Embed Size (px)
Citation preview
Orthodontics
The importance of the seated condylar positionin orthodontic correctionFrank E. Cordray, DDS, MS'
It has been proposed that the discrepancy between the seated and unseated condyiar position be identi-fied and eliminated when the ooolusion is reorganized. Identification ot this discrepancy is most accuratelyaccomplished through the use ol diagnostic casts that haue been taken trom a deprogrammed patient andmounted in the seated condylar position on a se m i adjustable articulator through an estimated facebowtransler. The amount and direction ol any discrepancy is determined three dimensionally with condylarposition instrumentation, (Quintessence int 2002:33:284-293)
Key words: articulator, oondylar dispiacement, condylar distraction, orthodontics, seated condyiar
position, unseated condyiar position
Aprevious article outlined steps that orthodontistsmust take to advance the specialty into the new
millennium';
1. Specific, comprehensive, and universal treatmentgoals must be developed.
2. Occlusion, temporomandibular joint function,facial esthetics, and periodontics must receivegreater emphasis in graduate orthodontic programs.
3. The quality of orthodontic records must beupgraded to include diagnostic study casts mountedin the seated condylar position.
4. A comprehensive orthodontic classification systemmust be developed.
5. Orthodontic diagnosis must become more accurate.6. Orthodontic treatment time must be minimized.
These issues constitute the foundation for state-of-the-arf orthodontic treatment in the 21st century,which will include the following:
1. The use of a repositioning splint to ehminate mus-cle symptoms and attain a comfortable, stable, andrepeatable seated condylar position
2. Instrumental anaiysis of diagnostic study casts:mounting of diagnostic study casts in the seatedcondylar position on a semiadjustable articulatorthrough the use of af least an estimated facebowtransfer
'Assistant Cliriical Proiessoi, Department of Orthodonlics, Ohio SlateUniversity, Colurrbus, Ohio,
Reprinl requesis: Dr Frank E. Cordray, 96 Northwoods Boulevard, Worth-irglon, Ohio 43235. E-mail: [email protected]
Presented at the 100th Annual Session of the Arrerican Association ofOrlhodontists, Chicago, May 2000.
3. Measurements of jaw deflections caused by tooth-dictated positions (currently measurahle with theCondylar Path Indicator [CPI] [Panadent], theIVIandibular Position Indicator [MPI] [SAM], andCranio-Mandibular Fosition [CMF] [Denar]instrumentation)
4. Computer-assisted treatment planning, includingcorrected cephalometrics (conversion of lateralcephalograms from maximum intercuspation-centric occlusion (IVIIC-CO) to the seated condylarposition); comptiterized cephaiometric analysescorrected for jaw deflections; computerized growthdeterminations; and computer-aided treatmentforecasts (Visualized Treatment Objectives [VTOs])
5. Video imaging as an aid to optimizing dental, skele-tal, and soft tissue esthetics
Howaf et aP have stated, "Orthodontic assessment ofpatients has evolved as treatment goals have changed,"which ieads to the discussion of a fundamental aspect oforthodontic treatment: What are the goals of orthodonticcorrection? Ultimately it comes down to clinical results.Two overriding concerns for those delivering orthodonticcare are improved esthetics (facial and dental) andincreased longevity of the dentition and associated stmc-tures (periodontium and temporomandihular joints).
How are these goals accomplished? Consistentlyexcellent resuits are achieved by the application cfsophisticated treatment goals and utilization of asophisticated appliance system. Two areas of primeimportance for both the practitioner (from a practicemanagement standpoint) and the patient (from a satis-faction standpoint} are satisfying the patient's chiefconcern and treating the patient in the shortest timepossible, to achieve the desired result.
284
Cordray •
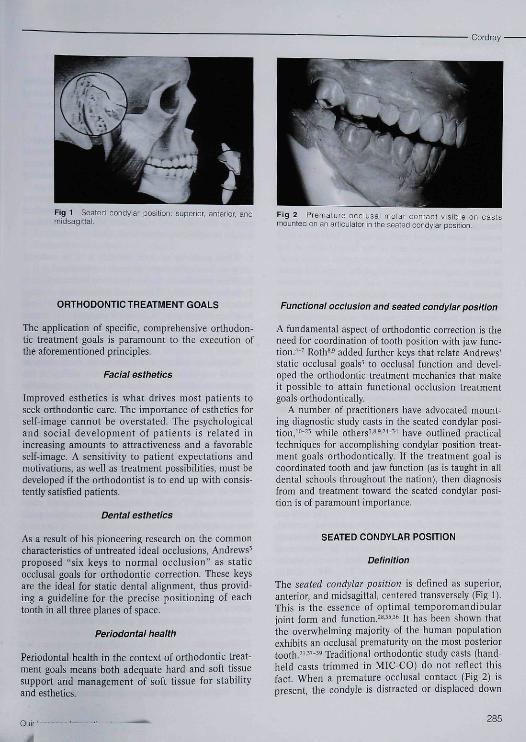
Fig 1 Seated condyiar position, superior, anterior, andmidsagittai
Fig 2 Prematuie occlusai molar contact visible on castsmounted on an articulator in the seated condylar position.
ORTHODONTIC TREATMENT GOALS
The application of specific, comprehensive orthodon-tic treatment goals is paramount to the execution ofthe aforementioned principles.
Facial esthetics
Improved esthetics is what drives most patients toseek orthodontic care. The importance of esthetics forself-image cannot be overstated. The psychologicaland social development of patients is related inincreasing amounts to attractiveness and a favorableself-image. A sensitivity to patient expectations andmotivations, as well as treatment possibilities, must bedeveloped if the orthodontist is to end up with consis-tently satisfied patients.
