Embed Size (px)
Citation preview
This article was downloaded by: [University of Missouri - St Louis]On: 01 October 2013, At: 14:08Publisher: RoutledgeInforma Ltd Registered in England and Wales Registered Number: 1072954Registered office: Mortimer House, 37-41 Mortimer Street, London W1T 3JH,UK
Women & TherapyPublication details, including instructions forauthors and subscription information:http://www.tandfonline.com/loi/wwat20
The Influence of SilentLearning Disorders on the Livesof WomenSara J. Hoffschmidt PhD a & Cheryl S. Weinstein PhDb ca Harvard Medical School in the combinedneuropsychology training program of MassachusettsMental Health Center (MMHC) and the Beth-IsraelDeaconess Medical Center (BIDMC)., USAb Psychology of Harvard Medical School, USAc Center for Cognitive Remediation at the Beth IsraelDeaconess Hospital, USAPublished online: 10 Oct 2008.
To cite this article: Sara J. Hoffschmidt PhD & Cheryl S. Weinstein PhD (2003) TheInfluence of Silent Learning Disorders on the Lives of Women, Women & Therapy,26:1-2, 81-94, DOI: 10.1300/J015v26n01_05
To link to this article: http://dx.doi.org/10.1300/J015v26n01_05
PLEASE SCROLL DOWN FOR ARTICLE
Taylor & Francis makes every effort to ensure the accuracy of all theinformation (the “Content”) contained in the publications on our platform.However, Taylor & Francis, our agents, and our licensors make norepresentations or warranties whatsoever as to the accuracy, completeness,or suitability for any purpose of the Content. Any opinions and viewsexpressed in this publication are the opinions and views of the authors, andare not the views of or endorsed by Taylor & Francis. The accuracy of theContent should not be relied upon and should be independently verified withprimary sources of information. Taylor and Francis shall not be liable for any
losses, actions, claims, proceedings, demands, costs, expenses, damages,and other liabilities whatsoever or howsoever caused arising directly orindirectly in connection with, in relation to or arising out of the use of theContent.
This article may be used for research, teaching, and private study purposes.Any substantial or systematic reproduction, redistribution, reselling, loan,sub-licensing, systematic supply, or distribution in any form to anyone isexpressly forbidden. Terms & Conditions of access and use can be found athttp://www.tandfonline.com/page/terms-and-conditions
Dow
nloa
ded
by [
Uni
vers
ity o
f M
isso
uri -
St L
ouis
] at
14:
08 0
1 O
ctob
er 2
013
DORMANTAND PART-TIME DISABILITIES
The Influence of Silent Learning Disorderson the Lives of Women
Sara J. HoffschmidtCheryl S. Weinstein
SUMMARY. Longstanding neurocognitive deficits such as learningdisorders greatly influence development of a woman’s personality, rela-tionships, and educational and vocational attainment. In our clinical
Sara J. Hoffschmidt, PhD, is a post-doctoral fellow in neuropsychology at HarvardMedical School in the combined neuropsychology training program of MassachusettsMental Health Center (MMHC) and the Beth-Israel Deaconess Medical Center(BIDMC). Cheryl S. Weinstein, PhD, is Assistant Professor of Psychology of HarvardMedical School and Director of the Center for Cognitive Remediation at the Beth IsraelDeaconess Hospital. She is also Assistant Director of Training in the neuropsychologytraining program of the MMHC and the BIDMC.
Address correspondence to: Sara J. Hoffschmidt, Massachusetts Mental Health Cen-ter/Harvard Medical School, 74 Fenwood Road, Boston, MA 02115.
[Haworth co-indexing entry note]: “The Influence of Silent Learning Disorders on the Lives of Women.”Hoffschmidt, Sara J., and Cheryl S. Weinstein. Co-published simultaneously in Women & Therapy (TheHaworth Press, Inc.) Vol. 26, No. 1/2, 2003, pp. 81-94; and: Women with Visible and Invisible Disabilities:Multiple Intersections, Multiple Issues, Multiple Therapies (ed: Martha E. Banks, and Ellyn Kaschak) TheHaworth Press, Inc., 2003, pp. 81-94. Single or multiple copies of this article are available for a fee from TheHaworth Document Delivery Service [1-800-HAWORTH, 9:00 a.m. - 5:00 p.m. (EST). E-mail address:[email protected]].
