Embed Size (px)
Citation preview

11% of APLs in our series were CD56(+) by flow cytometry, which is comparable to data
reported in the literature (11-15%).
CD56 expression correlated with microgranular morphology and high WBC count, as
shown by other authors.
In contrast to a recent study, there was no association of CD56 expression with CD2,
CD7, CD15, CD34, CD117, or HLA-DR positivity. In addition, we did not find an association
with increased risk of relapse in CD56(+) APLs.
H. Olteanu, MD, PhD; A.M. Harrington, MD; S.H. Kroft, MD; *N.J. Karandikar, MD, PhD, and *F.F. Fuda, DO.
Departments of Pathology, Medical College of Wisconsin, Milwaukee, WI and *UT Southwestern Medical Center, Dallas, TX
The Incidence of CD56 Expression by Flow Cytometry in Acute Promyelocytic Leukemia
in Patients Treated with All-Trans Retinoic Acid and Anthracycline Drug Combinations
Conclusions
Introduction
Background: Recent cooperative studies have
linked CD56 positivity in acute promyelocytic
leukemia (APL) with an increased risk of relapse, and
with the presence of immaturity-associated and T-cell
antigens on leukemic promyelocytes. The drawbacks
of these multicenter studies are twofold: lack of
centralized immunophenotypic analysis prevented a
systematic standardization of flow cytometric results,
and a possible selection bias resulting from not all
centers assessing for CD56 expression. Because of
these confounding factors, we studied the expression
of CD56 by flow cytometry in APL with a rigorously
standardized flow cytometric protocol, and correlated
it with clinicopathologic parameters.
Design: 64 consecutive diagnostic APL bone
marrows or peripheral bloods were evaluated by 4-
color flow cytometry and cluster analysis, with
antibodies against CD2, CD3, CD4, CD5, CD7, CD8,
CD10, CD11b, CD13, CD15, CD16, CD19, CD20,
CD33, CD34, CD38, CD45, CD56, CD79a, CD117,
HLA-DR, MPO, and Tdt. An antigen was considered
positive in promyelocytes if >20% cells exceeded a
2% isotype control threshold. CD56 expression
status was correlated with clinical and pathologic
parameters.
Results: 7/64 APLs (11%) were CD56(+).
Comparative clinicopathologic parameters for all APL
cases, based on CD56 expression status, included
age, gender, morphology (microgranular vs.
granular), CBC data, cytogenetic and molecular
findings. A higher proportion of patients with CD56(+)
APL had microgranular morphology (p=0.027), and
they presented with a higher WBC count (p=0.003),
as compared to those with CD56(-) APL. There were
no other immunophenotypic differences between the
two groups.
Conclusion: 11% of APLs in our series are CD56(+)
by flow cytometry, which is comparable to data
reported in the literature (11-15%). CD56 expression
correlated with microgranular morphology and high
WBC count, as shown by other authors. In contrast
to a recent study, there was no association of CD56
expression with CD2, CD7, CD15, CD34, CD117, or
HLA-DR positivity.
Abstract
Materials and Methods
Acute promyelocytic leukemia (APL) is a specific subtype of acute myeloid leukemia
(AML) characterized by distinct morphologic, immunophenotypic, cytogenetic, and
clinical features. The unique chromosomal abnormality, t(15;17), results in the
formation of the PML/RARalpha fusion protein and a subsequent block in
granulocytic differentiation. Clinically, this blockade can be overcome by
pharmacologic doses of all-trans retinoic acid (ATRA), which may also ameliorate the
severe bleeding diathesis that is frequently associated with APL. The combination of
ATRA and chemotherapy as frontline therapy has dramatically improved the outcome
of the disease, so that most patients treated with this regimen are expected to
become long-term survivors. However, as a result of early hemorrhagic death and
early disease relapse, treatment failure is still recorded in 5-30% of patients with APL.
It is therefore useful to identify prognostic markers that are associated with these
adverse events. Of the prognostic factors that may predict for an inferior outcome in
APL, older age, high initial leukocyte count, and low platelet count have been
associated with increased relapse risk. More recent reports have demonstrated that
the expression of CD56 was associated with an unfavorable clinical outcome.