Dental esthetics
As a result of his pioneering research on the commoncharacteristics of untreated ideal occlusions, Andrews'proposed "six keys to normal occlusion" as staticocclusal goals for orthodontic correction. These keysare the ideal for static dental alignment, thus provid-ing a guideline for the precise positioning of eachtooth in all three planes of space,
Periodontai health
Periodontal health in the context of orthodontic treat-ment goals means both adequate hard and soft tissuesupport and management of soft tissue for stabilityand esthetics.
Functional occlusion and seated condyiar position
A fundamental aspect of orthodontic correction is theneed for coordination of tooth position with jaw func-tion.''-' Roth*' added further keys that relate Andrews'static occlusal goals^ to occlusal function and devel-oped the orthodontic treatment mechanics that makeit possible to attain functional occlusion treatmentgoals orthodontically.
A number of practitioners have advocated mount-ing diagnostic study casts in the seated condylar posi-tion,'"-" while others " - "- " have outlined practicaltechniques for accomplishing condylar position treat-ment goals orthodontically. If the treatment goal iscoordinated tooth and jaw function (as is taught in alldentai schools throughout the nation), then diagnosisfrom and treatment toward the seated condylar posi-tion is of paramount importance.
SEATED CONDYLAR POSITION
Definition
The seated condylar position is defined as superior,anterior, and midsagittai, centered transversely (Fig I).This is the essence of optimal temporomandibularjoint form and function. *"-'*' It has been shown thatthe overwhelming majority of the human populationexhibits an occlusal prematurity on the most posteriortooth. '•"" ' Traditional orthodontic study casts (hand-held casts trimmed in MIC-CO) do not reflect thisfact. When a premature occlusal contact (Fig 2) ispresent, the condyle is distracted or displaced down
Quir-285
• Cordray
and away from the optimal seated position, in order tointercuspate the teeth into MIC-CO {the occlusion-dictated condylar position),
Condylar dhti-action or displacement is defined asthe difference in condylar position between the seatedand unseated (occlusion-dictated) positions (the posi-tion of the condyle caused hy intercuspation of theteeth). Most condylar displacements arc vertical dis-placements, not horizontal displacements, because thecondyle drops inferiorly in the fossa as the mandibleshifts superiorly in the region of the incisors.
Measurement techniques
Previous attempts to measure the seated condyiarposition have utilized methods such as intraoral visualestimation,'"' measurement of the hit-and-slide at theocclusal level,"" radiographs (panoramic, transcranial,or lateral cephalometric radiography, corrected tomo-graphy, and arthrography),-' and magnetic resonanceimaging or computed tomography scans,-'' However,these do not allow measurement of the mandibularfunctional shift from the unseated (occlusion-dictated)condylar position to the seated condylar position in alltiiree planes of space to 0,2 mm. In fact, it has beenshown that condylar position cannot be accuratelydetermined radiographi cal ly,•'•'"" The new gold stan-dard for the measurement of condylar position wasproposed hy the author in 1997,*'' Only three-dimen-sional condylar graph measurements made from artic-ulated study casts that have heen mounted in theseated condylar position from a deprogrammedpatient will yield this information.
Identification of the discrepancy between the seatedand unseated (occlusion-dictated) condylar position ismost accurately accomplished with diagnostic studycasts taken from a deprogrammed patient; these castsmust be mounted in the seated condylar position on asemiadjustablc articulator through the use of at leastan estimated facebow transfer, ""'-'*'-*'*-* The amount(millimeters) and direction (anteroposterior, vertical,and transverse) of any discrepancy between the seatedand unseated condylar position can he determinedwith ease through the use of condylar position instru-mentation available today {CPI; MPI; CMP;Verichcck, Denar; modified Buhnergraph, Whip Mix).
Advantages and indications
The condylar graph measurement technique has anumber of advantages:
1, It is simple and easy to perform,2, It is available to every dental practitioner,3, It is inexpensive (the most cost-effective method
available to determine condylar position),4. It is noninvasive,5, It is highly accurate (the most accurate method for
determining condylar position in all three planes ofspace to within 0,2 mm anteroposteriorly and verti-cally and 0,1 mm transversally).
The seated condylar position is a three-dimen-sional entity that must be assessed with a three-dimensional measuring device. This is a much moresophisticated and accurate method for measuringcondylar position, '' ''' ''' -'-"
Howat et aF have stated that the discrepancybetween the seated and unseated condylar positionmust he identified and eliminated when the occlusionis to he reorganized, which is required:
1, When posterior occlusal stability is to be restoredby occlusal adjustment or tooth restoration,
2, When mandibular dysfunction is to be treated.3, Before placement of multiunit restorations,4, Before fabrication of complete dentures,5, When orthodontic treatment is planned,6, When the condyle is to be positioned during
orthognathic surgery.
Success or failure of treatment in each of theseareas is completely dependent on the ability of theoperator to attain a comfortahie, stable, repeatahleseated condylar position as a reference point.
Importance to orthodontic correction
The importance of the seated condylar position inorthodontic correction is as follows: orthodontics pro-vides the ability to move every tooth in all threeplanes of space, making orthodontic treatment compa-rable to complete-mouth restoration or a completedenture setup,"*™ Thus it is imperative to have a com-fortable, stable, and repeatable seated condylar posi-tion to work from.