2003 by The Haworth Press, Inc. All rights reserved. 81
Dow
nloa
ded
by [
Uni
vers
ity o
f M
isso
uri -
St L
ouis
] at
14:
08 0
1 O
ctob
er 2
013

practice, we increasingly see women with previously undiagnosed “si-lent learning disorders.” Educational and career milestones, problems inthe workplace, parenting a child with a learning disorder, and normal ag-ing along with common medical conditions can exacerbate these “silentlearning disorders.” As a result, neurocognitive deficits might appearmore pronounced as former ways of compensating for learning problemsno longer are adequate. When such learning disorders are not detected,women and their therapists might not avail themselves of interventionsthat can help to treat the reading, visual-spatial, organizational, or otherneurocognitive deficits, and indirectly help with patterns of anxiety, de-pression, and low self-esteem. In the present paper, we characterizewomen with silent learning disorders, discuss implications if disordersremain undetected, and present case examples. A model and strategiesfor detecting silent learning disorders also are presented. [Article copiesavailable for a fee from The Haworth Document Delivery Service:1-800-HAWORTH. E-mail address: <[email protected]> Website:<http://www.HaworthPress.com> © 2003 by The Haworth Press, Inc. All rights re-served.]
KEYWORDS. Learning disorders, undiagnosed learning disorders,women
INTRODUCTION
Women’s neurocognitive abilities influence their understanding ofthe world, their ability to connect with others, and educational and vo-cational achievement. The ability to attend to information, to processlengthy communication, and to inhibit distractions are essential compo-nents of interaction. If neurocognitive deficits are present (such asdistractibility, language processing deficits, reduced attention span),the entire course of development will be affected (Weinstein, Seidman,Feldman, & Ratey, 1991). Although cognitive vulnerabilities ulti-mately create a lot of “noise” and interrupt therapeutic, family, educa-tional, work, and social relationships (Sands & Ratey, 1986), manywomen find ways of compensating or “covering up” these areas of diffi-culty. As a result, such deficits (or “silent learning disorders”) are quitepainful because they might not be identified. Further, our culture com-pounds the struggle to compensate for neurocognitive difficulties by
82 WOMEN WITH VISIBLE AND INVISIBLE DISABILITIES
Dow
nloa
ded
by [
Uni
vers
ity o
f M
isso
uri -
St L
ouis
] at
14:
08 0
1 O
ctob
er 2
013

conveying the expectation that women be “superwomen,” juggling thedemands of a modern career along with more traditional roles of wifeand mother.
It is our experience conducting neuropsychological evaluations in anoutpatient hospital-based psychiatry department that women with “si-lent learning disorders” constitute a significant but often under-referredclinical population. In the current paper, we will: (1) characterize theclinical population of women with “silent learning disorders”; (2) dis-cuss implications if learning disorders remain undetected and presentcase examples; and (3) provide a model and strategy for detecting andtreating silent learning disorders.
Characterizing “Silent Learning Disorders”
We define a “silent learning disorder” as a previously undiagnosedlearning disorder in which a neurocognitive function of attention, mem-ory, planning and organization, visual-spatial processing, motor plan-ning, or reading, spelling, mathematical, or writing skills is 1.5 standarddeviations below intellectual functions. Further, these deficits cannot beaccounted for by cultural, emotional, or socio-economical explana-tions. Women with silent learning disorders might struggle to workaround these unacknowledged deficits. Because their difficulties arenot readily apparent, problems in functioning might be commonlymisattributed to laziness or failure to live up to potential. Problems infunctioning also can be mistakenly ascribed to emotional factors suchas depression, anxiety, or stress, but when a careful educational orneuropsychological evaluation is completed, it becomes clear that anxi-ety and depression are secondary to primary learning problems.
Implications of Silent Learning Disorders
Unfortunately one major consequence for women with silent learn-ing disorders is continuous “misses” in understanding others. In otherwords, an individual with language processing problems is more likelyto insert incorrect information that makes sense to her or him but mightnot have been presented. Attentional or auditory processing problemsalso can impede processing of social cues. Such miscommunications inprocessing and understanding the details of life can result in the failureto deepen relationships and determine what people mean when they saythings. When such an error occurs in a therapeutic setting, the lis-tener/therapist might not be aware of their patient’s auditory processing
Sara J. Hoffschmidt and Cheryl S. Weinstein 83
Dow
nloa
ded
by [
Uni
vers
ity o
f M
isso
uri -
St L
ouis
] at
14:
08 0
1 O
ctob
er 2
013
problems. Thus, detail or processing errors can be interpreted as resis-tance or a defense. This unfortunately might lead the patient to blameherself, not fully appreciating the role of her learning disability.
