth suppression caused by anti-Kell
glycoprotein. The degree of suppression caused by anti-Kell glycoprotein with Z-VAD diluent
was 20-51%. The diluent control in the presence and absence of anti-Kell glycoprotein
confirmed that DMSO did not have an effect on cell growth.
The proliferation of erythroid progenitors in the presence of etoposide and Z-VAD-FMK was
examined. Z-VAD was able to partially rescue extreme growth suppression caused by etoposide.
By day 3 of inducement, there were no visible viable cells in etoposide treated cultures. In Z-
VAD and etoposide treated cells, growth suppression was only 57% compared to the isotype
control (Figure 10). There was no growth suppression in Z-VAD-only or Z-VAD diluent treated
cells.

45
Figure 9. Suppression of progenitor proliferation by anti-Kell glycoprotein in the presence
of Z-VAD-FMK.
Percent growth suppression was normalized to cells treated with isotype control. Z-VAD-FMK
(100 µM) did not significantly rescue the growth suppression caused by anti-Kell glycoprotein (p
> 0.05). Z-VAD diluent did not cause additional suppression compared to anti-Kell glycoprotein
alone (see Figure 10 for Z-VAD diluent alone data). Results are expressed as mean percent
suppression (±SEM) with three vials of CD34+ cells (n = 3).

46
Figure 10. Suppression of progenitor proliferation by etoposide and partial rescue by Z-
VAD.
Addition of etoposide (200 µM) to erythroid cultures resulted in complete growth suppression by
day +3 after addition. Z-VAD (100 µM) partially rescued growth suppression caused by the
presence of etoposide. Results are expressed as mean percent suppression (±SEM) with two vials
of CD34+ cells.

47
4.8 Caspase activation in anti-Kell glycoprotein induced erythroid cell cultures
To examine caspase activation in anti-Kell glycoprotein induced cultures, ApoStat staining was
examined using flow cytometry. Healthy cells and cells treated with etoposide were used as
negative and positive controls, respectively (Figure 11). The mean fluorescence intensity (MFI)
for etoposide treated cells was 26.9. Healthy cells had a mean fluorescence value of 4.03. Mean
fluorescence intensity values show that anti-Kell glycoprotein treated cells (MFI = 6.3) have
comparable ApoStat staining to the isotype control (MFI = 7.2). This suggests that caspases are
not significantly activated in anti-Kell glycoprotein treated cultures (p = 0.76). Cells treated with
etoposide and Z-VAD had a moderate fluorescence value (MFI = 7.7). In addition, cells treated
with Z-VAD alone had low levels of ApoStat fluorescence (MFI = 3.9).

48
Figure 11. Mean fluorescence intensity of ApoStat of erythroid progenitors treated with
anti-Kell glycoprotein.
ApoStat labeling of cells cultured for 3 days in the presence of antibody or reagent (see
Appendix G for flow cytometry histograms). Anti-Kell glycoprotein treated cells did not have
significantly increased levels of ApoStat staining compared to the isotype control (p = 0.76).
Results are expressed as mean fluorescence intensity (±SEM) with two vials of CD34+ cells.

49
4.9 Mitochondrial membrane potential of anti-Kell glycoprotein treated cells
To investigate whether the growth suppression caused by anti-Kell glycoprotein involved
mitochondrial membrane depolarization occurring in apoptosis, JC-1 labeling was performed on
day 3 after antibody addition and the results analyzed by flow cytometry. JC-1 is a cationic dye
that exhibits transmembrane potential-dependent accumulation in the mitochondria, indicated by
a fluorescence emission shift from green (~525 nm) to red (~ 590 nm). Thus, mitochondrial
membrane depolarization is indicated by a loss of red fluorescence. Anti-Kell glycoprotein
treated samples had a slight but not statistically significantly loss of JC-1 red fluorescence as
compared to the isotype control (p = 0.09) (Figure 12, Table 4).
A. B. C.
Figure 12. JC-1 assay of anti-Kell glycoprotein treated erythroid progenitors
Representative flow cytometry analysis of erythroid progenitors labeled with JC-1. Percent of
events with loss of JC-1 red fluorescence (lower right quadrant) is indicated. A. Cells treated
with isotype control. B. Cells treated with anti-Kell glycoprotein. There was no significant
difference (n = 5, p = 0.09) between the samples in the number of events that were JC-1 red
negative (lower right quadrant). C. Cells treated with the mitochondrial membrane potential
disrupter, CCCP, prior to JC-1 labeling (positive control).
12.0% 13.4% 64.3%

50
Percent of events with loss of JC-1 red fluorescence (lower right quadrant)
Isotype control Anti-Kell glycoprotein Trial 1 11.96 13.41 Trial 2 5.77 22.85 Trial 3 12.50 13.63 Trial 4 26.42 44.99 Trial 5 3.87 8.52 Mean 12.10 20.68 SEM 3.95 6.49
Table 4. Percent of events with loss of JC-1 red fluorescence.
A total of 5 trials were performed to evaluate mitochondrial membrane depolarization. Anti-Kell
glycoprotein treated samples had a slight but not statistically significantly loss of JC-1 red
fluorescence as compared to the negative control (p = 0.09).

51
4.9 Ability of serial additions of erythropoietin to rescue growth suppression caused by
anti-Kell glycoprotein
The suppression of erythroid progenitor cell growth caused by anti-Kell glycoprotein was
examined in the presence of excess erythropoietin added serially during the antibody inducement
period. The presence of excess Epo with either the negative control or anti-Kell glycoprotein
resulted in lower levels of proliferation compared to regular levels of Epo (Figure 13). In
samples with serially added Epo, anti-Kell glycoprotein caused similar growth suppression of
40-46% on days 2 and 3 after antibody inducement. In cultures containing the standard level of
Epo, anti-Kell glycoprotein inhibited growth by 39-55%. By day 4, anti-Kell glycoprotein
sample plus excess Epo inhibited the growth of erythroid progenitors by 43% compared to the
negative control. Anti-Kell glycoprotein samples with regular levels of Epo resulted in 48%
growth suppression on day 4.

52
Figure 13. Proliferation of erythroid progenitors in the presence of serially added excess
erythropoietin and anti-Kell glycoprotein.
Mean viable cell count with mean percent growth suppression. The addition of excess
erythropoietin did not rescue the growth suppression caused by anti-Kell glycoprotein. Erythroid
progenitor cultures with excess erythropoietin had lower levels of proliferation compared to
cultures with regular amounts of erythropoietin. Results are expressed as mean viable cell count
(±SEM) with two separate sources of CD34+ cells.

53
Chapter 5
Discussion

54
5.1 Clinical and laboratory impact of HDFN
The improvements in Rh immunoglobulin administration, prenatal care, non-invasive
monitoring, and intrauterine transfusion have provided effective treatment to even the most
severely affected fetuses and infants by HDFN. Early intervention requires accurate diagnosis of
a fetus at risk for the disease. HDFN continues to be a challenge in the management of fetal
morbidity and mortality and fetal blood group genotyping is an important component of the
appropriate management of fetuses at risk for HDFN. Further invasive procedures for the
purposes of monitoring for HDFN can be limited for the antigen-negative fetus and antigen-
positive fetuses can be offered targeted management. This strategy is particularly important for
HDFN due to anti-K since antibody titers and amniotic fluid bilirubin levels are unreliable
predictors of anemia. In addition, clinical procedures to continually monitor women with fetuses
at risk for HDFN incur health care costs. To evaluate the significance of HDFN due to anti-Kell
and its clinical impact on health care resources, a retrospective review was performed of the
laboratory fetal blood group genotyping tests and clinical procedures necessary to monitor
fetuses at risk for HDFN.
5.1.1 Laboratory review of fetal blood group genotyping tests
The antigen distribution of requests for fetal blood group genotyping over a ten-year period is a
measure of the clinical significance of an antigen in HDFN. Requests for KEL1 genotyping
comprised roughly one-fifth of the total requests, which is second in number only to RHD, which
received two-fifths of requests. This is consistent with reports that maternal anti-K is the second
most common alloantibody after anti-D (Vaughan et al. 1991). Therefore, anti-K HDFN
represents a significant clinical problem that requires further study.
Since fetal blood group genotyping is recommended only when there is maternal
alloimmunization and the father is heterozygous for the antigen or if the father is unavailable,
there should be a 50:50 chance that the fetus is positive for the antigen of interest. However, for
the K antigen, there were significantly greater numbers of negative compared with positive
results. Since antibody titer does not necessarily reflect the risk of anemia (Bowman et al. 1992),
which may occur early in gestation, there may be a less stringent selection process on the part of