It has been asserted that in 25% to 30"/o of ortho-dontic cases the decision-making process would beaffected hy an articulator mounting in the seatedcondylar position, because of the presence of a signifi-cant condylar distraction,^"-" However, the clinicalexperience of the author is that this informationaffects every orthodontic case that is treated. Sevenimportant decision-making areas are affected:
1, Diagnosis:a. Magnitude (mm) of the horizontal discrepancy
(Class II, Class III) tobe correctedb. Magnitude (mm) of the vertical discrepancy
(open bite, deep bite) to be corrected
286
Cordray •
C, Magnitude (mm) of the transverse diserepancy tobe corrected
d. Direction of mandibular growthe. Direction of tiiandibular rotation anticipated
with treatment2, Treatment planning;
a. Extraction versus nonextractiortb, Nonsurgical versus surgical treattnent
3, Anchorage requirements (minimum, moderate, ormaximum)
4, Treatment mecbanics (dictated by all of the above,especially the diagnosis and anchorage require-ments)
5, Occlusal finishing (arch coordination in all threeplanes of space)
6, Evaluation of orthodontic treatment effects1. Evaluation of orthodontic relapse
It is faster, easier, less expensive, and tnore accurateto mount diagnostic study casts in the seated condylarposition than to trim them in MIC-CO (habitual posi-tion), -'• •'•' Diagnostic accuracy is increased becausemuscle splinting is eliminated. Muscle spiinting is partof the neurotnuscular protective mechanism and pos-tures the mandible into the best tooth fit. It does notallow the operator to detect the discrepancy betweenthe seated and unseated condylar position clinically atthe chairside wben manipulating tbe jaw. Musclesplinting may disappear during orthodontic treatment,allowing the mandible to drop back, revealing a largerdiscrepancy tban at the start of treatment (dual bite).
The problem hes in tbe fact tbat the effect of mus-cle splinting is not detectable clinically."-'-'^"
Because tbe neuromusculature is programmed toclose tbe mandible into tbe best tootb fit, it is difficultto identify tbe seated condylar position throughclinical evaluation or mandibular manipulation alone.Patients avoid interferences and occlude into the besttootb fit, even at the expense of the joints. Occlusaldisbarmonies cannot be studied (or even consistentlydetected) in tbe functioning moutb because tbe mus-cles and nerve reflexes protect tbe teetb by overridingthe joint's guidance,
Neuromuscular deprogramming is the key toreproducibility.'"'^^""-^^'*-^^ Witbout deprogram-ming, it is highly unlikely tbat the seated condylarposition will be captured clinically, Tberefore what isseen in the mouth may not be wbat is really beingtreated.'- '' ' ""' «'' ^-' ' ''' '*'-^^ When indicated, a repo-sitioning splint is an extremely valuable, reversible,and conservative appliance tbat aids in tbe therapeu-tic, diagnostic, and treatment planning phases ofortbodontic correction,326.3i).6o,í3-99
This infortnation directly affects cephaiometricevaluations as well. First, a significant condylar dis-
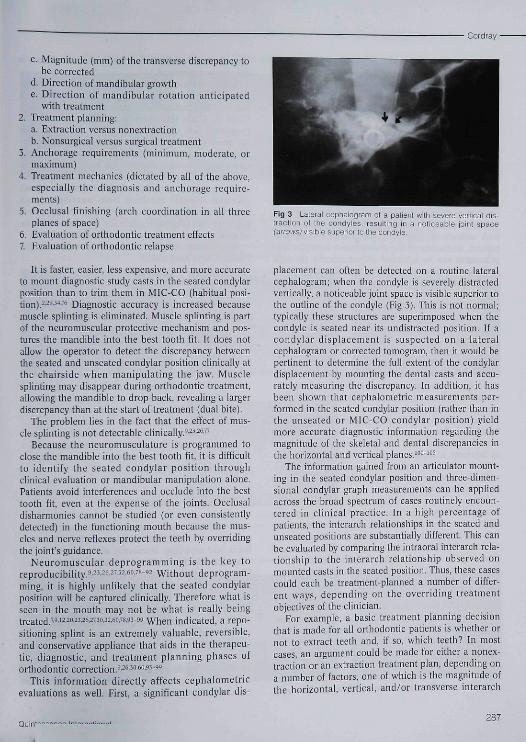
Fig 3 Lateral cephalogram of a patient witti severe veiticai UIK-traction of ttie condyles. resulting in a notioeable joint space("arraWE,) visible superior to ttie condyie.
placement can often be detected on a routine lateralcepbaiogram; wben tbe condyie is severely distractedvertically, a noticeable joint space is visible superior tothe outline of the condyie (Fig 3). This is not normal;typically tbese structures are superimposed when thecondyie is seated near its undistracted position. If acondylar displacement is suspected on a lateraleephalogratii or corrected tomogram, then it would bepertinent to determine the fuil extent of the condylardisplacement by mounting the dental casts and accu-rately measuring the discrepancy. In addition, it hasbeen sbown that cepbalometric measurements per-formed in the seated condylar position (rather than inthe unseated or MIC-CO condylar position) yieldmore accurate diagnostic information regarding themagnitude of the skeletal and dental discrepancies inthe horizontal and vertical plan es,'"""'"^
The information gained from an articulator mount-ing in the seated condylar position and three-dimen-sional condylar graph measurements can be appliedacross tbe broad spectrum of cases routinely encoun-tered in clinicai practice. In a high percentage ofpatients, tbe interarcb relationships in the seated andunseated positions are substantially different. Tbis canbe evaluated by comparing the intraorai interarcb rela-tionsbip to the interarch relationship observed onmounted casts in tbe seated position. Tbus, these casescould each be treatment-planned a number of differ-ent ways, depending on tbe overriding treatrnentobjectives of the clitiieian.
For example, a basic treatment planning decisionthat is tTiade for all orthodontic patients is whether ornot to extract teeth and, if so, which teetb? In mosteases, an argument could be made for cither a nonex-traction or an extraction treatmetit plan, depending ona number of factors, one of wbicb is the magnitude oftbe borizontal, vertical, and/or transverse interarch
Quin'-287
• Cordray
discrepancy present, Tbis information is preciselyrevealed hy an articulator mounting in tbe seatedcondylar position. In addition, an articulator mount-ing may reveai an interarch discrepancy that may havea surgical treatment option as well as conventionalorthodontic treatment options.