Difficulties with processing also impact development of authenticityand mutuality, behaviors that are necessary for satisfying relationships(Jordan, Kaplan, Miller, Stiver, & Surrey, 1991). When successful, mu-tuality reflects genuine interest shown in another individual, most oftenaccomplished through listening and paying attention. When one has aneurocognitive deficit that includes problems processing details, thecommunication flow that would lead to a deepening of relationship isnow disrupted, and partners, therapists, teachers, co-workers, andfriends might be left wondering “Are you with me?” or perhaps “Areyou interested?” Nontraditional therapeutic interventions that can im-prove communication might be considered, such as writing down de-tails of the session in the last ten minutes. Rather than taking the focusoff of more emotional material, the latter approach can actually help thepatient incorporate the ideas of therapy and improve the relationship.
Women in academic settings often face a complex interaction of silentlearning disorders and other psychological and developmental issues.Students might present to the therapist with complaints of depressedmood, anxiety, and lowered self-image, and the focus of therapy can beseparation from the family or improving ways of coping with stress.Rarely will a student say to a therapist, “I can’t take notes in largeclasses because I miss critical details,” or “I read slowly and can’t finishassignments.” Client One illustrates how both clients and therapistsmight focus more on emotional or family themes.
CLIENT EXAMPLE 1
RF, a twenty-six year old female graduate student from a presti-gious college, was not having success in dealing with her anxietyafter two years of intensive psychotherapy. Following years oftreatment for cancer, her mother died when RF was in the seventhgrade. Because her mother was so ill when she was learning toread, RF always thought that sadness about this contributed toanxiety when she was reading and writing. During the interview,however, we discovered that her father had atypical reading hab-its. He misread words during church services and his e-mail letterswere “short blips of language.” Although her father always encour-aged her education, she saved her money for a neuropsychological
84 WOMEN WITH VISIBLE AND INVISIBLE DISABILITIES
Dow
nloa
ded
by [
Uni
vers
ity o
f M
isso
uri -
St L
ouis
] at
14:
08 0
1 O
ctob
er 2
013

evaluation that he perceived as a “narcissistic exercise.”On formal evaluation, RF appeared slightly anxious and
provided psychological and emotional explanations when she haddifficulty on testing. She was puzzled by her “slowness.” Overallintellect was in the superior range, but RF appeared to have both aspelling disorder (10th percentile) and a reading disorder (1st per-centile). Anxiety did not account for the slowed reading as the pa-tient was unaware that her reading was slowed. A treatment shiftoccurred based on the neuropsychological evaluation. The mean-ing of RF’s anxiety was expanded to include her experience ofcoping with a silent learning disorder. Specifically, it was hard tomake decisions about her career and whether to pursue a graduatedegree without anyone realizing how very hard she worked orcommending her for her efforts.
Other women who are students might find they have exhausted theirresources for coping with a silent learning disorder when they face ma-jor challenges such as graduate school admissions. A frequently heardissue is “If the law school ever knows that I read slowly, I’ll never getin,” or “I can’t tell my professor I need extended time for an examina-tion. He’ll think I’m weak, and there will be no job recommendation.”Client Two highlights such difficulties.
CLIENT EXAMPLE 2
Patient MB presented for neuropsychological evaluation ques-tioning whether she had a learning disorder. She was in the processof applying to a highly competitive graduate program and wasconcerned that her grades, which were above average but notstraight “As,” would be reason to reject her. MB persisted in fear-ing that the current evaluation would reveal that she was “reallydumb,” even though learning difficulties were identified during aprevious evaluation in her native country. Focusing on her per-ceived intellectual deficit, she presented with symptoms of anxi-ety and depression, and ignored that the prior evaluation hadshowed reading deficits in the context of very high intellect.