55
obstetricians referring cases for KEL1 genotyping. The desire to ensure all K-positive fetuses are
identified may result in referral despite the lack of clinical evidence.
5.1.2 Retrospective review of health care resource utilization
This study evaluated a population that is representative of the distribution of the types of HDFN
cases encountered in major prenatal care centres. The cost differential was based on the
difference between two groups with a fetal blood group genotype: antigen-positive versus
antigen-negative fetuses. Centres that offer specialized care for high-risk pregnancies may vary
in the management of low risk and known antigen-negative pregnancies. Therefore, the costs to
continually monitor a pregnancy at risk for HDFN without performing a fetal blood group
genotype was estimated. The cost differences in our health care resource analysis may be
smaller if low risk pregnancies with an antigen-positive fetus are managed differently or if
fetuses with an unknown antigen status are not monitored closely. Similarly, due to the potential
severity and the non-reliability of antibody titers to predict HDFN due to anti-K, monitoring at
risk fetuses in the presence of maternal anti-K may require increased resources than we have
estimated. Provincial sources and reliable published sources were consulted to evaluate the
impact of a fetal blood group genotyping program on health care resources. However, detailed
resource allocation of staff, consumables, overhead, and capital equipment costs have not been
estimated for the clinic and the laboratory. Consequently, a comprehensive estimate of the actual
resources utilized to provide the health care service is not commonly available.
The benefits of prenatal genetic testing for HDFN include the opportunity to determine an
appropriate management plan for the at-risk pregnancy as well as the reassurance to the couple
by a negative blood group antigen outcome. The relative benefit of the diagnostic information
acquired by amniocentesis must be considered in light of the physical risk posed by obtaining it.
In addition, there may be parental psychological anxiety that accompanies predictive genetic
testing including concern about procedural complications and the test outcome (Tercyak et al.
2001). Women report that after a normal outcome of a prenatal diagnostic test, they worry less
about the expected child and experience the pregnancy as more untroubled (Sjögren et al. 1989).
In a study evaluating the cost utility of amniocentesis for the prenatal diagnosis of chromosomal
disorders, Harris and colleagues measured the desire for reassurance offered by the test by the
decrease in quality of life from not having chromosomal information (Harris et al. 2004). The

56
authors found that the reassurance desired by the women was the primary reason for the cost-
effectiveness of amniocentesis. While these factors are difficult to quantify and take into
account, it is important to not only assess the economic value of prenatal testing, but also to
recognize the emotional benefits to the family. Predictive fetal blood group genotyping involves
a degree of physical and emotional risk as well as economic costs.
It is more costly to monitor all pregnancies for HDFN risk regardless of the fetal blood group
than it is to perform fetal blood group genotyping tests. Approximately half of the pregnancies
being continually monitored for HDFN through titers and non-invasive measures involve fetuses
who are antigen-negative since their fathers are either heterozygous for the blood group antigen
or unavailable. Therefore by determining the fetal antigen through blood group genotyping, a
significant proportion of these pregnancies with elevated titres and a high-risk obstetrical history
could forego the costly management. Invasive procedures have associated risks including
pregnancy loss or transplacental hemorrhage leading to stimulation of maternal antibody levels
and a worsening of fetal anemia (Eisenberg et al. 2002; Alfirevic et al. 2007). As a non-invasive
test, a few European centres now use fetal DNA extracted from maternal plasma to identify the
blood group antigen-positive fetus (including K antigen) (Lo et al. 1998; Finning et al. 2002;
Finning et al. 2007; Li et al. 2008). An accurate predictive diagnostic test for a fetal blood group
targets appropriate management for the antigen-positive fetus and amniocenteses would be
unnecessary in the antigen-negative fetus.
It is cost effective to offer patients molecular testing, but additional benefits include decreased
risks for the mother and fetus and decreased anxiety overall. We conclude that a prenatal
diagnosis programme for blood group genotyping is justifiable and provides patients with
improved more targeted health care. The retrospective reviews performed of the laboratory and
clinical aspects of HDFN have not only confirmed that HDFN continues to be a significant
problem, but that anti-K is a special case in the clinical and laboratory management of HDFN.
The significance of HDFN due to anti-K warrants a better understanding of the pathobiology of
the condition.

57
5.2 In vitro suppression of erythroid progenitor cells
The clinical manifestations of HDFN mediated by anti-K have features that are distinguishable
from the classical form of the disease due to anti-D. Affected fetuses may have lower numbers
of circulating reticulocytes and normoblasts compared to fetuses with anti-D HDFN, with levels
that are inappropriately low for the degree of fetal anemia (Weiner et al. 1996). As well,
antibody titers and amniotic fluid bilirubin levels are not reliable predictors of anemia. These
clinical characteristics suggest that the mechanism by which antibodies to Kell lead to anemia is
through suppression of erythropoiesis (Vaughan et al. 1998). Previous in vitro studies have
reported the suppression of erythroid BFU-E and CFU-E by Kell blood group specific antibodies
and antibodies to the Kell glycoprotein (Vaughan et al. 1998; Shahcheraghi 2005). However,
these studies have used cord blood progenitor cells grown in semi-solid (methylcellulose) media
containing Epo (3U/ml). Although semi-solid medium colony-forming methods are useful in
evaluating the number of progenitor colonies, the immobilization of cells renders it difficult to
perform quantitative biochemical analyses of the effect of antibodies on growth and development
of erythroid cells. In addition, the one-step continuous culture makes it difficult to test the
effects of altering the culture conditions since it is difficult to add or subtract components
to/from culture. These disadvantages can be overcome by liquid suspension cultures of CD34+
progenitor cells. A liquid culture system allows the manipulation of culture conditions and
components during erythroid development. Importantly, a liquid culture system could facilitate
biochemical and molecular analysis such as phosphorylation and cytoskeletal reorganization
studies (Fibach et al. 1989). This study developed a liquid culture system model in which to
show suppression of cord blood erythroid progenitor cell growth by antibodies to Kell
glycoprotein. This work established the experimental conditions necessary to investigate the
mechanism of anti-K growth suppression.
5.2.1 Progression through erythropoiesis in liquid cell culture
The cell surface marker expression profile of CD34+ cells seeded in liquid culture revealed that
by Day 3, cells were predominantly in the latter stages of erythropoiesis (Table 3). Glycophorin
A is a marker of more mature erythroid cells, because it first appears at the basophilic
normoblast stage of development after which its expression increases throughout the rest of
erythroid differentiation (Gahmberg et al. 1978; Robinson et al. 1981). CD34 is a marker of

58
early progenitor cells and is not expressed after the BFU-E stage. While glycophorin C was
expressed early in the culture system, Kell glycoprotein expression reached appreciable levels a
few days after initial culture. These results are consistent with other time course analyses of cell
surface antigen expression during erythropoiesis (Bony et al. 1999; Southcott et al. 1999; Daniels
et al. 2000). Immunophenotype analysis showed that cord blood-derived CD34+ cells seeded in
our liquid culture system successfully underwent erythropoiesis. The cell surface antigen profile
of erythroid progenitors differentiating in the presence of anti-Kell glycoprotein was not altered.
This suggests that anti-Kell glycoprotein treated cells do not differ from untreated cells in their
differentiation during erythropoiesis. Thus, the inhibitory effects of antibodies to Kell
glycoprotein are not due to altering the normal course of erythropoiesis.
5.2.2 Suppression by antibodies to Kell glycoprotein and blood group specific antibodies
Addition of anti-Kell glycoprotein and anti-Kpb, a high incidence Kell antigen, induces growth
suppression in the liquid culture model. The reduction in cell number in the presence of
antibodies to Kell suggest that these antibodies cause anemia in HDFN through suppressing the
proliferation of erythroid progenitors rather than through inhibiting differentiation. The similar
viabilities of the anti-Kell glycoprotein treated and control cultures provide evidence that anti-
Kell glycoprotein does not reduce viable cell numbers by increasing the number of non-viable
cells since anti-Kell glycoprotein treated cultures have lower total cell numbers compared to
controls. The degree of growth suppression is comparable to that observed previously in semi-
solid methylcellulose cultures (20-50%) (Shahcheraghi 2005). Antibodies targeting Kell
glycoprotein were used for this study because these murine antibodies are monoclonal and target
a defined epitope. Therefore, using anti-Kell glycoprotein allowed for the development of a
standardized cell culture model system. The similar growth suppression observed with cell
cultures treated with anti-Kpb from human sera confirms the results obtained with the murine
anti-Kell glycoprotein. This erythroid liquid culture model was shown to be a suitable system in
which to investigate the mechanism of antibody suppression.