Furthermore, the anchorage requirements andchoice of treatment mechanics is directiy affected,depending on the magnitude of the horizontal or verti-cal interarch discrepancy present pretreatment, whichis precisely revealed by an articulator mounting in theseated condylar position. However, the treatmentplanning and mechanÍL;al choices are limited if theoverriding treatment objective is to reduce the pre-treatment condylar displacement. Seating the condylewith orthodontic correction requires precise verticalcontrol. Reduction of the pretreatment condylar dis-placement can be achieved orthodontically throughthe use of various treatment methods (extraction,nonextraction, high-pull facehow, transpalatal bars,bite blocks, elastics, mounted tooth positioner, splintwear, orthognathic surgery, and equiiibration),
Occlusal flnishing can be more accurately accom-plished if the pre-dcband casts are first mounted in theseated condylar position. The mounting is then used intwo ways. First, it is used to assess the interarch rela-tionships near the end of treatment, allowing the clini-cian to adjust tooth positioning as needed (anteropos-teriorly, vertically, or transversaily). Often thismounting wiil reveal either posterior torque deficien-cies or transverse arch discrepancies (inclined planecontacts or arch coordination problems) that have tobe addressed to gain posterior intercuspation withoutcondylar displacement. Second, the mounting is usedto fabricate a tooth positioner from an ideal setupwith the condyle seated. The positioner is used tomaintain condylar seating while settling of the denti-tion is controlled vertically.
Moreover, the seated condylar position is thebenchmark from which true comparisons of treatmenteffectiveness (both skeletal and dental) can be made.It is the only valid reference point for comparison oftreatment effects in orthodontics. The unseated(occlusion-dictated) condylar position (condylar posi-tion in iVIIC-CO) bas inherent error as a referencepoint because of tbe lack of understanding of the mag-nitude of the mandibular functional shift (hit andslide) present before and after treatment. Failure tounderstand this principle has been the source of greatconfusion, misunderstanding, and miscommunicationin hoth dentistry in general and orthodontics in partic-ular, "'" To obtain precise measurements of the skele-tal and dental changes witb treatment, it is essential tobegin with a stable, repeatable condylar position andend with a stable, repeatable condylar position and
then assess the result. This Is how treatment efficacy isaccurately determined.
In the evaluation of orthodontic relapse, certainphenomena such as dual bites (both vertically andhorizontally), relapse of horizontal (anteroposterior:Class II, Class III) correction, relapse of vertical(superoinferior: open bite, deep bite) correction, andthe development of symptoms of temporomandibulardysfunction after orthodontic correction have previ-ously been explained as dental compensations toorthodontic corrections. However, it is now under-stood that they are often skeletal compensations(skeletal relapse) resulting from treatment to anunseated condylar position. '""^^- ''' "' ''-*''"' Thus it isapparent that diagnostic accuracy is enhanced hy anarticulator mounting in the seated condylar position.
This concept is further reinforced by Ackerman andProffit,'"' who have stated:
It is clear that the condyles should not be dis-placed during treatment by more than a smalldistance from their relaxed (retruded) position.In addition to the possibility of TMD symptoms,treatment methods that reposition the mandiblemore than a small amount are likely to fail in thelong run due to the musculature returning themandible to a seated condylar position. Whenthis occurs after treatment it is perceived asrelapse. ("The boundaries of dental compensa-tion for an underlying jaw discrepancy are estab-lished by,,,tbe neuromuscular influence onmandihuiar position.") Neuromuscular harmonyis at risk when the condyles are not within 1 mmor so of a seated position when the teeth are inMIC. This is an important soft tissue limitationon orthodontic treatment.
CASE REPORT
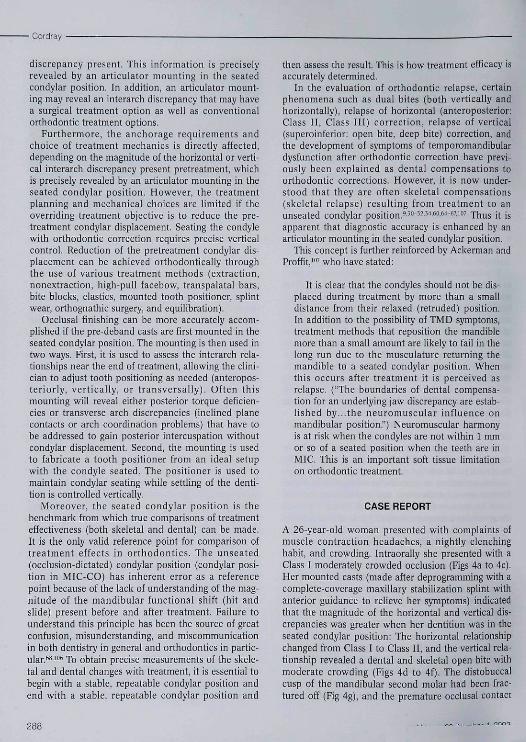
A 26-year-old woman presented with complaints ofmuscle contraction headaches, a nightly clenchinghabit, and crowding. Intraorally she presented with aCiass I moderately crowded occlusion (Figs 4a to 4c),Her mounted casts (made after deprogramming with acomplete-coverage maxillary stabilization splint withanterior guidance to relieve her symptoms) indicatedthat the magnitude of the horizontal and vertical dis-crepancies was greater when her dentition was in theseated condyiar position; Tbe horizontal relationshipchanged from Class I to Class II, and the vertical rela-tionship revealed a dental and skeletal open bite withmoderate crowding (Figs 4d to 4f), The distobuccalcusp of the mandibular second molar had been frac-tured off (Fig 4g), and tbe premature occlusal contact
288
Cordray •
Figs 4a ío 4c Pretreatment inlraorai views ol Ihe patient in maximum inlercuspalion-centric occlusion.
Fig 4a Fig 4b Fig 4c
Figs 4d to 4f Pretreatment casts mounted in the seated condylar position (afler ihe patient hadbeen deprogrammed with a complete-coverage maxillary stabilization splint with anterior guidanceto relieve her symptoms). Note the premature contacts on itie mandibular left molars, the fractureddistobuccal cusp oí the mandibular leít second molar, and the increased magnitude ot the horizontal(Class 11] and vertical (open bite) interarcli discrepancies
Fig4d Fig4e Fig4f
Fig 4g Fractured rjisiobuccal cusp of themandibular letl second moiar (arrow).