Results of our evaluation were consistent with her priorevaluation. Her verbal intellect was within the very superior range(> 99th percentile rank), yet her reading rate and comprehension
Sara J. Hoffschmidt and Cheryl S. Weinstein 85
Dow
nloa
ded
by [
Uni
vers
ity o
f M
isso
uri -
St L
ouis
] at
14:
08 0
1 O
ctob
er 2
013

were severely lowered (1st percentile rank and 12th percentilerank, respectively). Although she struggled with the knowledgethat her reading was so low, a major intervention was accom-plished in again reinforcing the excellence of her intellect. Shealso was able to focus on ways of coping with her deficits, in effectexpanding treatment of her depression beyond medication to aca-demic areas that were devastating to her self-esteem.
Once they leave school, women with silent learning disorders mightconclude that learning problems are no longer an issue. In part, theyhope that they will “outgrow” their learning problems (Hechtman,1996). Unfortunately learning difficulties are likely to persist, manifest-ing themselves in the workplace. A woman might find herself workinglong hours to circumvent slowed reading, or continuously misunder-standing work assignments because of poor organization or mishearingdetails of a project. Such women can present to the therapist with com-plaints related to loneliness because there is no time for a social life.Frustration levels might increase as they see seemingly less intelligentindividuals get promoted. Other women with silent learning problemsmight succeed, but interpersonal issues in the work environment are asource of significant stress. Because of the measures they take to com-pensate, they might be seen as rigid or demanding, as with Client Three.
CLIENT EXAMPLE 3
LP is a thirty-seven year old married mother of two children. Sheworked as a lawyer in an environment where there were specificrules to follow (e.g., preparing wills, contracts, etc.). She experi-enced significant success at work, but she had much difficultyworking with her secretarial staff. Notably she was demanding andwas prone to “blow up” when the necessary information was not infront of her. There were also problems at home where LP becameparticularly upset when there was not a plan for the day. While sheprided herself in getting things done, it was particularly frustratingto her when her family did not follow a schedule. She was referredfor a neuropsychological evaluation because of marital difficulties.LP’s husband worried that LP was not aware of her behavior atwork and the overflow of problems to the home environment.
On neuropsychological assessment, LP’s intellect was wellabove average (84th percentile rank). She excelled on planning and
86 WOMEN WITH VISIBLE AND INVISIBLE DISABILITIES
Dow
nloa
ded
by [
Uni
vers
ity o
f M
isso
uri -
St L
ouis
] at
14:
08 0
1 O
ctob
er 2
013
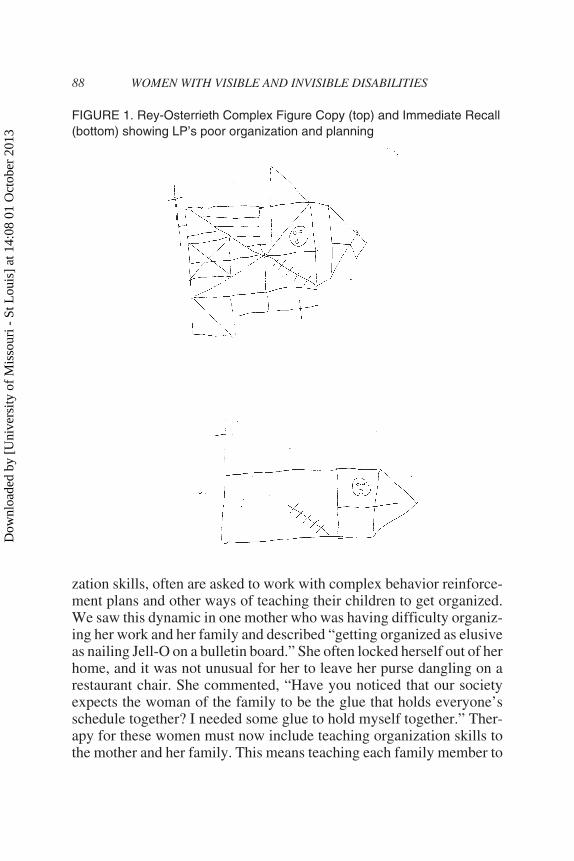
problem solving tasks when the information was in front of her. Incontrast, organization and planning skills on less structured taskswere markedly inefficient. This was seen on the copy of the ReyOsterrieth Complex Figure (Osterrieth, 1944) in which she startedon the right side of space rather than the expected left side ofspace. She copied parts of the design rather than looking at the ma-jor organization components of the design (“the big picture”). Thisled to significant memory problems when she had to reproduce thedesign immediately after she drew it (see Figure 1).