59
5.3 Requirement for antigen co-ligation for growth inhibitory effect
The Kell glycoprotein is known to be associated with the underlying cell cytoskeleton. While
the exact nature of its attachment to cytoskeletal components is unknown, it is conceivable that
alterations to the Kell glycoprotein may affect cytoskeletal organization or signaling
components. The possibility that alterations to the organization of Kell glycoprotein may have
implications for the underlying cytoskeleton is supported by the observation that co-ligation by
bivalent antibody is required for growth suppression. Glycophorin C is a sialoglycoprotein that,
like Kell glycoprotein, is expressed early in erythroid development. The cytoplasmic domain of
glycophorin C is known to associate with the erythrocyte membrane skeleton via Protein 4.1 and
p55 (Marfatia et al. 1994). In vitro erythroid colony-forming studies using anti-glycophorin C
have shown a dramatic suppressive effect (68 – 75%) (Denomme et al. 2006; Denomme et al.
2007; Denomme et al. 2008). Thus, preliminary erythroid proliferation studies with anti-GYPC
Fab provided an ideal system in which to develop a protocol to test for the requirement of
antigen co-ligation with the more subtle suppressive effects of anti-Kell glycoprotein. As well,
these studies offered the opportunity to explore possible parallels between anti-GYPC and anti-
Kell glycoprotein in the mechanisms of erythroid progenitor suppression.
5.3.1 Characterization of Fab products
SDS-PAGE analysis of the anti-Kell glycoprotein Fab and anti-GYPC Fab products showed that
the purified digest contained mostly Fab fragments and not whole IgG. Indirect agglutination
tests were performed to ensure functionality of the Fab fragments to bind to red cells. The ability
of anti-(heavy and light chain) to agglutinate the Fab/RBC solution confirm that when anti-
(H+L) is added to anti-Kell glycoprotein Fab and erythroid progenitors in the liquid culture
system, anti-(H+L) and Fab can potentially ligate two Kell glycoproteins on the same erythroid
precursor cell.

60
5.3.2 Effect of Fab products on erythroid progenitor proliferation
Previous studies in our lab demonstrating the suppression of erythroid colony formation in semi-
solid methylcellulose culture by bivalent anti-Kell glycoprotein F(ab’)2 have shown that the Fc
portion of the anti-Kell glycoprotein immunoglobulin is not necessary for growth suppression.
Results from both the anti-Kell glycoprotein and anti-GYPC Fab studies show that binding of a
monovalent Fab fragment to the respective antigen does not suppress the proliferation of
erythroid progenitors compared to the whole immunoglobulin. However, when anti-(H+L) is
added to the Fab and erythroid progenitors in liquid culture, significant partial growth
suppression was observed (20-23%). The addition of anti-(H+L) to the Fab and erythroid
progenitors reconstituted the bivalency of the immunoglobulin and allowed it to ligate two
antigens on the erythrocyte surface. There are several explanations that may explain why there is
only partial suppression when anti-(H+L) was added to Fab. The preparation of the Fab product
by papain digestion may have reduced the affinity of the Fab for the antigen. Secondly, anti-
(H+L) may not be able to completely reconstitute the bivalency of the Fab fragments as
suggested by the lower degree of agglutination in the indirect agglutination test when compared
with whole IgG of equal concentration.
The necessity of co-ligation of Kell glycoprotein and GYPC for the suppression of erythroid
proliferation suggests that the spatial arrangement of the antigens in the membrane can have
intracellular effects due to Kell glycoprotein and GYPC’s attachment to the membrane skeleton.
Alteration of the steady state arrangement of the membrane proteins from co-ligation caused by
the binding of a bivalent antibody may cause alterations in the organization of the membrane
skeleton and/or downstream signaling leading to growth suppression of early erythroid cells.
Kell glycoprotein’s association with XK may be of significance in the mechanism of erythroid
growth suppression due to anti-Kell glycoprotein. Since Kell glycoprotein is covalently linked to
XK, co-ligation of Kell could cause alterations to XK. XK has also been shown to associate with
the membrane skeleton (Salomao et al. 2008). Thus, cytoskeletal reorganization or other
intracellular alterations triggered by changes to Kell glycoprotein and XK on the cell surface
may lead to the perturbation of a cascade of intracellular signaling pathways that are important
for red cell proliferation.

61
5.4 Role of apoptosis in the growth inhibitory effect of anti-Kell glycoprotein
Throughout this study, bivalent antibodies to Kell glycoprotein were shown to suppress the
proliferation of erythroid progenitor cells. However, it was unclear by what intracellular
mechanism the antibodies mediate the growth suppression. To determine whether apoptosis is
involved in the mechanism of erythroid progenitor growth suppression of anti-Kell glycoprotein,
markers of apoptosis such as loss of phosphatidylserine asymmetry and mitochondrial membrane
depolarization was evaluated in erythroid cell culture. To investigate the role of caspases, a
general caspase inhibitor was added to anti-Kell glycoprotein induced cell cultures. As well, a
caspase activation assay was performed.
5.4.1 Phosphatidylserine asymmetry in anti-Kell glycoprotein induced erythroid
progenitors
The externalization of the membrane phospholipid phosphatidylserine on the plasma membrane
surface has been shown to be a marker of both necrotic and apoptotic modes of cellular death
(Koopman et al. 1994; Cocco et al. 2001). PS expression on the cell surface can be detected
using the high affinity acidic phospholipid binding protein Annexin-V (Vermes et al. 1995). In
this study, Kell glycoprotein ligation with anti-Kell glycoprotein was not found to significantly
induce the expression of PS on erythroid progenitors. This observation is consistent with the
similar cell viabilities, as determined by trypan blue exclusion, between the negative control and
anti-Kell glycoprotein treated cultures. As well, another group has found that antibodies to Kell
glycoprotein did not induce any significant PS expression on mature erythrocytes (Head et al.
2005). The vital dye, PI, is used to detect necrotic cells. Since, anti-Kell glycoprotein treated
cells did not have increased PI staining compared to the negative control, the treated cells do not
appear to undergo a necrotic pathway of cell death.

62
5.4.2 Effect of a general caspase inhibitor on the growth inhibitory effect of anti-Kell
glycoprotein
Members of the caspase gene family (cysteine proteases with aspartate specificity) play
significant roles in apoptosis. Caspases exhibit catalytic and substrate-recognition motifs that
have been highly conserved and allow caspases to interact with both positive and negative
regulators of their activity (Cryns et al. 1998). The substrate preferences or specificities of
individual caspases have been exploited for the development of peptides that compete for
caspase binding. Z-VAD-FMK is a general caspase inhibitor that acts as an irreversible inhibitor
with no added cytotoxic effects in our cell culture system. Z-VAD’s ability to rescue classical
apoptosis due to caspase activation was shown in studies with etoposide, an antitumor agent that
blocks cell cycle progression.
This study showed that Z-VAD did not rescue the growth suppression caused by anti-Kell
glycoprotein. The implication is that caspases are not involved or are not the sole pathway by
which antibodies to Kell glycoprotein suppress erythroid progenitor proliferation.
5.4.3 Caspase activation in anti-Kell glycoprotein induced erythroid cell cultures
To further investigate whether caspases play a role in the mechanism by which anti-Kell
glycoprotein suppresses the growth of erythroid progenitors, a caspase activation assay was
performed. Fluorescein-conjugated V-D-FMK (ApoStat) binds to activated caspases and allows
for the intracellular detection of caspase activation.
This study showed that anti-Kell glycoprotein treated cultures did not have significantly
activated caspases. This observation is consistent with the finding that erythroid progenitor
growth suppression induced by anti-Kell glycoprotein could not be rescued by a general caspase
inhibitor. The ApoStat fluorescence of both the anti-Kell glycoprotein and isotype control
treated cultures were relatively high compared to healthy cells, which were maintained in
exponential growth phase in culture. Cells to which antibody or Z-VAD/etoposide reagent was
added were analyzed after a three-day period of incubation. During this period, no additional
nutrients were added to the cultures. As well, there is variability between different vials of
CD34+ erythroid progenitors in proliferation and cell viability. Thus, the relatively high