Figs 4h to 4¡ PI•osttreatment intraoral .-lews ol the patient m maximum intercuspation-<;entric occlusion
Fig4h
Ou"
Fig4iFig4i
289
• Cordray
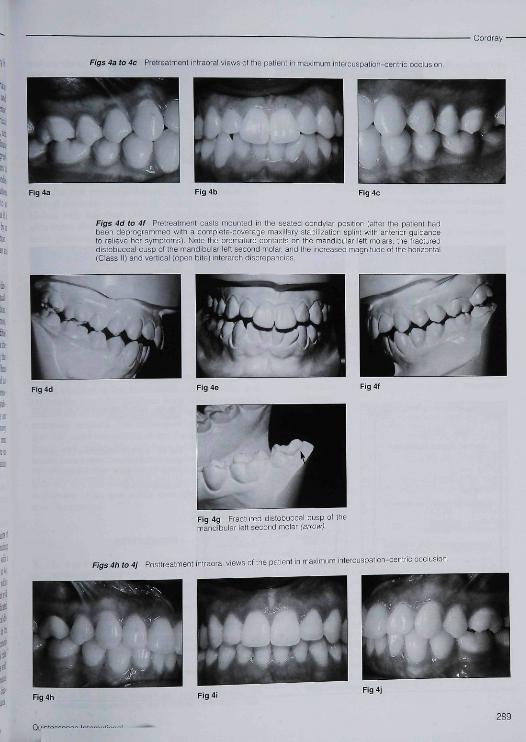
Figs 4k and 41 Püsttreatment intraorai views of iaterai excursions, demonstiating theachievement of a mutualiy protected oociusion with canine guidance.
Figs 4m to 4o Postfreatment casts mounted in the seated condylar position. Note the reduction ofthe horizontal and vertical interarch discrepancies.
Fig 4m Fig4n Fig4o
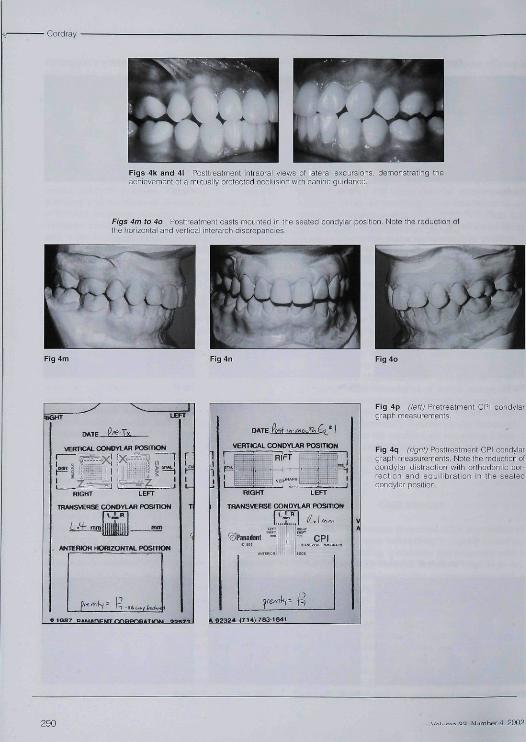
VERTICAL CONOVIAR POSITtON
IRIWSVEflSE CONDYLAf) POSITION
ANTERIOR HOKOONJtí POSmON
VERTICAL CONDYLAR POSITION
RIFT
TRANSVERSE CONDYIAR POSITIONI L < R I J, ,
OPanaJent CPI
Fig 4p (ieñ) Pretreatment CPI condylargraphmeasurements.
Fig 4q irÍQÍ~\i) Posttreatment CPI condylargraph measurements. Note the reduction oícondylar distraction with orthodontic cor-rection and equilibration in the seatedcondyiar position
290
Cordray •
was on these same mandibular second molars. Thegoal of orthodontic correction in this case was to gainideal alignment and occlusal interdigitation while atthe same time decreasing the condylar distraction towithin normal limits (within 1 mm of the seatedcondylar position).
Treatment included extraction of four second pre-molars (to decrease the vertical dimension of occlu-sion) instead of four first premolars; thus, the treat-ment mechanics and anchorage requirements for thispatient were substantially different (moderate to maxi-mum for first premolar extractions and minimum forsecond premolar extractions). Finishing was accom-plished with full-sized (21 x 25) braided rectangulararch wires, short vertical (Class II) elastics, a mountedtooth positioner, and complete-mouth equilibration.The symptoms were eliminated while function andesthetics were improved; total treatment time was 26months (Figs 4h to 4o), The pretreatment and post-treatment CPI recordings are shown in Figs 4p and4q; the pretreatment condylar distraction or displace-ment has been reduced by ortbodontic correction andcomplete-mouth equilibration.
CONCLUSION
It has heen shown in all areas of dentistry that theseated position is the most stähle, comfortable, andrepeatable condylar position from which extensiverestoration of the dentition should be diagnosed andtreatment planned. The techniques and instrumenta-tion that make assessment of this position possible aresimple and predictable and have proven to be faster,easier, less expensive, and more accurate than tradi-tional orthodontic diagnostic techniques. Diagnosticaccuracy and treatment execution are enhanced by theavailability of an articulator mounting in the seatedcondyiar position.
REFERENCES
1, Cordray FE, A crisis in orthodontics? It's time to iookwithin. Am J Onhod 1992:101:472-476,
2, Howat AP, Capp N], Barrett NV\. A color atlas of occiu-sion and malocclusion, St Louis: Mosby, 1991,
3, Andrews LF. The six keys to normal occlusion. Am ]Orthod 1972;63:296-309.
4, Thompson JR, Function-The neglected phase of ortho-dontics. Angle Orthod 1956;26:!29-143.
5, Perry HT Mandibular function: An orthodontic responsi-bility AmJ Orthod 1975 ;67:317-323.