Based on the neuropsychological evaluation, LP and herhusband were referred for therapy to help them to better under-stand the meaning of LP’s neurocognitive strengths and relativedeficits. For LP, recognizing her difficulty problem solving whenthe information was not in front of her was important. She sharedthis with her staff who looked at her in a more empathic manner.She also could begin to address ways to work with staff to improveand take responsibility for her organization skills. At the sametime, ways for LP to deal with organization problems at homewere initiated. Her husband now understood her “demanding” be-havior, and jointly they worked in therapy to problem solve in amore effective way.
Adult women can again confront silent learning problems when theysee their children struggle and get diagnosed with a formal learning dis-order. They often identify with their children’s difficulties, and mightexperience feelings of both pain and guilt as they relive their own diffi-culties in their child’s learning problems. At this point many womenwith silent learning disorders can better appreciate their own struggles,leading them to reassess their problems in learning. Specifically, ques-tions might arise such as “Maybe I wasn’t just talkative or a daydreamerbecause I was a girl. Maybe I had attention deficit disorder too!” or“Maybe math wasn’t impossible for me just because I was a girl!”
Compounding their heightened awareness of their own learningproblems, mothers of children with learning disorders can face greatfrustration when their children’s teachers tell them to organize theirchildren. Such a mother, with her own impaired organizational skills,might unfortunately be viewed as an unhelpful or disinterested parent.When impairments are more obvious, as in the case of multiple sclerosisor Parkinson’s disease, parents are not typically expected to teach theirchild to work rapidly or get more organized. Yet, parents with otherbrain based difficulties, such as learning disorders with reduced organi-
Sara J. Hoffschmidt and Cheryl S. Weinstein 87
Dow
nloa
ded
by [
Uni
vers
ity o
f M
isso
uri -
St L
ouis
] at
14:
08 0
1 O
ctob
er 2
013
zation skills, often are asked to work with complex behavior reinforce-ment plans and other ways of teaching their children to get organized.We saw this dynamic in one mother who was having difficulty organiz-ing her work and her family and described “getting organized as elusiveas nailing Jell-O on a bulletin board.” She often locked herself out of herhome, and it was not unusual for her to leave her purse dangling on arestaurant chair. She commented, “Have you noticed that our societyexpects the woman of the family to be the glue that holds everyone’sschedule together? I needed some glue to hold myself together.” Ther-apy for these women must now include teaching organization skills tothe mother and her family. This means teaching each family member to
88 WOMEN WITH VISIBLE AND INVISIBLE DISABILITIES
FIGURE 1. Rey-Osterrieth Complex Figure Copy (top) and Immediate Recall(bottom) showing LP’s poor organization and planning
Dow
nloa
ded
by [
Uni
vers
ity o
f M
isso
uri -
St L
ouis
] at
14:
08 0
1 O
ctob
er 2
013
use a memory notebook in which they can all see everything they needto do for the day. It will also be important to calculate the amount oftime it would take to do the task, the family member who is responsiblefor the activity, and a backup plan if there is a problem.
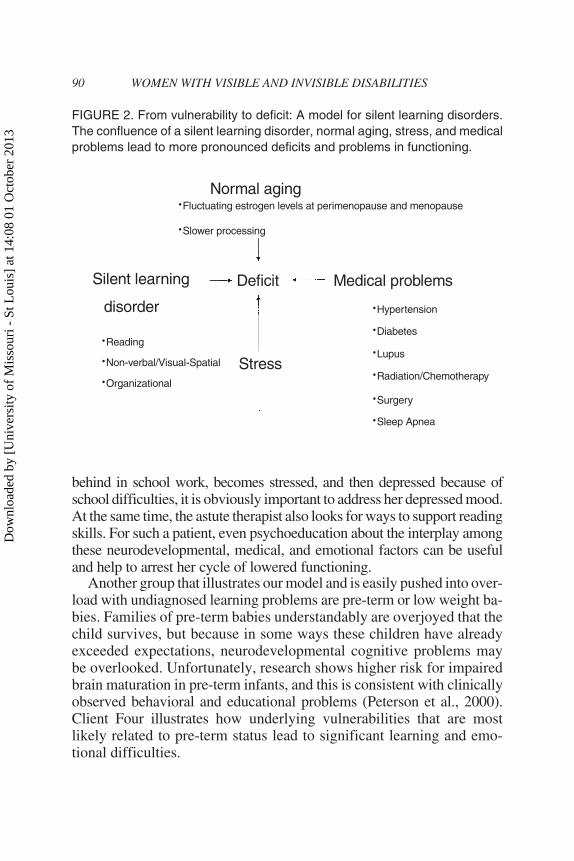