63
background fluorescence observed in the isotype control cultures can be attributed to culture
conditions and individual variability. Future studies should be conducted to confirm these results
and can evaluate cultures at earlier timepoints.
5.4.4 Mitochondrial membrane potential of anti-Kell glycoprotein treated cells
Loss of mitochondrial membrane potential is an early event in apoptosis (Zamzami et al. 1995).
To investigate whether the growth suppression induced by anti-Kell glycoprotein causes
membrane depolarization involved in apoptosis, JC-1 labeling was performed. JC-1 is a cationic
dye that exhibits transmembrane potential-dependent accumulation in the mitochondria, forming
J-aggregates with intense red fluorescence (~590 nm). In apoptotic cells with low mitochondrial
membrane potential, JC-1 remains in the monomeric form, which shows only green fluorescence
(~525 nm). Thus, mitochondrial depolarization is indicated by a loss of red fluorescence.
This study showed that anti-Kell glycoprotein treated cell cultures did not have significantly
increased levels of mitochondrial membrane depolarization. This observation is consistent with
the finding that other key events and markers of apoptosis such as loss of phosphatidylserine
asymmetry and caspase activation are not involved in the erythroid progenitor growth
suppression induced by anti-Kell glycoprotein. Thus, these results suggest that the mechanism
of suppression of anti-Kell glycoprotein is distinct from either classical or caspase-independent
apoptosis.
5.5 Ability of serial additions of erythropoietin to rescue growth suppression caused by
anti-Kell glycoprotein
Studies have shown that erythropoietin represents the main cytokine involved in the control of
erythropoiesis. The main targets of Epo are represented by bone marrow erythroid cells
expressing the single transmembrane receptor, erythropoietin receptor (EpoR): particularly,
CFU-E and proerythroblasts, where the EpoR is maximally expressed (about 1000 receptors per
cell). However, Epo and its receptor are not required for the commitment of hemopoietic stem
cells to the erythroid lineage (Wu et al. 1995). The use of recombinant Epo has been reported in
the successful management of late onset anemia due to anti-KEL1 (Dhodapkar et al. 2001) and

64
anti-KEL5 (Manoura et al. 2007). Thus, it is conceivable that erythropoietin may rescue the
growth suppressive effects of anti-Kell glycoprotein on erythroid progenitors.
This study showed that serially adding excess erythropoietin did not reduce the suppressive
effect of anti-Kell glycoprotein on erythroid progenitors. The implication may be that increased
signaling through the EpoR cannot abrogate the blocked or altered signaling pathways through
which anti-Kell glycoprotein suppresses the proliferation of progenitor cells. Therefore, Epo
therapy may be beneficial in the clinical setting by overcoming anti-K suppression through
targeting cells with no antibody bound to them. Our experimental results suggest that Epo does
not rescue the growth suppression of cells that are coated with anti-Kell glycoprotein.
The absence of markers of apoptosis, such as phosphatidylserine externalization, mitochondrial
membrane depolarization and caspase activation, in cell cultures treated with anti-Kell
glycoprotein suggests that the mechanism of growth suppression is distinct from programmed
cell death and necrosis. While anti-Kell glycoprotein may lead to an altered or blocked critical
intracellular signal, its effects are not lethal to the erythroid progenitor cell. This is in contrast to
the effects of anti-GYPC on erythroid progenitors, which causes dramatic growth suppression,
mitochondrial membrane depolarization, increased exofacial expression of PS, and an uptake of
PI (Denomme et al. 2007; Denomme et al. 2008).
5.6 Summary
HDFN due to anti-K is a significant challenge in the management of fetal morbidity and
mortality. The antigen distribution of requests for fetal blood group genotyping over a ten-year
period revealed that requests for KEL1 genotyping comprised 21.8% of the total requests, which
is second in number only to RHD. Therefore, anti-K HDFN represents a significant clinical
problem that requires further study.
The retrospective reviews performed of the laboratory and clinical aspects of HDFN have not
only confirmed that HDFN continues to be a significant problem, but that anti-K is a special case
in the clinical and laboratory management of HDFN. Due to the potential severity and the
unreliability of antibody titers to predict HDFN, monitoring at risk fetuses in the presence of
maternal anti-K may require increased resources compared to other antigen-positive fetuses.

65
Thus, the significance of HDFN due to anti-K warrants a better understanding of the unique
pathobiology of the condition.
The clinical manifestations of HDFN mediated by anti-K have features that are distinguishable
from the classical form of the disease due to anti-D. Affected fetuses may have lower numbers
of circulating reticulocytes and normoblasts compared to fetuses with anti-D HDFN, with levels
that are inappropriately low for the degree of fetal anemia. As well, antibody titers and amniotic
fluid bilirubin levels are not reliable predictors of anemia. These clinical characteristics and
previous in vitro studies suggest that the mechanism by which antibodies to Kell glycoprotein
leads to anemia is through suppression of erythropoiesis.
The study established a liquid in vitro erythroid progenitor cell culture model in which to
perform biochemical analyses on the mechanism of the suppressive growth effect of anti-Kell
glycoprotein. Using this culture model, this study explored the intracellular implications of the
binding of antibodies to Kell glycoprotein to erythroid progenitors. Results demonstrated the
requirement for co-ligation of Kell glycoprotein by a bivalent antibody for growth suppression.
The absence of markers of apoptosis, such as phosphatidylserine externalization, mitochondrial
membrane depolarization and caspase activation, in cell cultures treated with anti-Kell
glycoprotein suggests that the mechanism of growth suppression is distinct from programmed
cell death and necrosis. Furthermore, this growth suppression cannot be rescued by direct
addition of erythropoietin. Presently, the underlying mechanism of the inhibitory effect of anti-
Kell glycoprotein is not known.
5.7 Future Directions
The findings of this study elucidated the suppressive effect of co-ligating Kell glycoproteins on
the red cell surface by antibodies similar to those that can cause HDFN. As well, this study
evaluated whether apoptosis is involved in the erythroid progenitor growth suppression induced
by anti-Kell glycoprotein and whether erythropoietin can rescue the growth suppression.
However, it is still unclear what role Kell glycoprotein has in red cell maturation, and how the
binding of antibodies to this blood group antigen interfere with erythropoiesis.

66
Although studies have shown that Kell glycoprotein is associated with the underlying membrane
skeleton, the exact nature of the interaction is not clear. This study has shown the requirement of
co-ligation of Kell glycoprotein for erythroid progenitor growth suppression. Thus, the
organizational alteration due to the binding of a bivalent antibody to Kell glycoprotein likely
affects its interaction with the cytoskeleton. The present study focused on the Kell glycoprotein,
however, its association with XK may be of significance. Since Kell glycoprotein is covalently
linked to XK, co-ligation of Kell could cause alterations to XK. XK has also been shown to
associate with the membrane skeleton (Salomao et al. 2008). To examine if there are
organizational alterations to the membrane skeleton due to the binding of anti-Kell glycoprotein
on the cell surface, future work can utilize confocal or immunoelectron microscopy to examine
cystoskeletal components such as Protein 4.1, actin, and spectrin. Future studies should also
examine the effect of antibodies to XK on erythroid progenitor proliferation and cytoskeletal
organization. Unfortunately, monoclonal antibodies to XK are not available at the moment.
Cytoskeletal reorganization or other alterations to Kell glycoprotein and XK may lead to the
activation of a cascade of intracellular signaling pathways that are important for red cell
maturation. Future studies should elucidate the nature of these pathways. Studies have indicated
that Kell glycoprotein is phosphorylated and may be a substrate for casein kinase I and II
(Carbonnet et al. 1998). As well, there are numerous phosphorylation sites on the XK C-
terminal cytoplasmic domain (Carbonnet et al. 1998). Future experiments should examine if the
binding of antibodies to Kell glycoprotein or XK alters the phosphorylation of the cytoplasmic
domains of these transmembrane proteins.
Several decades of studies have shown that Epo represents the main cytokine involved in the
control of erythropoiesis. The main targets of Epo are erythroid cells expressing the
erythropoietin receptor, EpoR: particularly, CFU-E and proerythroblasts, where the EpoR is
maximally expressed. The signal transduction pathways induced by the activated EpoR are
complex and have been elucidated only in part. Active signaling molecules translocating to the
plasma membrane via docking to the phosphorylated EpoR activate a signaling cascade. An
example is the translocation of son of sevenless protein through adapter protein Grb-2 to activate
the mitogen-activated protein (MAP) kinase/ERK1/2 cascade. Alternatively, EpoR initiates