6, Perry HT Temporomandibtilar joint and occiusion. AngleOrthod 1976:46:284-293,
7 Parker WS, Centric reiation and centric occiusion-Anorthodontic responsibiiity. Am J Orthod 1978;74:481-500,
8. Rulli KH. Functional occiusioii for the orthodontisL | ClinOrthod 1981;15:1-8C,
9. Rolh RH, The maintenance system and occlusai dynamics.Dent Ciin North Am 1976:20:751-788.
10, Roth RH, Temporomandihular pain-dysfunction andocciusal relationships. Angle Orthod 1973;43;136-153,
11, Williamson EH, Occlusion and temporomandibular iointdysfunction. [ Clin Orthod 1981;15:333-350.
12, Williamson EH. The role of craniomaiîdibular dysfunctionin orthodontic diagnosis and treatment planning. DentClin North Am 1983:27:541-560.
13, Posselt V. Physiology of occlusion and rehabilitation, ed 2.Oxford, England: Elackwell Seientiric,1968,
14, Ackerman |L, Proffit WR, The characteristics of malocclu-sion: A modern approach of classification and diagnosis.Am J Orthod 1969;56:443-454.
15, Proffit WR. Contemporary Orthodontics, Si Louis: Mosby,1986,
16, Wood DP, Elliott RW, Reproducibility of the centric rela-tion bite registration technique. Angle Orthod 1994;64:211-221.
17, Timm TA, Herremans EL, Ash MM, Occlusion and ortho-dontics. Am I Orthod 1976,70.138-145,
18, Aubrey RB. Occlusal objectives in orthodontic treatment.Am ) Orthod 1978;74:162-175,
19, Moffett BC A biologic consideration of centric relationbased on skeletal and connective tissue responses. In:Celenza FV, Nasedkin JN (eds). Occlusion: The State ofthe Art. Chicago: Quintessence, 1978:13-18,
20, Gilboe DB. Centric relation as the treatment position,I Prosthet Dent 1983:53:685-689,
21, Ramtiord SP, Ash MM (eds). Occlusion, ed 3, Philadelphia:Saunders, 1983.
22, Wood GN, Centrie relation as the treatment position inrehabihtating occlusions: A physiologic approach. 2. Thetreatment position. J Prosthet Dent 1988:60:8-15.
23, Limdeen H, Centric relation reeords-Tlie effects of mus-cle action. I Prosthet Dent 1972:31:244-251.
24, Stuart CE, Good occlusion for natural teeth, J ProsthetDentl964;14:716-724.
25, Williamson EH, Steinke RM, Morse PK, Swift TR, Centricrelation: A comparison of muscle-determined position andoperator guidance. Am | Orthod 1980:77:133-145,
26, Coulson R. Should fhe phenomena of muscle splinting beruled out prior to maliing an orthodontic diagnosis?Annual Session of the American Association ofOrthodontists, St Louis: May 5, 1992,
27 Crawford S. The relationship hetween condylar axis posi-tion as determined by the occlusion and measured by theCPI instrument and signs and symptoms of temporo-mandibular joint dysfunction. Angle Orthod 1999;69:102-116,
28, OifesonJP. Management of Temporomandibular Disordersand Occlusion, ed 3, St Louis: Mosby, 1985.
29, Bennett JC. McLaughlin RP, Orthodontic management ofthe dentition with the prc-adjusted appliance, Oxford,England: Isis Medical Media,1997,
30 Dawson PE. Evaluation, diagnosis, and treatment ofocclusal problems. St Louis: Mosby, 1989:28-33,590-591,
31 Guichet NF, Applied gnathology: Why and how. ]Amglocont Dent Soc 1972;26:14-19.
291
• Cord ray
32. Huffman RW, Régenos |W Principles of Occlusion,Columbus, OH; Hand R Press, 1978.
33. Slavicek R]. Clinical and instrumental functional analysisfor diagnosis and treatment planning, 1, J Clin Orthod1988;22:358-370.
34. Slavicek R), Clinical and instrumental futictional analysisfor diagnosis and treatment planning. 4, Instrumentalanalysis of mandibular casts using the MandibularPosition Indicator. ) Clin Orthod 1988;22;566-575,
35. Sicher H. Oral Anatomy, ed 4. St Louis: Mosby, 1965.
36. Hylander WL. Functional anatomy. In; Sarnat BG, LaskinDM (eds). The Temporomandibuiar joint. Springfield, IL'Thomas, 1979.
37. Ingervall B. Tooth contacts on the functional and non-functional side in children and young adults. Arch OralBiol 1972;17(l);191-200.
38. Agerberg G, Santstorm R, Frequency of occlusal interfer-ences; A clinical study in teenagers and young adults.J Prostbet Dent 1988:39:212-217.
39. deLaat A, van Steenberghe D. Occlusal relationships andtemporomandibuiar joint dysfunction. 1 Epidemiologicalfindings, J Prosthet Dent 1985;54;S35-842.
40. Magnusson T, Carlsson GE, Occlusal adjustment inpatients with residual or recurrent signs of mandibulardysfunction. ] Prosthet Dent 1983;49;706-710.
4L Johnston LE, Hoffman R. Gnathologic assessment of cen-tric slides in post-retenti on orthodontic patients. J ProsthetDent 1988:60:712-715.
42. Mohl ND. Reliability and validity of diagnostie modalitiesfor temporomandibuiar disorders. Adv Dent Res 1993;7;113-119.
43. Alexander SR, Moore RN, Dubois LM. Mandibularcondyie position: Comparison of articulator mountingsand magnetic resonance imaging. Am J Orthod 1993;104:230-239.
44. Blaschke DD, Blasehke TJ. Normal temporomandibularjoint bony relationships in eentric occlusions, J Dent Res1981:60 ;98-104.