The process of aging leads yet another group of women to becomemore aware of silent learning problems when they are diagnosed withmedical problems. When interviewed, they may say “I am in goodhealth . . . with just a little hypertension” or “I only have thyroid prob-lems” or “I only snore a little bit . . . just a little sleep apnea.” In additionto medical problems that can impact neurocognitive functioning such ashypertension, hypothyroidism, sleep apnea, and diabetes, the normalaging process also can present changes in thinking. Older patients arelikely to experience slower processing speed, and changes in estrogenlevels due to menopause can lead to changes in executive functions suchas directed attention, working memory, inhibition of inappropriate re-sponses, and cognitive flexibility (Keenan, Ezzat, Ginsburg, & Moore,2001). When these patients come to therapy with complaints of difficul-ties coping or feeling more easily stressed, it is important to reviewschool records. After a neuropsychological assessment, it might be-come clear that there is a longstanding silent learning disorder. Up untilthis point, hard work and other ways of compensating have helped todisguise the disorder, but once even a mild medical problem develops,the deficit is more apparent. Unfortunately, the normal aging processmakes it harder to circumvent longstanding deficits, and it appears that“a little reading disorder” plus mild hypothyroidism along with normalaging pushes the patient into overload (see Figure 2).
FROM VULNERABILITY TO DEFICIT:A MODEL FOR SILENT LEARNING DISORDERS
Figure 2 demonstrates the overload model where a confluence ofseemingly mild problems leads to a deficit. A physician might look ateach problem in isolation given the demands of managed care, and deter-mine that the woman is stressed. This can lead to focused treatment thatcannot address all relevant biological, psychological, and social factors.
The psychotherapist, however, is challenged to look at the big pic-ture, and integrate all relevant factors that can contribute to learningproblems. For example, a college student might work around slowed read-ing with success. She can, however, have premenstrual dysphoric prob-lems, and at such times reading is extremely difficult. If the patient gets
Sara J. Hoffschmidt and Cheryl S. Weinstein 89
Dow
nloa
ded
by [
Uni
vers
ity o
f M
isso
uri -
St L
ouis
] at
14:
08 0
1 O
ctob
er 2
013
behind in school work, becomes stressed, and then depressed because ofschool difficulties, it is obviously important to address her depressed mood.At the same time, the astute therapist also looks for ways to support readingskills. For such a patient, even psychoeducation about the interplay amongthese neurodevelopmental, medical, and emotional factors can be usefuland help to arrest her cycle of lowered functioning.
Another group that illustrates our model and is easily pushed into over-load with undiagnosed learning problems are pre-term or low weight ba-bies. Families of pre-term babies understandably are overjoyed that thechild survives, but because in some ways these children have alreadyexceeded expectations, neurodevelopmental cognitive problems maybe overlooked. Unfortunately, research shows higher risk for impairedbrain maturation in pre-term infants, and this is consistent with clinicallyobserved behavioral and educational problems (Peterson et al., 2000).Client Four illustrates how underlying vulnerabilities that are mostlikely related to pre-term status lead to significant learning and emo-tional difficulties.
90 WOMEN WITH VISIBLE AND INVISIBLE DISABILITIES
Normal agingFluctuating estrogen levels at perimenopause and menopause·Slower processing·
Silent learning
disorder
Deficit Medical problems
Stress
Reading·Non-verbal/Visual-Spatial·Organizational·
Hypertension·Diabetes·Lupus·Radiation/Chemotherapy·Surgery·Sleep Apnea·
FIGURE 2. From vulnerability to deficit: A model for silent learning disorders.The confluence of a silent learning disorder, normal aging, stress, and medicalproblems lead to more pronounced deficits and problems in functioning.