67
signal transduction through the activation of the Janus kinase (Jak2) (Wojchowski et al. 1999).
Through Jak2 activation, EpoR induces multiple signaling pathways that act together to prevent
apoptosis and to support terminal erythroid proliferation and differentiation. Among them, the
phosphatidyl-inositol 3 kinase, AKT kinase and RAS signaling pathways play a key role in the
mediation of many biological actions induced by Epo. Another important pathway activated by
EpoR is represented by Stat5, a member of the signal transducer and activator of transcription
(Stat) family, acting downstream numerous cytokine receptors and regulating cell growth
survival and differentiation via activation of target genes acting as a transcription factor. As a
consequence of EpoR activation Stat5 binds to phosphorylated tyrosines present on the
cytoplasmic tail of the EpoR, and itself becomes phosphorylated. The activated Stat5 dimerizes
and translocates to the nucleus, where it modulates the expression of several genes involved in
the control of cell proliferation and differentiation. In addition to these genes, Stat5 activates the
expression of several antiapoptotic genes in erythroid cells, most notably Bcl-XL (Dumon et al.
1999). The analysis of Stat5 knockout mice strongly suggests that the antiapoptotic effect of this
transcription factor in erythroid cells is exerted at the level of immature erythroid cells and is
mediated mainly via modulation of Bcl-XL. Future directions should investigate whether anti-
Kell glycoprotein growth suppression is mediated through altered Jak2 activation or Stat5
phosphorylation status.
As antibodies to the Kell blood group system do not appear to induce apoptosis to suppress the
proliferation of erythroid progenitors, it is possible that these antibodies interfere with cell cycle
progression in erythropoiesis. The increased proliferation at the CFU-E stage of erythropoiesis is
accompanied by upregulation of cyclins D3 and E and cyclin-dependent kinase (cdk) 2, whereas
late stage erythroblasts downregulate cyclins D3 and E (Dai et al. 2000). The inhibition of G1-
phase cyclins through their associated cdks plays a role in the regulated cessation of cell division
as CFU-Es mature to late erythroblasts (Hsieh et al. 2000). The retinoblastoma protein (pRb) has
also been implicated as a key regulator of erythroid differentiation (Jacks et al. 1992). Future
studies can evaluate whether antibodies to Kell glycoprotein alter levels of cell cycle-related
proteins cyclins D3 and E and cdk2 or alter the phosphorylation status of pRb. Other cell cycle
analyses can also be performed such as 5-bromo-2-deoxyuridine (BrdU) incorporation to
evaluate the effect of anti-Kell glycoprotein on erythroid cell replication.

68
Chapter 6
References

69
Alfirevic, Z. and A. Tabor (2007). "Pregnancy loss rates after midtrimester amniocentesis."
Obstet Gynecol 109(5): 1203-4; author reply 1204.
Allen, F. H., S. M. R. Krabbe and P. A. Corcoran (1961). "A new phenotype (McLeod) in the
Kell blood-group system." Vox Sang 6: 555-560.
Archer, G. T. (1965). "Phagocytosis by human monocytes of red cell coated wth Rh antibodies."
Vox Sang 10: 590-598.
Arndt, P. A., G. Garratty, G. Daniels, C. A. Green, A. M. Wilkes, P. Hunt, J. Do, S. Glenn and
D. Peterson (2005). "Late onset neonatal anaemia due to maternal anti-Ge: possible association
with destruction of eythroid progenitors." Transfus Med 15(2): 125-32.
Ballas, S. K., S. M. Bator, J. P. Aubuchon, W. L. Marsh, D. E. Sharp and E. M. Toy (1990).
"Abnormal membrane physical properties of red cells in McLeod syndrome." Transfusion 30:
722-727.
Bertelson, C. J., A. O. Pogo, A. Chaudhuri, W. L. Marsh, C. M. Redman, D. Banerjee, W. A.
Symmans, T. Simon, D. Frey and L. M. Kunkel (1988). "Localization of the McLeod locus (XK)
within Xp21 by deletion analysis." Am J Hum Genet 42(5): 703-11.
Bieber, E. (2001). "Erythropoietin, the biology of erythropoiesis and epoetin alfa. An overview."
J Reprod Med 46(5 Suppl): 521-30.
Bony, V., P. Gane, P. Bailly and J. P. Cartron (1999). "Time-course expression of polypeptides
carrying blood group antigens during human erythroid differentiation." Br J Haematol 107(2):
263-74.
Bowman, J. M., B. Chown, M. Lewis and J. Pollock (1977). "Rh isoimmunization, Manitoba,
1963-75." Can Med Assoc J 116(3): 282-4.
Bowman, J. M., J. M. Pollock, F. A. Manning, C. R. Harman and S. Menticoglou (1992).
"Maternal Kell blood group alloimmunization." Obstet Gynecol 79(2): 239-44.

70
Caine, M. E. and E. Mueller-Heubach (1986). "Kell sensitization in pregnancy." Am J Obstet
Gynecol 154: 85-90.
Calenda, G., J. Peng, C. M. Redman, Q. Sha, X. Wu and S. Lee (2006). "Identification of two
new members, XPLAC and XTES, of the XK family." Gene 370: 6-16.
Carbonnet, F., C. Hattab, J. P. Cartron and O. Bertrand (1998). "Kell and Kx, two disulfide-
linked proteins of the human erythrocyte membrane are phosphorylated in vivo." Biochem
Biophys Res Commun 247(3): 569-75.
Carbonnet, F., C. Hattab, E. Collec, C. Le van Kim, J. P. Cartron and O. Bertrand (1997).
"Immunochemical analysis of the Kx protein from human red cells of different Kell phenotypes
using antibodies raised against synthetic peptides." Br J Haematol 96(4): 857-63.
Chown, B. (1954). "Anemia from bleeding of the fetus into the mother's circulation." Lancet 1:
1213-1215.
Claperon, A., C. Hattab, V. Armand, S. Trottier, O. Bertrand and T. Ouimet (2007). "The Kell
and XK proteins of the Kell blood group are not co-expressed in the central nervous system."
Brain Res 1147: 12-24.
Cocco, R. E. and D. S. Ucker (2001). "Distinct modes of macrophage recognition for apoptotic
and necrotic cells are not specified exclusively by phosphatidylserine exposure." Mol Biol Cell
12(4): 919-30.
Coombs, R. R. A., A. E. Mourant and R. R. Race (1946). "In vivo isosensitisation of red cells in
babies with haemolytic disease." Lancet i: 244-266.
Cormier, F., P. de Paz and F. Dieterlen-Lievre (1986). "In vitro detection of cells with monocytic
potentiality in the wall of the chick embryo aorta." Dev Biol 118(1): 167-75.
Cryns, V. and J. Yuan (1998). "Proteases to die for." Genes Dev 12(11): 1551-70.
Dai, M. S., C. R. Mantel, Z. B. Xia, H. E. Broxmeyer and L. Lu (2000). "An expansion phase
precedes terminal erythroid differentiation of hematopoietic progenitor cells from cord blood in

71
vitro and is associated with up-regulation of cyclin E and cyclin-dependent kinase 2." Blood
96(12): 3985-7.
Daniels, G., W. A. Flegel, A. Fletcher, G. Garratty, C. Levene, C. Lomas-Francis, J. M. Moulds,
J. J. Moulds, M. L. Olsson, M. A. Overbeeke, J. Poole, M. E. Reid, P. Rouger, C. E. van der
Schoot, M. Scott, P. Sistonen, E. Smart, J. R. Storry, Y. Tani, L. C. Yu, S. Wendel, C. M.
Westhoff and T. Zelinski (2007). "International Society of Blood Transfusion Committee on
Terminology for Red Cell Surface Antigens: Cape Town report." Vox Sang 92(3): 250-3.
Daniels, G. and C. Green (2000). "Expression of red cell surface antigens during erythropoiesis."
Vox Sang 78 Suppl 2: 149-53.
Daniels, G., A. G. Hadley and C. Green (2003). "Cause of fetal anemia in hemolytic disease due
to anti-K." Transfusion 43: 115-116.
Daniels, G., F. Weinauer, C. Stone, M. Ho, C. Green, H. J. Jochem and A. P. Monaco (1996). "A
combination of the effects of rare genotypes at the XK and KEL blood group loci results in
absence of Kell system antigens from the red blood cells." Blood 88: 4045-4050.
Daniels, G. L. and I. Bromilow (2006). Essential Guide to Blood Groups, Blackwell Publishing.
Darrow, R. R. (1938). "Icterus gravis (erythroblastosis) neonatorum: examination of etiologic
considerations." Arch Path 25: 378-417.
Denomme, G. A., J. Micieli, J. Shu, D. Wang and B. Fernandes (2007). Anti-glycophorin C
induces a loss of mitochondrial membrane potential but fails to activate apoptotic caspases.
Abstracts of the American Society of Hematology 49th Annual Meeting, December 8-11, 2007,
Atlanta, Georgia, USA. 110: 8a-1093a.
Denomme, G. A., J. Micieli, D. Wang and B. Fernandes (2008). Anti-glycophorin C induces
mitochondrial membrane depolarization and a loss of ERK1/2 activity that is reversed by pre-
treatment with cytochalasin D: implications for anti-Ge3 HDFN. Abstracts of the XXXth
International Congress of the International Society of Blood Transfusion. June 7-12, 2008.
Macao, SAR, China.