45. Katzberg RW, Keith DA, Ten Eik WR. Guralnik WC.Internal derangements of the temporomandibuiar joint:An assessment of condylar position in centric occlusion.J ProsthKt Dent 1983;49;250-254,
46. Dixon DC, Graham GS, Mayhew RB, The validity of tran-scranial radiology in diagnosing temporomandibuiar jointanterior disc displacement. J Am Dent Assoc 1984:108;615-618,
47. Aquilino SA. Matteson SR, Holland GA. Phillips C.Evaluation of condylar position from temporomandibuiarjoint radiography. J Prosthet Dent 1985:53;88-97,
48. Pullinger AG, Holländer L, Solberg WK, Petersson A.A tomographic study of mandibular condyie position in anasymptomatic population. J Prosthet Dent 1985:53;706-713.
49. Pullinger AG, Solberg WK, Hollender L, Guichet D,Tomographic condyie position in diagnostic subgroups ofTMD. J Prostbet Dent 1986:55:723-729.
50. Bean LR, Thomas CA. Significance of condylar positionsin patients with temporomandibuiar disorders. I Am DentAssoc 1987:n4;76-77
51. Ronquilo HI, Gray J, Tallants RH Tomographic analysisof mandibular condyie position as compared to arthro-graphic findings of the temporomandibuiar joint. JCraniomandib Disord 1988;2:59-64.
52. Brand JW, Whinery JG, Anderson QN. Condylar positionas a predictor of temporomandibular joint internalderangements. Oral Surg Oral Med Oral Pathol 1989;67;469-476,
53. Dixon DC, Diagnostic imaging of the temporomandibularjoint. Dent Clin North Am 1991;35:53-74,
54. Leidberg J, Rohiin M, Westesson PL, Observer perfor-mance in assessment of condylar positiun in temporo-mandibular joint radiographs. Acta Odontol Scand1985;43;53-58,
55. Laskin D, Greenfield W, Gale E Rugh J, Neff P, Ailing C,Ayer WA (eds). The President's Conference on theExamination. Diagnosis, and Management ofTemporomandibular Disorders, Chicago; American DentalAssociation, 1982.
56. Griffiths RH. Report of the President's Conference on theExamination, Diagnosis, and Management of Temporo-mandibular Disorders. ¡ Am Dent Assoc 1983;106;75-77.
57 McNeil D, Mohl ND, Rugh JD, Tanaka TT Temporo-mandibular disorders; Diagnosis, management, educationand research. J Am Dent Assoc 1990:120:253-269.
58. Laskin DM, Greene CS. Diagnostic methods for temporo-mandibular disorders: What have we learned in twodecades? Anesth Prog 1990:37;56-71.
59. Pullinger AG, Hollender L. Variation in condyle-fossarelationships according to different methods of evaluationin tomograms. Oral Surg Oral Med Oral Patbol 1986;62;710-727
60. Girardot RA, The nature of condylar displacement itipatients with temporomandibular pain-dysfunction.OrtbodRev 1987:l;16-23,
61. American Dental Association Council on DentalMaterials, Instruments, and Equipment. Recommen-dations in radiographie practices, 1984. J Am Dent Assoc1984;109;764-765,
62. American Academy of Craniomandibular Disorders,Craniomandibular disorders; guidelines for evaluation,diagnosis, and management, Chicago; Quintessence, 1990:25-33.
63. Cordray FE. The relationship of occlusion to TMD.Presented to the Northeast Society of Orthodontists,New York City, Deeember 1997
64. Utt TW. Meyers CE, Wierzba TF, Hondmm SO. A three-dimensionaj comparison of eondylar position changesbetween centric relation and centric occlusion using theMandibular Position Indicator. Am [ Orthod 1995:107:298-308.
65. Hoffman PJ, Silverman SI, Garfinkel L. Comparison ofcondylar position in centric relation and in centric occlu-sion in dentulous patients, J Prosthet Dent 1973:30;582-588.
66. Rosner D, Goldberg GF Condylar retruded contact posi-tion and intercuspal position and correlation in dentulouspatients. 1. Three dimensional analysis of condylar regis-trations. I Prosthet Dent 1986:56;230-239.
67. Esmay TR. The Relationship of Condylar PositionCbanges Between Centric Relation and MaximumIntercuspation in Orthodontic Treated and Non-Orthodontic Treated Individuals, [thesis]. New York; NewYork University, 1995 [unpublisbed],
68. Girardot A. Contemporary comprehensive clinical ortho-dontics, Ohio State Ortbodontic Alumni FoundationMeeting, Columbus, Ohio. March 1998,
292
Cord ray
69,
71.