Dow
nloa
ded
by [
Uni
vers
ity o
f M
isso
uri -
St L
ouis
] at
14:
08 0
1 O
ctob
er 2
013

CLIENT EXAMPLE 4
AL presented for a neuropsychological consultation to determinewhether neurocognitive factors were contributing to her disablingdifficulties with anxiety and depression. She also reported long-standing difficulties with reading. During the interview, it becameapparent that although she was successful in her job, AL felt help-less and demoralized from years of difficulty with concentration,thinking, depression, and anxiety. Notably, AL was born two and ahalf months premature, and her mother smoked during the preg-nancy. AL’s difficult childhood included shyness, bedwetting, andexcessive worrying. As an adult, she had three inpatient psychiatrichospitalizations for depression. With great effort, she completedboth undergraduate and graduate degrees. Neuropsychological test-ing revealed that in addition to depression and anxiety, AL had asignificant neurodevelopmental learning disorder impacting atten-tion, organization of information, and regulation of affect. Testingfurther indicated both reading and mathematics disorders, in con-trast to her excellent intellect and strong verbal reasoning skills.
AL’s prematurity is hypothesized to have influenced success-ful brain organization, leading to significant frontal networkdeficits in attention and organization of information as well asstress, depression, and anxiety. Prior to her evaluation, AL had fo-cused more on the emotional aspects of her problems, with less ofan appreciation for the major impact of her pre-term birth.Reframing her difficulties in this way allowed her to go back totherapy with a different focus; there was grieving about the cir-cumstances of her birth to be done, but also less self-blame for herdifficulties. The evaluation further helped AL to commend herselffor her successes and better grasp how remarkable her educationalachievements were in light of her learning disorders.
STRATEGIES FOR DETECTINGAND TREATING SILENT LEARNING DISORDERS
Therapists can begin to address silent learning disorders by expand-ing the questions that are asked in a diagnostic interview (see Table 1).This includes addressing biological vulnerabilities such as “Were you abed wetter?” or “Did you have frequent ear infections in childhood?”Questions about early school experiences are particularly importantsuch as “Did you have difficulty with your handwriting?” or “Were you
Sara J. Hoffschmidt and Cheryl S. Weinstein 91
Dow
nloa
ded
by [
Uni
vers
ity o
f M
isso
uri -
St L
ouis
] at
14:
08 0
1 O
ctob
er 2
013

a slow reader?” Problems can emerge at different grade levels. For ex-ample, the 4th grade is often a time when students are first asked to bemore independent. During the seventh grade children with learningproblems often have more difficulties as they change classes and the or-ganization of a single classroom is removed. At the high school levelthe workload increases significantly and a foreign language might beintroduced. Standardized test scores such as the PSAT and SAT can beparticularly interesting measures to the clinician as an indication ofreading abilities under timed conditions.
We find it productive to ask about the process of selecting a college,and whether parents or siblings went to similarly competitive settings.Oftentimes asking specifically about each sibling and where they wentto school helps to contextualize the patient’s experience in the family,giving clues about the possible presence of an undetected learning dis-order. Another area of focus might be the transition to college, as a cli-ent with a silent learning disorder might report problems beginning incollege, particularly when the support of family is removed and they arefacing significantly less structure and less sleep.
Overall, a thorough intake interview and survey of symptoms high-lighting signs of problems in learning will help detect silent learningdisorders. This can be difficult for the therapist, particularly if the pa-
92 WOMEN WITH VISIBLE AND INVISIBLE DISABILITIES
TABLE 1. Areas that may signal silent learning disorders
Speech and language: Circumstantial, rambling, or disorganizedThinking: Perseverating, difficulty connecting thoughts, problems prioritizing informationAttention: Excessive daydreaming, difficulty doing two things simultaneously, distractibility,problems following directions, absentmindednessAcademic Skills: Poor reading, writing, spelling, and arithmetical skills, failure to achieve inschool and career at predicted levelsMotor Functions: Hyperactivity, unexplained tremor, fidgeting, writing that is micrographic,poorly formed, or fragmentedMemory: Cannot recall recent events, complaints about poor memory, difficulty following di-rections, poor performance after a work promotion requiring new learningVisual-spatial abilities: Gets lost, difficulty driving to new or familiar locations, poor manualskills, disorganized household and officeEmotions and Comportment: Apathy, irritability that is inappropriate to an incident, sociallearning problems and awkwardness, excessive shyness or a “loner,” difficulty understandinghumor and other social nuances
Source: Adapted from Howieson, D. B., & Lezak, M. D. (1992). The Neuropsychological Eval-uation, in S. C. Yudofsky & R. E. Hales (Eds.), American Psychiatric Textbook of Neuro-psychiatry, 2nd Edition (p.139). Washington, DC: American Psychiatric Press.