CD56 is an isoform of the neural cell adhesion molecule (NCAM) involved in cell-to-
cell interaction; it also may function in cell-mediated cytotoxicity. This antigen is
normally expressed in NK cells and a subset of cytotoxic T cells, and has been also
detected in various hematopoietic neoplasms. Recent studies have linked CD56
positivity in APL with an increased risk of relapse, and with the presence of
immaturity-associated and T-cell antigens on leukemic promyelocytes. The
drawbacks of these multicenter studies are twofold: lack of centralized
immunophenotypic analysis prevented a systematic standardization of flow
cytometric results, and a possible selection bias resulting from not all centers
assessing for CD56 expression. Because of these confounding factors, we studied
the expression of CD56 by flow cytometry in APL with a rigorously standardized flow
cytometric protocol, and correlated it with clinicopathologic parameters.
64 patients with APL from the Medical College of Wisconsin and UT Southwestern
Medical Center, that had flow cytometry (FC) data available for review were included
in the study.
Four-color FC was performed with antibodies against CD2, CD3, CD4, CD5, CD7,
CD8, CD10, CD11b, CD13, CD15, CD16, CD19, CD20, CD33, CD34, CD38, CD45,
CD56, CD79a, CD117, HLA-DR, MPO, and Tdt. Positivity for an antigen was defined
as at least 20% of events beyond a 2% isotype control threshold.
Clinical and laboratory data was available from chart review.
Results
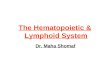
Figure 1. Immunophenotypic findings in a patient with CD56(+) acute promyelocytic
leukemia. Neoplastic promyelocytes are in red, normal T cells are in green, B cells are in
blue, plasma cells are in yellow, and NK cells are in violet.
7/64 APLs (11%) were CD56(+).
Comparative clinicopathologic parameters for all APL cases, based on CD56
expression status, are presented in Table 1. A higher proportion of patients with
CD56(+) APL had microgranular morphology (p=0.027), and presented with a higher
WBC count (p=0.003), as compared to those with CD56(-) APL .
There were no other differences, including immunophenotypic features, between
the two groups.
Table 1. Comparison of clinical and laboratory findings in patients
with acute promyelocytic leukemia (APL), separated based on
CD56 expression status.
Parameter CD56(-) CD56(+) p
n (%), APL 57 (89%) 7 (11%)
Age, median, (range) 42 (20-93) 46 (25-88) 0.941
Age, ≥ 65 years 14.0% 14.3% 1.000
M:F 24:33 2:5 0.695
Microgranular 15.8% 57.1% 0.027
WBC, x10e3/uL,
median, (range)
2.9
(0.43 – 126.8)
54.9
(2.9 – 107.0) 0.003
Hgb, g/dL, median,
(range)
9.7
(5.8 – 14.6)
9.6
(4.8 – 12.0) 0.926
Platelets, x10e3/uL,
median,(range)
27
(3 – 245)
73
(17 – 280) 0.135
DIC 56.1% 42.9% 0.687
Complex cytogenetics 33.6% 14.3% 0.409
Relapse rate 9.6% 14.3% 0.548
Immunophenotype
CD2(+) 41.8% 42.9% 1.000
CD4(+) 14.0% 28.6% 0.299
CD7(+) 7.0% 0% 1.000
CD10(+) 0% 0% 1.000
CD13(+) 98.2% 100% 1.000
CD14(+) 0% 0% 1.000
CD15(+) 87.7% 71.4% 0.253
CD33(+) 98.2% 100% 1.000
CD34(+) 33.3% 57.1% 0.239
CD38(+) 94.7% 100% 1.000
CD45(+) 100% 100% 1.000
CD64(+) 57.9% 71.4% 0.691
CD117(+) 97.8% 100% 1.000
HLA-DR(+) 10.5% 14.3% 0.574
MPO(+) 100% 100% 1.000
Tdt(+) 4.9% 14.3% 0.335