Okeson J, Inter-disciplinary treatment: TMJ, AnnualSession of the Ameriean Association of Orthodontists,Dallas. Texas, May 1999,McNeil C, Inter-disciplinary treatment: TfWJ, AnnualSession of the American Association of Orthodontists,Dallas, Texas, May 1999,Williamson EH. Temporomandibular dysfunction in pre-treatment adolescent patients. Am J Orfhod 1977:72-429-433,Wigdorowica-Makowerowa N, Crodzki C, Panek H,Maslanka T, Plonka K, Palacha A, Epidemiológica! studieson prevalence and etiology of functional disturbances ofthe masticatory system, J Prosthet Dent 1979:41:76-82,Grosfeld O, Jaekovvska M. Czarnecka B, Results of epi-demiologieal examinations of the temporomandibularjoint in adolescents and young adults, J Oral Rehabil1985:12:95-105,
Nilner J, Lassing SA, Prevalence of functional distur-bances and diseases of tbe stomatognathic system in 7-14year olds. Swed Dent J 1981:5:173-188.Egermark-Eriksson 1, Carlson GE, Ingervall B, Prevaleneeof mandibular dysfunction and orofacial parafunction in7-, 11-, 15-year-old Swedisb children. Eur ] Orthod1981,3:163-172,Vlazis AD. Atlas of Orthodontics: Principles and ClinicalApplications. Philadelphia: Saunders, 1993,Wasseil RW, Do occlusal factors play a part in dysfunc-tion? J Dent 1989;17(3):101-I10.Karl PJ, Foley TF. The use of a deprogramming applianceto obtain centrie relation records. Angle Orthod 1999:59:117-125.Lucia VO. Modern Gnathological Coneepts-tJpdated,Chicago: Quintessence,1983:39-53,Pruim GJ, Dejongh HJ, Ten Bosch JJ, Forces acting on themandible during bilateral static bite at different force lev-els. J Blomech 1980:13:755-763.Teo CS, Wise MD, Comparison of retruded axis artieulatormountings with and without applied muscular force. JOral Rehabil 1981;8;363-376,Hannam AG. Regulation of tbe jaw bite force in man.Arch Oral Biol 1976;21:641-644,Throciimorton GS, Groshan GJ, Boyd SB. Muscle activitypatterns and control of temporomandibular joint loads.J Prosthet Dent 1990:63:685-695,Lucia VO, A technique for recording centric relation.J Prosthet Dent 1964.14:492-505.Long JH, Locating centric relation with a leaf gauge.J Prosthet Dent 1973;29:608-610.Woeffel JB. Sliding and guiding the mandible into theretruded arc without pushing, Compend Contin EdueDent 1991:12:614-623.Kantor ME, Silverman SI, Garfinkel L. Centric relationrecording technics-A comparative investigation.J Prosthet Dent 1972;28:593-600.Lee SH, Woelfel JB. Suggested modifications for the leafwafer system. J Prosthet Dent 1991:65:287-289Shankland WE, Ralston SJ, The fabrication and use of aleaf gauge to locate centric relation, Ohio Dent] 1983;57:43-45,
90. Wood DP, Floreani KJ, Galil IÍA, Teteruk WR. The effectof incisai bite force on condylar seating. Angle Orthod1992:64:1-9.
91, Fenlon MR, Woelfel JB, Condylar position recorded usingleaf gauges and specific closure forces. Int | Prosfhodont1993:6:402-408,
92. Greco PM, Vanarsdall RL, An evaluation of anterior tem-poralis and masseter muscle activity in appliance therapy.Angle Orthod 1999:69:141-146,
93, Calagna LS, Silverman SI, Garfinkel L. Influenee of neu-romuscular conditioning on centric registrations. JProsthet Dent 1973:30:598-604.
94. Capp NJ. Clayton JA, A technic for evaluation of centricrelation tooth contacts, 2. Following use of an occlusalsplint for treatment of tem puro mandibular joint dysfune-tion. J Prosthet Dent 1985;54:697-705.
95. Koveleski WC, DeBoever J. Influence of occlusal splintson jaw position and musculature in patients with tem-poromandibular joint dysfunction. J Prosthet Dent1975:33:321-327
96. Hannam AG. DeCou RE, Scott JD, Wood WW Tbe rela-tionship between dental occlusion, muscle activity, andassociated jaw movement in man. Arch Oral Biol 1977:22:25-32,
97, Solberg WK, Clark GT, Rugh JD, Nocturnal EMG evalua-tion of bruxism patients undergoing short-term splint ther-apy. J Oral Rehabil 1975:2:215-223,
98, McNeill C, Danzig WM, Parraw WB, et al. Cranio-mandibular disorders-The state of the art, J Prosthet Dent1980:44:434-437
99, Williamson EH, Evans DL, Barton WA, Williams BH, Theeffect of biteplane use on terminal hinge axis location.Angle Orthod 1977:47:25-33,
100. Wood CR. Centrieally-related cephalometrics. Am JOrthod 1977:71:156-172.
101. Williamson EH, Caves SA, Edenfield RJ, Morse PK.Cephalometric analysis: Comparisons between Ml andCR, Am J Orthod 1978:74:672-677,
102. Sbildkraut M, Wood DP, Hunter WS, The CR-CO discrep-ancy and ils effect on eephalometric measurements. AngleOrthod 1994,64:333-342.
103. Roth RH. Treatment mechanics for the straightwire appli-ance. In: Graber TM, Swain BF (eds). Orthodontics:Current Prineiples and Teehniques, St Louis: Mosby,1985:665-716.
104. Ricketts RM, Roth RH, Chaconas SJ. OrthodonticDiagnosis and Planning, Denver: Rocky MountainOrthodontics, 1982:293-298,
105. McHorris WH. Occlusion-With particular emphasis onthe functional and parafunctional role of anterior teeth, Jdin Orthod iy79;l 3:606-620.
106 Pameijer J, Periodontal and Oeclusal Factors in Crownand Bridge Proeedures, Amsterdam: DeBussy, 1985,
107 Ackerman J, Proffit W. Soft tissue limitations in orthodon-tics: Treatment planning guidelines. Angle Orthod1997;67:327-336.
293




![Conservative Approach to Unilateral Condylar Fracture in a … · 2016-10-09 · of condylar fractures [7]. It appears that pediatric condylar fractures could be managed by closed](https://img.pdfslide.us/doc/110x75/5f48360e47a39a42e102f2f1/conservative-approach-to-unilateral-condylar-fracture-in-a-2016-10-09-of-condylar.jpg)
![Oral & Maxillofacial Surgeryopenaccessebooks.com/oral-maxillofacial-surgery/condylar-fractures.pdftreatment of mandibular condylar process fractures [10]. It was found that treatment](https://img.pdfslide.us/doc/110x75/5e27326a457720282958fba6/oral-maxillofacial-sur-treatment-of-mandibular-condylar-process-fractures.jpg)


![Condylar Resorption - d39pscuc60gk9c.cloudfront.net€¦ · of condylar resorption. Kerstens and colleagues [4] reported on 12 of 206 patients with high-angle mandibular retrognathia](https://img.pdfslide.us/doc/110x75/5ed6b8fde3edf541e3459c3d/condylar-resorption-of-condylar-resorption-kerstens-and-colleagues-4-reported.jpg)