72
Denomme, G. A., A. Shahcheraghi, D. P. Blackall, K. K. Oza and G. Garratty (2006). "Inhibition
of erythroid progenitor cell growth by anti-Ge3." Br J Haematol 133(4): 443-4.
Dhodapkar, K. M. and F. Blei (2001). "Treatment of hemolytic disease of the newborn caused by
anti-Kell antibody with recombinant erythropoietin." J Pediatr Hematol Oncol 23(1): 69-70.
Diamond, L. K., K. D. Blackfan and J. M. Baty (1932). "Erythroblastosis fetalis and its
association with universal edema of the fetus, icterus gravis neonatorum and anemia of the
newborn." J Pediatr 1: 269-309.
Dumon, S., S. C. Santos, F. Debierre-Grockiego, V. Gouilleux-Gruart, L. Cocault, C. Boucheron,
P. Mollat, S. Gisselbrecht and F. Gouilleux (1999). "IL-3 dependent regulation of Bcl-xL gene
expression by STAT5 in a bone marrow derived cell line." Oncogene 18(29): 4191-9.
Eder, A. F. and C. S. Manno (2004). Alloimmune hemolytic disease of the fetus and newborn.
Philadelphia, PA, Lippincott, Williams & Wilkins.
Eisenberg, B. and R. J. Wapner (2002). "Clinical procedures in prenatal diagnosis." Best Pract
Res Clin Obstet Gynaecol 16(5): 611-627.
Fibach, E., D. Manor, A. Oppenheim and E. A. Rachmilewitz (1989). "Proliferation and
maturation of human erythroid progenitors in liquid culture." Blood 73(1): 100-3.
Finning, K., P. Martin, J. Summers and G. Daniels (2007). "Fetal genotyping for the K (Kell)
and Rh C,c, and E blood groups on cell-free fetal DNA in maternal plasma." Transfusion 47:
2126-2133.
Finning, K. M., P. G. Martin, P. W. Soothill and N. D. Avent (2002). "Prediction of fetal D
status from maternal plasma: introduction of a new noninvasive fetal RHD genotyping service."
Transfusion 42(8): 1079-85.
Gahmberg, C. G., M. Jokinen and L. C. Andersson (1978). "Expression of the major
sialoglycoprotein (glycophorin) on erythroid cells in human bone marrow." Blood 52(2): 379-87.

73
Gane, P., C. Le Van Kim, V. Bony, W. El Nemer, I. Mouro, V. Nicolas, Y. Colin and J. P.
Cartron (2001). "Flow cytometric analysis of the association between blood group-related
proteins and the detergent-insoluble material of K562 cells and erythroid precursors." Br J
Haematol 113(3): 680-8.
Giblett, E. R. (1961). "A critique of the theoretical hazard of inter vs intra-racial transfusion."
Transfusion 1: 233-238.
Harris, R. A., A. E. Washington, R. F. Nease, Jr. and M. Kuppermann (2004). "Cost utility of
prenatal diagnosis and the risk-based threshold." Lancet 363(9405): 276-82.
Head, D. J., Z. E. Lee, J. Poole and N. D. Avent (2005). "Expression of phosphatidylserine (PS)
on wild-type and Gerbich variant erythrocytes following glycophorin-C (GPC) ligation." Br J
Haematol 129(1): 130-7.
Ho, M., J. Chelly, N. Carter, A. Danek, P. Crocker and A. P. Monaco (1994). "Isolation of the
gene for McLeod syndrome that encodes a novel membrane transport protein." Cell 77: 869-880.
Hsieh, F. F., L. A. Barnett, W. F. Green, K. Freedman, I. Matushansky, A. I. Skoultchi and L. L.
Kelley (2000). "Cell cycle exit during terminal erythroid differentiation is associated with
accumulation of p27(Kip1) and inactivation of cdk2 kinase." Blood 96(8): 2746-54.
Hughes-Jones, N. S. and C. A. Clarke (1982). Hemolytc disease of newborn. Oxford, Blackwell
Scientific Publications.
Huyhn, A., M. Dommergues, B. Izac, L. Croisille, A. Katz, W. Vainchenker and L. Coulombel
(1995). "Characterization of hematopoietic progenitors from human yolk sacs and embryos."
Blood 86(12): 4474-85.
Jacks, T., A. Fazeli, E. M. Schmitt, R. T. Bronson, M. A. Goodell and R. A. Weinberg (1992).
"Effects of an Rb mutation in the mouse." Nature 359(6393): 295-300.
Ji, P., S. R. Jayapal and H. F. Lodish (2008). "Enucleation of cultured mouse fetal erythroblasts
requires Rac GTPases and mDia2." Nat Cell Biol 10(3): 314-21.

74
Jung, H. H., M. Hergersberg, M. Vogt, J. Pahnke, V. Treyer, B. Rothlisberger, S. S. Kollias, D.
Russo and B. M. Frey (2003). "Mcleod phenotype associated with a XK missense mutation
without hematologic, neuromuscular, or cerebral involvement." Transfusion 43: 928-938.
Khamlichi, S., P. Bailly, D. Blanchard, D. Goossens, J. P. Cartron and O. Bertrand (1995).
"Purification and partial characterization of the erythrocyte Kx protein deficient in McLeod
patients." Eur J Biochem 228(3): 931-4.
Koopman, G., C. P. Reutelingsperger, G. A. Kuijten, R. M. Keehnen, S. T. Pals and M. H. van
Oers (1994). "Annexin V for flow cytometric detection of phosphatidylserine expression on B
cells undergoing apoptosis." Blood 84(5): 1415-20.
Landsteiner, K. and A. S. Weiner (1940). "Agglutinable factor in human blood recognized by
immune sera for rhesus blood." Proc Soc Exp Bio Med(43): 223.
Lee, S. (1997). "Molecular basis of Kell blood group phenotypes." Vox Sang 73(1): 1-11.
Lee, S. (2007). "The value of DNA analysis for antigens of the Kell and Kx blood group
systems." Transfusion 47(1 Suppl): 32S-9S.
Lee, S., A. K. Debnath and C. Redman (2003). "Active amino acids of the Kell blood group
protein and model of the ectodomain based on the structure of neutral endopeptidase 24.11."
Blood 102: 3028-3034.
Lee, S., M. Lin, A. Mele, Y. Cao, J. Farmar, D. Russo and C. Redman (1999). "Proteolytic
processing of big endothelin-3 by the Kell blood group protein." Blood 94: 1440-1450.
Lee, S., D. Russo and C. Redman (2000). "Functional and structural aspects of the Kell blood
group system." Transfusion Medicine Reviews 14(2): 93-103.
Lee, S., D. Russo and C. M. Redman (2000). "The Kell blood group system: Kell and XK
membrane proteins." Semin Hematol 37(2): 113-21.
Lee, S., D. Russo, A. P. Reiner and J. H. Lee (2001). "Molecular defects underlying the Kell null
phenotype." J Biol Chem 276: 27281-27289.