Dow
nloa
ded
by [
Uni
vers
ity o
f M
isso
uri -
St L
ouis
] at
14:
08 0
1 O
ctob
er 2
013

tient is focused on sharing painful experiences. Using a checklist suchas the Wender Utah Scale (Wender, Reimherr, & Wood, 1985) or theNeuropsychology Symptom Checklist (Schinka, 1986) can be helpfulto screen for learning problems. If a learning disorder is suspected, re-ferral for neuropsychological evaluation might help to clarify the natureand degree of neurocognitive or neurodevelopmental deficit. The refer-ral question also may include asking why a woman seems to be pushedinto “overload” at this particular time of her life.
CONCLUSIONS
In our experience conducting outpatient neuropsychological evalua-tions, women with silent learning disorders represent an often over-looked clinical population. Too often, women “work harder,” blamingthemselves and attempting to compensate for long-standing neuro-developmental problems. We have attempted to describe some in-stances in which silent learning disorders become more apparent aswomen develop and meet new challenges in school, at work, in the fam-ily, and with their health. Focusing on an interactive model, we pro-posed that neurocognitive vulnerabilities combined with life stressors,developmental milestones, normal aging, and medical problems mightmake it impossible for a woman to continue to cope as she is now trulyexperiencing deficits. We further suggested strategies for determiningwhether a complete neuropsychological evaluation can be helpful. It isour hope that incorporating awareness of silent learning disorders candramatically alter the range and effectiveness of treatment interven-tions, helping patients to work through shame about their difficulties to-ward greater self acceptance.
REFERENCES
Hechtman, L. (Ed.). (1996). Do they grow out of it? Long-term outcomes of childhooddisorders. Washington, DC: American Psychiatric Press, Inc.
Howieson, D. B., & Lezak, M. D. (1992). The Neuropsychological Evaluation, in S. C.Yudofsky & R. E. Hales (Eds.), American Psychiatric Textbook of Neuropsychiatry,2nd Edition (p. 139). Washington, DC: American Psychiatric Press.
Jordan, J., Kaplan, A., Miller, J., Stiver, I., & Surrey, J. (1991). Women’s Growth inConnection. New York: Guilford Press.
Sara J. Hoffschmidt and Cheryl S. Weinstein 93
Dow
nloa
ded
by [
Uni
vers
ity o
f M
isso
uri -
St L
ouis
] at
14:
08 0
1 O
ctob
er 2
013

Keenan, P. A., Ezzat, W. H., Ginsburg, K., & Moore, G. J. (2001, February).Prefrontal cortex as the site of estrogen’s effect on cognition. Poster session pre-sented at the bi-annual meeting of the International Neuropsychological Society,Chicago, IL.
Osterrieth, P. A. (1944). Le test de copie d’une figure complexe. Archives dePsychologie, 30, 206-356.
Peterson, B. S., Vohr, B., Staib, L. H., Cannistraci, C. J., Dolberg, A., Schneider, K. C.,Katz, K. H., Westerveld, M., Sparrow, S., Anderson, A. W., Duncan, C. C.,Makuch, R. W., Gore, J. C., & Ment, L. R. (2000). Regional brain volume abnor-malities and long-term cognitive outcome in pre-term infants. Journal of the Ameri-can Medical Association, 284, 1939-1947.
Sands, S., & Ratey, J. J. (1986). The concept of noise. Psychiatry, 49, 290-297.Schinka, J. A. (1986). The Neuropsychological Symptom Checklist. Odessa, FL: Psy-
chological Assessment Resources, Inc.Weinstein, C. S., Seidman, L. J., Feldman, J. J., & Ratey, J. (1991). Neurocognitive
disorders in psychiatry: A case example of diagnostic and treatment dilemmas. Psy-chiatry, 54, 65-75.
Wender, P. H., Reinherr, F. W., & Wood, D. (1985). A controlled study ofmethylphenidate in the treatment of attention deficit disorder, residual type, inadults. American Journal of Psychiatry, 142, 522-547.
94 WOMEN WITH VISIBLE AND INVISIBLE DISABILITIES
Dow
nloa
ded
by [
Uni
vers
ity o
f M
isso
uri -
St L
ouis
] at
14:
08 0
1 O
ctob
er 2
013