75
Lee, S., X. Wu, M. Reid, T. Zelinski and C. Redman (1995). "Molecular basis of the Kell (K1)
phenotype." Blood 85(4): 912-916.
Lee, S., E. Zambas, W. L. Marsh and C. Redman (1993). "The human Kell blood group maps to
chromosome 7q33 and its expression is restricted to erythroid cells." Blood 81: 2804-2809.
Leggat, H. M., J. M. Gibson, S. L. Barron and M. M. Reid (1991). "Anti-Kell in pregnancy." Br
J Obstet Gynaecol 98(2): 162-5.
Levine, P., L. Burnham, E. M. Katzin and P. Vogel (1941). "The role of isoimmunization in the
pathogenesis of erythroblastosis fetalis." Am J Obstet Gynecol 42: 925.
Levine, P. and R. E. Stetson (1939). "An unusual case of intra-group agglutination." J Amer Med
Ass 113: 126-127.
Li, Y., K. Finning, G. Daniels, S. Hahn, X. Zhong and W. Holzgreve (2008). "Noninvasive
genotyping fetal Kell blood group (KEL1) using cell-free fetal DNA in maternal plasma by
MALDI-TOF mass spectrometry." Prenat Diagn 28(3): 203-8.
Lo, Y. M., N. M. Hjelm, C. Fidler, I. L. Sargent, M. F. Murphy, P. F. Chamberlain, P. M. Poon,
C. W. Redman and J. S. Wainscoat (1998). "Prenatal diagnosis of fetal RhD status by molecular
analysis of maternal plasma." N Engl J Med 339(24): 1734-8.
Mancini, M., B. O. Anderson, E. Caldwell, M. Sedghinasab, P. B. Paty and D. M. Hockenbery
(1997). "Mitochondrial proliferation and paradoxical membrane depolarization during terminal
differentiation and apoptosis in a human colon carcinoma cell line." J Cell Biol 138(2): 449-69.
Manoura, A., E. Korakaki, E. Hatzidaki, E. Saitakis, S. Maraka, I. Papamastoraki, E.
Matalliotakis, K. Foundouli and C. Giannakopoulou (2007). "Use of recombinant erythropoietin
for the management of severe hemolytic disease of the newborn of a K0 phenotype mother."
Pediatr Hematol Oncol 24(1): 69-73.
Marfatia, S. M., R. A. Lue, D. Branton and A. H. Chishti (1994). "In vitro binding studies
suggest a membrane-associated complex between erythroid p55, protein 4.1, and glycophorin C."
J Biol Chem 269(12): 8631-4.

76
Marsh, W. L. and C. Redman (1987). Kell antigens and the McLeod red cell pheotype. Paris,
Librairie Arnette.
Marsh, W. L. and C. M. Redman (1990). "The Kell blood group system: a review." Transfusion
30(2): 158-67.
Martin, J. A., B. E. Hamilton, P. D. Sutton, S. J. Ventura, F. Menacker and M. L. Munson
(2002). "Births: Final data for 2002." Natl Vital Stat Rep 52: 1-116.
Moise, K. J. (2005). "Red blood cell alloimmunization in pregnancy." Semin Hematol 42(3):
169-78.
Moise, K. J. (2008). "Fetal anemia due to non-Rhesus-D red-cell alloimmunization." Semin Fetal
Neonatal Med 13(4): 207-14.
Moise, K. J., Jr. (2005). "Red blood cell alloimmunization in pregnancy." Semin Hematol 42:
169-178.
Palis, J. and M. C. Yoder (2001). "Yolk-sac hematopoiesis: the first blood cells of mouse and
man." Exp Hematol 29(8): 927-36.
Petz, L. D. and D. R. Branch (1983). Serological tests for the diagnosis of immune hemolytic
anemias. Immune Cytopenias. R. McMillan. New York, Churchill Livingstone.
Poole, J. and G. Daniels (2007). "Blood group antibodies and their significance in transfusion
medicine." Transfusion Medicine Reviews 21(1): 58-71.
Race, R. R. and R. Sanger (1975). Blood Groups in Man, 6th ed. Oxford, Blackwell Scientific.
Rautmann, H. (1912). "Uber Bltbildungbei fotaler allgemeiner Wassersucht." Beitr Path Anat
Allg Path 54: 332-339.
Redman, C. M., G. Avellino, S. R. Pfeffer, T. K. Mukherjee, M. Nichols, P. Rubinstein and W.
L. Marsh (1986). "Kell blood group antigens are part of a 93,000-dalton red cell membrane
protein." J Biol Chem 261(20): 9521-5.

77
Redman, C. M., W. L. Marsh, K. A. Mueller, G. P. Avellino and C. L. Johnson (1984). "Isolation
of Kell-active protein from the red cell membrane." Transfusion 24(2): 176-8.
Robinson, J., C. Sieff, D. Delia, P. A. Edwards and M. Greaves (1981). "Expression of cell-
surface HLA-DR, HLA-ABC and glycophorin during erythroid differentiation." Nature
289(5793): 68-71.
Russo, D., C. Redman and S. Lee (1998). "Association of XK and Kell blood group proteins." J
Biol Chem 273(22): 13950-6.
Russo, D., X. Wu, C. M. Redman and S. Lee (2000). "Expression of Kell blood group protein in
nonerythroid tissues." Blood 96(1): 340-6.
Sadahira, Y. and M. Mori (1999). "Role of the macrophage in erythropoiesis." Pathol Int 49(10):
841-8.
Salmon, C., J. P. Cartron and P. Rouger (1984). The Human Blood Groups. New York, Masson.
Salomao, M., X. Zhang, Y. Yang, S. Lee, J. H. Hartwig, J. A. Chasis, N. Mohandas and X. An
(2008). "Protein 4.1R-dependent multiprotein complex: new insights into the structural
organization of the red blood cell membrane." Proc Natl Acad Sci U S A 105(23): 8026-31.
Sha, Q., C. Redman and S. Lee (2006). "Endothelin-3-converting enzyme activity of the KEL1
and KEL6 phenotypes of the Kell blood group system." J Biol Chem 281(11): 7180-7182.
Shahcheraghi, A. (2005). The pathophysiology of anti-Kell "hemolytic disease of newborn".
Laboratory Medicine and Pathobiology. Toronto, University of Toronto. Master's of Science:
85.
Sinkule, J. A. (1984). "Etoposide: a semisynthetic epipodophyllotoxin. Chemistry,
pharmacology, pharmacokinetics, adverse effects and use as an antineoplastic agent."
Pharmacotherapy 4(2): 61-73.
Sjögren, B. and N. Uddenberg (1989). "Prenatal diagnosis and psychological distress:
amniocentesis or chorionic villus biopsy?" Prenat Diagn 9: 477-487.

78
Southcott, M., M. Tanner and D. J. Anstee (1999). "The expression of human blood group
antigens during erythropoiesis in a cell culture system." Blood 93: 4425-4435.
Steck, T. L. (1989). Red cell shape. Cell Shape: Determinants, Regulation, Regulatory Role. W.
Stein and F. Bonner. New York, Academic Press.
Stjernquist, M. (1998). "Endothelins--vasoactive peptides and growth factors." Cell Tissue Res
292(1): 1-9.
Tercyak, K. P., S. B. Johnson, S. F. Roberts and A. C. Cruz (2001). "Psychological response to
prenatal genetic counseling and amniocentesis." Patient Education and Counseling 43: 73-84.
van Kamp, I. L., F. J. Klumper, D. Oepkes, R. H. Meerman, S. A. Scherjon, F. P. Vandenbussche
and H. H. Kanhai (2005). "Complications of intrauterine intravascular transfusion for fetal
anemia due to maternal red-cell alloimmunization." Am J Obstet Gynecol 192: 171-177.
Vaughan, J. I., M. Manning, R. M. Warwick, E. A. Letsky, N. A. Murray and I. A. Roberts
(1998). "Inhibition of erythroid progenitor cells by anti-Kell antibodies in fetal alloimmune
anemia." N Engl J Med 338(12): 798-803.
Vaughan, J. I., R. Warwick, C. R. Welch and E. A. Letsky (1991). "Anti-Kell in pregnancy." Br
J Obstet Gynaecol 98(9): 944-5.
Vermes, I., C. Haanen, H. Steffens-Nakken and C. Reutelingsperger (1995). "A novel assay for
apoptosis. Flow cytometric detection of phosphatidylserine expression on early apoptotic cells
using fluorescein labelled Annexin V." J Immunol Methods 184(1): 39-51.
Wagner, T., G. Lanzer and K. Geissler (2002). "Kell expression on myeloid progenitor cells."
Leuk Lymphoma 43(3): 479-85.
Walker, R. H., H. H. Jung, C. Dobson-Stone, L. Rampoldi, A. Sano, F. Tison and A. Danek
(2007). "Neurologic phenotypes associated with acanthocytosis." Neurology 68: 92-98.
Weiner, C. P. and J. A. Widness (1996). "Decreased fetal erythropoiesis and hemolysis in Kell
hemolytic anemia." Am J Obstet Gynecol 174(2): 547-51.

79
Wojchowski, D. M., R. C. Gregory, C. P. Miller, A. K. Pandit and T. J. Pircher (1999). "Signal
transduction in the erythropoietin receptor system." Exp Cell Res 253(1): 143-56.
Wu, H., X. Liu, R. Jaenisch and H. F. Lodish (1995). "Generation of committed erythroid BFU-
E and CFU-E progenitors does not require erythropoietin or the erythropoietin receptor." Cell
83(1): 59-67.
Zaks, T. Z., D. B. Chappell, S. A. Rosenberg and N. P. Restifo (1999). "Fas-mediated suicide of
tumor-reactive T cells following activation by specific tumor: selective rescue by caspase
inhibition." J Immunol 162(6): 3273-9.
Zamzami, N., P. Marchetti, M. Castedo, C. Zanin, J. L. Vayssiere, P. X. Petit and G. Kroemer
(1995). "Reduction in mitochondrial potential constitutes an early irreversible step of
programmed lymphocyte death in vivo." J Exp Med 181(5): 1661-72.
Zon, L. I. (1995). "Developmental biology of hematopoiesis." Blood 86(8): 2876-91.

80
Chapter 7
Appendices

81
Grading Appearance of red cells
4+ One large agglutinate; no free cells; background clear
3+ Several large agglutinates; few free cells; background clear
2+ Moderate size agglutinates in a sea of smaller clumps and some free cells;
background cloudy
1+ Many small agglutinates; background cloudy
0 No agglutinates seen
Appendix A. Agglutination grading of indirect agglutination test (Petz et al. 1983).

82
Day 0
A. Isotype B. CD34 C. GYPA D. Kell gp E. GYPC
Day 1
F. Isotype G. CD34 H. GYPA I. Kell gp J. GYPC
Day 3
K. Isotype L. CD34 M. GYPA N. Kell gp O. GYPC
Appendix B. Cell surface marker expression of CD34+ cells seeded in liquid culture.
Flow cytometry analysis of cells cultured for 3-6 days and labeled with CD34-FITC, GYPA-
FITC, Kell gp-FITC, GYPC-FITC, or isotype control. To evaluate the suppressive effect,
antibody addition occurs on day 3 of initial culture (termed “Day 0” throughout this study). A-E.
Cells cultured for 3 days. A. Isotype control. B. CD34-FITC. C. Glycophorin A. D. Kell
glycoprotein. E. Glycophorin C. F-J. Cells cultured for 4 days. F. Isotype control. G.
CD34-FITC. H. Glycophorin A. I. Kell glycoprotein. J. Glycophorin C. K-O. Cells
cultured for 6 days. K. Isotype control. L. CD34-FITC. M. Glycophorin A. N. Kell
glycoprotein. O. Glycophorin C.

83
1 2 3
Appendix C. Non-reducing SDS-PAGE analysis of Kell glycoprotein Fab product.
Dialyzed anti-Kell glycoprotein Fab product () was analyzed by non-reducing SDS-PAGE to
determine purity. Lane 1 contains proteins eluted from the Protein A column used to purify the
Fab digest. The protein A column binds to undigested IgG (150 kDa) and Fc fragments (~ 50
kDa). Lanes 2 and 3 contain the purified Fab product (50 kDa).
49 100 Da -
209 000 Da -
124 000 Da -
28 900 Da -
Fab

84
Appendix D. Characterization of anti-GYPC Fab product
Studies with anti-glycophorin Fab were used as a model to evaluate suppression because GYPC
is expressed on the erythroleukemic cell line, K562. The K562 cell line provided a convenient
system in which to develop a Fab study protocol which would be further tested on CD34+ cell-
derived erythroid progenitors.
The anti-GYPC Fab product after papain digestion and Protein A column purification was
analyzed by non-reducing SDS-PAGE for purity. SDS-PAGE analysis of Fab fragments showed
two main bands at approximately 50 kDa and 60 kDa (Appendix E). Since whole anti-GYPC
was in the form of tissue culture supernatant, it contained other proteins other than whole IgG.
These other proteins can be seen in lane 5 in the anti-GYPC solution prior to digest but are
absent in the IgG only solution in lane 6. A faint band can be detected at 40 kDa, but the
absence of a band at 150 kDa indicated the absence of intact IgG. The BCA protein assay
determined the concentration of the Fab sample to be 461 µg/ml. Since whole anti-GYPC was in
the form of tissue culture supernatant, the concentration of anti-GYPC in the Fab product could
not be determined. Based on the reactivity of the whole anti-GYPC product in other cell culture
experiments, the volume of the Fab product was reduced by 48X with a centrifugal device to
concentrate the sample. The indirect agglutination test showed that the Fab product alone did not
agglutinate RBCs (degree of agglutination = 0). When the cells were washed and ~(H+L) was
added to the RBC/Fab solution, agglutination was observed (degree of agglutination = 2). There
was no agglutination observed when an antibody to the Fcγ portion of immunoglobulins was
added to the RBC/Fab solution. Whole IgG anti-GYPC agglutinated RBCs alone (degree of
agglutination = 2) and when ~Fcγ was added, a pellet was observed (degree of agglutination =
4). There was no agglutination when an isotype control was added to RBCs, nor when ~(H+L)
or ~Fcγ was added.

85
1 2 3 4 5 6
Appendix E. Non-reducing SDS-PAGE analysis of anti-GYPC Fab product.
Dialyzed anti-GYPC Fab product () was analyzed by non-reducing SDS-PAGE to determine
purity. Lane 1-3 contains the purified Fab product (50 kDa). Whole anti-GYPC solution is in
the form of tissue culture supernatant so it contains other proteins. Lane 4 contains the
unpurified digest, which includes undigested IgG (150 kDa), Fc fragments (50 kDa) and Fab (50
kDa). Lane 5 contains the whole anti-GYPC solution prior to papain digestion. Lane 6 contains
purified IgG prior to papain digestion (150 kDa).
209 000 Da -
49 100 Da -
124 000 Da -
34 800 Da -
80 000 Da -
Fab

86
Appendix F. Effect of anti-GYPC Fab on erythroid progenitor proliferation
The growth suppression of erythroid progenitors was examined in the presence of anti-GYPC
Fab fragments and anti-(H+L). Anti-GYPC Fab alone did not inhibit progenitor proliferation.
Anti-GYPC with anti-(H+L) inhibited the proliferation of erythroid progenitors by 49% relative
to the IgG Fab product alone on day +3 after antibody inducement. Anti-(H+L) with IgG Fab
did not cause suppression. Whole IgG anti-GYPC suppressed proliferation by 74%.
Viable cell count
(x 105 cells/ml) (mean ± SEM)
Percent growth suppression
(mean ± SEM)
IgG Fab 7.0 (0.1) 0
Anti-GYPC Fab 6.6 (0.1) 6 (0.5)
Whole anti-GYPC 1.9 (0.4) 74 (5.5)
Anti-GYPC Fab + anti-(H+L) 3.5 (0.3) 49 (3.5)
Suppression of progenitor proliferation by anti-GYPC Fab and anti-(H+L).
Viable cell count and percent growth suppression as compared to IgG Fab alone. GYPC Fab
fragments did not cause significant suppression of erythroid progenitor proliferation. Anti-
GYPC Fab and anti-(H+L) caused suppression relative to anti-GYPC Fab alone. Results are
expressed as mean percent suppression (±SEM) with three vials of CD34+ cells on day +3 (n =
3).

87
A. Healthy cells B. Etoposide C. Isotype control D. Anti-Kell glycoprotein
E. Z-VAD F. Z-VAD + Etoposide
Appendix G. Caspase activation of erythroid progenitors treated with anti-Kell
glycoprotein
Representative flow cytometry histograms of cells cultured for 6 days with antibody added on
day 3 and stained with ApoStat. The ordinate measures the number of cells displaying the
fluorescent intensity given by the abscissa. Dotted lines, negative control; solid unfilled line,
positive control. A. Healthy cells used as the negative gating control. M1 represents the percent
of cells in the positive staining region. 16.5% of healthy cells fell within the positive staining
region. B. Cells treated with etoposide. 97.6% of etoposide treated cells fell within the positive
staining region. C. Cells treated with isotype control. 60.0% of treated cells fell within the
positive staining region. D. Cells treated with anti-Kell glycoprotein. 64.6% of treated cells fell
within the positive staining region. E. Cells treated with Z-VAD only. 18.4% of treated cells
fall within the positive staining region. F. Cells treated with etoposide and Z-VAD. 68.0% of
treated cells fall within the positive staining region.
64.6%
60.0% 97.6%
18.4%
16.5%
68.0%